cerebral he mi atrophy
TRANSCRIPT
A Clinical & A Clinical & Radiological Radiological
Observation on Observation on Cerebral Cerebral
HemiatrophyHemiatrophy. .
INVESTIGATOR CHIEF SUPERVISORINVESTIGATOR CHIEF SUPERVISOR Dr. Anupam Jaiswal Prof. M. K. Singh Dr. Anupam Jaiswal Prof. M. K. Singh (DM)(DM) Senior Resident ProfessorSenior Resident ProfessorDepartment of Neurology Department of Department of Neurology Department of NeurologyNeurologyCSM Medical University CSM Medical CSM Medical University CSM Medical UniversityUniversity Lucknow LucknowLucknow Lucknow
INTRODUCTIONINTRODUCTION
Cerebral hemiatrophy is a clinical & radiological Cerebral hemiatrophy is a clinical & radiological condition that describes a condition of different condition that describes a condition of different etiologies, characterized by hypoplasia or atrophy etiologies, characterized by hypoplasia or atrophy of one of the cerebral hemispheres .of one of the cerebral hemispheres .
Hemiatrophy of the brain may occur in adults and Hemiatrophy of the brain may occur in adults and in old age as a result of degenerative or vascular in old age as a result of degenerative or vascular disorders, but the name is more commonly disorders, but the name is more commonly applied to the congenital or the infantile variety applied to the congenital or the infantile variety of the condition. It was proposed by Alpers and of the condition. It was proposed by Alpers and Dear (1939) that the two varieties be designated Dear (1939) that the two varieties be designated secondary and primary respectively.secondary and primary respectively.
1.Dyke CG, Davidoff LM, Masson CB. Cerebral hemiatrophy with homolateral hypertrophy ofthe skull and sinuses. Surg GynecolObstet I 1.Dyke CG, Davidoff LM, Masson CB. Cerebral hemiatrophy with homolateral hypertrophy ofthe skull and sinuses. Surg GynecolObstet I 933;57 : 588-600933;57 : 588-600
2.Alpers, B. J., and Dear, R. B. (1939). J. nerv. ment. Dis., 89, 653.2.Alpers, B. J., and Dear, R. B. (1939). J. nerv. ment. Dis., 89, 653.

CAUSES CAUSES PrimaryPrimary
Idiopathic Idiopathic (primary) (primary)
Intrauterine Intrauterine vascular injuryvascular injury
1. Dyke CG, Davidoff LM, Masson CB. Cerebral hemiatrophy with homolateral hypertrophy ofthe skull and sinuses. Surg GynecolObstet I 1. Dyke CG, Davidoff LM, Masson CB. Cerebral hemiatrophy with homolateral hypertrophy ofthe skull and sinuses. Surg GynecolObstet I 933;57 : 588-600933;57 : 588-6002. Alpers BJ, Dear RB. Hemiatrophy of the brain. J Nerv Ment Dis 1 939;89 :653-6692. Alpers BJ, Dear RB. Hemiatrophy of the brain. J Nerv Ment Dis 1 939;89 :653-6693. Ross AT. Cerebral hemiatrophy with compensatory homolateral hypertrophy of the skull and sinuses, and diminution of cranial volume. 3. Ross AT. Cerebral hemiatrophy with compensatory homolateral hypertrophy of the skull and sinuses, and diminution of cranial volume. AJR 1941;5:332-341AJR 1941;5:332-3414. Childe AE, Penfield W. The role of x-ray in the study of local atrophic lesions of the brain. Am J Psychiatry 1944;101 :30- 354. Childe AE, Penfield W. The role of x-ray in the study of local atrophic lesions of the brain. Am J Psychiatry 1944;101 :30- 355. McRae DL. Focal epilepsy: correlation of the pathological and radiological findings. Radiology 1948;50 : 439-4575. McRae DL. Focal epilepsy: correlation of the pathological and radiological findings. Radiology 1948;50 : 439-4576. Malamud N, Itabashi HH, Castor J, Messinger HB. An etiologicand diagnostic study of cerebral palsy. J Pediatr 1 964;65:270-2936. Malamud N, Itabashi HH, Castor J, Messinger HB. An etiologicand diagnostic study of cerebral palsy. J Pediatr 1 964;65:270-2937. Towbin A. Mental retardation due to germinal matrix infarction.Science 1969;1 64:156-1617. Towbin A. Mental retardation due to germinal matrix infarction.Science 1969;1 64:156-1618. Sener RN, Jinkins JR. MR of craniocerebral hemiatrophy. Clin Imaging. 1992; 16: 93-97. 8. Sener RN, Jinkins JR. MR of craniocerebral hemiatrophy. Clin Imaging. 1992; 16: 93-97. 9. J. Elizabeth, G. Menon,S. Nair,R.N. Bhattacharya,V.V. Radhakrishnan. Neurol India, 2002; 50 : 84-869. J. Elizabeth, G. Menon,S. Nair,R.N. Bhattacharya,V.V. Radhakrishnan. Neurol India, 2002; 50 : 84-86
Secondary Secondary Rasmussen encephaltitisRasmussen encephaltitis Postictal cerebral hemiatrophy Postictal cerebral hemiatrophy Basal ganglia germinomaBasal ganglia germinoma Trauma Trauma Infection Infection Vascular abnormalities e.g. Sturge-Vascular abnormalities e.g. Sturge-
Weber syndromeWeber syndrome Ischaemia Ischaemia Hypoxia Hypoxia Subependymal germinal matrix and Subependymal germinal matrix and
intraventricular hemorrhage in intraventricular hemorrhage in premature infantspremature infants

Clinical FeaturesClinical Features Seizures.Seizures. Contralateral hemiplegia or Contralateral hemiplegia or
hemiparesis.hemiparesis. Facial asymmetry.Facial asymmetry. Learning difficulties. Learning difficulties. Other associated findings described Other associated findings described
are sensory loss, speech and are sensory loss, speech and language disorders, and psychiatric language disorders, and psychiatric manifestations like schizophrenia. manifestations like schizophrenia.
MRI FEATURESMRI FEATURES Considered Gold StandardConsidered Gold Standard Features are Features are Unilateral loss of cerebral volume.Unilateral loss of cerebral volume. Varying degrees of dilatation of one lateral ventricle and Varying degrees of dilatation of one lateral ventricle and
displacement of the midline structures toward the atrophic side displacement of the midline structures toward the atrophic side . .
Compensatory cerebral hypertrophy.Compensatory cerebral hypertrophy. Subarachnoid sulci may be widened on the affected side.Subarachnoid sulci may be widened on the affected side. Compensatory bone alterations in the calvarium, such as Compensatory bone alterations in the calvarium, such as
thickening, hyperpneumatization of the paranasal sinuses and thickening, hyperpneumatization of the paranasal sinuses and mastoid cells.mastoid cells.
Elevation of the petrous ridge and greater wing of the sphenoid Elevation of the petrous ridge and greater wing of the sphenoid bone.bone.
1. Afifi AK, Godersky JC, Menezes A, et al. Cerebral hemiatrophy, hypoplasia of internal carotid artery and intracranial aneurysm. Arch Neurol 1987;44:232-352. Sener RN, Jinkins JR. MR of craniocerebral hemiatrophy. Clin Imaging 1992;16:93-97.3. Tasdemir HA, Incesu L, Yazicioglu AK, et al. Dyke-Davidoff-Masson syndrome. Clin Imaging. 2002;26(1):13-17.
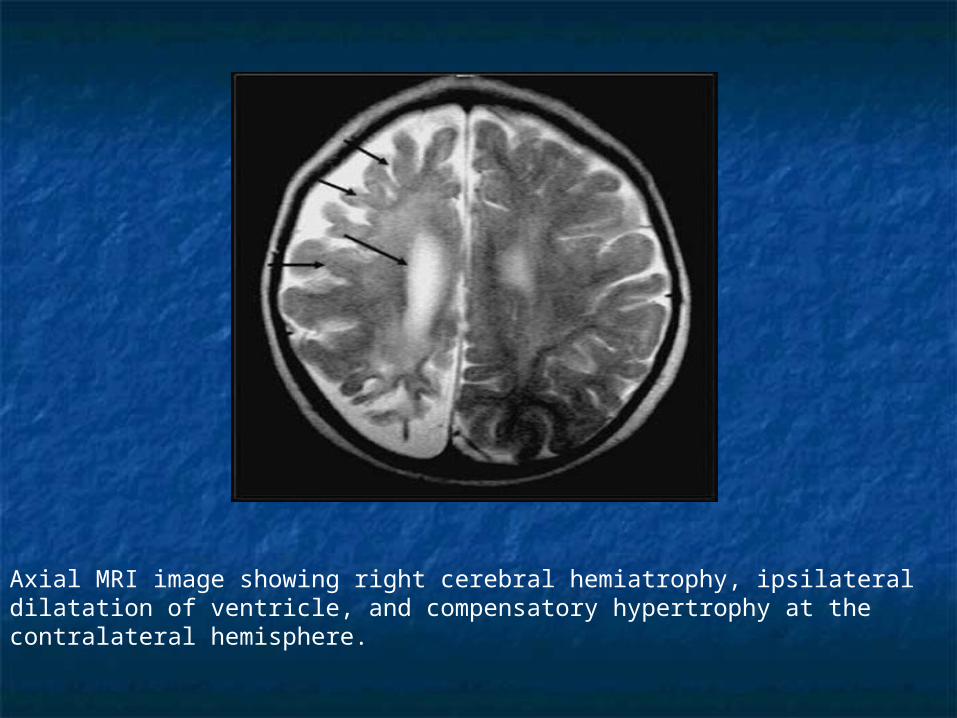
Axial MRI image showing right cerebral hemiatrophy, ipsilateral dilatation of ventricle, and compensatory hypertrophy at the contralateral hemisphere.
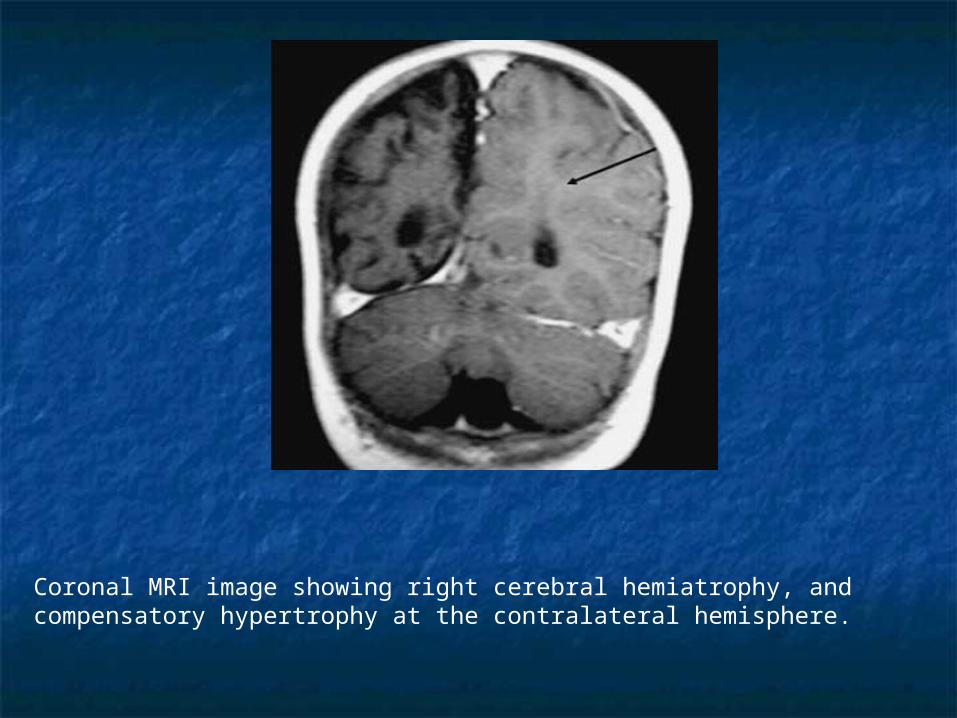
Coronal MRI image showing right cerebral hemiatrophy, and compensatory hypertrophy at the contralateral hemisphere.
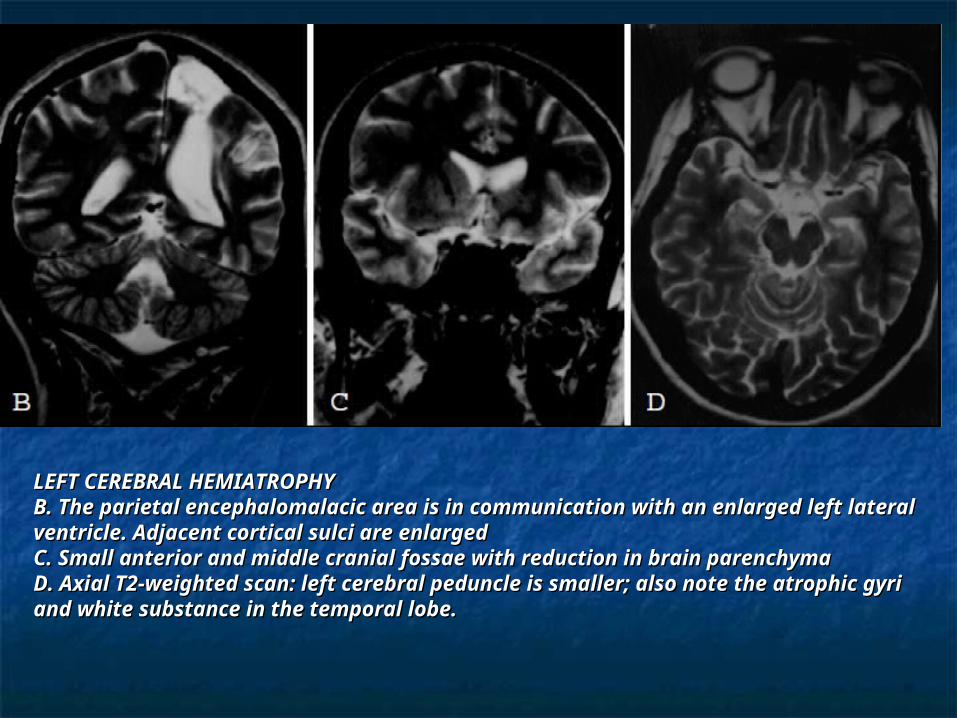
LEFT CEREBRAL HEMIATROPHYLEFT CEREBRAL HEMIATROPHYB. The parietal encephalomalacic area is in communication with an B. The parietal encephalomalacic area is in communication with an enlarged left lateral ventricle. Adjacent cortical sulci are enlargedenlarged left lateral ventricle. Adjacent cortical sulci are enlargedC. Small anterior and middle cranial fossae with reduction in brain C. Small anterior and middle cranial fossae with reduction in brain parenchymaparenchymaD. Axial T2-weighted scan: left cerebral peduncle is smaller; also note the D. Axial T2-weighted scan: left cerebral peduncle is smaller; also note the atrophic gyri and white substance in the temporal lobe.atrophic gyri and white substance in the temporal lobe.
Pathologic FeaturesPathologic Features Thinning of the grey matter cortex Thinning of the grey matter cortex Reduced volume of the underlying white matter Reduced volume of the underlying white matter +/- reduced / abnormal myelination +/- reduced / abnormal myelination Enlargement of the lateral ventricle Enlargement of the lateral ventricle Reduced size of cerebral peduncle (ipsilateral) Reduced size of cerebral peduncle (ipsilateral) Reduced size of cerebellar hemisphere Reduced size of cerebellar hemisphere
(contralateral)(contralateral)
INVESTIGATIONSINVESTIGATIONS
RoutineRoutine EEGEEG MRI brain.MRI brain. Other investigations as required for Other investigations as required for
finding etiology & in treatment.finding etiology & in treatment.
DYKE-DAVIDOFF-MASSON SYNDROMEDYKE-DAVIDOFF-MASSON SYNDROME
Dyke-Davidoff-Masson syndrome is cerebral Dyke-Davidoff-Masson syndrome is cerebral hemiatrophy due to a congenital, neonatal hemiatrophy due to a congenital, neonatal or early infantile condition & characterized or early infantile condition & characterized clinically by variable degrees of facial clinically by variable degrees of facial asymmetry, seizures, contralateral asymmetry, seizures, contralateral hemiplegia or hemiparesis, and mental hemiplegia or hemiparesis, and mental retardation. retardation.
Mental retardation is not alwayspresentMental retardation is not alwayspresent1-3.1-3.
Seizures may appear months or years after Seizures may appear months or years after the onset of hemiparesisthe onset of hemiparesis33. .
Patients may also have speech or language Patients may also have speech or language disordersdisorders11..
1. Parker CE, Harris N, Mavalwala J. Dyke-Davidoff-Masson syndrome: five case studies and deductions from dermatoglyphics. Clin 1. Parker CE, Harris N, Mavalwala J. Dyke-Davidoff-Masson syndrome: five case studies and deductions from dermatoglyphics. Clin Pediatr 1972;11:288-292.Pediatr 1972;11:288-292.2. Sener RN, Jinkins JR. MR of craniocerebral hemiatrophy. Clin Imaging 1992;16:93-97.2. Sener RN, Jinkins JR. MR of craniocerebral hemiatrophy. Clin Imaging 1992;16:93-97.3. Zilkha A . CT of cerebral hemiatrophy. AJR 1980;135:259-262.3. Zilkha A . CT of cerebral hemiatrophy. AJR 1980;135:259-262.

THANKSTHANKS