companion november2010
TRANSCRIPT

The essential publication for BSAVA members
How To…Approach the anorexic catP13
Wildlife WelfareNew initiative at the Royal DickP20
The essential publication for BSAVA members
companionNOVEMBER 2010
Petsavers ProjectResults of urine culture studyP23
Farmyard to backyard
01 OFC.indd 1 20/10/2010 14:52

2 | companion
companion
3 Association News Latest news from BSAVA
4 Thanks to Frank Beattie Karen Wendlandt describes how the Frank Beattie Travel Scholarship award helped her
5–8 Poultry Passions Increasing numbers of clients are keeping poultry as pets; John Bonner reports on what practitioners need to know
9–12 Clinical Conundrum Consider investigation of laboured breathing in a young Springer Spaniel
13–17 How To… Approach the anorexic cat
18–19 Small Animal Medicine Modular An overview of BSAVA’s forthcoming modular courses
20–22 Publications New venture at Edinburgh
23–24 Petsavers Latest fundraising news
25–27 WSAVA News The World Small Animal Veterinary Association
28–29 The companion Interview Harvey Locke
30 Spotlight on Scottish Congress Report on the recent 25th Annual Scottish Congress
31 CPD Diary What’s on in your area
Additional stock photography Dreamstime.com© Andrey Davidenko; © Dmitry Kalinovsky; © Marazem; © Minyun9260; © Reddogs; © Richard Thomas; © Selenka; © Vasiliy Vishnevskiy
companion is published monthly by the British Small Animal Veterinary Association, Woodrow House, 1 Telford Way, Waterwells Business Park, Quedgeley, Gloucester GL2 2AB. This magazine is a member only benefit and is not available on subscription. We welcome all comments and ideas for future articles.
Tel: 01452 726700Email: [email protected]
Web: www.bsava.com
ISSN: 2041-2487
Editorial BoardEditor – Mark Goodfellow MA VetMB CertVR DSAM DipECVIM-CA MRCVSSenior Vice-President – Richard Dixon BVMS PhD CertVR MRCVS FRSE
■■ CPD Editorial TeamIan Battersby BVSc DSAM DipECVIM-CA MRCVSEsther Barrett MA VetMB DVDI DipECVDI MRCVSSimon Tappin MA VetMB CertSAM DipECVIM-CA MRCVS
■■ Features Editorial TeamCaroline Bower BVM&S MRCVSAndrew Fullerton BVSc (Hons) MRCVS
■■ Design and ProductionBSAVA Headquarters, Woodrow House
No part of this publication may be reproduced in any form without written permission of the publisher. Views expressed within this publication do not necessarily represent those of the Editor or the British Small Animal Veterinary Association.
For future issues, unsolicited features, particularly Clinical Conundrums, are welcomed and guidelines for authors are available on request; while the publishers will take every care of material received no responsibility can be accepted for any loss or damage incurred.
BSAVA is committed to reducing the environmental impact of its publications wherever possible and companion is printed on paper made from sustainable resources and can be recycled. When you have finished with this edition please recycle it in your kerbside collection or local recycling point. Members can access the online archive of companion at www.bsava.com .
OFFICE OPENING TIMES FOR CHRISTMASApart from the seasonal bank holidays, Woodrow House will be open over the Christmas period, though will operate with reduced staff on 27–31 December. On 3 January (a bank holiday) the office will be open for Congress queries only, as this is the Early Bird deadline. Of course, you will be able to access all your online benefits 24 hours a day all over Christmas, including ordering Manuals, booking courses, or registering for Congress.
A date with membershipYou get more every year with your BSAVA membership. Members who renew for consecutive years are going to be rewarded for their loyalty in stages – with benefits including online journal access and Congress podcasts on CD.
You will get full details of your entitlement in your membership renewal information. As an additional benefit, once you have renewed you will receive a
useful free calendar with key association dates for 2011.If you have any questions about your renewal or
which benefits you are entitled to please email [email protected] or call 01452 726700. ■
Watch your mail box
In the next few weeks you will be getting two key pieces of mail from BSAVA – your membership renewal information, and your Congress booking pack.
Look out for both or check our website to make sure you don’t miss out on loyalty bonuses for renewing members or the lowest prices for Congress booking.
If you have any questions or concerns about your membership renewal then please email [email protected] or call 01452 726700 and our team will be happy to help you. ■
02 Page 02.indd 2 20/10/2010 14:22

companion | 3
ASSOCIATION NEWS
More online tools –downloadable formsFrom December members will be able
to download useful forms from www.bsava.com – including anaesthetic
record forms and dentistry charts. They can be downloaded and even personalised from the Advice area of the website (within the For the Practice section). Feel free to comment on the forms and suggest additions or amendments, and let us know what other similar resources BSAVA can help members with. Email [email protected] to comment. ■
JSAPgets biggerimpact factorThe Institute of
Scientific Information
(ISI) has published this year’s Journal Citation Report, which provides data on citation performance for peer-reviewed journals across all subject areas. JSAP’s ‘Impact Factor’, which is a measure of recent citations to articles published in the preceding two years, rose to 0.965. Articles from JSAP were cited more than 2,350 times during 2009. BSAVA members get free access to the online JSAP archive via www.bsava.com. ■
Neurology roadshowThere are a few places available in each
location of the Neurology Roadshow with Simon Platt and Laurent Garosi this month.
Visit www.bsava.com or call 01452 726700 for more information or to book. ■
■ Derby – 18 November ■ Yorkshire – 19 November ■ South Wales – 22 November ■ Surrey – 23 November
BVOA websitefrom BSAVAThe British Veterinary Orthopaedic Association
have launched their new website at www.bvoa.org.uk, with the help of the IT and
creative team at BSAVA. As a much-valued affiliate group to BSAVA, BVOA called on Woodrow House resources to establish a more functional website and a new logo which features a stylised canine knee joint. Speaking after the launch Gareth Arthurs of BVOA said, “We now have a new logo and website that has a clean, fresh and very contemporary feel, and is easy to navigate”. ■
RCVS nominationsNominations have now opened for candidates
who wish to stand in the 2011 elections to RCVS Council and RCVS Veterinary Nurses
Council. Visit www.rcvs.org.uk or get nomination forms and candidate information forms from [email protected]. ■
Don’t forget that the Early Bird deadline for Congress 2011 is even earlier than usual. You might be
used to it being in February; however, due to the complications and added expense coming with the new VAT value, we’ve had to bring it forward. So you need to register for Congress before 3 January to benefit from early booking discount – and save a further 5% on your registration by booking online at www.bsava.com. ■Early Bird reminder
03 Page 03.indd 3 20/10/2010 15:35

4 | companion
FRANK BEATTIE AWARD
Thanks to Frank Beattie
On graduation day from vet school at the ripe old age of 40, I stood there waiting to enter the Usher Hall in Edinburgh and thought,
“Here I am, starting a new career in a new country. The rest of my life would be just icing on the cake.” I could have ‘dropped off the perch’ the next day and still would have had no regrets. I had arrived in a new life and the next years, no matter how many, were going to be better.
Since then I’ve worked with some great people, and been very fortunate to develop my passion for ophthalmology, all thanks to Frank and Annie Beattie.
Maintaining enthusiasmWhen you’ve worked in general practice for over a decade you can become entrenched in just getting through a day’s caseload. It’s not easy to step back and look at the forest rather than the trees and try to identify the pathway forward. We all need that intellectual drive to keep the enthusiasm and growth. Some can even experience a mid-career crisis. But how do you take time out to pursue that interest? For me, this is where Frank Beattie and the BSAVA stepped in.
In June 2008, as a “fifty-something”, I used the Frank Beattie Travel Scholarship to attend the Eighth Biannual William Magrane Basic Science Course in Veterinary and Comparative Ophthalmology and Histologic Basis of Ocular Disease in Madison, Wisconsin. After several attempts I passed the Certificate Examination in Veterinary Ophthalmology in 2009.
Scholarship supportThe travel scholarship Mrs Beattie set up in memory of her husband has helped many veterinary surgeons pursue varied areas of interest, and given, as in my case, that ‘leg-up’ to further qualification. The travel scholarship opened doors and introduced me to international specialists I otherwise would not have met. Friendships forged on CPD courses can last a lifetime, they’ve certainly added to the quality of my life. After all, we are but a summation of our experiences.
Taking up this opportunity was not without its
sacrifices. Using holiday time for a three week CPD course requires an understanding family and employer. There were young mothers on the course with adolescent children being cared for by husbands and grandparents. Plus, for myself and others, the travel distance was another factor. Delegates from all over the world came to Wisconsin University for this intensive course.
The non-American contingency made up about a third of the numbers and came from Australia, Belgium, Columbia, Germany, Israel, Italy, Japan, Latvia, Portugal, Spain and the United Kingdom. The majority of the North American participants were residents in ophthalmology at American and Canadian veterinary schools.
There is a great sense of job satisfaction that comes with additional knowledge in clinical work. I started out on this journey with one purpose in mind – to make a difference for my clients and their animals in first-opinion practice. My priority is treating the whole animal and developing my understanding of ophthalmology substantially increases that ability; the eye is after all the window into the body. Every day I continue to learn with each new challenge. This is the most gratifying journey I have ever struggled through. It’s been my own private Mt. Everest. If you have a passion, don’t let age stand in your way from pursuing it. n
Karen Wendlandt, winner of the 2008 BSAVA Frank Beattie Travel Scholarship, describes how the award helped develop her interest in ophthalmology, and why after graduating as a mature student she still loves to learn more about the profession she entered in her middle years
04 Frank Beattie Awards .indd 4 20/10/2010 14:55

companion | 5
POULTRY
There has been phenomenal growth over the past 20 years in the number of households keeping backyard chickens, according to Victoria
Roberts, who has a lifelong interest in poultry rearing and lectures on avian health and welfare to her veterinary colleagues.
Small hobby flocks don’t have to be registered with Defra and so there are no precise figures on the numbers of birds but all the indirect indicators are pointing in the same direction. Membership of poultry clubs has risen and three new publications for poultry enthusiasts have been launched in the past five years, all of which continue to thrive. And a glance inside one of these publications shows that there are a growing number of companies offering livestock, housing or feedstuffs.
MotivationEach new keeper of chickens may have slightly different reasons for becoming involved but there are many who are drawn to the idea of a pet that also provides something as useful as fresh eggs. “If I thought about the time and effort that goes into keeping birds, it would be cheaper and make more sense to buy the eggs at the supermarket – but I do
think our own taste so much better,” says Rowena Evans, who started with three chickens at her home near Canterbury, and now keeps 40 laying hens and a smaller flock of Pekin bantams as pets for her children.
Branwen Davis, a small animal practitioner in South Wales, believes that concern about the welfare of farmed birds is another major factor in this growing popularity. “Getting the eggs is a part of it because people want to know that their food comes from animals living in conditions that they have somecontrol over.”
There has been phenomenal growth over the past 20 years in the number of households keeping
think our own taste so much better,” says Rowena Evans, who started with three chickens at her home near Canterbury, and now keeps 40 laying hens and a smaller flock of Pekin bantams as pets for her children.
Branwen Davis, a small animal practitioner in South Wales, believes that concern about the welfare of farmed birds is another major factor in this growing popularity. “Getting the eggs is a part of it because people want to know that their food comes from animals living in conditions that they have somecontrol over.”
Poultry passionsWhy did the chicken cross the road? Well, it may have been
that she was being taken by her owners for treatment at their local veterinary practice. That is because increasing
numbers of clients are now keeping poultry as pets, rather than just to provide them with eggs and meat. John Bonner asks what practitioners need to know if they want to provide a good service to these clients
Figure 1: (A) Light Brahma pair. (B) Silver grey Dorking cockReproduced from the BSAVA Manual of Farm Pets
A
B
05-08 Chickens.indd 5 20/10/2010 15:07

6 | companion
POULTRY
Poultry passions
There are many more benefits not just fresh eggs for breakfast. “Keeping chickens fits in well with vegetable growing, providing a weeding service plus first class manure. Chickens are generally friendly, easily bribed and interesting. And they make good pets for children to learn about the responsibilities of pet ownership,” Victoria notes.
Breed and benevolenceThere are similarly worthy reasons behind the choice of birds. “In the past 10 years, rescuing spent battery hens has been heavily promoted and this is how many recent chicken keepers have begun. It is reckoned that 250,000 ex-bats have been re-homed so far,” she explains. Commercially reared birds don’t usually live very long in an outdoor environment, but by then the experience of keeping poultry will often encourage owners to look for hardier outdoor hybrids, or they may progress on to fancy breeds, many of which produce unusual and attractively coloured eggs.
Keeping friends and neighbours supplied with these eggs will often encourage new owners to increase the size of their flock, as happened in Rowena’s case. “I am from a farming background and I suppose that I am quite pragmatic about the laying
hens. With the Pekins, it is different – they are there for the children and there have been a few tears when one of those birds dies. I think you cross the threshold when you start to give your
chickens names.”
Poultry in practiceLarge-scale poultry keepers will often know a good deal about
maintaining a healthy flock, but the less experienced keeper may
well need to bring a sick individual in for treatment at their veterinary
practice. Branwen is one of the vets with a developing interest in this area but like
most small animal colleagues, she will admit that her veterinary degree left her ill-
prepared for dealing with chickens. “I think we had a few lectures on pigs and poultry
but that was really just an introduction and was more geared to dealing with health issues in a commercial situation.” Moreover, few cases have turned up in her consult room since graduation. Her former boss, Jean Morris, has a reputation in South Wales as a poultry vet and clients would naturally demand to see her.
So if a chicken appears on their consulting room table for the first time, what does a small animal vet need to know? “First of all, you need to handle and examine a chicken competently and know the normal signs of health,” Victoria explains. “Then, you should have knowledge of the most common husbandry and/or disease problems and whether there is a successful treatment. For example, the older battery hens are prone to egg peritonitis, which is generally untreatable”.
Figure 2: How poultry should be heldReproduced from the BSAVA Manual of Farm Pets
Owner know-howHowever, veterinary surgeons should appreciate that they may not be the only source of information that is available for an inexperienced poultry keeper. John Sinclair keeps a smallholding near Bradford and was given his first chicken to look after in 1941. Over the subsequent years he has built up a huge base of practical knowledge and rarely needs to see his vet, except when it is necessary to obtain wormers and other prescription medicines.
05-08 Chickens.indd 6 20/10/2010 15:07

companion | 7
POULTRY
As well as asking for advice from people like Mr Sinclair, keepers will also share information among themselves on internet discussion groups and in local poultry clubs. Most of the causes of ill health in backyard hens are well characterised conditions like red mites and respiratory disease due to Mycoplasma infection and so it is usually pretty clear what steps need to be taken.
Challenges and threatsOverall, the standard of care provided by backyard poultry keepers is fairly good and chickens may be less likely than some pets to suffer problems when the novelty of having them wears off. “Lack of interest does not seem to be a problem. Lack of knowledge can be, but most people are willing to learn,” Victoria explains. Those supplying poultry to new owners will usually give basic instruction and there are plenty of paper and web-based information sources, “although some websites are just based on beginners’ experience, which can be confusing,” she warns.
Inexperience is likely to be the main reason for health problems. “Things are likely to go wrong if the birds are fed by throwing food around in the garden, as that is going to attract wild birds and rodents that are the most probable source of a new disease,” Mr Sinclair suggests.
However, the major threat to any backyard poultry is the fox, and new keepers may not appreciate the dangers until they find a bloody pile of feathers or,
worse, they leave their hen house open and lose the whole flock. Victoria has drawn up guidelines on biosecurity for birdkeepers, which are disseminated via the Poultry Club (www.poultryclub.org) and the Animal Oracle websites (www.animaloracle.com). The latter is a decision tree for poultry keepers which will give guidance on the seriousness of any health problems and indicate when it may be necessary to contact their veterinary practice, she says.
Figure 3: Nebraskan Spotted turkey with mycoplasmosis. The sinus is swollen (arrowed)Reproduced from the BSAVA Manual of Farm Pets
➘
Figure 4: Chicken ark Reproduced from the BSAVA Manual of Farm Pets
Growing trendProvided they are able to keep Reynard at bay, the likely trend is for new poultry keepers to want to acquire more and more birds.”I suppose it is rather addictive,” Rowena admits. And not just for the public, as some members of the profession have also got the bug. Fife-based vet Jan Dixon started off five years ago with three birds and now has about a dozen hens of different breeds, nine ducks and five peafowl. Jan also has a batch of eggs in an incubator, bought to compensate for the feckless parenting that is sometimes a feature of the old rare breeds. So it can be very easy to slip largely unnoticed across the threshold of 50 birds at which the flock should be registered, she warns.
Having a large flock will not be so much of a problem for a small animal practitioner when sourcing medicines from their normal wholesaler for their clients or their own birds. Many of the products licensed for use in poultry are mainly directed at
05-08 Chickens.indd 7 20/10/2010 15:08

8 | companion
POULTRY
Look out for a backyard chicken clinical conundrum next month which will further explore some of the issues raised in this piece.
| companion
Look out for a backyard chicken clinical conundrum next month which will further explore some of the issues raised in this piece.
commercial flocks and so it may be necessary to break down a large pack into smaller volumes and to copy the data sheet for hobby keepers. Yet the growth in the numbers of small-scale poultry keeping does make it increasingly easy to obtain drugs in economical amounts.
TreatmentProducts like the wormer Flubenvet are now dispensed in pack sizes appropriate for the backyard flock. Of course, where there is no licensed treatment for birds it is always possible to apply the cascade system, notes Branwen, who recalls using Canaural ear drops to treat a condition very similar to canker in a client’s birds.
“Of course, you need to make sure the client understands what you are doing and signs an off-licence consent form. They must also appreciate that they shouldn’t allow anyone to eat the eggs from a bird that is being treated in this way.”
As that case demonstrates, there will be the occasional situation in which the appropriate course of action may not be immediately obvious even to an experienced practitioner with an active interest in poultry medicine. So for complete newcomers to the field there will be a need for guidance. Probably the most practical source of information on the health and welfare of backyard birds is the BSAVA Manual of Farm Pets. However, there many other useful sources of CPD on chickens and the other domestic poultry species. It was standing room only for the lectures that Victoria gave on chickens at 2010’s BSAVA Congress, so there are plans for a whole session in 2011. ■
FARM PETS – AN ESSENTIAL GUIDE FOR SMALL ANIMAL VETSFrom the ‘backyard chicken’ to the pet llama, an increasing number of farm animals are kept in small numbers by ‘hobby farmers’ or as purely companion animals. These animals often require a different type of care to large flocks and this may well fall to the predominantly small animal veterinary surgeon. The BSAVA Manual of Farm Pets provides practical information on health, husbandry, medicine and surgery of companion animals more commonly regarded as farm species.
Health and husbandry chapters include:
■ Management ■ Nutrition and feeding ■ Health planning ■ Legal considerations.
Medicine and surgery chapters detail:
■ The clinical approach to the farm pet patient (history taking, physical examination, diagnostic tests)
■ Common medical conditions ■ Surgical procedures.
The chapters for each group are organized in a consistent format to aid information retrieval. A separate chapter on post-mortem examination of galliform and anseriform birds shows how diseases manifest in the appearance of the internal organs of these birds. An introductory chapter sets the scene within a framework of animal health and welfare and associated legislation, and the final chapter of the Manual shows how organic farming practices relate to the keeping of livestock.
“…this is an excellent book which is well worthy of a place on the shelves of veterinary surgeons especially those dealing with the occasional farm animal. It is full of vital information.” Journal of Small Animal Practice
Member price £49.00Non-member price £75.00
Poultry passions
05-08 Chickens.indd 8 20/10/2010 15:41

companion | 9
CLINICAL CONUNDRUM
Clinical conundrumconundrum
Alex Lynch, intern at Dick White Referrals, invites you to consider investigation of laboured breathing in a young Springer Spaniel
Case presentationAn 18-month-old male neutered English Springer Spaniel is presented with a 5 day history of depression, inappetence and laboured breathing. No previous medical problems have been reported. He is thin, weighing 16.6 kg (body condition score 2/5), and is quiet, alert and responsive. He is cardiovascularly stable (heart rate 120 beats/minute) but with obvious increased breathing effort and tachypnoea (50 breaths/minute) at rest. Rectal temperature is 39.8°C. Bilateral dullness is noted ventrally on thoracic auscultation and percussion, but harsh respiratory sounds are heard more dorsally. Abdominal palpation is resented but the rest of the physical examination is normal.
■■ Upper airway dyspnoea tends to be associated with increased inspiratory effort and respiratory sounds (e.g. stridor, stertor). Coughing and sneezing may also be noted. The physical examination findings were not suggestive of upper airway pathology. Potential differentials include inhalation of a foreign body, inflammation, abscessation and neoplasia.
■■ Lower airway (i.e. bronchi and bronchioles) disorders may be associated with tachypnoea and the auscultation of abnormal respiratory sounds (e.g. crackles). Differential diagnosis would include bronchitis, bronchopneumonia and smoke inhalation.
■■ Pleural space disorders may be associated with tachypnoea, increased breathing effort and sometimes exaggerated abdominal movement. The ventral dullness noted on thoracic auscultation is also highly suggestive of a pleural space disorder. Potential aetiologies to consider are pneumothorax, pleural effusion, diaphragmatic hernia/rupture and neoplasia. A pleural space disorder was therefore considered likely in this case.
■■ Parenchymal disease may be associated with auscultation of harsh respiratory sounds. There are numerous potential causes for parenchymal disease, e.g. cardiogenic and non-cardiogenic pulmonary oedema, pneumonia, aspiration pneumonitis, adult respiratory distress syndrome (ARDS), pulmonary thromboembolism, neoplasia, pulmonary haemorrhage/
contusions and inflammation. Clues from the history and physical examination help to refine the potential differentials. For instance, no abnormalities in the cardiovascular system were appreciated, making cardiogenic pulmonary oedema less likely. No apparent history of trauma made pulmonary haemorrhage or contusions appear less likely.
Non-respiratory causes of dyspnoea may reflect elevation in body temperature (hyperthermia or pyrexia), pain, hyperadrenocorticism/exogenous steroid administration or acute haemorrhage.
Elevated body temperature may reflect hyperthermia (e.g. due to elevated environmental temperature, anxiety or over-exertion) or pyrexia (e.g. infectious disease – bacterial, viral, parasitic or fungal, immune-mediated disorders, inflammatory or neoplastic conditions).
How would you investigate this case further?The patient must be stable before pursuing further diagnostics. Oxygen supplementation delivered in a minimally stressful way is advisable, along with calm patient handling. Baseline laboratory information (complete blood count and biochemistry profile) and thoracic imaging are required. Given the strong suspicion of a pleural space disorder based on physical examination findings, diagnostic thoracocentesis is also indicated. Thoracocentesis may be performed in the emergency management of unstable dyspnoeic animals (especially feline patients) prior to thoracic radiography, where restraint for radiography may prove potentially life-threatening. The dog was sedated using low-dose acepromazine and butorphanol. When dealing with dyspnoeic patients, the clinician must be prepared to perform endotracheal intubation if necessary.
What are the dog’s main problems?The dog’s main problems are dyspnoea and elevated body temperature. Depression and inappetence are likely secondary to an underlying primary disease process.
Consider differential diagnoses for his problems tailored to the physical examination findingsDyspnoea may occur due to respiratory or non-respiratory causes. Classification of respiratory causes of dyspnoea by anatomical location is useful.
09-12 Clinical Conundrum.indd 9 20/10/2010 15:08

10 | companion
CLINICAL CONUNDRUM
Clinical conundrum
Parameter Value Reference range
Haemoglobin 13.9 12.0–18.0 g/dl
RBC 5.92 5.5–8.5 x 1012/l
HCT 0.40 0.37–0.55 l/l
MCV 66.9 60.0–77.0 fl
MCHC 35.1 30.0–38.0 g/dl
MCH 23.5 19.5–25.5 pg
White cell count 17.5 6.0–15.0 x 109/l
Neutrophils 11.6 3.0–11.5 x 109/l
Lymphocytes 3.6 1.0–4.8 x 109/l
Monocytes 2.1 0.2–1.4 x 109/l
Eosinophils 0.2 0.1–1.2 x 109/l
Basophils 0.0 0.0–0.1 x 109/l
Nucleated red cells 0.3
Platelets 296 200–500
White cell morphology Neutrophils have slightly foamy cytoplasm
Red cell morphology Occasional polychromasia
Platelet morphology Platelets consistent with analyser count. No clumping seen.
Table 1: Haematology
Parameter Value Reference range
Total protein 64 54–77 g/l
Albumin 18 25–40 g/l
Globulins 46 23–45 g/l
Urea 3.2 2.5–7.4 mmol/l
Creatinine 59 40–145 µmol/l
Potassium 4.4 3.4–5.6 mmol/l
Sodium 144 139–154 mmol/l
Sodium:Potassium ratio 32.7 > 27.0
Chloride 112 105–122 mmol/l
Calcium 2.2 2.3–2.9 mmol/l
Magnesium 0.62 0.62–0.86 mmol/l
Inorganic phosphate 1.3 0.60–1.40 mmol/l
Glucose 4.3 3.3–5.8 mmol/l
ALT 13 13–88 IU/l
AST 26 0–49 IU/l
ALP 63 14–105 IU/l
GGT 1 0–10 IU/l
Bilirubin 3 0–16 µmol/l
Bile acids 1.1 0–10 µmol/l
Cholesterol 5.7 3.8–7.0 mmol/l
Triglyceride 0.8 0.56–1.14 mmol/l
Creatine kinase 85 0–190 IU/l
Table 2: Biochemistry profile
How would you interpret the laboratory results shown in Tables 1 and 2?Haematology:
■■ Evidence of mild neutrophilia and monocytosis suggests an established inflammatory response
Biochemistry:
■■ Moderate hypoalbuminaemia may reflect reduced albumin production (i.e. liver dysfunction), increased losses (e.g. protein-losing enteropathy, protein-losing nephropathy, secondary to chronic exudation) or be a feature of the acute phase response.
■■ Mild increase in globulins was thought likely to reflect chronic inflammation or immune stimulation
■■ Mild decrease in calcium was likely attributable to low albumin
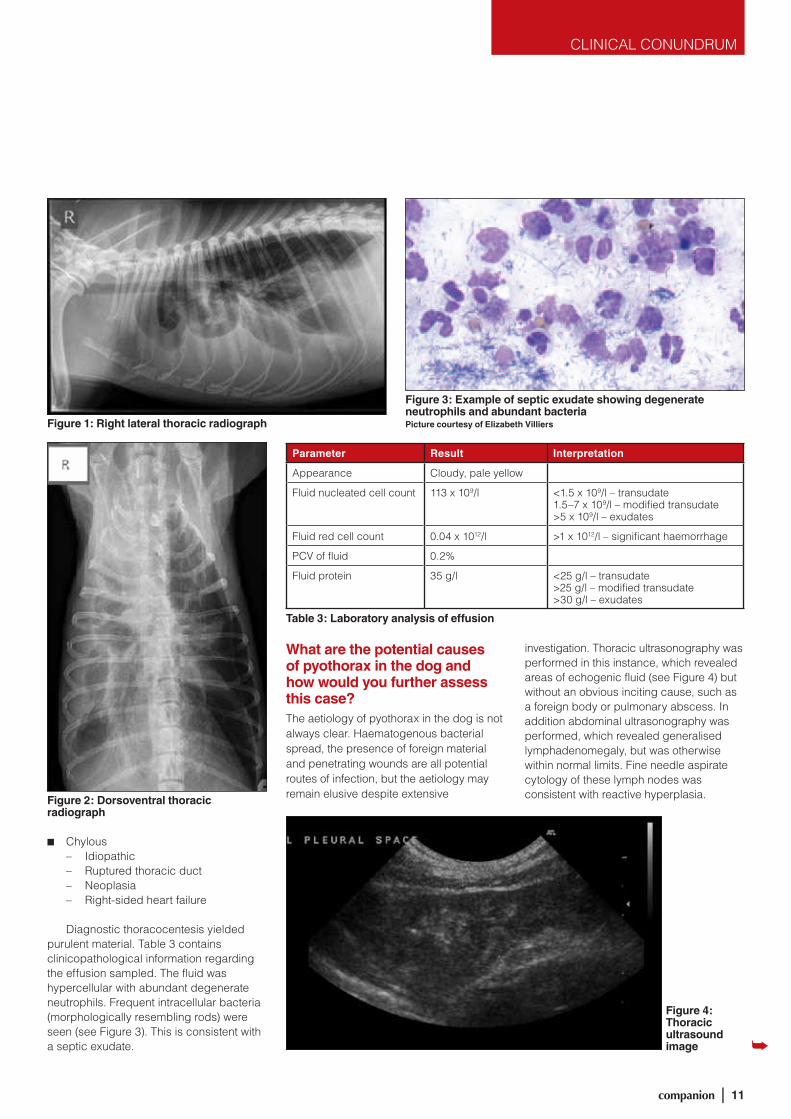
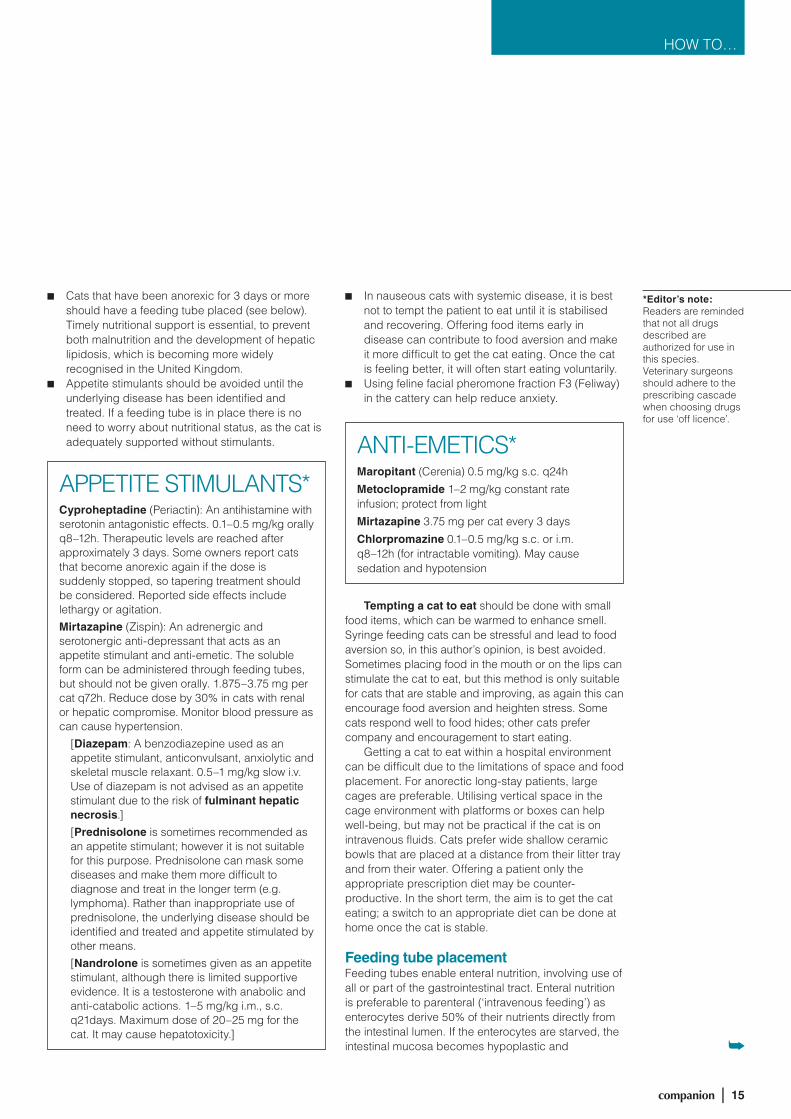
Describe the radiographic changes in Figures 1 and 2The lateral radiograph shows evidence of lung lobe retraction and scalloping, due to the presence of a ventral soft tissue opacity, consistent with a pleural effusion. The dorsoventral view confirms bilateral but asymmetrical effusions, with fissure lines and retracted lung lobes visible. The fluid appeared predominantly right-sided.
ThoracocentesisThoracocentesis was performed to assess the character of the pleural effusion and hence determine the likely underlying aetiopathogenesis:
■■ Transudate – Hypoalbuminaemia
■■ Modified transudate – Neoplasia – Diaphragmatic rupture – Right-sided heart failure – Vasculitis – Pancreatitis
■■ Exudate – Septic inflammation – Non-septic inflammation – Neoplastic
■■ Haemorrhagic – Trauma – Coagulopathy – Neoplasia – Lung lobe torsion
09-12 Clinical Conundrum.indd 10 20/10/2010 15:08
companion | 11
CLINICAL CONUNDRUM
■■ Chylous – Idiopathic – Ruptured thoracic duct – Neoplasia – Right-sided heart failure
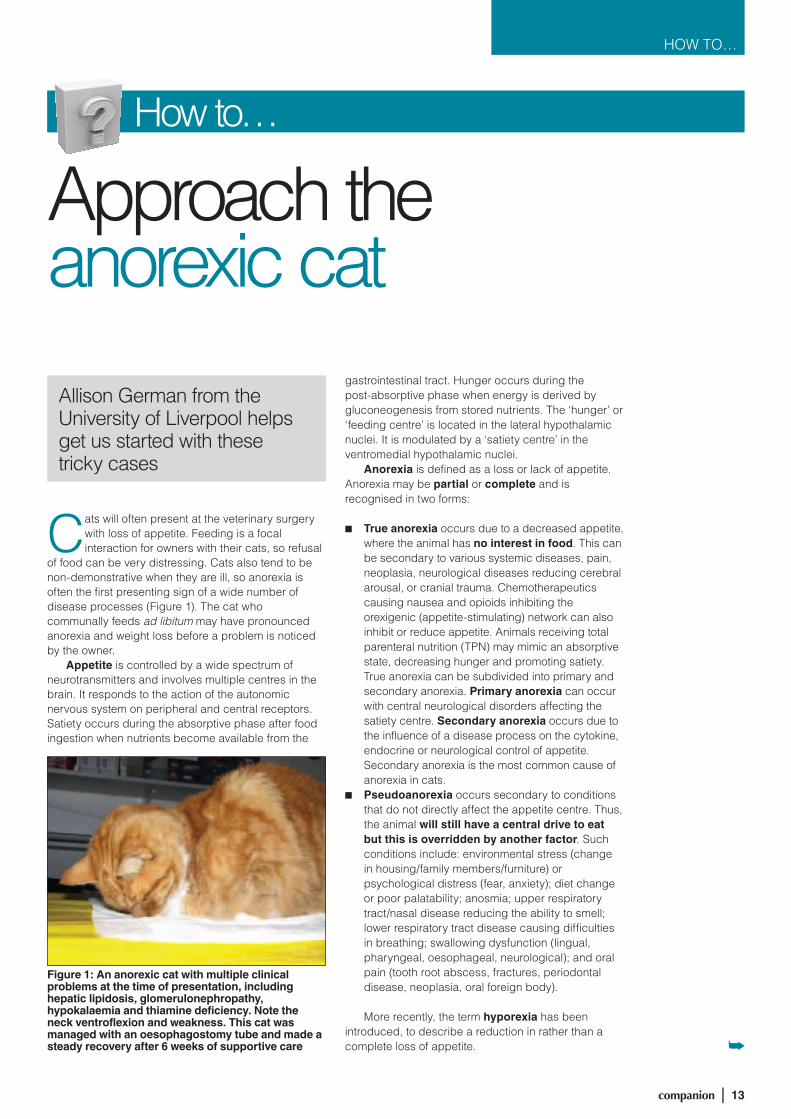
Diagnostic thoracocentesis yielded purulent material. Table 3 contains clinicopathological information regarding the effusion sampled. The fluid was hypercellular with abundant degenerate neutrophils. Frequent intracellular bacteria (morphologically resembling rods) were seen (see Figure 3). This is consistent with a septic exudate.
What are the potential causes of pyothorax in the dog and how would you further assess this case?The aetiology of pyothorax in the dog is not always clear. Haematogenous bacterial spread, the presence of foreign material and penetrating wounds are all potential routes of infection, but the aetiology may remain elusive despite extensive
investigation. Thoracic ultrasonography was performed in this instance, which revealed areas of echogenic fluid (see Figure 4) but without an obvious inciting cause, such as a foreign body or pulmonary abscess. In addition abdominal ultrasonography was performed, which revealed generalised lymphadenomegaly, but was otherwise within normal limits. Fine needle aspirate cytology of these lymph nodes was consistent with reactive hyperplasia.
Parameter Result Interpretation
Appearance Cloudy, pale yellow
Fluid nucleated cell count 113 x 109/l <1.5 x 109/l – transudate1.5–7 x 109/l – modified transudate>5 x 109/l – exudates
Fluid red cell count 0.04 x 1012/l >1 x 1012/l – significant haemorrhage
PCV of fluid 0.2%
Fluid protein 35 g/l <25 g/l – transudate>25 g/l – modified transudate>30 g/l – exudates
Table 3: Laboratory analysis of effusion
Figure 2: Dorsoventral thoracic radiograph
Figure 1: Right lateral thoracic radiograph
Figure 3: Example of septic exudate showing degenerate neutrophils and abundant bacteriaPicture courtesy of Elizabeth Villiers
Figure 4: Thoracic ultrasound image
09-12 Clinical Conundrum.indd 11 20/10/2010 15:08

12 | companion
CLINICAL CONUNDRUM
Clinical conundrum
If available, alternative imaging techniques such as computed tomography (CT) may be useful in providing further information in the investigation of pyothorax. CT is a sensitive imaging modality for identification of underlying septic foci (e.g. foreign bodies or abscesses) and intrathoracic pathology (e.g. lung lobe consolidation). Concurrent CT of the lumbar spine may enable sublumbar abscesses to be identified, which may be associated with migrating foreign bodies.
CT is also useful in helping to pinpoint cases where surgery may be indicated. Exploratory thoracotomy may be required to remove foreign material from the pleural cavity, if medical treatment proves unsuccessful or in relapsing clinical cases. However the recommendation for surgical intervention must be made on a case-by-case basis.
How would you manage this case?Whether to manage cases of pyothorax medically or surgically is an ongoing debate. Surgery was not felt necessary in the initial management of this case, since there was no obvious source of infection (e.g. foreign body) that would require surgical correction, and good results have been obtained with medical management alone. In this instance bilateral thoracostomy tubes were placed under anaesthesia to enable closed drainage of the thorax, alongside aggressive antibiotic therapy. However, good results have also been reported with one-off thoracocentesis and administration of long courses of antibiotics without thoracostomy tube placement. Thoracic radiographs were obtained after placement to ensure appropriate positioning (see Figure 5).
Initially fluid drainage was difficult due to the inherent turbidity of the fluid and fluid pocketing within the pleural cavity. Thoracic lavage was performed twice daily over the next 5 days using 500 ml of normal saline. Thoracic drainage was performed four times daily. Opioid analgesia was provided, based on regular assessment of pain scores, and bupivacaine was administered
via the thoracostomy tubes for intrapleural analgesia. In addition carprofen was administered.
Which antibiotics would you choose and for how long would you advise administering them?Common bacteria implicated in pyothorax in the dog include Escherichia coli, Nocardia and Actinomyces. Broad-spectrum antibiotic cover, to include antimicrobials effective against anaerobes, is advisable as first-choice therapy. Intravenous potentiated amoxicillin and metronidazole was begun, although alternative antibiotic combinations have also been used successfully.
A more detailed in-house assessment of the fluid could have been undertaken, and can enable the clinician to target empirical antibiotic therapy whilst awaiting culture results. For example, Gram staining
*Editor’s note: Readers are reminded that not all drugs described are authorized for use in this species. Veterinary surgeons should adhere to the prescribing cascade when choosing drugs for use ‘off licence’.
of pleural fluid may also be useful in making antibiotic choices. Identifying a Gram-negative bacterium would justify selection of antimicrobials with good activity against Gram-negative organisms, whereas the presence of sulphur granules within the pleural fluid would suggest Actinomyces and/or Nocardia infection. Samples for culture and sensitivity testing should always be obtained before starting antibiotics.
In this case culture of the pleural fluid did not yield bacterial growth, which may reflect the difficulty in culturing anaerobes. Indeed, some clinicians inoculate pleural fluid into blood culture bottles to facilitate identification of more fastidious organisms. Irrespective of the organism identified, a long course of antibiotics is recommended – a 6-week course was initially prescribed in this case.
Over the next 5 days the dog’s demeanour improved dramatically and he regained his appetite. Repeat analysis of the pleural fluid was performed, revealing progressive improvement in cellularity and gross appearance. In addition serum albumin increased to 24 g/l by the fifth day of treatment. The improvement in hypoalbuminaemia was attributed to slowing the protein losses into the septic exudate within the pleural cavity. However, mild hypoalbuminaemia and hyperglobulinaemia are also seen as part of the acute phase response in dogs. Repeat thoracic radiographs were obtained on day 5 and showed resolution of most of the effusion; both thoracostomy tubes were removed. No complications associated with thoracostomy tube placement occurred in this case. The dog was discharged on oral potentiated amoxicillin and metronidazole.
Thoracic radiographs were obtained a further 3 weeks later, which showed further resolution of pleural effusion. Antibiotics were stopped after a complete 6-week course. Surgical exploration of the thorax was not required in this case as the dog continued to do well without recurrence of his clinical signs. ■
Figure 5: Dorsoventral thoracic radiograph following thoracostomy tube placement – note pleural space on left now appears wider compared to original radiographs but with overall reduction in fluid volume
09-12 Clinical Conundrum.indd 12 20/10/2010 15:08
companion | 13
HOW TO…
How to…
Approach the anorexic cat
Allison German from the University of Liverpool helps get us started with these tricky cases
Cats will often present at the veterinary surgery with loss of appetite. Feeding is a focal interaction for owners with their cats, so refusal
of food can be very distressing. Cats also tend to be non-demonstrative when they are ill, so anorexia is often the first presenting sign of a wide number of disease processes (Figure 1). The cat who communally feeds ad libitum may have pronounced anorexia and weight loss before a problem is noticed by the owner.
Appetite is controlled by a wide spectrum of neurotransmitters and involves multiple centres in the brain. It responds to the action of the autonomic nervous system on peripheral and central receptors. Satiety occurs during the absorptive phase after food ingestion when nutrients become available from the
gastrointestinal tract. Hunger occurs during the post-absorptive phase when energy is derived by gluconeogenesis from stored nutrients. The ‘hunger’ or ‘feeding centre’ is located in the lateral hypothalamic nuclei. It is modulated by a ‘satiety centre’ in the ventromedial hypothalamic nuclei.
Anorexia is defined as a loss or lack of appetite. Anorexia may be partial or complete and is recognised in two forms:
■■ True anorexia occurs due to a decreased appetite, where the animal has no interest in food. This can be secondary to various systemic diseases, pain, neoplasia, neurological diseases reducing cerebral arousal, or cranial trauma. Chemotherapeutics causing nausea and opioids inhibiting the orexigenic (appetite-stimulating) network can also inhibit or reduce appetite. Animals receiving total parenteral nutrition (TPN) may mimic an absorptive state, decreasing hunger and promoting satiety. True anorexia can be subdivided into primary and secondary anorexia. Primary anorexia can occur with central neurological disorders affecting the satiety centre. Secondary anorexia occurs due to the influence of a disease process on the cytokine, endocrine or neurological control of appetite. Secondary anorexia is the most common cause of anorexia in cats.
■■ Pseudoanorexia occurs secondary to conditions that do not directly affect the appetite centre. Thus, the animal will still have a central drive to eat but this is overridden by another factor. Such conditions include: environmental stress (change in housing/family members/furniture) or psychological distress (fear, anxiety); diet change or poor palatability; anosmia; upper respiratory tract/nasal disease reducing the ability to smell; lower respiratory tract disease causing difficulties in breathing; swallowing dysfunction (lingual, pharyngeal, oesophageal, neurological); and oral pain (tooth root abscess, fractures, periodontal disease, neoplasia, oral foreign body).
More recently, the term hyporexia has been introduced, to describe a reduction in rather than a complete loss of appetite.
Figure 1: An anorexic cat with multiple clinical problems at the time of presentation, including hepatic lipidosis, glomerulonephropathy, hypokalaemia and thiamine deficiency. Note the neck ventroflexion and weakness. This cat was managed with an oesophagostomy tube and made a steady recovery after 6 weeks of supportive care
13-17 How To.indd 13 20/10/2010 15:09

14 | companion
HOW TO…
Approach the anorexic cat
The clinical examination can help define a tighter differential list by: assessment of any physical abnormality; observation of behaviour; assessment of the ability to smell; palpation to investigate pain; assessment of dental health; and evaluation of the respiratory tract. The possibility of systemic disease should be investigated, particularly if the cat has fever, pale mucous membranes, abdominal discomfort, orthopaedic pain, masses, respiratory abnormalities or a cardiac murmur. Ocular examination is important when considering infectious diseases (FeLV, FIV, toxoplasmosis, FIP) and lymphoma.
The diagnostic work-up will be directed by the clinical findings. This may entail a complete blood count, biochemistry panel, urinalysis, feline pancreatic lipase immunoreactivity (fPLI), cobalamin and virus screening; more complicated cases may require diagnostic imaging, cytology/histopathology or more advanced procedures (depending on indication) such as bone marrow biopsy and exploratory coeliotomy. In the majority of cases, the cause of anorexia can be identified through a thorough clinical examination and minimum database. A minimum of packed cell volume, total protein and electrolyte measurements should be repeated once the cat is rehydrated and at regular intervals for monitoring.
Bodyweight and body condition score (BCS) should be recorded on admission and then daily (twice daily for more critical patients). Bodyweight alone does not give information on body condition and
will be affected by faecal mass (anorexic cats are often dehydrated and constipated) and effusion volume (the long-term anorexic patient will be protein-deficient and prone to effusion development, particularly following rehydration). BCS is measured on either a 5 point (edney and Smith, 1986) (Figure 2) or 9 point (Laflamme et al., 1994) scale.
InterventionFeeding an anorexic patient prevents malnutrition. Malnutrition compromises the immune system, delays healing, decreases hepatic detoxification and increases intestinal permeability. ensuring adequate nutrition thus enhances recovery rates and reduces morbidity and mortality. Intervention should occur early, once fluid and electrolyte imbalances have been corrected. Current advice is to intervene when weight loss is above 10% (including in obese patients) or when there has been partial (<85% calculated energy requirements) or complete anorexia for more than 3 days. In addition, those patients in a catabolic state (burns, severe inflammation, major surgery or trauma) require nutritional support.
Management is based on identifying and treating the underlying cause. Some general treatment goals follow:
■■ The patient should be rehydrated and reassessed. Sometimes, once fluid balance has been restored, the cat will eat.
■■ electrolytes should be supplemented as indicated from regular monitoring, particularly potassium.
Body Condition Score – FelineBody Condition Score
Very ThinMore than 20% belowideal body weight
ThinBetween 10 and 20% below ideal weight
Ideal Weight
Overweight20% aboveideal weight
Markedly Obese40% aboveideal weight
1
2
3
4
5
Characteristics
■ Ribs, spine and pelvic bones are easily visible (in short haired pets)■ Obvious loss of muscle mass■ No palpable fat on chest
■ Ribs, spine and pelvic bones visible■ Obvious waist■ Minimal abdominal fat
■ Ribs, spine and pelvic bones not visible but easily palpable■ Obvious waist■ Little abdominal fat
■ Ribs, spine and pelvic bones are hardly palpable■ Waist is absent■ Heavy abdominal fat deposits
■ Massive fat deposits on chest, spine and the abdomen■ Obviously distended abdomen
The Body Condition Score combines the evaluation of visible characteristics and palpation of certain areas of the body. The scoring system offers the advantage of being easy to use by the veterinary surgeon of veterinary nurse and also by the owner and can be applied both for diagnosis of obesity and active prevention. Nutritional recommendations may be made following body condition scoring which will vary in relation to the cat’s lifestyle (indoors, outdoors), his age and level of activity.
Figure 2: Royal Canin 5 grade body condition scoring systemModified from Edney and Smith, 1986. Reproduced with permission from Royal Canin, Crown Pet Foods Ltd., UK
Serum potassium
Amount to add to 250 ml 0.9% NaCl
<2 mmol/l 20 mmol
2–2.5 mmol/l 15 mmol
2.5–3 mmol/l 10 mmol
3–3.5 mmol/l 7 mmol
5 mmol represents the minimum daily requirement in anorexic cats
■■ Adequate analgesia, for example sublingual buprenorphine 0.01–0.02 mg/kg q6–12h, should be provided for cats in any painful condition. Recognising pain in cats can sometimes be difficult. If in doubt as to whether a patient would benefit from analgesia, a therapeutic trial can be instituted and behaviour monitored to see whether analgesia results in improvement.
13-17 How To.indd 14 20/10/2010 15:09
companion | 15
HOW TO…
■■ Cats that have been anorexic for 3 days or more should have a feeding tube placed (see below). Timely nutritional support is essential, to prevent both malnutrition and the development of hepatic lipidosis, which is becoming more widely recognised in the United Kingdom.
■■ Appetite stimulants should be avoided until the underlying disease has been identified and treated. If a feeding tube is in place there is no need to worry about nutritional status, as the cat is adequately supported without stimulants.
APPeTITe STIMULANTS*Cyproheptadine (Periactin): An antihistamine with serotonin antagonistic effects. 0.1–0.5 mg/kg orally q8–12h. Therapeutic levels are reached after approximately 3 days. Some owners report cats that become anorexic again if the dose is suddenly stopped, so tapering treatment should be considered. Reported side effects include lethargy or agitation.
Mirtazapine (Zispin): An adrenergic and serotonergic anti-depressant that acts as an appetite stimulant and anti-emetic. The soluble form can be administered through feeding tubes, but should not be given orally. 1.875–3.75 mg per cat q72h. Reduce dose by 30% in cats with renal or hepatic compromise. Monitor blood pressure as can cause hypertension.
[Diazepam: A benzodiazepine used as an appetite stimulant, anticonvulsant, anxiolytic and skeletal muscle relaxant. 0.5–1 mg/kg slow i.v. Use of diazepam is not advised as an appetite stimulant due to the risk of fulminant hepatic necrosis.]
[Prednisolone is sometimes recommended as an appetite stimulant; however it is not suitable for this purpose. Prednisolone can mask some diseases and make them more difficult to diagnose and treat in the longer term (e.g. lymphoma). Rather than inappropriate use of prednisolone, the underlying disease should be identified and treated and appetite stimulated by other means.
[Nandrolone is sometimes given as an appetite stimulant, although there is limited supportive evidence. It is a testosterone with anabolic and anti-catabolic actions. 1–5 mg/kg i.m., s.c. q21days. Maximum dose of 20–25 mg for the cat. It may cause hepatotoxicity.]
ANTI-eMeTICS*Maropitant (Cerenia) 0.5 mg/kg s.c. q24h
Metoclopramide 1–2 mg/kg constant rate infusion; protect from light
Mirtazapine 3.75 mg per cat every 3 days
Chlorpromazine 0.1–0.5 mg/kg s.c. or i.m. q8–12h (for intractable vomiting). May cause sedation and hypotension
■■ In nauseous cats with systemic disease, it is best not to tempt the patient to eat until it is stabilised and recovering. Offering food items early in disease can contribute to food aversion and make it more difficult to get the cat eating. Once the cat is feeling better, it will often start eating voluntarily.
■■ Using feline facial pheromone fraction F3 (Feliway) in the cattery can help reduce anxiety.
Tempting a cat to eat should be done with small food items, which can be warmed to enhance smell. Syringe feeding cats can be stressful and lead to food aversion so, in this author’s opinion, is best avoided. Sometimes placing food in the mouth or on the lips can stimulate the cat to eat, but this method is only suitable for cats that are stable and improving, as again this can encourage food aversion and heighten stress. Some cats respond well to food hides; other cats prefer company and encouragement to start eating.
Getting a cat to eat within a hospital environment can be difficult due to the limitations of space and food placement. For anorectic long-stay patients, large cages are preferable. Utilising vertical space in the cage environment with platforms or boxes can help well-being, but may not be practical if the cat is on intravenous fluids. Cats prefer wide shallow ceramic bowls that are placed at a distance from their litter tray and from their water. Offering a patient only the appropriate prescription diet may be counter-productive. In the short term, the aim is to get the cat eating; a switch to an appropriate diet can be done at home once the cat is stable.
Feeding tube placementFeeding tubes enable enteral nutrition, involving use of all or part of the gastrointestinal tract. enteral nutrition is preferable to parenteral (‘intravenous feeding’) as enterocytes derive 50% of their nutrients directly from the intestinal lumen. If the enterocytes are starved, the intestinal mucosa becomes hypoplastic and
*Editor’s note: Readers are reminded that not all drugs described are authorized for use in this species. Veterinary surgeons should adhere to the prescribing cascade when choosing drugs for use ‘off licence’.
13-17 How To.indd 15 20/10/2010 15:09

16 | companion
HOW TO…
Approach the anorexic cat
hypofunctional, with increased permeability. Furthermore, parenteral nutrition is technically challenging, requires good asepsis and should be reserved for malabsorption syndromes, acute severe pancreatitis and severe persistent vomiting.
Practically, enteral nutrition is suitable in most situations and can be achieved in a number of ways. When choosing the method of enteral nutrition delivery, the site of tube placement should depend on the anticipated duration of support and the site of the disease (tubes should be placed distal to the problem area).
Short-term support
■■ Naso-oesophageal (NO) tube (Figure 3). Use for patients without oral, nasal, pharyngeal or oesophageal disease and that are not vomiting. The advantages are that placement of an NO tube is quick and easy, and does not require anaesthesia or sedation in most cases. However, NO tubes are only suitable for a short duration of use, diet choice is limited by what can pass through the narrow tube diameter, and some cats do not tolerate the positioning of the tube around their face.
affect the whiskers or grooming as much as the naso-oesophageal tube.
■■ Gastrostomy tubes are most practical for long-term feeding (such as in hepatic lipidosis) and are suitable for prolonged use (12 months or more). Tubes can be placed surgically or endoscopically (PeG). Gastrostomy tubes are contraindicated in gastroduodenal disorders, especially where persistent vomiting is present.
■■ Jejunostomy/enterostomy tubes (Figure 5) are rarely indicated and require placement by an experienced surgeon. Consider use in gastric
Figure 3: Naso-oesophageal tube in a cat diagnosed with multifocal alimentary lymphoma, FIV infection and hepatic lipidosis. Naso-oesophageal tubes can be used for short-term support, as in this case, for a few days at home before euthanasia
Figure 4: Oesophagostomy tube in a cat with vestibular disease, secondary to polyp surgery and total bulla osteotomy. Foley catheters can be used if there are no appropriate oesophagostomy tubes available
Figure 5: Jejunostomy tube in a cat with hepatic lipidosis, vomiting and severe malnutrition. The tube attaches to a syringe driver for continuous food infusion. These tubes require intensive management. This cat was supported for 4 weeks until it started eating voluntarily
Longer-term support
■■ Oesophagostomy tube (Figure 4). Very useful and well tolerated in cats. Suitable for cats with oral and nasal disease but not those with vomiting or oesophageal disease. A wide-bore tube can be used, making feeding easier. The tube is comfortably bandaged at the neck and does not
13-17 How To.indd 16 20/10/2010 15:09
companion | 17
HOW TO…
disorders where small intestinal function remains normal. As the stomach is bypassed, food is not mixed and stored appropriately, so the patient is more prone to complications such as vomiting, diarrhoea and abdominal pain. Similarly, continuous infusions are required to trickle food into the intestine.
Feeding guidelines
How much should I feed?Food requirements are based on energy, as this is the most important factor. Calculation of energy requirements is controversial in both human and veterinary patients. For critical care patients, the daily requirements are best calculated from estimated resting energy requirement (ReR). The main controversy involves how much this ReR differs in critical illness. Correction factors used to be applied, but there is no validation for these factors. A better approach is to work with ReR and monitor the patient’s weight and body condition and adjust the intake as necessary. For cats that have not fed for a prolonged period, slowly introduce feeding over a 3-day period, starting at 1/3 ReR divided into multiple small meals. This is particularly important in hepatic lipidosis and severe malnutrition cases, to help avoid refeeding syndrome (where metabolic and fluid disturbances occur within 4 days of reinstituting feeding).
matter produced, although the cat should be monitored closely and hydration kept optimal to ensure against constipation.
How long should I tube feed?
■■ Patients should be supported until their voluntary intake is >85% of maintenance requirements.
■■ Gastrostomy and enterostomy tubes must remain in place for at least 7–10 days to allow a seal to form with the abdominal wall.
■■ Oesophagostomy and gastrostomy tubes can be managed on an out-patient basis, allowing owners to feed their cat at home. This is particularly useful for cats with hepatic lipidosis, chronic kidney disease or those with severe rostral trauma. ■
What diet do I choose?Use any tasty food to get the cat interested initially. Ask the owner for the cat’s preferences. For tube feeding, it is best to use a commercial diet as these will satisfy energy, protein and micronutrient requirements. A high-energy, high-protein, easily digestible diet is recommended, although this may be manipulated depending on the underlying disease. Liquid enteral diets (such as Fortol) are best for small-diameter feeding tubes. Larger-bore tubes can carry liquidised prescription diets. As enteral diets are low residue, there will be little faecal
Readers are reminded that a comprehensive guide to the placement of oesophagostomy tubes and more information on calculating energy requirements can be found in companion February 2010 and in the BSAVA Guide to Procedures in Small Animal Practice.
CASe STUDIeSTo see how these principles can be applied to patients in practice, take a look at the new BSAVA Manual of Rehabilitation, Supportive and Palliative Care. As part of the book’s holistic approach to patient management, feeding considerations are just one aspect considered for cats (and dogs) in a range of situations from postoperative care to trauma. each case also includes information on: medical/surgical management; pain management; fear and stress; physical therapies; nursing and homecare.
Member price: £49Non-member: £75
Options for calculating RER
ReR (kcal) = 70 x (current bodyweight in kilograms)0.75
OR
For animals >5 kg: ReR(kcal) = 30 x BWkg +70
1 kJ = 4.185 kcal
13-17 How To.indd 17 20/10/2010 15:09

18 | companion
CPD
CritiCal Care MediCineHow to save the sickest – 27 January■■ Speaker: Amanda Boag
including hypoadrenocorticism, insulinoma, diabetic ketoacidosis and calcium disorders; and the endocrine effects on blood pressure. There will be a series of tutorials interspersed with case examples for participants to work through in order to allow as much interaction as possible and to provide veterinary surgeons with practical information and useful tips that can help them in their clinical practice.
CliniCal PatHologyinterpretation of biochemical data and an introduction to diagnostic cytology – 26 May■■ Speaker: Elizabeth Villiers
This course will focus on interpretation of biochemical data and cytology. The morning concerns data interpretation and is case-based, with plenty of questions from the speaker to help the delegates work through the cases. These will focus on liver and pancreatic disease, renal disease and electrolyte disturbances. In the afternoon, lectures will cover techniques such as fine needle aspiration and tips on staining and using the microscope, as well as an introduction to cytological interpretation. This is followed by a practical session in which delegates use good-quality microscopes to examine cytology slides with accompanying questions and answers.
git idiseases of the canine and feline liver and pancreas: is diagnosis and treatment a waste of time or can i really make a difference? – 30 June■■ Speaker: Penny Watson
This module will discuss the diagnosis, potential causes and treatment of hepatic and pancreatic diseases in dogs and cats,
endoCrinology iPU/Pd and alopecia: Why dogs and old men are different – 17 February■■ Speaker: Ian Ramsey
Small Animal Medicine Modular
The BSAVA offers a modular programme that will allow you to get a broad new perspective in 2011
Critically ill patients can be some of the most challenging yet rewarding patients we treat. Advances in in-house diagnostics and increased availability of therapeutic options means we are now able to support and treat many more critically ill patients. A successful outcome is most likely when the clinician understands when and how to use advanced critical care techniques whilst never losing sight of the importance of doing the basics well. This one-day course will use a mixture of lectures, case examples and interactive discussion to explore how to maximize survival in the critically ill.
This course is aimed at small animal practitioners who have some experience of endocrine disorders but wish to improve their confidence at dealing with these patients. The course will provide a focus for veterinary surgeons to reflect on current thinking and trends. Every delegate should come away with ideas to put into use in their own practices. Endocrinology can pose many problems, some clinical and others practical, in private practice. This course will provide lots of useful tips for dealing with these cases and help delegates feel more confident when confronted with a dog or cat with PU/PD and/or endocrine alopecia. This will be the fourth year that Ian Ramsey has presented this course. Previous delegates found the course to be both intellectually stimulating and useful for dealing with cases in private practice.
endoCrinology iiendocrine emergencies, collapse and effect on blood pressure – 28 April■■ Speaker: Michael E. Herrtage
Endocrinology II specifically deals with three important problems in veterinary endocrinology: management of the unstable diabetic dog and cat; the approach to episodic collapse, concentrating particularly on the endocrine and metabolic causes of collapse
At the Radisson Blu (SAS) Hotel, near Manchester Airport, between January and November next year,
you can take part in any or all of 8 courses that will offer insight in many aspects of small animal medicine, from emergency care to nutrition.
18-19 CE.indd 18 20/10/2010 15:10

companion | 19
CPD
with a focus on chronic hepatitis in dogs, hepatic lipidosis and cholangitis in cats and chronic pancreatitis in both species. The challenge of differentiating primary from secondary liver disease will be addressed. Medical management of congenital and acquired portosystemic shunts will also be considered, along with controversies in the treatment of acute pancreatitis. There will be some new insights into potential causes of ‘idiopathic’ canine chronic hepatitis and canine chronic pancreatitis, and many case examples will be used to illustrate diseases and treatments. Delegates will be encouraged to perform more biopsies and to read pathology reports more thoroughly. By the end of the course, they should have a better understanding of decision-making in the diagnostic work-up and treatment of those frustrating liver cases.
git iidiseases of the oesophagus, stomach and intestines – 29 September■■ Speaker: Alex German
HaeMatologyanaemia – 27 October■■ Speaker: Clare M. Knottenbelt
Delegates with an interest in small animal internal medicine will develop a clear methodical approach to the investigation and management of red cell disorders. The course will equip delegates with a logical approach to interpreting the haemogram and investigating patients with anaemia or polycythaemia. The investigation of blood loss anaemia, haemolytic anaemia and non-regenerative anaemia will be covered in detail. The management of different causes of anaemia including the role of blood transfusions and immunosuppresive agents will be discussed. The format will primarily be problem-oriented and lecture-based; however, case-based examples of the approaches learnt will provide opportunities for discussion.
CliniCal nUtritionlet food be your first medicine – 24 November■■ Speaker: Penny Watson
Penny Watson will share her nutrition expertise to explain how nutritional
BOOK EARly TO SAVEBook before 13 January 2011 to get a 5% discount on course fees to get more from your CPD budget.
Prices from 13 January 2011 BSaVa Member Fee (inc. Vat)
non Member Fee (inc. Vat)
Full modular £1433.76 £2150.64
Individual module £213.83 £320.74
4 Modules booked at the same time £813.24 £1219.86
Clinical Pathology Individual £238.41 £357.62
early Bird Price – 5% discount on all Small animal Medicine Modular bookings received by 12 January
BSaVa Member Fee (inc. Vat)
non Member Fee (inc. Vat)
Full modular £1362.07 £2043.11
Individual module £203.14 £304.70
4 Modules booked at the same time £772.58 £1158.86
Clinical Pathology Individual £226.49 £339.74
management is as central to the effective treatment of most diseases in dogs and cats as is drug therapy. In some diseases, effective nutrition has been shown to speed recovery and reduce complications and hospitalisation times. But, how many vets know as much about diets as pharmaceuticals and respect dietary modification as much as other treatments?
Good and sufficient feeding speeds recovery from most diseases and surgeries – and yet how often do we monitor dietary intake as closely as fluid intake? Clinical diets should not be used without a good knowledge of the indications and possible side effects – inappropriate use of clinical diets can lead to severe and potentially life-threatening ‘reactions’ such as acute pancreatitis. It is therefore important not just to reach for the bag with the name of the disease on it, but also to understand what is in the bag! ■
This module will consider disorders of the canine and feline oesophagus, stomach and intestines. Initially, approach to diagnosis and management will be reviewed, followed by in-depth discussions about current GI tests and investigating problem cases. The latest information (and controversies) on various gastrointestinal disorders will also be covered. Interactive case-based sessions will also be used to illustrate approach to diagnosis and management.
For more information or to book visit www.bsava.com, email [email protected] or call 01452 726700
18-19 CE.indd 19 20/10/2010 15:10

20 | companion
PUBLICATIONSPUBLICATIONS
New ventureat EdinburghIn June of this year the Hospital for Small Animals at the royal (Dick) School of Veterinary Studies opened its doors to the public to receive and treat injured wildlife. Emma keeble, the driving force behind this new initiative, explains further
The opening of the wildlife emergency clinic at Edinburgh’s veterinary school is a new and exciting venture, the first of its kind at a Uk vet
school, and aims to help teach veterinary students about wildlife medicine and surgery. The hope is to encourage an interest in treating wildlife when in general practice and to provide basic training of all students graduating from Edinburgh in this subject. It also enables full case responsibility and encourages self-thought and decision-making.
The clinics are student-led, with final year students on clinical rotation responsible for each case from the point of admission to release or rehabilitation. Veterinary surgeons with specialist knowledge in the field are at hand to advise and supervise the students at all times, but the overall aim is to encourage the students to manage their own cases at all levels. This will lead to experience in wildlife triage assessment, practical emergency first aid skills and wildlife handling skills as well as an understanding of the unique biology and ecology of each species.
FundingThe clinic relies entirely on donations from the general public and the money generated from fundraising activities. The students were asked to help raise an initial fund to start the clinic. Members of the student Edinburgh Veterinary Zoological Society rose to the challenge, organising cake stalls, raffles and sponsored events. With the money these events raised, as well as generous donations from the Dick Vet Fundraising Committee and a member of the public, the students raised over £500 towards the set-up costs of the clinic.
20-22 Publications.indd 20 20/10/2010 15:10
companion | 21
PUBLICATIONS
Wildlife casualtiesEncounters with wildlife casualties are sadly increasingly commonplace (Figure 1). Whether these are due to natural occurrences or manmade problems, such as road traffic accidents in owls, fishing hook injuries in swans or litter entanglement in hedgehogs, there is a duty of care for the welfare of that animal. With the facilities and expertise available at the clinic, immediate assessment to determine the extent of the problem and triage to deliver emergency first aid care are possible.
We have a dedicated wildlife ward at the Dick Vet with facilities to house all wildlife casualties, from heated incubators for baby mice and hedgehogs, to isolation pens for deer, foxes and badgers. There are specially designed pens with pools for injured waterfowl and a larger outdoor pool for injured seal pups. We also have facilities for washing birds and mammals covered in oil.
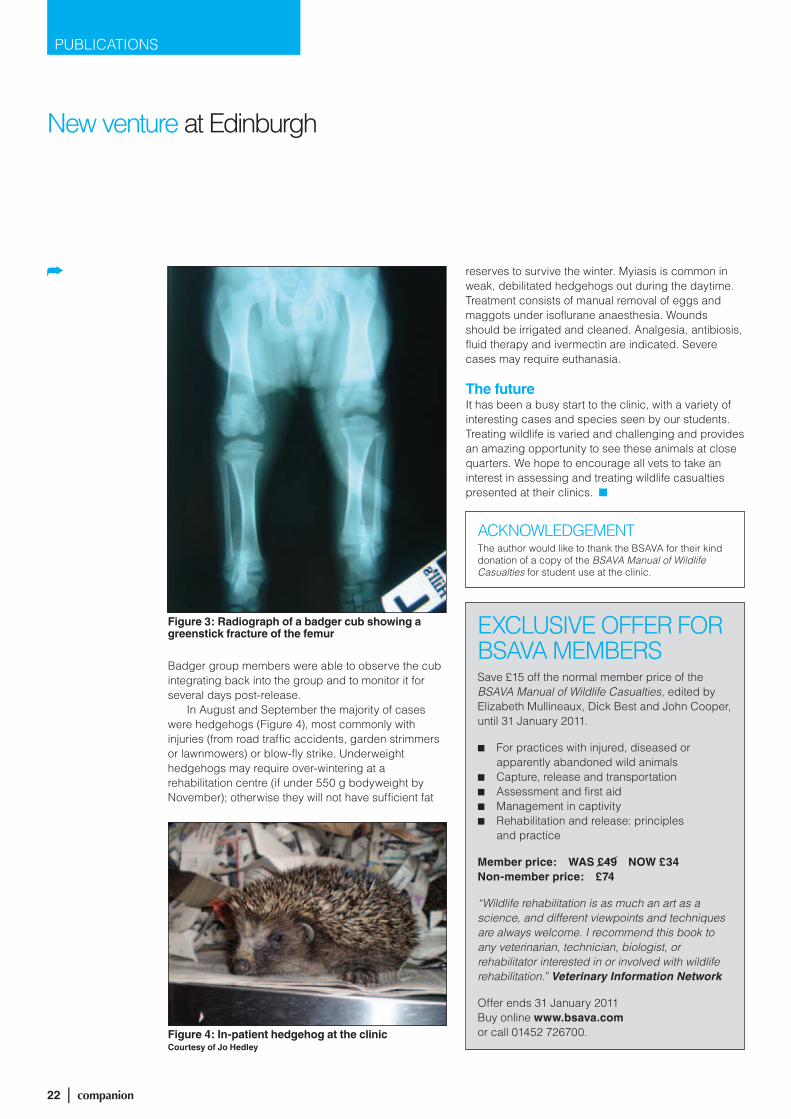
Figure 2: Eye examination of a roe deer involved in a road traffic accidentCourtesy of Livia Benato
June also saw an influx of roe deer injured in road traffic accidents. Head trauma is commonly seen and early triage with full clinical examination is essential in these cases (Figure 2). Central blindness is often diagnosed and carries a poor prognosis. Severe internal haemorrhage and bruising may not be evident externally but are extremely common and also carry a poor prognosis. Deer that can be easily handled or clinically examined without sedation are likely to be either juvenile or severely injured. Euthanasia should be considered in severely injured cases. There are also considerable welfare issues associated with keeping deer in captivity. Deer should be kept away from other animals, ideally in specialist facilities, since they are easily stressed. Extreme care is required when handling deer to avoid injury to the handler. In cases with injuries requiring long-term rehabilitation, the decision whether to euthanase or to treat should be carefully weighed.
Figure 1: Juvenile sparrow presented at the wildlife emergency clinic
First visitorsTo date the clinic has been busy. In June the most common admissions were fledgling birds, the majority of which had been attacked by cats. Superficial wounds were treated with topical antiseptic, cleaning and systemic analgesia and antibiotics. Septicaemia is a common secondary problem in birds injured by cats and systemic antibiotics are essential in these cases. Pasteurella multocida is the organism most commonly isolated.
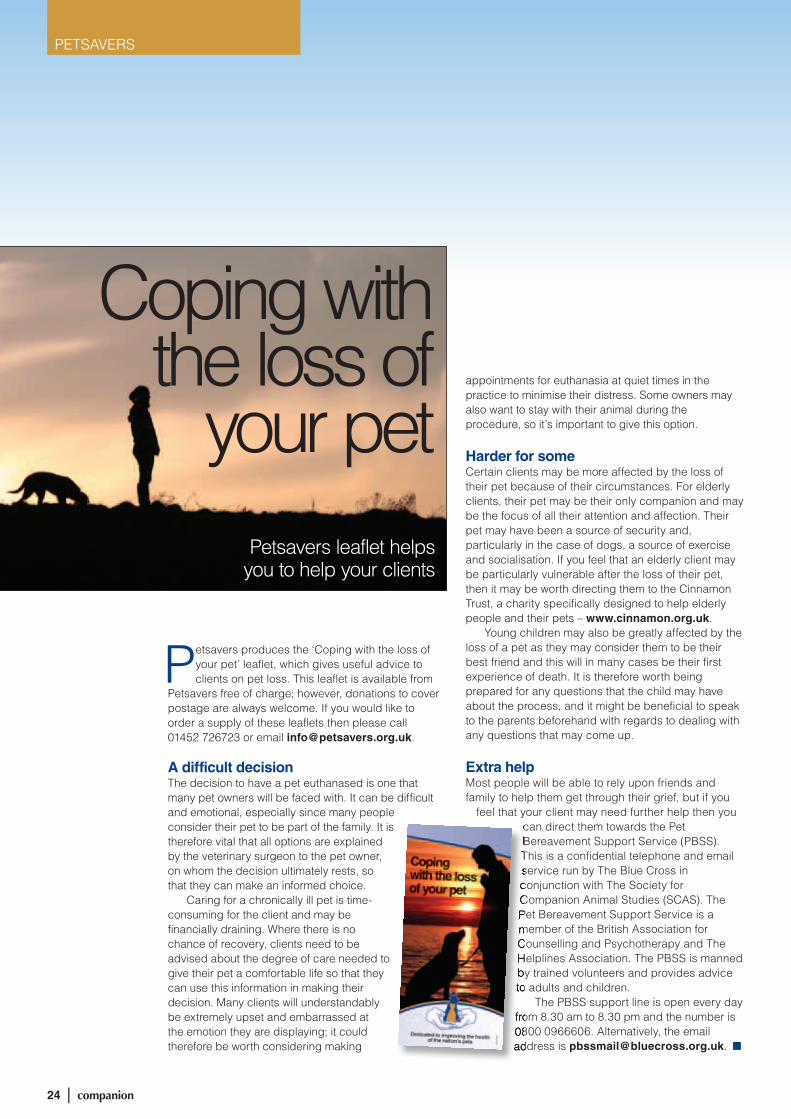
Summer admissionsIn July a juvenile badger was admitted to the clinic after being observed by a local badger group as lame and outside the sett during the day. After sedation, radiography revealed a greenstick fracture of the femur, possibly secondary to a bite wound (Figure 3). Analgesia, systemic antibiotics and a support bandage were used and the badger cub recovered well, being released back to its own sett 3 days later.
20-22 Publications.indd 21 20/10/2010 15:11
22 | companion
PUBLICATIONS
New venture at Edinburgh
Figure 4: In-patient hedgehog at the clinicCourtesy of Jo Hedley
reserves to survive the winter. Myiasis is common in weak, debilitated hedgehogs out during the daytime. Treatment consists of manual removal of eggs and maggots under isoflurane anaesthesia. Wounds should be irrigated and cleaned. Analgesia, antibiosis, fluid therapy and ivermectin are indicated. Severe cases may require euthanasia.
The futureIt has been a busy start to the clinic, with a variety of interesting cases and species seen by our students. Treating wildlife is varied and challenging and provides an amazing opportunity to see these animals at close quarters. We hope to encourage all vets to take an interest in assessing and treating wildlife casualties presented at their clinics. n
Figure 3: Radiograph of a badger cub showing a greenstick fracture of the femur
Badger group members were able to observe the cub integrating back into the group and to monitor it for several days post-release.
In August and September the majority of cases were hedgehogs (Figure 4), most commonly with injuries (from road traffic accidents, garden strimmers or lawnmowers) or blow-fly strike. Underweight hedgehogs may require over-wintering at a rehabilitation centre (if under 550 g bodyweight by November); otherwise they will not have sufficient fat
ACkNOWLEDgEMENTThe author would like to thank the BSAVA for their kind donation of a copy of the BSAVA Manual of Wildlife Casualties for student use at the clinic.
ExCLUSIVE OFFEr FOr BSAVA MEMBErSSave £15 off the normal member price of the BSAVA Manual of Wildlife Casualties, edited by Elizabeth Mullineaux, Dick Best and John Cooper, until 31 January 2011.
■n For practices with injured, diseased or apparently abandoned wild animals
■n Capture, release and transportation■n Assessment and first aid■n Management in captivity■n rehabilitation and release: principles
and practice
Member price: WAS £49 NOW £34Non-member price: £74
“Wildlife rehabilitation is as much an art as a science, and different viewpoints and techniques are always welcome. I recommend this book to any veterinarian, technician, biologist, or rehabilitator interested in or involved with wildlife rehabilitation.” Veterinary Information Network
Offer ends 31 January 2011Buy online www.bsava.com or call 01452 726700.
20-22 Publications.indd 22 20/10/2010 15:11

companion | 23
PETSAVERS
Improving the health of the nation’s pets
Focus on Petsavers project
Bacterial culture of urine is commonly performed in veterinary practice. It is accepted that cystocentesis is the most reliable method of
collection of urine to avoid false positive bacterial cultures but the optimal method of submission of urine to the laboratory remains controversial. The addition of boric acid to urine samples is recommended by some laboratories, as it is suggested that this may prevent bacterial growth during transit to the laboratory, therefore preventing accidental bacterial contaminants from producing
Rachel Burrow details her Petsavers grant awarded project, undertaken at the University of Liverpool with Laura Blackwood and Mary Rowlands, looking at the effect of boric acid on bacterial culture of cat and dog urine submitted to the laboratory by rapid service postal delivery
Improving the health of the nation’s petsImproving the health of the nation’s petsImproving the health of the nation’s pets
Focus on Petsavers
false positive results; however, this remains unproven. The aim of this study, funded by Petsavers, was to identify the optimal method of canine and feline urine submission to the laboratory for culture.
In this study, urine specimens were obtained by cystocentesis from dogs and cats suspected of having urinary tract infections. Each specimen was divided into three aliquots. The first provided our ‘true’ reference test result and was collected without preservative. This was analysed on site at the University of Liverpool Veterinary Pathology Laboratory, with urine culture and cytological examination of the urine sediment performed within 2 hours of collection. The other two aliquots were stored at room temperature for up to 7 hours and then posted by guaranteed next day delivery to Idexx Laboratories, UK, where culture was performed.
One aliquot was placed in a sterile container without preservative; the other aliquot was placed in a sterile container containing the preservative boric acid. Urine bacterial counts higher than 1x103 colony-forming units/ml were considered significant.
The results of this study revealed that there was no significant difference between reference test results and those of samples posted without preservative. However, samples posted in boric acid were significantly less likely to give a positive result, suggesting that the addition of boric acid can actually ‘mask’ a true bacterial infection.
‘In-house’ cytological evaluation of the reference urine samples demonstrated that 17% of samples with a positive culture had normal findings on sediment examination.
In conclusion, the findings of our study suggest that to maximise the chance of achieving a true positive identification of a urinary tract infection it is better for veterinary surgeons to submit urine samples in plain rather than boric acid tubes for overnight posting. This study suggests that urine sediment examination is not very sensitive at predicting urinary tract infection and hence urine cultures should always be recommended to confirm a suspected diagnosis of urinary tract infection. ■
23-24 Petsavers.indd 23 20/10/2010 15:11
24 | companion
PETSAVERS
Petsavers produces the ‘Coping with the loss of your pet’ leaflet, which gives useful advice to clients on pet loss. This leaflet is available from
Petsavers free of charge; however, donations to cover postage are always welcome. If you would like to order a supply of these leaflets then please call 01452 726723 or email [email protected].
A difficult decisionThe decision to have a pet euthanased is one that many pet owners will be faced with. It can be difficult and emotional, especially since many people consider their pet to be part of the family. It is therefore vital that all options are explained by the veterinary surgeon to the pet owner, on whom the decision ultimately rests, so that they can make an informed choice.
Caring for a chronically ill pet is time-consuming for the client and may be financially draining. Where there is no chance of recovery, clients need to be advised about the degree of care needed to give their pet a comfortable life so that they can use this information in making their decision. Many clients will understandably be extremely upset and embarrassed at the emotion they are displaying; it could therefore be worth considering making
appointments for euthanasia at quiet times in the practice to minimise their distress. Some owners may also want to stay with their animal during the procedure, so it’s important to give this option.
Harder for someCertain clients may be more affected by the loss of their pet because of their circumstances. For elderly clients, their pet may be their only companion and may be the focus of all their attention and affection. Their pet may have been a source of security and, particularly in the case of dogs, a source of exercise and socialisation. If you feel that an elderly client may be particularly vulnerable after the loss of their pet, then it may be worth directing them to the Cinnamon Trust, a charity specifically designed to help elderly people and their pets – www.cinnamon.org.uk.
Young children may also be greatly affected by the loss of a pet as they may consider them to be their best friend and this will in many cases be their first experience of death. It is therefore worth being prepared for any questions that the child may have about the process, and it might be beneficial to speak to the parents beforehand with regards to dealing with any questions that may come up.
Extra helpMost people will be able to rely upon friends and family to help them get through their grief, but if you
feel that your client may need further help then you can direct them towards the Pet Bereavement Support Service (PBSS). This is a confidential telephone and email service run by The Blue Cross in conjunction with The Society for Companion Animal Studies (SCAS). The Pet Bereavement Support Service is a member of the British Association for Counselling and Psychotherapy and The Helplines Association. The PBSS is manned by trained volunteers and provides advice to adults and children.
The PBSS support line is open every day from 8.30 am to 8.30 pm and the number is 0800 0966606. Alternatively, the email address is [email protected]. ■
Coping with the loss of
your petPetsavers leaflet helps
you to help your clients
can direct them towards the Pet Bereavement Support Service (PBSS). This is a confidential telephone and email service run by The Blue Cross in conjunction with The Society for Companion Animal Studies (SCAS). The Pet Bereavement Support Service is a member of the British Association for Counselling and Psychotherapy and The Helplines Association. The PBSS is manned by trained volunteers and provides advice to adults and children.
from 8.30 am to 8.30 pm and the number is 0800 0966606. Alternatively, the email address is
23-24 Petsavers.indd 24 20/10/2010 15:11

companion | 25
Get ready for WSAVA World Congress 2011!
On behalf of the 2011 WSAVA•FASAVA World Congress Organizing Committee, I am delighted to invite you to the 2011
WSAVA•FASAVA World Congress, to be held on 14–17 October 2011 in Jeju Island, the Republic of Korea. The Organizing Committee is preparing to make this event a great forum for exchanging the latest information on veterinary medicine and making friends among fellow veterinary surgeons from all over the world.
The 2011 WSAVA•FASAVA World Congress will be a top-class congress that offers lectures by first-rate scholars and experts in veterinary science around the world and will cover the latest trends and information on advanced technologies in veterinary science. In order to present a high-quality academic congress, the Organizing Committee has cooperated consistently and closely with various international veterinary associations, assisted by the WSAVA Headquarters. As a result, the congress will feature some 250 lectures delivered by 91 scholars in 33 topics.
The congress will be held for four days from Friday to Monday for the convenience of all participants, including veterinary practitioners and scholars. All participants will be given a certificate of participation.
Those from Korea and the United States will be awarded continuing education credit. English will be the official language during the congress, but a simultaneous interpretation service in Japanese, Chinese and Korean will be available for certain lectures. In addition, multi-language services will be provided during the congress for the convenience of the participants from non-English-speaking countries.
Jeju Island, the venue of the 2011 WSAVA•FASAVA World Congress, is a beautiful place designated as a World Natural Heritage site by UNESCO for its natural beauty, unique culture and clean and comfortable resorts. Korea is a dynamic country with 5000-year history, boasting numerous historical and recreational sites. We look forward to welcoming you in 2011!
Jong-Il Kang, DVM9th President, Korean Animal Hospital Association/
Director of Committee At-Large,2011 WSAVA•FASAVA World Congress
Jong-Il Kang, President of the Korean Animal Hospital Association, gives a warm welcome to Jeju Island, Korea
25-27 WSAVA News.indd 25 20/10/2010 15:30

26 | companion
WSAVA NEWS
PRACTICE, ENLIGHTENMENT, WELCOME AND HOPEWe have used the image of the Korean traditional lantern, chung-sa-cho-rong to emphasize the Korean image of practice, enlightenment, welcome and hope. Within this image, small animals and the bright light become one to symbolize the light of hope this congress brings. By using a brush technique and the red and the blue of the yin and yang, we tried to differentiate the symbol for the Korean congress from meetings in previous years.
REGISTRATION ■ Early-Bird Registration: 1 January to
28 February 2011 ■ Pre-Registration: 1 March to
30 September 2011Please contact [email protected] visit www.wsava2011.org for more information:
JOON-HO JUNG APPOINTED HONORARY AMBASSADOR FOR WSAVA 2011!
Joon-Ho Jung has been appointed as honorary ambassador for the 2011 WSAVA·FASAVA World Congress by the Korean organizing committee. Jung was chosen not only because he is a renowned film star who has performed in many smash hit dramas, but also because of his animal-friendly and warm personality.
■ Acupuncture / Herbal Medicine ■ Animal Welfare ■ Behaviour ■ Cardiology and Pulmonology ■ Critical Care and
Anaesthesiology & Traumatology
■ Cytology, Haematology & Clinical Pathology
■ Dentistry ■ Dermatology
■ Diagnostic Imaging ■ Ear-Nose-Throat ■ Endocrinology ■ Exotics ■ Feline Medicine ■ Gastroenterology ■ Hepatology ■ Hereditary & Genetic Diseases ■ Parasitic Diseases ■ Medicine (Standards of Care) ■ Nephrology & Urology
■ Nutrition ■ Pharmacology ■ Reproduction ■ Surgery (Soft Tissue Surgery) ■ Surgery (Orthopaedic Surgery) ■ Surgery (Onco-surgery) ■ Veterinary Management ■ NAVC – Oncology ■ NAVC – Ophthalmology ■ WSAVA Award Lectures
FASAVA FACTSFASAVA is a non-profit organization that was formed to encourage communication and cooperation between veterinarians throughout the Asian Pacific region and to promote the adoption of new technology and techniques. Its objective is to develop and increase the status of veterinary knowledge in the Asian Pacific region in order to substantially improve the welfare and health of animals in the Asian region. It holds a Congress every two years and member countries include Australia, Hong Kong, Korea, Malaysia, New Zealand, Thailand and Taiwan.
WSAVA STATE OF THE ART LECTURES
25-27 WSAVA News.indd 26 20/10/2010 15:30

companion | 27
WSAVA NEWS
major public health issues and needs in the next 15 years. Many of these issues are with us now, especially those driven by environmental factors such as global warming and increasing pressures on land usage and freshwater requirements. We need to approach these issues in a holistic and cooperative way if we want to be able to predict and respond to outbreaks of emerging diseases with greater certainty and speed and, in so doing, ensure that our world remains a healthy environment for future generations.
Michael Day and Diane Sheehan will represent the WSAVA ‘One Health’ Committee to give presentations on Positioning Companion Animals in Global Infectious Disease Surveillance and Promoting Comparative Clinical Research – the Value of the Companion Animal Model.
The host city, Melbourne, is renowned as a global sports capital and the surrounding area offers something for everyone. So the invitation goes beyond the science and thought and extends to enjoying all that Australia has to offer as a unique venue for such meetings. We look forward to sharing this with you in February 2011. Visit www.OneHealth2011.com for more information. ■
This inaugural International ‘One Health’ Congress will focus on the risks and challenges brought about by the interactions between animal and human
health and the environment. It will consider these in the general context of the science and research being undertaken, but critically it will focus on the outcomes that need to be achieved to manage effectively the growing risks to global health.
The congress aims to provide an opportunity to think ‘outside the box’ and into the future in order to make recommendations on policy and organizational changes, using the underlying science to inform and drive the process. For the first time it is envisaged that a global consideration of interrelated issues of animal and human health and the relationship with the environment can take the science to the policy-makers, and thus drive real and profound change. We see this as setting a pathway that in the next 10–15 years will result in a seamless approach to infectious disease management, with a close link between the resources and those with the skills and knowledge.
We expect the meeting to define the current situation and, based on this knowledge, to develop a vision of the
The first International‘One Health’ Congress will be
held in Melbourne, Australia, on 14–16 February 2011
One Health Congress
25-27 WSAVA News.indd 27 20/10/2010 15:31
28 | companion
THE companion INTERVIEW
Harvey LockeBVSc CertSAC MRCVS
Harvey Locke was born and brought up in Stockport. His father was a company director and his mother stayed at home to bring up the family. He has one brother who has worked for Intervet all his career and lives in Norfolk. Harvey was educated at Stockport Grammar School, as were both his daughters. A 1969 Liverpool graduate, he spent four years in mixed practice in Staffordshire before returning to his home town and entering small animal practice. There are now five generations of vets in the family. His great grandfather was president of the RCVS 1909–10 but tragically died during his year of office and his grandfather was also RCVS President in 1935–36, and was an equine practitioner with a practice in the centre of Manchester, looking after the city’s working horse population. Harvey’s uncle Richard and his son David both devoted their careers to the State Veterinary Service. The dynasty has continued with his niece Samantha joining the profession in 2005 and going into mixed practice in Suffolk. Harvey’s younger daughter Helen qualified from Liverpool in 2009 and is in small animal practice in Lancashire. Her elder sister Rachel works for Mars Petcare at Waltham and has just completed a three year management training programme. Harvey was BSAVA President 1999–2000 and is now President of BVA.
QWhat do you consider to be your most important achievement?
AThis has to be the success of my practice, Woodcroft Veterinary Group. In 1976, I bought a rather dilapidated house in Heaton Moor,
slapped some paint on the walls, put my plate up and waited for the first client. This happened to be a friend with a budgie which had to be put to sleep and I hadn’t the heart to charge her a fee. I thought this had better not become a habit or I would end up bankrupt. The practice started to grow and I joined up with David Skilton who had a single-handed
practice on the other side of town and then shortly afterwards Geoff Little joined us. The partnership thrived and the group now has 18 vets, a central veterinary hospital and five branches. The practice also provides a multidiscipline referral service and an emergency clinic providing 24 hour cover for 21 local practices.
What has been your main interest outside work?I love being outdoors, whether it is walking in the Peak District or the Lakes with our local walking group or sailing with friends around the Balearics in the Med where I have a share in a yacht.
28-29 Interview.indd 28 20/10/2010 14:31

companion | 29
THE companion INTERVIEWTHE companion INTERVIEW
If you were given unlimited political power, what would you do with it?Ensure everyone is given the same opportunities in life; then what they do with them is a personal choice. I would also like to stamp out government corruption, especially in third world countries where so many people are suffering often needlessly because resources are being siphoned off before getting to the needy.
Which historical or literary figure do you most admire?Nelson Mandela without a doubt – what an amazing person, to be able to suffer so much and so long for his beliefs and, when he was finally released from all those years incarcerated on Robben Island, to have such an influence not only on his native South Africans but on a global scale by showing no desire for retribution and only goodwill.
If you could change one thing about yourself what would it be?I would like to think that I am not a vain person so I am happy with my appearance but if I could change one thing it would be not to prejudge people at the first meeting and always try to appreciate that another person’s views are always worthy of consideration.
What is your most important possession? This has to be my family, although during my BVA presidential year my laptop and mobile phone run a close second. They have become permanent appendages.
What would you have done if you hadn’t been a vet?This is a difficult one as I have never wanted to do anything other than follow a veterinary career, but I have always had a love of flying and obtained my private pilot’s licence back in the 1970’s. However, the pressure on disposable income when the family came along meant the flying had to stop. If I had not been a vet then being an airline pilot would have been the next choice. n
When and where are you happiest?At the end of a strenuous day’s sailing, anchoring up in a quiet cove and sharing a beer or two with friends on board.
Who has been the most inspiring influence on your career?When I was 14 years old I asked our local vet, a charming Scot called Angus Andrew, if I could come and do some work experience. I spent as much time as possible in his practice at weekends and school holidays.
He was a brilliant mentor, always having time to teach and inspire me about life as a vet. Providing work experience to young people can sometimes seem a nuisance in a busy clinic but I always remind myself of the patience that Angus showed to me when we have students in our practice.
What is the most significant lesson you have learned so far?To decide what you want to achieve and go for it. There will be set backs but persistence will pay off in the end.
What do you regard as the most important decision that you have made?Getting married to Margaret and being blessed with two lovely daughters. On a professional basis an important decision was allowing myself to be persuaded by Ian Hughes to get involved with the running of North West BSAVA – this has led to 25 years of involvement in veterinary politics in BSAVA, in Europe and now with BVA. I have made many great friends. I would urge younger vets to get involved with association work – it is very rewarding and gives you a much broader insight into our profession.
What is the most frustrating aspect of your work?The increasing bureaucracy of health and safety regulations and employment law can be very frustrating. Don’t get me wrong, I appreciate that many of these laws are necessary but some do seem to go over the top. Increasing client expectations are tending to drive vets to practice defensive medicine which is not always in the best interest of the animal.
…if I could change one thing it would be not to prejudge people at the first meeting and always try to appreciate that another person’s views are always worthy of consideration.
28-29 Interview.indd 29 20/10/2010 14:31

30 | companion
SCOTTISH CONGRESS
From its beginning in Crieff to a number of years at St Andrews, Scottish Congress has had a number
of homes, and the latest move to Edinburgh was influenced by feedback from delegates and exhibitors, as well as the changes in the type of CPD requested.
The key guiding principle of BSAVA regional CPD has always been providing world-class affordable science to small animal veterinary practitioners. This year Scottish committee did not disappoint with their annual weekend.
Super Scottish scienceThe keynote speakers were: Derek Flaherty, the renowned anaesthetist and speaker from Glasgow Vet School who lectured to the vets and nurses on anaesthesia and analgesia; Amanda Boag, double boarded diplomate in Medicine and Emergency & Critical Care, who gave a very lively and engaging lecture stream to the veterinary nurses; and Sue Paterson, specialist in dermatology based at Rutland House referrals, who spoke to the vets on skin disease, from the routine to the more weird and wonderful.
One stream of the scientific programme was dedicated directly to
veterinary nurses, and this proved very popular with delegates. Again the seminar stream provided delegates with the opportunity to see some world-renowned speakers, such as Professor Stuart Carmichael who gave a thought-provoking and informative talk on arthritis in dogs, and also newcomers to the lecturing world who no doubt will be of similar renown in years to come.
Great new venueEdinburgh Conference Centre is based at Herriot Watt University campus, and the facilities were one of the factors influencing the switch of venue, along with the ease of transport and reduced costs. Delegates and Exhibitors were pleasantly surprised by the facilities, with the committee overhearing comments such as, “I couldn’t believe the range of food available for breakfast or the amount you could have”, and, “I had so much at breakfast I’m too full for lunch”.
BSAVA Scottish Congress has always been very grateful for the support of many commercial companies, and this year with over two hundred delegates in total the exhibitors were kept occupied informing delegates of the options for veterinary equipment, services and technology.
The social side of Scottish Congress is critical to its appeal, and this year’s gala dinner in Dynamic Earth lived up to the expectations with over 250 people attending. Nestled between the Scottish Parliament building, and the imposing Arthur’s Seat, the venue was a great appeal, especially for those delegates who had travelled from as far as Australia and Canada.
After a drinks reception within the museum itself, the bagpipes called the diners to take their seats for a three-course dinner in the stunning venue. This was accompanied by an address to the diners by Grant Petrie, the current President of BSAVA. He took the opportunity to highlight passionately the provision of CPD by BSAVA throughout the UK, the launch of the BSAVA Certificate, and to pay thanks – on behalf of all those attending – to the volunteers without which the weekend could not have occurred.
After dinner there was much celebration, with a lively ceilidh until late in the evening, and a friendly bar as many delegates reinforced old acquaintances, while others made new friends.
Please email [email protected] if you would like to be kept informed of the date, venue and CPD for next year’s Scottish Congress, or visit www.bsava.com n
Spotlight on Scottish CongressThe 25th Annual BSAVA Scottish Congress in Edinburgh was a huge success and delegates delighted in the new venue, the great science, and the superb social
HEARD AT CONGRESS“It’s been a great weekend and you should be proud of what you have achieved” Exhibitor
“Excellent value for money, and super location” Delegate
“I really enjoyed the congress, I will certainly try to go again next year” Delegate
“The lectures have all been excellent, the venue is great and it was ideally situated for me” Delegate
“Well done to Scottish committee for a well organised and informative Congress this year” Delegate
“Congratulations to the Scottish Region volunteers for what they achieve year after year and for putting on yet another great meeting in 2010” Grant Petrie, BSAVA President
SCOTTISH CONGRESS
30-31 Diary.indd 30 20/10/2010 14:31
companion | 31
CPD diary
EVENING MEETING – SURREY AND SUSSEX REGION
Thursday 11 NovemberPancreatitisSpeaker: Penny WatsonLeatherhead Golf Club, Kingston Road, Surrey KT22 0EEDetails from [email protected]
EVENING MEETING – SCOTTISH REGION
Thursday 18 NovemberChronic diarrhoeaSpeaker: Rory BellGlasgow Vet School, 464 Bearsden Road, Glasgow G61 1QHDetails from [email protected]
EVENING MEETING – SOUTHERN REGION
Wednesday 24 November Medical mystery tour: challenging medical casesSpeaker: David ChurchPotters Heron Hotel, Romsey SO51 9ZFDetails from [email protected]
DAY MEETING – NORTH EAST REGION
Sunday 28 November Feline itchySpeaker: Peter ForsytheThorpe Park Hotel, 1150 Century Way, Leeds, West Yorkshire LS15 8ZBDetails from [email protected]
EVENING MEETING – SOUTH WEST REGION
Wednesday 1 December ToxicologySpeaker: Alex CampbellAlveston House Hotel, Alveston, Thornbury, Bristol BS35 2LADetails from [email protected]
EVENING MEETING – NORTHERN IRELAND REGION
Thursday 2 December NeurologySpeaker: Nick JefferyVSSCo, Lisburn, Co AntrimDetails from [email protected]
DAY MEETING – EAST ANGLIA REGION
Sunday 21 November Feline lower urinary tract disease (FLUTD)Speakers: Jane Ladlow & Martha CannonThe Cambridge Belfry, Cambourne, Cambridge CB23 6BWDetails from [email protected]
DAY MEETING – METROPOLITAN REGION
Saturday 13 November Practical ultrasonography: the abdomenSpeaker: Francisco Llabrés DiazDavies Veterinary Specialists, Manor Farm Business Park, Higham Gobion, Hertfordshire SG5 3HRDetails from [email protected]
DAY MEETING – NORTH WEST REGION
Wednesday 17 November Chronic vomiting and diarrhoeaSpeaker: Clive ElwoodHoliday Inn, HaydockDetails from [email protected]
DAY MEETING – SOUTH WALES REGION
Wednesday 17 NovemberCats, canines, creatinine and calcium: renal disease through the eyes of a pathologist. Introducing IRISSpeaker: Nick CarmichaelSMART Clinic, Cardiff CF3 2EQDetails from [email protected] ADDITIONAL CPD COURSES
Visit www.bsava.com for full details
EVENING MEETING – NORTH EAST REGIONWednesday 8 December An approach to the hot dog – and cat!Speaker: Roger Wilkinson
EVENING MEETING – MIDLANDS REGIONThursday 9 DecemberTop tips in abdominal surgerySpeaker: Liz Welsh
DAY MEETING
Thursday 11 NovemberAngry eyes: uveitis, glaucoma and orbital diseaseSpeakers: Christine Heinrich & Claudia HartleyKettering Park Hotel & Spa, Northants NN15 6XTDetails from [email protected]
DAY MEETING
Thursday 25 NovemberCanine and feline medical neurologySpeaker: Jacques PenderisThorpe Park Hotel & Spa, Leeds LS15 8ZBDetails from [email protected]
DAY MEETING
Thursday 2 DecemberPoor vision: diseases of retina, lens and beyondSpeakers: Christine Heinrich & Claudia HartleyKettering Park Hotel & Spa, Northants NN15 6XTDetails from [email protected]
DAY MEETING
Tuesday 7 December Medicine, surgery and emergency care of retilesSpeakers: Simon Girling & Romain PizziMottram Hall, Cheshire SK10 4QTDetails from [email protected]
DAY MEETING – MIDLANDS REGION
Wednesday 17 November Steps towards more successful dentistrySpeaker: Norman JohnsonYew Tree, Kegworth, Derby DE74 2DFDetails from [email protected]
DAY MEETING
Thursday 18 November Neurology for Busy Practitioners RoadshowSpeakers: Simon Platt & Laurent GarosiYew Tree, Kegworth, Derby DE74 2DFDetails from [email protected]
Neurology for Busy Practitioners
DAY MEETING
Friday 19 November Neurology for Busy Practitioners RoadshowSpeaker: Simon Platt & Laurent GarosiOulton Hall, Rothwell Lane, Leeds LS26 8HNDetails from [email protected]
Neurology for Busy Practitioners
DAY MEETING
Monday 22 November Neurology for Busy Practitioners RoadshowSpeakers: Simon Platt & Laurent GarosiMiskin Manor Country Hotel and Health Club, Miskin, nr Cardiff CF72 8NDDetails from [email protected]
Neurology for Busy Practitioners
DAY MEETING
Tuesday 23 November Neurology for Busy Practitioners RoadshowSpeakers: Simon Platt & Laurent GarosiGorse Hill, Hook Heath Road, Woking, Surrey GU22 0QHDetails from [email protected]
Neurology for Busy Practitioners
DAY MEETING
Tuesday 23 NovemberClinical nutrition: let food be your first medicineSpeaker: Penny WatsonBSAVA Headquarters, Gloucester GL2 2ABDetails from [email protected]
30-31 Diary.indd 31 20/10/2010 14:31

British Small Animal Veterinary AssociationWoodrow House, 1 Telford Way, Waterwells Business Park,
Quedgeley, Gloucester GL2 2ABTel: 01452 726700 Fax: 01452 726701
Email: [email protected]: www.bsava.com
For more information or to order visit www.bsava.com, email [email protected] or call 01452 726700.Order online to save on Postage & Packing
NEW Manuals From BSAVA Publications
BSAVA Manual of Canine and Feline
Rehabilitation, Supportive and Palliative Care:Case Studies in Patient ManagementEdited by Samantha Lindley and Penny Watson
Published September 2010 416 pagesMember price £49Price to non-members £75
BSAVA Manual of Canine and Feline
Reproduction and Neonatology, 2nd editionEdited by Gary Englandand Angelika von Heimendahl
Companion animals are undergoing previously uncontemplated treatments and surviving what would once have been rapidly fatal conditions. This truly innovative Manual is aimed at the whole veterinary team, and includes:
■ The principles behind pain and its management, clinical nutrition and physical therapies
■ Clinical applications with reference to published evidence ■ Case Studies presenting a range of canine and feline patients,
designed to illustrate the considerations to be made and the options available
Published October 2010 240 pagesMember price £45Non-member price £75
This fully updated new edition covers:
■ The reproductive cycle ■ Infertility ■ Pregnancy and parturition ■ Neonatology ■ Clinical approach to common conditions
32 OBC.indd 32 20/10/2010 14:30