commissioning with frailty - clinical senateemsenate.nhs.uk/downloads/documents/clinical...
TRANSCRIPT

East Midlands Clinical Senate Advisory ReportCommissioning services for an ageing population and those living with frailty

Report byDr Ben PearsonConsultant Physician
East Midlands Clinical Senate Council member
Suzanne HorobinEast Midlands Strategic Clinical Networks and Senate
3East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
1. Executive summary � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 4
2. Introduction and purpose of the report � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 6
2.1. East Midlands Clinical Senate � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 6
2.2. Supporting commissioning � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 6
2.3. Understanding the demographics � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 7
3. What is frailty? � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 9
4. Demographic imperative for change � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 11
4.1. Variation in outcomes � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 12
4.2. Falls and hip fractures - forward projection � � � � � � � � � � � � � � � � � � � � � � � � � � � 13
5. What does the literature tell us and what are we doing about it?
� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 16
5.1. Access all ages - Royal College of Surgeons of England � � � � � � � � � � � � � � � 16
5.2. Cochrane Review of Physical Activity in Older People � � � � � � � � � � � � � � � � � 18
5.3. National Audit of Intermediate Care � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 18
5.4. Making our health and care systems fit for an ageing population � � � � � 20
5.5. Previously published commissioning guidance � � � � � � � � � � � � � � � � � � � � � � � � 23
5.6. Workforce development � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 26
5.7. East Midlands Academic Health Science Network response � � � � � � � � � � � 28
6. Comprehensive Geriatric Assessment � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 29
7. Principles and standards underpinning good practice � � � � � � � � � � � � � � 33
8. Referenced evidence base � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 34
8.1. Literature review � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 34
8.2. Collation and summary of existing professional and national guidelines
� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 35
9. Acknowledgements � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 36
Content

4East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
1. Executive summary
Commissioning services for an ageing population and those
living with frailty needs to change� The emerging evidence
around frailty, the existing evidence for comprehensive
geriatric assessment and the absolute need to provide
holistic person centered care for everyone, particularly older
people, mandates that change�
There is a demographic imperative to change the way we
commission services� As an example: older people living
with frailty are at increased risk of falls and hip fracture�
Across the East Midlands in 2012 - 13 there were 4805 falls
with hip fracture in people aged over 65 (HES data)� There
was significant variation in spend by CCG in relation to hip
fractures over the same period from under £500,000 to
£3,500,000� The population aged over 65 living across the
East Midlands is going to increase by 43% by 2030�
If we continue to commission for illness-based condition-
specific pathways we will continue to frustrate and fragment
the experience of healthcare for our most vulnerable
population� Patients with dementia are particularly at risk if
we fail to balance the complexities of co-morbidities or to
understand our patient’s views�
“The NHS must change to meet the needs of a population that lives longer, for the
millions of people with long-term conditions, and for all patients who want person
centred care. It means breaking down the boundaries between family doctors and
hospitals, between physical and mental health and between health and social care.”
- Simon Stevens
5East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
1. Executive summary
We reference the extensive evidence base and summarise
recent national publications with valuable guidance on
delivering services for older people and those living with
frailty� Comprehensive geriatric assessment is described
along with evidence for benefits realisation� Important
principles and standards underpinning good practice are
stated�
We have included a number of examples of good practice
in the form of case studies from around the region
demonstrating the application of best practice� Models
include the use of comprehensive geriatric assessment,
service redesign and innovative approaches to workforce
and training�
The report concludes with important messages from the
recent literature� Our aim has been to bring together our
regional expertise in good clinical practice to endorse a
commissioning strategy for our ageing population and those
living with frailty�
Commissioners who understand frailty and who ensure their
services are “Fit for Frailty” will achieve better outcomes
for their older population, for those with dementia and for
those who live with frailty�
6East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
2. Introduction and purpose of the report
2.1. East Midlands Clinical Senate
The East Midlands Clinical Senate is the clinical conscience
and guiding intelligence for strategic service change in the
new NHS� Combining expert clinical leaders with patient
involvement, the Clinical Senate provides proactive and
reactive advice across the health care system for the benefit
of improved patient outcomes and population health�
The Clinical Senate supports healthcare commissioners
across the East Midlands to make improvements in the
quality, safety and experience of patient care by providing
clinically lead, expert, strategic advice in areas of major
healthcare challenge�
The Senate Council made an early decision to produce two
proactive reports; one covering physical activity and exercise
medicine and this report, on commissioning services for an
ageing population and those living with frailty�
2.2. Supporting commissioning
We intend this report to be a useful, practical resource
for commissioners� And while we recognise that different
detailed solutions work in different areas, we feel that
concepts like “frailty” and interventions like “comprehensive
geriatric assessment” are incredibly important� This report is
an opportunity to explain the language, help understanding
and ensure that value adding principles and standards drive
commissioning�

7East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
2. Introduction and purpose of the report
There is also a strong feeling that we do not reinvent the
wheel� Many sensible conclusions exist in the literature and
evidence base� Our feeling is that these are either not well
understood or that current commissioning strategies are
based on unhelpful condition specific pathways, silo working
or are constrained by existing provider organisational
structures�
2.3. Understanding the demographics
Demographic data support an imperative case for change�
The Office for National Statistics estimates that the number
of people in Britain over the age of 65 will increase by
65% over the next 25 years� The Institute of Public Care’s
Projecting Older People Population Information (POPPI)
programme predicts a 43% increase in the over 65
population in the East Midlands by 2030, with greater
increases of 78%, 72% and 116% in the 80-84, 85-89 and
90 and over populations respectively�
We recognise the significant needs of people living with
dementia, both patients and those who care for them�
This report is not intended to specifically focus on any one
diagnosis that may contribute to the clinical syndrome of
having frailty� However if services are well designed for frail
older people we would expect to see benefit for patients
with dementia�

8East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
2. Introduction and purpose of the report
In explaining the concept of frailty we also have to
acknowledge that there is no single symptom or sign, or
diagnostic disease label that can reliably identify frailty�
Surrogate markers from population health outcome data
however help to illustrate relevant points� In the report
we have used falls and hip fracture data in the over 65
population to serve this purpose�
We have set out detailed public health comparative
information for the East Midlands population aged over 65
and related that to existing outcomes� Maps of variation will
draw commissioners’ attention to inequalities�

9East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
3. What is frailty?
A 2014 NHS England, South report states that the clinical
condition of ‘frailty’ is one of the most challenging
consequences of population ageing�
• Anageingpopulationisatriskofanincreasing
number of individuals having frailty
• Havingfrailtycanbethoughtofasastateof
vulnerability due to accumulated impairments in
physical, mental or environmental wellbeing
• Adiagnosisofdementiacanindicatefrailtyevenwhen
the patient’s physical state does not
• Peoplelivingwithfrailtyareatriskoffunctional
decline and crises following small changes in their
physical, mental or environmental state
• Managingfrailtyrequiresongoingcomprehensive
multidisciplinary, multidimensional, multi-agency
assessment, diagnoses and care planning
• Olderpeoplewithfrailtycanbereadilyidentifiedand
may already be known to local professionals� They
often have weak muscles and conditions like arthritis,
poor eyesight, deafness and memory problems�
They typically walk slowly, get exhausted quickly and
struggle to get out of a chair or climb stairs
Between a quarter and half of people older than 85 are
estimated to be frail, with an overall prevalence in people
aged 75 and over of approximately 9%� People with frailty
have a substantially increased risk of falls, disability, long-
term care and death�
On the background of ongoing research to define frailty,
there are some simple approaches described� At present we
do not formally ‘diagnose’ frailty or identify it with a specific
Healthcare Resource Group code� This makes systematic

10East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
3. What is frailty?
case-finding and proactive care difficult� Slow walking
speed is a simple test that could help; taking more than five
seconds to walk four metres is highly indicative of frailty�
Although there is no evidence around primary intervention
at present, there is for secondary prevention of some aspects
of the frailty syndrome e�g� falls� However the 2014 British
Geriatrics Society publication “Fit for Frailty” advises against
a systematic case-finding approach at this stage�
Frailty has a significant impact on those living with it, their
families and carers and the care system� Frailty impacts
on the ability to live independently and to maintain social
interactions and is often related to a decline in mental
health� Frailty is closely linked to an increased risk of falls
and consequent fractures� It can also lead to social isolation,
a need for social care and ultimately transition from home
into a residential or nursing care setting�
CASE STUDY SUPPORTING FRAILTY THROUGH HOME IMPROVEMENTS AND MODIFICATIONS�
The Kings Fund have recently suggested that for every £1 spent on improving homes the NHS saves £70
over 10 years (Making the Case for Public Health Interventions, 2014)�
Derby’s Healthy Housing Service (HHS) partnership recognises that people have the potential to enjoy a
better home environment and improved health and well-being when they feel comfortable, confident,
safe, and secure at home� The aim of the service is to help those most vulnerable to poor health outcomes
as a consequence of poor housing and fuel poverty� Interventions include home improvements and
modifications to reduce the risk of poor health and home accidents�
By way of newly established referral routes, many individuals who might ordinarily miss out on or fail to
engage with initiatives offered by Derby City Council and its partners are now directly referred for support
from an expansive pool of professionals and community volunteers; contributing to the reduction in health
inequalities in the city�
In a sample (n=150) of falls clients who had been referred into the service over the period July 2012 to
June 2013 there was a reduction of 37% in A&E activity and 54% in emergency admissions to hospital in
the six months post intervention in contrast with the six months pre intervention�
Andrew Muirhead, Senior Public Health Analyst

11East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
4. Demographic imperative for change
The East Midlands data show us that demographic
imperatives for change are stark:
• Theover65populationwillincreaseby43%between
now and 2030
• Thepredictedriseintheover85spopulationiseven
greater with a 167% increase predicted by 2035 on
the 2013 baseline from 102,866 to 274,600
• Thepredictedriseinfallsrelatedadmissionsandhip
fractures cannot be met with current resources or
service design
• Wewillseeasignificantriseinthenumberofolder
people living with frailty in the population
12East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
4. Demographic imperative for change
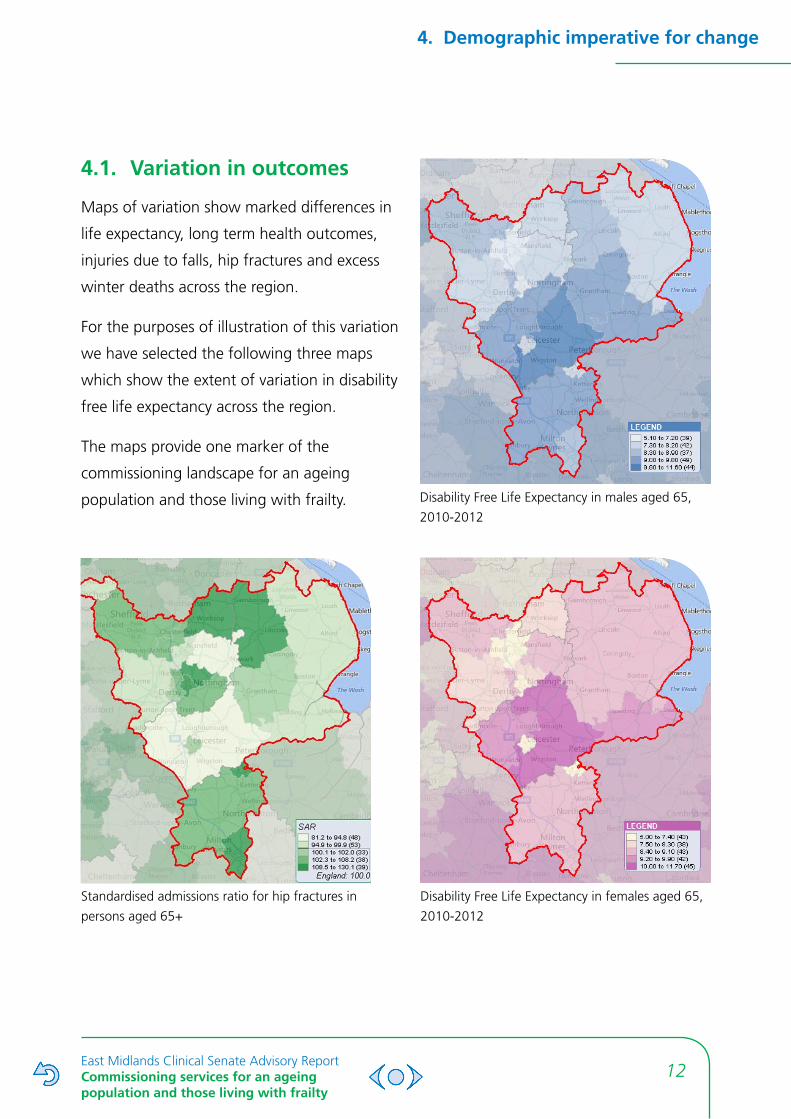
4.1. Variation in outcomes
Maps of variation show marked differences in
life expectancy, long term health outcomes,
injuries due to falls, hip fractures and excess
winter deaths across the region�
For the purposes of illustration of this variation
we have selected the following three maps
which show the extent of variation in disability
free life expectancy across the region�
The maps provide one marker of the
commissioning landscape for an ageing
population and those living with frailty� Disability Free Life Expectancy in males aged 65,
2010-2012
Disability Free Life Expectancy in females aged 65,
2010-2012
Standardised admissions ratio for hip fractures in
persons aged 65+

13East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
4. Demographic imperative for change
Although improvements in disability free life expectancy
are predicted to reduce the overall prevalence of frailty
in this group, the rise in the number of over 65s (and the
expectation that a far greater proportion of this group
will be in the 85+ age group) indicates that we will see a
significant rise in the number of older people living with
frailty in the population�
This is likely to result in increased healthcare need to prevent
and manage the higher levels of frailty related morbidity
that can be expected�
The delivery of a sustainable care system for this population
group will require a paradigm shift, with a greater focus
on primary and secondary prevention to reduce the
prevalence and consequences of frailty, through coordinated
approaches across the health and social care system�
4.2. Falls and hip fractures - forward
projection
Hospital Episode Statistics (HES) data for the East Midlands
show 15,957 falls related hospital admissions amongst the
over 65s occurred in the 2012/13 financial year, with 5,255
of these being coded as ‘with complications’� The cost of
this activity was £47,442,307� The data also show 4,805
hip fractures amongst the over 65s in the East Midlands
over the same period with 1,698 of these coded as ‘with
complications’ costing £27,670,203�
The following graphs highlight the roughly 2:1 gender ratio
for falls admissions and 4:1 gender ratio for hip fractures
with females experiencing the higher incidence of both�
14East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
4. Demographic imperative for change
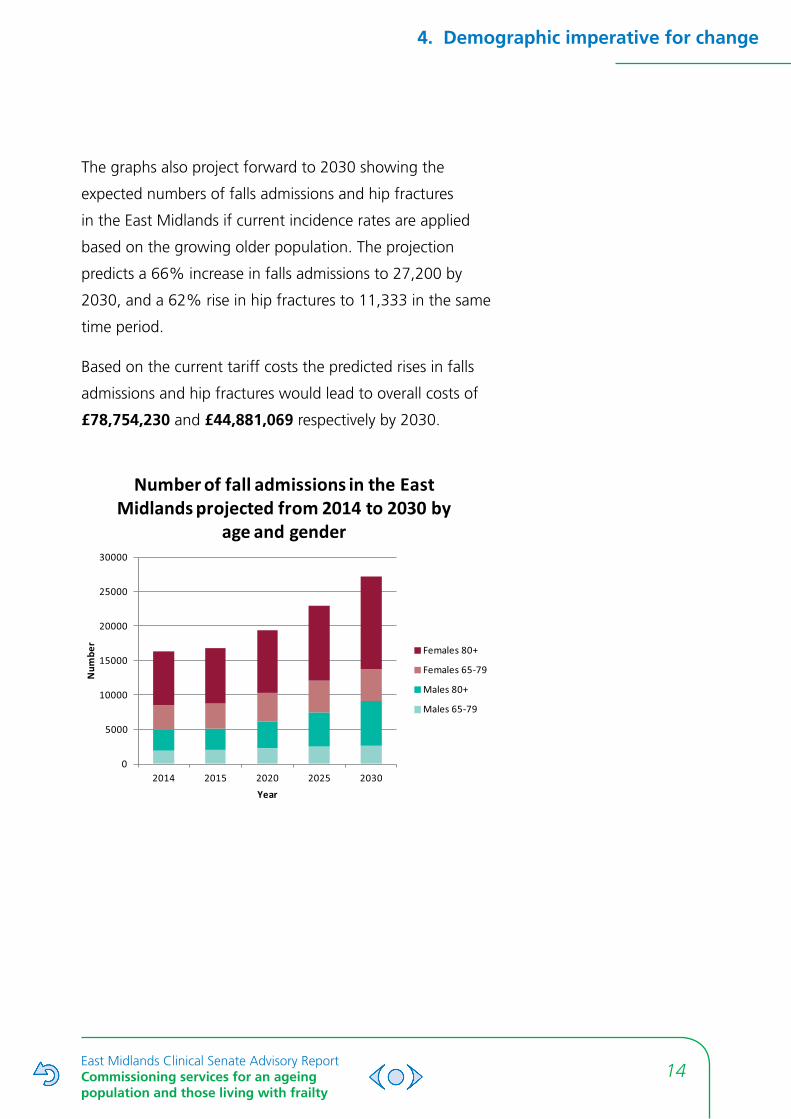
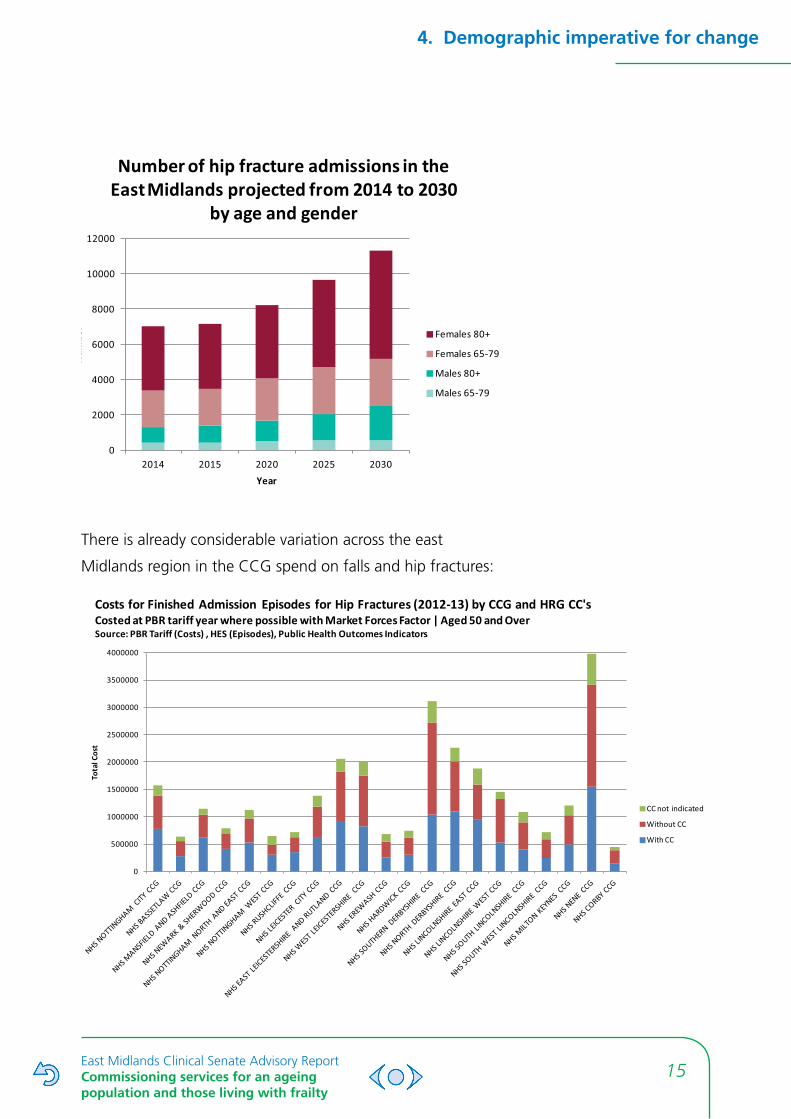
The graphs also project forward to 2030 showing the
expected numbers of falls admissions and hip fractures
in the East Midlands if current incidence rates are applied
based on the growing older population� The projection
predicts a 66% increase in falls admissions to 27,200 by
2030, and a 62% rise in hip fractures to 11,333 in the same
time period�
Based on the current tariff costs the predicted rises in falls
admissions and hip fractures would lead to overall costs of
£78,754,230 and £44,881,069 respectively by 2030�
0
5000
10000
15000
20000
25000
30000
2014 2015 2020 2025 2030
Num
ber
Year
Number of fall admissions in the East Midlands projected from 2014 to 2030 by
age and gender
Females 80+
Females 65-79
Males 80+
Males 65-79
15East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
4. Demographic imperative for change
0
2000
4000
6000
8000
10000
12000
2014 2015 2020 2025 2030
Num
ber
Year
Number of hip fracture admissions in the East Midlands projected from 2014 to 2030
by age and gender
Females 80+
Females 65-79
Males 80+
Males 65-79
There is already considerable variation across the east
Midlands region in the CCG spend on falls and hip fractures:
0
500000
1000000
1500000
2000000
2500000
3000000
3500000
4000000
Tota
l Cos
t
Costs for Finished Admission Episodes for Hip Fractures (2012-13) by CCG and HRG CC'sCosted at PBR tariff year where possible with Market Forces Factor | Aged 50 and OverSource: PBR Tariff (Costs) , HES (Episodes), Public Health Outcomes Indicators
CC not indicated
Without CC
With CC
16East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
5. What does the literature tell us and what are we doing about it?
This report has considered the advice of a number of
publications, including:
• Access all ages - Royal College of Surgeons of England
• Cochrane review of physical activity in older people
(2012)
• National audit of intermediate care (2013)
• Kings Fund report - Making our health and care
systems fit for an ageing population (2014)
• Safe, compassionate care for frail older people using
an integrated care pathway
We highlight here content from each of these reports
considered to be particularly relevant to commissioners of
health and social care in the East Midlands�
5.1. Access all ages - Royal College of
Surgeons of England
This report states that a patient’s relative need for a range of
health interventions, including surgical treatment, increases
with age� Despite this the report shows that across a range
of common conditions, elective surgical treatment rates
decline steadily for the over-65s�
There are a number of explanations for these trends:
Clinical factors
For example the impact of existing conditions or health
needs, which could mean that the risks of treatment
outweigh the benefits�

17East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
5. What does the literature tell us and what are we doing about it?
Clinical approaches
The way in which individual clinicians approach the
treatment of older people based on their own experience,
attitudes and evidence:
• Apatient’schronologicalageandhisorherbiological
age may be conflated - this means decisions may not
always be made on the basis of a comprehensive and
objective assessment but on a series of assumptions
about fitness in older age
• Theclinicalbenefitofprovidingtreatmentmaybe
questioned when relative life expectancy is shorter�
• Communicationwithpatientstodiscussrisksand
benefits, and to inform and to reflect on issues and
anxieties, may be limited or ineffective
• Theremaybeashortageofevidence,tools,strategies
and specialist clinical input to support surgical
treatment in older age
Patient awareness and preference
Patients may lack the information they need to make an
informed decision about whether surgery is right for them�
Even with the right information and support, patients may
opt out of treatment for a range of personal reasons�
The 25 recommendations of this report focus on 6 key areas:
1. Informing and communicating with patients to
encourage them to seek help and take part in
decisions about their treatment and care
2. Improving the evidence base to further our
understanding of the impact of age on surgical
decision making
3. Developing guidance to promote age equality in
surgical care
CASE STUDY REDUCING LENGTH OF STAY
SCOPES (Systematic Care
of Older People in Elective
Surgery) is a clinical
intervention designed to apply
the tenets of Comprehensive
Geriatric Assessment (CGA)
in older people presenting
for elective hip and knee
replacement to Nottingham
University Hospitals NHS Trust�
All over 75 year olds
presenting for elective hip
or knee replacement, with
an Edmonton Frailty Score
≥ 5, are seen 16-18 weeks
pre-op by a geriatrician
led multidisciplinary team
comprising physiotherapist,
occupational therapist and
nurse with access to other
services including social work
as required�
Assessment follows a 5
domain CGA model (medical,
psychological, environmental,
social and functional) with
comprehensive history taking
and examination accompanied
by baseline indices including
mental state evaluation, lying
and standing blood pressure,
3 minute timed up and go,
peak expiratory flow rate,
body mass index, an ECG and
routine bloods�
(continued...)
18East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
5. What does the literature tell us and what are we doing about it?
5.2. Cochrane Review of Physical
Activity in Older People
This report has shown a wide range of benefits to balance,
wellbeing, mobility, cognition and bone fragility from
evidence-based tailored exercise interventions� There is
particularly clear evidence regarding the benefits of exercise
for older people�
The East Midlands Clinical Senate has produced a report
for commissioners entitled Physical Activity and Exercise
Medicine�
5.3. National Audit of Intermediate Care
In drawing attention to the importance of multi-agency
working across whole systems this report offers alternatives
to the current system response of hospital care; step
up care for hospital avoidance and step down care for
early hospital discharges� Intermediate care services were
benchmarked using Patient Reported Experience Measures
using the “I” statements recommended by National Voices�
This 2013 audit demonstrated that the current provision of
intermediate care is around half of that required to avoid
inappropriate admissions and provide adequate post-acute
care for older people�
4. Delivering the most appropriate care by improving
models of working and developing guidance for
clinicians
5. Measuring progress and tackling underperformance
6. Delivering high quality commissioning for older
people
(...continued)
Interventions focus on
management of long-term
conditions, identifying and
treating occult diagnoses,
environmental risk assessment
and provision of aids and
appliances as required and
a bespoke programme of
physiotherapy, ranging from
a written exercise programme
to day-case attendance at the
NUH rehabilitation unit�
The intervention also includes
a robust anaemia diagnosis
and treatment algorithm,
developed in conjunction with
the blood transfusion service�
During the first six months
the approach resulted in
a reduction in average
length of stay of 2�1 days
for hip surgery and 2�35
for knee surgery� On the
day cancellations of elective
hip and knee surgery was
reduced to zero� This delivered
a cost saving of £166,000
based upon bed savings and
repatriation of patients from
the private sector back to
NUH�
Dr Adam Gordon
Consultant and Honorary
Associate Professor in
Medicine of Older People
19East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
5. What does the literature tell us and what are we doing about it?
Weak local strategic planning processes were identified as a
reason for lack of improvement in intermediate care capacity
since 2012� Truly integrated services across health and social
care are fundamental to delivering “person centred and co-
ordinated” care�
CASE STUDY SUPPORTING ADMISSION AVOIDANCE THROUGH EARLY INTERVENTION
NHS Nene & NHS Corby Clinical Commissioning
Groups commission independent care homes to
provide health funded placements for patients� To
ensure the clinical quality and safety of placements
a team of quality improvement managers
undertake review visits to care homes� The visits
are rated and reports, with recommendations, are
issued to each provider�
Analysis of the clinical review visit outcomes
highlighted a need to drive forward improvement
across the care home sector; to shift focus to early
intervention, treatment and prevention, develop
service provision and drive clinical quality�
A Frail and Older People work stream was
developed to:
• improveoutcomesforpatients
• educatestaffwiththeskillsandconfidence
to deliver appropriate care
• improvestandardsandpromotegood
practice
• preventavoidableadmissions
• reducedistrictnurseinput
• reduceGPcallouts
A training toolkit consists of:
• FacilitationSkillstraining
• FallsandFractureManagement
• UrinaryCatheterManagement
• DeliriumAssessment
• Anti-Psychoticstraining
• Diabetesmanagement
• Tissueviability
• Venepuncture
• SubcutaneousFluidsandNutrition
As a result falls have reduced by 13%, prescription
of antipsychotics has reduced by 25% and referrals
to emergency departments were down by 47�9%�
Overall the improvements delivered savings of
£159,000�
Waseem Shahzad - Health Education East Midlands

20East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
5. What does the literature tell us and what are we doing about it?
CASE STUDY EMPOWERING FRONT LINE STAFF
Through a series of engagement workshops with care home
managers and health and social care professionals from across
Nottinghamshire, a Clinical Quality Framework was created� This
has been trialled at a basic level, forming the foundation of a new
bespoke ‘tiered training’ approach�
The Clinical Quality Framework is a toolkit consisting of a training
programme, training resource (workbook) and a Competency
Assessment Framework� This toolkit was successfully used to deliver
training to 187 members of staff from 5 care homes (residential and
nursing) in 6 half day training sessions�
The Clinical Quality Framework proved effective in empowering
frontline staff in care homes to deliver sustainable, evidence based
care� 93% of participants stated the training would have a positive
change on their daily working practice and 95% of the attendees
stated their knowledge around the subject had increased�
This method of a tiered training approach has been successful in
delivering training on a large scale within a short period of time,
focusing on the key essential messages� This training supported
with relevant resources ensures care homes can keep building on
the learning and the consistency of the same trainers� Training
programme delivery to all five homes shows the ability to reduce
unwarranted variation across the City�
Sandra Hynes , Community Programme - Nottinghamshire County
council, Nottingham City Council, Nottingham CityCare, County
Health Partnerships, Clinical Commissioning Groups in South
Nottinghamshire, Nottingham University Hospitals and the Carers
Federation
5.4. Making our
health and care
systems fit for an
ageing population
In their report the Kings
Fund identifies the key
components of service
delivery for older people,
recommending improvement
efforts consider them all
since many older people use
multiple services:
• agewellandstaywell
• livewellwithone
or more long term
conditions
• livewellwithcomplex
co-morbidities,
dementia and frailty
• rapidsupportcloseto
home in times of crisis
• goodacutehospital
care when needed
• gooddischarge
planning and post-discharge support
• goodrehabilitationandre-ablementafteracuteillness
or injury
• highqualitynursingandresidentialcareforthosewho
need it
• choice,controlandsupporttowardstheendoflife
• integrationtoprovidepersoncentredco-ordinated
care

21East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
5. What does the literature tell us and what are we doing about it?
The report quotes the dissatisfaction of older people and
their carers with out-of-hours provision and rapid general
practice responses� It recommends that service leaders
should review the effectiveness and consistency of local
provision for urgent primary care and carry out regular
reviews of admissions for, and accident and emergency
attendances by, frail older people so that lessons from
preventable admissions can inform service redesign�
Many older people experience needs that tend to be
characterised as ‘minor’ but which can significantly affect
their independence, wellbeing and social engagement�
These include:
• mobilityproblems
• foothealth
• chronicpain
• visualandhearingimpairment
• incontinence
• malnutrition
• oralhealth.
These conditions are also characterised by highly variable
access and quality in terms of treatment� Local service
leaders must not underestimate the importance of providing
services to address these ‘minor’ needs, and should re-
examine local provision, addressing any gaps�
22East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
5. What does the literature tell us and what are we doing about it?
A key aspect of good
management of long term
conditions is ensuring that
the services and support
provided reflect the persons'
own circumstances and
preferences� People with
long term conditions
should be enabled to
engage in collaborative
care planning through pre-
arranged appointments,
co-producing a single
holistic care plan with their
care coordinator� This is
particularly important for
older people with multiple
long term conditions, since
interventions and care
planning approaches that
focus on single chronic
conditions can lead to
chaotic overall care for these
patients�
The crucial role of carers in maintaining older peoples’
independence and wellbeing is recognised in the Dilnot
Review on Care and Support, and the National Strategy
for Carers� The World Health Organisation, in its strategy
for healthy ageing in Europe, identified ‘public support
for informal caregiving’ as a key strategic priority� Local
leaders in health and social care, mental health, local
government and their voluntary sector partners should
CASE STUDY USING INTEGRATED TEAMS TO SUPPORT PATIENTS WITH FRAILTY
Lincolnshire West CCG commissioned ‘integrated teams’ in 2012/3�
The teams are made up of professional staff from local health and
social care providers� The aim of the team is to proactively manage
the care needs of frail people through early identification of frailty
and proactive management�
Since this work commenced, the Lincolnshire Health and Care
(LHAC) review is leading to the development of neighbourhood
teams� The initial focus of the neighbourhood teams is in managing
those with frailty�
Where integrated teams already exist, it is envisaged that they will
swiftly develop into neighbourhood teams�
An example of how the team is working with and for patients:
A patient with mental health issues living in rented accommodation
was about to be made homeless and have his benefits stopped� With
the patients consent, these concerns were taken to the Neighbourhood
Team where staff from the mental health, housing, safeguarding
and well-being teams were present, along with the patient’s General
Practitioner, to discuss how these issues could be addressed�
The NT were able to prevent this gentleman from being evicted,
and later got him rehomed into council accommodation� They were
also able to sort out direct payment for his rent in order to prevent
him getting into arrears again� A patients’ advocate was arranged
to help this gentleman with future care and ensure he is seen on
a regular basis by the mental health team to prevent him reaching
crisis in the future�
Tracy Means - Lincolnshire Community Health Services
23East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
5. What does the literature tell us and what are we doing about it?
review the needs of carers for older people in terms of peer
support, education, information and training, and respite,
incorporating these into all health and wellbeing plans and
mapping their own service provision against any national
strategies to support carers�
Key issues highlighted in the King’s Fund report were the
use of comprehensive geriatric assessment at the right time
and an understanding of frailty� Many health and social care
economies are describing a “left shift” towards prevention,
pro-active care and self-management and services provided
away from hospitals, closer to home� Achieving this will
require much more integrated working to ensure that the
right mix of services is available in the right place at the right
time� Incremental, marginal change is not sufficient; change
is needed at scale and at pace�
5.5. Previously published commissioning
guidance
The 2014 report “Safe, compassionate care for frail older
people using an integrated care pathway: Practical guidance
for commissioners, providers and nursing, medical and allied
health professional leaders” states that
• Iffrailolderpeoplearesupportedtoliveindependently
and understand their long term conditions, and
educated to manage them effectively, they are less
likely to reach crisis, require urgent care support and
experience harm
• Commissionerandproviderorganisationsneedto
decide which case finding and identification tools
they will use, but it is important to have a consistent
approach across all organisations involved in the care
pathway

24East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
5. What does the literature tell us and what are we doing about it?
• NHSEnglandrecommendssettingarangeofCQUINs
with providers at critical points of the frailty pathway
to help resource and embed service redesign� They
suggest that CQUINs should be developed that
encompass
o Establishment of case-finding in primary care and
a register of frail older people
o Systematic screening for frailty in people over the
age of 75 when they present in primary care, at
hospital admission and in the community setting
o Comprehensive geriatric assessment using shared
templates across all providers
o Personalised care planning, shared across all
organisations
o Development of seven-day services to support
frail older people closer to home
o The training of the voluntary sector in simple
frailty screening, and the establishment of referral
pathways, by community services
o Same-day discharge of frail older people using
discharge to assess methodology
CQUINs relating to frailty should be based on
recognised evidence� NICE Quality Standards for
dementia, hip fracture, mental wellbeing of older
people in care homes and stroke can be found at
http://www�nice�org�uk/guidance/qualitystandards/
QualityStandardsLibrary�jsp
• Outcomemeasuresareofkeyimportance,butprocess
and balancing measures should not be excluded� These
can be very useful in determining effective change
and action in the short term especially where an
intervention is particularly complex or where outcome
measures can take a long time to determine

25East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
5. What does the literature tell us and what are we doing about it?
CASE STUDY INTEGRATED HEALTH AND SOCIAL CARE MODEL IMPROVING CARE
The PRISM (Profiling Risk, Integrating Care,
Systematising Self Care) programme is predicated
on a requirement to shift the approach from the
current disease specific and reactive model of care
to one where patients are proactively managed
in a holistic way by multidisciplinary integrated
health and social teams supporting all of a patient’s
needs�
The PRISM model is based on systematic and
concurrent implementation of 6 key elements:
• Riskstratificationofthepopulationusinga
sophisticated computer based algorithm (the
Devon tool) to identify those at high risk of
admission to hospital
• Developmentofmultidisciplinaryhealthand
social care teams, working with named GP
practices to deliver complex and proactive
case management of patients at high risk of
admission to hospital
• Systematisationofself-caretosupport
people to live more independently and be
involved in decisions about their care
• Integratedhospitaldischargepathways
which bring together acute and community
teams to facilitate timely discharge from
hospital and support to live independently at
home
• DevelopmentofanenhancedIntermediate
care model which delivers Intermediate
care and rehabilitation in the patient’s own
home�
• CoordinatedandIntegratedapproachto
end of life care planning and care delivery
• Supportfororganisationsandstaffto
understand and address cultural and
behavioural barriers which may reduce their
ability to work seamlessly across the system�
The model was piloted in Newark and Sherwood
CCG during 2012/13 with 3 locality based multi-
disciplinary health and social care teams covering
100% of the CCG adult population� It has now
been scaled up and rolled out across the whole of
Mid Nottinghamshire with all the adult population
now covered by one of 8 locality based health
and social care multi-disciplinary teams working in
partnership with named GP practices�
Whilst an independent evaluation of the pilot is
near completion, initial qualitative data confirms a
consensus from all stakeholders that PRISM is more
effective than the previous approach in terms of
patient satisfaction, staff satisfaction, and patient
outcomes including hospital admissions�
During the 6 months following the launch of
the first multi-disciplinary team non- elective
admissions for patients with Long Term Conditions
reduced by 16%� This reduction was seen within
every GP practice involved in that locality, a trend
which has continued across the CCG as the
additional teams have become operational� Overall
across Nottinghamshire County (5 CCG’s) the
numbers of non-elective admissions have increased
by 0�4% in the last year, however within Newark
and Sherwood CCG we have seen a decrease of
1�9% - the largest decrease of all of the CCGs�
Mansfield and Ashfield CCG, Newark and
Sherwood CCG, Sherwood Forest NHS Foundation
Trust, Nottinghamshire Healthcare NHS Trust,
Nottinghamshire County Council, East Midlands
Ambulanced Services and Central Nottinghamshire
Clinical Services.

26East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
5. What does the literature tell us and what are we doing about it?
5.6. Workforce development
Health Education East Midlands’ Mandate states “The
priority is to train and retain a healthcare workforce
equipped with the skills to deliver much more proactive
care and support for patients in the community, and with
the right skills to support people with long-term medical
conditions to live with dignity in their own homes� Increasing
the number of General Practitioners and community
nurses will be crucial in delivering more proactive and
community based care to all and in providing and leading on
personalised care for frail older people�”
Its governing body has endorsed the move to focus its
educational investment on the workforce caring for the Frail
Elderly�
An agreement to develop a national career framework is
being developed for nurses caring for older people� The
Framework is comprised of three tiers of education and
training based on delivering the core knowledge and skills
required at foundation, specialist and higher specialist level�
The aim in splitting the education and training into three
tiers is to ensure that nurses caring for older people receive
education and training specifically focussed to support the
role they perform�
The three tiers are:
• Foundationleveleducationwhichissuitableforall
registered nurses
• Specialistleveleducationwhichissuitablefornurses
who work predominately with older people
• Higherspecialisteducationwhichissuitablefornurses
in a specialist care of older people role

27East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
5. What does the literature tell us and what are we doing about it?
More locally, Health Education East Midlands is:
• Commissioningtrainingandeducationforarangeof
health and social care staff who are caring for older
people with complex needs (including Allied Health
Professionals, Social Workers and the wider support
workforce)
• Workingcloselywiththenationalprogramme
supporting a post-registration education framework
for nurses working with older people with complex
needs
• Increasingtherateofrolloutofdementiatrainingfor
all NHS staff working with patients with dementia
• Supportingincreasednumbersofstaffundertaking
training alongside other professions (multi-professional
development)
The Nursing and Midwifery Council provides guidance on
the care of older people in its report of the same name�
The report suggests that whilst older people do not have
a particular need for the care outlined compared with any
other age group, inherent ageism in society can mean
that they are less likely to receive it� The guidance aims to
encourage nurses to develop a positive attitude towards
older people, and embrace positive feelings of respect and
an understanding that older people are important members
of society, the majority of who have the potential to
participate actively and be in control of their own lives�

28East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
5. What does the literature tell us and what are we doing about it?
5.7. East Midlands Academic Health
Science Network response
The East Midlands Academic Health Science Network Frail
Older People programme aims to advance the delivery of
Comprehensive Geriatric Assessment (CGA) to frail older
people across the region, focussing on certain areas where
it is felt that currently it is not adequately or uniformly
delivered, and in the community whenever possible� These
areas are:
• urgentcare
• dementia
• falls
• healthcareincarehomes
• healthpromotionforolderpeoplewithfrailty
They seek to achieve their aims by supporting patients,
carers, professionals and organisations around the region to
share innovation and best practice� They are encouraging
leaders in each part of the region to use this to drive up
standards against these benchmarks of quality� This process
has been started through the creation of a knowledge hub
which is an online community for knowledge transfer and
exchange� http://emfop�org�uk/

29East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
6. Comprehensive Geriatric Assessment
Comprehensive geriatric assessment (CGA) is the most
thoroughly researched model for healthcare delivery to frail older
patients� CGA delivers measurable health improvements for frail
older people� Although well understood by specialists to improve
outcomes for older people it is not routinely commissioned�
CGA is the gold standard for the care of people with frailty�
Because it is a multifaceted complex intervention it may
be misunderstood by those unfamiliar with it� CGA is a
multidimensional assessment, treatment plan and regular review
delivered by a multidisciplinary team usually including doctors,
nurses, physiotherapists, occupational therapists and social
workers�
A core component of CGA is the provision of a holistic medical
review that will diagnose medical illnesses, optimise treatment
and formulate a care plan; apply an evidence based medication
review (e�g� STOPP/START criteria) and include discussion with the
person and their carers to agree an individualised comprehensive
care and support plan�
Key elements of CGA include:
• Itisforthosewithfrailty(notnecessarilyeveryone)
• Clinicaljudgementandexperienceshoulddrivethe
recognition and identification of frailty
• Theassessmentmustbecomprehensive;thatismedical,
psychiatric, functional, social and environmental (not single
issue or single agency or discipline)
• Acareplanmustbemadebasedontheassessmentwhich
should form the basis of case management
• AdvancedCarePlanningisoftenanessentialpartoffrailty
management
• Careplandeliveryrequiresco-ordination,integration,
iteration and leadership
CASE STUDY IMPROVING PATHWAYS
A Frail Elderly Assessment
Team (FEAT) at the Royal Derby
Hospital has developed an
improved pathway for all older
people with frailty admitted to
the acute trust�
All acute admissions are
screened for frailty on arrival
in the Emergency Department
or Medical Assessment Unit�
Acute medical care takes
priority and unwell patients
have aspects of the assessment
deferred�
Once identified as at
risk of frailty a parallel
multidisciplinary assessment
begins� This allows the
therapists to conduct their
assessment alongside and
in some cases before a full
medical review has taken place,
expediting Comprehensive
Geriatric Assessment and timely
discharge where possible�
The team have access to
speech and language therapy,
dieticians, discharge facilitators
and the psychiatry liaison team�
Dedicated FEAT pharmacists
undertake medication reviews
and reconciliation�
Of 2598 patients seen by the
team, 71% went home the
same day� Initial monitoring
shows no increase in
readmission rates�
(continued...)
30East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
6. Comprehensive Geriatric Assessment
CGA done half-heartedly does not work� Sufficient intensity
and duration of therapy is required to produce meaningful
benefit e�g� in preventing falls� Consistent and appropriate
physical environments are important for people with
dementia, including in care homes�
CGA needs to take account of individual variation - that is,
physical and mental health, personality, biography, ethnicity,
preferences and beliefs�
CGA may conclude that the best care plan for an individual does
not follow what is recommended in disease-specific guidelines�
CGA has to interface with social care and end of life care -
especially given the different funding and service models for
social care�
CGA needs to include provision for dealing with crises,
acute illness and acute deteriorations in function that give
equitable access to proper assessment and investigation,
including inpatient and intermediate care services� Flu and
pneumococcal vaccination, vascular disease and bone
health management and falls prevention, day care and carer
support are all important interventions� Anticipatory care and
proactive support to care homes is also needed�
A framework for providing the core principles of CGA in
community and outpatient settings is presented in the British
Geriatrics Society publication “Fit for Frailty”�
The delivery of CGA will have substantial workforce
and training implications that need to be understood by
commissioners� A 5 to 10 year planning timetable is needed -
those who will be dependent then are alive now and we have
the population and dependency projections� Research and
training should be accommodated within those plans�
(...continued)
The recognition and coding
of frailty has increased
by 700%� Frailty and its
assessment are now at the
forefront of everyone’s mind
and it is central to the trusts
future thinking and planning�
Quotes from the Emergency
Care Intensive Support Team
report;
“The simplicity of the four
frailty markers make it
simple for ED to use and
flag patients� The electronic
system means that patients
can be easily identified by
the FEAT once they have left
ED�”
“FEAT work in partnership
with acute physicians
and there is no separate
frailty unit which keeps
it integrated into core
assessment function and
everyone’s business�”
“We felt that the FEAT model
was an example of good
practice for the assessment
and management of frail
patients� It encompasses
recognised good practice
(See Silver Book or recent
Kings Fund publication
by David Oliver on frailty
pathways)� We particularly
liked the working relationship
with acute medicine�”
Derby Hospitals NHS
Foundation Trust

31East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
6. Comprehensive Geriatric Assessment
CASE STUDY USING COMPREHENSIVE GERIATRIC ASSESSMENT WITH PATIENTS AT HOME
With timely intervention covering the 5 domains
of Comprehensive Geriatric Assessment (CGA),
some frail older people could continue to live at
home with additional support - thus preventing
unnecessary admission into hospital and/or care
homes�
Two trials were conducted in Nottingham City and
Nottingham West areas to evidence social worker
initiated CGA� Admissions were reduced as were
problems associated with polypharmacy�
Referrals were made by social workers to a
Community Geriatrician who responded within 48
to 72 hours� A letter was sent from the Geriatrician
to the Social Worker, Care Home Manager, GP and
any other relevant community based therapists� A
package of support was then co-ordinated by the
Social Worker to reflect assessment and all follow
up actions are assigned to the GP�
The project was successful in delivering social
worker initiated CGA� It was recognised that social
worker intervention may possibly be too late in
the process of effectively enacting a CGA� During
the trial, referrals identified people at high risk
of deterioration, so intervention was reactive for
patients already identified as in crisis� To be proactive
and to prevent a patient deteriorating, an earlier
‘trigger’ point needs to be identified in the process�
It was also established that the medical component
of CGA may be appropriately delivered by a
community matron or supervised geriatric medicine
speciality trainee registrar�
Sandra Hynes, Community Programme -
Nottinghamshire County council, Nottingham
City Council, Nottingham CityCare, County Health
Partnerships, Clinical Commissioning Groups in
South Nottinghamshire, Nottingham University
Hospitals and the Carers Federation

32East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
6. Comprehensive Geriatric Assessment
CASE STUDY
USING COMPREHENSIVE CGA AND COLLABORATIVE WORKING
A trial delivering Comprehensive Geriatric Assessment (CGA) to frail older people on the acute medical
assessment ward at Nottingham University Hospitals delivered positive outcomes�
Staff from the Acute Trust, City and County councils, Nottingham City Care Partnership, County Health
Partnerships and the four local CCGs collaborated to provide assessment and care�
The CGA team was made up of:
• AcuteMedicalGeriatricians(10sessions)
• SeniorNurseCGACoordinator
• RegisteredGeneralNurse
• Physiotherapist
• Physiotherapyassistant
• Supportworker
• Rapidresponseliaisonpsychiatricnurse
• SocialworkCommunityCareOfficer(1city/1countysocialservices)
• CommunityMatrons(dailyrotasystemCityCare/CountyHealthPartnerships)
A clinical presentation model was used to identify patients requiring referral to the team:
A single CGA document has been implemented and is used across care settings facilitated by local
electronic care record systems�
The team ensures that frail older people either go home on the day of admission or are appropriately
moved to health care of older people wards with a plan in place�
Transfer of care within and from hospital is supported by a multi-disciplinary CGA plan of care�
Sandra Hynes, Community Programme - Nottinghamshire County council, Nottingham City
Council, Nottingham CityCare, County Health Partnerships, Clinical Commissioning Groups in South
Nottinghamshire, Nottingham University Hospitals and the Carers Federation
Over 70 years and presenting with:
1 Falls / ‘collapse’ / syncope
2 Delirium and acute confusion
3 Previous admission in the last month
4 Known Parkinson’s Disease
5 Decision made to admit to Health Care of Older People team, but Acute Physician judgement that
CGA team and Geriatrician review would be useful
6 Acute physician request for review by CGA team (with specific question i�e� complex discharge
planning / medication review / ongoing or complex delirium)

33East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
7. Principles and standards underpinning good practice
In this report we have emphasised to commissioners that
there is a very strong clinical consensus, a strengthening
evidence base and a stark demographic imperative to
change the way services for frail older people are provided�
We have to move away from the current focus on disease-
based systems of care to a more holistic and goal-orientated
approach� Achieving this will require commissioners to
think beyond organisational boundaries and to involve
experienced health and social care professionals in their
plans� Measuring what matters to patients and their carers
will help inform commissioning strategies�
The East Midlands Clinical Senate recommends the following:
• Commissionedservicesforolderpeople
should include an assessment that helps
to identify individuals who have frailty
• Interventionsforolderpeoplewhohave
frailty should be evidence based
• Themanagementofolderpeoplewith
frailty should include the process of
care known as Comprehensive Geriatric
Assessment
• Whenpeoplelivingwithfrailtyshow
functional decline or suffer crises
the health and social care response
must be quick, comprehensive, and
multidisciplinary and delivered as close
to home as judged safe and effective by
a senior responsible decision maker
• Thecareandmanagementofpeople
living with frailty should promote
autonomy, be least restrictive, allow
choice and provide rehabilitation and re-
ablement wherever possible
• Thevision,strategyanddetailedplans
of commissioners should be enhanced
by the involvement of patients, carers
and experienced health and social care
professionals

34East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
8. Referenced evidence base
8.1. Literature review
Frailty in Elderly People - Clegg A, Young J, Iliife S, Rikkert MO,
Rockwood K�- Lancet, 2013
Prevalence of frailty in community dwelling older persons: a
systematic review - Collard et al - Am Geriatr Soc, Vol� 60
Physical rehabilitation for older people in long-term care - Crocker
T, Forster A, Young J, Brown L, Ozer S, Smith J, Green J, Hardy J,
Burns E, Glidewell E, Greenwood DC - Cochrane, 2012
Effective exercise for the prevention of falls: A systematic review
and meta-analysis - Sherrington C, Whitney JC, Lord SR, Herbert
RD, Cumming RG, Close JCT - Journal of the American Geriatrics
Society, 2008, Vol� 56
Effects of physical exercise therapy on mobility, physical
functioning, physcial activity and quality of life in community-
dwelling older adults with impaired mobility, physical disability
and/or multi-morbidity: a meta analysis - de Vries N, Ravensberg C,
Hobbelen J, Olde Rikkert M, Staal J, Nijhuis-van der Sanden M� 1,
s�l� : Ageing Research Reviews, 2012, Vol� 11�
Do home based exercise interventions improve outcomes for frail
older people? Clegg A, Barber S, Young J, Forster A, Iliffe S� 1, s�l� :
Reviews in Clinical Gerontology, 2012, Vol� 22
Better management of patients with multimorbidity� M, Roland�
s�l� : British Medical Journal, 2013, Vol� 346�
Ordering the chaos for patients with multimorbidity� J, Haggerty�
s�l� : British Medical Journal, 2012, Vol� 345�
Community care of vulnerable older people: cause for concern�
Beales D, Tulloch A� 615, s�l� : British Journal of General Practice: the
Journal of the Royal College of General Practitioners, 2013, Vol� 63�

35East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
8. Referenced evidence base
Epidemiology of multimorbidity and implications for health care,
research, and medical education: a cross sectional study� Barnett K,
Mercer S, Norbury M, Watt G, Wyke S, Guthrie B� 9836, s�l� : The
Lancet, 2012, Vol� 380�
The Identification of Frailty: A Systemative Literature Review�
Shelley A� Sternberg, Andrea Wershof Schwartz, Sathya
Karunananthan, Howard Bergman and A� Mark Clarfield� s�l� : The
American Geriatrics Society, 2001�
The Frailty Syndrome: Definition and Natural History� Xue, Qian-Li�
Baltimore : s�n�, 2010�
8.2. Collation and summary of existing
professional and national guidelines
Safe, compassionate care of frail older people using an integrated
care pathway: Practical guidance for commissioners, providers and
nursing, medical and allied health professionals - NHS England,
South (2014)
Fit for Frailty - British Geriatric Society (2014)
Access all Ages - Royal College of Surgeons (2012)
Physical activity and exercise medicine - Prof Mark E Batt, East
Midlands Clinical Senate (2014)
National Audit of Intermediate Care - Benchmarking Network
(2013)
Making our health and care systems fit for an ageing population -
The Kings Fund, (2014)
Delivering better services for people with long-term conditions:
building the house of care - Kings Fund, 2014�

36East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
9. Acknowledgements
The author of this report, Dr Ben Pearson is a consultant
physician with interests in acute and general medicine
and geriatrics� He is the Divisional Medical Director for
the Division of Integrated Care for Derby Hospitals NHS
Foundation Trust, the secondary care doctor for Mansfield &
Ashfield Clinical Commissioning Group governing body and
a member of the East Midlands Clinical Senate Council�
The Clinical Senate would like to thank the following Senate
Council and Assembly members for their contribution to the
preparation of this advisory report:
Anne Marlow - Director of Innovation, Health Education
East Midlands
Cath Chisholm - Transformation Programme Facilitator -
Kettering General Hospital
Clare Credland - Interim Matron for unplanned care,
Lincolnshire Community Health Services
Darren Aw - Consultant Geriatrician, Nottingham University
Hospitals
Hazel Firmin - Clinical Team Lead, Lincoln South Locality,
Lincolnshire Community Health Services
Pui-Shan Tang - Advanced Analyst, East Midlands
Academic Health Science Network
Tasso Gazis - Consultant Physician, Endocrinology, Diabetes
and General Medicine, Nottingham University Hospitals
Brian J Rowlands - Professor of Surgery (Emeritus),
Nottingham University Hospitals

37East Midlands Clinical Senate Advisory Report Commissioning services for an ageing population and those living with frailty
9. Acknowledgements
Ben Anderson - Consultant in Public Health (Healthcare),
Public Health England Centre East Midlands
Fiona Moor - Head of Dietetic Services, Derby Hospitals
Tracy Means - Clinical Team Leader / Complex Case
Manager, Lincolnshire Community Health Services
Further thanks to:
Professor John Gladman
Professor Rowan Harwood
Dr Adam Gordon
Dr Adrian Blundell
Dr David Stokoe
Dr Simon Conroy
Dr Jane Youde
Dr Judy Underwood
Dr Amanda Sullivan
Kathleen Sartain - Patient representative
Maureen Godfrey - Patient representative

SKYLINE. GRAPHIC DESIGN www�skylinedesign�org�uk
skyline@mail�org