coniotomy - tracheotomymedia.bsbb.de/dif/delank.pdf · große struma trachealdeformitäten...
TRANSCRIPT

Coniotomy - TracheotomyK.-W. Delank
HNO-Klinik Klinikum Ludwigshafen/Rhein

….. direct and safe gateway to the windpipe
… a simple hole

???
Front or Rear ??
Take notice of the margins !

Pars cartilaginea + Pars membranacea
variable and mobile
Anatomy of the upper Airways
Variation of
Cross Section and Length
Age
Gender
Cricothyroid Membrane
1 Hyoid
2 Larynx
3 Cricoid
4 Trachea
Swallowing
Neck
movements

Cervical landmarks
- Coniotomy -
ICA
IJVN

Cricothyreoidotomy (Coniotomy)
Tools and Technique
QuickTrach®
Disposable Set for Coniotomy

Indications or Coniotomy
can„t intubate - can„t ventilate

Cervical landmarks
Tracheotomy
up to 5 cm
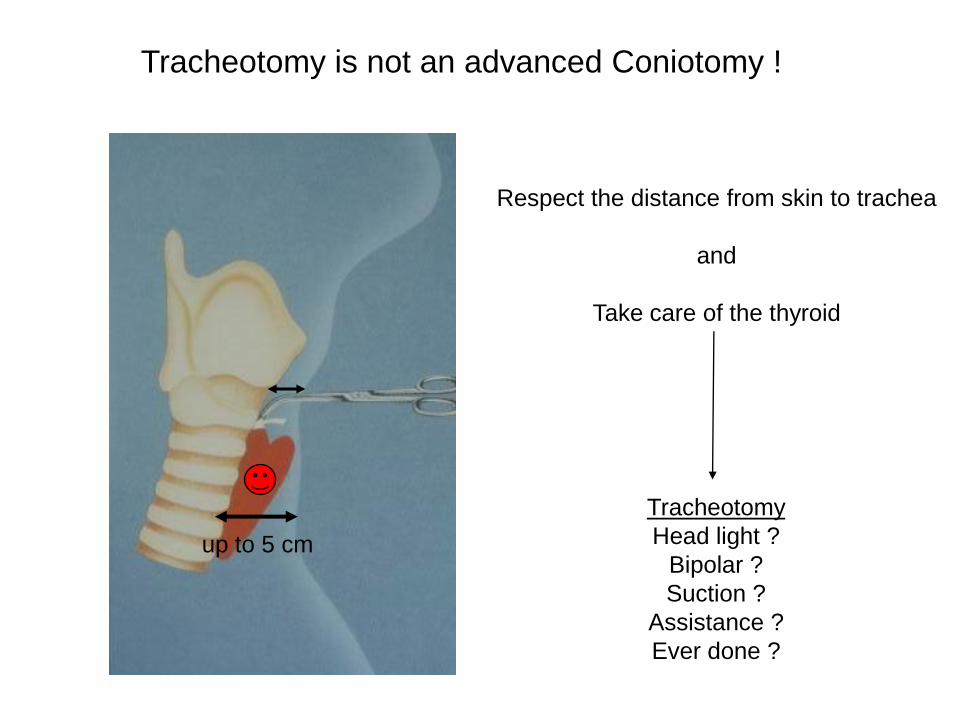
Respect the distance from skin to trachea
and
Take care of the thyroid
Tracheotomy is not an advanced Coniotomy !
Tracheotomy
Head light ?
Bipolar ?
Suction ?
Assistance ?
Ever done ?
up to 5 cm

ElectiveEndolaryngeal / transcervical
Oncosurgery
Pre- RCTX
Long- term ventilation
Prevalence of tracheotomy in HNSCC
T1 – T 2 b: < 10%
T3 : 30%
supraglottic tumors : 60%
microvascular tissue transfer: > 90%
Indications for “Surgical” TracheotomySaving the Airways – Prevention of Aspiration – Protection of Surgical Results
UrgentlyTrauma
Tumor
Inflamation
Dysmorphia
Revision
Coagulation
disorders

Minimally- Invasive Technique ???
Visor Tracheotomy !H TUResection or insertion of
the cartilage

Horizontal or Vertikal Skin Incision ?
surgical
overview
cosmetically
outcome
horizontal vertical

Tracheal Stenosis
Dislocation/ Via falsa
Cannula
Trachea
Emphysema
Bleeding
intraop./postop.
Complications and Risks
Infection/Granulation

Dislocation of tracheal cartilage
after tracheotomy
Risk of Stenosis
Horizontal incision
Vertical incision
H-shaped incision
Inverted U-Flap
Resection of cart.


Alternatives ?

„ No.1“
Modified Ciaglia Technique
Single-Step Dilatation
Blue Rhino© Ultra Perc©

less logitic agreements
spontaneous closure of the tracheostoma
less infections
less expensive
less effort in time (controversial)
operable at the beside (controversial)
better cosmetically results (controversial)
Advantages of Percutaneous Tracheotomy
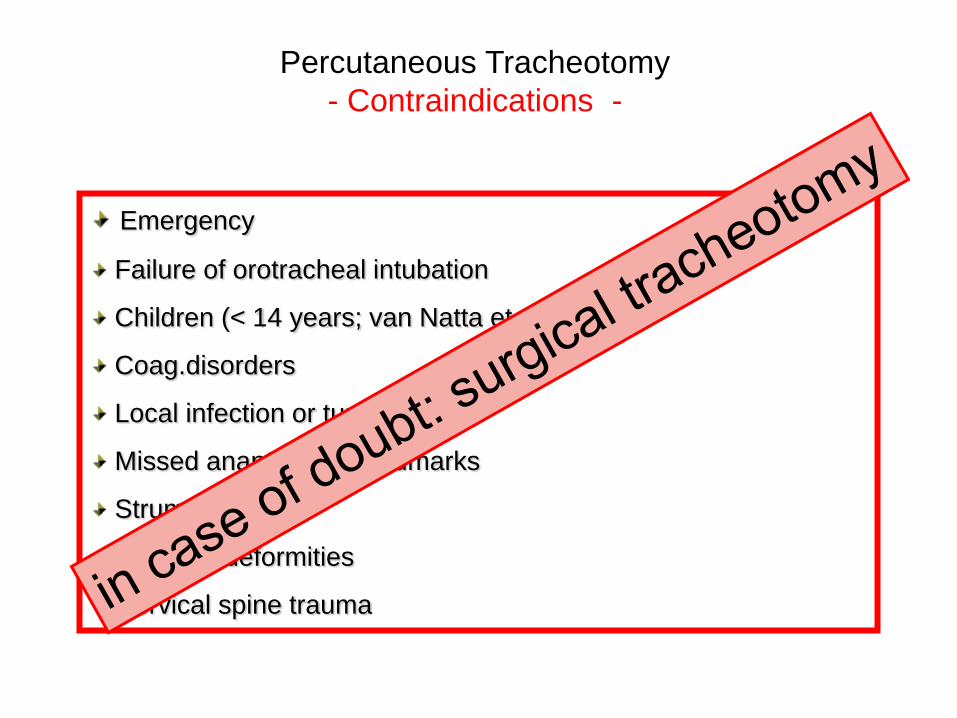
Emergency
Failure of orotracheal intubation
Children (< 14 years; van Natta et al. 2006)
Coag.disorders
Local infection or tumor
Missed anantomical landmarks
Struma °IV
Tracheal deformities
Cervical spine trauma
Percutaneous Tracheotomy
- Contraindications -
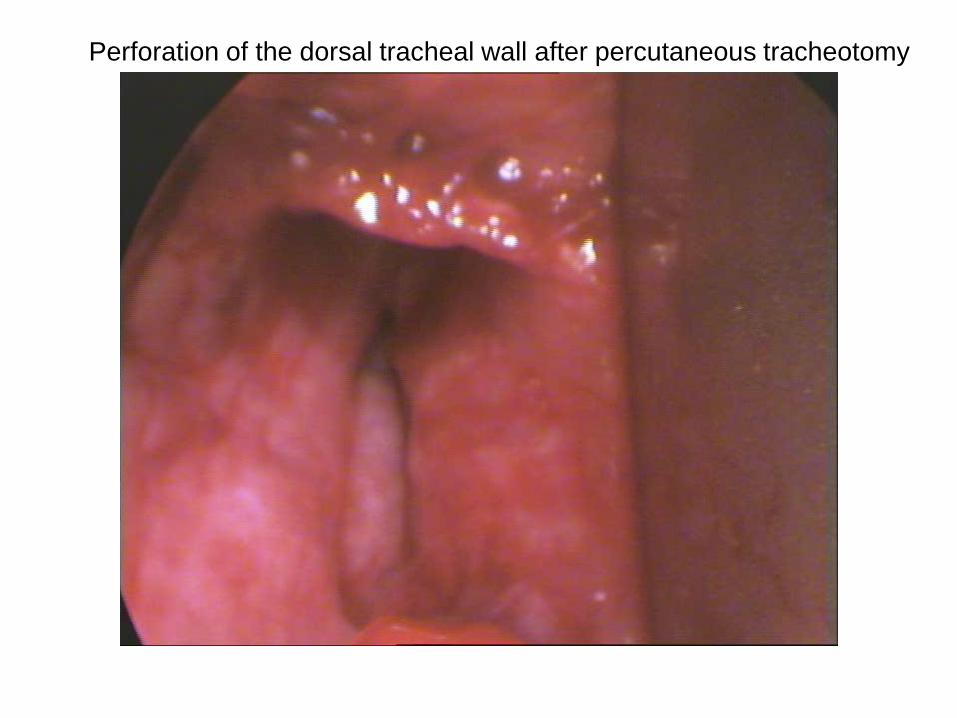
Perforation of the dorsal tracheal wall after percutaneous tracheotomy


„Landmarken“ nicht abgrenzbar
Große Struma
Trachealdeformitäten
Instabile Halswirbelsäule
Erhöhter ICP (Lagerung)
Geplantes endgültiges Tracheostoma
Notwendige Trachealkanüle > 9,0 mm
Perkutane Tracheotomie
- Kontraindikationen II -
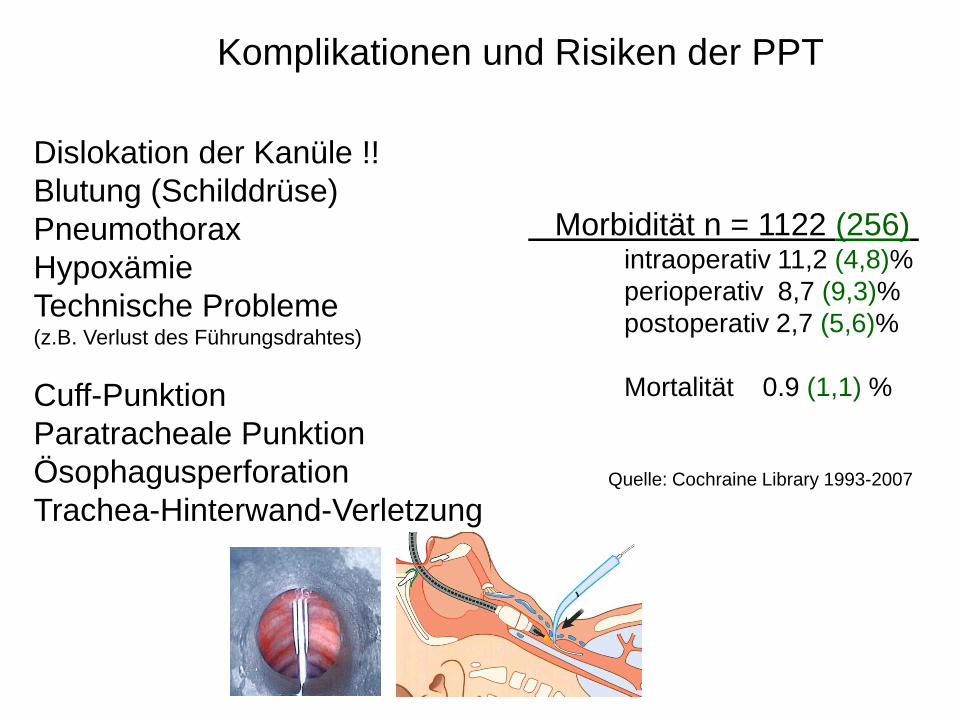
Komplikationen und Risiken der PPT
Dislokation der Kanüle !!
Blutung (Schilddrüse)
Pneumothorax
Hypoxämie
Technische Probleme(z.B. Verlust des Führungsdrahtes)
Cuff-Punktion
Paratracheale Punktion
Ösophagusperforation
Trachea-Hinterwand-Verletzung
Morbidität n = 1122 (256)intraoperativ 11,2 (4,8)%
perioperativ 8,7 (9,3)%
postoperativ 2,7 (5,6)%
Mortalität 0.9 (1,1) %
Quelle: Cochraine Library 1993-2007

Shelden: 1. perkutane Tracheotomie mittels Trokar (1955)
Toye und Weinstein: PT mittels Seldingertechnik (1969)
Ciaglia: Erste Dilatationstracheotomie mittels
Seldingertechnik und Bougierung (1985)
Modifikationen der Ciaglia-Technik:
Dissektionstracheotomie: Schachner (1989) und Griggs (1990)
Fantoni: Translaryngeale Durchzugstracheotomie (1997)
PercuTwist: A new single- dilator- technique
Frova G, Quintel M (2002)
Historie der perkutanen Tracheotomietechniken

„Der Klassiker“
Dilatationstracheotomie nach Ciaglia (1985)
Punktion der Trachea
Führungsdraht
Dilatation mit abgestuften Dilatatoren
Punktion mit Bronchoskopie
Insertion des Seldingerdrahtes
Bronchoskopische Kontrolle
Hautinzision
Weitung mit Dilatatoren

„ Die rote Methode “
Methode nach Griggs (1990)
Punktion der Trachea
Führungsdraht
Weitung des Punktionskanals mittels Spreizpinzette
Höchstes Blutungsrisiko aller Methoden

„ Die Schraube “
Dilationstracheotomie nach Frova und Quintel (2002)
Große Akzeptanz unter Intensivmedizinern
Dilatation mittels konischer Schraube mit
selbstschneidendem Gewinde

„Die andere Methode“
Translaryngeale Durchzugstracheotomie nach Fantoni
(1997)Punktion der Trachea
Führungsdraht nach kranial
Dilatation von innen nach außen
Vorteil: Kein Druck auf Trachea und HWS
Nachteile: - Technisch anspruchsvoll
- Umintubation erforderlich

Alternative: „Notrohr“

Vaskularisation der Trachea
• A. thyroidea inferior
• Gefäße liegen an der Tracheaseitenwand
• vaskuläres “Strickleiter”-System

Halskonturen und Landmarken
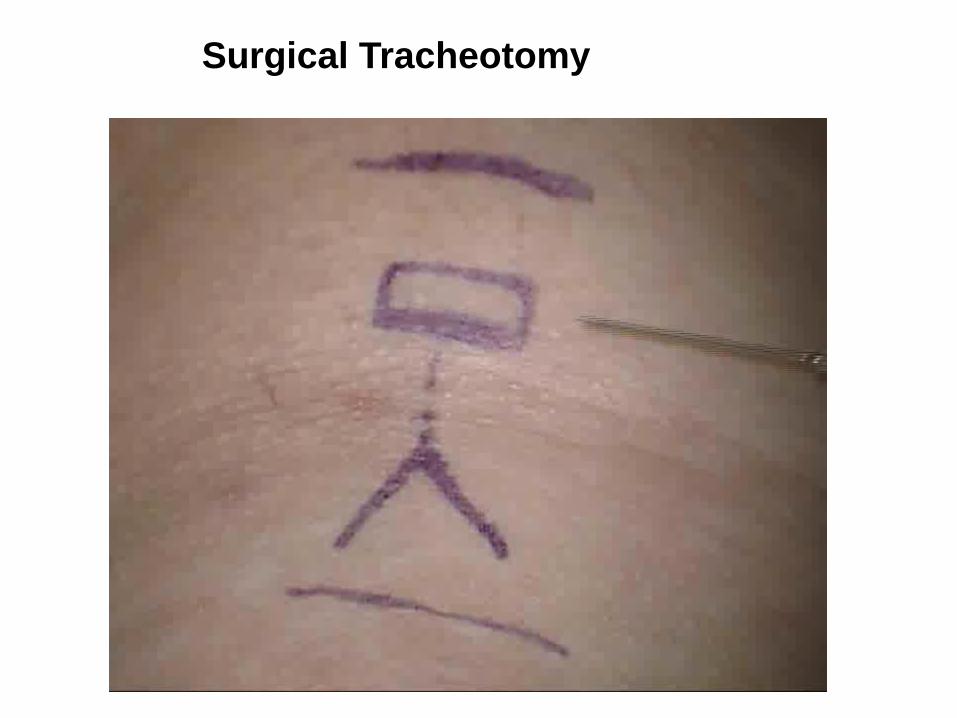
Surgical Tracheotomy

0
1
2
3
4
5
6
Dyspnoe Wundheilungstörung
1 2 3 4 5 6 7 7-22 ab 22
n = 219; Alter: 6 – 82 Jahre
Plastischer Tracheostomaverschluss: ambulant oder stationär ?