chirurgische behandeling van kanker - nvvoncologie.nl · chirurgische behandeling van kanker. p2...
TRANSCRIPT
p 1
chirurgische behandeling van kanker
p 2
chirurgische behandeling van kanker

p 3
geen “how I do it”

p 4
“wet van de afnemende meeropbrengst”
2009

p 5
chirurgische oncologietrends laatste 100 jaar
meer is beter
less is more
meer is beter!!

p 6
chirurgische oncologietrends
meer was beter
mag het iets minder?
meer is beter!!

p 7
Meer was beter
marge

p 8
Meer was beter
voorbeeld:
Halsted-principe
p 9
The results of operations for the cure of cancer of the breast performed at the Johns Hopkins hospital from
June 1889 to January 1894
Halsted WS
Ann Surg 1894

p 10
The results of operations for the cure of cancer of the breastperformed at the Johns Hopkins hospital from June 1889 to
January 1894
n=50
3/50 recidieven

p 11
Halsted-principe
Als borstkanker eerst uitzaait naar de lymfeklieren en vandaar naar elders.....
p 12
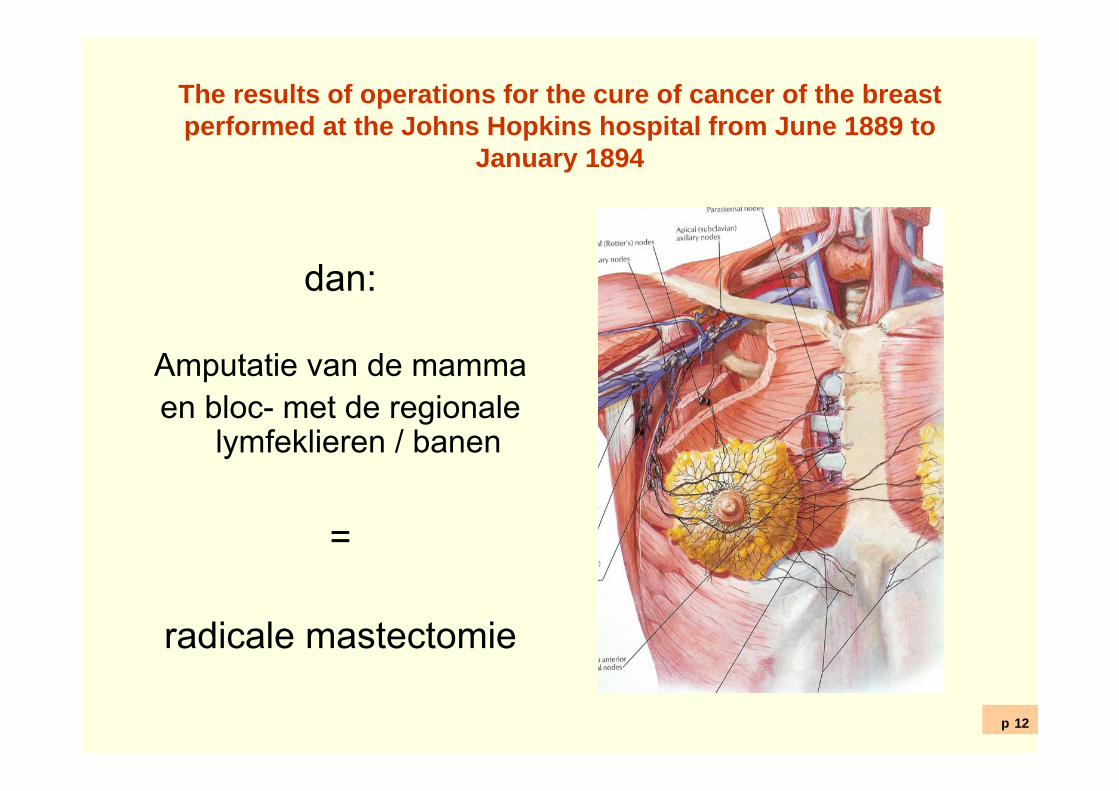
The results of operations for the cure of cancer of the breastperformed at the Johns Hopkins hospital from June 1889 to
January 1894
dan:
Amputatie van de mamma en bloc- met de regionale
lymfeklieren / banen
=
radicale mastectomie

p 13
The results of operations for the cure of cancer of the breast performed at the Johns Hopkins hospital from
June 1889 to January 1894
Halsted WS
Ann Surg 1894

p 14
Halsted paradigma:niet alleen bij borstkanker
oesofaguscarcinoom
tumor-en bloc met lymfadenectomie

p 15
Extended transthoracic resection compared withlimited transhiatal resection for adenocarcinoma of the
esophagus.Hulscher, NEJM 2002
TTE vs THE
114 vs 106

p 16
THE
TTE
p 17
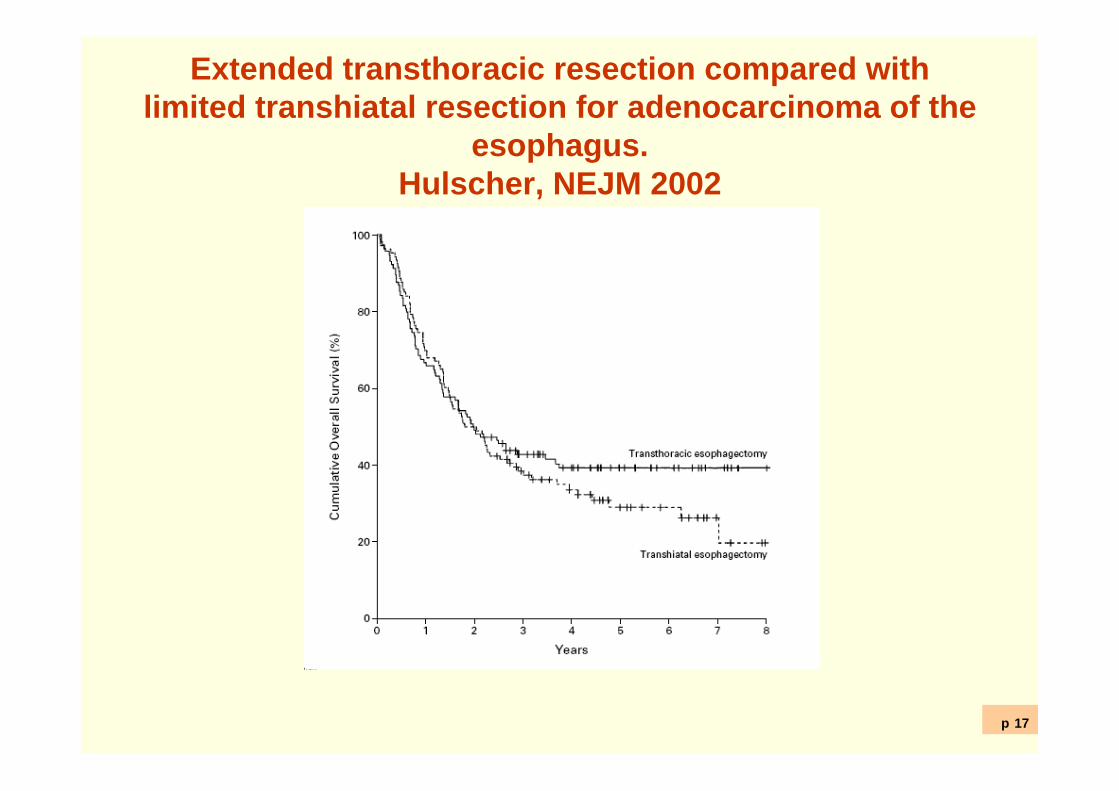
Extended transthoracic resection compared withlimited transhiatal resection for adenocarcinoma of the
esophagus.Hulscher, NEJM 2002
TTE vs THE
5 jrs overleving 70 vs 60%

p 18
chirurgische oncologietrends
Is meer echt beter?
Zo compleet mogelijke verwijdering van de
regionale lymfeklieren

p 19
Radical mastectomy versus radical mastectomy plus internalmammary dissection: five year results of an international co-
operative studyLacour, Cancer 1976
ook lymfeafvloed
p 20
Radical mastectomy versus radical mastectomy plus internalmammary dissection: five year results of an international co-
operative studyLacour, Cancer 1976
n=1580
morbiditeit >>

p 21
Radical mastectomy versus radical mastectomy plus internalmammary dissection: five year results of an international co-
operative studyLacour, Cancer 1976
n=1580
overall survival=
p 22
chirurgische oncologietrends
Is meer echt beter?
Mwah!

p 23
Extended transthoracic resection compared withlimited transhiatal resection for adenocarcinoma of the
esophagus.Hulscher, NEJM 2002
TTE vs THE
5 jrs overleving 70 vs 60%
p 24
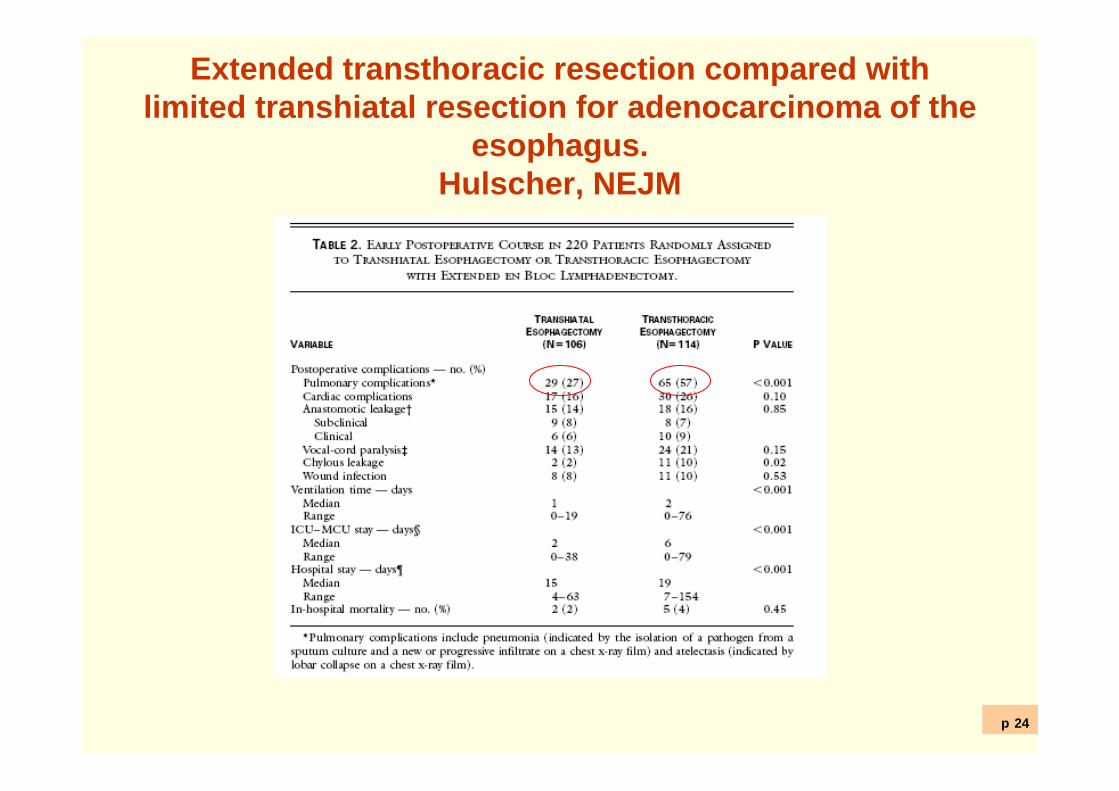
Extended transthoracic resection compared withlimited transhiatal resection for adenocarcinoma of the
esophagus.Hulscher, NEJM
TTE
morbiditeit >>
p 25
Is meer beter?
morbiditeit neemt toe
opbrengst van “maximale” chirurgie beperkt

p 26
The results of operations for the cure of cancer of the breastperformed at the Johns Hopkins hospital from June 1889 to
January 1894
n=50
3/50 recidieven(anno1895)

p 27
A study of the results of operations for the cure of cancer of the breast performed at the Johns Hopkins hospital from 1889 to 1931
Lewis, Ann Surg 1932
n=950
5-jrs overall survival22%

p 28
Is meer beter?
effect van chirurgie is “begrensd”

p 29
chirurgische oncologietrends
meer ≠ beter
kan het ook met minder?
meer is beter!!

p 30
Mag het iets minder?
Als meer chirurgie geen gunstig effect …..
p 31
Mag het iets minder?
………dan geeft zuiniger chirurgie misschien wel
minder ellende

p 32
A study of the results of operations for the cure of cancer of the breast performed at the Johns Hopkins hospital from 1889 to 1931
Lewis, Ann Surg 1932
n=950
5-jrs overall survival22%
(78% overleden)

p 33
The radium treatment of carcinoma of the breastKeynes J, Br J Surg 1931
n=171lokale excisie en radium–naalden
3 jaar FU: 77% in leven (cNo)46% in leven (cN1)

p 34
Comparing radical mastectomy with quadrantectomy, axillarydissection, and radiotherapy in patients with small cancers of the
breast
Veronesi, NEJM 1981
349 vs 352

p 35
Comparing radical mastectomy with quadrantectomy, axillarydissection, and radiotherapy in patients with small cancers of the
breastVeronesi, NEJM 1981

p 36
Comparing radical mastectomy with quadrantectomy, axillarydissection, and radiotherapy in patients with small cancers of the
breastVeronesi, NEJM 1981
lokaal recidief
3/349 vs 1/352*
*in 1981 2002
p 37
Less is more?Borstkanker I
Mammasparende therapie: cosmetisch superieur
p 38
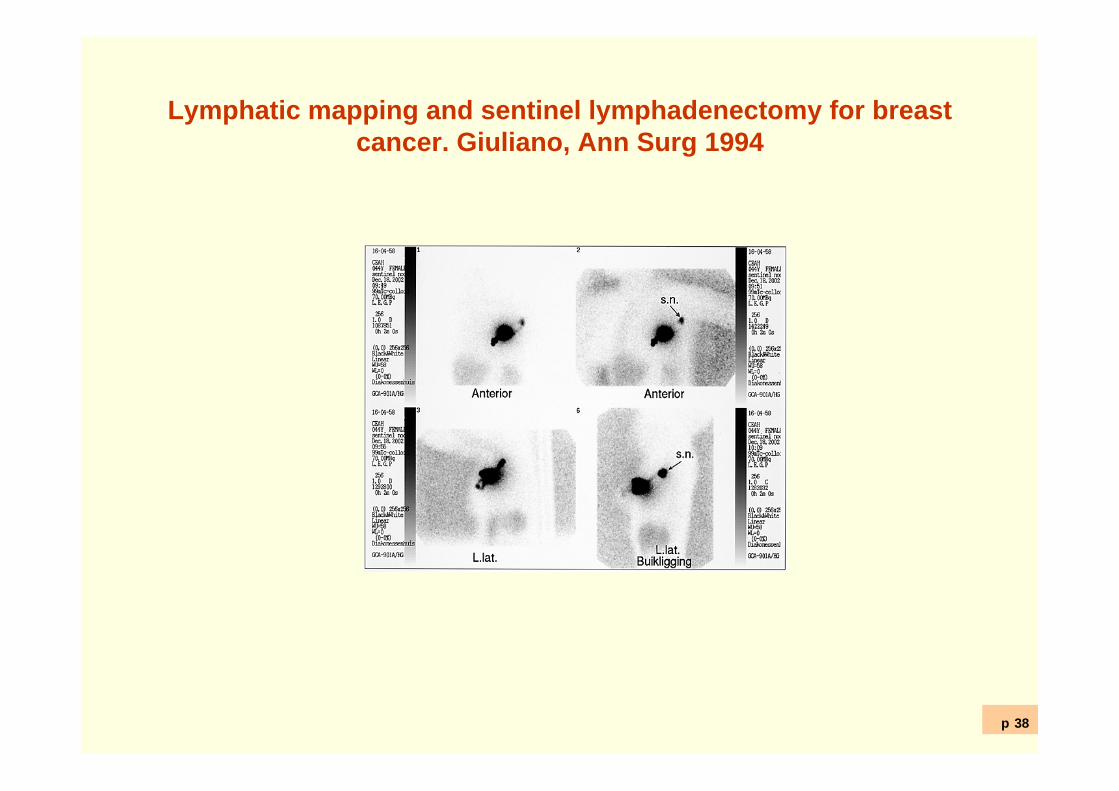
Lymphatic mapping and sentinel lymphadenectomy for breastcancer. Giuliano, Ann Surg 1994
p 39
Less is more?Borstkanker II
Mammasparende therapie: cosmetisch superieur
Schildwachtklierprocedure: morbiditeit oksel <<

p 40
Less is more?schildwachtklierprocedure
………bespaart ca. 50% van de vrouwen met
borstkanker een okselklierdissectie

p 41
Less is more?Maligne melanoom
• 1 vs 3 cm excision of /Meirion Thomas

p 42
Less is more?laparosopie
Systematic review on the short-term outcomeof laparoscopic resection for colon and
rectosigmoid cancerJ. J. Tjandra and M. K. Y. Chan
p 43
Mag het iets minder?colonchrirurgie
Laparoscopie: sneller herstel

p 44
Less is more?colonchirurgie
Sneller herstel
…… een beetje een troostprijs

p 45
Lacy 2002(Lancet)
RCT: lap. vs. open colonchirurgie
single institution
n=219

p 46
Lacy 2002 (Lancet) RCT: lap. vs. open colonchirurgie
Laparoscopisch = beter dan open
HR overlijden = 0.48 (0.23-1.01)HR recidief ziekte = 0.38 (0.19-0.82)
p 47
Lacy 2008 (Lancet Oncol) RCT: lap. vs. open colonchirurgie
zelfde trial, 8 jaar FU
idem

p 48
= veelbelovend

p 49
,echter
RCT: lap. vs. open colonchirurgie
multicentre, (o.a. Barcelona)
n=1200
p 50
Buunen 2009 (Lancet oncology) RCT: lap. vs. open colonchirurgie
Laparoscopisch ≠ beter dan open
OS: 82 vs 84% (p=0.45)DFS, etc vergelijkbaar
p 51
Buunen 2009 (Lancet oncology) RCT: lap. vs. open colonchirurgie
Laparoscopisch ≠ beter dan open
“…. cannot rule out difference in favour of open colectomy.
……..however, difference in dfs betweengroups justifies implementation of
laparosopic surgery into daily practice”

p 52
Less is more?colonchirurgie
Hm!

p 53
Vgl.
"We are in possession of what I think to becompelling evidence that SaddamHussein has, and has had for a numberof years, a developing capacity for the production and storage of weapons of mass destruction.",
December 2002

p 54
chirurgische oncologietrends
meer ≠ beter
mag het iets minder?
meer is beter!!

p 55
Mag het iets minder?
zuiniger chirurgie geeft minder ellende

p 56
Mag het iets minder?
……, maar daar wordt nog wel een prijs voor
betaald.

p 57
voorbeeld 1Comparing radical mastectomy with quadrantectomy, axillary dissection, and radiotherapy in patients with
small cancers of the breastVeronesi, NEJM 1981
*
2002

p 58
Voorbeeld 2Schildwachtklierprocedure niet 100% sensitief
3.5% van alle patienten met een “schone”SWK heeft toch lymfogene metastasen,
………..en dat accepteren we
p 59
chirurgische oncologie
meer ≠ beter
kan vaak met minder net zo goed

p 60
chirurgische oncologietrends
meer was niet beter
mag het iets minder?
meer toch beter!!!
p 61
meer is beter
volume
vs.
uitkomst
p 62
meer is beter
Invloed van ziekenhuis- en chirurg volume
1. morbiditeit / mortaliteit
2. overleving
p 63
a systematic review of the impact of volume of surgeryand specialization om patient outcome.
Chowdhury Br J Surg 2007
long, pancreas, oesofagus, colorectaal, lever,
schildklier, ..

p 64
meer is beterprobleem:
wat is “high”, wat is “low”

p 65
meer is beteroplossing?
regionalisering van zorg?
“oncocentra”

p 66
meer is beteroplossing?
“politiek gevoelig”
p 67
meer is beteroplossing?
concentratie van zorg is een probleem
spelers: IKC’s, UMC’s, alg. ziekenhuizen, patienten,
ziektekostenverzekeraars

p 68
chirurgische oncologie
meer ≠ beter
minder vaak net zo goed
vaker doen is echt beter

p 69
chirurgisch oncologie
veranderende rol voor de chirurg

p 70
grootste rek is eruit
2009
p 71
chirurgisch oncoloog
grens aan de opbrengst van eigen handelen
recente winst vooral op niet chirurgische terreinen

p 72
chirurgisch oncoloog
grens aan de opbrengst van eigen handelen
recente winst vooral op andere terreinen
besef belang multidisciplinaire aanpak

p 73
Combination chemotherapy as an adjuvant treatment in operablebreast cancer
Bonadonna, NEJM 1976
CMF vs. –n=386
5% vs 24% recidief ziekte
(FU=27 mnd)

p 74
chirurgisch oncoloog
belangrijke rol in multidisciplinair team

p 75
chirurgisch oncoloogin multidisciplinair team
TME trial + preoperatieve RT
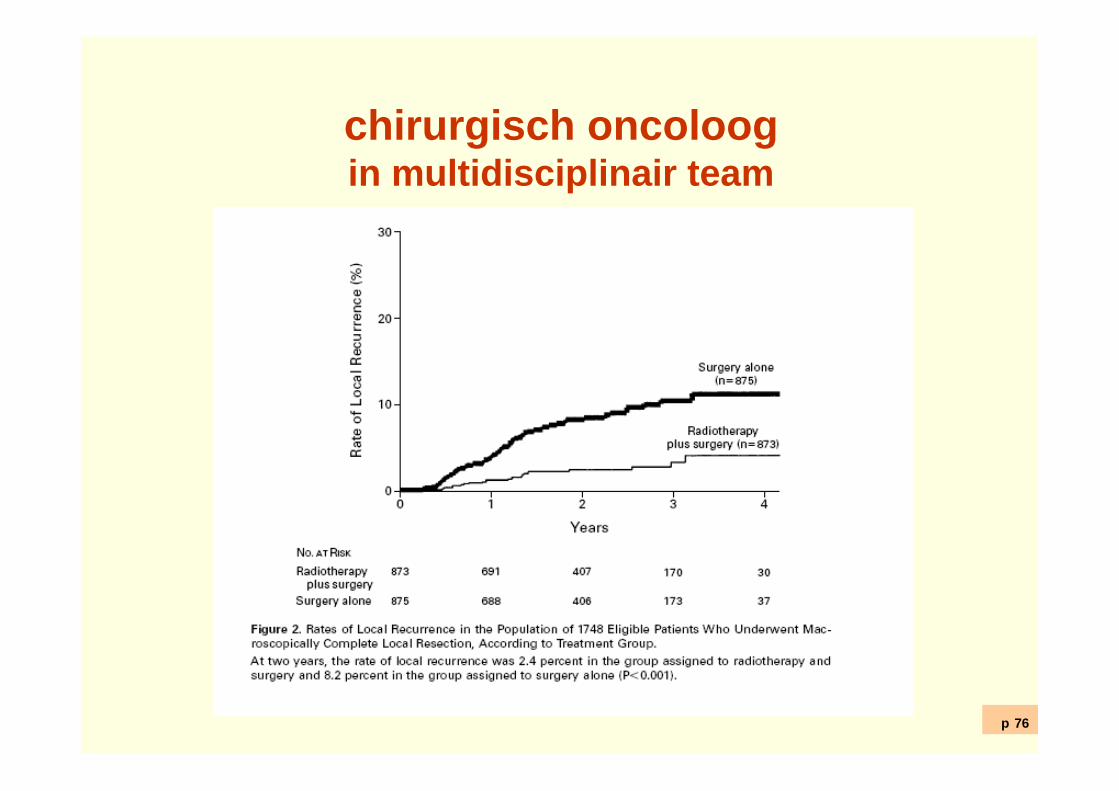
p 76
chirurgisch oncoloogin multidisciplinair team
TME trial + preoperatieve RT
6 vs 2% lokaal recidieven

p 77
grootste rek is eruit
2009
p 78
chirurgisch oncoloog
rol in multidisciplinair team
verantwoordelijk voor volume