clinical safety of fospropofol disodium during diagnostic and therapeutic procedures john b. leslie...
TRANSCRIPT

Clinical Safety of Fospropofol Clinical Safety of Fospropofol Disodium During Diagnostic and Disodium During Diagnostic and
Therapeutic ProceduresTherapeutic Procedures
John B. Leslie MD; Lawrence B. Cohen, MD; Gerard Silvestri, MD; Tong-J Gan, MDJohn B. Leslie MD; Lawrence B. Cohen, MD; Gerard Silvestri, MD; Tong-J Gan, MD

Fospropofol MetabolismFospropofol Metabolism(Enzymatic Liberation of Propofol)(Enzymatic Liberation of Propofol)
Fechner J, et al. Fechner J, et al. Anesthesiology.Anesthesiology. 2003;99:303-1313. 2003;99:303-1313.
• Alkaline phosphatases are widely distributed in bodyAlkaline phosphatases are widely distributed in body• Fospropofol disodium is rapFospropofol disodium is rapidly and completely metabolizedidly and completely metabolized• Phosphate, formaldehyde and formate do not accumulate above endogenous levelsPhosphate, formaldehyde and formate do not accumulate above endogenous levels
Fospropofol Fospropofol disodiumdisodium
alkalinealkaline
phosphatasephosphatase
PropofolPropofol FormaldehydeFormaldehyde PhosphatePhosphate
OHOH OO
HHHH OO
PP
OO
OOOOOO
OO
OO OO
OOPP
FormateFormate
OO
OOHH

FospropofolFospropofol Development Priority Development Priority
• Develop a “propofol experience” without the limitations of Develop a “propofol experience” without the limitations of current propofol administration restrictions and current propofol administration restrictions and minimization of propofol AEsminimization of propofol AEs
• Minimize sedation-related adverse eventsMinimize sedation-related adverse events– Limit peak effects from bolus injectionLimit peak effects from bolus injection
• Respiratory depressionRespiratory depression– Pain on injectionPain on injection– Expertise in dosing and titrationExpertise in dosing and titration
• Define a Dose-Specific routine for sedation routines in Define a Dose-Specific routine for sedation routines in specific clinical scenarios to minimize adverse events but specific clinical scenarios to minimize adverse events but provide “ideal outcomes”provide “ideal outcomes”
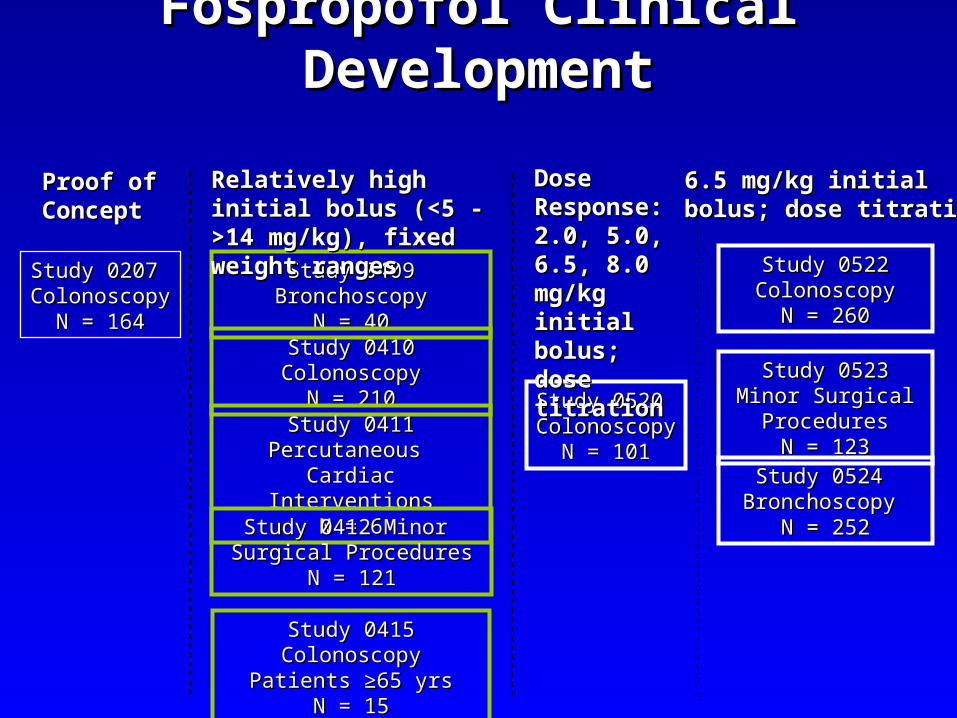
Fospropofol Clinical DevelopmentFospropofol Clinical Development
Study 0207 Study 0207 ColonoscopyColonoscopy
N = 164N = 164
Study 0409 BronchoscopyStudy 0409 BronchoscopyN = 40N = 40
Study 0410 ColonoscopyStudy 0410 ColonoscopyN = 210N = 210
Study 0411 Percutaneous Study 0411 Percutaneous Cardiac InterventionsCardiac Interventions
N = 6N = 6
Study 0412 Minor Study 0412 Minor Surgical ProceduresSurgical Procedures
N = 121N = 121
Study 0415 ColonoscopyStudy 0415 ColonoscopyPatients ≥65 yrsPatients ≥65 yrs
N = 15N = 15
Study 0520 Study 0520 ColonoscopyColonoscopy
N = 101N = 101
Study 0522 Study 0522 ColonoscopyColonoscopy
N = 260N = 260
Study 0523 Minor Study 0523 Minor Surgical ProceduresSurgical Procedures
N = 123N = 123
Study 0524 Study 0524 Bronchoscopy Bronchoscopy
N = 252N = 252
Proof ofProof ofConceptConcept
Relatively high initial Relatively high initial bolus (<5 - >14 mg/kg), bolus (<5 - >14 mg/kg), fixed weight rangesfixed weight ranges
DoseDoseResponse:Response:2.0, 5.0, 6.5, 2.0, 5.0, 6.5, 8.0 mg/kg 8.0 mg/kg initial bolus; initial bolus; dose titrationdose titration
6.5 mg/kg initial 6.5 mg/kg initial bolus; dose titrationbolus; dose titration

Fospropofol 6.5 mg/kg Titrated Fospropofol 6.5 mg/kg Titrated Bolus - Metabolism BenefitsBolus - Metabolism Benefits
• Well known, well characterized active moiety -- propofolWell known, well characterized active moiety -- propofol– Predictable PK/PD profile with slower onset & lower Predictable PK/PD profile with slower onset & lower
CCmaxmax compared to IV bolus propofol compared to IV bolus propofol
• Early fixed high-dose (>8 mg/kg) studies produced dose-Early fixed high-dose (>8 mg/kg) studies produced dose-related higher level of sedation-related adverse events related higher level of sedation-related adverse events (primarily respiratory)(primarily respiratory)
• Modified dose-titration routine with initial 6.5 mg/kg dose Modified dose-titration routine with initial 6.5 mg/kg dose and adjustments based on age, weight, and ASA status and adjustments based on age, weight, and ASA status implemented to minimize sedation-related AEs with implemented to minimize sedation-related AEs with optimal outcomesoptimal outcomes
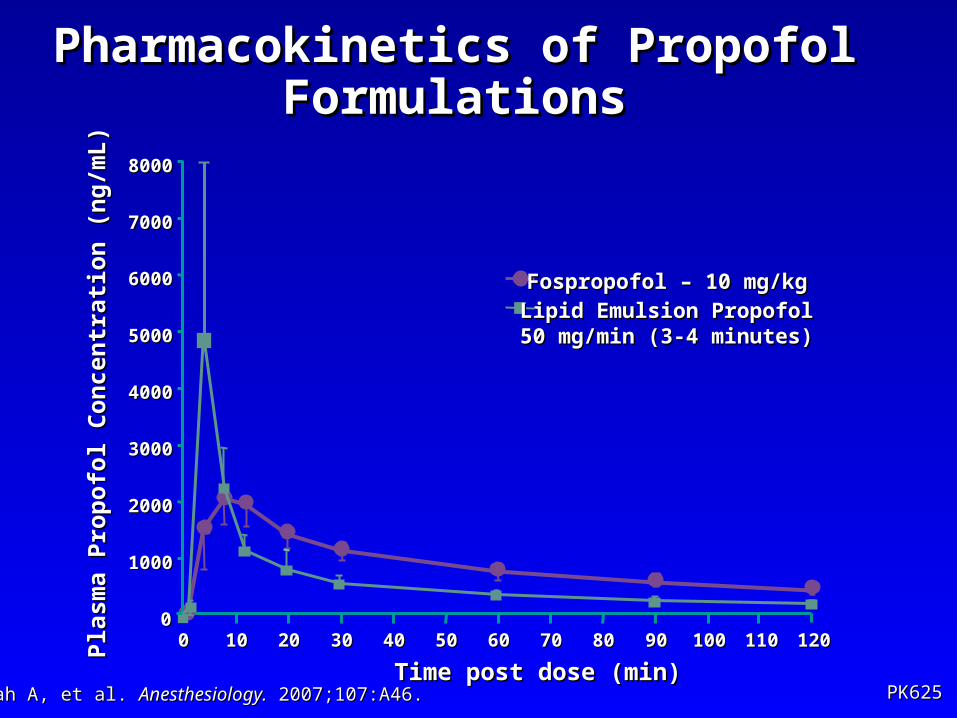
Pharmacokinetics of Propofol Pharmacokinetics of Propofol FormulationsFormulations
00
10001000
20002000
30003000
40004000
50005000
60006000
70007000
80008000
00 1010 2020 3030 4040 5050 6060 7070 8080 9090 100100 110110 120120
Time post dose (min)Time post dose (min)
Pla
sma
Pro
po
fol
Co
nce
ntr
atio
n (
ng
/mL
)P
lasm
a P
rop
ofo
l C
on
cen
trat
ion
(n
g/m
L)
PK625PK625
Fospropofol – 10 mg/kgFospropofol – 10 mg/kg
Shah A, et al. Shah A, et al. Anesthesiology.Anesthesiology. 2007;107:A46. 2007;107:A46.
Lipid Emulsion Propofol Lipid Emulsion Propofol 50 mg/min (3-4 minutes) 50 mg/min (3-4 minutes)
Metabolic Products of FospropofolMetabolic Products of Fospropofol(Enzymatic Liberation of Propofol)(Enzymatic Liberation of Propofol)
• The metabolic products of Fospropofol The metabolic products of Fospropofol breakdown: Formaldehyde, Formate, and breakdown: Formaldehyde, Formate, and Phosphate levels produced are not Phosphate levels produced are not clinically significant nor do they produce clinically significant nor do they produce drug or sedation-related adverse eventsdrug or sedation-related adverse events
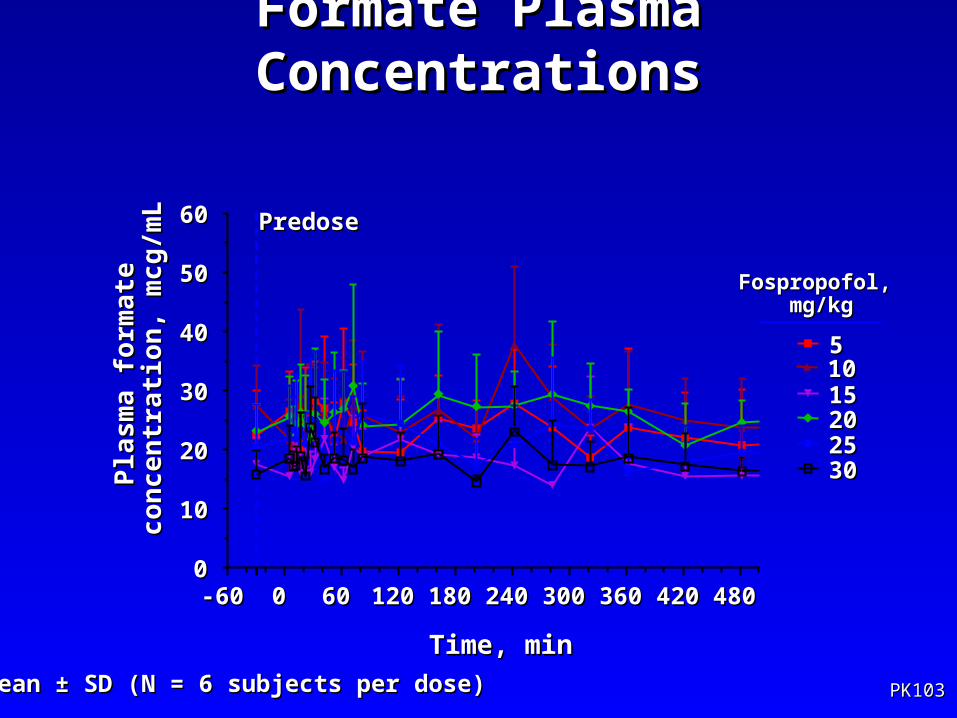
Formate Plasma ConcentrationsFormate Plasma Concentrations
PredosePredose
Fospropofol, Fospropofol, mg/kgmg/kg
Mean ±Mean ± SD (N = 6 subjects per dose)SD (N = 6 subjects per dose)
-60-60 00 6060 120120 180180 240240 300300 360360 420420 48048000
1010
2020
3030
4040
5050
6060
5510101515
25252020
3030
Time, minTime, min
Pla
sm
a fo
rmat
eP
las
ma
form
ate
co
nc
en
trat
ion
, mc
g/m
Lc
on
ce
ntr
atio
n, m
cg
/mL
PK103PK103
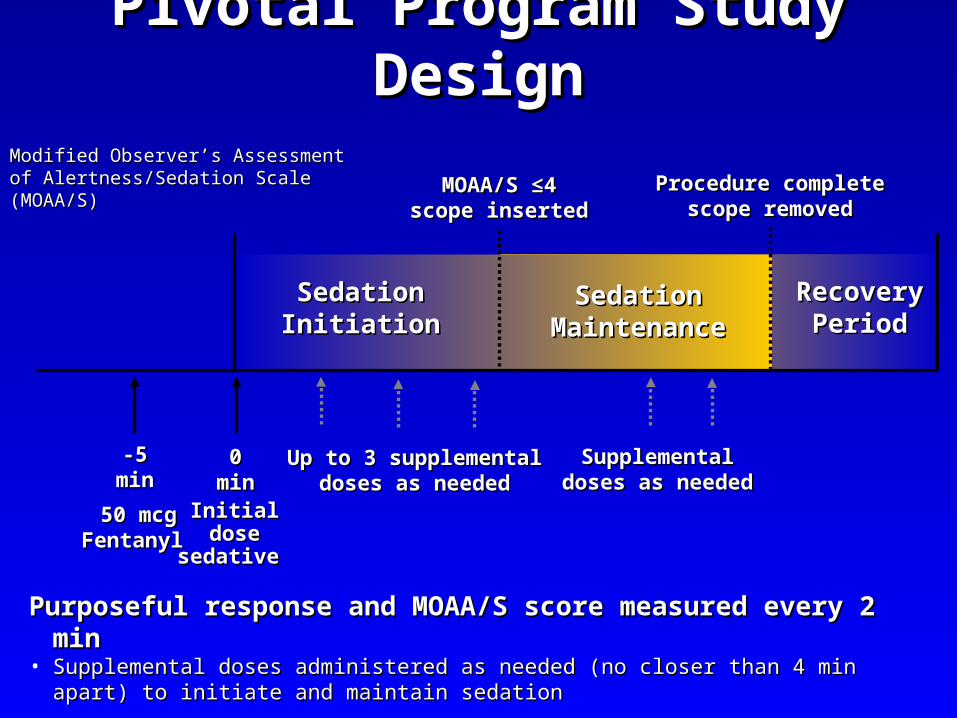
Pivotal Program Study DesignPivotal Program Study Design
Purposeful response and MOAA/S score measured every 2 minPurposeful response and MOAA/S score measured every 2 min• Supplemental doses administered as needed (no closer than 4 min apart) to initiate and Supplemental doses administered as needed (no closer than 4 min apart) to initiate and
maintain sedationmaintain sedation
MOAA/S MOAA/S ≤4≤4scope insertedscope inserted
Procedure completeProcedure completescope removedscope removed
SedationSedationInitiationInitiation
SedationSedationMaintenanceMaintenance
50 mcg50 mcgFentanylFentanyl
-5-5minmin
InitialInitialdosedose
sedativesedative
00minmin
Up to 3 supplementalUp to 3 supplementaldoses as neededdoses as needed
SupplementalSupplementaldoses as neededdoses as needed
RecoveryRecoveryPeriodPeriod
Modified Observer’s AssessmentModified Observer’s Assessmentof Alertness/Sedation Scale (MOAA/S)of Alertness/Sedation Scale (MOAA/S)

Patient Demographics by ProcedurePatient Demographics by Procedure
ColonoscopyColonoscopyN=183N=183
Minor Surgical Minor Surgical ProceduresProcedures
N=123N=123BronchoscopyBronchoscopy
N=149N=149
AgeAge 18 - 64 yrs18 - 64 yrs 157 (85.5)157 (85.5) 99 (80.5)99 (80.5) 89 (59.7)89 (59.7) ≥ ≥65 yrs65 yrs 26 (14.2)26 (14.2) 24 (19.5)24 (19.5) 60 (40.0)60 (40.0) ≥ ≥75 yrs**75 yrs** 4 (2.2)4 (2.2) 11 (8.9)11 (8.9) 19 (12.8)19 (12.8)GenderGender
MaleMale 87 (47.5)87 (47.5) 56 (45.5)56 (45.5) 85 (57.1)85 (57.1)WeightWeight <60 kg<60 kg 15 (8.2)15 (8.2) 18 (14.6)18 (14.6) 27 (18.1)27 (18.1) 60 - <90 kg60 - <90 kg 99 (54.1)99 (54.1) 69 (56.1)69 (56.1) 81 (54.4)81 (54.4)
≥ ≥90 kg90 kg 69 (37.7)69 (37.7) 36 (29.3)36 (29.3) 41 (27.5)41 (27.5)ASA statusASA status P1P1 68 (37.2)68 (37.2) 33 (26.8)33 (26.8) 7 (4.7)7 (4.7) P2P2 110 (60.1)110 (60.1) 67 (54.5)67 (54.5) 74 (49.6)74 (49.6) P3P3 5 (2.7)5 (2.7) 22 (17.9)22 (17.9) 61 (41.0)61 (41.0) P4P4 0 (0.0)0 (0.0) 1 (0.8)1 (0.8) 7 (4.7)7 (4.7)
Patients*, n (%)Patients*, n (%)
*6.5 mg/kg Dosage Regimen; COLO520, COLO522, MSURG523, BRONCH524*6.5 mg/kg Dosage Regimen; COLO520, COLO522, MSURG523, BRONCH524**Patients ≥ 75 yr are also included in ≥ 65 yr category**Patients ≥ 75 yr are also included in ≥ 65 yr category

Types of Minor Surgical Procedures at ProposedTypes of Minor Surgical Procedures at Proposed Dosage Regimen Dosage Regimen
Study 0523 Minor ProceduresStudy 0523 Minor Procedures
Fospropofol Fospropofol 6.5 mg/kg6.5 mg/kg
Duration of Duration of procedure, minprocedure, min
Procedure
Patients, n Patients, n (%)(%)
N = 123N = 123 MedianMedian MinMin MaxMax
EsophagogastroduodenoscopyEsophagogastroduodenoscopy 27 (22.0)27 (22.0) 44 22 2525
ArthroscopyArthroscopy 22 (17.9)22 (17.9) 17.517.5 1212 2626
HysteroscopyHysteroscopy 21 (17.1)21 (17.1) 1212 33 3131
BunionectomyBunionectomy 18 (14.6)18 (14.6) 43.543.5 2626 105105
Transesophageal Transesophageal echocardiogramechocardiogram
13 (10.6)13 (10.6) 1414 44 2626
UreteroscopyUreteroscopy 10 (8.1)10 (8.1) 1212 88 3232
LithotripsyLithotripsy 8 (6.5)8 (6.5) 29.529.5 2424 5656
Dilatation & CurettageDilatation & Curettage 3 (2.4)3 (2.4) 88 77 2626
Arteriovenous shuntArteriovenous shunt 1 (0.8)1 (0.8) 4545 –– ––

Exposure to fospropofol by Procedure Exposure to fospropofol by Procedure and Total Dose and Total Dose
(All Patients—All Studies)(All Patients—All Studies)Patients, n (%)Patients, n (%)
ProcedureProcedure ≤≤ 450 mg450 mg > 450 - 700 mg> 450 - 700 mg > 700 - 950 mg> 700 - 950 mg > 950 - 1200 mg> 950 - 1200 mg > 1200 mg> 1200 mg
Colonoscopy Colonoscopy (N = 750)(N = 750)
151 (20.1)151 (20.1) 116 (15.5)116 (15.5) 242 (32.3)242 (32.3) 194 (25.9)194 (25.9) 47 (6.3)47 (6.3)
Bronchoscopy Bronchoscopy (N = 292)(N = 292)
144 (49.3)144 (49.3) 73 (25.0)73 (25.0) 50 (17.1)50 (17.1) 19 (6.5)19 (6.5) 6 (2.1)6 (2.1)
Minor Minor procedures procedures (N = 250)(N = 250)
12 (4.8)12 (4.8) 51 (20.4)51 (20.4) 88 (35.2)88 (35.2) 75 (30.0)75 (30.0) 24 (9.6)24 (9.6)
Prolonged Prolonged exposure exposure (N = 46)(N = 46)
10 (21.7)10 (21.7) 5 (10.9)5 (10.9) 2 (4.3)2 (4.3) 3 (6.5)3 (6.5) 26 (56.5)26 (56.5)
Healthy Healthy volunteers volunteers (N = 273)(N = 273)
70 (25.6)70 (25.6) 38 (13.9)38 (13.9) 45 (16.5) 45 (16.5) 36 (13.2)36 (13.2) 84 (30.8)84 (30.8)
Total (N = 1611)Total (N = 1611) 387 (24.0)387 (24.0) 283 (17.6)283 (17.6) 427 (26.5)427 (26.5) 327 (20.3)327 (20.3) 187 (11.6)187 (11.6)
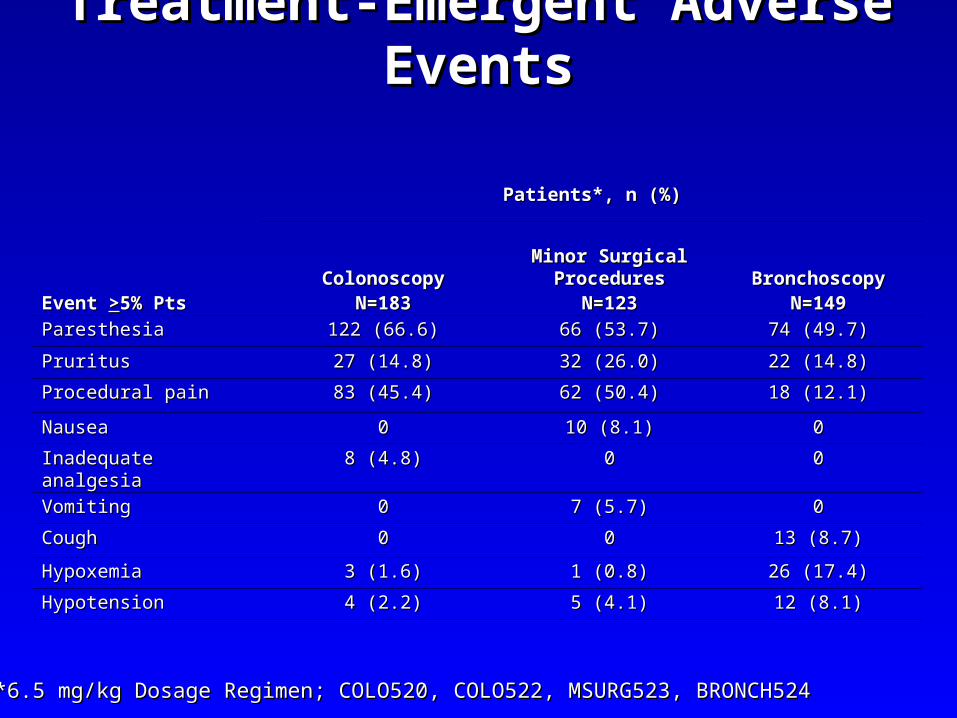
Treatment-Emergent Adverse EventsTreatment-Emergent Adverse Events
Patients*, n (%)Patients*, n (%)
ColonoscopyColonoscopyN=183N=183
Minor Surgical Minor Surgical ProceduresProcedures
N=123N=123BronchoscopyBronchoscopy
N=149N=149Event Event >>5% Pts5% Pts
ParesthesiaParesthesia 122 (66.6)122 (66.6) 66 (53.7)66 (53.7) 74 (49.7)74 (49.7)
PruritusPruritus 27 (14.8)27 (14.8) 32 (26.0)32 (26.0) 22 (14.8)22 (14.8)
Procedural painProcedural pain 83 (45.4)83 (45.4) 62 (50.4)62 (50.4) 18 (12.1)18 (12.1)
NauseaNausea 00 10 (8.1)10 (8.1) 00
Inadequate analgesiaInadequate analgesia 8 (4.8)8 (4.8) 00 00
VomitingVomiting 00 7 (5.7)7 (5.7) 00
CoughCough 00 00 13 (8.7)13 (8.7)
HypoxemiaHypoxemia 3 (1.6)3 (1.6) 1 (0.8)1 (0.8) 26 (17.4)26 (17.4)
HypotensionHypotension 4 (2.2)4 (2.2) 5 (4.1)5 (4.1) 12 (8.1)12 (8.1)
*6.5 mg/kg Dosage Regimen; COLO520, COLO522, MSURG523, BRONCH524*6.5 mg/kg Dosage Regimen; COLO520, COLO522, MSURG523, BRONCH524
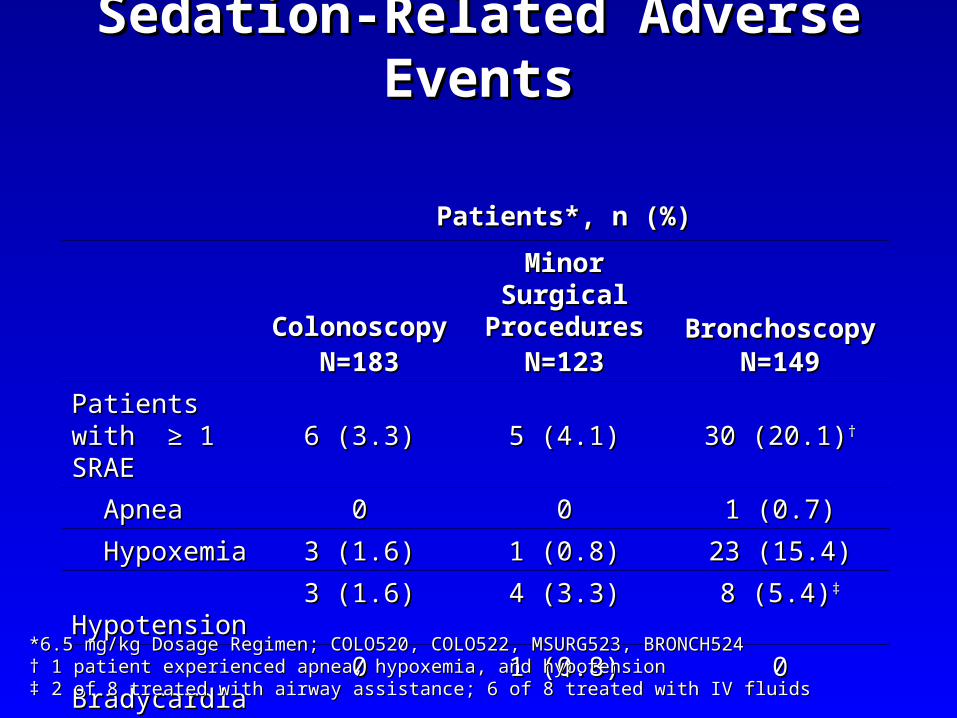
Sedation-Related Adverse EventsSedation-Related Adverse Events
Patients*, n (%)Patients*, n (%)
ColonoscopyColonoscopyN=183N=183
Minor Surgical Minor Surgical ProceduresProcedures
N=123N=123BronchoscopyBronchoscopy
N=149N=149
Patients with Patients with ≥≥ 1 SRAE 1 SRAE 6 (3.3)6 (3.3) 5 (4.1)5 (4.1) 30 (20.1)30 (20.1)††
ApneaApnea 00 00 1 (0.7)1 (0.7)
HypoxemiaHypoxemia 3 (1.6)3 (1.6) 1 (0.8)1 (0.8) 23 (15.4)23 (15.4)
HypotensionHypotension 3 (1.6)3 (1.6) 4 (3.3)4 (3.3) 8 (5.4)8 (5.4)‡‡
BradycardiaBradycardia 00 1 (0.8)1 (0.8) 00
*6.5 mg/kg Dosage Regimen; COLO520, COLO522, MSURG523, BRONCH524*6.5 mg/kg Dosage Regimen; COLO520, COLO522, MSURG523, BRONCH524† † 1 patient experienced apnea, hypoxemia, and hypotension1 patient experienced apnea, hypoxemia, and hypotension‡ ‡ 2 of 8 treated with airway assistance; 6 of 8 treated with IV fluids2 of 8 treated with airway assistance; 6 of 8 treated with IV fluids
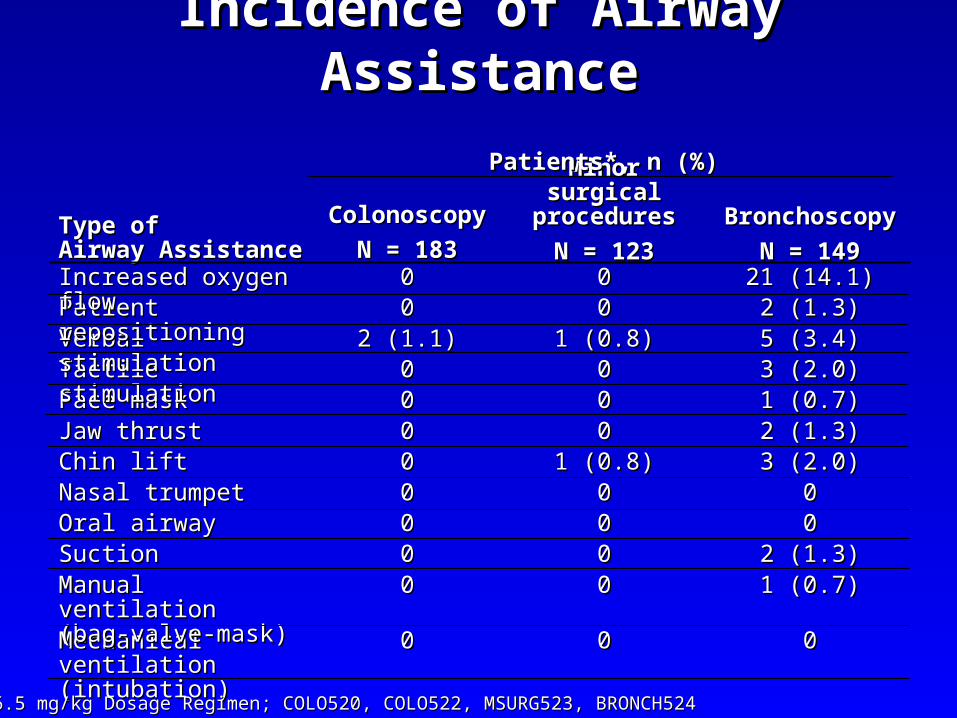
Incidence of Airway AssistanceIncidence of Airway Assistance
BronchoscopyBronchoscopy
N = 149N = 149
Minor surgical Minor surgical proceduresprocedures
N = 123N = 123
ColonoscopyColonoscopy
N = 183N = 183Type of Type of Airway AssistanceAirway Assistance
000000Mechanical ventilation Mechanical ventilation (intubation)(intubation)
1 (0.7)1 (0.7)0000Manual ventilation Manual ventilation (bag-valve-mask)(bag-valve-mask)
2 (1.3)2 (1.3)0000SuctionSuction000000Oral airwayOral airway000000Nasal trumpetNasal trumpet
3 (2.0)3 (2.0)1 (0.8)1 (0.8)00Chin liftChin lift2 (1.3)2 (1.3)0000Jaw thrustJaw thrust1 (0.7)1 (0.7)0000Face maskFace mask3 (2.0)3 (2.0)0000Tactile stimulationTactile stimulation5 (3.4)5 (3.4)1 (0.8)1 (0.8)2 (1.1)2 (1.1)Verbal stimulationVerbal stimulation2 (1.3)2 (1.3)0000Patient repositioningPatient repositioning
21 (14.1)21 (14.1)0000Increased oxygen flowIncreased oxygen flow
Patients*, n (%)Patients*, n (%)
*6.5 mg/kg Dosage Regimen; COLO520, COLO522, MSURG523, BRONCH524*6.5 mg/kg Dosage Regimen; COLO520, COLO522, MSURG523, BRONCH524
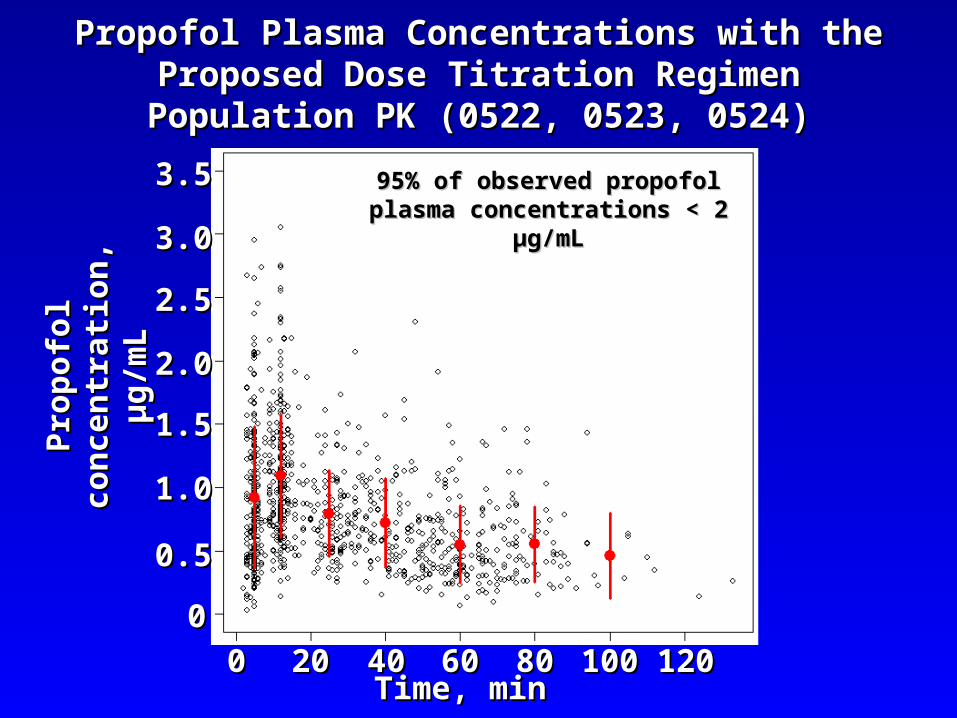
Propofol Plasma Concentrations with the Proposed Propofol Plasma Concentrations with the Proposed Dose Titration RegimenDose Titration Regimen
Population PK (0522, 0523, 0524)Population PK (0522, 0523, 0524)
00
Pro
po
fol
Pro
po
fol
con
cen
trat
ion
, co
nce
ntr
atio
n,
µg
/mL
µg
/mL
2020 4040 6060 8080 100100 120120Time, minTime, min
00
0.50.5
1.01.0
1.51.5
2.02.0
2.52.5
3.03.0
3.53.5 95% of observed propofol plasma 95% of observed propofol plasma concentrations < 2 µg/mLconcentrations < 2 µg/mL
DeathsDeathsAll PatientsAll Patients
• No deaths were considered to be related No deaths were considered to be related to fospropofolto fospropofol
• No deaths occurred within 24 hr of exposure No deaths occurred within 24 hr of exposure to fospropofolto fospropofol
• 10 deaths occurred during the clinical program10 deaths occurred during the clinical program– 5 patients in phase 3 bronchoscopy study5 patients in phase 3 bronchoscopy study– 55†† patients in prolonged exposure (ICU) study patients in prolonged exposure (ICU) study
† † 1 patient received Diprivan only.1 patient received Diprivan only.

Safety SummarySafety Summary
• Safety of fospropofol evaluated in: Safety of fospropofol evaluated in: – Wide range of patient age and ASA status Wide range of patient age and ASA status – Proposed dose and higher dose regimens (more than Proposed dose and higher dose regimens (more than
twice the proposed label dose)twice the proposed label dose)– Considerable clinical trial experience with fospropofol at Considerable clinical trial experience with fospropofol at
wide range of procedureswide range of procedures• Simple airway maneuvers support patients with sedation-Simple airway maneuvers support patients with sedation-
related adverse eventsrelated adverse events• All patients with sedation-related events recovered without All patients with sedation-related events recovered without
sequelae sequelae
Efficacy with Fospropofol*Efficacy with Fospropofol*• Successful procedural sedation experienceSuccessful procedural sedation experience
– Sedation Success: 87 – 89%Sedation Success: 87 – 89%
– Treatment success: 88 - 91%Treatment success: 88 - 91%
– Few procedure or drug discontinuations Few procedure or drug discontinuations
– Rate of sedation related adverse events that is in line with the Rate of sedation related adverse events that is in line with the experience and expectations of those performing procedural sedationexperience and expectations of those performing procedural sedation
• Rapid recovery experience Rapid recovery experience
– Median time to fully alert: 5 minutesMedian time to fully alert: 5 minutes
– Median time to Aldrete Median time to Aldrete >>9: <10 minutes9: <10 minutes
– Potential for reduced duration of monitoring and burden on patient Potential for reduced duration of monitoring and burden on patient care teamcare team
*6.5 mg/kg Dosage Regimen COLO522, *6.5 mg/kg Dosage Regimen COLO522, BRONCH524BRONCH524
• Most patients did not recallMost patients did not recall– Being awake during the procedureBeing awake during the procedure– Pain or discomfortPain or discomfort– Disagreeable aspects of the procedureDisagreeable aspects of the procedure
• High level of patient and physician satisfaction High level of patient and physician satisfaction with the drug and sedation experience using the with the drug and sedation experience using the proposed dosing regimenproposed dosing regimen– 95% of patients would receive fospropofol again95% of patients would receive fospropofol again– Physicians rated it 9 out of 10 on satisfaction scalePhysicians rated it 9 out of 10 on satisfaction scale
• Supplemental doses of sedative and analgesia Supplemental doses of sedative and analgesia – Fospropofol initiation period: 0.9 – 1.6 doses Fospropofol initiation period: 0.9 – 1.6 doses – Total supplemental doses of fospropofol: 1.7 – 2.3Total supplemental doses of fospropofol: 1.7 – 2.3– Patients receiving supplemental analgesia: 17% - 55%Patients receiving supplemental analgesia: 17% - 55%
Efficacy with Fospropofol*Efficacy with Fospropofol*(cont)(cont)
*6.5 mg/kg Dosage Regimen COLO522, *6.5 mg/kg Dosage Regimen COLO522, BRONCH524BRONCH524
• No burning on injectionNo burning on injection– Paresthesia and Pruritus better tolerated by patientsParesthesia and Pruritus better tolerated by patients
• Reduced CReduced Cmaxmax with less interpatient variability with less interpatient variability– Minimal sedation-related adverse eventsMinimal sedation-related adverse events– Effectively tested bolus dose adjustments for higher risk Effectively tested bolus dose adjustments for higher risk
patients patients
• Delayed onset due to metabolic conversion Delayed onset due to metabolic conversion to propofolto propofol
– Time to pre-oxygenate - position patient – refine protocolsTime to pre-oxygenate - position patient – refine protocols
The Future of Fospropofol?The Future of Fospropofol?
• Longer duration of effect from single bolus doses Longer duration of effect from single bolus doses vs. propofolvs. propofol
– Less frequent re-dosing or inadequate sedation intervals Less frequent re-dosing or inadequate sedation intervals • Rapid recovery to fully alert and discharge Rapid recovery to fully alert and discharge
readinessreadiness– ““Propofol Experience” with reduced variability and titration Propofol Experience” with reduced variability and titration
issuesissues– Improved post-procedure patient alertness and instruction Improved post-procedure patient alertness and instruction
recallrecall• Improved patient outcomes with reduced overall Improved patient outcomes with reduced overall
procedure costsprocedure costs– Reduced opioids & sedation-related adverse events, Reduced opioids & sedation-related adverse events,
reduced PONV, faster dischargereduced PONV, faster discharge
The Future of Fospropofol?The Future of Fospropofol?