complete revascularization in elderly - when it’s contraindicated
DESCRIPTION
COMPLETE REVASCULARIZATION IN ELDERLY - When it’s contraindicated. Giuseppe Biondi-Zoccai S. Giovanni Battista “Molinette” Hospital University of Turin. 3rd International Interventional Forum – Turin, 18 January 2008 (h 12.20-12.40). Learning goals. - PowerPoint PPT PresentationTRANSCRIPT
www.metcardio.org
COMPLETE REVASCULARIZATION IN COMPLETE REVASCULARIZATION IN
ELDERLY - When it’s contraindicatedELDERLY - When it’s contraindicated
Giuseppe Biondi-ZoccaiGiuseppe Biondi-Zoccai
S. Giovanni Battista “Molinette” Hospital
University of Turin
3rd International Interventional Forum – Turin, 18 January 2008 (h 12.20-12.40)

www.metcardio.org
Learning goals
• How do you define complete
revascularization (MVD)?
• What is the risk-benefit balance of culprit
vs multivessel PCI in stable MVD?
• What is the risk-benefit balance of culprit
vs multivessel PCI in acute MVD?
• When is complete revascularization
contraindicated in the elderly?

www.metcardio.org
To achieve a greater To achieve a greater
understanding, let us begin with understanding, let us begin with
an example from a related field…an example from a related field…

www.metcardio.org
Is it safer to target one only?

www.metcardio.org
Is it safer to target one only?

www.metcardio.org
Or all of them at once?

www.metcardio.org
Learning goals
• How do you define complete
revascularization (MVD)?

www.metcardio.org
Defining revascularization
I.I. Anatomically completeAnatomically complete:: PCI of every occluded or stenotic epicardial vessel
II.II.Functionally complete:Functionally complete: PCI of every occluded or stenotic epicardial vessel of adequate size and supplying a zone of viable myocardium
III.III.Incomplete (culprit only):Incomplete (culprit only): PCI of occluded or stenotic epicardial vessel identified by comprehensive clinical judgement as responsible for signs/symptoms of ischemia
IV.IV.Incomplete (truly):Incomplete (truly): everything else

www.metcardio.org
Defining revascularization
I.I. Anatomically completeAnatomically complete:: PCI of every occluded or stenotic epicardial vessel
II.II.Functionally complete:Functionally complete: PCI of every occluded or stenotic epicardial vessel of adequate size and supplying a zone of viable myocardium
III.III.Incomplete (culprit only):Incomplete (culprit only): PCI of occluded or stenotic epicardial vessel identified by comprehensive clinical judgement as responsible for signs/symptoms of ischemia
IV.IV.Incomplete (truly):Incomplete (truly): everything else

www.metcardio.org
23
39
1612 14
20
4852
2836
81
90
9
2114
18
37
47
2 40
15
30
45
60
75
90
Female Obese PriorCABG
PriorPCI
DM HTN Renalfailure
LVEF<35%
3VD ULM
<75 years >75 years
Wiemer et al, AHJ 2004
%
ALL P<0.05
Scope of the problem

www.metcardio.org
Hazards of MVD stenting

www.metcardio.org
Hazards of MVD stenting

www.metcardio.org
Hazards of MVD stenting
Orlic et al, JACC 2004

www.metcardio.org
Learning goals
• What is the risk-benefit balance of culprit
vs multivessel PCI in stable MVD?

www.metcardio.org
TIME trial supports PCI in elderly
Pfisterer et al, JAMA 2003

www.metcardio.org
TIME trial
Pfisterer et al, JAMA 2003

www.metcardio.org
Yet PCI based on oculostenotic reflex
is not always justified in stable MVD

www.metcardio.orgBoden et al, NEJM 2007

www.metcardio.orgBoden et al, NEJM 2007

www.metcardio.org
Symptomatic benefits in the COURAGE trial
Boden et al, NEJM 2007

www.metcardio.org
Evidence in non-randomized trials

www.metcardio.org

www.metcardio.orgIjsselmuiden et al, AHJ 2004

www.metcardio.org
Learning goals
• What is the risk-benefit balance of culprit
vs multivessel PCI in acute MVD?

www.metcardio.org
Early invasive management in elderly with ACS: TACTICS
Study
Brener et al, Am J Cardiol 2002
www.metcardio.org
Yet PCI based only on oculostenotic
reflex is also not justified in acute MVD
Hirsch et al, Lancet 2007

www.metcardio.orgHirsch et al, Lancet 2007

www.metcardio.orgHirsch et al, Lancet 2007

www.metcardio.org
What about complete PCI in STEMI?
Single vs multivessel treatment during primary
angioplasty: results of the multicentre
randomised HEpacoat for cuLPrit or
multivessel stenting for Acute Myocardial
Infarction (HELP AMI) Study.
Di Mario C, Sansa M, Airoldi F, Sheiban I, Manari A, Petronio A, Piccaluga E, De
Servi S, Ramondo A, Colusso S, Formosa A, Cernigliaro C, Colombo A, Monzini N,
Bonardi MA.
Int J Cardiovasc Intervent. 2004;6(3-4):128-33.

www.metcardio.org
53
69
0 3
35
1722 20
0
10
20
30
40
50
60
70
Length ofprocedure
In-hospitalMACE
12-monthrePCI
12-monthcosts
Culprit PCI group Complete PCI group
53 vs 69 minutes, p<0.05
0 vs 4%, p=NS
35% vs 17% p=NS
22,330€ vs 20,382€, p=NS
Di Mario et al, Int J Cardiovasc Intervent 2004
%

www.metcardio.org
Learning goals• When is complete revascularization
contraindicated in the elderly?

www.metcardio.org
Learning goals• When is complete revascularization
contraindicated in the elderly?
• Mainly when its expected benefits do not
overwhelm the expected risks

www.metcardio.org
Lack of symptoms/signs of myocardial ischemia

www.metcardio.org
COURAGE Nuclear Substudy
Shaw et al, AHA 2007
0
5
10
15
20
25
30
Ischemiareduction>5%
No ischemiareduction
Ris
k o
f d
eath
or
MI (
%)
P=0.037

www.metcardio.org
Extremely diffuse disease or challenging lesions

www.metcardio.org
Extremely diffuse disease or challenging lesions
Sianos et al, EI 2005

www.metcardio.orgSianos et al, EI 2005
SYNTAX score

www.metcardio.org
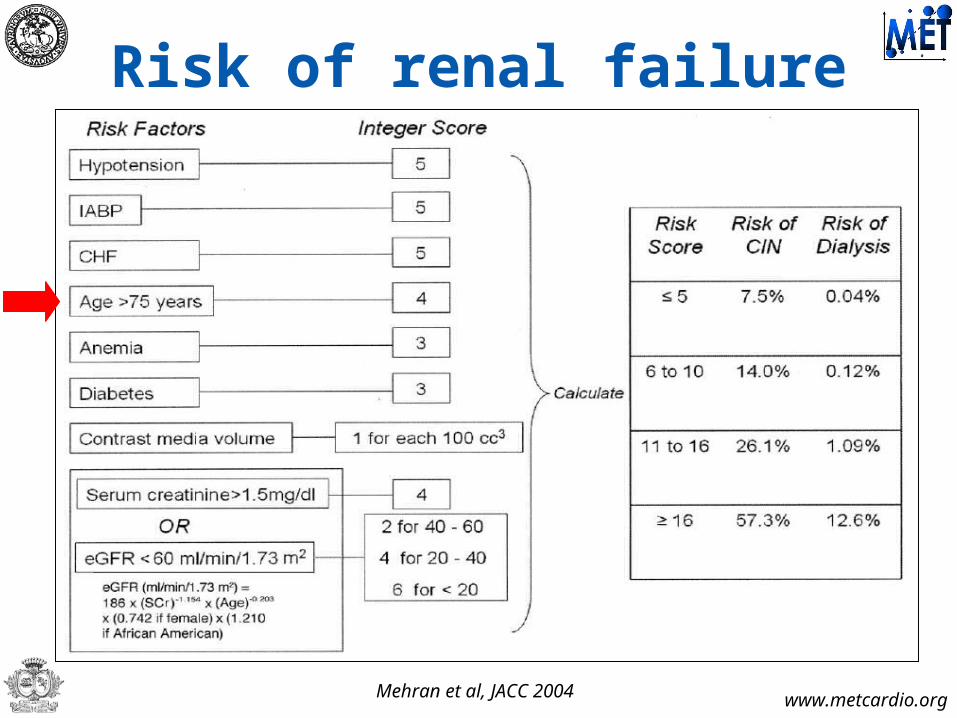
Risk of renal failure

www.metcardio.org
Risk of renal failure
Mehran et al, JACC 2004
www.metcardio.org
Risk of renal failure
Mehran et al, JACC 2004

www.metcardio.org
Increased bleeding risk

www.metcardio.org
Increased bleeding risk
Nikolsky et al, EHJ 2007

www.metcardio.org
Increased bleeding risk
Nikolsky et al, EHJ 2007

www.metcardio.org
Poor compliance or life expectancy

www.metcardio.org
Take home messages

www.metcardio.org
Take home messages
• Current data disCOURAGE from extensive
multivessel PCI based only on
angiographic assessment in stable MVD
• No definite benefits have been shown
from multivessel PCI in patients with acute
CAD and MVD
• According to evidence available to date,
PCI of non-culprit vessels cannot thus be
recommended routinely

www.metcardio.org
Take home messages• Thus, major contraindications to
complete revascularization in elderly are:
Lack of clear-cut signs/symptoms of ischemia Extremely diffuse disease or challenging
lesions Increased bleeding or renal failure risk Lack of compliance or poor life expectancy
• Individualized clinical decision making is pivotal to maximize benefit and minimize risks

www.metcardio.org
For further slides on these topics please feel free to visit the metcardio.org website:
http://www.metcardio.org/slides.html