common elbow fractures in children - zielinski …zielinskifam.com/lit/peds/ped-elbow.pdfcommon...
TRANSCRIPT
American Family Physician
Common Elbow Fractures in ChildrenDALE J. TOWNSEND, M.D., and GEORGE S. BASSETT, M.D.Childrens Hospital Los Angeies, Los Angeles, California
Approximately 75 percent of all fracturessustained by children occur in tiie upperextremities and frequently occur during afaii onto an outstretched hand. The majorityof these injuries involve the wrist and fore-arm, but the elbow alone accounts for ap-proximately 10 percent of all fractures inchildren. Eibow fractures in chiidren arechalienging because of the abundance ofunossified cartilage and the high potentialfor iimb-threatening damage to neurovascu-iar structures. Common types of elbow frac-tures include supracondylar, iaterai condy-lar, mediai epicondyiar, radiai neck andtransphyseal fractures.
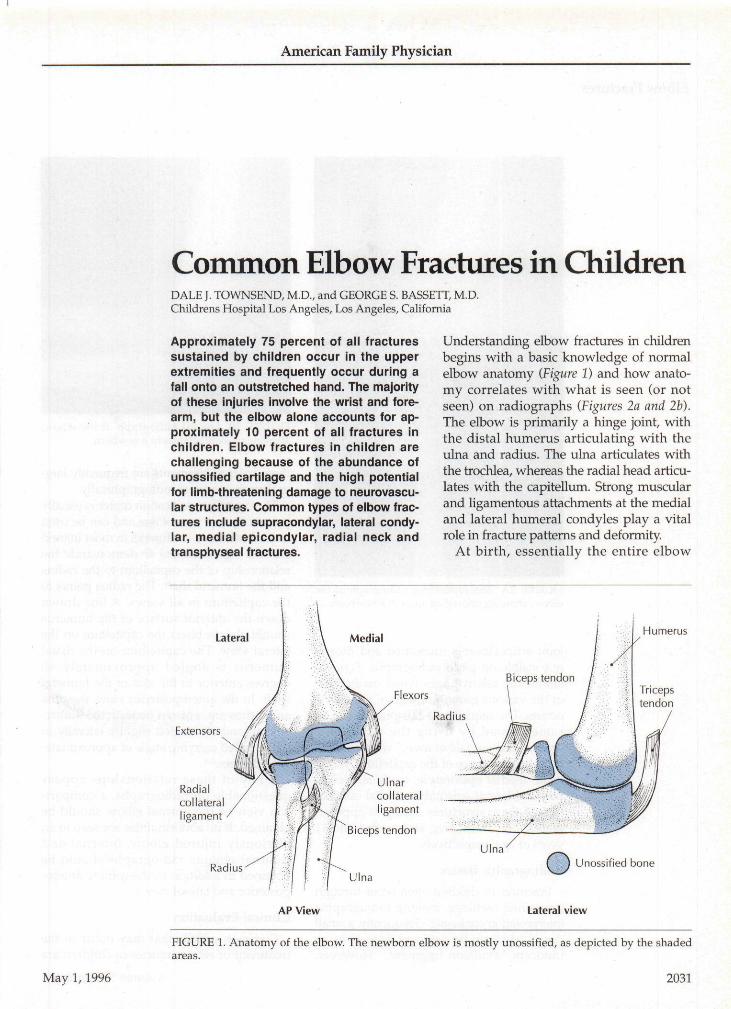
Understanding elbow fractures in childrenbegins with a basic knowledge of normalelbow anatomy (Figure 1) and how anato-my correlates with what is seen (or notseen) on radiographs {Figures 2a and 2b).The elbow is primarily a hinge joint, withthe distal humerus articulating with theulna and radius. The ulna articulates withthe trochlea, whereas the radial head articu-lates with the capitellum. Strong muscularand ligamentous attachments at the medialand lateral humeral condyles play a vitalrole in fracture patterns and deformity.
At birth, essentially the entire elbow
Lateral Medial
Extensors
Radialcollateralligament
Radius
Ulnarcollateralligament
Biceps tendon
Humerus
Flexors
AP View Lateral view
FIGURE 1. Anatomy of the elbow. The newborn elbow is mostly unossified, as depicted by the shadedareas.
May 1,1996 2031
American Family Physician
Elbow Fractures
; • • ' - ! i ' '. i ':'
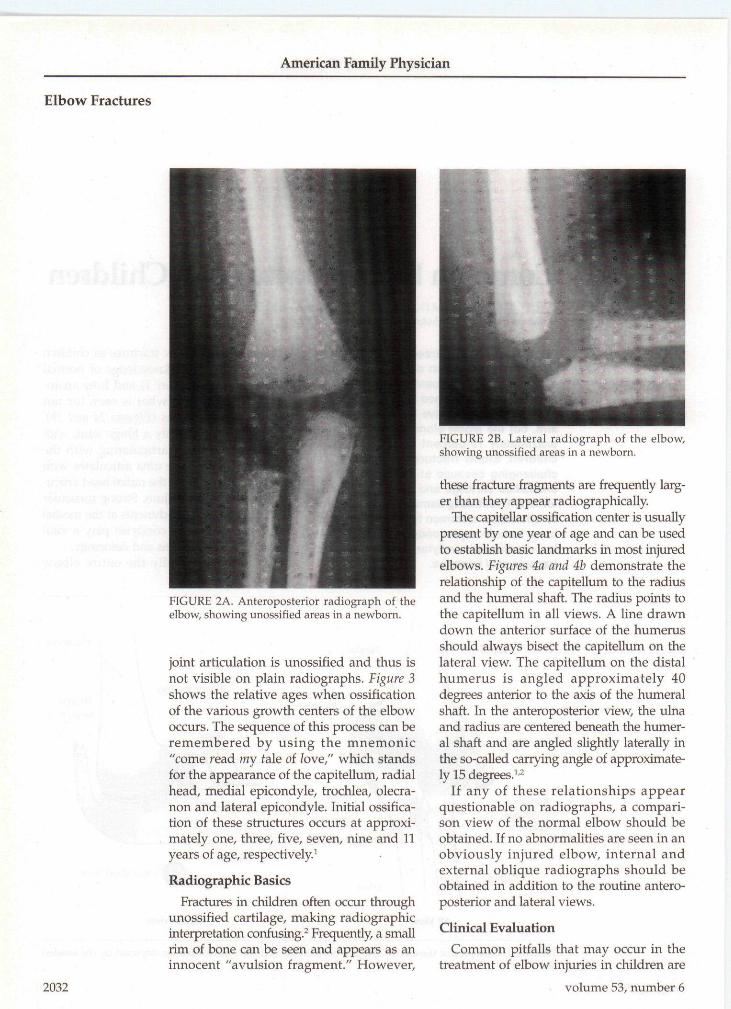
FIGURE 2A. Anteroposterior radiograph of theelbow, showing unossified areas in a newborn.
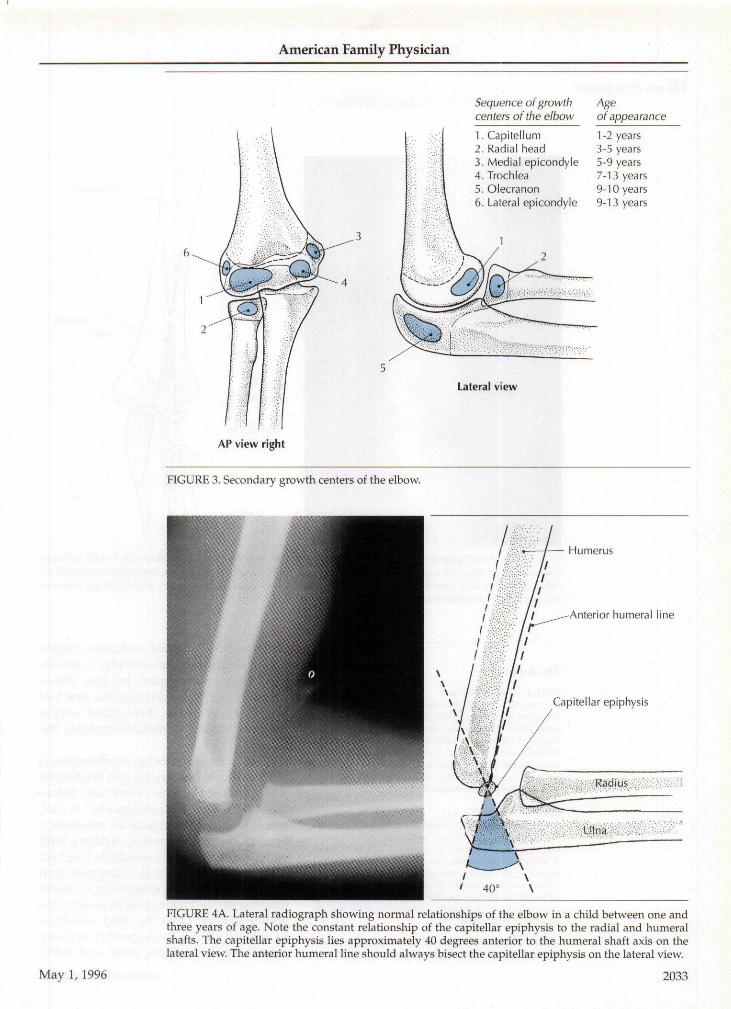
joint articulation is unossified and thus isnot visible on plain radiographs. Figure 3show s the relative ages when ossificationof the various growth centers of the elbowoccurs. The sequence of this process can beremembered by using the mnemonic"come read my fale of love," which standsfor the appearance of the capitellum, radialhead, medial epicondyle, trochlea, olecra-non and lateral epicondyle. Initial ossifica-tion of these structures occurs at approxi-mately one, three, five, seven, nine and 11years of age, respectively^
Radiographic BasicsFractures in children often occur through
unossified cartilage, making radiographicinterpretation confusing. Frequently, a smallrim of bone can be seen and appears as aninnocent "avulsion fragment." However,
2032
FIGURE 2B. Lateral radiograph of the eibow,showing unossified areas in a newborn.
these fracture fragments are frequently larg-er than they appear radiographically.
The capitellar ossification center is usuallypresent by one year of age and can be usedto establish basic landmarks in most injuredelbows. Figures 4a and 4b demonstrate therelationship of the capitelltim to the radiusand the humeral shaft. The radius points tothe capitellum in all views. A line drawndown the anterior surface of the humerusshould always bisect the capitellum on thelateral view. The capitellum on the distalhumerus is angled approximately 40degrees anterior to the axis of the humeralshaft. In the anteroposterior view, the ulnaand radius are centered beneath the humer-al shaft and are angled slightly laterally inthe so-called carrying angle of approximate-ly 15 degrees.''
If any of these relationships appearquestionable on radiographs, a compari-son view of the normal elbow should beobtained. If no abnormalities are seen in anobviously injured elbow, internal andexternal oblique radiographs should beobtained in addition to the routine antero-posterior and lateral views.
Clinical EvaluationCommon pitfalls that may occur in the
treatment of elbow injuries in children are
> volume 53, number 6
American Family Physician
Sequence of growthcenters ofthe elbow
1. Capitellutn2. Radial head3. Medial epicondyle4. Trochlea5. Olecranon
Ageof appearance
1 -2 years3-5 years5-9 years7-13 years9-10 years
6. Lateral epicondyie 9-13 years
Lateral view
AP view right
FIGURE 3. Secondary growth centers of the elbow.
May 1,1996
FIGURE 4A. Lateral radiograph showing normal relationships of the elbow in a child between one andthree years of age. Nofe the constant relationship of the capitellar epiphysis to the radial and humeralshafts. The capitellar epiphysis lies approximately 40 degrees anterior to fhe humeral shaft axis on thelateral view. The anterior humeral line should always bisect the capitellar epiphysis on the lateral view.
2033

American Family Physician
Elbow Fractures
Capitellarepiphysis
Radial shaftaxis line
Radius
Humerus
15° carryingangle
Ulna
FIGURE 4B, Anteroposterior radiograph showing normal relationships of the elbow in a child betweenone and three years of age. The radial shaft axis should always point to the capitellar epiphysis onanteroposterior and lateral radiographs. There is an approximately 15 degree carrying angle betweenthe humeral and radial shaft axis lines.
The Authors
DALE J, TOWNSEND, M,D,is currently a pediatric orthopedic surgeon at KaiserPermanente Hospital, Hayward, Calif. A graduate ofLoma Linda (Calif,) University School of Medicine, Dr.Townsend completed a residency in family practice at TheMedical Center, Columbus, Ga, He also completed a resi-dency in orthopedic surgery at the University of Hawaii,Honolulu, and a fellowship in pediatric orthopedics atChildrens Hospital Los Angeles in Los Angeles, Calif,
GEORGE S. BASSETT, M,D-is a pediatric orthopedic surgeon at Childrens HospitalLos Angeles and associate professor of orthopedicsurgery at the University of Southern California Schoolof Medicine, Los Angeles, Dr, Bassett earned a medicaldegree at the State University of New York HealthScience Center, Syracuse, He completed a residency inorthopedic surgery at the University of Iowa, Iowa City,and a fellowship in pediatric orthopedics at the duPontInstitute in Wilmington, Del.
Address correspondence to Dale j . Townsend, M.D., Kaiser-Hayward, 27400 Hes-perian Blvd., Hayward, CA 94545.
2034
listed in Table 1. Initial evaluation beginswith a thorough neurovascular examina-tion. This is paramount, because elbowfractures can often damage the brachialartery or any of the three major nerves(median, ulnar and radial) supplying thehand.
While a neurovascular examination isoften difficult in a crying and frightenedchild, it must be done—preferably beforethe child is sent for radiographs. A cool,pulseless extremity signals an emergency.Brachial and radial pulses, capillary refilland hand temperature should be checked.If the pulse is equivocal, a Doppler scanshould be done. An evaluation of nervefunction can be challenging in an uncoop-erative patient. Does the child withdrawto stimuli of the "autogenous sensoryzones" for the median, ulnar and radial
volume 53, number 6

American Family Physician
nerves (the tip of the index finger, the tipof the small finger and the dorsal thumbweb space, respectively)? This withdraw-al maneuver can usually be used to docu-ment the child's ability to flex and extendthe fingers and wrist. Can the child raisethe thumb or wrist (radial n:\otor nerve)?Will he or she flex the thumb or index fin-ger (median motor nerve)? The motor sta-tus of the ulnar nerve is the most difficultto assess in an uncooperative patient, butflexion of the tip of the fifth finger is usu-ally the easiest method. Medial and later-al movement of the index finger (Egawa'ssign), when obtainable, is the most sensi-tive indicator of ulnar nerve function. In acooperative patient, the fastest way toevaluate all three motor nerves is to havethe patient flex the fingers with the meta-carpophalangeal joints actively extendedand then appose the thumb to the littlefinger."*
As part of the physical examination,other associated injuries should beconsid-ered. The joints above and below the siteof obvious injury should also be exam-ined. During a fall, the entire extremity issubjected to the same load, and, especial-ly in the presence of supracondylar frac-tures, an associated wrist, forearm orshoulder fracture is not uncommon.^ Also,any signs of an open fracture should benoted. Any blood oozing from even a tiny.
TABLE 1
Common Errors in the Managementof Elbow Fractures in Children
Failure to perform a thorough neurovascular evaluation . ;Failure to identify an open fractureFailure to splint the injured extremity before transferring the patient
or sending the patient for radiographsFailure to identify an evolving compartment syndromeFailure to identify associated injuries in the same extremityAttempting to reduce a radial head dislocation ("nursemaid's elbow")
before obtaining radiographsConfusing a growth center with an avulsion fracture, or vice versa ..-, , •
May 1,1996
pinprick-sized hole in the skin constitutesan open fracture and often represents amuch larger opening than is apparent.Open fractures and/or neurovascular in-juries require urgent orthopedic surgicalintervention and should be approached astrue emergencies.
COMPARTMENT SYNDROME
Increasing pain in the forearm anddecreasing sensation in the hand are cardi-nal signs that a compartment syndrome isbeginning. Compartment syndrome withvascular compromise is more common insupracondylar fractures than in other typesof fractures, but it can occur in any elbow orforearm fracture. The pain of compartmentsyndrome is exacerbated by stretching themuscles that are becoming ischemic, usual-ly the volar forearm compartments.^ If pas-sive extension of the fingers causes severepain, a volar compartment syndrome islikely. Volkmann's ischemic contracture isthe preventable end result of untreatedforearni compartment syndrome and is notsalvageable once the muscles have becomenecrotic. The patient is left with a nearlyuseless hand.
SPLINTING THE ELBOW
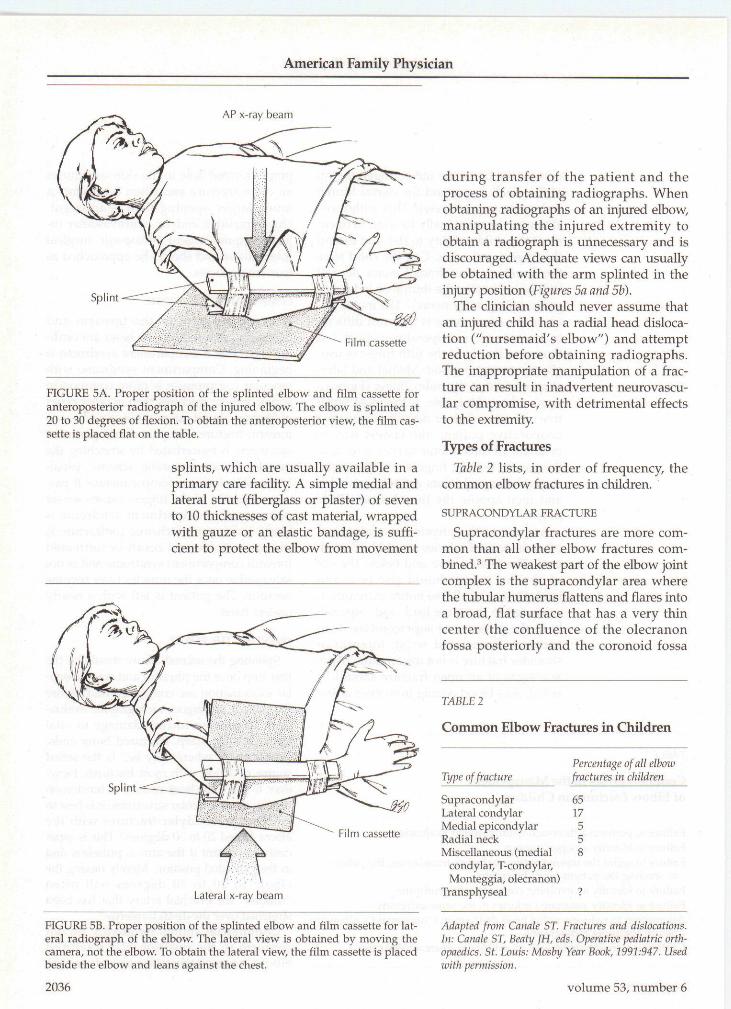
Splinting the injured elbow should be thefirst step once the physical and neurovascu-lar examination are completed and beforethe patient undergoes radiographic evalua-tion. To prevent further damage to vitalstructures by sharp, fractured bony ends,"splint them where they lie" is the safestcourse of action with most fractures. How-ever, to place the least amount of tension onnearby neurovascular structures, it is best tosplint supracondylar fractures with theelbow flexed 20 to 30 degrees. This is espe-cially important if the arm is pulseless andin the extended position. Merely flexing theelbow to 20 to 30 degrees will often"unkink" the brachial artery that has beenstretched over the distal humerus."
Commercial splints frequently do notconforn:\ to the position of a fracturedelbow, necessitating the use of casting
2035
American Family Physician
AP x-ray beam
Film cassette
FIGURE 5A. Proper position of the splinted elbow and film cassette foranteroposterior radiograph of the injured elbow. The elbow is splinted at20 to 30 degrees of flexion. To obtain the anteroposterior view, the film cas-sette is placed flat on the table. .. , . . . . • , . . . .
•••:•'•• ^ : splints, which are usually available in a' ' primary care facility. A simple medial and
lateral strut (fiberglass or plaster) of seven• • •••• • ' . •• t o 10 t h i c k n e s s e s of cas t m a t e r i a l , w r a p p e d
-•'• '••. •'•'•'-• •••'• w i t h g a u z e o r a n e las t ic b a n d a g e , is suffi-
• ' ''. - dent to protect the elbow from movement
Lateral x-ray beam
FICURE 5B. Proper position of the splinted elbow and film cassette for lat-eral radiograph of the elbow. The lateral view is obtained by moving thecamera, not the elbow. To obtain the lateral view, the film cassette is placedbeside the elbow and leans against the chest. "
during transfer of the patient and theprocess of obtaining radiographs. Whenobtaining radiographs of an injured elbow,manipulating the injured extremity toobtain a radiograph is unnecessary and isdiscouraged. Adequate views can usuallybe obtained with the arm splinted in theinjury position {Figures 5a and 5b).
The clinician should never assume thatan injured child has a radial head disloca-tion ("nursemaid's elbow") and attemptreduction before obtaining radiographs.The inappropriate manipulation of a frac-ture can result in inadvertent neurovascu-lar compromise, with detrimental effectsto the extremity.
Types of Fractures
Table 2 lists, in order of frequency, thecommon elbow fractures in children.
SUPRACONDYLAR FRACTURE
Supracondylar fractures are more com-mon than all other elbow fractures com-bined. The weakest part of the elbow jointcomplex is the supracondylar area wherethe tubular humerus flattens and flares intoa broad, flat surface that has a very thincenter (the confluence of the olecranonfossa posteriorly and the coronoid fossa
TABLE 2 ,
Common Elhow Fractures in Children
Type of fracture
SupracondylarLateral condylarMedial epicondylarRadial neckMiscellaneous (medial
condylar, T-condylar,Monteggia, olecranon)
T r a n s p h y s e a l •' •" • '; •' •
Percentage of all elbowfractures in children
6 5 •-•'•': - ••• • • ' ' • - - ' ' ^ : : ^ -
1755 • • •
8 •'• • • • •
Adapted from Canale ST. Fractures and dislocations.In: Canale ST, Beaty ]H, eds. Operative pediatric orth-opaedics. St. Louis: Mosby Year Book, 1991:947. Usedwith permission.
2036 volume 53, number 6

American Family Physician
anteriorly). Ghildren are uniquely suscepti-ble to fractures here because of the strong,but hypermobile, joint capsule and liga-ments, which allow the elbow to hyperex-tend.^ Thus, axial loading can force theelbow into a locked hyperextension pos-ture, which then fails as the joint furtherhyperextends, driving the olecranon intoits fossa and producing the extension-typesupracondylar fracture (Figure 6). The pres-ence of a posterior fat pad sign—evidenceof hemarthrosis—may be the only radio-graphic abnormality in nondisplaced su-pracondylar fractures.
The flexion type of fracture is uncom-mon, accounting for only 3 percent of allsupracondylar fractures, and is caused bya fall onto a flexed elbow.
The average age of children with supra-condylar fractures is five to eight years,and about twice as many boys as girls sus-tain this type of fracture. Seven percent ofchildren with this type of fracture have anassociated nerve injury, and up to 3 percenthave an open fracture.' Vascular compro-mise has been reported in up to 10 percentof cases,^ but with reduction and sta-bilization, less than 5 percent of all supra-condylar fractures require vascular surgeryintervention.^
Orthopedic intervention is recommend-ed for most supracondylar fractures. Anydisplacement of a supracondylar fracturerequires surgical intervention, which is
FIGURE 6. Lateral radiograph of a minimallydisplaced extension-type supracondylar elbowfracture. Note the posterior fat pad sign (arrow).This type of fracture is usually caused by a fallonto a locked, extended elbow.
usually accomplished by closed reductionand percutaneous pinning.'-^ Occasionally,open reduction and pinning are requiredfor displaced fractures or fractures w ithassociated neurovascular injuries. Nondis-placed fractures are casted for three to fourweeks.
Supracondylar fractures are usuallyproximal to the growing physis, so growtharrest is rare.* Deformities can occur, how-ever, and are usually a cubitus vanis angu-lation, with loss of the normal carryingangle (Figure 7). This deformity is almostalways secondary to malreduction or loss
FIGURE 7. Cubitus varus ("gunstock") deformity of the right elbow following malreduction of a supracondylar elbt)vv fracture.
May 1,1996 2037
American Family Physician
Elbow Fractures
of reduction, not growth arrest. Cubitusvarus deformity is mainly a cosmetic con-cern, but the "gunstock" appearance isunsightly enough that many parents oryoung adults seek surgical correction byhumeral osteotomy.
Nerve injury, most commonly of themedian or radial nerve, is usually a neura-praxia that resolves within a few weeks. -If recovery does not occur within threemonths, neurophysiologic evaluation and,possibly, surgery are indicated. If perma-nent nerve injury occurs, tendon transfersusually restore adequate function to thehand to minimize the deficiency.
LATERAL CONDYLAR FRACTURE
Lateral condylar fracture is the secondmost common elbow fracture, but it is themost common fracture of the elbow that in-volves the epiphysis and/or the joint sur-face. The wrist extensor muscles, the bra-chioradialis muscle and the lateral collateralligaments attach to the lateral condyle ofthe humerus. A fall onto an outstretchedhand can avulse the lateral humeral con-dyle by application of a varus force.
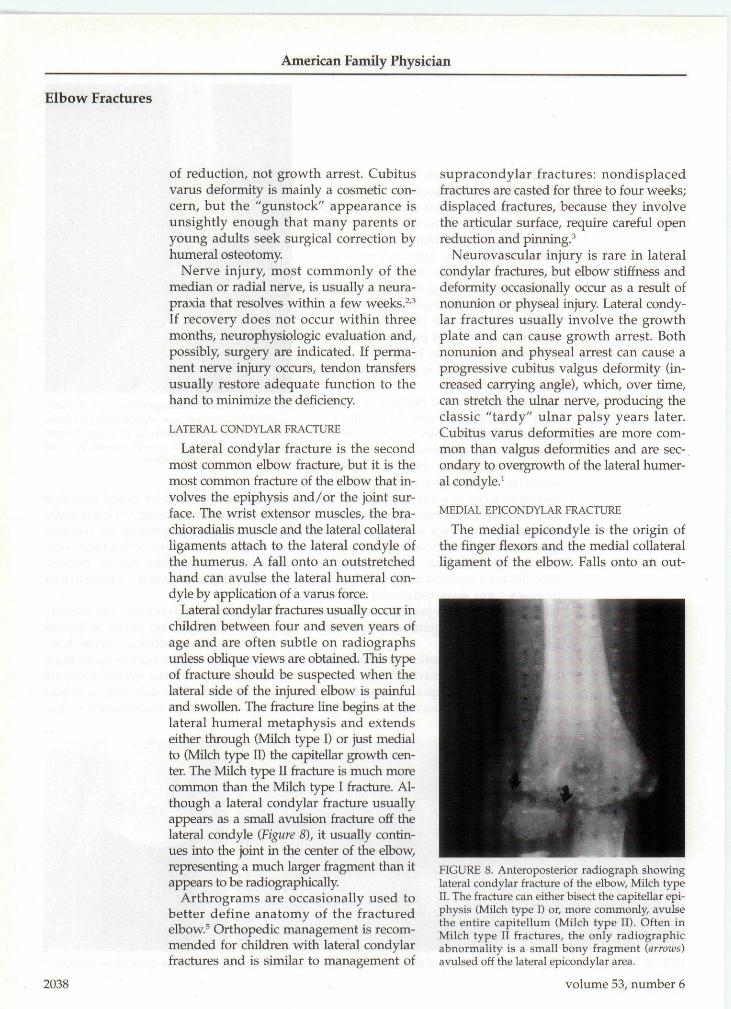
Lateral condylar fractures usually occur inchildren betw^een four and seven years ofage and are often subtle on radiographsunless oblique views are obtained. This typeof fracture should be suspected when thelateral side of the injured elbow is painfuland swollen. The fracture line begins at thelateral humeral metaphysis and extendseither through (Milch type I) or just medialto (Milch type 11) the capitellar growth cen-ter. The Milch type 11 fracture is much morecommon than the Milch type I fracture. Al-though a lateral condylar fracture usuallyappears as a small avulsion fracture off thelateral condyle (Figure 8), it usually contin-ues into the joint in the center of the elbow,representing a much larger fragment than itappears to be radiographically.
Arthrograms are occasionally used tobetter define anatomy of the fracturedelbow."' Orthopedic management is recom-mended for children with lateral condylarfractures and is similar to management of
supracondylar fractures: nondisplacedfractures are casted for three to four weeks;displaced fractures, because they involvethe articular surface, require careful openreduction and pinning.^
Neurovascular injury is rare in lateralcondylar fractures, but elbow stiffness anddeformity occasionally occur as a result ofnonunion or physeal injury. Lateral condy-lar fractures usually involve the growthplate and can cause growth arrest. Bothnonunion and physeal arrest can cause aprogressive cubitus valgus deformity (in-creased carrying angle), which, over time,can stretch the ulnar nerve, producing theclassic "tardy" ulnar palsy years later.Cubitus varus deformities are more com-mon than valgus deformities and are sec-ondary to overgrowth of the lateral humer-al condyle.^
MEDIAL EPICONDYLAR FRACTURE
The medial epicondyle is the origin ofthe finger flexors and the medial collateralligament of the elbow. Falls onto an out-
2038
FIGURE 8, Anteroposterior radiograph showinglateral condylar fracture of the elbow. Milch typeII. The fracture can either bisect the capitellar epi-physis (Milch type I) or, more commonly, avulsethe entire capitellum {Milch type II). Often inMilch type II fractures, the only radiographicabnormality is a small bony fragment (arrows)avulsed off the lateral epicondylar area.
volume 53, number 6
American Family Physician
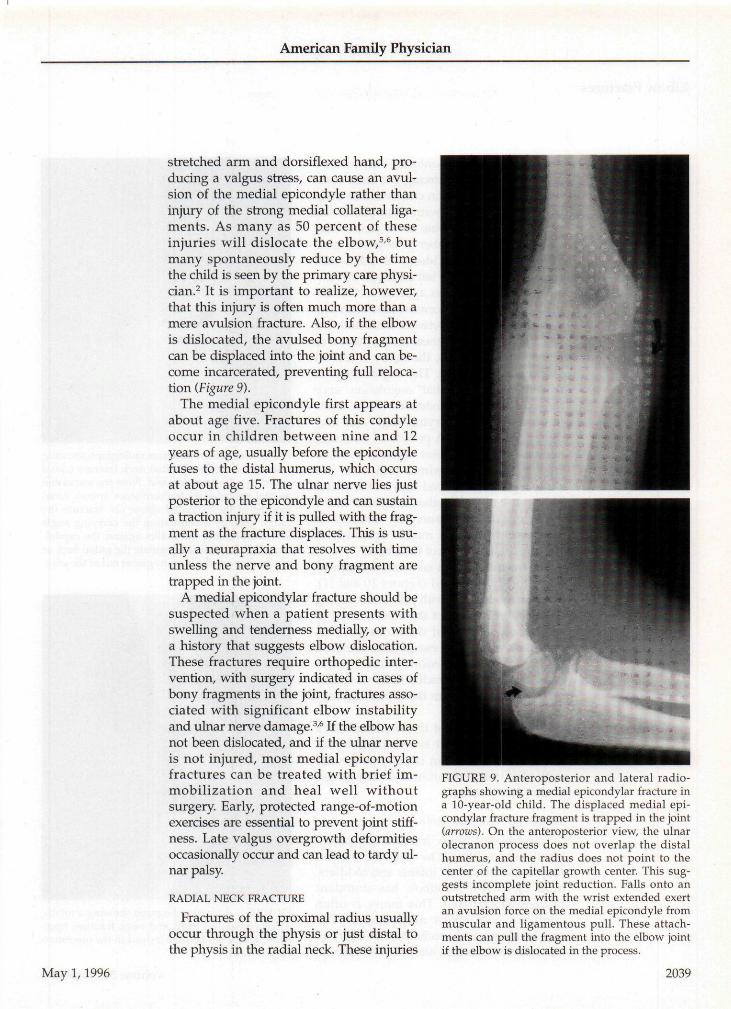
stretched arm and dorsiflexed hand, pro-ducing a valgus stress, can cause an avul-sion of the medial epicondyle rather thaninjury of the strong medial collateral liga-ments. As many as 50 percent of theseinjuries will dislocate the elbow,'''^ butmany spontaneously reduce by the timethe child is seen by the primary care physi-cian.^ It is important to realize, however,that this injury is often much more than amere avulsion fracture. Also, if the elbowis dislocated, the avulsed bony fragmentcan be displaced into the joint and can be-come incarcerated, preventing full reloca-tion (Figure 9).
The medial epicondyle first appears atabout age five. Fractures of this condyleoccur in children between nine and 12years of age, usually before the epicondylefuses to the distal humerus, which occursat about age 15. The ulnar nerve lies justposterior to the epicondyle and can sustaina traction injury if it is pulled with the frag-ment as the fracture displaces. This is usu-ally a neurapraxia that resolves with timeunless the nerve and bony fragment aretrapped in the joint.
A medial epicondyiar fracture should besuspected when a patient presents withswelling and tenderness medially, or witha history that suggests elbow dislocation.These fractures require orthopedic inter-vention, with surgery indicated in cases ofbony fragments in the joint, fractures asso-ciated with significant elbow instabilityand ulnar nerve damage. *' If the elbow hasnot been dislocated, and if the ulnar nerveis not injured, most medial epicondyiarfractures can be treated with brief im-mobilization and heal well withoutsurgery. Early, protected range-of-motionexercises are essential to prevent joint stiff-ness. Late valgus overgrowth deformitiesoccasionally occur and can lead to tardy ul-nar palsy.
RADIAL NECK FRACTURE
Fractures of the proximal radius usuallyoccur through the physis or just distal tothe physis in the radial neck. These injuries
May 1,1996
FIGURE 9. Anteroposterior and lateral radio-graphs showing a medial epicondyiar fracture ina lO-year-oId child. The displaced medial epi-condyiar fracture fragment is trapped in the joint(arrows). On the anteroposterior view, the ulnarolecranon process does not overlap the distalhumerus, and the radius does not point to thecenter of the capitellar growth center. This sug-gests incomplete joint reduction. Falls onto anoutstretched arm with the wrist extended exertan avulsion force on the medial epicondyle frommuscular and ligamentous pull. These attach-ments can pul] the fragment into the elbow jointif the elbow is dislocated in the process.
2039
American Family Physician
Elbow Fractures
are caused by a fall onto an outstretchedhand, but they are among the least com-mon elbow fractures in children. The aver-age age of children with fractures of theproximal radius is nine to 10 years, withalmost an equal number of boys and girlsaffected. Also, the incidence of radial neckfractures is similar for left and right arms.
The radial epiphysis appears as the sec-ond elbow growth center, just after thecapitellar epiphysis, between three and fiveyears of age. Because there are no muscle orligament attachments, the injury is causedby pure axial loading. The displacement isusually an "apex-medial" angulation, sincethe axial load on an extended elbow tendsto accentuate the carrying angle and pro-duce a valgus force. A portion of the radialneck is outside the joint capsule, so somefractures of the proximal radius do notcause a posterior fat pad sign on the lateralradiograph unless another associated elbowinjury occurs simultaneously (usually anolecranon fracture, a medial epicondylarfracture or dislocation of the elbow).
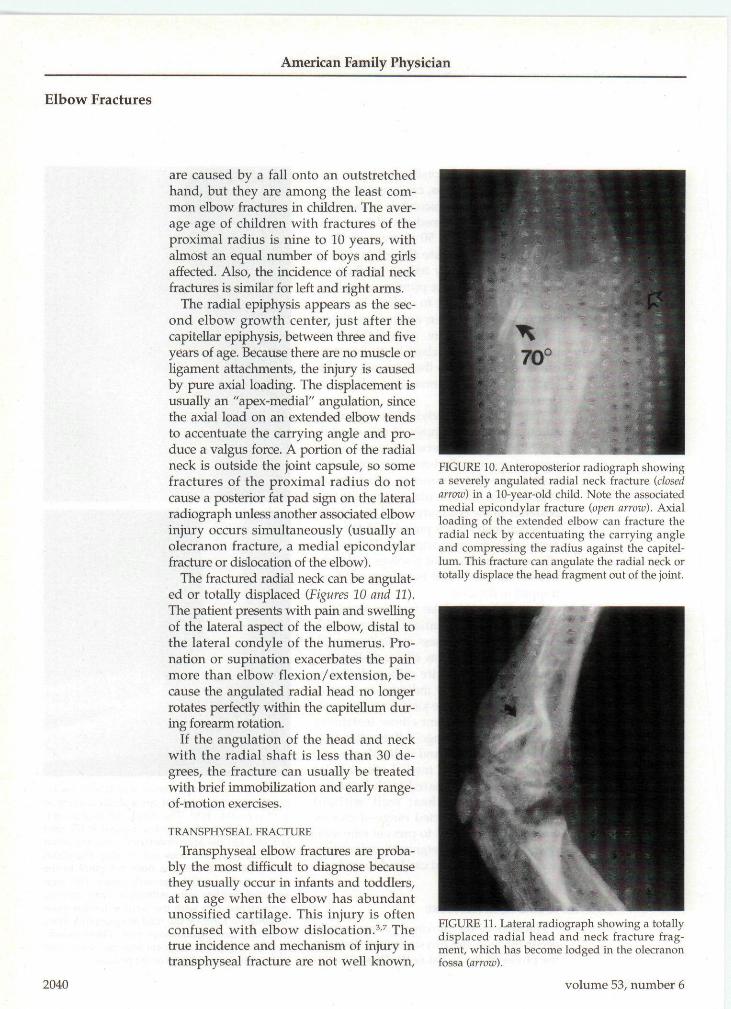
The fractured radial neck can be angulat-ed or totally displaced {Figures 10 and 11).The patient presents with pain and swellingof the lateral aspect of the elbow, distal tothe lateral condyle of the humerus. Pro-nation or supination exacerbates the painmore than elbow flexion/extension, be-cause the angulated radial head no longerrotates perfectly within the capitellum dur-ing forearm rotation.
If the angulation of the head and neckwith the radial shaft is less than 30 de-grees, the fracture can usually be treatedwith brief immobilization and early range-of-motion exercises.
TRANSPHYSEAL FRACTURE '
Transphyseal elbow fractures are proba-bly the most difficult to diagnose becausethey usually occur in infants and toddlers,at an age when the elbow has abundantunossified cartilage. This injury is oftenconfused w ith elbow dislocation.''-^ Thetrue incidence and mechanism of injury intransphyseal fracture are not well known.
FIGURE 10. Anteroposterior radiograph showinga severely angulated radial neck fracture (closedarrow) in a 10-year-old child. Note the associatedmedial epicondylar fracture (open arroxv). Axialloading of the extended elbow can fracture theradial neck by accentuating the carrying angleand compressing the radius against the capitel-lum. This fracture can angulate the radial neck ortotally displace the head fragment out of the joint.
2040
FIGURE 11. Lateral radiograph showring a totallydisplaced radial head and neck fracture frag-ment, which has become lodged in the olecranonfossa {arrow).
volume 53, number 6

American Family Physician
FIGURE 12A. Anteroposterior radiograph show-ing transphyseal fracture of the elbow. The frac-ture is displaced medially (arrow).
partly because this injury pattern is oftennot recognized. ' Like supracondylar frac-tures that occur in older children, manytransphyseal fractures probably occur as ahyperextension and/or rotation injury thatdisplaces the entire distal humeral physis.In an infant, the physis is more proximal,actually at the supracondylar area.^-*Transphyseal fracture should be suspectedin any child under one year of age whohas swelling of the elbow secondary tosuspected trauma. Because this injury oc-curs in very young children, the clinicianshould alw^ays be alert for suspected childabuse.'-''
Often the only anteroposterior radio-graphic abnormality is that the ulna andradius are not centered beneath the distalhumerus in comparison to the appearanceof the uninjured elbow. The displacementis usually posteromedial.^ The lateralradiograph shows posterior displacementand, unless the capitellar growth center isossified, the elbow appears to be dislocatedposteromedially (Figures 12a and 12b).However, three facts argue against elbow^dislocation: (1) elbow dislocations are rarein children under 10 years of age, (2) elbow^dislocations are usually posterolateral, notposteromedial, and (3) the relationship ofthe proximal radius and capitellar growthcenter is disrupted in a dislocated elbow. Inthe case of a transphyseal fracture, the
FIGURE 12B. Lateral radiograph showing trans-physeal fracture of the elbow. A small bony frag-ment shell of fhe distal humerus can be seen(open arrow). Nofe that the radius is aligned withthe capitellar growth center (solid arrow). If theelbow were dislocated, this relationship betweenthe radius and the capitellar growth centerwould not be seen.
proximal radius and capitellar growth cen-ter remain aligned with each other.'
Treatment of transphyseal elbow frac-tures in infants includes splinting and im-mediate referral to an orthopedist for re-duction and pinning. A skeletal survey torule out child abuse may also be indicated.
This manuscript was submitted for publication inconjunction with the Education Committee of thePediatric Orthopaedic Society of North America(POSNA).
REFERENCES
1. Wilkins KE. Fractures and dislocations of the elbowregion. In: Rockwood CA Jr, Wilkins KE, King RE,eds. Fractures in children. 3d ed. Philadelphia: Lip-pincott, 1991:509-828.
2. Tolo VT, Wood B, eds. Pediatric orthopaedics inprimary care. Baltimore: Williams & Wilkins, 1993;38-54.
3. Canaie ST. Fractures and dislocations. In: CanaleST, Beaty JH, eds. Operative pediatric orthopae-dics. St. Louis: Mosby Year Book, 1991-
4. Kasser JR. Percutaneous pinning of supracondylarfractures of the humerus. Instr Course Lect 1992;41:385-90.
5. Beaty JH. Fractures and dislocations about theelbow in children. Instr Course Lect 1992;41:373-84,
6. Wilkins KE, Morrey BF, Jobe FW, Kvitne RS,Coonrad RW, Figgie HE 3d, et al. The elbow. InstrCourse Lect 1991 ;40:1-87,
7. Moseley CE. Occult fractures. Instr Course Lect1992;41:361-7.
May 1,1996 2041
