clinical conference pathophysiology and management...
TRANSCRIPT
131
Clinical Conference
Pathophysiology and Management ofHypertension in Acute Ischemic Stroke
Principal DiscussantStephen J. Phillips
Camp Hill Medical Centre and Department of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada
Hypertension, defined in different ways by vari-ous investigators over a period of many years,has been shown to be a major risk factor for
stroke.1-2 In fact, the strength of the evidence suggeststhat hypertension causes stroke. But by what mecha-nisms? The value of treating chronic hypertension toprevent stroke is well established, but what should bedone about blood pressure elevations in the setting ofacute stroke?
Stroke is a generic term for a clinical syndrome thatincludes focal cerebral infarction (ischemic stroke),focal hemorrhage in the brain, and subarachnoid hem-orrhage.3 Hypertension is an important precursor ofcerebral infarction and intracerebral hemorrhage.Whether hypertension predisposes to subarachnoidhemorrhage is less certain because of conflicting evi-dence from epidemiologic, clinical, and laboratoryinvestigations.47
This article will focus on the pathophysiology andmanagement of elevated blood pressure in the setting ofacute ischemic stroke. A review of the subject seemstimely given the frequency of the problem, the paucityof clinically relevant scientific data,8 and contemporaryinterest in salvaging ischemic brain before infarctionoccurs.9-10
How Does Hypertension CauseCerebral Infarction?
Attempts to answer this question have tended tofocus on the pathoanatomic effects of chronic hyperten-sion, mainly because they are more amenable to studythan the pathophysiological mechanisms of hyperten-sion and cerebral ischemia during the acute phase ofstroke. Clearly, one would expect both types of mecha-nism to be involved, but unfortunately, the picture isincomplete and our knowledge fragmentary. Insightsinto pathoanatomic mechanisms come from epidemio-logic investigations, autopsy studies, and clinical trials.Study of the pathophysiological mechanisms of acutefocal cerebral ischemia has been enhanced by thedevelopment of new techniques such as positron emis-sion tomography and diffusion-weighted magnetic reso-
Reccived October 27,1992; accepted in revised form October 5,1993.
Correspondence to Dr S.J. Phillips, Camp Hill Medical Centre,Department of Medicine, 5303 Morris St, Halifax, Nova Scotia B3J1B6, Canada.
nance imaging.11-'2 Animal models of stroke permitrigorous scientific study of the mechanisms of cerebralinfarction, but the relevance of such laboratory findingsto human stroke is not always clear.
Chronic hypertension aggravates atherosclerosis13
and induces complex pathological changes in the mediasof arteries and arterioles.1415 These structural changesincrease vascular resistance and protect the cerebralmicrocirculation from the deleterious effects of systemichypertension.16 Paradoxically, however, the structuralchanges may predispose to cerebral ischemia by impair-ing vasodilator responsiveness.17-18
The small-diameter penetrating end arteries in thebrain have been considered particularly vulnerable tothe deleterious effects of elevated blood pressure be-cause they arise directly from main arterial trunks.19
The hypertension-associated morphological changes1-20
that occur in these vessels include microaneurysm for-mation,2123 lipohyalinosis,24 and microatheroma.25 Ap-parently as a consequence of these changes but bymechanisms not fully understood, either rupture orocclusion of the diseased vessel may occur, producingintracerebral hemorrhage or infarction. The small in-farcts that occur deep in the cerebral hemispheres orbrain stem as a consequence of occlusion of thesediseased vessels have been postulated to represent aspecific complication of hypertension (lacunar infarc-tion), recognizable clinically as lacunar syndromes.25-26
More recent clinical and epidemiologic data,2729 how-ever, suggest that hypertension is no more important inthe pathogenesis of lacunar infarction (small-vesselterritory stroke) than in the development of large-vesselterritory stroke caused by presumed atherothromboem-bolic mechanisms (Table). Cerebral small-vessel diseasealso occurs in aged normotensive subjects. Collectively,the data suggest that hypertension has an aggravatingand accelerating but nonspecific influence on degener-ative cerebrovascular disease, and the existence of aunique cerebrovascular lesion attributable to hyperten-sion remains in question.30
An overview analysis of 14 randomized trials ofantihypertensive drug therapy31 showed that coronaryheart disease events were reduced by only 14% (95%confidence interval, 4% to 22%). A reduction of 20% to25% would have been expected on the basis of evidencefrom observational epidemiologic studies.32 In contrast,stroke was reduced by 42% (95% confidence interval,33% to 50%). The disparate effect of antihypertensive
by guest on May 8, 2018
http://hyper.ahajournals.org/D
ownloaded from

132 Hypertension Vol 23, No 1 January 1994
Comparison of Frequency of Prestroke HypertensionAmong Patients With Flrst-Ever Ischemic Stroke in theRochester Epidemiology Project37 and OxfordshireCommunity Stroke Project28
Prestroke Hypertension
CBF
Rochester* Oxfordshire!
Lacunar infarction, % 80
Nonlacunar infarction, % 70
44
47
Prestroke hypertension was defined by two blood pressurereadings a 160/95 mmHg in the Rochester project and twoblood pressure readings > 160/90 in the Oxfordshire project.
Difference between proportions within studies: *P=.O5 (P=.11if patients with a cardiac source of emboli are excluded); tP=-6.
treatment on apparently similar pathological processeshas generated considerable debate and has not beenfully explained. Because myocardial infarction (the ma-jor contributor to the end point "coronary heart dis-ease" in clinical trials) is almost invariably a complica-tion of coronary artery atherosclerosis, whereascerebral infarction has several causes, the data suggestthat the effect of antihypertensive therapy on strokeincidence was not mediated solely through an effect onatherothromboembolic mechanisms.
The results of the antihypertensive treatment trialsindicate that both fatal and nonfatal strokes are pre-vented within just a few years of blood pressure lower-ing, even among chronically hypertensive elderly sub-jects33 who would be expected to have advancedirreversible structural arterial disease. This suggeststhat differences in the physiological regulatory mecha-nisms of the cerebral and myocardial circulations andtheir dynamic adaptation to changes in perfusion pres-sure may be important determinants of the effects ofantihypertensive treatment.34
Functional brain imaging studies using positron emis-sion tomography have helped reveal the pathophysio-logical consequences of acute cerebral arterial occlu-sion.35-3* Some compensatory responses to reducedcerebral perfusion pressure are shown in Fig 1. Theinfluence of blood pressure on these responses is notwell understood. In a recent study37 of 16 patients whohad hypertension and an acute middle cerebral arteryterritory infarct, blood flow in the ischemic region (asestimated by single-photon emission computed tomog-raphy) increased as blood pressure fell in patientstreated with captopril (n=3) or clonidine hydrochloride(n=2). In the patients who were given placebo (n=6) ornicardipine hydrochloride (n=5), the fall in blood pres-sure was not associated with a significant change incerebral blood flow. The nicardipine-treated patientshad the greatest fall in blood pressure from baseline.These data are difficult to interpret because of the smallnumber of patients studied.
The time interval between arterial occlusion andirreversible brain injury may be as long as 6 to 9hours.35-38-39 Conceptualized as the ischemic penum-bra,40"42 this period is viewed as a "window of opportu-nity" for therapeutic intervention to restore regionalcerebral blood flow.43-44 The window would be expectedto be widest in zones of cortical ischemia where thepotential for collateral flow is greatest, and narrowest inthe territory of small-diameter penetrating end arteries,
Perfusion Pressure(mm Hg)
FKB 1. Rot shows compensatory responses to reduced cere-bral perfusion pressure. As cerebral perfusion pressure falls,cerebral blood flow (CBF) Is initially maintained by dilation ofprecapillary resistance vessels. As a result, cerebral bloodvolume (CBV) increases. When vasodilation can no longercompensate, cerebral autoregulation fails, and blood flow be-gins to fall (vertical line at 60 mm Hg). If perfusion pressurecontinues to fall, an increase in the oxygen extraction fraction(OEF) maintains cerebral oxygen metabolism (CMRO2). Oncethis mechanism becomes maximal (vertical line at 30 mm Hg),further decline in blood flow leads to substrate depletion, energyfailure, disruption of cellular homeostasis, and ultimately, isch-emic necrosis (ie, infarction). Dashed lines indicate conditionsfor which data are inadequate to draw firm conclusions. (Usedwith permission from Powers.38)
occlusion of which results in small, deep (lacunar)cerebral infarcts. The influence of blood pressure onthis window is, clearly, worthy of further study.
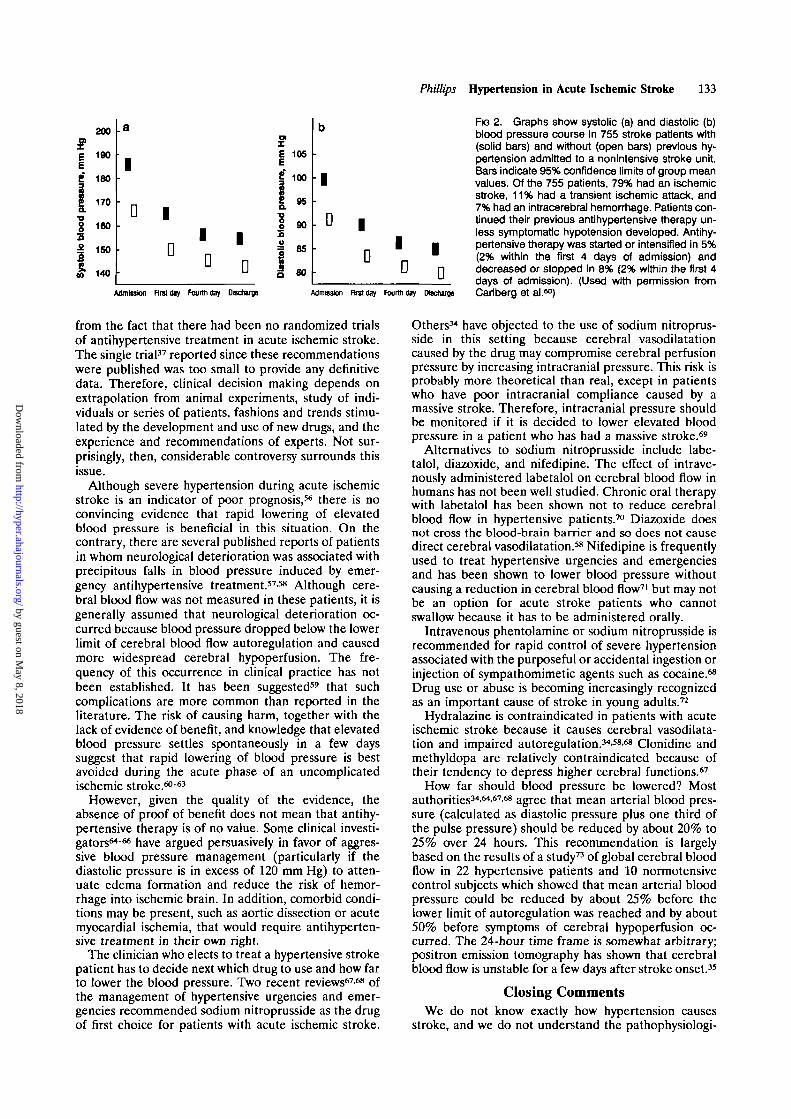
Acute increases in blood pressure superimposed on achronic hypertensive state ("acute-on-chronic hyperten-sion") is common in acute ischemic stroke; about half ofall patients have a history of preexisting hyperten-sion,45"48 and on average these individuals have higherblood pressures than those who were previously nor-motensrve.48"50 After 3 or 4 days in the hospital, bloodpressure falls spontaneously (Fig 2).45"47-50-51
The reasons for acute hypertension in the setting ofacute stroke are poorly understood. Because it occurs inpatients with transient ischemic attacks as well as strokepatients,50-51 Cushing's phenomenon (increased bloodpressure secondary to elevated intracranial pressure)cannot be responsible, except in cases of massive cere-bral infarction. There seems to be no definite correla-tion with lesion size or location.49 Therefore, it isdifficult to incriminate ischemic damage to the insularcortex,52 nucleus tracrus solitarius, or other structuresinvolved in the physiological regulation of blood pres-sure.53 Most explanations are based on the premise thatthe hypertension is secondary to the stroke, eg, aresponse to increased plasma catecholamines,54 or thestress of hospital admission.48-50
How Should Elevated Blood Pressure BeManaged in the Setting of Acute
Ischemic Stroke?The answer to this question is "rarely and cautiously"
according to the recent report of the Emergency Car-diac Care Committee and Subcommittees of the Amer-ican Heart Association.55 This statement stems mainly
by guest on May 8, 2018
http://hyper.ahajournals.org/D
ownloaded from
Phillips Hypertension in Acute Ischemic Stroke 133
21i
1•D
sza
I
200
190
180
170
160
150
140
a
1
' D 1
D1D
|D
E 105
| 100
I K1 90
= ash
80
b
1
. D 1
D 1
D1D
First diy Fourth day Discharge Admission First day Fourth d»y Hscturoe
F G 2. Graphs show systolic (a) and diastolic (b)blood pressure course in 755 stroke patients with(solid bars) and without (open bars) previous hy-pertension admitted to a nonintensive stroke unit.Bars indicate 95% confidence limits of group meanvalues. Of the 755 patients, 79% had an ischemicstroke, 11% had a transient ischemic attack, and7% had an intracerebral hemorrhage. Patients con-tinued their previous antihypertensive therapy un-less symptomatic hypotension developed. Antihy-pertensive therapy was started or intensified in 5%(2% within the first 4 days of admission) anddecreased or stopped in 8% (2% within the first 4days of admission). (Used with permission fromCarlberg et al.M)
from the fact that there had been no randomized trialsof antihypertensive treatment in acute ischemic stroke.The single trial37 reported since these recommendationswere published was too small to provide any definitivedata. Therefore, clinical decision making depends onextrapolation from animal experiments, study of indi-viduals or series of patients, fashions and trends stimu-lated by the development and use of new drugs, and theexperience and recommendations of experts. Not sur-prisingly, then, considerable controversy surrounds thisissue.
Although severe hypertension during acute ischemicstroke is an indicator of poor prognosis,5* there is noconvincing evidence that rapid lowering of elevatedblood pressure is beneficial in this situation. On thecontrary, there are several published reports of patientsin whom neurological deterioration was associated withprecipitous falls in blood pressure induced by emer-gency antihypertensive treatment.57-58 Although cere-bral blood flow was not measured in these patients, it isgenerally assumed that neurological deterioration oc-curred because blood pressure dropped below the lowerlimit of cerebral blood flow autoregulation and causedmore widespread cerebral hypoperfusion. The fre-quency of this occurrence in clinical practice has notbeen established. It has been suggested59 that suchcomplications are more common than reported in theliterature. The risk of causing harm, together with thelack of evidence of benefit, and knowledge that elevatedblood pressure settles spontaneously in a few dayssuggest that rapid lowering of blood pressure is bestavoided during the acute phase of an uncomplicatedischemic stroke.60*63
However, given the quality of the evidence, theabsence of proof of benefit does not mean that antihy-pertensive therapy is of no value. Some clinical investi-gators64"66 have argued persuasively in favor of aggres-sive blood pressure management (particularly if thediastolic pressure is in excess of 120 mm Hg) to atten-uate edema formation and reduce the risk of hemor-rhage into ischemic brain. In addition, comorbid condi-tions may be present, such as aortic dissection or acutemyocardial ischemia, that would require antihyperten-sive treatment in their own right.
The clinician who elects to treat a hypertensive strokepatient has to decide next which drug to use and how farto lower the blood pressure. Two recent reviews67'68 ofthe management of hypertensive urgencies and emer-gencies recommended sodium nitroprusside as the drugof first choice for patients with acute ischemic stroke.
Others34 have objected to the use of sodium nitroprus-side in this setting because cerebral vasodilatationcaused by the drug may compromise cerebral perfusionpressure by increasing intracranial pressure. This risk isprobably more theoretical than real, except in patientswho have poor intracranial compliance caused by amassive stroke. Therefore, intracranial pressure shouldbe monitored if it is decided to lower elevated bloodpressure in a patient who has had a massive stroke.69
Alternatives to sodium nitroprusside include labe-talol, diazoxide, and nifedipine. The effect of intrave-nously administered labetalol on cerebral blood flow inhumans has not been well studied. Chronic oral therapywith labetalol has been shown not to reduce cerebralblood flow in hypertensive patients.70 Diazoxide doesnot cross the blood-brain barrier and so does not causedirect cerebral vasodilatation.58 Nifedipine is frequentlyused to treat hypertensive urgencies and emergenciesand has been shown to lower blood pressure withoutcausing a reduction in cerebral blood flow71 but may notbe an option for acute stroke patients who cannotswallow because it has to be administered orally.
Intravenous phentolamine or sodium nitroprusside isrecommended for rapid control of severe hypertensionassociated with the purposeful or accidental ingestion orinjection of sympathomimetic agents such as cocaine.68
Drug use or abuse is becoming increasingly recognizedas an important cause of stroke in young adults.72
Hydralazine is contraindicated in patients with acuteischemic stroke because it causes cerebral vasodilata-tion and impaired autoregulation.34'58'68 Clonidine andmethyldopa are relatively contraindicated because oftheir tendency to depress higher cerebral functions.67
How far should blood pressure be lowered? Mostauthorities34'64'67'68 agree that mean arterial blood pres-sure (calculated as diastolic pressure plus one third ofthe pulse pressure) should be reduced by about 20% to25% over 24 hours. This recommendation is largelybased on the results of a study73 of global cerebral bloodflow in 22 hypertensive patients and 10 normotensivecontrol subjects which showed that mean arterial bloodpressure could be reduced by about 25% before thelower limit of autoregulation was reached and by about50% before symptoms of cerebral hypoperfusion oc-curred. The 24-hour time frame is somewhat arbitrary;positron emission tomography has shown that cerebralblood flow is unstable for a few days after stroke onset.35
Closing CommentsWe do not know exactly how hypertension causes
stroke, and we do not understand the pathophysiologi-
by guest on May 8, 2018
http://hyper.ahajournals.org/D
ownloaded from

134 Hypertension Vol 23, No 1 January 1994
cal mechanisms producing elevated blood pressure dur-ing acute focal cerebral ischemia. Nor do we know therelative risks and benefits of antihypertensive treatmentin patients who present with an acute ischemic stroke orwhether one antihypertensive agent is better thananother.
Fortunately, the new wave of interest in salvagingischemic brain is likely to change this dismal state ofaffairs because of the realization that blood pressureand its pharmacological manipulation have the poten-tial to interact —directly or indirectly, beneficially ordetrimentally—with other treatments currently beingevaluated for acute ischemic stroke. For example, in therecently published pilot studies74-76 of tissue plasmino-gen activator administered within minutes to hours ofstroke onset, patients with severe hypertension wereexcluded because they were considered to be at highrisk of hemorrhage into the region of reperfused isch-emic brain.
It is hoped that future research will bridge the gapsbetween laboratory science and clinical investigationand between the theory and practice of antihyperten-sive treatment in acute ischemic stroke.
Ack nowledgmen tDr Phillips receives support from the W. Garfield Weston
Foundation.
Questions and AnswersDr Gerald DiBona (University of Iowa, Iowa City):Given the impressive return of blood pressure to nearnormal levels by day 4 after acute stroke in the Swedishstudy50 (Fig 2), is there a cutoff value for admissionblood pressure that should be treated?Dr Phillips: No, the authors did not make any recom-mendations for treatment. Other authors have done so,but cutoff values do not take into account the prestrokeblood pressure. For example, a stroke patient with ablood pressure of 190/115 mm Hg and a premorbidblood pressure of 170/90 mm Hg would probably beconsidered to require different management than an-other stroke patient with the same level of acute hyper-tension but a premorbid blood pressure of 140/90mm Hg. Unfortunately, the premorbid blood pressure isusually unknown to the treating physician when apatient presents to the emergency room because of astroke.Dr Donald Heistad (University of Iowa, Iowa City): Isthere a way to individualize treatment for patients? Areneurological symptoms or other approaches useful inevaluating responses to reduction of blood pressure inacute stroke?Dr Phillips: Currently, no. Physicians tend to feelcompelled to act when the systolic pressure is 180mm Hg or more, particularly if the patient's neurologi-cal status is deteriorating. Conversely, if a patient'sneurological status deteriorates because of or despiteantihypertensive treatment, then the treatment wouldusually be discontinued. However, because of the tre-mendous variation in the clinical severity and course ofacute focal cerebral ischemia, it is difficult to tell in anindividual patient whether the administration of antihy-pertensive treatment influences outcome. Although thisis apparently paradoxical to many clinicians, we arelikely to learn more about the treatment of individuals
by studying large numbers of patients in randomizedtrials.Dr William Lawton (University of Iowa, Iowa City): Arethere different effects of various calcium blockers interms of efficacy; eg, does nimodipine or nicardipinehave special properties to commend their use over otherdihydropyridines?Dr Phillips: Not as far as we know. Nimodipine is ofproven value for the prevention of secondary cerebralischemic damage in patients with acute subarachnoidhemorrhage but has not been shown to be of definitevalue in patients with acute ischemic stroke.77 Thebenefit of nimodipine therapy in subarachnoid hemor-rhage patients is probably due to a cytoprotective effectrather than a blood pressure-lowering effect. In tworandomized placebo-controlled trials of nimodipine inpatients with acute ischemic stroke,78-79 there were nosignificant differences in blood pressure between thenimodipine- and placebo-treated groups. Different cal-cium channel blockers have not been compared inclinical stroke trials.Dr William Lawton (University of Iowa, Iowa City): Docalcium channel blockers or other vasodilators producea "steal syndrome" in acute stroke and worsen ischemicareas?Dr Phillips: Possibly. Vorstrup et al80 measured regionalcerebral blood flow using the xenon-133 inhalationmethod before and after the intravenous administrationof PY 108-068 (a dihydropyridine calcium antagonistdeveloped by Sandoz Ltd) in 11 patients who had acerebral infarct confirmed by computed tomography inthe preceding 1 to 9 days. Cerebral blood flow in theischemic areas did not improve. In 3 patients, cerebralblood flow decreased even further in the ischemic area.In 1 other patient, cerebral blood flow increased in partof the peri-infarct area. These changes in cerebral bloodflow were not accompanied by any change in the pa-tients' clinical status. The results are difficult to inter-pret because the experiment was uncontrolled, a smallnumber of patients were studied, and the cerebral bloodflow measurements were made at different times aftereach stroke. The investigators did not clearly demon-strate an increase in blood flow in one area of the brainand a concomitant decrease in another (ie, a "steal"phenomenon).
References1. Phillips SJ, Whisnant JP. Hypertension and stroke. In: Laragh JH,
Brenner BM, eds. Hypertension: Pathopliysiology, Diagnosis, andManagement. New York, NY: Raven Press, Publishers; 1990:417-431.
2. Phillips SJ, Whisnant JP, on behalf of the National High BloodPressure Education Program. Hypertension and the brain. ArchIntern Med. 1992;152:938-945.
3. Whisnant JP, Basford JR, Bernstein EF, Cooper ES, Dyken ML,Easton JD, Little JR, Marler JR, Millikan CH, Petito CK, PriceTR, Raichle ME, Robertson JT, Thiele B, Walker MD, Zim-merman RA. Qassification of cerebrovascular diseases III. Stroke.1990;21:637-676.
4. Broderick JP, Phillips SJ, Whisnant JP, O'Fallon WM, BergstralhEJ. Incidence rates of stroke in the eighties: the end of the declinein stroke? Stroke. 1989;20:577-582.
5. Bonita R. Cigarette smoking, hypertension and the risk of sub-arachnoid hemorrhage: a population-based case-control study.Stroke. 1986;17:831-835.
6. McCormick WF, Schmalstieg EJ. The relationship of arterialhypertension to intracranial aneurysms. Arch Neurol. 1977;34:285-287.
by guest on May 8, 2018
http://hyper.ahajournals.org/D
ownloaded from
Phillips Hypertension in Acute Ischemic Stroke 135
7. Stehbens WE. Etiology of intracranial berry aneurysms. J Neumsurg1989:70:823-831.
8. Powers WJ. Acute hypertension after stroke: the scientific basis fortreatment decisions. Neurology 1993;43:461-467.
9. Pulsinelli W. Pathophysiology of acute ischaemic stroke. Lancet.1992;339:533-536.
10. Sandercock P, Willems H. Medical treatment of acute ischaemicstroke. Lancet. 1992;339:537-539.
11. Fisher M, Sotak CH, Minematsu K, Li L. New magnetic resonancetechniques for evaluating cerebrovascular disease. Ann NeuroL1992;32:115-122.
12. Prichard JW, Brass LM. New anatomical and functional imagingmethods. Ann NeuroL 1992;32:395-4O0.
13. Chobanian AV. The influence of hypertension and other hemo-dynamic factors in atherogenesis. Prog Cardiovasc Dis. 1983;26:177-196.
14. Graham DI. Hypoxia and vascular disorders. In: Hume Adams J,Corsellis JAN, Duchen LW, eds. Greenfield's Neuropathology. 5thed. New York, NY: Oxford University Press; 1992:153-268.
15. Baumbach GL, Heistad DD. Remodeling of cerebral artenoles inchronic hypertension. Hypertension. 1989^3:968-972.
16. Baumbach GL, Heistad DD. Cerebral circulation in chronicarterial hypertension. Hypertension. 1988;12:89-95.
17. Heistad DD, Mayhan WG, Coyle P, Baumbach GL. Impaireddilatation of cerebral artenoles in chronic hypertension. BloodVessels. 1990;27:258-262.
18. Baumbach GL, Heistad DD. Adaptive changes in cerebral bloodvessels during chronic hypertension. / Hypertens. 1991;9:987-991.
19. Hughes W. Origin of lacunes. Lancet. 1965;2:19-21.20. Ross Russell RW. How does blood-pressure cause stroke? Lancet.
1975;2:1283-1285.21. Ross Russell RW. Observations on intracerebral aneurysms.
Brain. 1963;86:425-442.22. Cole FM, Yates PO. The occurrence and significance of intrace-
rebral micro-aneurysms. J Pathol Bacteriol. 1967;93:393-411.23. Fisher CM. Cerebral miliary aneurysms in hypertension. Am J
Pathol. 1972;66:313-324.24. Fisher CM. The arterial lesions underlying lacunes. Ada Neuro-
pathol (Bed). 1969;12:1-15.25. Fisher CM. Lacunar stroke and infarcts: a review. Neurology. 1982;
32:871-876.26. Bamford JM, Warlow CP. Evolution and testing of the lacunar
hypothesis. Stroke. 1988;19:1074-1082.27. Lodder J, Bamford JM, Sandercock PAG, Jones LN, Warlow CP.
Are hypertension or cardiac embolism likely causes of lacunarinfarction? Stroke. 1990;21:375-381.
28. Sacco SE, Whisnant JP, Broderick JP, Phillips SJ, O'Fallon WM.Epidemiological characteristics of lacunar infarcts in a population.Stroke. 1991;22:1236-1241.
29. Lodder J, Boiten J. Incidence, natural history, and risk factors inlacunar infarction. In: Pullicino PM, Caplan LR, Hommel M, eds.Advances in Neurology. New York, NY: Raven Press, Publishers;1993;62:213-227.
30. Ostrow PT, Miller LL. Pathology of small artery disease. In: Pul-licino PM, Caplan LR, Hommel M, eds. Advances in Neurology.New York, NY: Raven Press, Publishers; 1993;62:93-123.
31. Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, EberleinKA, Godwin J, Qizilbash N, Taylor JO, Hennekens CH. Bloodpressure, stroke, and coronary heart disease. Part 2, short-termreductions in blood pressure: overview of randomised drug trials intheir epidemiological context. Lancet 1990;335:827-838.
32. MacMahon S, Peto R, Cutler J, Collins R, Sorlie P, Neaton J,Abbott R, Godwin J, Dyer A, Stamler J. Blood pressure, stroke,and coronary heart disease. Part 1, prolonged differences in bloodpressure: prospective observational studies corrected for theregression dilution bias. Lancet. 1990;335:765-774.
33. SHEP Cooperative Research Group. Prevention of stroke by anti-hypertensive drug treatment in older persons with isolated systolichypertension: final results of the Systolic Hypertension in theElderly Program (SHEP). JAMA. 1991:265:3255-3264.
34. Strandgaard S, Paulson OB. Hypertensive disease and the cerebralcirculation. In: Laragh JH, Brenner BM, eds. Hypertension: Patho-physiology, Diagnosis, and Management. New York, NY: RavenPress, Publishers; 1990:399-416.
35. Baron JC. Pathophysiology of acute cerebral ischemia: PETstudies in humans. Cerebrovasc Dis. 1991;l(suppl 1):22-31.
36. Powers WJ. Cerebral hemodynamics in ischemic cerebrovasculardisease. Ann NeuroL 1991;29:231-240.
37. Lisk DR, Grotta JC, Lamki LM, Tran HD, Taylor JW, MolonyDA, Barron BJ. Should hypertension be treated after acute stroke?
A randomized controlled trial using single photon emissioncomputed tomography. Arch Neural. 1993;50:855-862.
38. Pulsinelli WA, Brierley JB, Plum F. Temporal profile of neuronaldamage in a model of transient forebrain ischemia. Ann Neural.1982;ll:491-498.
39. Petito CK, Feldmann E, Pulsinelli WA, Plum F. Delayed hippo-campal damage in humans following cardiorespiratory arrest. Neu-rology. 1987:37:1281-1286.
40. Astrup J, Siesjo BK, Symon L. Thresholds in cerebral ischemia: theischemic penumbra. Stroke. 1981;12:723-725.
41. Hakim A. The cerebral ischemic penumbra. Can J Neural Sci.1987;14:557-559.
42. Lassen NA, Astrup J. Ischemic penumbra. In: Wood JH, ed.Cerebral Blood Flow. Physiologic and Clinical Aspects. New York,NY: McGraw-Hill Book Co; 1987:458-466.
43. Lassen NA, Fieschi C, Lenzi GL. Ischemic penumbra andneuronal death: comments on the therapeutic window in acutestroke with particular reference to thromborytic therapy. Cere-bwvasc Dis. 1991;l(suppl l):32-35.
44. Marchal G, Serrati C, Rioux P, Petit-Taboue MC, Viader F, De LaSayette V, Le Doze F, Lochon P, Derlon JM, Orgogozo JM, BaronJC. PET imaging of cerebral perfusion and oxygen consumption inacute ischaemic stroke: relation to outcome. Lancet. 1993;341:925-927.
45. Wallace JD, Levy LL. Blood pressure after stroke. JAMA. 1981;246:2177-2180.
46. Britton M, Carlsson A, de Faire U. Blood pressure course inpatients with acute stroke and matched controls. Stroke. 1986;17:861-864.
47. Loyke HF. Lowering of blood pressure after stroke. Am J Med Sci1983;286:2-11.
48. Carlberg B, Asplund K, Hagg E: Factors influencing admissionblood pressure levels in patients with acute stroke. Stroke. 1991;22:527-530.
49. Britton M, Carlsson A. Very high blood pressure in acute stroke.J Intern Med. 1990;228:611-615.
50. Carlberg B, Asplund K, H3gg E. Course of blood pressure indifferent subsets of patients after acute stroke. Cerebrovasc Dis.1991;l:281-287.
51. Jansen PAF, Schulte BPM, Poels EFJ, Gribnau FWJ. Course ofblood pressure after cerebral infarction and transient ischemicattack. Clin Neurol Neurosurg. 1987;89:243-246.
52. Ruggiero DA, Mraovitch S, Granata AR, Anwar M, Reis DJ. Arole of insular cortex in cardiovascular function. J Comp Neurol.1987;257:189-207.
53. Talman WT. Cardiovascular regulation and lesions of the centralnervous system. Ann NeuroL 1985;18:1-12.
54. Jansen PAF, Thien T, Gribnau FWJ, Schulte BPM, Willemsen JJ,Lamers KJB, Poels EFJ. Blood pressure and both venous andurinary catecholamines after cerebral infarction. Clin Neurol Neu-rosurg. 1988;90:41-45.
55. Emergency Cardiac Care Committee and Subcommittees,American Heart Association: Guidelines for cardiopulmonaryresuscitation and emergency cardiac care. Part IV: special resus-citation situations: stroke. JAMA. 1992;268:2242-2244.
56. Davalos A, Cendra E, Teruel J, Martinez M, Genfs D. Deterio-rating ischemic stroke: risk factors and prognosis. Neurology. 1990;40:1865-1869.
57. Jansen PA, Schulte BP, Gribnau FW. Cerebral ischaemia andstroke as side effects of antihypertensive treatment: special dangerin the elderly. A review of the cases reported in the literature. NethJ Med. 1987;30:193-201.
58. Barry DI. Cerebrovascular aspects of antihypertensive treatment.Am J CardioL 1989;63:14C-18C
59. Graham DI. Ischaemic brain damage following emergency bloodpressure lowering in hypertensive patients. Ada Med Scand SuppL1983;678:61-69.
60. Yatsu FM, Zivin J. Hypertension in acute ischemic strokes: not totreat. Arch NeuroL 1985;42:999-1000.
61. Hachinski V. Hypertension in acute ischemic strokes. Arch NeuroL1985;42:1002.
62. Lavin P. Management of hypertension in patients with acutestroke. Arch Intern Med. 1986;146:66-68.
63. Britton M, de Faire U, Helmers C. Hazards of therapy forexcessive hypertension in acute stroke. Ada Med Scand. 1980;207:253-257.
64. Brott T, MacCarthy EP. Antihypertensive therapy in stroke. In:Fisher M, ed. Medical Therapy of Acute Stroke. New York, NY:Marcel Dekker, Inc; 1989:117-141.
by guest on May 8, 2018
http://hyper.ahajournals.org/D
ownloaded from

136 Hypertension Vol 23, No 1 January 1994
65. Brott T, Reed RL. Intensive care for acute stroke in the com-munity hospital setting: the first 24 hours. Stroke. 1989;20:694-697.
66. Spence JD, Del Maestro RF. Hypertension in acute ischemicstrokes: treat. Arch Neurol. 1985;42:1000-1002.
67. Calhoun DA, Oparil S. Treatment of hypertensive crisis. N EnglJMed. 1990;323:l 177-1183.
68. Gifford RW Jr. Management of hypertensive crises. JAMA. 1991;266:829-835.
69. Ropper AH, Rockoff MA. Treatment of intracranial hypertension.In: Ropper AH, Kennedy SF, eds. Neurological and NeurosurgicalIntensive Care. Rockville, Md: Aspen Publishers, Inc; 1988:23-41.
70. Griffith DNW, Newbury JPA, Woollard ML. The effect of beta-adrenoceptor blocking drugs on cerebral blood flow. Br J ClinPharmacol. 1979;7:491-494.
71. Bertel O, Conen D, Radu EW, Muller J, Dubach UC. Nifedipinein hypertensive emergencies. BMJ. 1983;286:19-21.
72. Sloan MA, Kittner SJ, Rigamonti D, Price TR. Occurrence ofstroke associated with use/abuse of drugs. Neurology. 1991;41:1358-1364.
73. Strandgaard S. Autoregulation of cerebral blood flow in hyper-tensive patients: the modifying influence of prolonged antihyper-tensive treatment on the tolerance to acute, drug-induced hypo-tension. Circulation. 1976^3:720-727.
74. Brott TG, Haley EC Jr, Levy DE, Barsan W, Broderick J,Sheppard GL, Spilker J, Kongable GL, Massey S, Reed R, MarlerJ. Urgent therapy for stroke. Part I. Pilot study of tissue plas-
minogen activator administered within 90 minutes. Stroke. 1992;23:632-640.
75. Haley EC Jr, Levy DE, Brott TG, Sheppard GL, Wong MCW,Kongable GL, Torner JC, Marler JR. Urgent therapy for stroke.Part II. Pilot study of tissue plasminogen activator administered91-180 minutes from onset. Stroke, 1992;23:641-645.
76. del Zoppo GJ, Poeck K, Pessin MS, Wolpert SM, Furlan AJ,Ferbert A, Alberts MJ, Zivin JA, Wechsler L, Busse O, GreenleeR Jr, Brass L, Mohr JP, Feldmann E, Hacke W, Kase CS, Biller J,Gress D, Otis SM. Recombinant tissue plasminogen activator inacute thrombotic and embolic stroke. Ann NeuroL 1992;32:78-86.
77. Langley MS, Sorkin EM. Nimodipine: a review of its pharmaco-dynamic and pharmacokinetic properties, and therapeuticpotential in cerebrovascular disease. Drugs. 1989;37:669-699.
78. Gelmers HJ, Gorter K, De Weerdt CJ, Wiezer HJA. A controlledtrial of nimodipine in acute ischemic stroke. N Engl J Med. 1988;318:203-207.
79. Trust Study Group: Randomised, double-blind, placebo-controlledtrial of nimodipine in acute stroke. Lancet. 1990;336:1205-1209.
80. Vorstrup S, Andersen A, Blegvad N, Paulson OB. Calciumantagonist (PY 108-068) treatment may further decrease flow inischemic areas in acute stroke. J Cereb Blood Flow Metab. 1986;6:222-229.
KEY WORDS • antihypertensive agents • cerebral ischemia •cerebral infarction • hypertension, chronic • hypertension, acute
Presentation and publication of this Clinical Conference Is supported by an educational grant fromHealth Sciences Service, Merck Sharp & Dohme.
by guest on May 8, 2018
http://hyper.ahajournals.org/D
ownloaded from
S J PhillipsPathophysiology and management of hypertension in acute ischemic stroke.
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 1994 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/01.HYP.23.1.131
1994;23:131-136Hypertension.
http://hyper.ahajournals.org/content/23/1/131.citationWorld Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOffice. Once the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertension Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 8, 2018
http://hyper.ahajournals.org/D
ownloaded from