displaced supracondylar fractures of elbow ... d’ambrosia 1972)butrequires aprolonged stay...
TRANSCRIPT

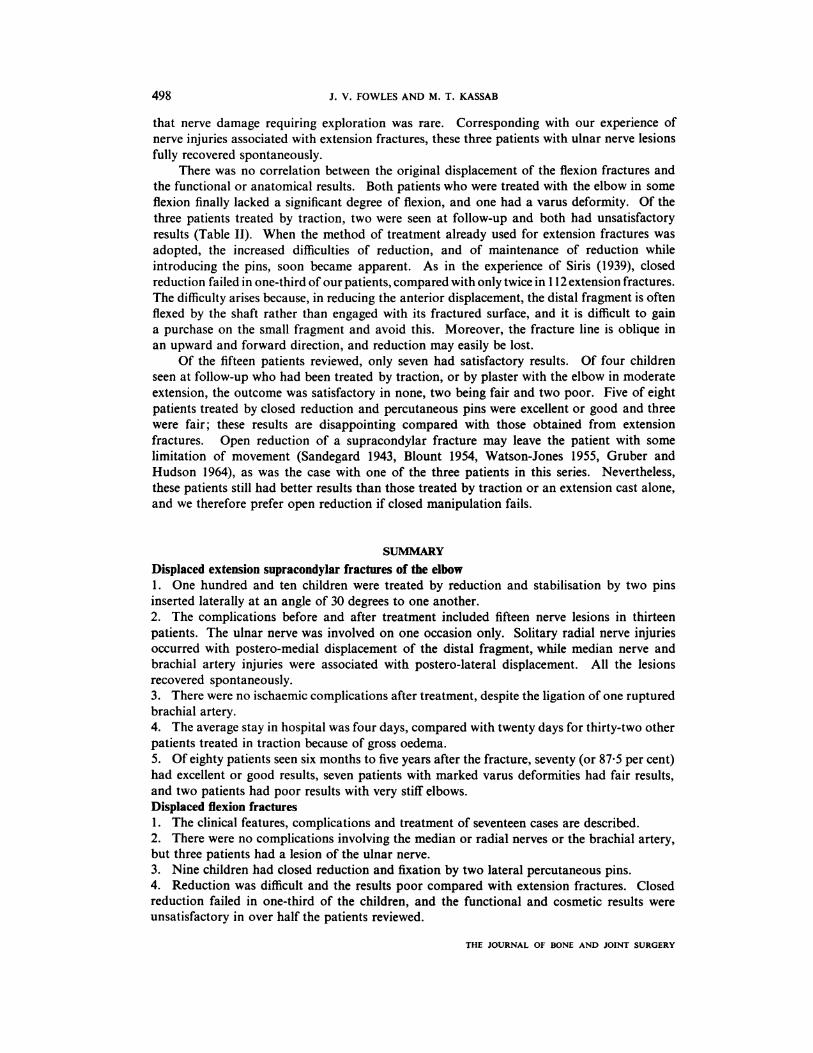
Antero-posterior and lateral radiographs of an elbow showing a Type 4 extension fracturewith complete posterior displacement of the distalfragment.
490 THE JOURNAL OF BONE AND JOINT SURGERY
DISPLACED SUPRACONDYLAR FRACTURES OF THE ELBOW
IN CHILDREN
A Report on the Fixation of Extension and Flexion Fractures
by Two Lateral Percutaneous Pins
J. V. FOWLES, MONTREAL, CANADA, and M. T. KASSAB, TuNis, TUNISIA
From the Centre for Orthopaedics, Kassar Said, Tunis
The orthopaedic service in Tunisia was opened in 1964 with 100 beds for a population
of some five million people. Referrals included patients with Volkmann’s ischaemic contracture
or with gangrene of the hand following supracondylar fracture of the humerus treated with
the elbow in acute fiexion. It was thus incumbent upon us to develop a reliable method of
treatment which would avoid these tragedies without blocking the limited bed space.
CLINICAL MATERIAL
Between 1966 and 1971, 175 children were admitted to the service with displaced
supracondylar fractures of the elbow across the olecranon fossa. Seventeen had fiexion
fractures and are the subject of the second part of this paper. One hundred and fifty-eight
children had extension fractures, the distal fragment being displaced posteriorly (Fig. 1).
Because of gross oedema, thirty-two patients were treated by skeletal traction using a Kirschner
wire through the olecranon, and were in hospital for an average of twenty days; two more
were treated in traction after failure of closed reduction, and fourteen had closed reduction
and fixation with one percutaneous Kirschner wire after the technique described by Jean Judet
in 1953. In order to improve the stability one of us (M. T. K.) modified this method by using
two pins, both inserted laterally so as to avoid the ulnar nerve. The remaining 110 children

DISPLACED SUPRACONDYLAR FRACTURES OF THE ELBOW IN CHILDREN 491
were treated by this method and are the subject of the first part of this paper. The technique
and its complications are described, and the results in eighty children, examined between six
months and five years later, are presented.
Clinical details-By the classification of Lagrange and Rigault (1962), all these I 10 fractures
were either Type 3, with rotation of the distal fragment and only one remaining point of
contact, or Type 4, with no contact whatsoever. The ages of the children varied from two to
fifteen years, the majority being between five and ten. There were eighty-nine boys and
twenty-one girls. The fracture was on the left side in sixty-three children and on the right in
forty-seven. Seventy-one patients were treated the same day; the remaining thirty-nine were
treated on average three days later, the longest delay being nine days.
TREATMENT
One hundred and four of the 1 10 patients were treated primarily by closed reduction.
Of the other six, four with grossly swollen elbows were treated first with skeletal traction for
several days to reduce the oedema and then had closed reduction, while two patients each
with a large open wound had open reduction. All the fractures were stabilised by two lateral
percutaneous pins (Fig. 2).
Technique-Under general anaesthesia, the patient’s arm was prepared and draped. Following
the technique described by Charnley (1961), with the elbow in extension and the forearm
supinated, the carrying angle was restored ; the elbow was then flexed and the reduction
confirmed radiographically. A fine Kirschner wire mounted in a chuck or electric drill was
driven into the distal humeral epiphysis immediately lateral to the olecranon, entering the
epiphysis at the junction of trochlea and capitellum. After crossing the fracture line the pin
was drilled 4 or 5 centimetres up the medullary canal of the diaphysis. A second wire was
introduced close to the first but at an angle of 30 degrees to it, and after crossing the fracture
line at a point well medial to the other pin, penetrated the medial cortex of the diaphysis.
Radiographs were taken (Fig. 2), and if the reduction and fixation were satisfactory, the pins
were bent outside the skin to prevent migration and then cut off, a sterile dressing was applied,
and a plaster back-slab made with the elbow at a right angle and the forearm in neutral
rotation. The following day the cast was completed, the reduction again confirmed by
radiographs, and the patient sent home. The average stay in hospital was four days. The
patient was seen at weekly intervals and three or four weeks later the cast and pins were
removed without anaesthetic.
COMPLICATIONS
Complications of the injury-On admission eight children had a faint or absent radial pulse;
seven had lateral displacement of the distal fragment. Another patient, aged four, had an
open supracondylar fracture with complete division of the brachial artery and displaced
fractures of both bones of the same forearm. At operation the artery was ligated, the fracture
reduced and pinned and the wound closed ; the forearm fractures were then reduced and held
with the cast. A stellate ganglion block was also done. The hand soon became warm and pink.
Six other patients had open fractures. One patient had open reduction through a large
wound; for the others the wounds were explored and closed and the fractures then reduced
and pinned in the usual manner.
Seven patients had nerve injuries. Three had a partial motor paralysis of the radial nerve
with normal sensibility, and another had sensory loss only. Three patients had a median
nerve injury-one complete paralysis, one motor weakness with complete anaesthesia, and
the third sensory loss only. The radial nerve injuries were associated with medial displacement
of the elbow, the median nerve lesions with lateral displacement. There were no ulnar nerve
lesions.
Six patients, including the girl with the ruptured brachial artery, had fractures of both
VOL. 56B, NO. 3, AUGUST 1974

FIG. 2Antero-posterior and lateral radiographs taken in the operating theatre immediately afterreduction and pinning of an extension fracture. The pins were later bent to avoid migration
and cut off outside the skin.
492 J. V. FOWLES AND M. T. KASSAB
THE JOURNAL OF BONE AND JOINT SURGERY
Antero-posterior and lateral radiographs of the same elbow as shown in Figure 2, takentwo years later. The distal humeral epiphysial plate appears normal, the olecranon andcoronoid fossae are well maintained, and the carrying angle and mobility of the elbow
are the same as on the other side.

DISPLACED SUPRACONDYLAR FRACTURES OF THE ELBOW IN CHILDREN 493
bones of the same forearm. These were reduced and held in plaster after fixation of the
supracondylar fracture.
Complications of the freatment-Of the patients with no nerve lesions before reduction, two
had complete radial nerve paralysis after closed reduction, and another a complete median
nerve paralysis ; a fourth had motor paralysis only of the median nerve and a fifth had sensory
loss only. The radial nerve lesions were associated with medial displacement of the distal
fragment, and the median nerve lesions with lateral displacement. Another patient, a girl
of thirteen with greenstick fractures of both bones of the same forearm, had complete paralysis
and anaesthesia of the hand after operation, but no signs of ischaemia. These post-reduction
palsies were no doubt due to the additional trauma of the manipulative procedures.
Infection of the elbow joint occurred in three patients, two of whom were treated
immediately by drainage and closed irrigation (Compere, Metzger and Mitra 1967). The
third had a low grade infection which was not apparent for three months ; he was then treated
with systemic antibiotics. Five other patients had pin track infections withoutjoint involvement.
None of these eight patients had an open fracture. Three children required a general
anaesthetic to remove the wires, which had not been bent and had migrated.
RESULTS
Eighty children were examined on average two years after the fracture, the shortest
follow-up being six months and the longest five years. Based on the classification of Lagrange
and Rigault (1962), the results were divided into the following categories. Excellent-a normal
arm and hand ; good-either a deficit of less than 20 degrees in the range of movement of
the elbow or a change in the carrying angle of less than 10 degrees (if both abnormalities
were present the patient was placed in the next category); fair-a deficit in the range of
movement of less than 50 degrees, or a change in the carrying angle of less than 20 degrees;
and poor-the range of movement decreased by more than 50 degrees, or a change in the
carrying angle of more than 20 degrees.
TABLE I
THE RESULTS IN EIGHTY CHILDREN WITH EXTENSION FRACrURES
TREATED BY CLOSED REDUCTION AND Two LATERAL PINS
Result � Type 3 � Type 4 � Totals
Excellent . � 6 � 26 32
Good . . 5 33 38
Fair . . 0 � 8 8
Poor . . 0 � 2 � 2
The results are shown in Table I. Thirty-two patients (40 per cent) had an excellent result
(Figs. 3 and 4). Thirty-eight patients (47�5 per cent) had a good result; twelve lost less than
10 degrees of movement; and three less than 20 degrees; the other twenty-three had a change
of less than 10 degrees of the carrying angle; two of these had an increase of 6 degrees, while
the rest had a decrease. Eight patients (10 per cent) had a fair result; seven had varus
deformities with good mobility of the elbow; one lost 7 degrees of the carrying angle and
15 degrees of movement. Two children (2�5 per cent) had poor results, with only a few degrees
of movement from the right angle. One patient had a low grade infection recognised late;
the other, the girl of thirteen mentioned earlier, had a total paralysis of the median, radial
and ulnar nerves after operation, and the pins were left in place for eight weeks.
VOL. 56 B, NO. 3, AUGUST 1974

FIG. 4
494 J. V. FOWLES AND M. T. KASSAB
THE JOURNAL OF BONE AND JOINT SURGERY
A patient aged 7, sixteen months after an extension fracture of the right elbow was reduced and pinned bythe method described. Movement of the elbow and the carrying angle are normal.
In general, 90 per cent of the full range of movement of the elbow was regained by a year.
Improvement however continued into the fourth year, when eighteen of the nineteen patients
examined had full movement and one lacked only 10 degrees of flexion.
All the open wounds healed by primary intention and the patients regained a full range
of movement. There were no permanent vascular sequelae. All the children with a diminished
or absent radial pulse on admission had good vascularity of the hand after reduction and all
ultimately had a normal pulse. The patient with a divided brachial artery, when last seen
three years later, had a normal arm and hand. All the patients with nerve lesions, whether
before or after reduction, had full spontaneous recovery over the ensuing weeks. Of the five
patients with pin track infections, four returned for follow-up ; only one had loss of movement
-I 5 degrees of extension. Of the two patients whose joint infections were treated promptly,
one had full movement at eight months and the other was lost to review.
DISCUSSION OF EXTENSION FRACTURES
For a satisfactory result a displaced supracondylar fracture should be reduced accurately
and stabilised (Mouchet 1898, Sandegard 1943, Judet 1953, Watson-Jones 1955, Gruber and
Hudson 1964). Attenborough (1953) has shown that acceptance of a poor position leads to
imperfect results ; all four of his patients treated without reduction had limited movement of
the elbow, and three also had a varus deformity. Of the common methods of treatment, a
cast with the elbow in acute flexion is the most dangerous because of the risk of ischaemia
and its irrevocable sequelae (MacLennan 1937, Blount 1950, Judet 1953, B#{246}hler1956, F#{232}vre
and Judet 1957, Maylahn and Fahey 1958). If the elbow is not flexed sufficiently, however,
the fracture is likely to redisplace (Swenson 1948, Judet 1953, Charnley 1961). Treatment by
traction may give good results (H#{248}yer1952, Maylahn and Fahey 1958, Mitchell and Adams
1961, D’Ambrosia 1972) but requires a prolonged stay in hospital, constant surveillance and
frequent radiographs, all of which are drawbacks in a socio-economic environment such as
that of Tunisia.
These disadvantages are largely eliminated when reduction is maintained by crossed
percutaneous pins. The usual technique is to place one pin laterally and the other medially,
with some risk of damaging the ulnar nerve (Swenson 1948; Jones 1967; Haddad, Saer and
Riordan 1970; Anderson 1971). The use of two lateral pins avoids the risk of ischaemia
from acute flexion of the elbow, does not endanger any major nerve or vessel, ensures stability
of the reduction and greatly reduces the time in hospital. The technique is relatively simple
and easy to learn; our patients were in fact treated by no less than twenty-one doctors of
varying backgrounds and levels of training. The pins penetrate the distal humeral epiphysis
between trochlear and capitellum, without damaging articular cartilage. Although the fine

DISPLACED SUPRACONDYLAR FRACTURES OF THE ELBOW IN CHILDREN 495
Kirschner wires cross the epiphysial growth plate, they do not interfere with its function
(Judet 1953 ; Campbell, Grisolia and Zanconato 1959). Thus of our eighty patients reviewed,
one developed a valgus deformity of 6 degrees over the first two years but none of the others
showed any growth disturbance (Fig. 3).
The radial and median nerves and the brachial artery are particularly vulnerable in
extension fractures, being at risk of stretch over the jagged edge of the shaft by the backward
and upward displacement ofthe distal fragment and elbow (Meyerding 1936, Hammond 1952,
Lipscomb and Burleson 1955, B#{246}hler 1956, Gartland 1959, Ottolenghi 1971). The brachial
artery and median nerve are injured mainly with radialdisplacement ofthe distal fragment; thus
Ottolenghi (1971) reported that thirty-five of thirty-nine arterial injuries occurred with radial
displacement. The radial nerve is injured mainly with medial displacement, because radial
displacement pulls the nerve away from the sharp edge of the diaphysial fracture. The ulnar
nerve is rarely injured by supracondylar fractures in extension (Hammond 1952, Lichtenberg
1954, Lagrange and Rigault 1962), being relaxed and carried backward away from the fracture
edge. The paper of Edman and L#{246}hr(1963) is unusual in reporting eleven ulnar nerve injuries
in a total of twenty-seven nerve lesions among 161 patients with supracondylar fractures, but
they did not differentiate between fractures in extension and in flexion. There was only one
ulnar nerve lesion in our series, the girl who had temporary paralysis of all three major nerves
at the elbow after the reduction.
With regard to infection, the elbow joint capsule is attached to the superior margins of
the olecranon and coronoid fossae (Ashhurst 1910, Smith 1954, Gray’s Anatomy 1958), and
a supracondylar fracture crossing these fossae is therefore intra-articular (Hammond 1952).
Hence the track of a pin crossing the fracture must communicate with the joint space. We
believe that the risk of a pin track infection extending into the joint is no greater with the
method we have described than with any other. The problem of infection lies in the
environment rather than in the technique.
The results compare favourably with those of other series (Sins 1939 ; Aitken, Smith and
Blackett 1943; Sandegard 1943; Holmberg 1945; Judet 1953; Lagrange and Rigault 1962;
Edman and L#{246}hr1963 ; El-Sharkawi and Fattah 1965). Seventy patients, or 875 per cent of
those followed for more than six months, had satisfactory results. Lagrange and Rigault found
that mobility of the elbow improved for two years after the fracture, but some of our patients
continued to regain movement into the fourth year. Those followed for a shorter period
should therefore continue to improve.
FRACTURES IN FLEXION
Clinical material-There were thirteen boys and four girls, aged from three to fourteen years.
The fracture was on the left side in eleven. Based on the classification of Lagrange and Rigault
(1962), three patients had Type 2 fractures with only a forward tilt of the distal fragment;
three had a Type 3 fracture, the distal fragment being rotated as well as tilted forward, with
only one point of contact; and eleven patients had a Type 4 fracture, with complete forward
displacement and no contact (Fig. 5).
Complications of the injury-Two patients had hypoaesthesia in the ulnar nerve territory;
another had weakness of the interossei as well. All three lesions were associated with radial
displacement of the distal fragment. There were no other nerve injuries, and no patient with
symptoms or signs of vascular insufficiency.
TREATMENT
Two patients early in the series were treated by closed reduction and immobilisation for
three weeks with the elbow flexed 30 degrees. Three others were treated by overhead skeletal
traction using a Kirschner wire through the olecranon, two after failure of closed reduction,
VOL. 56B, NO. 3, AUGUST 1974

RESULTS
Fifteen patients were seen on average two
and a half years after the fracture, the shortest
follow-up being seven months and the longest
in Table II, were based on the classification of
496 J. V. FOWLES AND M. T. KASSAB
THE JOURNAL OF BONE AND JOINT SURGERY
the third because of gross oedema. Nine children had closed reduction and immobilisation
by two lateral percutaneous pins ; three were treated on the day of injury, the other six one to
three days later. Reduction was performed by traction with the elbow in 45 degrees of flexion,
the lateral and anterior displacement being corrected by direct digital pressure on the distal
fragment. The elbow was then flexed a further 20 degrees by the assistant and two Kirschner
wires were introduced lateral to the olecranon, following the technique already described. A
plaster backslab was applied with the elbow at
90 degrees and the forearm in neutral rotation.
Next day the cast was completed, and if the
radiographs showed a satisfactory position the
patient was discharged and seen at weekly
intervals until the cast and pins were removed
at three or four weeks.
Three patients in whom closed reduction
was unsuccessful had open reduction by the
Campbell posterior approach described by Boyd(1971). In two of the three the medial corner of
the shaft had buttonholed the triceps postero-
medially and had to be released before the
fracture could be reduced; in each instance the
ulnar nerve was sharply angled over the jagged
edge of the shaft and required careful retraction.
Complications-The only complication was one
pin track infection.
FIG. 5
A lateral radiograph of a Type 4 flexion fracturewith the distal fragment displaced forwards and
upwards.
four and a half years. The results, shown
Lagrange and Rigault (1962).
DISCUSSION OF FLEXION FRACTURES
Though two types of supracondylar fracture have been recognised for many years
(Malgaigne 1859, Hamilton 1880), fractures in flexion have received little attention in the past.
Their incidence is reported to be 4 per cent or less of all supracondylar fractures (Mouchet
1898, Sins 1939, Blount 1954, Watson-Jones 1955, Salter 1959, Mitchell and Adams 1961,
Lagrange and Rigault 1962). The high frequency in this paper, 10 per cent, is matched only
by the 1 1 per cent of Sorrel and Sorrel-Dejerine (1938) and the 10 per cent noted by Coventry
and Henderson (1956). The majority of boys over girls and of the left side over the right,
however, is similar to that reported in other series (Holmberg 1945, Lipscomb and Burleson
1955, Maylahn and Fahey 1958, Lagrange and Rigault 1962, Edman and L#{246}hr1963).
Among the 110 patients with extension fractures reported earlier, nineteen (18 per cent)
had complications involving the brachial artery, the radial nerve or the median nerve. In
marked contrast, no patient with a flexion fracture had any such complication. However, three
patients with flexion fractures (17 per cent) had some deficit of the ulnar nerve, compared
with only one patient with an extension fracture (1 per cent). When the distal fragment is
displaced anteriorly, the ulnar nerve is carried with it and may be sharply angled and stretched
over the fracture margin of the shaft as this juts posteriorly. This is even more likely if the
distal fragment is also displaced radially, as then the ulnar nerve is pulled laterally across

Closed reductionand pins
26 5-140 Lost 4 Fair(0-155)
0-145(0-145) No change Excellent
VOL. 56B, NO. 3, AUGUST 1974
DISPLACED SUPRACONDYLAR FRACTURES OF THE ELBOW IN CHILDREN 497
TABLE II
DETAILS OF SEVENTEEN CHILDREN WITH DISPLACED SUPRACONDYLAR FLExI0N FRACTURES OF THE ELBOW
Range of Change inLength of� movement
Sex Age Type of Complications Treatment follow-up J(normal side c�’j� Result‘(years) fracture� (months) in brackets) angle
(degrees)(degrees)
0-95Lost 12 PoorFemale 8 4 Cast in extension �
0-120Male 9 4 Cast in extension � Lost 2 Fair
Male 4 4 Failed manipulation,�traction
24 0-135(0-145)
10-110(0-145)
Lost 4
Varus 15
Fair
PoorMale 11 3 Ulnar nervehypoaesthesia
Failed manipulation,’traction ‘
Male 3 4 Traction�
Did notreturn
Female 8 4
‘
Closed reduction ,
and pins01400-14o
���
No change Excellent
Male 6 4 Closed reductionand pins
�
Did notreturn
Male 13 � 2
Closed reduction‘ 10 0-145 Nochange ExcellentFemale 7 , 3 � and pins � (0-145)
Closed reduction26 � 0-160 Lost 2 GoodMale 12 � 2‘ and pins � (0-160)
Closed reduction41 � 0-150 No change ExcellentFemale 6 4 and pins � (0-150)
Male 12 4 Pin track Closed reduction , 22 � 5-125 No change Fairinfection and pins � ‘ (0-145)
Closed reduction ‘ 0-15543Male 6 3 and pins , � (0-160) Lost 10 Fair
� , Ulnar nerve � Closed reduction � 0-145Lost 3 GoodMale 12 � hypoaesthesia ‘ and pins � (0-140)
Male � 14 � 4 � Openreduction 18 � 25135 Fair(0-145)
Ulnar nerve
Male 14 4 hypoaesthesia � Open reductionand weaknessof interossei
0-140Male 12 4 Open reduction 48 (0-140) Lost 4 Good� I
the shaft and cannot escape it. The vessels and nerves in front of the elbow, on the other hand,
are carried forward and upward away from the shaft and are therefore less vulnerable. This
reaffirms previous observations (Sorrel and Sorrel-Dejerine 1938, Hammond 1952, Smith 1954,
Lipscomb and Burleson 1955, B#{246}hler1956).
Sorrel and Sorrel-Dejerine recommended surgical exploration and release of an injured
ulnar nerve if there were no signs of recovery by ten or fifteen days. Hammond stated that
six weeks was the optimum period to wait before exploring the nerve. Seddon (1947) believed
498 i. V. FOWLES AND M. T. KASSAB
that nerve damage requiring exploration was rare. Corresponding with our experience of
nerve injuries associated with extension fractures, these three patients with ulnar nerve lesions
fully recovered spontaneously.
There was no correlation between the original displacement of the flexion fractures and
the functional or anatomical results. Both patients who were treated with the elbow in some
flexion finally lacked a significant degree of flexion, and one had a varus deformity. Of the
three patients treated by traction, two were seen at follow-up and both had unsatisfactory
results (Table II). When the method of treatment already used for extension fractures was
adopted, the increased difficulties of reduction, and of maintenance of reduction while
introducing the pins, soon became apparent. As in the experience of Sins (1939), closed
reduction failed in one-third of our patients, compared with only twice in 1 12 extension fractures.
The difficulty arises because, in reducing the anterior displacement, the distal fragment is often
flexed by the shaft rather than engaged with its fractured surface, and it is difficult to gain
a purchase on the small fragment and avoid this. Moreover, the fracture line is oblique in
an upward and forward direction, and reduction may easily be lost.
Of the fifteen patients reviewed, only seven had satisfactory results. Of four children
seen at follow-up who had been treated by traction, or by plaster with the elbow in moderate
extension, the outcome was satisfactory in none, two being fair and two poor. Five of eight
patients treated by closed reduction and percutaneous pins were excellent or good and three
were fair ; these results are disappointing compared with those obtained from extension
fractures. Open reduction of a supracondylar fracture may leave the patient with some
limitation of movement (Sandegard 1943, Blount 1954, Watson-Jones 1955, Gruber and
Hudson 1964), as was the case with one of the three patients in this series. Nevertheless,
these patients still had better results than those treated by traction or an extension cast alone,
and we therefore prefer open reduction if closed manipulation fails.
SUMMARY
Displaced extension supracondylar fractures of the elbow1 . One hundred and ten children were treated by reduction and stabilisation by two pins
inserted laterally at an angle of 30 degrees to one another.
2. The complications before and after treatment included fifteen nerve lesions in thirteen
patients. The ulnar nerve was involved on one occasion only. Solitary radial nerve injuries
occurred with postero-medial displacement of the distal fragment, while median nerve and
brachial artery injuries were associated with postero-lateral displacement. All the lesions
recovered spontaneously.
3. There were no ischaemic complications after treatment, despite the ligation of one ruptured
brachial artery.
4. The average stay in hospital was four days, compared with twenty days for thirty-two other
patients treated in traction because of gross oedema.
5. Of eighty patients seen six months to five years after the fracture, seventy (or 875 per cent)
had excellent or good results, seven patients with marked varus deformities had fair results,
and two patients had poor results with very stiff elbows.
Displaced flexion fractures1. The clinical features, complications and treatment of seventeen cases are described.
2. There were no complications involving the median or radial nerves or the brachial artery,
but three patients had a lesion of the ulnar nerve.
3. Nine children had closed reduction and fixation by two lateral percutaneous pins.
4. Reduction was difficult and the results poor compared with extension fractures. Closed
reduction failed in one-third of the children, and the functional and cosmetic results were
unsatisfactory in over half the patients reviewed.
THE JOURNAL OF BONE AND JOINT SURGERY

DISPLACED SUPRACONDYLAR FRACTURES OF THE ELBOW IN CHILDREN 499
REFERENCES
AITKEN, A. P., SMITh, L., and BLACKETr, C. W. (1943): Supracondylar fractures in children. American Journal
ofSurgery, 59, 161-171.
ANDERSON, L. D. (1971): In Campbell’s Operative Orthopaedics. Fifth edition, Volume I, p. 653. Edited byA. H. Crenshaw. St Louis : C. V. Mosby Co.
ASHHURST, A. P. C. (1910) : An Anatomical and Surgical Study of Fractures of the Lower End of the Humerus,
p. 23. Philadelphia and New York : Lea and Febiger.
ATTENBOROUGH, C. G. (1953): Remodelling of the humerus after supracondylar fractures in childhood. Journal
ofBone andJoint Surgery, 35-B, 386-395.
BLOUNT, W. P. (1950): Volkmann’s ischemic contracture (editorial). Surgery, Gynecology and Obstetrics,
90, 244-246.
BLOUNT, W. P. (1954): Fractures in Children, p. 26. Baltimore: The Williams and Wilkins Co.
B#{246}HLER, L. (1956): The Treatment of Fractures. Fifth English edition, Volume I, p. 639. New York : Gruneand Stratton.
BOYD, H. B. (1971): In Campbell’s Operative Orthopaedics. Fifth edition, Volume I, p. 119. Edited by A. H.Crenshaw. St Louis : C. V. Mosby Co.
CAMPBELL, C. J., GRISOLIA, A., and ZANCONATO, G. (1959): The effects produced in the cartilaginous epiphysealplate of immature dogs by experimental surgical traumata. Journal of Bone and Joint Surgery, 41-A,1221-1242.
CHARNLEY, J. (1961): The Closed Treatment of Common Fractures. Third edition, p. 113. Edinburgh : E. & S.
Livingstone Ltd.
COMPERE, E. L., METZGER, W. I., and Mrra�, R. N. (1967): The treatment ofpyogenic bone andjoint infectionsby closed irrigation (circulation) with a non-toxic detergent and one or more antibiotics. Journal of Boneand Joint Surgery, 49-A, 614-624.
COVENTRY, M. B., and HENDERSON, C. C. (1956) : Supracondylar fractures of the humerus-49 cases in children.
Rocky Mountain MedicalJournal, 53, 458-465.D’AMBRosIA, R. D. (1972): Supracondylar fractures of humerus-Prevention of cubitus varus. Journal of
Bone andJoint Surgery, 54-A, 60-66.
EDMAN, P., and LOHR, G. (1963): Supracondylar fractures of the humerus treated with olecranon traction.Acta chirurgica Scandinavica, 126, 505-516.
EL-SHARKAWI, A. H., and FArr&ii, H. A. (1965): Treatment ofdisplaced supracondylar fractures ofthe humerus
in children in full extension and supination. Journal ofBone andJoint Surgery, 47-B, 273-279.Fi�vxt�, M., and JUDET, J. (1957): Traitement des s#{233}quellesde Ia maladie de Volkmann. Revue de (‘hirurgie
Orthop#{233}dique et R#{233}paratrice de l’Appareil Moteur, 43, 437-450.GARTLAND, J. J. (1959): Management ofsupracondylarfractures ofthe humerus in children. Surgery, Gynecology
and Obstetrics, 109, 145-154.GRAY’S ANATOMY (1958): Thirty-second edition, p. 371. Edited by T. B. Johnston, D. V. Davies and F. Davies.
London : Longmans, Green and Co.GRUBER, M. A., and HursoN, 0. C. (1964): Supracondylar fractures of the humerus in childhood. Journal
ofBone andJoint Surgery, 46-A, 1245-1252.HADDAD, R. J., Jun., SAER, J. K., and Rtoamu.�, D. C. (1970): Percutaneous pinning ofdisplaced supracondylar
fractures of the elbow in children. Clinical Orthopaedics and Related Research, 71, 112-117.
HAMILTON, F. H. (1880): A Practical Treatise on Fractures and Dislocations. Sixth American edition, p. 271.
Philadelphia: Henry C. Lea’s Son & Co.
HAMMOND, G. (1952) : The management of supracondylar fractures of the humerus in children. Surgical
Clinics ofNorth America, 32, 747-762.HOLMBERG, L. (1945) : Fractures in the distal end of the humerus in children. Acta chfrurgica Scandinavica,
92, Supplementum 103.
HOYER, A. (1952) : Treatment of supracondylar fracture of the humerus by skeletal traction in an abductionsplint. Journal ofBone andJoint Surgery, 34-A, 623-637.
JONES, K. G. (1967) : Percutaneous pin fixation offractures of the lower end of the humerus. Clinical Orthopaedicsand Related Research, 50, 53-69.
JUDET, J. (1953) : Traitement des fractures sus-condyliennes transversales de l’hum#{233}ruschez l’enfant. Revuede Chfrurgie Orthop#{233}dique et R#{233}paratrice de l’Appareil Moteur, 39, 199-212.
LAGRANGE, J., and RIGAULT, P. (1962): Fractures supra-condyliennes. Revue de Chirurgie Orthop#{233}dique etR#{233}paratrice de l’Appareil Moteur, 48, 337-446.
LICHTENBERG, R. P. (1954): A study of 2,532 fractures in children. American Journal ofSurgery, 87, 330-338.
LIPSCOMB, P. R., and BURLESON, R. J. (1955): Vascular and neural complications in supracondylar fracturesof the humerus in children. Journal of Bone and Joint Surgery, 37-A, 487-492.
MACLENNAN, A. (1937): Common fractures about the elbow joint in children. Surgery, Gynecology and
Obstetrics, 64, 447-453.
VOL. 56 B, NO. 3, AUGUST 1974

500 J. V. FOWLES AND M. T. KASSAB
MALGAIGNE, J. F. (1859): A Treatise on Fractures, p. 437. Translated by J. H. Packard. Philadelphia: J. B.
Lippincott & Co.MAYLAHN, D. J., and FAHEY, J. J. (1958) : Fractures of the elbow in children. Review of 300 consecutive cases.
Journal ofthe American Medical Association, 166, 220-228.
MEYERDING, H. W. (1936) : Volkmann’s ischemic contracture associated with supracondylar fracture of humerus.Journal ofihe American Medical Association, 106, 1139-1144.
MITCHELL, W. J., and ADAiviS, J. P. (1961) : Supracondylar fractures ofthe humerus in children. A 10-year review.
Journal ofthe American Medical Association, 175, 573-577.MOUCHET, A. (1 898) : Fractures de l’extr#{233}mit#{233}inferieure de l’hum#{233}rus, avec radiographies, p. 120. Paris : G.
Stenheil.OTrOLENGHI, C. E. (1971) : Prophylaxie du syndrome de Volkmann dans les fractures supra-condyliennes du
coude chez l’enfant. Revue de Chirurgie Orthop#{233}dique et R#{233}paratrice de l’Appareil Moteur, 57, 517-525.
SALTER, R. B. (1959): Supracondylar fractures in childhood. Journal ofBone andJoint Surgery, 41-B, 881.SANDEGARD, E. (1943): Fracture of the lower end of the humerus in childhood: treatment and end results.
Acta chirurgica Scandinavica, 89, 1-16.
SEDDON, H. J. (1947) : Nerve lesions complicating certain closed bone injuries. Journal ofthe American Medical
Association, 135, 691-694.
SIRIS, I. E. (1939): Supracondylar fracture of the humerus. An analysis of 330 cases. Surgery, Gynecology and
Obstetrics, 68, 201-222.SMITH, F. M. (1954): Surgery of the Elbow, pp. 20 and 96. Springfield, Illinois:Charles C. Thomas.
SORREL, E., and SORREL-DEJERINE (1938): Les lesions du nerf cubital dans les fractures ferm#{233}essus-condyliennesr#{233}centesde l’hum#{233}rus. M#{233}moires de l’Acad#{233}mie de Chfrurgie, 64, 461-469.
SWENSON, A. L. (1948): The treatment of supracondylar fractures of the humerus by Kirschner-wire transfixion.
Journal of Bone and Joint Surgery, 30-A, 993-997.WATSON-JONES, R. (1955): Fractures and Joint Injuries. Fourth edition, Volume 2, pp. 525 and 532. Edinburgh
and London: E. & S. Livingstone Ltd.
THE JOURNAL OF BONE AND JOINT SURGERY