come seguire il nato pretermine - pinguini.net · unità di neonatologia e terapia intensiva...
TRANSCRIPT
Fare clic per modifcare lo stle del sotottolo dello schema
10/11/12
Come seguire il nato pretermine
Fabio Mosca – Monica Fumagalli
Unità di Neonatologia e Terapia Intensiva NeonataleDipartimento per la Salute della Donna, del Bambino e del Neonato
Fondazione IRCCS Ca’ Granda – Ospedale Maggiore Policlinico - Milano

10/11/12 Born Too Soon March of Dimes 2012

10/11/12 Born Too Soon March of Dimes 2012

Fare clic per modifcare lo stle del sotottolo dello schema
10/11/12
Mortalità (%) 1990-2011
Vermont Oxford Database

10/11/12 55
Come seguire il nato pretermine dopo la dimissione?
• I “problemi apert”
• Il tming delle valutazioni diagnostche
• Le modalità di valutazione
• Gli intervent terapeutci/abilitatvi/riabilitatvi

10/11/12 66
I problemi “apert” dopo la dimissione?
SviluppoNeurologico
comportamentale
FunzionalitàRespiratoria
CrescitaNutrizione

10/11/12 77
Come seguire il pretermine dopo la dimissione?
FunzionalitàRespiratoria

10/11/12 88
Outcome respiratorio

10/11/12
Broncodisplasia polmonare (BPD)
• Una delle più comuni complicazioni a lungo termine del pretermine
• La più comune forma di malattia polmonare cronica dell’infanzia
10/11/12
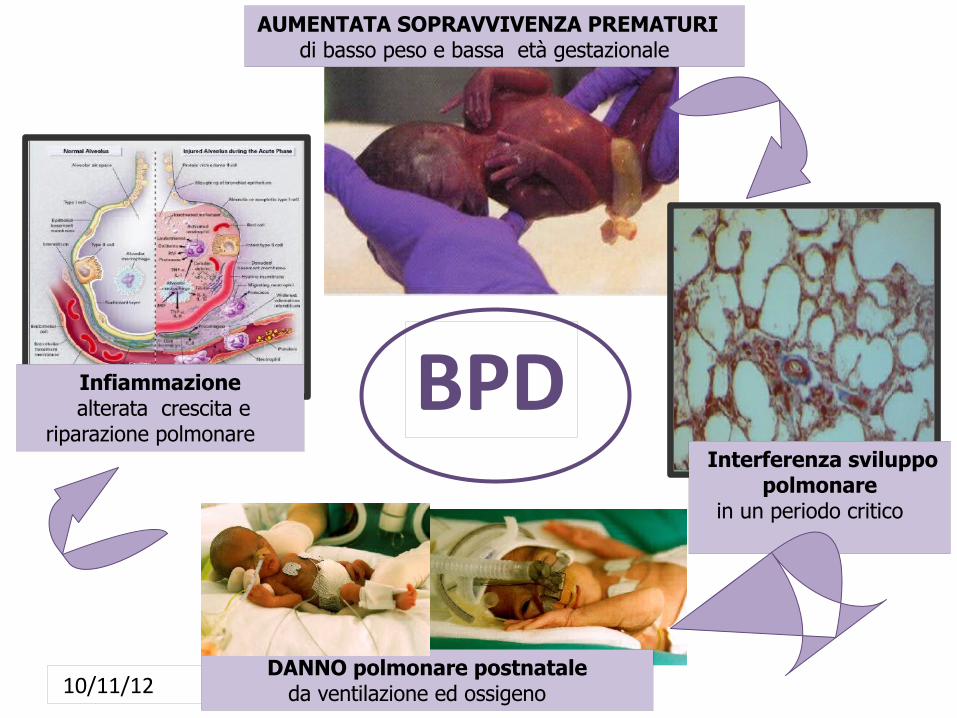
AUMENTATA SOPRAVVIVENZA PREMATURI di basso peso e bassa età gestazionale
Interferenza sviluppo polmonare
in un periodo critico
DANNO polmonare postnatale da ventilazione ed ossigeno
Infiammazione alterata crescita e
riparazione polmonare BPD

10/11/12
Definizione di gravità della BPD
PMA= post-menstrual-age
O2 per 28 giorni +
• Lieve: non O2 a 36sett.PMA
• Moderata: O2 ≤ 0.30 a 36 sett.PMA
• Grave: O2 ≥ 0.30 e/o assistenza respiratoria a 36 sett.PMA

10/11/12
CLD (%) 1990-2011
Vermont Oxford Database

10/11/12
Criteri per la dimissione di un neonato broncodisplasico a domicilio
Primhak RA. Semin Neonatol 2003;8:117-125
ü SatO2 stabile (> 94%) FiO2 stabile/ in riduzione ultime 2 sett.
ü Non crisi di apnea ultime 2 settimane
ü Familiari abili gestione di ossigenoterapia e monitoraggio domiciliareü Non modifiche terapeutiche ultime 2 sett.
ü Alimentazione orale totale (anche eventuale gavage)
ü Staff medico-infermieristico disponibile nei giorni successivi

ü Permette una dimissione più sicura
ü Favorisce la crescita somatica e del polmone
ü Riduce il rischio di cuore polmonare/ ipertensione polmonare
ü Riduce il rischio di broncocostrizione
Dimissione con ossigenoterapia domiciliare

10/11/12

10/11/12
1. Valutazione pneumologica periodica con esecuzione di prove di funzionalità respiratoria
1. Vaccinazioni obbligatorie/facoltatve e vaccino infuenzale (anche ai contat)
1. Immunoproflassi con palivizumab
1. Non inserimento in comunità
1. Controlli ecocardiografci periodici
1. Dieta ipercalorica e iperproteica.
Pratiche da adottare nel follow-up respiratorio di neonati con BPD

10/11/12
Lung function in extreme preterm (EP)with and without BPD compared to classmate controls at 11 yrs of age
Lum S, Eur Resp J 2011
Lung functon abnormalites: 78% EP children
Evidence of:
- airway obstructon - ventlaton inhomogeneity - gas trapping - airway hyperresponsiveness

10/11/12
Theoretical model of changes in FEV1 in survivors of BPD and healthy subjects according to age
Baraldi E, NEJM 2007

10/11/12
I sintomi respiratori (tosse, wheezing, infezioni ricorrent) negli nat pretermine migliorano con l’età ma persistono nell’adulto
Si verifca un certo catch growth e una normalizzazione della funzione polmonare in età adulta nei pretermine senza BPD
I pretermine con BPD presentano un’alterazione della funzione polmonare anche in età adulta

10/11/12 2020
I problemi “apert” dopo la dimissione?
CrescitaNutrizione

10/11/12
Clinica Mangiagalli 2010-2011128 VLBW nati AGA per peso
(EG: 28.5 ± 2.1 wks; PN: 1143 ±162 g)
% AGA alla nascita EUGR - alla dimissione EUGR + alla dimissione

10/11/12
Dopo la dimissione come deve essere nutrito il nato
pretermine?

10/11/12

10/11/12
Latte materno (fortificato?)
Formule per nati a termine
Formule postdischarge
Formule per pretermine
VON 2011Any human milk at discharge

10/11/12
10/11/12
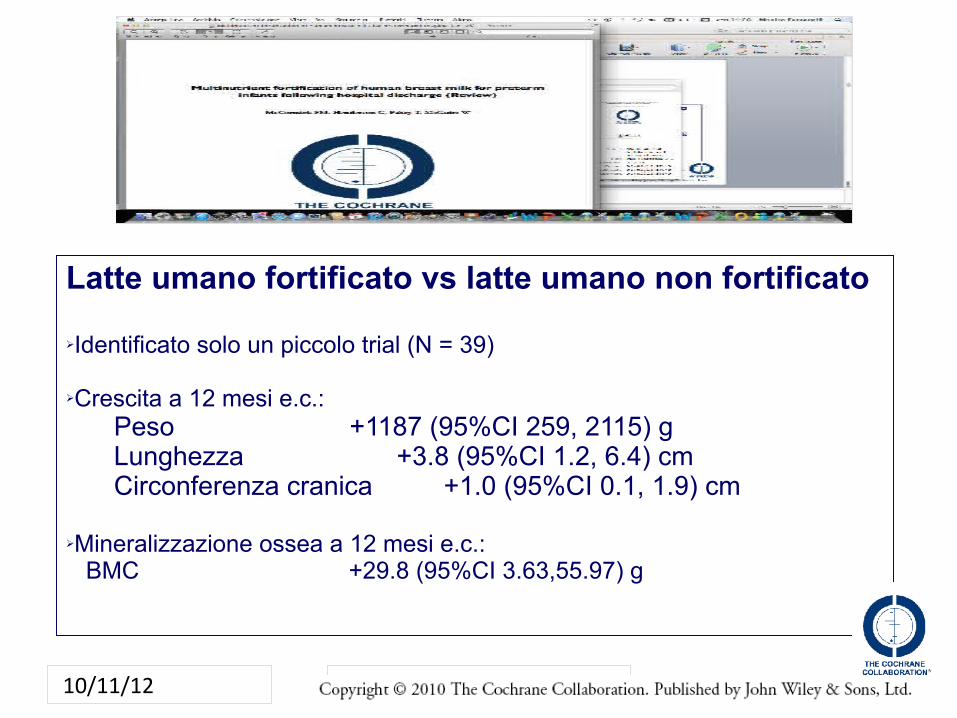
Latte umano fortificato vs latte umano non fortificato
ØIdentificato solo un piccolo trial (N = 39)
ØCrescita a 12 mesi e.c.:Peso +1187 (95%CI 259, 2115) gLunghezza +3.8 (95%CI 1.2, 6.4) cmCirconferenza cranica +1.0 (95%CI 0.1, 1.9) cm
ØMineralizzazione ossea a 12 mesi e.c.: BMC +29.8 (95%CI 3.63,55.97) g

10/11/12
Se non è disponibile latte materno vi è evidenza scientifica riguardo il tipo di
latte formulato da usare dopo la dimissione nel nato pretermine ?

10/11/12
Nato AGA – dimesso AGA
Nati AGA – dimessi SGA
Nati SGA – dimessi SGA
Nato SGA – dimesso AGA
Allattamento al seno
Formula per nati a termine
(+ LC-PUFA)
Latte materno fortificato
Formula arricchita
Almeno fino alla 40° settimana di età corretta, possibilmente fino alla 52°

10/11/12

10/11/12

10/11/12
Aim: TO EVALUATE WHETHER BEING FED AN ENRICHED FORMULA PROVIDES A GROWTH BENEFIT IN TWO GROUPS OF INFANTS CATEGORIZED ACCORDING TO INTRAUTERINE GROWTH PATTERN
Hypotesis:Can a higher protein intake promote lean mass accreton in both AGA and SGA preterm infants ?

10/11/12
41 SGAcompleted 1 year
67 AGA Enriched Formula
(High protein)
62 AGA completed 1 year
231 Enrolled141 AGA- 90 SGA
4 withdrawal
Randomizaton at Discharge-Term
Corrected Age
71 AGA Term Formula
(Low protein)
138 AGA 90 SGA
44 SGA Enriched Formula
(High protein)
46 SGA Term Formula
(Low protein) 68 AGA
completed 1 year44 SGA
completed 1 year
5 Dropout
3 Dropout
3 Dropout
2 Dropout
Enriched Formula: 75 Kcal/100 ml e 2,0 g/100 ml
Term Formula: 67 Kcal/100 ml e 1,4 g/100 ml

10/11/12
HEAD CIRCUMFERENCE (Z- score)

10/11/12
FAT MASS
% P<0.05

10/11/12
Facciamo il punto…

10/11/12

10/11/12
Quali sono i segnali di maggiore attenzione?
10/11/12
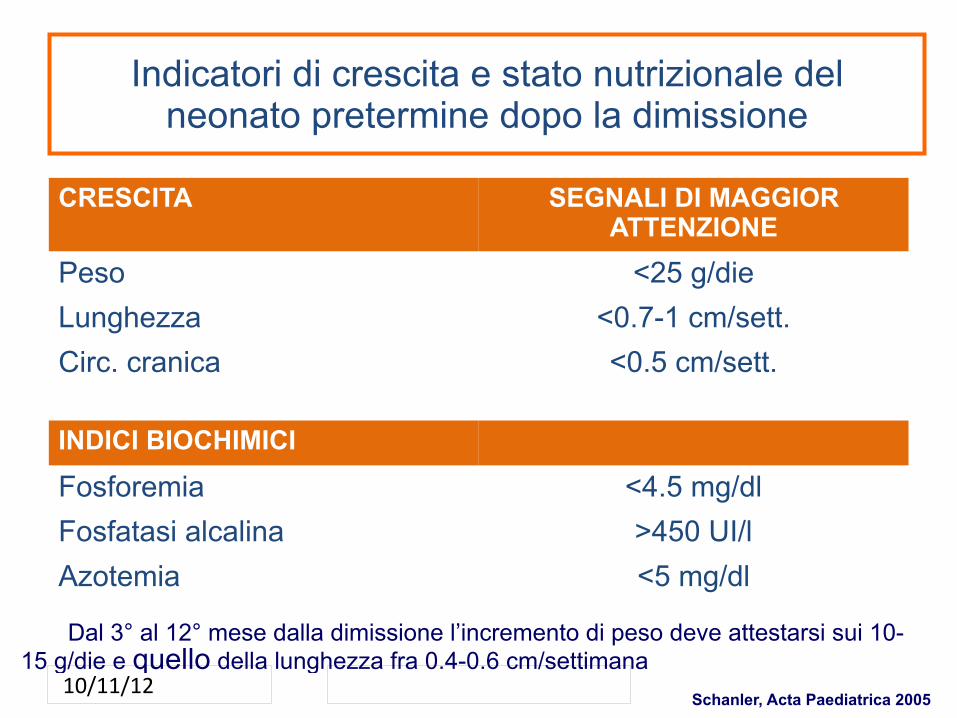
Indicatori di crescita e stato nutrizionale del neonato pretermine dopo la dimissione
CRESCITA SEGNALI DI MAGGIOR ATTENZIONE
Peso <25 g/die
Lunghezza <0.7-1 cm/sett.
Circ. cranica <0.5 cm/sett.
INDICI BIOCHIMICI
Fosforemia <4.5 mg/dl
Fosfatasi alcalina >450 UI/l
Azotemia <5 mg/dl
Dal 3° al 12° mese dalla dimissione l’incremento di peso deve attestarsi sui 10-15 g/die e quello della lunghezza fra 0.4-0.6 cm/settimana
Schanler, Acta Paediatrica 2005

10/11/12
- sostenere l’allattamento materno esclusivo durante il giorno e allattare con formula arricchita durante la notte.
- proseguire con tale regime fino a normalizzazione degli indicatori alterati.
- non è consigliabile l’utilizzo di formule per neonati a termine in quanto non propriamente rispondenti ai fabbisogni nutrizionali dei pretermine
Schanler, Acta Paediatrica 2005
INTERVENTI POSSIBILI IN CASO DI SCARSA CRESCITA

10/11/12
In caso di allattamento materno esclusivo sono consigliate le seguenti integrazioni:
FERRO: 2-4 mg/kg/die. Tale quantità può essere ridotta in accordo con il bilancio marziale ed in caso di integrazione con formula arricchita
VITAMINA D: 400 UI/die
Dall’Agnola Early Human Development, 2009
INTEGRAZIONI CONSIGLIATE

10/11/12
Esistono raccomandazioni/linee guida per il divezzamento ?

10/11/12
• Le raccomandazioni OMS consigliano LM esclusivo per 6 mesi con introduzione di cibi solidi “a partire dal 6° mese” nel nato a termine
• Nonostante rappresenti un momento di grosso cambiamento nell’alimentazione del lattante pretermine, il divezzamento ha sinora ricevuto una scarsa attenzione.
• Mancano linee guida o raccomandazioni specifiche per il divezzamento del nato pretermine

10/11/12
A reasonable compromise may need to be
adopted, such that weaning can be advised when
the infant weighs at least 5 kg, has lost the
extrusion reflex and is able to eat from a spoon.
Department of Health, UK- London, TSO, 2003

10/11/12

10/11/12
Perché non anticipare ?

10/11/12
Prematurità e allergiaNon esistono dat sicuri riguardo il ruolo dei cibi solidi nello sviluppo di allergia nell’ex-prematuro
Alcune segnalazioni (*) suggeriscono che: - una precoce introduzione-prima della 10a setmana di e.c. - più cibi introdot contemporaneamente - sesso maschile - familiarità positva per allergia
Maggior rischio allergico nel primo anno di età correta
Morgan et al, Arch Dis Child 2004

10/11/12
Conclusion: With limited evidence available and the heterogeneity
of the infant populaton born preterm, individual advice regarding
the introducton of solid foods should take into account the infant’s
gestatonal age at birth, early nutritonal intake, current nutritonal
status and requirements as well as developmental progress and
readiness.

10/11/12

10/11/12
Quali sono le categorie di pretermine a maggior rischio di mancato recupero?

10/11/12
üPresenza di complicanze mediche (CLD, danno cerebrale, enterocolite necrotizzante)
ü Bassa età gestazionale e peso alla nascita molto basso
ü Essere nati piccoli per età gestazionale
ü Sesso maschile
Fattori associati al mancato recupero di crescita

10/11/12
Healthy catch-up growth: the narrow pathway
Modifed afer Ong KK, Curr Opin Endocrinol Diabetes 2007
SGA/EUGR

10/11/12
Ø I nati pretermine sono a rischio di sviluppare un ritardo di crescita postnatale ed una alterazione della composizione corporea in termini soprattutto di deficit di massa magra durante il periodo della degenza ospedaliera e dalla dimissione al presunto termine.
Ø Nel periodo successivo si assiste nella maggior parte dei casi al recupero della crescita antropometrica.
Ø E’ importante monitorare strettamente la crescita non solo ponderale ma anche della lunghezza e della circonferenza cranica oltre alle modificazioni della composizione corporea.
Ø Un adeguato apporto proteico-energetico dopo la dimissione sembra favorire non solo il recupero di crescita ma anche la deposizione di massa magra.
Conclusioni

10/11/12 5353
I problemi “apert” dopo la dimissione?
• Evoluzione lesioni cerebrali perinatali (imaging)
• Sviluppo Neurologico Comportamentale• Defcit Neurosensoriali• Disturbi psichiatrici
10/11/12
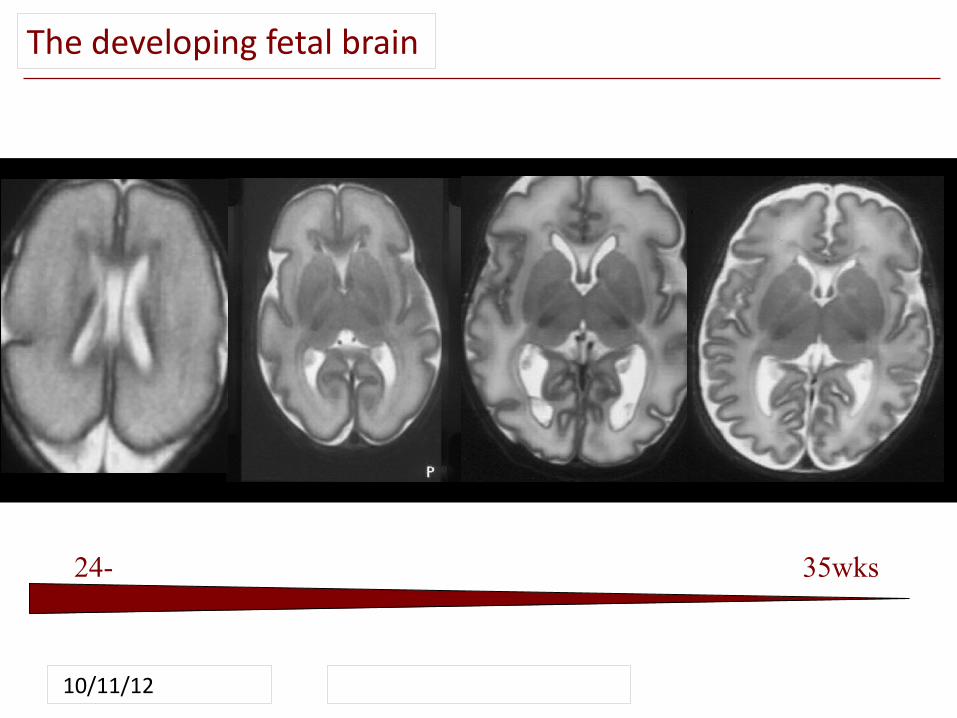
24-25wks
35wks
The developing fetal brain

10/11/12
Emorragia Intraventricolareda sanguinamento della Matrice Germinativa (GMH-IVH)
Patologia della sostanza bianca
INCIDENZA
nei VLBW
24 sett
28 sett
30 sett
10%
Età gestazionale
Problemi apert: il pretermine con lesioni cerebrali
10/11/12
Severe IVH (%) 1990-2011
Vermont Oxford Database

10/11/12
PVL (%) 1990-2011
Vermont Oxford Database

10/11/12 5858
Neuroimaging nel nato pretermine: Come e quando?
Ecografia
Risonanza Magnetica
vs

10/11/12
Emorragia intraventricolare

10/11/12
MI Levene
Dilatazione ventricolare postemorragica

10/11/12
EPIPAGE Pediatrics 2006Hintz SRPediatrics 2005EPICure Arch Dis Child Fetal Neonatal Ed 2005Hack M Arch Pediatr Adolesc Med 2000Pinto-Martin JA Dev Med Child Neurol 1999
Emorragia Intraventricolare 3°
Emorragia +Infarto venoso
Dilatazioneventricolare
• Elevata incidenza di disabilità motoria• Non significativo aumento di deficit cognitivo se non nei pazienti con grave disabilità motoria

10/11/12
Le cavitazioni all’ecografia rimangono il reperto più significativamente predittivo di paralisi cerebrale
Leucomalacia periventricolare con cavitazioni
(“cistica”)

10/11/12
Leucomalacia e outcome motorio
• Cavitazioni periventricolari > 5 mm
• Lesioni in sede posteriore
• Lesioni simmetriche
Significato prognostico negativo

10/11/12
Sequential cranial US for c-PVL
• During the first 4-6 postnatal weeks
• Between 36-40 weeks’ postmenstrual age
• Extensive cystic lesions in the white matter will still be
visible using cranial US at term equivalent age, in
contrast to only 50% of the small, localized cysts.
Linda de Vries Seminars Fetal Neon Med 2011

10/11/12
Nascita 1 volta/sett 40 sett3° - 7° gg
Follow-upDilatazione/idrocefalo
Ecografia cerebrale transfontanellare

10/11/12
…e il pretermine SENZA lesioni all’ecografa cerebrale ?
10/11/12 6767
B a s e d o n t h e s p a t i a l p r e s c r i p t i o n o f t h e i m a g e s w i t h t h e c o r p u sc a l l o s u m a n d i n t e r h e m i s p h e r i c f i s s u r e , t h e x, y , a n d z a x e s o f t h ei m a g i n g v o l u m e c o r r e s p o n d e d t o t h e b i o l o g i c a l d e v e l o p m e n t a la x e s . T h e r e f o r e , t h e g r i d d e d p a r c e l l a t i o n w a s p e r f o r m e d b e t w e e nv e n t r a l a n d d o r s a l , r o s t r a l a n d c a u d a l , a n d m e d i a l a n d l a t e r a ls u r f a c e s o f t h e b r a i n . T h e e q u i p a r t i t i o n , o n t h e o t h e r h a n d , w a sn o t a l i g n e d w i t h t h e a n a t o m y . Au n i t s p h e r e w a s f i r s t d i v i d e d i n t or e g i o n s o f e q u a l a r e a a n d t h e s e t o f c e n t e r p o i n t s o f t h e r e g i o n s w a sd e t e r m i n e d , i n o r d e r t o s e r v e a s t h e n o d e r e f e r e n c e p o i n t s . T h es p h e r e w a s t h e n s c a l e d t o t h e b r a i n s u r f a c e a n d e v e r y p o i n t o n t h eb r a i n s u r f a c e w a s a s s i g n e d t o t h e c l o s e s t n o d e r e f e r e n c e p o i n t . T h i ss i m p l e a n d p r a c t i c a l a p p r o a c h r e s u l t e d i n n o d e s o f a s i m i l a r s i z e .N o t e t h a t b o t h a p p r o a c h e s a v o i d i m p o s i n g a r b i t r a r y a n a t o m i c a l
c o n s t r a i n t s o n c o n n e c t i v i t y a n d t h e r e f o r e m a y b e b e t t e r s u i t e d t oa d d r e s s t h e d y n a m i c s t r u c t u r e o f t h e r a p i d l y c h a n g i n g d e v e l o p i n g
b r a i n , i n w h i c h t h e s u l c i a n d g y r i o f t h e a d u l t b r a i n c a n n o t b e u s e da s r e l i a b l e f i d u c i a l s .I n b o th c a se s t he n u mb e r o f n o de s w as c h os e n t o b e 40. P r e vi o u s
s t ud i es o f a d u lt c o n ne c ti v it y n et w or k s h av e u se d b e t we e n f i v e [11]a n d 998[12] c o rt i ca l r e gi o ns o f i n te r est. F or e x am pl e , H a gm a nn e ta l . [21]u se d a ‘ ‘l o w-re s o lu t io n’ ’ p a rc e ll at i o n i nt o 66 c o rt i ca l r e g io nso f v a ry in g s i z es u si n g a n a u to m at e d-lan d ma r k b a se d a lg o r it hm a nda ‘ ‘h i g h-re s o lu t io n’ ’ p a rc e ll at i o n w i th 241 ROIs o f a p pr o xi m at e lye q u al a r e a o f 6c m2 . I n o u r s t ud y , w e u s ed 40 ROIs o f s i mi l ars u r fa c e a r ea , s u ch t h at p a rc e ll at i o n o f t he r e l at i ve ly s m al l er i n fa n tb r ai n a ls o r e su lt e d i n ROIs w i th s u r fa c e a r e as o f a p pr o xi m at e ly6c m2 f o r b a bi e s a t a m e an g e st at i o na l a ge o f 31 w e ek s [22].C o n ne c ti v it y w a s t h en d e fi n ed u s in g t h e r e su l ts o f w h ole-b r ai n
f i be r t r ac t o gr a ph y . Al o we r c u to f f f i b er l e ng t h o f 10 m m w a s a p pl i edi n o r de r t o r e m ov e e x tr e m el y s h or t t r a ct s f r om f ur t h er a na l y sis. Any
F i g u r e 1 . F l o w c h a r t : A s s e m b l i ng a B a b y B r a i n S t r u c t u r a l N e t w o r k . A f ter a s e t o f d i f f u s i o n - w e i gh t e d i m a g e s i s a c q u i r e d (1), a q u a l i t ya s s u r a n c e s t e p i s p e r f o r m e d i n w h i c h d a t a a f f e c t e d b y m o t i o n a r e r e j e c t e d a n d t h e r e m a i n i n g i m a g e s a r e c o r r e c t e d f o r e d d y c u r r e n t d i s t o r t i o ns a n da f f i n e h e a d m o t i o n (2). A l t h o u g h t h i s s t e p m a y n o t b e n e c e s s a r y i n c o o p e r a t i ve a d u l t s , i t i s e s s e n t i a l f o r h i g h - q u al i t y t r a c t o g r a p hy i n i n f a n t s . T h ed i f f u s i o n t e n s o r i s c a l c u l a t e d f o r t h e r e s u l t i n g d a t a (3), a n d w h o l e - b r a i n s t r e a m l i n e f i b e r t r a c t o g r a p hy i s u n d e r t ak e n (4). T h e s u b c o r t i c a l s u r f a ce i se x t r a c t e d (5) a n d p a r t i t i o n e d i n t o n o d e s u s i n g e i t h e r t h e g r i d d e d o r e q u i p ar t i t i o n p a r c e l l a ti o n s c h e m e (6, s e e b e l o w ) . N o d e- t r a c k a n d n o d e - n o d ec o n n e c t i o n s a r e d e r i v e d (7) a n d t h e a d j a c e n c y m a t r i x i s c o n s t r u c t e d (8).doi:10.1371/ j o u r n a l . p o n e.0031029.g001
S t r u c t ur a l B a b y C o n n e c t o m e
PLoS ONE | w w w . p l o so n e . o r g 3 F e b r u a r y 2012 | V o l u m e 7 | I s s u e 2 | e31029
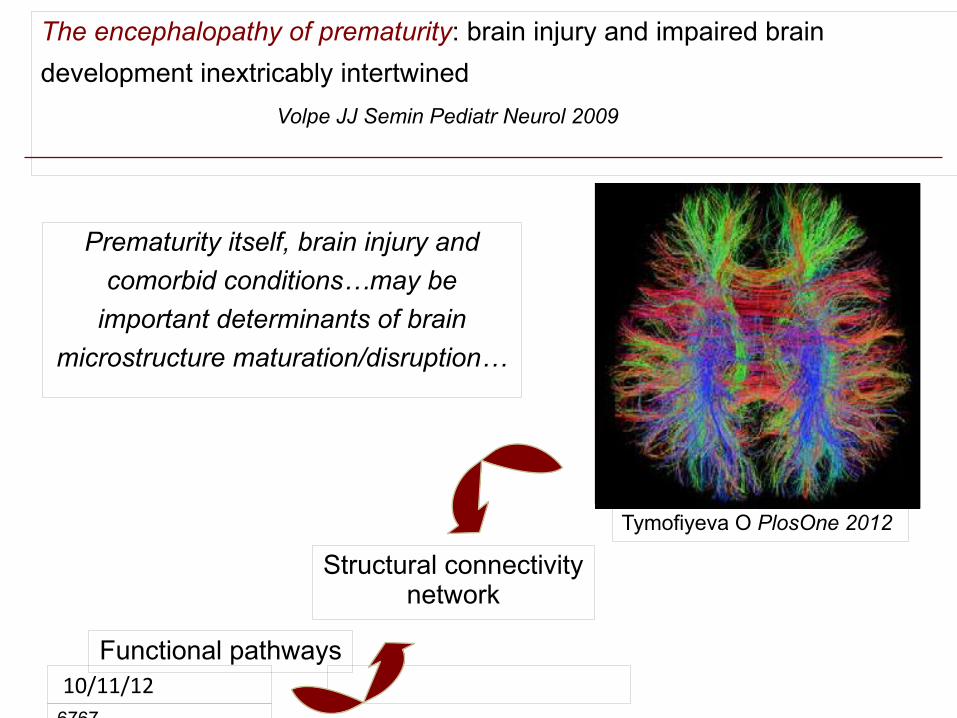
Prematurity itself, brain injury and
comorbid conditions…may be
important determinants of brain
microstructure maturation/disruption…
Tymofiyeva O PlosOne 2012
Structural connectivity network
Functional pathways
The encephalopathy of prematurity: brain injury and impaired brain
development inextricably intertwined
Volpe JJ Semin Pediatr Neurol 2009
10/11/12
B a s e d o n t h e s p a t i a l p r e s c r i p t i o n o f t h e i m a g e s w i t h t h e c o r p u sc a l l o s u m a n d i n t e r h e m i s p h e r i c f i s s u r e , t h e x, y , a n d z a x e s o f t h ei m a g i n g v o l u m e c o r r e s p o n d e d t o t h e b i o l o g i c a l d e v e l o p m e n t a la x e s . T h e r e f o r e , t h e g r i d d e d p a r c e l l a t i o n w a s p e r f o r m e d b e t w e e nv e n t r a l a n d d o r s a l , r o s t r a l a n d c a u d a l , a n d m e d i a l a n d l a t e r a ls u r f a c e s o f t h e b r a i n . T h e e q u i p a r t i t i o n , o n t h e o t h e r h a n d , w a sn o t a l i g n e d w i t h t h e a n a t o m y . Au n i t s p h e r e w a s f i r s t d i v i d e d i n t or e g i o n s o f e q u a l a r e a a n d t h e s e t o f c e n t e r p o i n t s o f t h e r e g i o n s w a sd e t e r m i n e d , i n o r d e r t o s e r v e a s t h e n o d e r e f e r e n c e p o i n t s . T h es p h e r e w a s t h e n s c a l e d t o t h e b r a i n s u r f a c e a n d e v e r y p o i n t o n t h eb r a i n s u r f a c e w a s a s s i g n e d t o t h e c l o s e s t n o d e r e f e r e n c e p o i n t . T h i ss i m p l e a n d p r a c t i c a l a p p r o a c h r e s u l t e d i n n o d e s o f a s i m i l a r s i z e .N o t e t h a t b o t h a p p r o a c h e s a v o i d i m p o s i n g a r b i t r a r y a n a t o m i c a l
c o n s t r a i n t s o n c o n n e c t i v i t y a n d t h e r e f o r e m a y b e b e t t e r s u i t e d t oa d d r e s s t h e d y n a m i c s t r u c t u r e o f t h e r a p i d l y c h a n g i n g d e v e l o p i n g
b r a i n , i n w h i c h t h e s u l c i a n d g y r i o f t h e a d u l t b r a i n c a n n o t b e u s e da s r e l i a b l e f i d u c i a l s .I n b o th c a se s t he n u mb e r o f n o de s w as c h os e n t o b e 40. P r e vi o u s
s t ud i es o f a d u lt c o n ne c ti v it y n et w or k s h av e u se d b e t we e n f i v e [11]a n d 998[12] c o rt i ca l r e gi o ns o f i n te r est. F or e x am pl e , H a gm a nn e ta l . [21]u se d a ‘ ‘l o w-re s o lu t io n’ ’ p a rc e ll at i o n i nt o 66 c o rt i ca l r e g io nso f v a ry in g s i z es u si n g a n a u to m at e d-lan d ma r k b a se d a lg o r it hm a nda ‘ ‘h i g h-re s o lu t io n’ ’ p a rc e ll at i o n w i th 241 ROIs o f a p pr o xi m at e lye q u al a r e a o f 6c m2 . I n o u r s t ud y , w e u s ed 40 ROIs o f s i mi l ars u r fa c e a r ea , s u ch t h at p a rc e ll at i o n o f t he r e l at i ve ly s m al l er i n fa n tb r ai n a ls o r e su lt e d i n ROIs w i th s u r fa c e a r e as o f a p pr o xi m at e ly6c m2 f o r b a bi e s a t a m e an g e st at i o na l a ge o f 31 w e ek s [22].C o n ne c ti v it y w a s t h en d e fi n ed u s in g t h e r e su l ts o f w h ole-b r ai n
f i be r t r ac t o gr a ph y . Al o we r c u to f f f i b er l e ng t h o f 10 m m w a s a p pl i edi n o r de r t o r e m ov e e x tr e m el y s h or t t r a ct s f r om f ur t h er a na l y sis. Any
F i g u r e 1 . F l o w c h a r t : A s s e m b l i ng a B a b y B r a i n S t r u c t u r a l N e t w o r k . A f t er a s e t o f d i f f u s i o n - w e i gh t e d i m a g e s i s a c q u i r e d (1), a q u a l i t ya s s u r a n c e s t e p i s p e r f o r m e d i n w h i c h d a t a a f f e c t e d b y m o t i o n a r e r e j e c t e d a n d t h e r e m a i n i n g i m a g e s a r e c o r r e c t e d f o r e d d y c u r r e n t d i s t o r t i o ns a n da f f i n e h e a d m o t i o n (2). A l t h o u g h t h i s s t e p m a y n o t b e n e c e s s a r y i n c o o p e r a t i ve a d u l t s , i t i s e s s e n t i a l f o r h i g h - q u al i t y t r a c t o g r a p hy i n i n f a n t s . T h ed i f f u s i o n t e n s o r i s c a l c u l a t e d f o r t h e r e s u l t i n g d a t a (3), a n d w h o l e - b r a i n s t r e a m l i n e f i b e r t r a c t o g r a p hy i s u n d e r t ak e n (4). T h e s u b c o r t i c a l s u r f a ce i se x t r a c t e d (5) a n d p a r t i t i o n e d i n t o n o d e s u s i n g e i t h e r t h e g r i d d e d o r e q u i p ar t i t i o n p a r c e l l a ti o n s c h e m e (6, s e e b e l o w ) . N o d e- t r a c k a n d n o d e - n o d ec o n n e c t i o n s a r e d e r i v e d (7) a n d t h e a d j a c e n c y m a t r i x i s c o n s t r u c t e d (8).doi:10.1371/ j o u r n a l . p o n e.0031029.g001
S t r u c t ur a l B a b y C o n n e c t o m e
PLoS ONE | w w w . p l o so n e . o r g 3 F e b r u a r y 2012 | V o l u m e 7 | I s s u e 2 | e31029
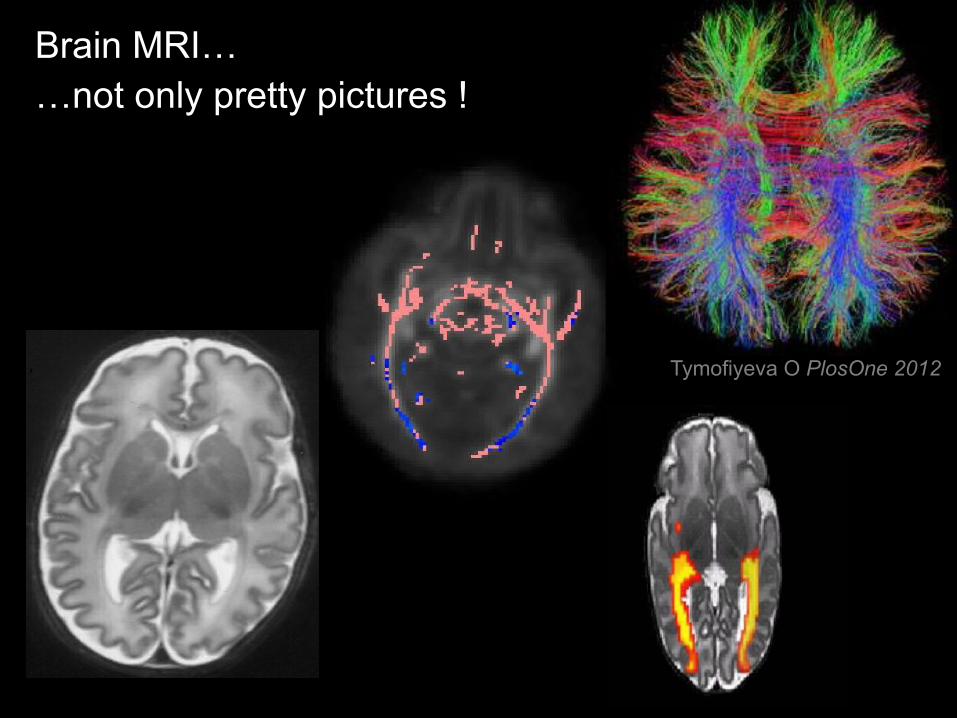
Brain MRI……not only pretty pictures !
Tymofiyeva O PlosOne 2012

A termine di età corretta
?Preterm at term Term baby
RM nel neonato a rischio: quando?

10/11/12
Motorio ComportamentaleCognitivo
Età cronologica
Problemi apert: outcome neurologico a distanza
Quali sono gli esiti a distanza della prematurità?
Come possiamo identificarli?
Come possiamo intervenire?
3 domande
Follow-up nato pretermine

Quali sono gli esiti della nascita prematura?
Come possiamo identificarli?
Come possiamo intervenire?
3 domande

J.E.Tyson, Intensive Care for Extreme Prematurity —Moving Beyond Gestational Age, N Engl J Med 358;16, april 2008
l cerebral palsy
l cognitive delay ( DQ < 70 )
l hearing loss (requiring amplification)
l visual impairment: bilateral blindness
Profound disability as having
• Cognitive delay below 50 ( DQ < 50)
l Level 5 of GMFCS
1. Major Impairment (severe disability)

Paralisi cerebrale (major impairment)
Danno ischemico alla sostanza bianca
Danno emorragico
Leucomalacia periventricolare
PVL
Emorragia intraventricolare
IVH
Disturbo persistente,
ma non immutabile,
del movimento e della postura,
dovuto ad un disordine non progressivo
del cervello immaturo
BRETT (1983)

2. Minor dysfunctions l 1. clumsiness
l 2. learning disabilities
l 3. behavioural disturbances
l 4. adaptive functions
25.3.2010
Ø Leonard e Piecuch, Seminars Perinatol 1998
Ø Vohr, Allan et al., JAMA 2003
ØCooke, Arch Dis Child 2003

1a. Clumsy child
l Impaccio
l problemi
di coordinazione
l problemi di equilibrio

1b. Anomalie posturalil Torace, rachide, arti
inferiori
l plagiocefalia
2. Learning disabilities
l organizzazione visuospaziale
l organizzazione percettiva
l disprassia

• Disturbi dei ritmi sonno-veglia
• Disturbi dell’alimentazione
• Deficit di regolazione emotiva
• Iperattività
• Inibizione
3. Behavioural disturbances

Quali sono gli esiti a distanza della prematuità?
Come possiamo identificarli?
Come possiamo intervenire?
3 domande

1. Neurofunctional assessment (Picciolini et al, 2006) 40 s - 7 a
2. Griffiths Developmental Scale (Revision 1996) 6 m - 7a
3. Bayley Scales of Infant Development (Third Edition 2003) 2a
4. Child Behavior Checklist (Achenbach, Vermont, 2001) 2a – 7a
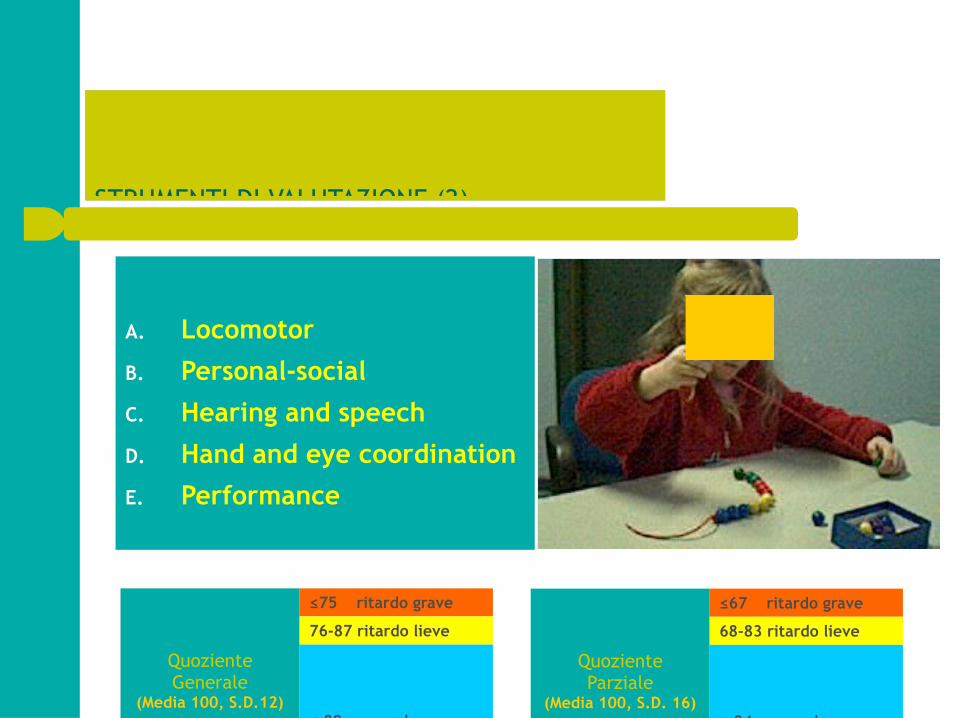
STRUMENTI DI VALUTAZIONE (2)
A. Locomotor
B. Personal-social
C. Hearing and speech
D. Hand and eye coordination
E. Performance
QuozienteParziale
(Media 100, S.D. 16)
≤67 ritardo grave
68-83 ritardo lieve
≤ 84 normale
QuozienteGenerale
(Media 100, S.D.12)
≤75 ritardo grave
76-87 ritardo lieve
≤ 88 normale

25.3.2010
85 - 114 nella norma70 – 84 (1^ DS) lieve ritardo55 - 69 (2^ DS) grave ritardo >114 prest accelerata
Quozienti:Media 100, S.D. 15 Second Edition 2007
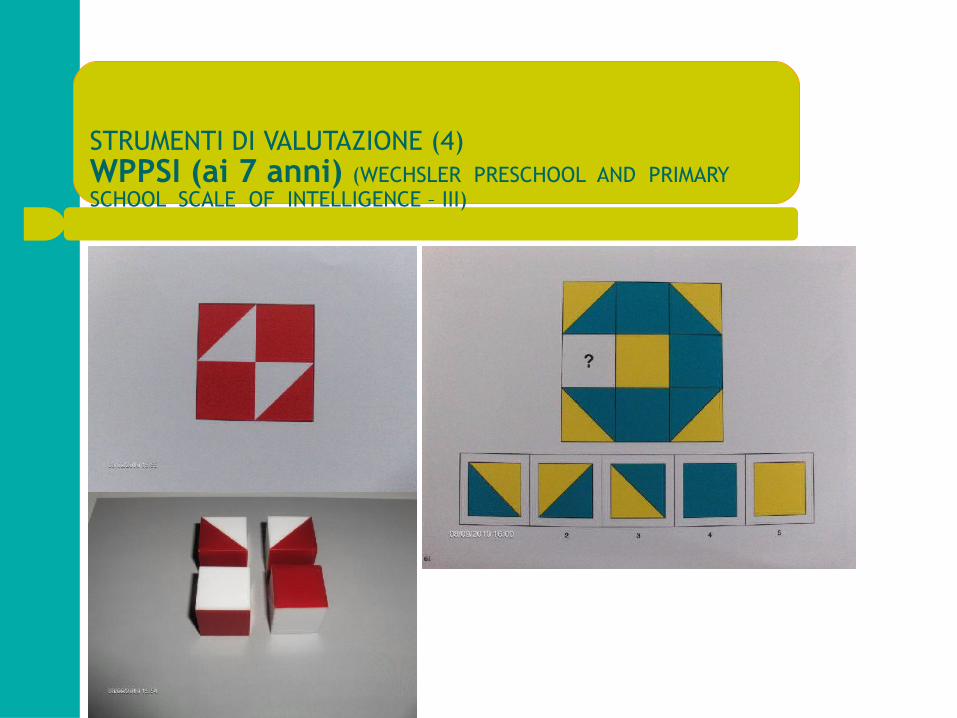
STRUMENTI DI VALUTAZIONE (4) WPPSI (ai 7 anni) (WECHSLER PRESCHOOL AND PRIMARY SCHOOL SCALE OF INTELLIGENCE – III)

Quali sono gli esiti della nascita prematura?
Come possiamo identificarli?
Come possiamo intervenire?
3 domande

Fare clic per modificare lo stile del sottotitolo dello schema
INTERVENTI RIABILITATIVI AMBULATORIALI
U.O. di Neonatologia e Terapia Intensiva Neonatale
Valutazione neurofunzionale
intervento ind. FT intervento FT con supervisione psicologica
gruppo mamma-bambino
psicomotricità
logopedia
invio ai Servizi
…………………………………………………………………………6-12 mesi
3-6 mesi
0-3 mesi
gruppo Feuersteinetàsuccessiv
e

Vermont Oxford NetworkELBW FOLLOW-UP
25.3.2010
INFANT ELIGIBILITY
● BW 401 - 1000 grams (inclusive)
or
● GA 22,0 – 27,6 weeks (inclusive)

10/11/12

10/11/12

10/11/12

10/11/12

10/11/12 9292
Quali altre funzioni possono essere alterate dalla nascita pretermine?
Quali strument di valutazione?

Fare clic per modifcare lo stle del sotottolo dello schema
10/11/12
Le funzioni visive

10/11/12
ROP ≥ 3 (%) 1990-2011
Vermont Oxford Database

10/11/12
FUNZIONI VISIVE NEL NEONATO
• si sviluppano presto, sono tra le prime funzioni cognitive a svilupparsi
• presentano tappe ben precise nel corso del primo anno di vita
• sono legate alla maturazione di specifici sistemi cortico e sottocorticali
• “Vision also serves as the basis for early developing sensory-motor and cognitive
skills, wich can be tracked through early childhood.” Atkinson J, Braddick O Progress in Brain Research Vol 164 2007

10/11/12

10/11/12
…Executive functions are broadly synonymous with
function of the prefrontal cortex of the brain and
supporting loops but may be variously interpreted as
functions needed to achieve goal directed behavior…
Neil Marlow Pediatrics 2007

10/11/12
Funzioni Esecutive
• Cosa sono? Obiettivi, piano per raggiungerli,
inibizione impulsi, memoria…
• Che importanza hanno? Strategie di apprendimento, per l’adattamento psicologico e sociale del bambino
• Se mancano? Problemi di attenzione/impulsività,
disorganizzazione, ridotta autonomia

10/11/12
Emerging executive skills in very preterm children at 2 years correct age:
a composite assessment
Pozzetto T, Marzocchi G, Ometto A, Mosca F...in press

10/11/12
Fino a quando seguire il nato pretermine ?

10/11/12
133
THE PRETERM PHENOTYPE - A COGNITIVE MODEL EXPLAINS THE PROSPECTIVE RELATIONSHIP BETWEEN PREMATURITY AND MATHEMATICAL PERFORMANCE
DEFICITS
J. Jaekel, D. Wolke, Germany, UK
Background and aims: The human brain is highly susceptible to the consequences of preterm birth. Cognitive tasks vary in complexity and resource requirements, thus performance on tasks with different demands may provide information on specific cognitive differences in children related to the degree of prematurity. Mathematical performance requires simultaneous processing of information which is particularly compromised in preterm children. Our aim was to investigate the relationships between task complexity and incremental performance deficit s across the full spectrum of gestational age (GA). Methods: 1,513 children ranging from 27 to 43 weeks GA were studied from birth to 8;5 years as part of a prospective geographically defined longitudinal investigation of neonatal at-risk children in South Germany (Bavarian Longitudinal Study). Children's cognitive performance at 8;5 years was measured with K-ABC subtests Number recall, Pattern reasoning, and Calculating and with a standardized mathema tics test. Results: Results were twofold: 1. Preterm children showed incremental performance deficits with increasing task complexity. 2. There was a curvilinear relationship between GA and task performance with a point of change around 32 weeks of GA. In general, every lost week of gestation increased the adverse impact on performance. However, this relationship was strongest among tasks which required the highest cognitive workload. Conclusions: With increasing cognitive workload preterm children fall behind in test scores. This suggests that brain organisation or damage limits cognitive resources. The relationship between GA and task performance is curvilinear. Our approach may offer a theoretical foundation to scrutinize the cognitive characteristics of the preterm phenotype.
1.513 children ranging from 27 to 43 weeks GA were studied from birth
to 8.5 years of age
Preterm children showed incremental performance deficits with increasing task complexity.
There was a curvilinear relationship between GA and task performance with a point of change around 32 weeks of GA.

10/11/12
Two-hundred non-disabled very preterm (mean age = 8.2 ± 2.5) and 230 term children (mean age = 8.3 ± 2.3), all born between 1996 and 2004
Very preterm children had significantly more mathematical and
attention problems than term. IQ significantly predicted mathematical problems

10/11/12
Arch Dis Child Fetal Neonatal Ed 2009;94:F283–F289.
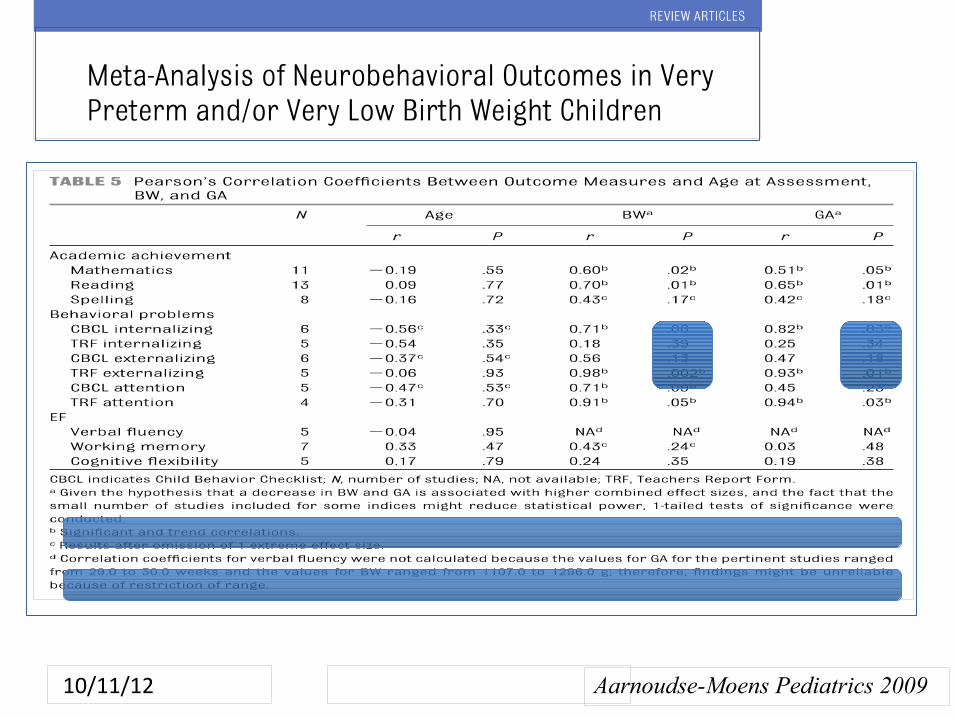
10/11/12 Aarnoudse-Moens Pediatrics 2009
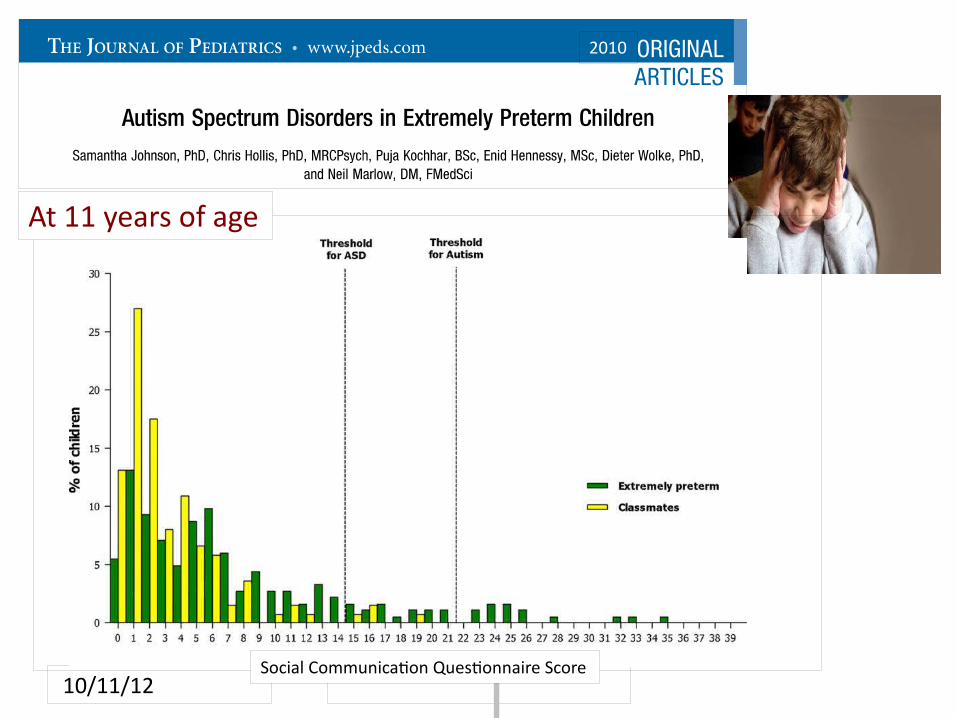
10/11/12 Social Communicaton Questonnaire Score
At 11 years of age
2010

10/11/12
Come seguire il nato pretermine dopo la dimissione?