combined modality multidisciplinary approach to cancer treatment
TRANSCRIPT

7/27/2019 Combined Modality Multidisciplinary Approach to Cancer Treatment
http://slidepdf.com/reader/full/combined-modality-multidisciplinary-approach-to-cancer-treatment 1/9
COMBINED MODALITY
MULTIDISCIPLINARY APPROACH TO
CANCER TREATMENT
Dr. Villa
January 20, 2014
Group 4
Basic principle in therapy:
To cure the disease
To control the disease
To palliate the patient’s symptoms with
minimum functional and structural impairment
Major Disciplines in the Management of Cancer
Surgery - qualified surgeons
Radiotherapy- qualified radiooncologists
Chemotherapy/ Hormonal Therapy/
Immunologic Therapy - qualified
internists/medical oncologists (i.e. adult
patients)
Current Anti-Cancer Approaches
Surgery Remove known tumor/masses
Chemotherapy Kills rapidly dividing tumor
cells
Radiation therapy Kills rapidly dividing tumor
cells (local treatment, no systemic effect)
Targeted therapy Specifically inhibit required
process in tumor cell growth
SURGERY
Most of the time, lobectomy is done to ensure
that the entire tumor and its circulation is out.
In patients who cannot tolerate having a lung
removed, no matter how small the tumor is,
surgery is not advised. Especially for female non-
smokers.
RADIATION THERAPY
Destruction of cancer cells using ionizing
radiation
Supplementary surgery and palliate pain (in bone
metastasis)
Complications: skin reactions, mucositis,
hoarseness of voice, hypothyroidism, low
blood counts, lung fibrosis, heart
complications, secondary cancers
A primary treatment
Before surgery to shrink a tumor
After surgery to eliminate any remaining cancer
cells To treat cancer that has spread to other areas of
the body
Types of Radiation
External Beam Radiation Therapy (EBRT):
delivers high doses of radiation to lung cancer
cells from outside the body, using a variety of
machine-based technologies.
High Dose Rate(HDR) Brachytherapy (Internal
Radiation): delivers high doses of radiationfrom implants placed close to, or inside, the
tumor(s) in the body
Advantages of EBRT
Accurately targets a tumor with higher doses
of radiation, while minimizing damage to
healthy lung tissue and nearby organs. As a

7/27/2019 Combined Modality Multidisciplinary Approach to Cancer Treatment
http://slidepdf.com/reader/full/combined-modality-multidisciplinary-approach-to-cancer-treatment 2/9
result, EBRT helps to lower the risk of side effects
typically associated with radiation treatment
for lung cancer, such as difficulty breathing or
heart damage
Some additional advantages of external beam
radiation therapy include:
- fast, painless outpatient procedure- does not carry the standard risks or
complications of surgery, such as surgical
bleeding, post-operative pain, or the risk of
stroke, heart attack, blood clot and external
treatment
- unlike chemotherapy, which circulates
throughout the body, ERBT is targeted to the
area being treated
CHEMOTHERAPY
Drug treatment to kill fast-growing cancer cells
- acts on DNA, RNA or proteins of signal
transduction
Examples: Capecitabine(Xeloda), Doxurubicin,
Oxaliplatin, Paclitaxel
Effects: systemic in nature
- Side Effects: low blood counts, nausea/vomiting,
alopecia, local reactions, mucositis, cardiotoxicity
etc.
Cell Cycle
Tumor Growth Kinetics
Tumor cell growth is logarithmic
Mechanism of Action
Most chemotherapeutic drugs work by impairing
mitosis (cell division), effectively targeting fast-
dividing cells
Cell Kill
Only a percentage of the cancer cells are killed
with each course of chemotherapy. Therefore,
repeated doses – or cycles of chemotherapy
must be done.
Tumor growth is exponential and kills constant
fraction of tumor cells.
Sites of Action of Cytotoxic Agents
Manner of Administration
1. Adjuvant therapy Cure
2. Neoadjuvant therapy R0 resection, Cure
3. Palliative Control, Quality of Life
7/27/2019 Combined Modality Multidisciplinary Approach to Cancer Treatment
http://slidepdf.com/reader/full/combined-modality-multidisciplinary-approach-to-cancer-treatment 3/9
CLASSIFICATION of CHEMOTHERAPY DRUGS
CYCLE SPECIFIC
● Antimetabolites
interfere with nucleic acid synthesis
attack during S phase of life cycle
Examples: Cytatabine, Floxuridine,
Fluorouracil, hydroxyurea,methotrexate, thioguanine
● Enzymes
useful only for leukemias
Example: Aspariginase
● Plant Alkaloids
cycle specific to M Phase
prevent mitotic spindle formation
Examples: Vinblastine, Vincristine
CYCLE NON-SPECIFIC
● Alkylating Agents
disrupt deoxyribonucleic acid(DNA)
Example: Carboplatin, Cisplatin,
Cyclophosphamide, Thiotepa
● Antibiotics
bind with DNA to inhibit synthesis of
DNA and RNA -Examples:
Bleomycin, Doxorubicin, Idarubicin,
Mitomycin, Mitoxantrone
TARGETED THERAPY
Personalized treatment
Understanding the biology of the tumor helps
the treatment regimen. Treatment is patterned
to the behavior of the tumor or to the direct
mutation it undergoes.
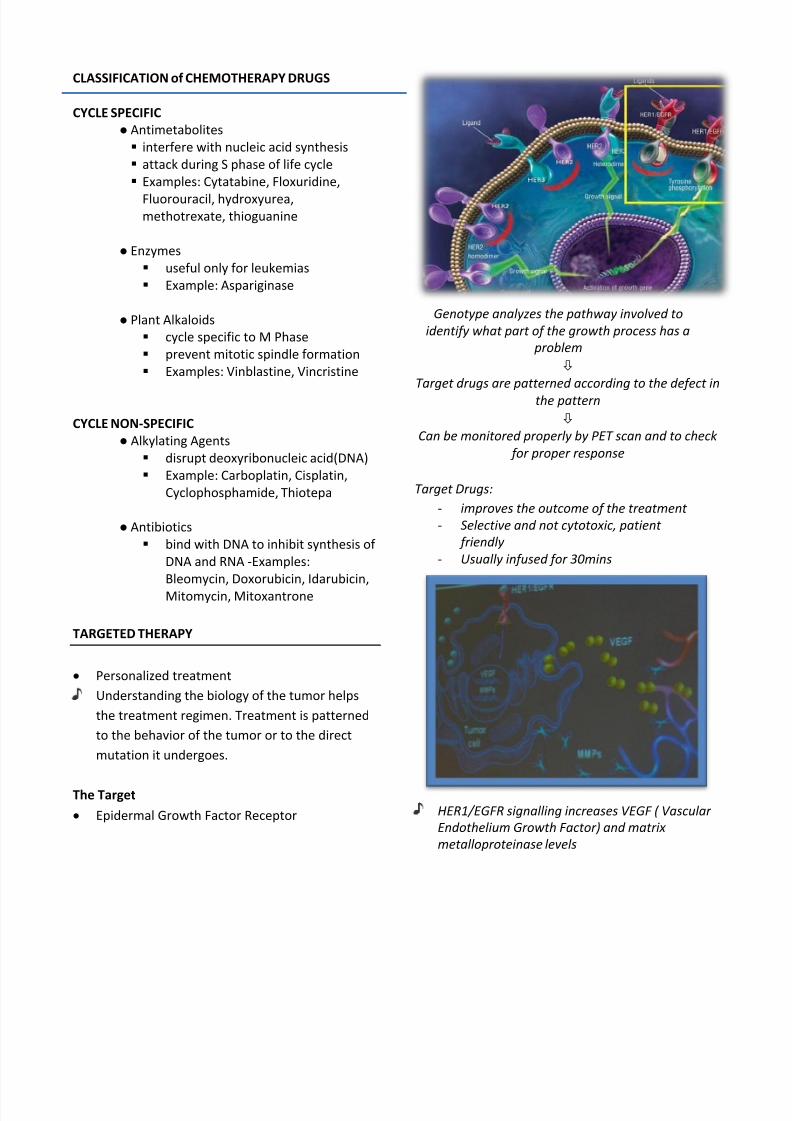
The Target
Epidermal Growth Factor Receptor
Genotype analyzes the pathway involved to
identify what part of the growth process has a
problem
Target drugs are patterned according to the defect in
the pattern
Can be monitored properly by PET scan and to check
for proper response
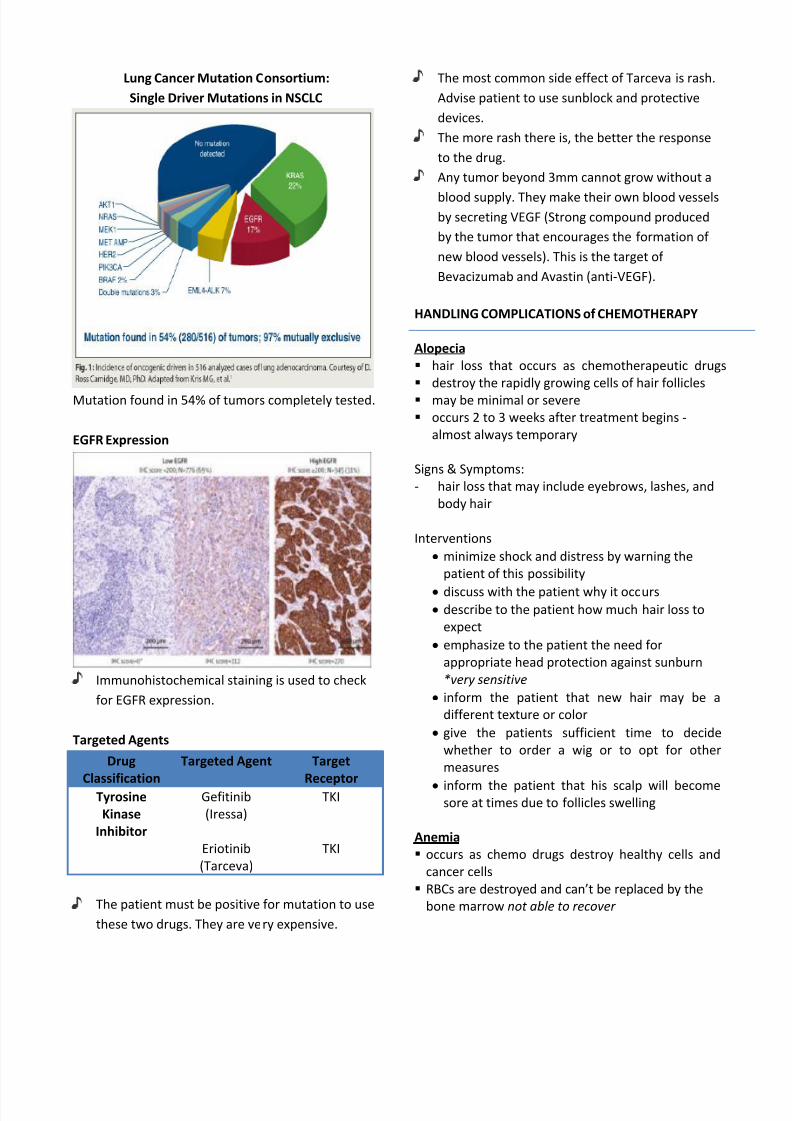
Target Drugs:
- improves the outcome of the treatment
- Selective and not cytotoxic, patient
friendly
- Usually infused for 30mins
HER1/EGFR signalling increases VEGF ( Vascular
Endothelium Growth Factor) and matrix
metalloproteinase levels
7/27/2019 Combined Modality Multidisciplinary Approach to Cancer Treatment
http://slidepdf.com/reader/full/combined-modality-multidisciplinary-approach-to-cancer-treatment 4/9
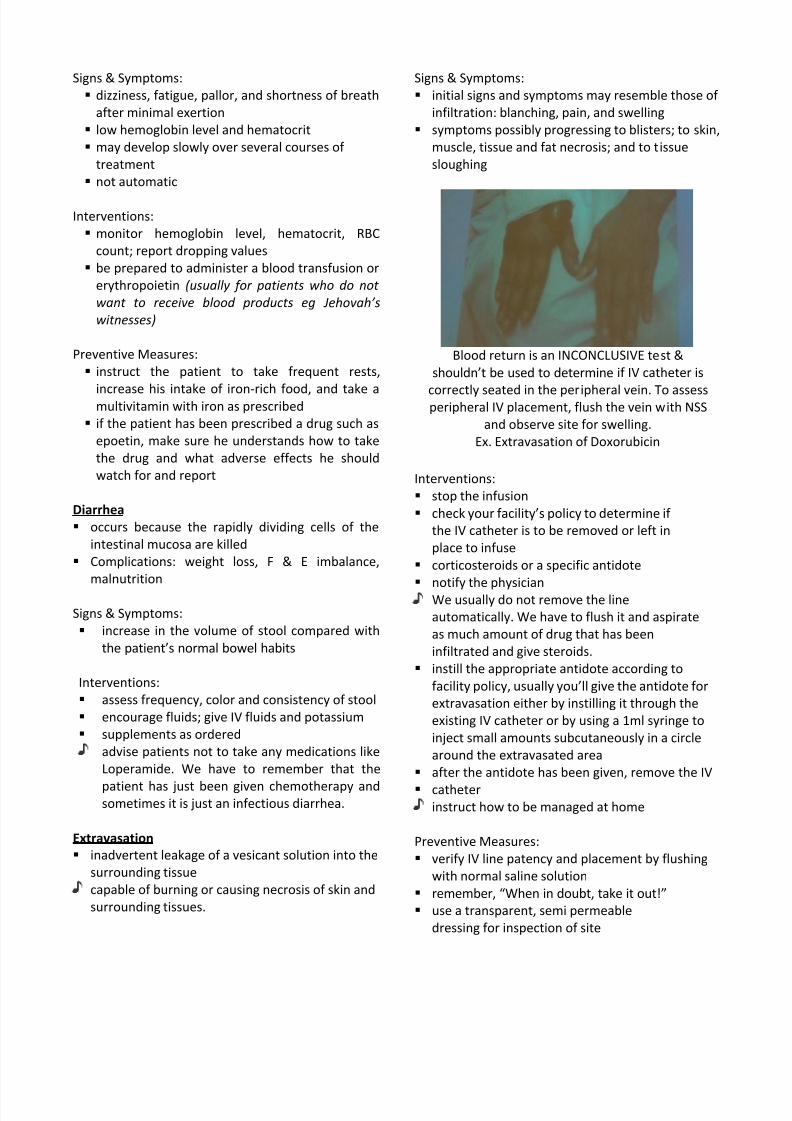
Lung Cancer Mutation Consortium:
Single Driver Mutations in NSCLC
Mutation found in 54% of tumors completely tested.
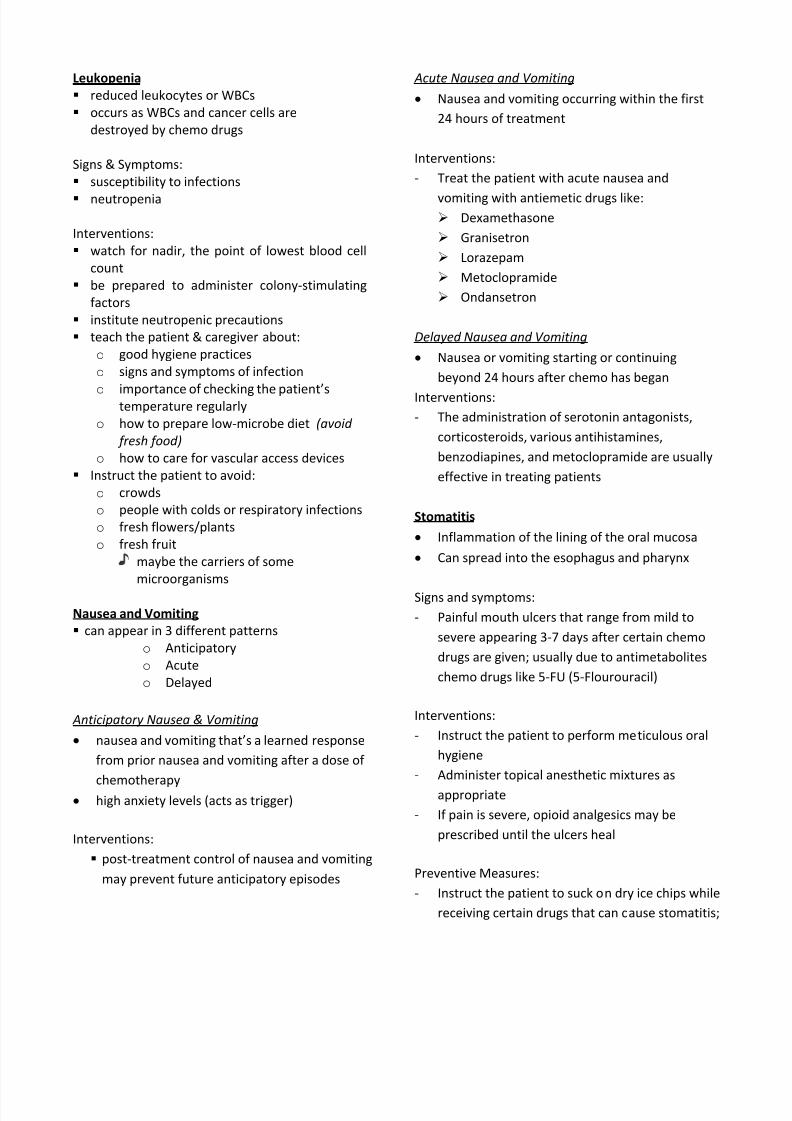
EGFR Expression
Immunohistochemical staining is used to check
for EGFR expression.
Targeted Agents
Drug
Classification
Targeted Agent Target
Receptor
Tyrosine
Kinase
Inhibitor
Gefitinib
(Iressa)
Eriotinib
(Tarceva)
TKI
TKI
The patient must be positive for mutation to use
these two drugs. They are very expensive.
The most common side effect of Tarceva is rash.
Advise patient to use sunblock and protective
devices.
The more rash there is, the better the response
to the drug.
Any tumor beyond 3mm cannot grow without a
blood supply. They make their own blood vesselsby secreting VEGF (Strong compound produced
by the tumor that encourages the formation of
new blood vessels). This is the target of
Bevacizumab and Avastin (anti-VEGF).
HANDLING COMPLICATIONS of CHEMOTHERAPY
Alopecia
hair loss that occurs as chemotherapeutic drugs
destroy the rapidly growing cells of hair follicles
may be minimal or severe
occurs 2 to 3 weeks after treatment begins -
almost always temporary
Signs & Symptoms:
- hair loss that may include eyebrows, lashes, and
body hair
Interventions
minimize shock and distress by warning the
patient of this possibility
discuss with the patient why it occurs describe to the patient how much hair loss to
expect
emphasize to the patient the need for
appropriate head protection against sunburn
*very sensitive
inform the patient that new hair may be a
different texture or color
give the patients sufficient time to decide
whether to order a wig or to opt for other
measures
inform the patient that his scalp will becomesore at times due to follicles swelling
Anemia
occurs as chemo drugs destroy healthy cells and
cancer cells
RBCs are destroyed and can’t be replaced by the
bone marrow not able to recover
7/27/2019 Combined Modality Multidisciplinary Approach to Cancer Treatment
http://slidepdf.com/reader/full/combined-modality-multidisciplinary-approach-to-cancer-treatment 5/9
Signs & Symptoms:
dizziness, fatigue, pallor, and shortness of breath
after minimal exertion
low hemoglobin level and hematocrit
may develop slowly over several courses of
treatment
not automatic
Interventions:
monitor hemoglobin level, hematocrit, RBC
count; report dropping values
be prepared to administer a blood transfusion or
erythropoietin (usually for patients who do not
want to receive blood products eg Jehovah’s
witnesses)
Preventive Measures:
instruct the patient to take frequent rests,
increase his intake of iron-rich food, and take amultivitamin with iron as prescribed
if the patient has been prescribed a drug such as
epoetin, make sure he understands how to take
the drug and what adverse effects he should
watch for and report
Diarrhea
occurs because the rapidly dividing cells of the
intestinal mucosa are killed
Complications: weight loss, F & E imbalance,
malnutrition
Signs & Symptoms:
increase in the volume of stool compared with
the patient’s normal bowel habits
Interventions:
assess frequency, color and consistency of stool
encourage fluids; give IV fluids and potassium
supplements as ordered
advise patients not to take any medications like
Loperamide. We have to remember that the
patient has just been given chemotherapy andsometimes it is just an infectious diarrhea.
Extravasation
inadvertent leakage of a vesicant solution into the
surrounding tissue
capable of burning or causing necrosis of skin and
surrounding tissues.
Signs & Symptoms:
initial signs and symptoms may resemble those of
infiltration: blanching, pain, and swelling
symptoms possibly progressing to blisters; to skin,
muscle, tissue and fat necrosis; and to tissue
sloughing
Blood return is an INCONCLUSIVE test &
shouldn’t be used to determine if IV catheter is
correctly seated in the peripheral vein. To assessperipheral IV placement, flush the vein with NSS
and observe site for swelling.
Ex. Extravasation of Doxorubicin
Interventions:
stop the infusion
check your facility’s policy to determine if
the IV catheter is to be removed or left in
place to infuse
corticosteroids or a specific antidote
notify the physicianWe usually do not remove the line
automatically. We have to flush it and aspirate
as much amount of drug that has been
infiltrated and give steroids.
instill the appropriate antidote according to
facility policy, usually you’ll give the antidote for
extravasation either by instilling it through the
existing IV catheter or by using a 1ml syringe to
inject small amounts subcutaneously in a circle
around the extravasated area
after the antidote has been given, remove the IV
catheterinstruct how to be managed at home
Preventive Measures:
verify IV line patency and placement by flushing
with normal saline solution
remember, “When in doubt, take it out!”
use a transparent, semi permeable
dressing for inspection of site
7/27/2019 Combined Modality Multidisciplinary Approach to Cancer Treatment
http://slidepdf.com/reader/full/combined-modality-multidisciplinary-approach-to-cancer-treatment 6/9
Leukopenia
reduced leukocytes or WBCs
occurs as WBCs and cancer cells are
destroyed by chemo drugs
Signs & Symptoms:
susceptibility to infections
neutropenia
Interventions:
watch for nadir, the point of lowest blood cell
count
be prepared to administer colony-stimulating
factors
institute neutropenic precautions
teach the patient & caregiver about:
o good hygiene practices
o signs and symptoms of infection
o importance of checking the patient’stemperature regularly
o how to prepare low-microbe diet (avoid
fresh food)
o how to care for vascular access devices
Instruct the patient to avoid:
o crowds
o people with colds or respiratory infections
o fresh flowers/plants
o fresh fruit
maybe the carriers of some
microorganisms
Nausea and Vomiting
can appear in 3 different patterns
o Anticipatory
o Acute
o Delayed
Anticipatory Nausea & Vomiting
nausea and vomiting that’s a learned response
from prior nausea and vomiting after a dose of
chemotherapy high anxiety levels (acts as trigger)
Interventions:
post-treatment control of nausea and vomiting
may prevent future anticipatory episodes
Acute Nausea and Vomiting
Nausea and vomiting occurring within the first
24 hours of treatment
Interventions:
- Treat the patient with acute nausea and
vomiting with antiemetic drugs like: Dexamethasone
Granisetron
Lorazepam
Metoclopramide
Ondansetron
Delayed Nausea and Vomiting
Nausea or vomiting starting or continuing
beyond 24 hours after chemo has began
Interventions:
- The administration of serotonin antagonists,
corticosteroids, various antihistamines,
benzodiapines, and metoclopramide are usually
effective in treating patients
Stomatitis
Inflammation of the lining of the oral mucosa
Can spread into the esophagus and pharynx
Signs and symptoms:
- Painful mouth ulcers that range from mild to
severe appearing 3-7 days after certain chemo
drugs are given; usually due to antimetabolites
chemo drugs like 5-FU (5-Flourouracil)
Interventions:
- Instruct the patient to perform meticulous oral
hygiene
- Administer topical anesthetic mixtures as
appropriate
- If pain is severe, opioid analgesics may be
prescribed until the ulcers heal
Preventive Measures:
- Instruct the patient to suck on dry ice chips while
receiving certain drugs that can cause stomatitis;
7/27/2019 Combined Modality Multidisciplinary Approach to Cancer Treatment
http://slidepdf.com/reader/full/combined-modality-multidisciplinary-approach-to-cancer-treatment 7/9
this decreases the blood supply to the mouth,
thus decreasing ulcer formation
Thrombocytopenia
Decrease platelet count, prone to bleeding
Signs and symptoms:- Bleeding gums
- Coffee-ground emesis
- Hematuria
- Hypermnorrhea
- Increased bruising
- Petechiae
- Tarry stools
Interventions:
- Monitor patient’s platelet count, critical point:
20,000 cell/mm
- Avoid unnecessary IM injections or venipuncture
- If an IM injection is necessary, apply pressure to
the site for at least 5mins, pressure dressing
- Instruct the patient to:
Avoid cuts and bruises
Shave with electric razor
Avoid blowing his nose
Stay away from irritants that would trigger
sneezing
Avoid using rectal thermometers
- Instruct the patient to report sudden headaches
(which could indicate potentially fatal
intracranial bleed)
PALLIATIVE CARE
An approach that improves the quality of life of
patients and family facing the problem
associated with life threatening illness, through
the prevention and relief of suffering by means
of early identification and impeccable
assessment and treatment of pain and other
problems, physical, psychological and spiritual.
Is applicable early in the course of illness, in
conjunction with other therapies that are
intended to prolong life such as chemo or
radiation therapy
Palliative Management
1. Medical management
2. Pain Management
3. Nutritional management4. Lung cancer counseling and support groups
5. Issues on death and dying
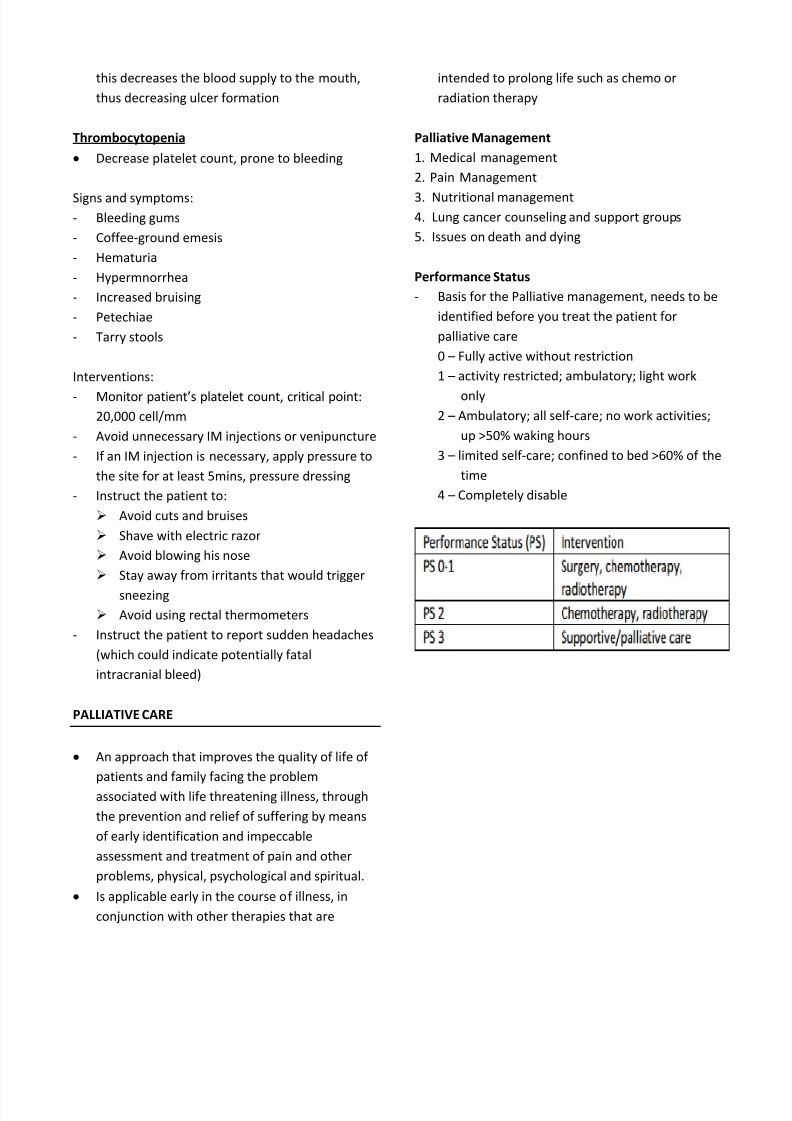
Performance Status
- Basis for the Palliative management, needs to be
identified before you treat the patient for
palliative care
0 – Fully active without restriction
1 – activity restricted; ambulatory; light work
only
2 – Ambulatory; all self-care; no work activities;
up >50% waking hours
3 – limited self-care; confined to bed >60% of the
time
4 – Completely disable
7/27/2019 Combined Modality Multidisciplinary Approach to Cancer Treatment
http://slidepdf.com/reader/full/combined-modality-multidisciplinary-approach-to-cancer-treatment 8/9
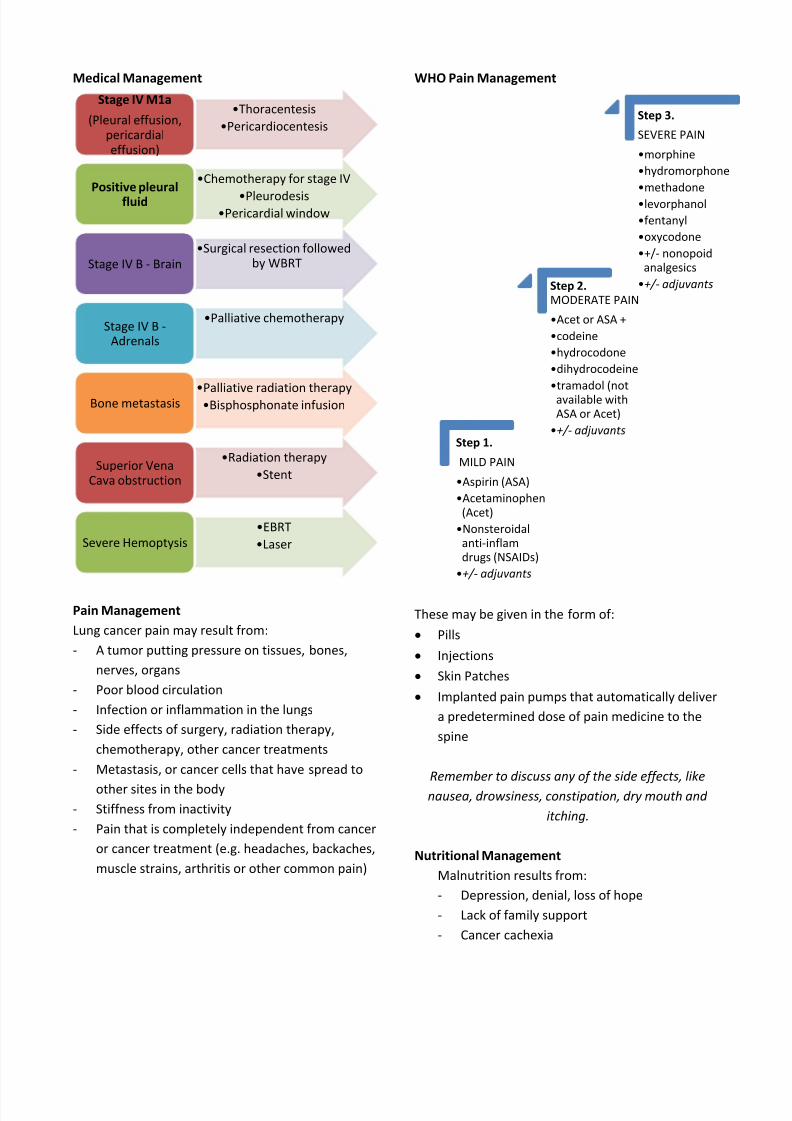
Step 1.
MILD PAIN
•Aspirin (ASA)
•Acetaminophen(Acet)
•Nonsteroidalanti-inflamdrugs (NSAIDs)
•+/- adjuvants
Step 2.MODERATE PAIN
•Acet or ASA +
•codeine
•hydrocodone
•dihydrocodeine
•tramadol (notavailable withASA or Acet)
•+/- adjuvants
Step 3.
SEVERE PAIN
•morphine
•hydromorphone
•methadone
•levorphanol
•fentanyl
•oxycodone
•+/- nonopoidanalgesics
•+/- adjuvants
Medical Management
Pain Management
Lung cancer pain may result from:
- A tumor putting pressure on tissues, bones,
nerves, organs
- Poor blood circulation
- Infection or inflammation in the lungs
- Side effects of surgery, radiation therapy,
chemotherapy, other cancer treatments
- Metastasis, or cancer cells that have spread to
other sites in the body
- Stiffness from inactivity
- Pain that is completely independent from cancer
or cancer treatment (e.g. headaches, backaches,
muscle strains, arthritis or other common pain)
WHO Pain Management
These may be given in the form of:
Pills
Injections
Skin Patches
Implanted pain pumps that automatically deliver
a predetermined dose of pain medicine to the
spine
Remember to discuss any of the side effects, like
nausea, drowsiness, constipation, dry mouth and
itching.
Nutritional Management
Malnutrition results from:
- Depression, denial, loss of hope
- Lack of family support
- Cancer cachexia
•Thoracentesis
•Pericardiocentesis
Stage IV M1a
(Pleural effusion,pericardialeffusion)
•Chemotherapy for stage IV
•Pleurodesis•Pericardial window
Positive pleuralfluid
•Surgical resection followedby WBRTStage IV B - Brain
•Palliative chemotherapyStage IV B -
Adrenals
•Palliative radiation therapy•Bisphosphonate infusionBone metastasis
•Radiation therapy
•StentSuperior Vena
Cava obstruction
•EBRT
•LaserSevere Hemoptysis
7/27/2019 Combined Modality Multidisciplinary Approach to Cancer Treatment
http://slidepdf.com/reader/full/combined-modality-multidisciplinary-approach-to-cancer-treatment 9/9
- Signs and symptoms of lung cancer
- Side of effects of treatment
Modes of Nutrition:
o Enteral
o Parenteral
o Feeding tubes
Death and Dying
Grief Stage Terminally Ill Patient
Response
Denial This can’t be happening
to me!
Anger Why is this happening to
me?
Bargaining I promise I’ll be a better
person if…
Depression I don’t care anymore.
Acceptance I’m ready for whatever
comes.
Months to year/years
1. Encourage designation of health care
2. Explore fears about dying and address
3. Assess decision making capacity and surrogate
decision maker
4. Initiate discussion of personal values and
preference for end of life care
5. Initiate discussion of palliative care option
Days to weeks
1. Implement and ensure compliance with advance
care plan
2. Clarify and confirm patient’s decision about life
sustaining treatment including CPR
Notes by: Catague R, Dizor J, Sameon N