case study nhs birmingham east & north. case study – nhs birmingham east & north (ben)...
TRANSCRIPT

Case study
NHS Birmingham East & North

Case study – NHS Birmingham East & North (BEN)
This slide pack uses the following tools to tell an health investment story for BEN:
• Programme Budgeting Spreadsheet;• Spend and Outcomes Tool;• Programme Budgeting Atlas;• NHS Comparators.
These tools allow commissioners to compare expenditure and outcomes at disease level.
This is a starting point for the process of making health investment decisions.

Prioritising Health InvestmentProgramme budgeting:
- Outlines PCTs’ spend by disease based categories
- Allows PCTs to compare their own spend and health outcomes to other PCTs
- Provides a starting point for making health investment decisions
Marginal analysis
- An appraisal of the changes in costs and benefits when resources in programmes are deployed in new ways
- Provides a framework for making health investment decisions in a transparent way that involves clinicians and patients
- Further information on marginal analysis will be provided on World Class Commissioning Networks

2008/09 Programme Level Expenditure in England
Programme Budgeting Category2008/09£000s
Mental Health Disorders 10,415,840 Problems of Circulation 7,420,201 Cancers and Tumours 5,134,948 Problems of the Respiratory System 4,247,325 Problems of Musculo Skeletal System 4,212,469 Problems of Gastro Intestinal System 4,097,920 Problems of Genito Urinary System 4,000,641 Neurological 3,683,873 Problems due to Trauma and Injuries 3,299,792 Social Care Needs 3,156,039 Maternity and Reproductive Health 3,100,821 Dental Problems 3,087,416 Problems of Learning Disability 2,916,182 Endocrine, Nutritional and Metabolic 2,526,152 Healthy Individuals 1,908,832 Problems of the Skin 1,794,226 Problems of Vision 1,664,102 Infectious Diseases 1,410,980 Disorders of Blood 1,253,786 Conditions of Neonates 1,101,470 Adverse effects and poisoning 955,442 Problems of Hearing 417,167 Other 24,836,323 Total Gross Expenditure 96,814,987

World Class Commissioning (WCC) / NHS Constitution
WCC Competency 6
Level 2 - Strategic investment and disinvestment initiatives are generated through insights from:
• Public and patient engagement • Local needs (e.g. JSNA) • Clinical evidence • Programme budgeting or equivalent
Level 3 - PCT develops programme budgeting or equivalent methodology demonstrating whole system approach to investment and disinvestment.
Level 4 - Mature programme budgeting or equivalent methodology for all key priority care pathways / disease groups with integrated investment / disinvestment plans of up to 10 years.
NHS Constitution
To provide best value for taxpayers’ money by way of the most effective, fair and sustainable use of finite resources.
Programme Budgeting Spreadsheet
• Programme budgeting spreadsheet each year on the DH website
www.dh.gov.uk/programmebudgeting
Configured to be easy to use, and provide information PCT boards can quickly comprehend.
• Data cut at Cancer and CVD Network level are also available

Birmingham East & North PCT Expenditure
Programming Budgeting Sheet

BEN PCT Expenditure per 100,000 population (weighted by age, sex and need) 2007/8 Rank Column shows PCT is a low spender on Mental Health, Neurological, Circulation, Dental and Gastro-Intestinal categories.
Programming Budgeting Sheet

BEN PCT Expenditure per 100,000 population (weighted by age, sex and need) on Problems of Circulation categoryGreen circle shows BEN PCT has lower spend than most PCTs, both nationally (blue diamonds), and in similar PCT cluster (purple triangles).
Programming Budgeting Sheet

BEN PCT Expenditure per 100,000 population (weighted by age, sex and need) on all categories compared to cluster averageBEN PCT spends £25m more on category 23 ‘Other’ and almost £10m less on category 10 ‘Circulation’ than similar PCTs.
Programming Budgeting Sheet
APHO Spend and Outcomes Tool (SPOT)
• The spend and outcomes tool has been developed by the Association of Public Health Observatories.
• The tool allows PCTs to compare their expenditure and outcome data for each of the 23 Programme Budget disease categories on a single page.
• The tool is interactive and allows PCTs to select different outcome measures and different views of the data – including a comparison with any other selected PCT.
• A very useful tool that quickly allows PCTs to identify areas of expenditure that warrant further investigation.
Outcomes against Spend for each categoryEach diamond represents a disease category and shows spend and outcomes compared to the national average. Circulation has lower spend and worse outcomes compared to other PCTs.
Mortality from all
circulatory diseases: Under 75s
Low birth weight births
Outcomes and expenditure relative to other PCTs in England
Inf Canc
Blood,Pois,HlthEnd
MH
LD,Hear,MuscNeuro,Gastro
Vision
Circ
Resp
Dent
Skin
TraumaGU
Mat
Neo
Soc
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
0.5
1.0
1.5
2.0
2.5
-2.5 -2.0 -1.5 -1.0 -0.5 0.0 0.5 1.0 1.5 2.0 2.5
Spend Z Score
Hea
lth
Ou
tco
me
Z S
core
Lower Spend, Better Outcome
Lower Spend,Worse Outcome
Higher Spend,Worse Outcome
Higher Spend,Better Outcome
Neonatal infant
mortality per 1,000
births
APHO Spend and Outcomes Tool

Programme Budgeting Atlases (1 of 2)
• The programme budgeting atlases are provided on our behalf by the National Centre for Health Outcomes Development, under contract to the Information Centre for Health and Social as part of the Compendium of Public Health Indicators.
• The atlas links programme budgeting expenditure data, as presented in the programme budgeting spreadsheet, with an array of outcome data.
• By using mapping software, bar charts and correlation plots, the atlases provides an illuminating and user-friendly way of analysing and presenting data.
• Atlases are available via an NHS Net connection from: nww.nchod.nhs.uk

Programme Budgeting Atlases (2 of 2)
• Atlases include a vast array of data configured in terms of:
Expenditure data.
Output dataPrimary care prescribing – number of items and expenditure;
For CVD only % of low cost Statins as per better care better value;
Admissions/ALOS/Bed days (total, non-elective, elective ordinary, daycase);
Day case rates.
Outcome dataMortality (and in some cases under 75 Years of Life Lost);
Prevalence data from QOF;
For Cancer, incidence data; QOF process outcomes e.g. blood pressure control, or cholesterol control;
Emergency readmissions data;
Deaths within 30 days of admission.

Circulation (CVD) expenditure per 100,000 population (weighted for age, sex and need) Darker areas represent higher spend. BEN PCT is in lowest spending 20% of PCTs nationally.
Programme Budgeting Atlas

CVD expenditure per 100,000 population (weighted for age, sex and need) filtered by ONS Cluster (Centres with Industry)Darker areas represent higher spend. BEN PCT is second lowest spending PCT compared to similar PCTs.
Programme Budgeting Atlas

CVD expenditure per 100,000 population (weighted by age, sex and need) filtered by SHA. Darker areas represent higher spend. BEN PCT is second lowest spending PCT in the West Midlands SHA.
Programme Budgeting Atlas

CVD Mortality data - Years of life lost under 75 years per 10,000 population (weighted for age, sex and need)Darker areas represent more years of life lost. BEN PCT is in highest 20% of PCTs nationally.
Programme Budgeting Atlas
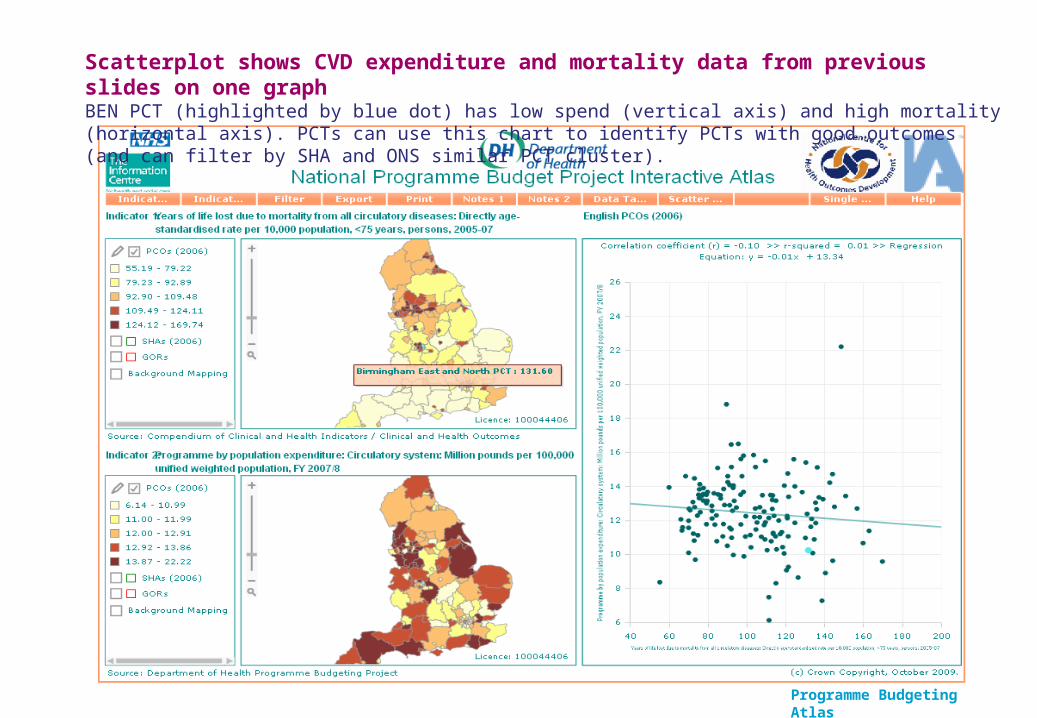
Scatterplot shows CVD expenditure and mortality data from previous slides on one graphBEN PCT (highlighted by blue dot) has low spend (vertical axis) and high mortality (horizontal axis). PCTs can use this chart to identify PCTs with good outcomes (and can filter by SHA and ONS similar PCT cluster).
Programme Budgeting Atlas

Expenditure on CVD Family Health Services Prescribing per 100,000 population (weighted for age, sex and need)Darker areas represent higher spend. BEN PCT spend is below national and SHA average.
Programme Budgeting Atlas

Percentage of Statins prescribed that are low costDarker areas represent higher proportion of low cost Statins. BEN PCT has low proportion of low cost Statins in FHS Prescribing.
Programme Budgeting Atlas

CVD Elective hospital admissions per 100,000 population (weighted for age, sex and need)Darker areas represent higher number of admissions. BEN PCT has a lower number of Elective Admissions than the national average.
Programme Budgeting Atlas

CVD non-elective hospital admissions per 100,000 population (weighted for age, sex and need)Darker areas represent higher number of admissions. BEN PCT has a high number of non-elective admissions.
Programme Budgeting Atlas

CVD non-elective average length of stay per spell in hospitalDarker areas represent higher LOS. BEN PCT has a low average LOS for non-elective admissions.
Programme Budgeting Atlas

CVD emergency readmissions to hospital within 28 days of dischargeDarker areas represent higher number of readmissions. BEN PCT has a high number of CVD emergency readmissions.
Programme Budgeting Atlas

Deaths within 30 days of admission for coronary heart diseaseDarker areas represent higher number of deaths. BEN PCT has a high number of deaths (but there are very large confidence intervals so caution must be used when interpreting this data)
Programme Budgeting Atlas

Scatterplot comparing recorded prevalence of CHD and hypertension from QOFBEN PCT has low recorded prevalence of CHD and hypertension but this not appear to fit with the high non-elective admissions and mortality indicators – is CVD being picked up in primary care?
Programme Budgeting Atlas

NHS Comparators
NHS Comparators provided by the IC on the NHS net: nww.nhscomparators.nhs.uk
• Holds data at England, SHA, PCT and practice• Data are timely and frequent – every quarter up to Q4 2008/9• Various sources of data including:
– total admissions – activity and expenditure;– non-elective admissions – activity and expenditure;– elective admissions – activity and expenditure;– prescribing – items and expenditure;– better care better value metrics – including low cost statin prescribing.
• Very powerful for showing variation, and time series – which allows to track change over time
• Outpatient referrals by GP

Expenditure on all admissions covered by PBR tariff (age and sex adjusted rate) Comparison with other PCTs. BEN PCT slightly higher expenditure than national average.
Table shows activity, expected activity based on national averages, and the resulting % difference, for PCT and SHA
Drill down to disease level
NHS Comparators

GP practice level comparison of expenditure on CVD emergency admissionsLarge variation between spend at practice level in BEN PCT.
Easy to identify high and low spending practices. Can compare practices within groups based on need of population
NHS Comparators

GP practice level comparison of average length of stay of CVD emergency admissions.Large variation at practice level in BEN PCT.
NHS Comparators

Managing variation in surgical thresholdsExpenditure at GP practice level on the six ‘better care better value’ procedures identified as low clinical value. Large variation at practice level in BEN PCT
NHS Comparators

Quarterly time series of BEN PCT expenditure on respiratory admissionsBEN PCT admissions rate is higher than SHA and national average rate.
PCT has over the last three years been constantly high spending for respiratory.
Peaks due to seasonality.
NHS Comparators

Higher than national and SHA rates for first outpatient attendances. Rising slower than the
national rate – but still 7% growth in 2008/9.
Quarterly time series of BEN PCT outpatient first attendances. BEN PCT rate is higher than SHA and national average rate. Breakdown by source of referral is also available.
NHS Comparators

Includes FHS prescribing data (volume and cost of prescriptions) BEN PCT has a lower than average proportion of low cost Statins.
NHS Comparators

This table is available at SHA, PCT, and Practice level, on a quarterly or annual basis.
The table shows for inpatient admissions in each disease area, actual spend, expected based on national averages, and expenditure differences in absolute and % terms.
Because expenditure is calculated as activity multiplied by tariff, the table is less useful where tariff is less well developed – e.g. mental health.
Breakdown of actual and expected expenditure on admissions by programme budget or disease categoryAlso available for FHS prescribing expenditure.
NHS Comparators

New and Future Work
• Analysis of variation in expenditure on inpatient admissions for four disease areas
• Analysis of variation in expenditure on inpatient admissions for twenty high volume procedures
• Analysis of variation in expenditure on inpatient admissions for twenty high growth procedures – will be linked to NICE clinical guidelines and thresholds
• Identification of low value activities (led by Sir Muir Gray)
• Analysis of variation in treatment thresholds and health gains from Patient Reported Outcomes Measures data

Health Investment Network Web Pages
More resources are available on:
http://www.networks.nhs.uk/nhs-networks/health-investment-network
Provides
• A tool for PCTs to explore this inpatient admissions analysis and identify the scope for potential savings
• Guides to using the tools outlined in this case study and other useful resources
• Links to useful tools to help with health investment • A forum for PCTs to share case-studies of work on prioritising investment, discuss key issues and learn about useful new events and products