cochlear implant lecture3 - rice universitybioewhit/courses/bioe592/mat/oghalai/lecture... · 1...
TRANSCRIPT

1
Cochlear ImplantsJohn S. Oghalai, MD
Division of Otology, Neurotology, and Skull Base SurgeryDept. of Otorhinolaryngology & Communicative Sciences
• Hearing allows us to be conscious of what goes on around us
• Always “working” to warn us of danger• Hearing allows communication• Hearing loss affects 28 million Americans
(1/10)• Isolation from society
Background
Frequency GradientHigh Low
Sound Propagation in theInner Ear

2
All Hair Cells Have Two FunctionsMechano-Electrical Transduction
Neurotransmission
Outer Hair Cells Carry OutElectro-Mechanical Transduction Passive Cochlear Model
• Mass• Stiffness• Damping
Mechanical models
Filtering
Passive
Frequency
Active Sensorineural Hearing Loss
• Mechanisms of sensorineural hearing loss– Congenital malformations (otic capsule
may or may not be involved)– Stria vascularis– Spiral ganglion cells– Organ of Corti / hair cells
• Presbyacusis (age- related hearing loss)• Noise- induced hearing loss
Loss of OHCs(12,000 max)

3
Normal Cochlea
AuditoryNerve
HairCells
Hearing-Impaired Apex
Scala Vestibuli
Spiral Ganglion
Organ ofCorti
(Hair Cells)
Bipolar Contacts
Auditory Nerve
Oval Window
Round Window
Electrode
Central Rib
BaseCochleostomy(scala tympani)
ClarionTM
Cochlear Implant
Common Components of all Cochlear Implant Systems
Microphone & Cable
Speech Processor
Antenna/Transmitter
Receiver/Stimulator
Electrode Array
Nucleus 3 system
1
Sound enters microphone on headpiece
2
Sound travels down cable to processor
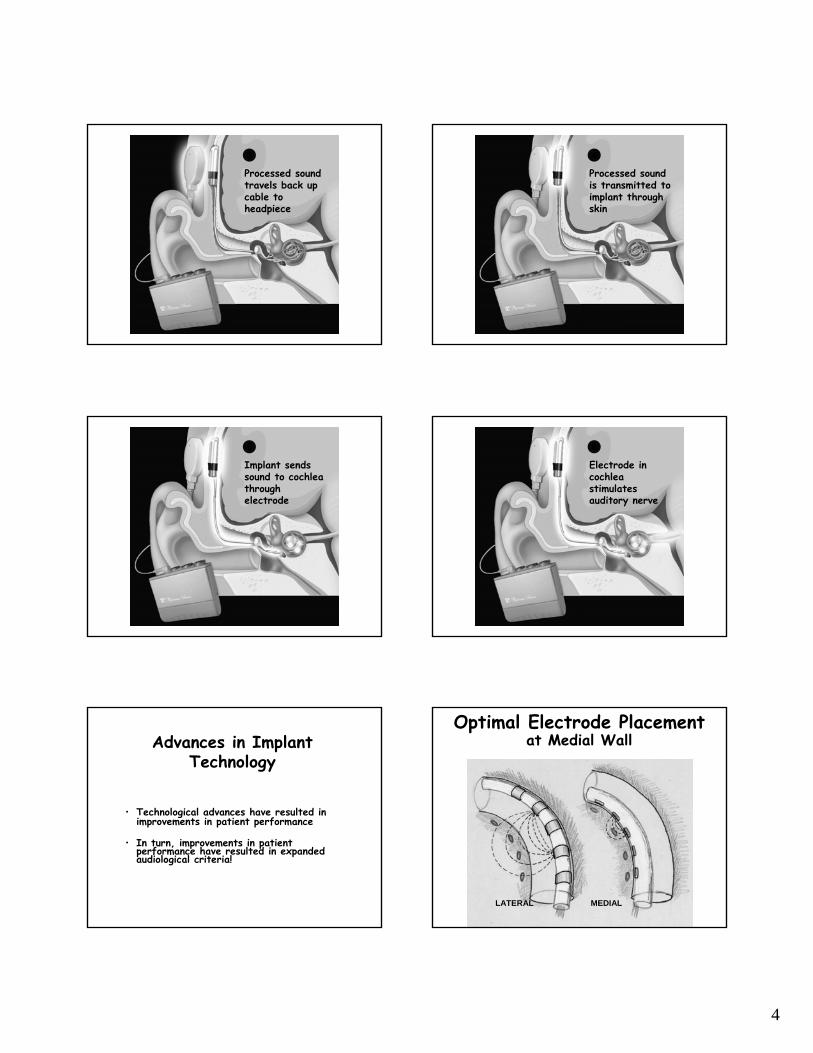
4
3
Processed sound travels back up cable to headpiece
4
Processed sound is transmitted to implant through skin
5
Implant sends sound to cochlea through electrode
6
Electrode in cochlea stimulates auditory nerve
Advances in Implant Technology
• Technological advances have resulted in improvements in patient performance
• In turn, improvements in patient performance have resulted in expanded audiological criteria!
Optimal Electrode Placementat Medial Wall
LATERAL MEDIAL

5
Advances in Electrode Design
Spiral Electrode(1990)
Spiral Electrode with Positioning System (EPS)
(1998)
HiFocus Electrode with Positioning System (EPS)
(1999)
CLARION & POSITIONER17 mm insertion 630º
CLARION ELECTRODE 24 mm insertion 500º
Design changes implemented so that the electrode closely hug the modiolus
Positioner
Mean Most Comfortable LevelsThree Electrode ConfigurationsMonopolar Pulsatile Stimulation
100
150
200
250
300
350
400
1 2 3 4 5 6 7 8Channel Number
Clin
ical
Uni
ts
Spiral alone at3 months(n=51)
Spiral + EPS at1 month (n=20)
HiFocus+EPSat 1 month(n=34)
Nucleus Contour ElectrodeStylet in place
Stylet removed
K117L, 12.5 mm el. #1
Insertion trauma: K117L, 11.5 mm el. #2Insertion trauma: K117L, 11.5 mm el. #2
SGSG
SGSGOSLOSL
Slide from Pat Leake, UCSF
SpLSpL
RMRM
ContourContourTM
ElectrodeElectrodeSpGSpG
OSLOSL
OticOticcapsulecapsule
Slide from Pat Leake, UCSF
SpGSpG
OSLOSL
ElectrodeElectrode
Sc Sc TymTym
Sc VestSc Vest
Slide from Pat Leake, UCSF

6
SpLSpLRMRM
ElectrodeElectrode
PositionerPositioner
OSLOSL
SpGSpGHiFocusHiFocus
OticOticCapsuleCapsule
Slide from Pat Leake, UCSF
External Equipment
Speech Processors• Automatic, Continuous
Functionality Check of All External and Internal Components
• Multiple Indicator Lights
• Programmable Acoustic Alarm
• ESD Resistant• Easy to Adjust Controls
> Built-in microphone tester
> Multiple Signal-to-Noise ratio options for FM/Accessories
“mini-computer”
BTE Sound Processor
8 Runs all processing strategies plus new ones under development
8 Rechargeable batteries for low operating cost
8 Compatible with all CLARION internal implants
8 Same functionality as Body worn PSP, except no warning lights/alarms
8 Check functionality with Sensor
Clarion
Nucleus
CLARION Sound Processor Development
13
100
S-Series Platinum Series & BTE
Million Instructions Per Second (MIPS)
Continuous Two-Way Telemetry
• Ongoing monitoring achieved with two distinct carrier frequencies
• Normal concurrent signal operation
• Benefit for children who are unable to communicate
Power & Data
BackTelemetry
Headpiece ICS
SP Status Indicator

7
Input Dynamic Range (IDR)
•The normal ear captures widely fluctuating speech intensities ranging over 50 dB as well as speech from talkers when they are far away or speaking softly•CLARION captures the widest range of incoming sounds through its electronics and software
CLARION60 dB IDR
Industry norm
30 dB IDRNormal
Hearing120 dB
50 dBPeaks
& Valleysof Speech
30
90
70
50
““Narrowed” IDR (30 dB)Narrowed” IDR (30 dB)Perceptual D
R (Perceptual D
R ( uAuA))
Soun
d Pr
essu
re L
evel (dB
SPL
)So
und
Pres
sure
Lev
el (dB
SPL
)
IDR T
M
AGCAGC
Speech ProcessorSpeech Processor ElectrodeElectrode
30
90
70
50
““Widened” IDR (60 dB)Widened” IDR (60 dB)
Perceptual DR (
Perceptual DR ( uAuA
))
Soun
d Pr
essu
re L
evel (dB
SPL
)So
und
Pres
sure
Lev
el (dB
SPL
)
IDR
T
M
AGCAGC
Speech ProcessorSpeech Processor ElectrodeElectrode
Acoustic Signal
Pass band 1 Envelope Compression Ch 1
Pulse Train Carrier
Pass band 2 Envelope Compression Ch 2
Pass band N Envelope Compression Ch N
AGC & Low Pass
high
low
mid
BTE Decals
Six inter-changeable color headpiece caps
Nucleus

8
Speech Processing
Speech Spectrum
S e n t e n ce
Spectral Resolution (Number of Channels)
• Most important factor is the number of spectral channels of information– number of distinct pitch channels
• Number of effective channels is not the same as the number of electrodes
9
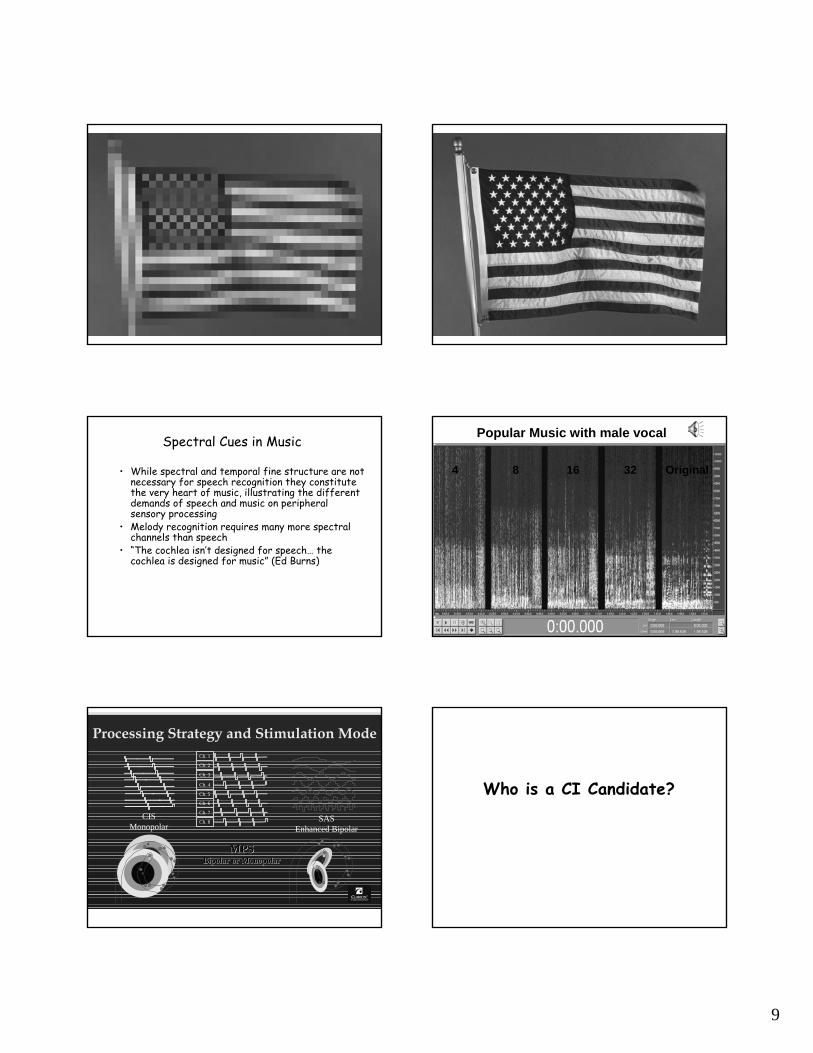
Spectral Cues in Music
• While spectral and temporal fine structure are not necessary for speech recognition they constitute the very heart of music, illustrating the different demands of speech and music on peripheral sensory processing
• Melody recognition requires many more spectral channels than speech
• “The cochlea isn’t designed for speech… the cochlea is designed for music” (Ed Burns)
4 8 16 32 Original
Popular Music with male vocal
Processing Strategy and Stimulation Mode
CISMonopolar
SASEnhanced Bipolar
Ch. 1
Ch. 2
Ch. 3
Ch. 4
Ch. 5
Ch. 7
Ch. 8
Ch. 6
MPSMPSBipolar or MonopolarBipolar or Monopolar
Who is a CI Candidate?

10
Who Should Get a Cochlear Implant? Children
• Children aged 12 mos-17 years
• Profound sensorineural hearing loss of 90 dB or greater in both ears (No Response ABR)
• Lack of benefit from high powered hearing aids – 3-6 month Required Hearing Aid Trial– < 2 on Questions 3, 5, & 6 on the IT-MAIS
Questionnaire• Older child (>6yrs): Some auditory skills
• 0-20% on tests of open-set word recognition (PB-K or MLNT)
Don’t Wait! The Younger the Better!
Who Should Get a Cochlear Implant? Children
• Rehabilitative or educational setting where development of listening and speaking skills are emphasized
• Positive family environment where device use through listening and speaking is encouraged
Adults Who Should Get a Cochlear Implant?
• Healthy adult over 18 years of age, no upper age limit
• Severe-Profound sensorineural hearing loss of 70 dB or greater in both ears
• Postlingual onset of deafness (after age 6 yrs)• Prelingual adults that are members of the hearing
community (lip readers, verbal intent)• Lack of benefit from hearing aids
– HINT Sentence score < 50%
Adult Referral Criteria
• PTA of >70dB in Both Ears
• Monosyllabic Word score of < 30% in Both Ears
Audiological Measurement:CI Candidate?
250 500 1000750 1500 2000 4000 6000 8000-10
01020304050
Hz
60708090
100110120
dB
X XX
XXX
86 Yr. Old AdultPTA=103dB ASPTA=105dB ADCNC Words:=0% AS =0% AD
O
OO
OO
O
X
CI CI CI CI CI
YESAudiological Measurement:
CI Candidate?
250 500 1000750 1500 2000 4000 6000 8000-10
01020304050
Hz
60708090
100110120
dB
X
X
XX
X
X
56 Yr. Old AdultPTA=83dB AS
PTA=75dB ADCNC Words
=12% AS =16% AD
O
OOO
O
O
X
XO
YES
11
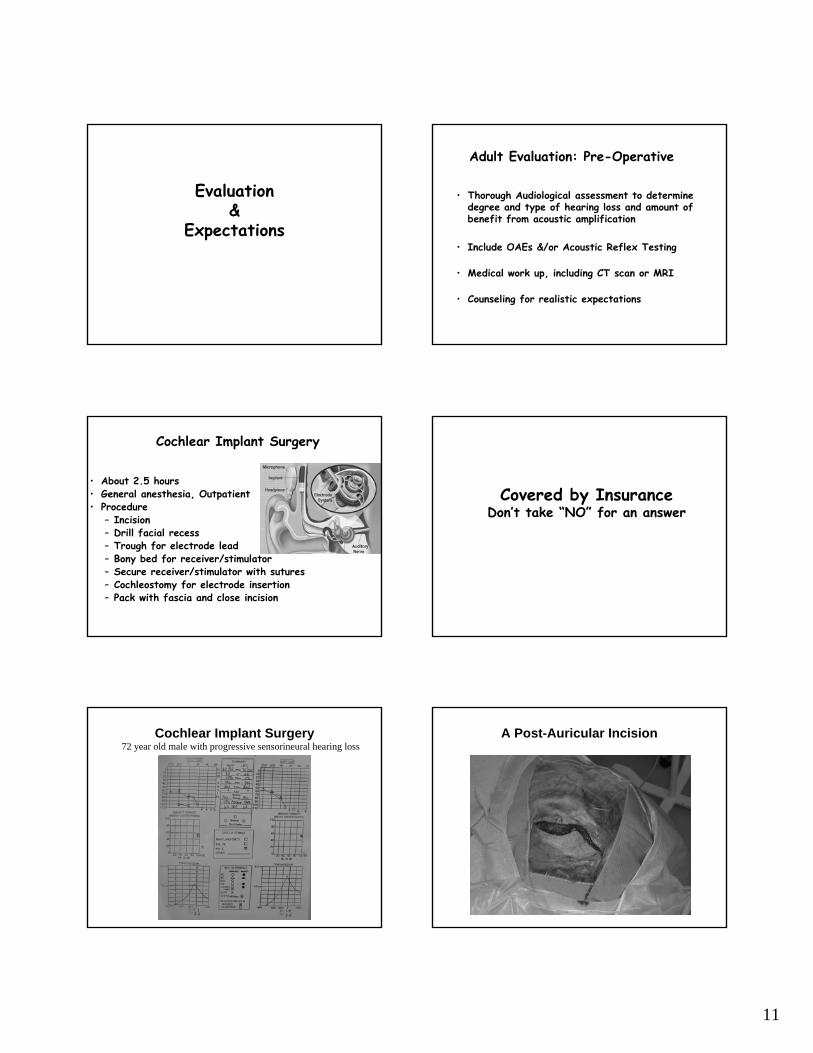
Evaluation &
Expectations
Adult Evaluation: Pre-Operative
• Thorough Audiological assessment to determine degree and type of hearing loss and amount of benefit from acoustic amplification
• Include OAEs &/or Acoustic Reflex Testing
• Medical work up, including CT scan or MRI
• Counseling for realistic expectations
Cochlear Implant Surgery
• About 2.5 hours• General anesthesia, Outpatient• Procedure
– Incision– Drill facial recess– Trough for electrode lead– Bony bed for receiver/stimulator– Secure receiver/stimulator with sutures– Cochleostomy for electrode insertion– Pack with fascia and close incision
Covered by InsuranceDon’t take “NO” for an answer
Cochlear Implant Surgery72 year old male with progressive sensorineural hearing loss
A Post-Auricular Incision

12
Exposure of the Mastoid Cortex Drilling the Mastoid and Countersinking the Implant
Securing the Implant The Facial Recess
Stapes
Round Window
Facial Nerve
LateralSCC
Incus
Placement of the Electrode Complications
• Hearing loss - in everyone– New techniques to reduce HL
• Variable outcomes • Chorda tympani nerve injury
COMMON
•Infections - uncommon•Flap necrosis - uncommon•Tinnitus & Imbalance - usually self limited •Facial nerve injury - congenital abnormality•MENINGITIS - a problem of mythic
proportions
UNCOMMON

13
Risk factors for meningitis
Inner Ear MalformationsPrior history of meningitisYoung children (esp.< 5 yrs).Otitis mediaImmune dysfunctionPrior ear surgery
Meningitis in Cochlear Implantation
• 91 people worldwide (N=60,000)• 17 deaths• 53 US cases (N= 25,000)
– Ages 18 mos to 84 yrs; Most under 7 years of age (n=33)
– Signs and Sx <24hrs to >6 yrs– 50% developed meningitis < 1 year postop
(N=32)– 29 Advanced Bionics CLARION (1996;N=7500) – 22 Cochlear Nucleus (1985; N=16,500)– 2 MED-EL (2001; N=770)
Design Flaws?
• Higher incidence with Clarion positioner
• Removed from the market
• HF1 electrode now available without the positioner
Positioner
Post-Operative Evaluations:Device Fitting and Follow-up
• Initial stimulation: 3-6 weeks post surgery
• Adjustments made regularly based on feedback from patients, parents, therapists and educators
• Speech perception evaluations semi-annually to annually
Evolution of Implant Outcomes
• Single-channel implants• Sound detection, perception of speech
rhythm, lipreading enhancement
• First generation multichannel implants• Closed-set word identification, some
open-set sentence recognition; poor open-set word recognition
Current Expectations
• Sound Field thresholds 20-45dB @ 250-6K Hz
• Cannot return to Hearing Aid in implanted ear
• >80% Postlingual Adults use the telephone
• >50% of Postlingual Adults enjoy music
• Near peak performance by 3 months!

14
Open-Set Speech RecognitionN=56 Postlinguistic Patients
Six-Month Scores
* Note: Only patients who score > 20% on HINT Sentences in quiet are administeredHINT Sentences in noise.
3%13%11%
20%
44%
57%
71%
35%
79%
40%51%
67%
47%
73%
52%
81%
0%
20%
40%
60%
80%
100%
CNC Words CID Sentences HINT in Quiet HINT +10 S/N*
Perc
ent C
orre
ct
Pre1Month3Month6Month
Individual CNC Word Scores at 3 Monthsand Duration of Deafness (n= 67)
High levels of CNC word recognition were achieved by patients with long as well as short duration of deafness.
0%10%20%30%40%50%60%70%80%90%
100%
0 0 1 1 1 1 2 2 2 2 2 3 3 3 6 6 7 7 8 10 12 12 15 17 20 20 21 26 26 28 30 38 43 58
Years of Deafness - Implanted Ear
Perc
ent C
orre
ct
0 00
Mean = 40% Median = 42%
Individual CNC Word Scores at 3 Monthsand Age at Implant (n=67)
31% of the sample was implanted at > 70 years of age. Some of these older patients show high levels of word recognition at three months. Others may require more implant experience before they demonstrate open-set word recognition abilities.
0%10%20%30%40%50%60%70%80%90%
100%
22 26 28 33 39 40 43 45 46 49 50 52 53 55 56 59 60 61 62 63 65 68 69 71 73 73 75 75 76 78 80 82 84 88
Age at Implant (Years)
Perc
ent C
orre
ct
00 0
Mean = 40% Median = 42%
SPIRAL GANGLION CELL DEGENERATIONFOLLOWING NEONATAL DEAFNESS
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12
Duration of Deafness (months or years)
< 1 year n = 56
r2 = 0.83 p<0.001
61 2 3 4 5 7
> 2 years n = 11 (6 cats)
Gan
glio
n C
ell D
ensi
ty (
% n
orm
al)
Slide from Pat Leake, UCSF
K117 L, GM1 Stimulated: K117 L, GM1 Stimulated: 5 mm, SG = 80% of normal5 mm, SG = 80% of normal
K117R, GM1 Deafened Control:K117R, GM1 Deafened Control:5 mm, SG = 40% of normal5 mm, SG = 40% of normal
Slide from Pat Leake, UCSF
Why Research Cochlear Implant Alternatives?
• Outcomes with a cochlear implant are good… but not as good as normal hearing
• Cochlear implants can not be used for mild or moderate levels of hearing loss

15
-10
0
10
20
30
40
50
60
70
80
90
100
110
120
125 250 500 1000 2000 4000 8000
FREQUENCY IN HERTZ
HEA
RIN
G L
EVEL
IN d
B(A
NSI
- 19
96)
750 1500 3000 6000
-10
0
10
20
30
40
50
60
70
80
90
100
110
120
125 250 500 1000 2000 4000 8000
FREQUENCY IN HERTZ
HEA
RIN
G L
EVEL
IN d
B(A
NSI
- 19
96)
750 1500 3000 6000
Pie in the Sky? Modulation of Cochlear Mechanics• Drug therapy• Gene therapy• Physical
manipulations
1) Measure hearing with various cochlear potentials (CAP, DPOAES, CM, & EP)
2) Measure basilar membrane motion using laser doppler vibrometer (2 picometersensitivity)
Ventral Exposure of the Guinea Pig Cochlea Perfusion Technique
CanaliculaePerforantes
Research Implications:Developing a Treatment for Cochlear Hearing Loss
• Techniques for performing surgery of the inner ear• Potential surgical objectives:
– Change mass, stiffness, or damping of organ of Corti• Laser• Physical manipulations
– Drug therapy • Modulate outer hair cell electromotility• Modulate stereociliary transduction
– Genetic manipulations:• Insert exogenous motor proteins (prestin)• Modulate tectorial membrane passive mechanics
– Electronic device implantation (bionic OHC’s)
16
Baylor College of MedicineChul-Hee Choi, Ph.D.Gentiana Wenzel, M.D.Anping Xia, M.D., Ph.D.Nicola Schug, M.S.
William E. Brownell, Ph.D.Ruth Anne Eatock, Ph.D.Fred Pereira, Ph.D.Peter Saggau, Ph.D.
University of California – San FranciscoPat A. Leake, Ph.D.Russell Snyder, Ph.D.
New York UniversityAnil K. Lalwani, M.D.
Stanford UniversityRobert K. Jackler, M.D.
Rice UniversityBahman Anvari, Ph.D.Robert Raphael, Ph.D.
Johns Hopkins UniversityAlex Spector, Ph.D
University of Tuebingen, GermanyMarkus Pfister, M.D., Ph.D.Nicola Schug, M.S.
National Institutes of HealthNational Organization for Hearing Research
Acknowledgments