chapter 6 – physiotherapy assessment of the hypermobile adult
DESCRIPTION
movimientoTRANSCRIPT

CHAPTER CONTENTS
Introduction 67
Recognition 68
Hypermoblllty, Instability and the hypermobilitysyndrome 69
Assessment of the JHS patient 71Symptoms 71Associated problems 74Previous history 74Physical examination 75
Observation 75Static posture 76Active movement testing 77Measuring hypermobility 79Passive movement testing 80Palpation 81
Women's health 81
6
Physiotherapyassessment of thehypermobile adult
Rosemary Keer
Conclusion 83 Aims1. To discuss how joint hypermobility syndrome
(JHS) presents in the adult2. To provide guidelines to aid recognition of the
syndrome3. To discuss possible mechanisms for the
production of symptoms reported by JHSpatients
4. To discuss possible implications of JHS in thepregnant woman
INTRODUCTION
Joint hypermobility syndrome (JHS), a collectionof musculoskeletal symptoms associated withgeneralized hypermobility of the joints, is underdiagnosed (Beighton et al. 1999) and frequentlyunrecognized by doctors and physical therapists.Physiotherapists are experienced in performingcomprehensive neuromusculoskeletal examinations and, as such, are well placed to identifyand treat joint hypermobility syndrome suffererseffectively. However, although physiotherapistsare familiar with the joint laxity caused by damage to ligaments in an isolated joint, such as ananterior cruciate-deficient knee, they have lessexperience of dealing with the consequences ofgeneralized laxity, as seen in the JHS patient. Thischapter aims to raise awareness of the condition,to aid recognition and understanding, and toexplore possible reasons why generalized hypermobility may cause problems.
67
68 HYPERMOBILITY SYNDROME
RECOGNITION
Recognition and understanding are the mostimportant factors in managing JHS for patientand physiotherapist alike. Recognition is oftendifficult. One of the main reasons for this wouldappear to be that JHS patients do not exhibit manyof the signs normally associated with painfulmusculoskeletal conditions. They frequently present with no reduction in range of movement andoften have no signs of inflammation (Russek 1999).A large part of the physiotherapist's examinationis concerned with the assessment of restrictedmovement, and when faced with a patient whohas a good range of movement there is a dangerthat it can lead to their condition being misunderstood, as the symptoms do not appear to fit withthe signs. At its worst, it can result in the patientbeing labelled as suffering from a psychologicaldisorder, with unhelpful comments such as 'it isall in the mind' being reported by patients inthe clinic and also in the literature (Child 1986,Lewkonia and Ansell 1983).
Physiotherapists, partly because of time constraints, can also be guilty of focusing on the mainproblem area during the examination, rather thanthe whole patient, and consequently miss the factthat the patient is displaying generalized hypermobility. Joint hypermobility is common (Larssonet al. 1995) and it is worth remembering that tomany, hypermobility poses no problems and canactually be of benefit (Larsson et al. 1993). However, there is a huge spectrum of presentations,ranging from the accomplished ballet dancer andgymnast who demonstrates marked hypermobility without suffering from the syndrome, tosomeone who is suffering from the syndromewith severe symptoms and may be relatively disabled and reliant on aids or in a wheelchair.
Recognizing JHS can be difficult becausepatients are often unable to give a reason for theonset of symptoms. Trivial everyday activitiescan cause significant pain, making them feel thatthere is something seriously wrong. Recognizingand understanding the condition ensure that the
patient is reassured that they are not sufferingfrom a life-threatening disorder, and also that thecondition can be successfully managed.
Patients often consult a physiotherapist without a diagnosis of JHS and it is important for avariety of reasons that, when present, the condition is recognized. Patients have often seen manydifferent practitioners, including doctors, physiotherapists, osteopaths, chiropractors and alternative therapists, without having been given adiagnosis, gaining no significant benefit, and insome cases they are actually made worse. Thissearch for help often leaves patients angry withthe medical profession, anxious and depressed.
Recognizing the syndrome also ensures thatpatients can get appropriate treatment.
Cherpel and Marks (1999) state that althoughjoint hypermobility is a common phenomenon, itis possibly undertreated or inappropriately treatedowing to a lack of basic knowledge about the condition. At its worst, this can lead to the patientundergoing a battery of unnecessary tests, invasiveorthopaedic procedures or inappropriate use ofpotent antirheumatic drugs (Lewkonia and Ansell1983),which only serves to increase suffering withno discernible benefit.
There is evidence to suggest that JHS predisposes to several articular and non-articularlesions (EI-Shahaly and EI-Sherif 1991), and eventhe early onset of osteoarthritis (OA) (Kirk et al.1967, Bird et al. 1978). It is important that patientsare aware of this possibility and given helpfulinformation and education to help prevent orreduce this potential complication. It is also possible that by recognizing the condition early andimplementing appropriate treatment and advice,the JHS patient can be prevented from becominga chronic pain sufferer.
Many sufferers report that physical therapy inthe past has made them worse, and this is almostcertainly because the condition was not identified.In JHS the collagenous tissues in the body are lessresilient and therefore more vulnerable to injury(Acasuso-Diaz et al. 1993) and musculoskeletaldisorders (Bridges et al. 1992). An appreciation of

PHYSIOTHERAPY ASSESSMENT OF THE HYPERMOBILE ADULT 69
this is necessary to avoid exacerbating symptoms or, even worse, causing further damage. Forthe physiotherapist it is therefore important totake extra care when handling the hypermobilepatient's tissues, both in examination and in treatment. Clinical experience also suggests that theJHS patient takes longer to treat. This is due tothe Widespread nature of symptoms, the lengthof time they have had problems - in some casesfor many years, which causes them to becomedeconditioned - and because their tissues takelonger to heal (Russek 2000).
HYPERMOBILITY, INSTABILITY ANDTHE HYPERMOBILITY SYNDROME
Hypermobility is said to be present when thereis an increase in the range of movement at a jointbeyond the accepted norm. This may apply toone joint in isolation, such as a ligament injury inthe knee following trauma. Generalized hypermobility is said to be present when many joints inthe body have an increased range of movement.This can be seen in certain groups of people, suchas gymnasts and ballet dancers (Gannon and Bird1999). In this group of people the increased mobility is considered to be the upper extreme of a widenormal variation in joint mobility, some of whichmay have been gained through training. This canbe considered an asset (Larsson et al. 1993), andappears to convey an elegance and grace to theirmovements. Many individuals with generalizedhypermobility do not appear to have any problems associated with their increased flexibility.
Joint hypermobility syndrome, however, isdefined as generalized joint laxity with associatedmusculoskeletal complaints in the absence of anysystemic disease (Kirk et al. 1967). JHS has beenshown to be an inherited form of generalizedconnective tissue disorder (Grahame 1999). It ispresumed that it is the increased mobility that iscontributing to the complaints of musculoskeletalsymptoms. However, Kirk et al. (1967) found thata higher hypermobility joint score did not always
accompany severe complaints or a more widespread pattern of referral. It is not known whatcauses the pain associated with JHS, but severaltheories have been proposed. Some believe painis produced as a result of joint microtrauma fromoveruse and misuse (Kirk et al. 1967, Russek 2000)of tissues that have an inherent weakness in theircollagen structure. Child (1986) suggeJits pain isdue to sensory nerve endings which are overstimulated by stretch, but which are poorly supportedby collagen fibrils and hence are overstimulated asthe lax capsule is stretched. It is clear that the painassociated with hypermobility may begin as alocalized joint pain, but frequently develops into achronic pain with alterations in central nervoussystem processing. There is also evidence to suggest that dysfunction in the autonomic nervoussystem may playa part (Gazit et al. 2003).
From a physiotherapy management point ofview, it is helpful to look in more detail at thetheories behind hypermobility or increased jointmobility and why it can sometimes cause problems. One of the mechanisms involved in thedevelopment of symptoms is likely to be a lack ofcontrol of the hypermobile joint range. This willmake it more susceptible to injury from overuseand misuse, or even normal use. The issue thenis one of joint stability. Stability is dynamic anddefined as the ability to transfer load effectively,and it follows that a stable joint is less likely tocause problems.
Panjabi (1992a) proposes a model of spinalstability and movement which can be applied toother joints in the body. He suggests that jointstability is dependent on three subsystems whichare functionally interdependent (Fig. 6.1):
1. Passive musculoskeletal subsystem, whichincludes the bones and the shape of thearticulating surfaces, ligaments, joint capsulesand the passive mechanical properties ofmuscle;
2. Active musculoskeletal subsystem, whichconsists of the muscles and tendonssurrounding the joint;
70 HYPERMOBILITY SYNDROME
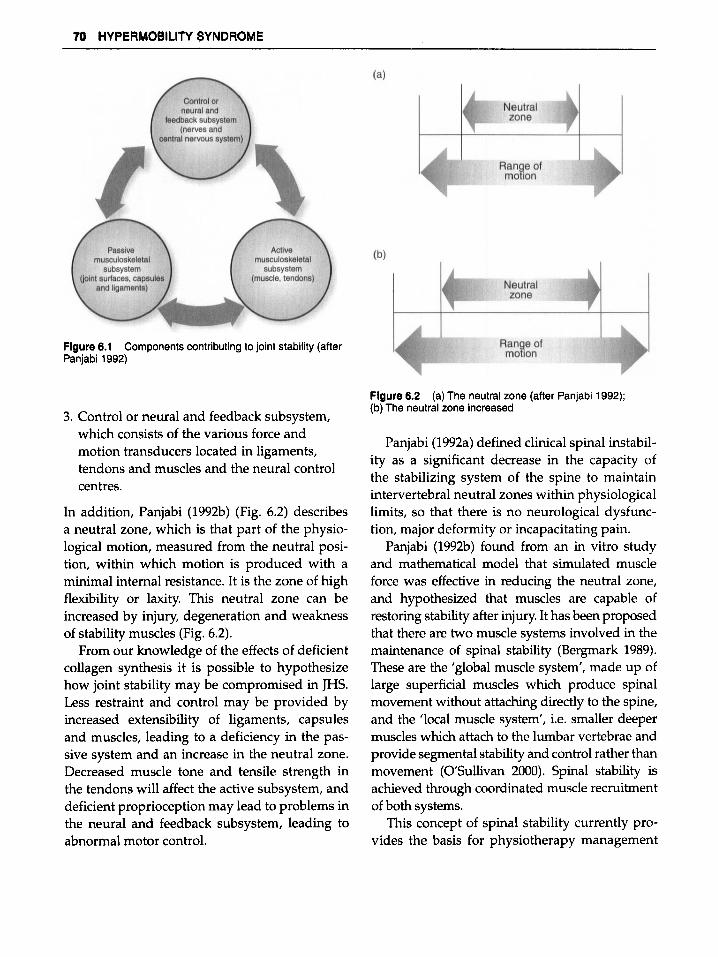
Figure 6.1 Components contributing to joint stability (afterPanjabi 1992)
3. Control or neural and feedback subsystem,which consists of the various force andmotion transducers located in ligaments,tendons and muscles and the neural controlcentres.
In addition, Panjabi (1992b) (Fig. 6.2) describesa neutral zone, which is that part of the physiological motion, measured from the neutral position/ within which motion is produced with aminimal internal resistance. It is the zone of highflexibility or laxity. This neutral zone can beincreased by injury, degeneration and weaknessof stability muscles (Fig. 6.2).
From our knowledge of the effects of deficientcollagen synthesis it is possible to hypothesizehow joint stability may be compromised in JHS.Less restraint and control may be provided byincreased extensibility of ligaments, capsulesand muscles, leading to a deficiency in the passive system and an increase in the neutral zone.Decreased muscle tone and tensile strength inthe tendons will affect the active subsystem, anddeficient proprioception may lead to problems inthe neural and feedback subsystem, leading toabnormal motor control.
Figure6.2 (a) The neutral zone (after Panjabi 1992);(b) The neutral zone increased
Panjabi (1992a) defined clinical spinal instability as a significant decrease in the capacity ofthe stabilizing system of the spine to maintainintervertebral neutral zones within physiologicallimits, so that there is no neurological dysfunction/ major deformity or incapacitating pain.
Panjabi (1992b) found from an in vitro studyand mathematical model that simulated muscleforce was effective in reducing the neutral zone,and hypothesized that muscles are capable ofrestoring stability after injury. It has been proposedthat there are two muscle systems involved in themaintenance of spinal stability (Bergmark 1989).These are the 'global muscle system', made up oflarge superficial muscles which produce spinalmovement without attaching directly to the spine,and the 'local muscle system', i.e. smaller deepermuscles which attach to the lumbar vertebrae andprovide segmental stability and control rather thanmovement (O'Sullivan 2000). Spinal stability isachieved through coordinated muscle recruitmentof both systems.
This concept of spinal stability currently provides the basis for physiotherapy management

PHYSIOTHERAPY ASSESSMENT OF THE HYPERMOBILE ADULT 71
of JHS, which is concerned with improvingthe stability and control of hypermobile joints.There has been little research to validate thisapproach, although the studies by Barton and Bird(1996) and Kerr et a1. (2000) have shown positiveeffects from a joint stabilization programme inJHS patients. In addition, work by Richardsonet a1. (1999) and O'Sullivan (2000) on segmentalstabilization is providing evidence of the efficacyof this approach in the treatment of low backpain, and much of this can be applied to themanagement of JHS.
This hypothesis of instability may go someway to explain why the JHS patient suffers painfrom seemingly normal or everyday activities,and why they appear to prefer resting at the endof range where they feel more secure. It may alsoexplain why the hypermobility syndrome affectsmany more females than males. Females havea tendency to increased range of movement andless muscle bulk, although a hormonal or geneticfactor may also be involved. This hypothesisdoes not, however, explain why some hypermobile individuals have no problems whereasothers have many, and further research in thisarea is clearly needed.
ASSESSMENT OF THE JHS PATIENT
Recognizing JHS as a cause for a patient's symptoms can be difficult. A range of characteristicswhich can help the physiotherapist identify anddiagnose JHS are discussed. These have beenidentified from clinical experience and research.It should be stressed that patients will not sufferall the symptoms discussed.
The gender of the patient can be relevant, asJHS is more common in females than males.Grahame (1986) found that 2% of 9275 patientsattending a rheumatology clinic were diagnosedwith JHS, and of these 85% were female.
Ethnicity is also important, as different raceshave different mobility characteristics. Joint hypermobility varies in prevalence from 5% of a cohort
of blood donors in the USA (Jessee et a1. 1980) tobetween 25% and 38% in a cohort of studentsin Iraq (Al-Rawi et a1. 1985). Asian Indians werefound by Wordsworth et a1. (1987) to be significantly more mobile than English Caucasians.
The dominant side is usually less mobile thanthe non-dominant side (Verhoeven et a1. 1999),owing to the tendency for more muscle development on the dominant side through increaseduse, or possibly better motor control.
Symptoms
If the patient has arrived without a diagnosisof JHS, recognition is often difficult because thepatient looks well and moves well. It is temptingto think they are overemphasizing their pain andcomplaints. This is often because they have beenbadly managed in the past by medical practitioners and other health professionals who havefailed to listen to them and heed their message.They need to feel that they have finally foundsomeone who will listen to them and believethem. It is advisable to allow extra time for thefirst assessment, as there is usually a long andcomplicated history, with symptoms involvingmany different areas.
The main complaint is pain, often widespread,diffuse and longstanding, going back from a fewmonths to several years. One study found theduration of musculoskeletal complaints associated with JHS to range from 15 days to 45 years(El-Shahaly and El-Sherif 1991). There may beother symptoms, including stiffness (Kirk et a1.1967), clicking, clunking, subluxations, paraesthesiae, and some rather more bizarre symptoms,such as feeling 'like a bag of fleas' (personalcommunication) .
These Widespread symptoms often do not fitwith how the patient looks or moves (Russek2000),and in addition they may also report feelingunwell, suffering flu-like symptoms, feeling faintand being particularly tired. It is worth askingabout other areas, as they may not volunteer information for fear of sounding like a hypochondriac
72 HYPERMOBlllTY SYNDROME
(Russek 2000, Lewkonia and Ansell 1983). Gettingthe complete picture not only helps with the diagnosis but gives the patient confidence that someone is really listening to them. It is helpful to letthe patient talk, with the physiotherapist trying toresist the temptation to be too closed in their questioning. A lot of very useful information can begained which will be helpful in piecing togetherthe jigsaw puzzle.
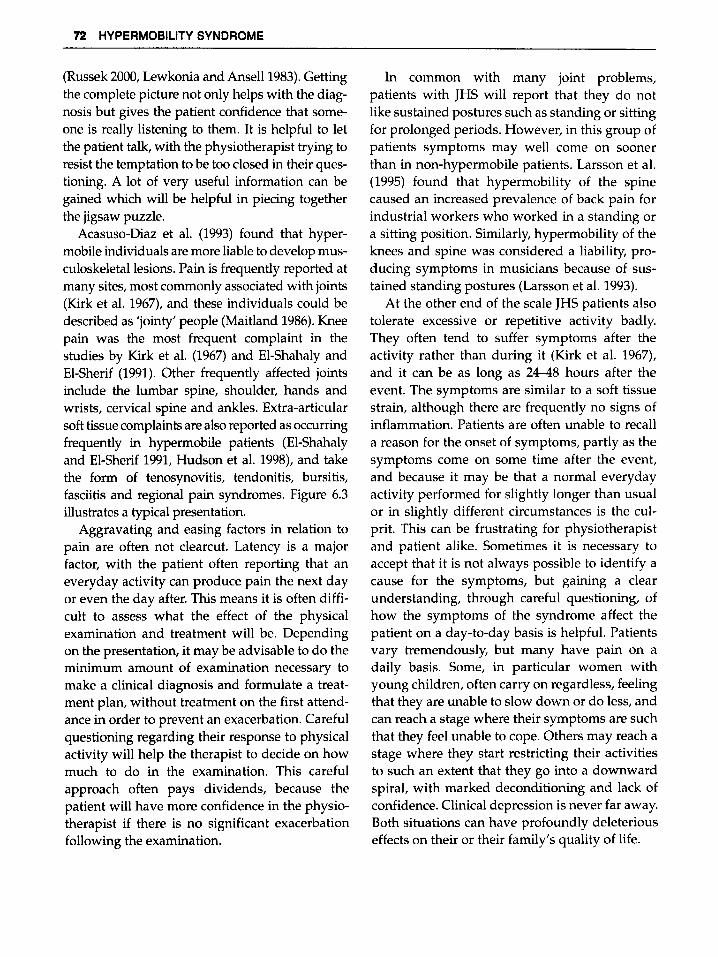
Acasuso-Diaz et al. (1993) found that hypermobile individuals are more liable to develop musculoskeletallesions. Pain is frequently reported atmany sites, most commonly associated with joints(Kirk et al. 1967), and these individuals could bedescribed as 'jointy' people (Maitland 1986). Kneepain was the most frequent complaint in thestudies by Kirk et al. (1967) and El-Shahaly andEl-Sherif (1991). Other frequently affected jointsinclude the lumbar spine, shoulder, hands andwrists, cervical spine and ankles. Extra-articularsoft tissue complaints are also reported as occurringfrequently in hypermobile patients (El-Shahalyand El-Sherif 1991, Hudson et al. 1998), and takethe form of tenosynovitis, tendonitis, bursitis,fasciitis and regional pain syndromes. Figure 6.3illustrates a typical presentation.
Aggravating and easing factors in relation topain are often not clearcut. Latency is a majorfactor, with the patient often reporting that aneveryday activity can produce pain the next dayor even the day after. This means it is often difficult to assess what the effect of the physicalexamination and treatment will be. Dependingon the presentation, it may be advisable to do theminimum amount of examination necessary tomake a clinical diagnosis and formulate a treatment plan, without treatment on the first attendance in order to prevent an exacerbation. Carefulquestioning regarding their response to physicalactivity will help the therapist to decide on howmuch to do in the examination. This carefulapproach often pays dividends, because thepatient will have more confidence in the physiotherapist if there is no significant exacerbationfollowing the examination.
In common with many joint problems,patients with JHS will report that they do notlike sustained postures such as standing or sittingfor prolonged periods. However, in this group ofpatients symptoms may well come on soonerthan in non-hypermobile patients. Larsson et al.(1995) found that hypermobility of the spinecaused an increased prevalence of back pain forindustrial workers who worked in a standing ora sitting position. Similarly, hypermobility of theknees and spine was considered a liability, producing symptoms in musicians because of sustained standing postures (Larsson et al. 1993).
At the other end of the scale JHS patients alsotolerate excessive or repetitive activity badly.They often tend to suffer symptoms after theactivity rather than during it (Kirk et al. 1967),and it can be as long as 24-48 hours after theevent. The symptoms are similar to a soft tissuestrain, although there are frequently no signs ofinflammation. Patients are often unable to recalla reason for the onset of symptoms, partly as thesymptoms come on some time after the event,and because it may be that a normal everydayactivity performed for slightly longer than usualor in slightly different circumstances is the culprit. This can be frustrating for physiotherapistand patient alike. Sometimes it is necessary toaccept that it is not always possible to identify acause for the symptoms, but gaining a clearunderstanding, through careful questioning, ofhow the symptoms of the syndrome affect thepatient on a day-to-day basis is helpful. Patientsvary tremendously, but many have pain on adaily basis. Some, in particular women withyoung children, often carry on regardless, feelingthat they are unable to slow down or do less, andcan reach a stage where their symptoms are suchthat they feel unable to cope. Others may reach astage where they start restricting their activitiesto such an extent that they go into a downwardspiral, with marked deconditioning and lack ofconfidence. Clinical depression is never far away.Both situations can have profoundly deleteriouseffects on their or their family's quality of life.

PHYSIOTHERAPY ASSESSMENT OFTHE HYPERMOBILE ADULT 73
Figure 6.3 Typical symptoms in a JHS patient
Stiffness is a frequently reported symptom,with some complaining that they 'feel like a90-year-old' when getting up in the morning. Thissubjective feeling of stiffness is often at oddswith their range of movement on examination.Although their range of movement may looknormal to the physiotherapist, questioning frequently reveals that it is restricted in comparisonto the patient's normal range of movement. Thisis seen particularly in the middle-aged patient
who has lost much of their former mobility. Inthe older patient, stiffness may be due to a generaldecrease in mobility with age (Seow et al. 1999),or secondary to joint injury or osteoarthritis. It isworth asking the patient if they were more flexible when younger, and a question such as 'haveyou ever been able to touch the floor with yourpalms flat' (Oliver 2000)often gives a clue to theirprevious flexibility and possible hypermobility.In addition, it may be helpful to ask whether

74 HYPERMOBILITY SYNDROME
they did ballet or gymnastics, as less flexiblechildren do not usually do well in these activities.The importance of historical hypermobility hasbeen acknowledged in the revised BrightonCriteria (Grahame et al. 2000), which in combination with other criteria can help with a diagnosisofJHS.
Hypermobile people often describe themselvesas uncomfortable or fussy people who are constantly fidgeting and trying to get into a comfortable position (Oliver 2000). Russek (2000) describesa patient who complained of pain from where herbody contacted the bed, and that this was relievedby using a thick feather comforter. This aspect ofthe hypermobility syndrome is reminiscent of thestory of the Princess and the Pea, and perhapssuggests she was also a sufferer.
JHS is a heritable disorder and, on questioning, the patient may tell you that siblings, children or parents are similarly affected. Biro (1983)found that 27% of his cohort of patients had otherfamily members with hypermobility, and Bridgeset al. (1992) and Finsterbush and Pogrund (1982)found that 65% of their patients had first-degreerelatives with a history of joint hypermobility. If apatient is unable to identify whether their relatives are hypermobile, it is worth asking if anyof their relatives were gymnasts or dancers, orsuffered from any joint problems. This will oftenreveal that a family member has had many diffuse chronic joint problems over the years, oftenhaving been given many diagnoses, such asosteoarthritis, spondylosis or disc prolapse without the symptoms being identified as due to JHS.Russek (2000) gives a good illustration of this.
Associated problems
As the hypermobility syndrome affects collagenous tissue there can be associated problems inother body systems. It is worth asking aboutother areas with this in mind. The presence ofsome of these can help to confirm the diagnosis.
There is evidence to suggest that uterine prolapse (El-Shahaly and El-Sherif 1991,Al-Rawi and
Al-Rawi 1982) and abdominal hernias (WynneDavies 1971) are more common in JHS. Nortonet al. (1995) found a significantly higher frequencyof cystocele (P = 0.001), rectocele (P = 0.0002)and uterine prolapse (P = 0.0002) in women withhypermobility than in non-hypermobile women.Interestingly, there was no increased prevalenceof stress incontinence in the hypermobile women.Tincello et al. (2002) likewise found that hypermobility was not associated with urinary incontinence, except that elbow hyperextension wasassociated with an increased incidence of postnatal urinary incontinence.
Patients report that they bruise very easily,noticing a bruise when they have no recollectionof knocking themselves. Pitcher and Grahame(1982), Bulbena (1992), Bridges et al. (1992) andKaplinsky et al. (1998) all report that easy bruisingcan be a feature of the hypermobility syndrome.
It has been suggested that patients with hypermobile joints often have laxity involving bloodvessels (Bird and Barton 1993), and an increasedincidence of varicose veins has been reportedby El-Shahaly and El-Sherif (1991).There is also apossible association with Raynaud's phenomenon, as this has been reported as being moreprevalent in a hypermobile group (Al-Rawi et al.1985, El-Garf et al. 1998).
The presence of neuropathies has also beenassociated with hypermobility. Francis et al. (1987)report that nine out of 11 consecutive patientswith tarsal tunnel syndrome were identified ashaving generalized hypermobility, and Marchet al. (1988) report on three patients in whom carpaltunnel syndrome was due to unusual sleep postures enabled by their joint hypermobility. Theymake the comment that identification of jointhypermobility and early management may meanthat surgery is not needed in many cases.
Previous history
Previous injury can give an indication of howoften and how easily a patient has injured themselves in the past. Hudson et al. (1998) found that

PHYSIOTHERAPY ASSESSMENT OFTHE HYPERMOBILE ADULT 75
hypermobile patients presenting to a rheumatology clinic were found to have significantly moreprevious episodes of soft tissue rheumatism(STR) and significantly more recurrent episodesat one site than non-hypermobile patients. Thisstudy also suggests that repetitive activity maybe a contributing factor to the development ofsymptoms in some hypermobile individuals.Details of the type of activity the patient is regularly performing will help to identify possiblemechanisms of injury and help in future management to prevent recurrences. A history of previous joint and soft tissue injury, in addition toindicating a possible diagnosis of JHS, will alsogive an indication of the speed of healing, whichtends to be slower in these patients (Russek 2000).
Joint dislocations and subluxations aremore common in people with hypermobility(Finsterbush and Pogrund, 1982). Spontaneousrelocation usually occurs, particularly after thefirst time. Subsequent dislocations and subluxations often occur with no trauma, and someindividuals can sub lux and relocate a joint at willwith little discomfort. The literature suggests theshoulder and patella to be the most frequentlyaffected in adults (Beighton et a1. 1989).
A history of pain in childhood or adolescencemay be a further clue to the diagnosis of JHS.Pain in the knee, foot, ankle and back appears tobe the most common, in descending order. Thepatient may also have complained of growingpains and delayed walking. This aspect is discussed in more detail in Chapter 4.
Patients frequently report that manual therapyhas made them worse, or at best has failed tohelp. This is a useful piece of information, notonly as a clue to a possible diagnosis of JHS, butalso to ensure that similar techniques are notused again. It is unclear why manual therapymay aggravate the symptoms of JHS, but failingto recognize hypermobility and performing techniques too vigorously could be one explanation.
Box 6.1 gives a list of additional questions toask during the subjective examination which canhelp in diagnosing JHS.
Box 6.1 Examples of additional questions that can beused to aid recognition of JHS
Previous historyDid they have pain as a child?Did they have growing pains?Did they do gymnastics or ballet when younger?Were they more flexible when younger?Did they feel better/worse in pregnancy?Have they had any dislocations/subluxations?Have they had many fractures?How have they responded to analgesia?
Present historyIs there a family history of increased fleXibility?Do they dislike sustained postures, such as standing,
sitting?Do they dislike too much activity?Do they bruise easily?Do they have any herniae, varicose veins or prolapses?Are they uncomfortable or fussy people?Do they have any neuropathies?Do they have Raynaud's phenomenon?
Physical examination
ObservationObservation starts from the moment a patientwalks into the room. Clues that may lead thephysiotherapist to begin to suspect JHS are theposition the patient chooses to sit in the chair,and the movement of their hands. As previouslymentioned, hypermobile patients often fidgetand do not sit in one position for very long. Theyalso often choose to sit in awkward positions,such as with one leg wrapped around the chairleg, or to side sit (Oliver 2000).This appears to bein an attempt to find more stability, using end-ofrange positions, relying on tension in their ligaments, rather than resting in a neutral, midrangeposition where there is more movement and lessstability. They frequently use their hands in anexpressive way when talking, and increasedmobility can often be observed in the metacarpalor interphalangeal joints (Fig. 6.4).
Skin can be thinner, stretchier and subject tostriae, which are not due to a large weight change(Child 1986, Grahame 1989). Striae can often beseen at the base of the spine, around the thighs,shoulders and knees. Scar formation is oftenpapyraceous or tissue-paper thin, and it is worth
76 HYPERMOBILITY SYNDROME
Figure 6.4 Hypermobility in the hands
looking at injection sites, childhood scars orsurgery scars to assess tissue healing.
Muscle bulk may be decreased in certainmuscles and hypermobile patients frequentlyhave a lower muscle tone. Kirk et al. (1967) notedthat several of their group of hypermobilepatients had poor muscular development.
Static posture
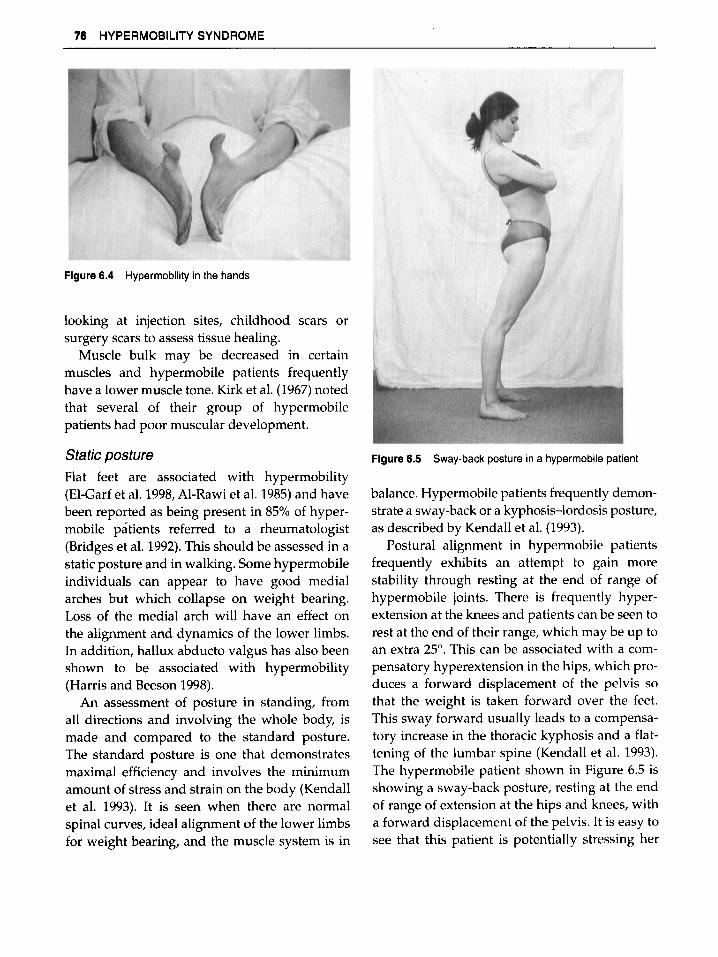
Flat feet are associated with hypermobility(El-Carf et al. 1998,Al-Rawi et al. 1985) and havebeen reported as being present in 85% of hypermobile patients referred to a rheumatologist(Bridges et al. 1992).This should be assessed in astatic posture and in walking. Some hypermobileindividuals can appear to have good medialarches but which collapse on weight bearing.Loss of the medial arch will have an effect onthe alignment and dynamics of the lower limbs.In addition, hallux abducto valgus has also beenshown to be associated with hypermobility(Harris and Beeson 1998).
An assessment of posture in standing, fromall directions and involving the whole body, ismade and compared to the standard posture.The standard posture is one that demonstratesmaximal efficiency and involves the minimumamount of stress and strain on the body (Kendallet al. 1993). It is seen when there are normalspinal curves, ideal alignment of the lower limbsfor weight bearing, and the muscle system is in
Figure 6.5 Sway-back posture in a hypermobile patient
balance. Hypermobile patients frequently demonstrate a sway-back or a kyphosis-lordosis posture,as described by Kendall et al. (1993).
Postural alignment in hypermobile patientsfrequently exhibits an attempt to gain morestability through resting at the end of range ofhypermobile joints. There is frequently hyperextension at the knees and patients can be seen torest at the end of their range, which may be up toan extra 25°. This can be associated with a compensatory hyperextension in the hips, which produces a forward displacement of the pelvis sothat the weight is taken forward over the feet.This sway forward usually leads to a compensatory increase in the thoracic kyphosis and a flattening of the lumbar spine (Kendall et al. 1993).The hypermobile patient shown in Figure 6.5 isshowing a sway-back posture, resting at the endof range of extension at the hips and knees, witha forward displacement of the pelvis. It is easy tosee that this patient is potentially stressing her
PHYSIOTHERAPY ASSESSMENT OF THE HYPERMOBILE ADULT rt
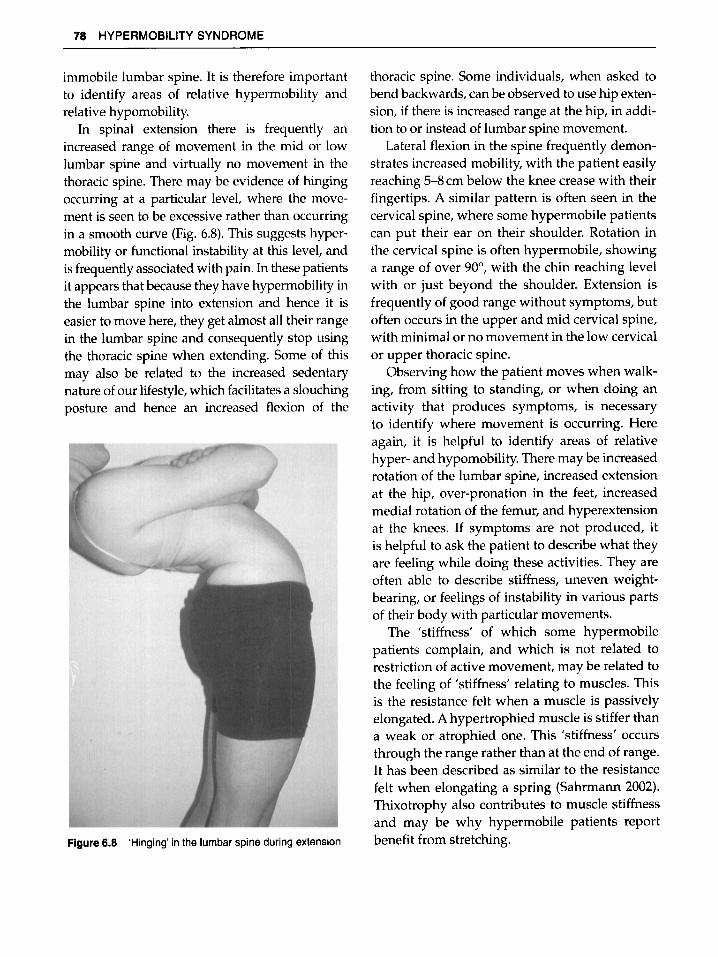
Figure 6.7 Increased thoracic spinal flexion during forwardspinal flexion
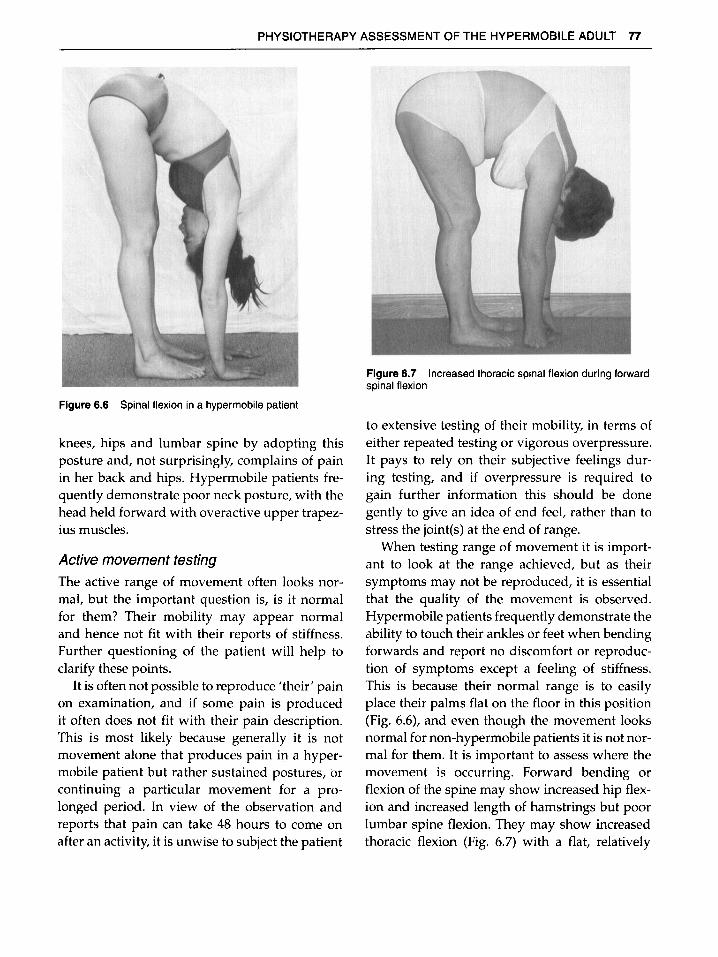
Figure 6.6 Spinal flexion in a hyper mobile patient
knees, hips and lumbar spine by adopting thisposture and, not surprisingly, complains of painin her back and hips. Hypermobile patients frequently demonstrate poor neck posture, with thehead held forward with overactive upper trapezius muscles.
Active movement testingThe active range of movement often looks normal, but the important question is, is it normalfor them? Their mobility may appear normaland hence not fit with their reports of stiffness.Further questioning of the patient will help toclarify these points.
It is often not possible to reproduce 'their' painon examination, and if some pain is producedit often does not fit with their pain description.This is most likely because generally it is notmovement alone that produces pain in a hypermobile patient but rather sustained postures, orcontinuing a particular movement for a prolonged period. In view of the observation andreports that pain can take 48 hours to come onafter an activity, it is unwise to subject the patient
to extensive testing of their mobility, in terms ofeither repeated testing or vigorous overpressure.It pays to rely on their subjective feelings during testing, and if overpressure is required togain further information this should be donegently to give an idea of end feel, rather than tostress the joint(s) at the end of range.
When testing range of movement it is important to look at the range achieved, but as theirsymptoms may not be reproduced, it is essentialthat the quality of the movement is observed.Hypermobile patients frequently demonstrate theability to touch their ankles or feet when bendingforwards and report no discomfort or reproduction of symptoms except a feeling of stiffness.This is because their normal range is to easilyplace their palms flat on the floor in this position(Fig. 6.6), and even though the movement looksnormal for non-hypermobile patients it is not normal for them. It is important to assess where themovement is occurring. Forward bending orflexion of the spine may show increased hip flexion and increased length of hamstrings but poorlumbar spine flexion. They may show increasedthoracic flexion (Fig. 6.7) with a flat, relatively
78 HYPERMOBILITY SYNDROME
immobile lumbar spine. It is therefore importantto identify areas of relative hypermobility andrelative hypomobility.
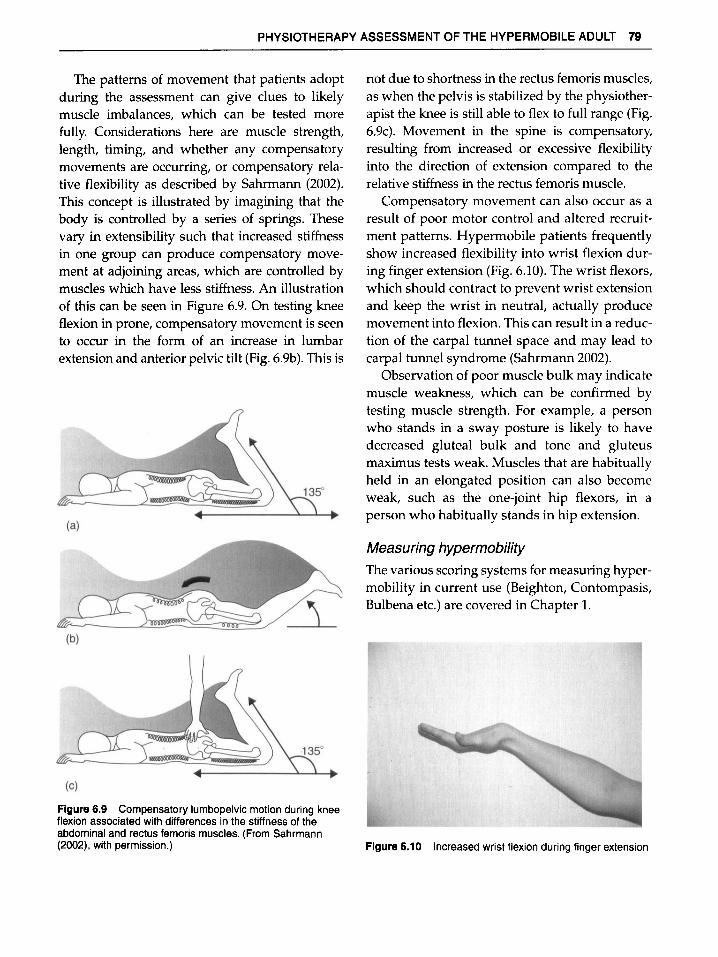
In spinal extension there is frequently anincreased range of movement in the mid or lowlumbar spine and virtually no movement in thethoracic spine. There may be evidence of hingingoccurring at a particular level, where the movement is seen to be excessive rather than occurringin a smooth curve (Fig. 6.8). This suggests hypermobility or functional instability at this level, andis frequently associated with pain. In these patientsit appears that because they have hypermobility inthe lumbar spine into extension and hence it iseasier to move here, they get almost all their rangein the lumbar spine and consequently stop usingthe thoracic spine when extending. Some of thismay also be related to the increased sedentarynature of our lifestyle,which facilitates a slouchingposture and hence an increased flexion of the
Figure 6.8 'Hinging' in the lumbar spine during extension
thoracic spine. Some individuals, when asked tobend backwards, can be observed to use hip extension, if there is increased range at the hip, in addition to or instead of lumbar spine movement.
Lateral flexion in the spine frequently demonstrates increased mobility, with the patient easilyreaching 5-8 cm below the knee crease with theirfingertips. A similar pattern is often seen in thecervical spine, where some hypermobile patientscan put their ear on their shoulder. Rotation inthe cervical spine is often hypermobile, showinga range of over 90°, with the chin reaching levelwith or just beyond the shoulder. Extension isfrequently of good range without symptoms, butoften occurs in the upper and mid cervical spine,with minimal or no movement in the low cervicalor upper thoracic spine.
Observing how the patient moves when walking, from sitting to standing, or when doing anactivity that produces symptoms, is necessaryto identify where movement is occurring. Hereagain, it is helpful to identify areas of relativehyper- and hypomobility. There may be increasedrotation of the lumbar spine, increased extensionat the hip, over-pronation in the feet, increasedmedial rotation of the femur, and hyperextensionat the knees. If symptoms are not produced, itis helpful to ask the patient to describe what theyare feeling while doing these activities. They areoften able to describe stiffness, uneven weightbearing, or feelings of instability in various partsof their body with particular movements.
The 'stiffness' of which some hypermobilepatients complain, and which is not related torestriction of active movement, may be related tothe feeling of 'stiffness' relating to muscles. Thisis the resistance felt when a muscle is passivelyelongated. A hypertrophied muscle is stiffer thana weak or atrophied one. This 'stiffness' occursthrough the range rather than at the end of range.It has been described as similar to the resistancefelt when elongating a spring (Sahrmann 2002).Thixotrophy also contributes to muscle stiffnessand may be why hypermobile patients reportbenefit from stretching.
PHYSIOTHERAPY ASSESSMENT OF THE HYPERMOBILE ADULT 79
The patterns of movement that patients adoptduring the assessment can give clues to likelymuscle imbalances, which can be tested morefully. Considerations here are muscle strength,length, timing, and whether any compensatorymovements are occurring, or compensatory relative flexibility as described by Sahrmann (2002).This concept is illustrated by imagining that thebody is controlled by a series of springs. Thesevary in extensibility such that increased stiffnessin one group can produce compensatory movement at adjoining areas, which are controlled bymuscles which have less stiffness. An illustrationof this can be seen in Figure 6.9. On testing kneeflexion in prone, compensatory movement is seento occur in the form of an increase in lumbarextension and anterior pelvic tilt (Fig. 6.9b). This is
Figure 6.9 Compensatory lumbopelvic motion during kneeflexion associated with differences in the stiffness of theabdominal and rectus femoris muscles. (From Sahrmann(2002), with permission.)
not due to shortness in the rectus femoris muscles,as when the pelvis is stabilized by the physiotherapist the knee is still able to flex to full range (Fig.6.9c). Movement in the spine is compensatory,resulting from increased or excessive flexibilityinto the direction of extension compared to therelative stiffness in the rectus femoris muscle.
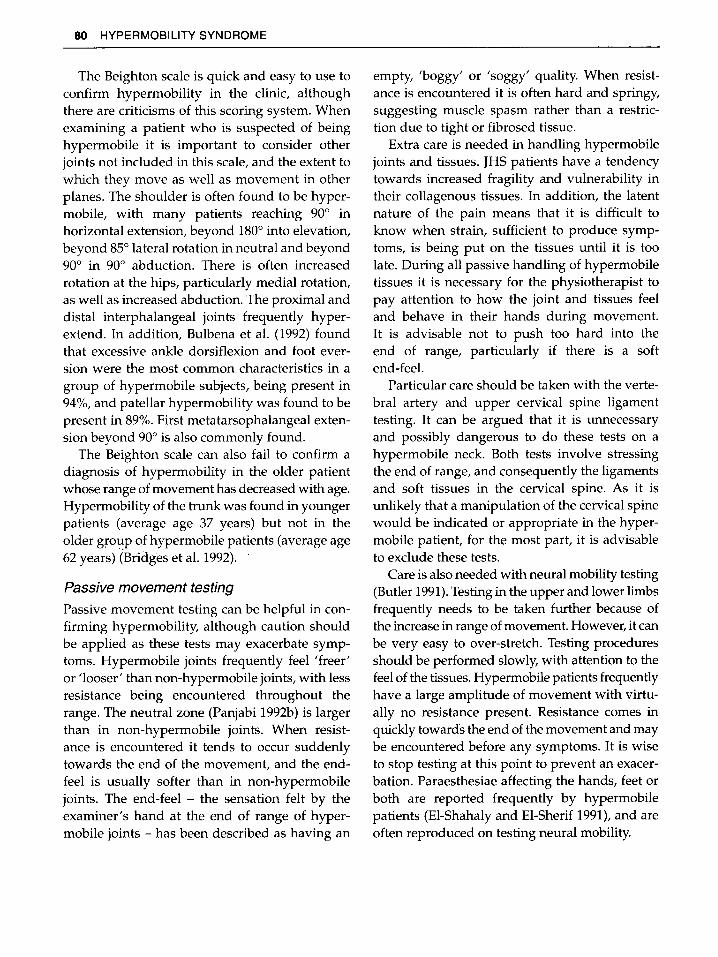
Compensatory movement can also occur as aresult of poor motor control and altered recruitment patterns. Hypermobile patients frequentlyshow increased flexibility into wrist flexion during finger extension (Fig. 6.10). The wrist flexors,which should contract to prevent wrist extensionand keep the wrist in neutral, actually producemovement into flexion. This can result in a reduction of the carpal tunnel space and may lead tocarpal tunnel syndrome (Sahrmann 2002).
Observation of poor muscle bulk may indicatemuscle weakness, which can be confirmed bytesting muscle strength, For example, a personwho stands in a sway posture is likely to havedecreased gluteal bulk and tone and gluteusmaximus tests weak. Muscles that are habituallyheld in an elongated position can also becomeweak, such as the one-joint hip flexors, in aperson who habitually stands in hip extension.
Measuring hypermobility
The various scoring systems for measuring hypermobility in current use (Beighton, Contompasis,Bulbena etc.) are covered in Chapter 1.
Figure 6.10 Increased wrist flexion during finger extension
80 HYPERMOBILITY SYNDROME
The Beighton scale is quick and easy to use toconfirm hypermobility in the clinic, althoughthere are criticisms of this scoring system. Whenexamining a patient who is suspected of beinghypermobile it is important to consider otherjoints not included in this scale, and the extent towhich they move as well as movement in otherplanes. The shoulder is often found to be hypermobile, with many patients reaching 90° inhorizontal extension, beyond 180° into elevation,beyond 85° lateral rotation in neutral and beyond90° in 90° abduction. There is often increasedrotation at the hips, particularly medial rotation,as well as increased abduction. The proximal anddistal interphalangeal joints frequently hyperextend. In addition, Bulbena et al. (1992) foundthat excessive ankle dorsiflexion and foot eversion were the most common characteristics in agroup of hypermobile subjects, being present in94%, and patellar hypermobility was found to bepresent in 89%. First metatarsophalangeal extension beyond 90° is also commonly found.
The Beighton scale can also fail to confirm adiagnosis of hypermobility in the older patientwhose range of movement has decreased with age.Hypermobility of the trunk was found in youngerpatients (average age 37 years) but not in theolder gro~p of hypermobile patients (average age62 years) (Bridgeset al. 1992).
Passive movement testing
Passive movement testing can be helpful in confirming hypermobility, although caution shouldbe applied as these tests may exacerbate symptoms. Hypermobile joints frequently feel 'freer'or 'looser' than non-hypermobile joints, with lessresistance being encountered throughout therange. The neutral zone (Panjabi 1992b) is largerthan in non-hypermobile joints. When resistance is encountered it tends to occur suddenlytowards the end of the movement, and the endfeel is usually softer than in non-hypermobilejoints. The end-feel - the sensation felt by theexaminer's hand at the end of range of hypermobile joints - has been described as having an
empty, 'boggy' or 'soggy' quality. When resistance is encountered it is often hard and springy,suggesting muscle spasm rather than a restriction due to tight or fibrosed tissue.
Extra care is needed in handling hypermobilejoints and tissues. JHS patients have a tendencytowards increased fragility and vulnerability intheir collagenous tissues. In addition, the latentnature of the pain means that it is difficult toknow when strain, sufficient to produce symptoms, is being put on the tissues until it is toolate. During all passive handling of hypermobiletissues it is necessary for the physiotherapist topay attention to how the joint and tissues feeland behave in their hands during movement.It is advisable not to push too hard into theend of range, particularly if there is a softend-feel.
Particular care should be taken with the vertebral artery and upper cervical spine ligamenttesting. It can be argued that it is unnecessaryand possibly dangerous to do these tests on ahypermobile neck. Both tests involve stressingthe end of range, and consequently the ligamentsand soft tissues in the cervical spine. As it isunlikely that a manipulation of the cervical spinewould be indicated or appropriate in the hypermobile patient, for the most part, it is advisableto exclude these tests.
Care is also needed with neural mobility testing(Butler 1991).Testing in the upper and lower limbsfrequently needs to be taken further because ofthe increase in range of movement. However, it canbe very easy to over-stretch. Testing proceduresshould be performed slowly, with attention to thefeel of the tissues. Hypermobile patients frequentlyhave a large amplitude of movement with virtually no resistance present. Resistance comes inquickly towards the end of the movement and maybe encountered before any symptoms. It is wiseto stop testing at this point to prevent an exacerbation. Paraesthesiae affecting the hands, feet orboth are reported frequently by hypermobilepatients (El-Shahaly and El-Sherif 1991), and areoften reproduced on testing neural mobility.
PHYSIOTHERAPY ASSESSMENT OF THE HYPERMOBILE ADULT 81
PalpationNot all the joints in a JHS patient are necessarilyhypermobile. Some areas, such as the thoracicspine and cervicothoracic junction, have a tendency to stiffen. This may be one reason for someof the bizarre symptoms reported which arebeing mediated via the sympathetic nervoussystem. These stiff areas have the potential toincrease stress on the hypermobile sections inthe spine, commonly the midcervical and lumbarspine, which may be responsible for symptoms.Palpation findings should confirm what has beenobserved during movement testing.
During passive movement testing it is important to ensure that movement is taking place whereit is intended to take place. When palpating astiff joint in the spine it is possible to producesymptoms at another area of the spine somedistance from the one being palpated. This isbecause the pressure normally exerted to producemovement at the stiff area is producing strainfurther away. It is important in this instance toobserve the whole spine, pay careful attention towhat is being felt, and support hypermobilesections when necessary. For example, palpationof a stiff thoracic spine in the prone position willplace less stress on the lumbar spine if a pillow isused to lift the lumbar spine out of extension.
WOMEN'S HEALTH
As generalized joint hypermobility and JHS arereported to occur more frequently in females it isappropriate to consider issues that affect women.
There have been some potential risks inpregnancy reported in women with joint hypermobility. Thornton et a1. (1988) report on twogenerations of women affected by JHS wherepregnancies were complicated by unexplainedmid trimester vaginal bleeding. Severe prematurity, due to cervical incompetence and prematurerupture of the membranes, has been reportedin a patient with the hypermobility type of EDS(DeVos et a1. 1999), and Charvet et a1. (1991), in a
literature review, report similar occurrences inaddition to tears and perineal haematomas. It isimportant that physiotherapists are aware ofthese potential complications, particularly if thepatient has not previously been identified ashypermobile. It may well be appropriate to havethe diagnosis confirmed by a rheumatologistso that the obstetrician can be informed of thesepotential problems.
Hypermobile women often report a considerable change in their feeling of wellbeing duringpregnancy. For some asymptomatic individualsit seems that pregnancy was the start of theirproblems and that they have been symptomaticever since. Others report that they felt the bestthey have ever felt, or even became symptom freefor the first time in years while pregnant, only tohave all their symptoms return soon after delivery.
The literature suggests that around 50% ofwomen suffer back or posterior pelvic pain whilepregnant (Ostgaard et a1. 1993). The reason for thehigh prevalence of spinal pain associated withpregnancy is not known. Several hypotheses havebeen put forward, but no one factor has beenfound to be responsible. It is likely that the cause ismultifactorial, although increased mobility of thepelvic joints due to hormonal changes affectingthe ligaments has been found to playa part, andmay be particularly relevant in the JHS patient.
Research in this area divides spinal pain associated with pregnancy into two distinct areas: backpain (lumbar spine) and peripartum pelvic pain(PPPP) (pain in the pelvic region) (Mens et a1.1996). PPPP has been found to be four times ascommon as back pain during pregnancy, andalthough fitness prior to pregnancy reduces theincidence of back pain in pregnancy, it was foundto make no difference to PPPP (Ostgaard et a1.1994). It has been suggested that the increasedlaxity of ligaments due to hormonal changes maybe responsible, with higher concentrations ofrelaxin being found in pregnant women withPPPP than in controls (MacLennan et a1. 1986).
Ligament laxity was found to increase throughout pregnancy, particularly from the 12th to the

82 HYPERMOBILITY SYNDROME
20th week (Ostgaard et al. 1993),and therefore thestability of the pelvis may be affected long beforeany significant weight gain has occurred. In addition, the study by Ostgaard et al. (1993) foundthat the increase in peripheral laxity in the primiparous pregnant group took 36 weeks to reachthe same level as the multipregnant group reachedat 12 weeks. This suggests that the increased peripherallaxity associated with pregnancy does notreturn to its prepregnancy level. This may haveconsequences for the hypermobile patient interms of further pregnancies, but may also help toexplain why for many hypermobile women theirsymptoms start with the first pregnancy and donot disappear after delivery. In addition, Franket al. (personal communication), found generalized hypermobility to be the only significantpredictor of postpartum spinal pain.
Ostgaard et al. (1993) found that a large sagittal diameter of the abdomen correlated weaklywith back pain in pregnancy, but strongly withperipheral laxity. They suggest that women withhigh peripheral laxity may develop larger abdomens owing to an increase in extensibility of theabdominal wall. This is due to collagen insufficiency caused by the hormones. This increasesthe flexion moment on the back and may increasethe risk of back pain. Back pain did not correlatewith laxity in multiparous women, but did correlate with laxity in primiparous women in the12th week. They conclude that an increase in collagen laxity would result in less ability to resiststretching, and may indicate a minor risk factorfor back pain in pregnant women.
It is not known what influence pregnancyhas on generalized joint hypermobility. Althoughthere is evidence that mobility in peripheraljoints increases significantly during pregnancy(Calguneri et al. 1982, Ostgaard et al. 1993), thestudy by Calguneri et al. (1982) showed no changein the Beighton score. This is probably due to alack of sensitivity inherent in the scale. In womenwho are already affected by generalized jointhypermobility, pregnancy could make them
unstable in certain areas, particularly the pelvis,causing symptoms. There is no evidence at present that hypermobile women have an increasedoccurrence of back pain during pregnancy orPPPP because of increased mobility. To theauthor's knowledge the only research that hasaddressed this issue is by van Dongen et al. (1999).This study examined hypermobility and PPPP in509 Cape Coloured pregnant women. Althoughthey found no correlation between hypermobilityand PPPP, they comment that PPPP was virtuallyabsent in this group and that hypermobility wassurprisingly low, at 5%. It is therefore difficult todraw any conclusions from this study, and furtherresearch in this area is clearly needed.
In spite of not knowing what effects generalized hypermobility may have in pregnancy it ishelpful to review what is known about the presentation of PPPP in pregnant women, insofaras it is related to joint laxity.
Women with PPPP usually present with painaround the sacroiliac joints, symphysis pubis,buttocks and upper legs. Pain is related toweight-bearing, such that standing and walkingprovoke pain (Ostgaard 1998), and many patientsshow a characteristic waddling gait (Mens et al.1996),with or without a marked limp on one side.The pain is time-dependent, with the patientbeing able to do most of what she used to do, butfor a shorter time. The pain, when provoked byoverdoing things, will often be felt the followingday rather than immediately, and this soundsremarkably similar to the onset of pain reportedby JHS patients. Twisting and asymmetric loading of the pelvis, as in vacuum cleaning, is mostpainful (Ostgaard 1998). The posterior pelvicpain provocation test (Ostgaard 1998), developedto differentiate women with pelvic pain ratherthan back pain, is positive. The test constitutes agentle longitudinal pressure applied along thefemur with the hip in 90° flexion and the patientsupine. The test is positive if pain is produced inthe posterior pelvis on the examined side only(Ostgaard 1998). PPPP is thought to be due to

PHYSIOTHERAPY ASSESSMENT OF THE HYPERMOBILE ADULT 83
Case study
A 36-year-old man was referred for physiotherapy Inconnection with a series of musculoskeletal complaints inthe presence of joint hypermobility. He was normally fit,exercising regularly, running, playing water polo andswimming competitively until 2 years pnor to referral.He had had no problems as a child, although he haddislocated his left elbow at the age of 17.
His problems started 4 years earlier, when he suffered leftknee pain and a feeling as if the joint had 'given out' after awalk down a mountain. This settled, but pain returned afterhe started running 2 years later. He stopped running anddiagnosed a tight iliolibial band (ITB) as the cause, andtreated this himself with stretches. The pain continued,settling into a fairly constant ache with a sharp pain onactivity, such as walking uphill, which could take a day ortwo to subside. He was still unable to run. In themeantime he had also injured his right anklesnowboarding, and this was diagnosed as a chronicstrain or tendonitis,
Six months prior to referral, he subluxed his nghtshoulder while SWimming. This relocated spontaneouslybut left him with some discomfort, which increased whendoing arm exercises with weights at the gym. He wasdiagnosed with an impingement syndrome and referredfor physiotherapy, which was unhelpful. At around thistime he also developed right knee pain, bilateral plantartasciitis. and a feeling of his hips being unstable. Hedescribes this as a period when his 'whole body went'.He stopped all physical activity, but this had no beneficialeffect on his symptoms: in fact he felt they were alldeteriorating. He reported feeling 'as if he was 100 yearsold' in the morning, feeling stiff and shuffling for an hourafter rising. His pain chart at the time of assessment ISillustrated in Figure 6.3.
He was in good health, although his weight had increasedbecause of the lack of exercise.He was in a sedentary deskjob. Non-steroidal anti-inflammatory medication had notbeen helpful. He had seen various medical practitioners
laxity of the ligaments and capsule of the sacroiliac joints owing to certain hormones, leading toinstability through inadequate force closure(Pool-Goudzwaard et al. 1998). Hip and spinalmovements are full and, interestingly, Ostgaard(1998) remarks that often these women can easilyreach the floor with straight knees, which maysuggest that generalized hypermobility is a factor in the development of this condition and thathyper-mobile women may be more at risk of suffering PPPP.
before seeing a rheumatologist, who recognized hisgeneralized hypermobility and referred him to our clinic. HIsblood tests were negative and X-rays and scans had shownmild degenerative changes in the left patella only
On examination he stood in a sway posture, with flatfeet, hyperextended knees and an increased thoracickyphosis He had a forward head posture and hisshoulders were forward with the scapulae abducted(nght left). He had decreased gluteal bulk and slightwasting of the quadriceps on the left. Muscle tone wasdecreased generally over much of his body. The range andquality of spinal mobility were good He could reach thefloor with his fingers on bending forward. and showedsome Increased flexibility In the lumbar spine intoextension and some sliffness in the thoracic spine.He scored 4/9 on the Beighton score (5/9 historically). andoutside the scale he showed increased mobility In his hipsinto lateral rotalion and abduction and his shoulders Intoelevation and external rotation.
He demonstrated poor trunk stability, With overactrvrty ofthe external oblique muscle There was muscle imbalancearound the hips, With shortness of ITB and dominance ofthe hamstnngs over gluteus maxim us. The gluteal musclestested weak. There was a painful arc In the nght shoulderand tenderness on palpation of supraspinatus. The upperfibres of trapezius were overactive, with weak lowertrapezius producing poor stabilization of the scapulaeduring movement. The patellotemoral joint showed lateraltracking (left worse than right), with some associated tilt.
The impression from the examination was that thishypermobile man expenenced no symptoms while he wasphysically fit and strong. An unresolved knee problem,which started after unaccustomed activity and a strain tothe ankle, set In motion compensatory mechanisms toprotect the JOints, and a gradual decrease In physicalexercise eventually resulted In further 10lntproblems and acessation of all exercise. resulting in the patient becomingdeconditioned and weaker.
CONCLUSION
Generalized joint hypermobility is frequentlythe cause of musculoskeletal symptoms reportedby patients consulting physiotherapists. Thecondition is often misunderstood and underrecognized. Gaining a better understanding ofhow the complaint presents and affects theJHS patient will help the physiotherapistrecognize the condition and aid assessment andmanagement.
84 HYPERMOBILITY SYNDROME
REFERENCES
Acasuso-Diaz, M., Collantes-Estevez, E. andSanchez Guijo, P. (1993) Joint hyperlaxity andmusculoligamentous lesions: study of apopulation of homogeneous age, sex and physicalexertion. British Journal of Rheumatology, 32, 120-2.
Al-Rawi, Z.5. and Al-Rawi, Z.T. (1982) Jointhypermobility in women with genital prolapse.Lancet, 1, 1439-41.
Al-Rawi, Z.5., Al-Aszawi, AJ. and Al-Chalabi, T.(1985) Joint mobility among university students inIraq. British Journal of Rheumatology, 4, 326-31.
Al-Rawi, Z. and Nessan, AH. (1997) Jointhypermobility in patients with chondromalaciapatellae. British Journal of Rheumatology, 12, 1324-7.
Barton, L.M. and Bird, H.A (1996) Improving pain bythe stabilization of hyperlax joints. Journal of OrthoRheumatology, 9, 46-51.
Beighton, P., Crahame, R. and Bird, H. (1989)Hypermobility of joints, 2nd edn. Springer-Verlag.
Beighton, P., Grahame, R. and Bird, H. (1999)Hypermobility of joints, 3rd edn, p 130.Springer-Verlag.
Bergmark, A (1989) Stability of the lumbar spine.A study in mechanical engineering. ActaOrthopedica Scandinatnca, 230 (Suppl), 20-4.
Bird, H.A and Barton, L. (1993) Joint hyperlaxity andits long term effect on joints. Journal of the RoyalSociety of Health, December, 327-9.
Bird, H.A, Tribe, C R. and Bacon, P.A. (1978) Jointhypermobility leading to osteoarthritis andchondrocalcinosis. Annals of the Rheumatic Diseases,37,203-11.
Biro, F.,Gewanter, H.L. and Baum, J. (1983) Thehypermobility syndrome. Pediatrics, 72, 701-6.
Bridges, AJ., Smith, E. and Reid, J. (1992) Jointhypermobility in adults referred to rheumatologyclinics. Annals of the Rheumatic Diseases, 51, 793-6.
Bulbena, A, Duro, J.C, Porta, M. et al. (1992) Clinicalassessment of hypermobility of joints: assemblingcriteria. Journal of Rheumatology, 19, 115-22.
Butler, 0.5. (1991) Mobilisation of the Nervous System.Churchill Livingstone.
Calguneri, M., Bird, H. and Wright, V. (1982) Changesin joint laxity during pregnancy. Annals of theRheumatic Diseases, 41, 126-8.
Charvet, P.Y., Salle, B., Rebaud, P. et al. (1991)[Ehlers-Danlos syndrome and pregnancy. Aproposof a case] [Abstract - article in French). Journalof Gynecology Biology and Reproduction (Paris),20,75-8.
Cherpel. A and Marks, R. (1999) The benign jointhypermobility syndrome. New Zealand Journal ofPhysiotherapy, 27, 9-22.
Child, AH. (1986) Joint hypermobility syndrome:inherited disorder of collagen synthesis. Journal ofRheumatology, 13, 239-43.
De Vos, M., Nuytinck, L., Verellen, C. andDe Paepe, A (1999) Preterm premature rupture ofmembranes in a patient with the hypermobilitytype of the Ehlers-Danlos syndrome. A casereport. Fetal Diagnostics and Therapy, 14, 244-7.
El-Carf, AX, Mahmoud, G.A and Mahgoub, E.H.(1998) Hypermobility among Egyptian children:prevalence and features. Journal of Rheumaiologu.B,1003-5.
El-Shahaly, H.A. and El-Sherif, AK. (1991) Is thebenign hypermobility syndrome benign? ClinicalRheumatology, 10, 302-7.
Finsterbush, A and Pogrund, H. (1982) Thehypermobility syndrome. Musculoskeletalcomplaints in 100 consecutive cases of generalizedjoint hypermobility. Clinical Orthopedics, 168, 124-7.
Francis, H., March, L., Terenty, 1. and Webb, J. (1987)Benign joint hypermobility with neuropathy:documentation of tarsal tunnel syndrome. journalof Rheumatology, 14, 577-81.
Gannon, L.M. and Bird, H.A. (1999) Thequantification of joint laxity in dancers andgymnasts. Journal of Sports Science, 9, 743-50.
Gazit, Y., Nahir, AM., Grahame, R. and Jacob, G.(2003) Dysautonomia in the joint hypermobilitysyndrome. American journal of Medicine, 115,33-40.
Grahame, R. (1986) Clinical manifesta tions of thejoint hypermobility syndrome. Reumaiologia(USSR), 2, 20-4.
Grahame, R. (1989)Clinical conundrum. How often,when and how does joint hypermobility lead toosteoarthritis? British Journal of Rheumatology, 28, 320.
Grahame, R. (1999) Joint hypermobility and geneticcollagen disorders: are they related? Archives ofDisease in Childhood, 80, 188-91.
Grahame, R. (2000) Heritable disorders of connectivetissue. In Bailliere'e Best Practice and Research inClinical Rheumatology (Balint and Bardin, eds),Vol. 14(2), pp. 345-361.
Grahame, R, Bird, H.A., Child, A et al. (2000) TheRevised (Brighton 1998) criteria for the Diagnosisof Benign Hypermobility Syndrome (BJHS).journal of Rheumatology, 27, 1777-9.
PHYSIOTHERAPY ASSESSMENT OF THE HYPERMOBILE ADULT 85
Harris, M.-C.R and Beeson, P. (1998) Generalizedhypermobility: is it a predisposing factor towardsthe development of juvenile hallux abductovalgus. The Foot, 8, 203-9.
Hudson, N., Fitzcharles, M.-A, Cohen, M.,Starr, M.R. and Esdaile, J.M. (1998) The associationof soft tissue rheumatism and hypermobility.British [ournal of Rheumatoioxy, 37, 382-6.
Jessee, E.P.,Owen, 0.5. and Sagar, K.B. (1980) Thebenign hypermobility syndrome. Arthritis andRheumatism, 23, 1053-6.
Kaplinsky, C, Kenet, G., Seligsohn, U. andRechavi, G. (1998) Association betweenhyperflexibility of the thumb and an unexplainedbleeding tendency: is it a rule of thumb? Britishiourna! of Haematology, 101, 260-3.
Kendall, P.P., McCreary, E.K. and Provance, P.G.(1993) Muscles: Testing and Function, 4th edn.Williams &Wilkins.
Kerr, A., Macmillan, C.E., Uttley, W.S. and Luqmani,RA. (2000) Physiotherapy for children withhypermobility syndrome. Physiotherapy, 86, 313-17.
Kirk, JA, Ansell, B.M. and Bywaters, E.G.L. (1967)The hypermobility syndrome. Muscular complaintsassociated with generalized joint hypermobility.Annalsof the Rheumatic Diseases, 26, 419-25.
Larsson, L.G., Baum, J., Mudholker, G.5. andKollia, G.O. (1993) Benefits and disadvantages ofjoint hypermobility among musicians.New England Journal of Medicine, 329, 1079-82.
Larsson, L.G., Mudholker, G.5., Baum, J. andSrivastava, O.K. (1995) Benefits and liabilities ofhypermobility in the back pain disorders ofindustrial workers. Journal of Internal Medicine, 5,461-7.
Lewkonia, RM. and Ansell, B.M. (1983) Articularhypermobility simulating chronic rheumaticdisease. Archives of Disease in Childhood, 12, 988-92.
Macl.ennan, AH., Nicholson, R, Green, RC. et al.(1986) Serum relaxin and pelvic pain of pregnancy.Lancet, ii. 243-5.
Maitland, GD. (1986) Vertebral Manipulation, 5th edn.Appendix 4, pp. 374. Butterworth Scientific.
March, L.M., Francis, H. and Webb, J. (1988) Benignjoint hypermobility with neuropathies:documentation of median, sciatic and commonperoneal nerve compression. Clinical Rheumatology,7,35-40.
Mens, J.M.A, Vleeming, A, Stoeckart, R et al. (1996)Understanding peripartum pelvic pain.Implications of a patient survey. Spine, 21, 1363-70.
Norton, P.A, Baker, J.E., Sharp, H.C. andWarenski, J.e. (1995) Genitourinary prolapse and
joint hypermobility in women. Obstetrics andGynecology, 85, 225-8.
Oliver, J. (2000) Hypermobility: recognition andmanagement. In Touch, 94, 9-12.
O'Sullivan, PB. (2000) Lumbar segmental 'instability':clinical presentation and specific stabilizingexercise management. Manual Therapy, 5, 2-12.
Ostgaard, H.C. (1998) Assessment and treatment oflow back pain in working pregnant women. In:Proceedings of the Third Interdisciplinary WorldCongress on Low Back Pain and Pelvic Pain(AVleeming, V. Mooney, H. Tilscher et al. eds),pp. 161-71. Vienna, Austria.
Ostgaard, H.C., Andersson, G.B.J., Schultz, AB. andMiller, JAA (1993) Influence of somebiomechanical factors on low-back pain inpregnancy. Spine, 18, 61-5.
Ostgaard, H.C., Zetherstrom, G., Roos-Hansson, E.and Svanberg, B. (1994) Reduction of back andposterior pelvic pain in pregnancy. Spine, 19,894-900.
Panjabi, M.M. (1992a) The stabilizing system of thespine. Part I. Function, dysfunction, adaptationand enhancement. Journal of Spinal Disorders, 5,383-9.
Panjabi, M.M. (1992b) The stabilizing system of thespine. Part II. Neutral zone and instabilityhypothesis. Journal of Spinal Disorders, 5, 390-7.
Pitcher, O. and Grahame, R (1982) Mitral valveprolapse and joint hypermobility: evidence fora connective tissue abnormality? Annals of theRheumatic Diseases, 4, 352-4.
Pool-Coodzwaard, AL., Vleeming, A, Stoeckart, Ret al. (1998) Insufficient lumbopelvic stability: aclinical, anatomical and biomechanical approachto 'a-specific' low back pain. Manual Therapy, 3,12-20.
Richardson, C, [ull, G., Hodges, P and Hides, J. (1999)Therapeutic Exercise for Spinal Segmental Stabilisationin Low Back Pain. Churchill Livingstone.
Russek. L.N. (1999) Hypermobility syndrome.Physical Therapy, 79, 591-9.
Russek, L.N. (2000) Examination and treatment ofa patient with hypermobility syndrome. PhysicalTherapy, 80, 386-98.
Sahrrnann, S. (2002) Diagnosis and Treatment ofMovement Impairment Syndromes. Mosby.
Seow, c.e., Chow, P.K. and Khong, K.5. (1999)A study of joint mobility in a normal population.Annals of theAcademyof Medicine of Singapore, 2,231-6.
Thornton, J.G., Hill, J. and Bird, H.A. (1988)Complications of pregnancy and benign familial

88 HYPERMOBILITY SYNDROME
joint hyperlaxity. Annalsof theRheumatic Diseases,47,228-31.
Tincello, A.G., Adams, E.J. and Richmond, D.H.(2002) Antenatal screening for postpartum urinaryincontinence in nulliparous women: a pilot study.European Journal ofObstetrics Gynecology andReproductive Biology, 1, 70-3.
van Dongen, P.W., de Boer, M., Lemmens, W.A. andTheron, G.B. (1999) Hypermobility andperipartum pelvic pain syndrome in pregnantAfrican women. European Journal ofObstetricsGynecology andReproductive Biology, 1, 77-82.
Verhoeven, J.J., Tuinman, M. and Van Dongen, P.w.(1999) Joint hypermobility in Africannon-pregnant nulliparous women. EuropeanJournal of Obstetrics Gynecology and ReproductiveBiology, 1, 69-72.
Wordsworth, P., Ogilvie, D., Smith, R. and Sykes, B.(1987) Joint mobility with particular reference toracial variation and inherited connective tissuedisorders. British Journal of Rheumatology, 1, 9-12.
Wynne-Davies, R. (1971) Familial joint laxity.Proceedings of the Royal Society ofMedicine, 64,689-90.