complex stroke cases and barriers in psc and cscwcm/@mwa/documents/... · complex stroke cases and...
TRANSCRIPT
Complex Stroke Cases and
Barriers in PSC and CSC
Marc A. Lazzaro, MD Assistant Professor of Neurology and Neurosurgery
Interventional and Vascular Neurology
Froedtert and Medical College of Wisconsin
June 14, 2013 Wisconsin Coverdell Stroke Program

Disclosures
• No financial interest in any product or manufacturer mentioned herein.

Outline
• Stroke center designations
– Comprehensive Stroke Center
– Primary Stoke Center
– Acute Stroke Ready Hospital
• Advanced stroke therapy cases
• Triage, transport, and transfer planning
– Statewide
– Regional

Stroke center designations
Acute Stroke Ready hospital (2015?) •Serves rural population where large distance from PSC or CSC •Designation not yet available
Primary Stroke Center (PSC) 2003 •Acute stroke team •Emergency department •Stroke unit •Neurosurgical services •Imaging, laboratory services •Rehab services •Stroke registry with outcomes •Educational programs
Comprehensive Stroke Center (CSC) 2012 •PSC requirements and… •Volume criteria
•Aneurysm coiling/clipping •IV tPA administration
•Catheter angiography and advanced imaging •NICU with dedicated beds •Peer review •Stroke research •Performance measures

What is certification?
• Certification recognizes centers that follow best
practices for stroke care
• Driven by randomized data, guidelines, and
consensus opinion
• Expectations include – Standardized delivery of care
– Demonstrate compliance with clinical practice guidelines by the
AHA/ASA or equivalent evidence-based guidelines.
– Performance measurement and improvement

Benefit of CSC
Benefit of CSC –Meretoja et al.
• Study of effectiveness of PSCs and CSCs in Finland
• > 61,000 patients included
• Centers defined by most of criteria published by
BAC
• Compared patients with 1st time ischemic stroke
admitted to PSC/CSC vs general hospital
• Triage largely determined by geography
Meretoja A, et al. Stroke 2010; 41:1102-1107.

Benefit of CSC –Meretoja et al.
• CSC/ PSC compared with the general hospitals
CSC PSC
1 year case-fatality reduction 16% 11%
Absolute reduction in death 2.4% 1.5%
Absolute risk reduction of institutional care at 1 year
1%
Meretoja A, et al. Stroke 2010; 41:1102-1107.

Outline
• Stroke center designations
– Comprehensive Stroke Center
– Primary Stoke Center
– Acute Stroke Ready Hospital
• Advanced stroke therapy cases
• Triage, transport, and transfer planning
– Statewide
– Regional
Acute Stroke Case #1
• 52 yo M h/o hyperlipidemia
• 2 weeks of severe coughing
• Presented with a left middle
cerebral artery (MCA) stroke
syndrome.
• NIHSS 19.
• Unknown onset. Last known
well 4.5 hours.

Acute Stroke Case #1

Aneurysmal subarachnoid
hemorrhage case
• 30 year old woman
presented with “worst
headache of life” and
nausea.
• CT head showed
diffuse subarachnoid
hemorrhage

Aneurysmal subarachnoid
hemorrhage case
• Catheter angiogram showed a right
anterior choroidal artery aneurysm.

Outline
• Stroke center designations
– Comprehensive Stroke Center
– Primary Stoke Center
– Acute Stroke Ready Hospital
• Advanced stroke therapy cases
• Triage, transport, and transfer planning
– Statewide
– Regional

Muliple Critical Access Hospitals -Future “Acute Stroke Ready” Hospitals?
Wisconsin Stroke Centers
2 Comprehensive Stroke Centers
29 Primary Stroke Centers

Ideal regional stroke system elements
• Patient-centered
• Organized
• Standardized
• Fast
• Non-duplication of services

Stroke system models
• Trauma model

Trauma centers
Trauma centers (Level 1)
http://www.emergencymap.org/Trauma.aspx

Trauma centers (Level 1,2,3) Stroke centers (CSC, PSC, ASR)
Trauma centers

Trauma center transport times
45 minute transport zones to Level 1/2 (purple regions) • Air or ambulance • Base helipads
indicated by stars

Trauma center transport times
60 minute transport zones to Level 1/2 (purple regions) • Air or ambulance • Base helipads
indicated by stars

60 min stroke center access
60 minute transport zones (purple regions) to potential advanced stroke center locations • Air or ambulance

60 min stroke center access
Tertiary referral to Comprehensive Stroke Center • Air transport

Primary stroke center
Comprehensive stroke center Regional Triage?

45 min ground transport to CSC in Milwaukee
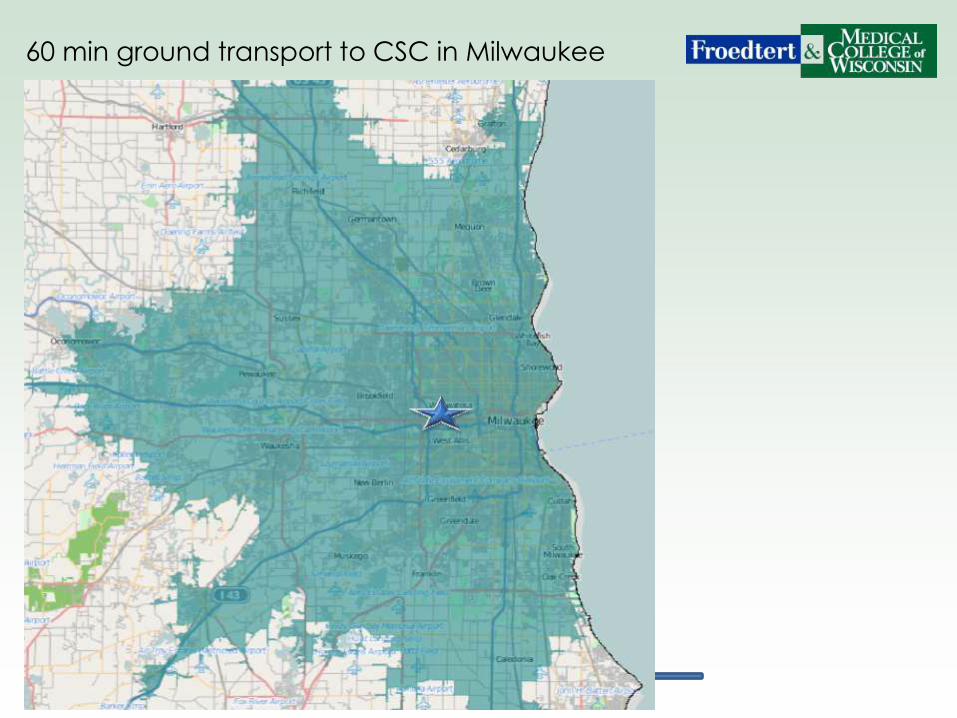
60 min ground transport to CSC in Milwaukee
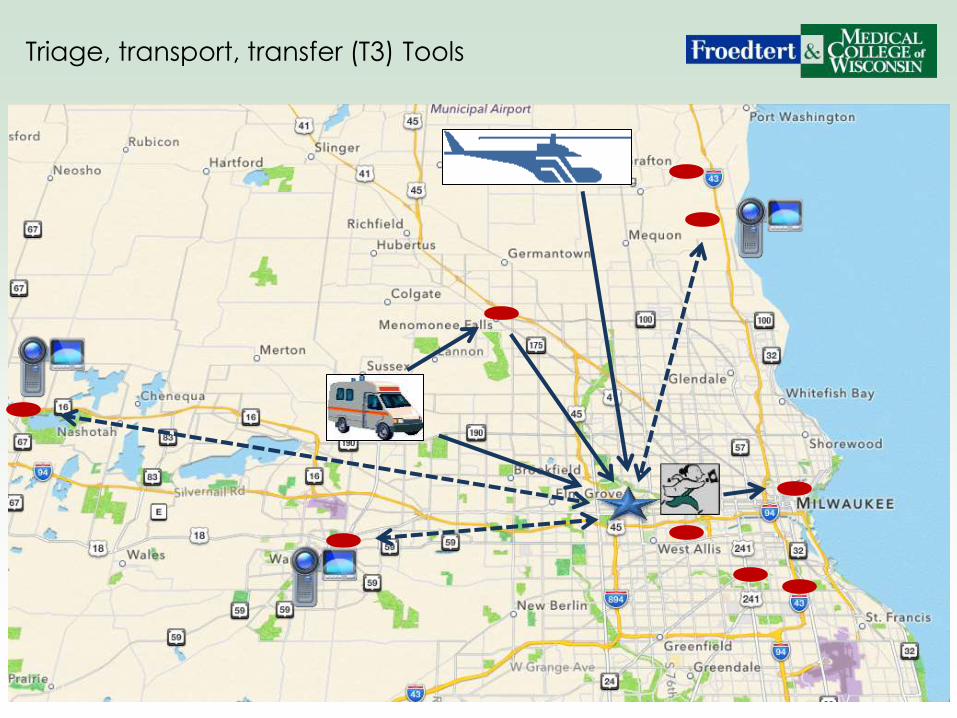
Triage, transport, transfer (T3) Tools

Triage by severity and time

Triage dilemma
• Patients need to be treated FAST
• Severely affected patients may benefit from a CSC
which may require longer transport.
Triage by severity and time
• Time remains the most important variable affecting
response to treatment.
• Guidelines have promoted triage of stroke patients to the
nearest Primary Stroke Center (PSC)
– This has resulted in an increase in delivery of IV tPA
• However, IV tPA does not work well with large blood
vessel blockages
Grotta JC. Stroke 2013; 44:555-557
Early Recanalization
• The greatest benefit is achieved with EARLY IV tPA
administration (early recanalization)
– Greatest benefit within 90 minutes1
• Strong correlation between recanalization and
good functional outcome at 3 months when
compared with non-recanalized patients.2
– Odds ratio 4.43 [95% CI, 3.32 to 5.91]
1. Hacke W et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet. 2004;363:768-774
2. Rha JH et al. The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke 2007;38:967-73.

Optimizing revascularization
• Location of vessel occlusion is important
Small vessel occlusions

Optimizing revascularization
• Location of vessel occlusion is important
Medium and large vessel occlusions

Thrombolysis in small vessel
disease
• A good outcome from IV
thrombolysis is more common in
stroke due to small vessel disease
than other subtypes1
– 957 patients treated with IV tPA
Stroke Subtype n Excellent outcome, mRS 0-1
Large artery atherosclerosis 217 (23%) OR 0.69 [CI 0.5 – 0.96]
Cardioembolic 389 (41%) OR 0.80 [CI 0.61 – 1.06]
Small vessel disease 101 (11%) OR 2.48 [CI 1.63 – 3.79]
Other 27 (2.8%) OR 0.32 [CI 0.11 – 0.94]
Undetermined 130 (14%) OR 1.85 [CI 1.27 – 2.70]
1. Mustanoja, S et al. Outcome by stroke etiology in patients receiving thrombolytic treatment: Descriptive Subtype Analysis. Stroke. 2011;42:102-106

Optimizing revascularization
• Distal vessel occlusions are more likely to
recanalize with IV tPA than larger proximal
vessels1
• 335 patients, median baseline NIH = 16,
mean time to IV tPA = 145 +/- 68 minutes
Location OR for complete
recanalization Number of patients
Distal MCA 2 50 of 113 (44.2%)
Proximal MCA 0.7 49 of 163 (30%)
Terminal ICA 0.1 1 of 17 (5.9%)
Tandem cervical ICA and MCA
0.7 6 of 22 (27%)
Basilar 0.96 3 of 10 (30%)
1. Saqqur, M et al. Site of arterial occlusion identified by TCD predicts response to IV thrombolysis for stroke. Stroke. 2007; 38:948-954.

ENDOVASCULAR THERAPY
Time-Location Based Recanalization
0 3 4.5 8 6 Hours
Clot
Location
Small Vessel
Large Vessel
IV tPA
IA -tPA
MECHANICAL THROMBECTOMY
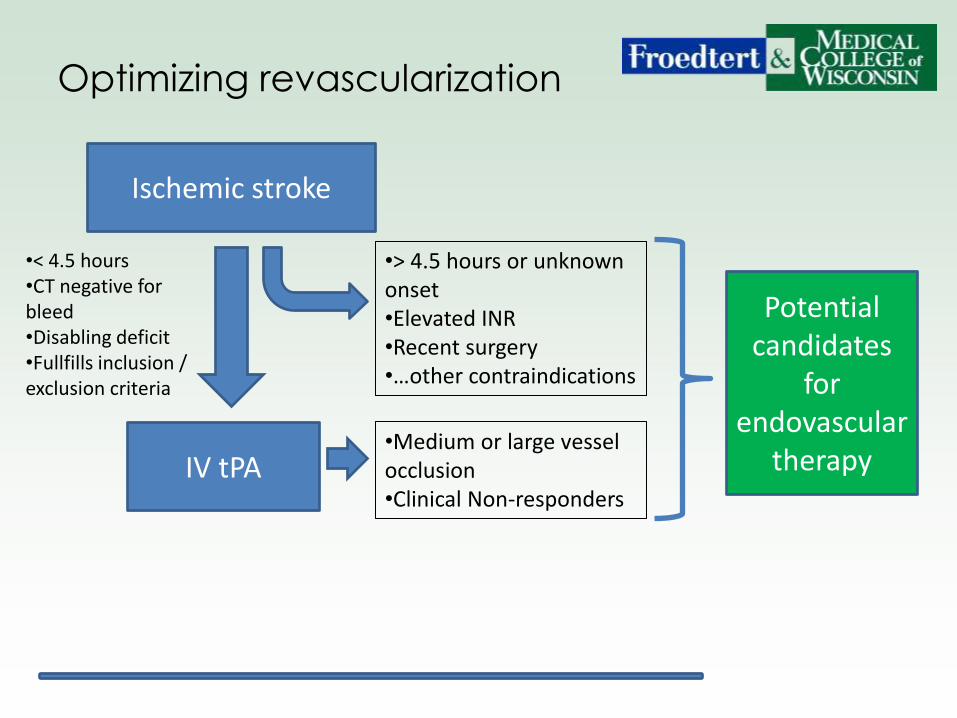
Optimizing revascularization
Ischemic stroke
•< 4.5 hours •CT negative for bleed •Disabling deficit •Fullfills inclusion / exclusion criteria
IV tPA
•> 4.5 hours or unknown onset •Elevated INR •Recent surgery •…other contraindications
•Medium or large vessel occlusion •Clinical Non-responders
Potential candidates
for endovascular
therapy

Endovascular therapies for
acute ischemic stroke
• Intra-arterial tPA
– Several randomized trials and case series have led to endorsement by multiple organizations
– American Heart Association recommendation for endovascular stroke therapy:1
• Class I, Level of evidence B recommendation for IA thrombolysis in select patients under 6 hours from symptom onset due to MCA occlusion
• Class II, Level of evidence B recommendation for mechanical thrombus extraction
1. Meyers, PM et al. Indications for the Performance of Intracranial Endovascular Neurointerventional Procedures. Circulation. 2009;119:2235-2249
Stroke triage
• Patients with severe stroke syndromes suggestive of a
large artery blockage may benefit from the longer transit
time to a CSC
• These centers may be able to offer more comprehensive
therapies for these complex stroke patients
– Endovascular clot removal
– Hemicraniectomy
– NICU care
Grotta JC. Stroke 2013; 44:555-557
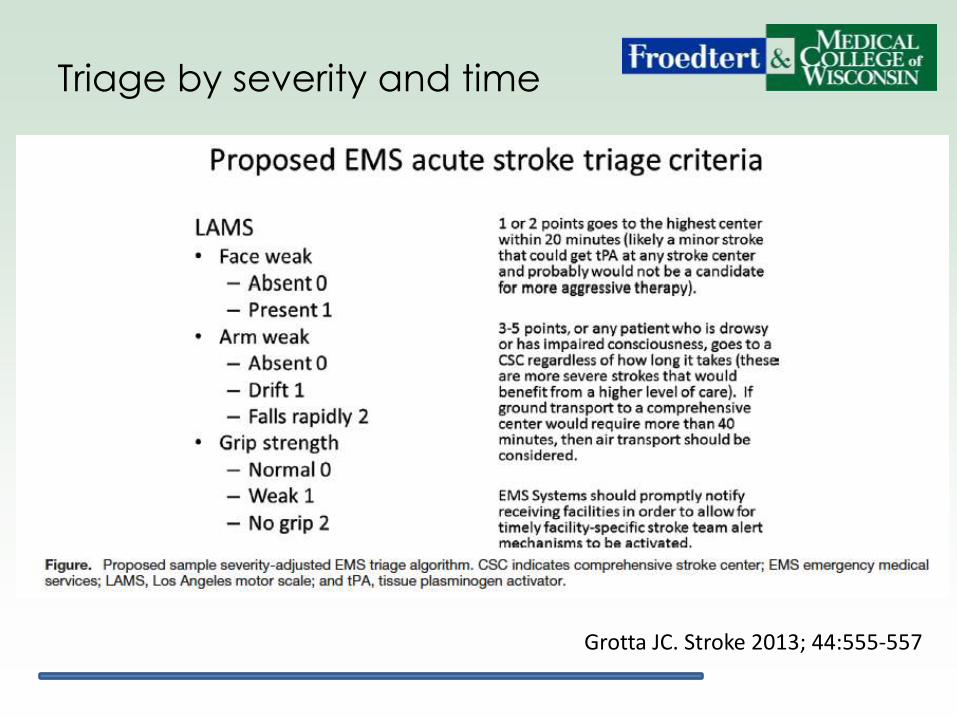
Triage by severity and time
Grotta JC. Stroke 2013; 44:555-557

Tiered regional EMS triage

Tiered regional EMS triage
Tier One: Mild stroke symptoms • LAMS score 1-2
Triage to highest center within 20 minutes • Likely needs IV tPA, less likely needs
more aggressive therapy
45 minute ground transport region marked in green

Tiered regional EMS triage
Tier Two: Moderate to severe stroke symptoms • LAMS score 3-5, or drowsy, or impaired
consciousness
Triage directly to comprehensive stroke center
45 minute ground transport region marked in green
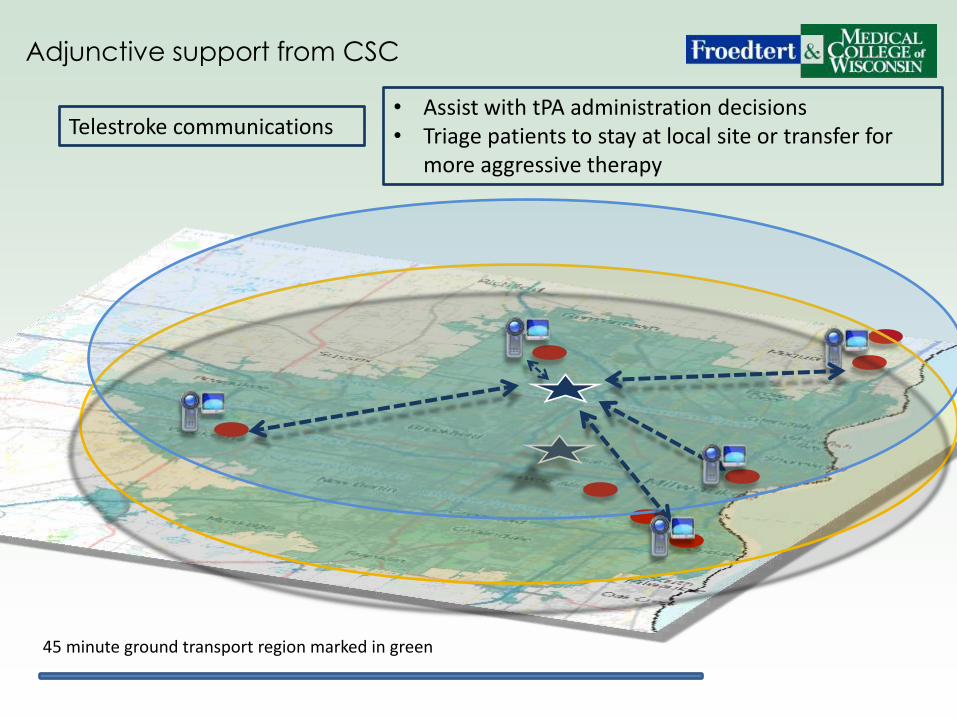
Adjunctive support from CSC
Telestroke communications • Assist with tPA administration decisions • Triage patients to stay at local site or transfer for
more aggressive therapy
45 minute ground transport region marked in green
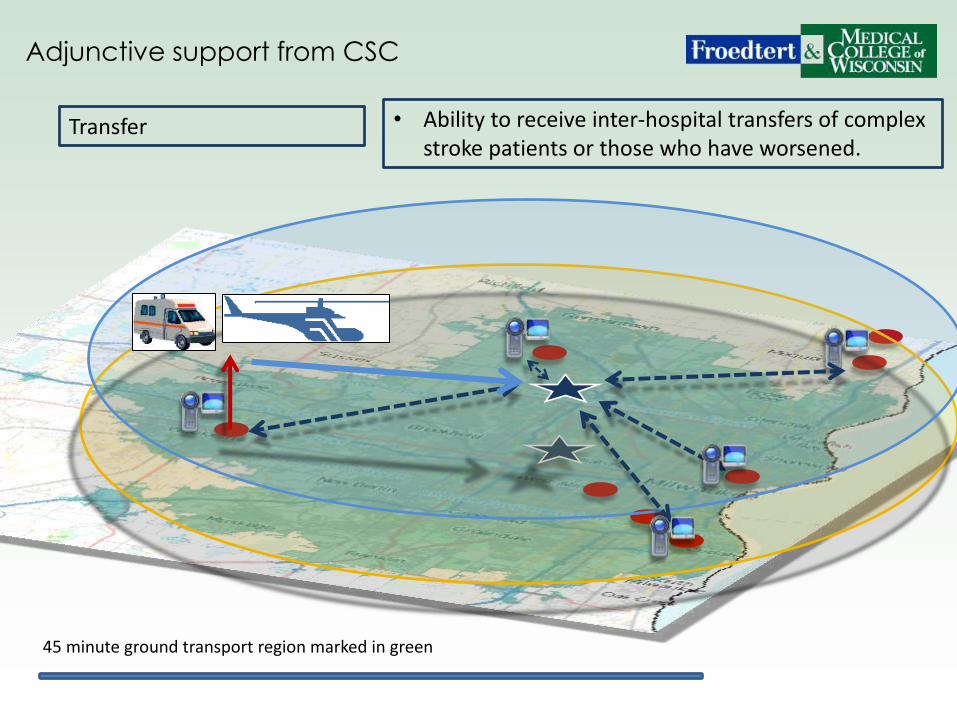
Adjunctive support from CSC
Transfer • Ability to receive inter-hospital transfers of complex stroke patients or those who have worsened.
45 minute ground transport region marked in green

Thank you for your attention
Marc Lazzaro, MD