case study #2 fawn mumbulo - 2014 670. encounter: 2/14/2014 @ sherburne bassett healthcenter c.s. is...
TRANSCRIPT

Case Study #2Fawn Mumbulo - 2014670

Encounter: 2/14/2014 @ Sherburne Bassett Healthcenter•C.S. is a 19 yo male who presented to the
clinic on 2/13/2014 with a raised macular papular rash dispersed t/o the body. He was treated with Zertec, and a urine protein was done.
•C.S. presented on 2/14/2014 with worsening symptoms. Rash has spread to face, mouth, and extremities. Patient c/o painful hands, wrists, knees, & feet – with swelling and redness at the joints.

PMH/Surgical hx Vital Signs
• Closed fx of the left fibula (2011)
• Cyst of the brain (2011)• Migraines• Left varicocele• Myopia• Regular astigmatism• Dysplastic nevus• Acne• Irritable bowel syndrome• Asthma• Eustachian tube
dysfunction• Environmental allergies
• BP 118/74• Pulse 84• Temp 99 degrees F• Resp 16• Ht 5’8”• Wt 151 lbs• BMI 23.08
• Immunizations are up to date

Medications – NKDA Family hx
• Wellbutrin 150 mg po daily for anxiety
• Zyrtec 10 mg, one tab po daily
• Naproxen 500 mg, one tab twice daily with meals
• Prednisone 60 mg po daily for 5 days
• Mother A/W• Father HTN,
hyperlipidemia• Two brothers A/W
Social
• Smoker 1 ppd• Occupation: milks cows

ROS• Constitutional: CS reports decreased activity & appetite. Decreased
activity is associated with painful ambulation and when bending knees. Reports wrists are tender to move.
• HENT: Reports facial swelling this am upon awakening. Left side of bottom lip was reported with decreased swelling t/o the day today.
• Eyes: Denies visual disturbances. Reports swelling above the right eye was noticeable this am.
• Respiratory: Denies SOB or dyspnea.• Cardiovascular: Denies chest pain or palpitations.• Gastrointestinal: C/o pain in lower abd above bladder area. Denies
difficulty with bowel movements.• Genitourinary: Denies dysuria, urgency, frequency, hematuria, flank
pain, decreased urine volume, discharge, penile swelling, scrotal swelling, enuresis, difficulty urinating, genital sores, penile/testicular pain. Reports that he is sexually active, uses a condom. Positive for pain in abd. above the bladder area.
• Musculoskeletal: Reports low back pain, joint swelling in upper/lower ext.
• Neurological: Denies imbalances, falls, or loss of sensations. • Skin: Reports that rash became present one day ago. Reports that if
clothes touch the rash then it becomes itchy. Reports no drainage from the rash lesions.

Differential Diagnosis• Acute abdomen• Inflammatory Bowel Disease• Acute hemorrhagic edema• Bacterial • Endocarditis• Familial Mediteranean Fever• Hypersensitivity (leukocytoclastic) Vasculitis• Henoch-Schonlein purpura• Rheumatoid Arthritis (ANA-antinuclear antibody & RF-rheumatoid factor)• Kawasaki Disease• Leukemia• Meningococcemia• Polyarteritis Nodosa• Rocky Mountain Spotted Fever• Thrombocytopenic Purpura• Wegener Granulomatosis
(Reamy, Williams, & Lindsay, 2009)

Maculopapular rash-swollen knee
(Adam, 2010; ByeByeDoctor.com, n.d.)
Clinical Presentation• General: Oriented to person, place, and time. Appears well
developed, well nourished with no distress.• HENT: Normocephalic – atraumatic. External ears normal. Nose
patent, no drainage. No lesions found internally or externally on mouth or throat.
• Eyes: Conjunctivae and EOM are normal. Pupils equal, round, and reactive to light. Eyes exhibit no discharge. Slight swelling above right eye lid.
• Neck: ROM intact, neck supple. No JVD present. No tracheal deviation present. No thyromegaly present. Left lymphadenopathy.
• Cardiovascular: Normal rate, regular rhythm, normal heart sounds with intact distal pulses. No gallop, rub, or murmurs heard.
• Pulmonary/Chest: Breath sounds clear, no SOB or dyspnea on exertion. No Tenderness.
• Abdominal: Soft, flat, non distended, no masses. BS present in 4 quads. Tenderness palpatable just above the umbilicus. No rebound or guarding.
• Musculoskeletal: Edema and tenderness in knees, ankles, hands, and wrists. Knees have the most pain with difficulty to ambulate.
• Skin: Warm, dry, intact. Maculopapular errythemia diffused rash that is confluent on inner left arm and back. Center of the maculopapular areas are white.
• Psychiatric: Normal mood and affect, behavior is normal, judgment and thought content normal.

Typical Symptoms• Headache, Anorexia, Fever, Fatigue with the disease usually
following an URI. HTN can be present.• Rash in 95-100% involving legs (Hallmark), erythematous
macular or urticarial lesions that progress to blanching papules then palpable purpura. Symmetrical dependent body areas over a period of 10 days.
• Abdominal pain & vomiting in 35-85%, bloody stools, hematemesis, duodenal ulcers, massive GI bleeds. Complication - intussusception.
• Joint pain (mostly knees & ankles) 60-84%, arthalgia (presenting feature in 25% cases) with rare involvement of wrists and fingers, swelling.
• Subcutaneous edema 20-25%• Scrotal edema (orchitis) 2-35%• Renal findings: (40-50%) greatest in those older then 10 yrs of
age. Acute glomerular lesions, mesangial hypercellularity, endocapillary proliferation, necrosis, cellular crescents, and leukocyte infiltration. Usually occurring within 1 – 6 months from rash. Patients with persistent proteinuria are at greatest risk of renal disease.
• Other findings: Involve vasculitis of the myocardium or lungs, stensosing ureteritis, priapism, vasculitis of the CNS (intracranial hemorrhage), bilateral subperiosteal orbital hematomas, adrenal hematomas, acute pancreatitis (rare), and cystic changes of ovaries.
(Domino, 2013; Medscape, 2013; Reamy, Williams, & Lindsay, 2009; Scheinfeld, 2013)

EpidemiologyPathophysiology
• Occurs in 10-22 persons out of 100,000 per year.
• Most common in late autumn to early spring.
• Over 90% are children younger than 10 years of age, with a peak incidence of 6 years of age.
• Can occur in infants, adolescents, and adults.
• Adults have a greater chance of having long term renal disease.
• Slight predominance in males.
• IgA immune complexes are deposited in sm. Vessels causing petechiae and palpable purpura.
• Immune complexes occur in the sm. Vessel intestinal wall that may lead to gastrointestinal hemorrhage.
• Immune complexes can affect the renal mesangium which can cause mild proliferative to severe escalating glomerulonephritis.
• Exposure of an antigen from an infection, medication, or environmental agents can trigger antibody and immune complex formation. Such as Group A streptococcus, parvovirus B19, Bartonella henselae, H-pylori, Haemophilus parainfluenza, Coxsackie virus, adenovirus, Hepatitis A and B, mycoplasma, Epstein-Barr virus, varicella, campylobacter, and methicillin-resistant staphylococcus aureus.
• Serum antistreptolysin-O titers are likely to be positive.(Reamy, Williams, & Lindsay, 2009)

Diagnosis HINT…• Who is this famous screen
writer and actor that recently died from a similar diagnosis presented in this case study?
•Harold Ramis
(pagesay.com, 2014)

Henoch-Scholnlein purpuraDefinition Prevalence
• Alternative names: ▫ Anaphylactoid purpura▫ Vascular purpura▫ Leukocytoclastic vasculitis
• Acute immunoglobulin A disorder characterized by generalized vasculitis involving small vessels of the skin, GI tract, kidneys, joints, & rarely lungs & CNS
• It is a subset of necrotizing vasculitis characterized by fibrinoid destruction of blood vessels & leukocytoclasis
• U.S. 14-15 cases per 100,000 with a peak age of 5 yrs old, 75% aged 12-11 yrs old
• United Kingdom 20.4/100,000• Whites are affected more
often than blacks• Occurring between
November & January• Male to female ratio is 1.5-2:1• Children younger than 3 yrs
old tend to have milder cases with fewer occurrences
(MedlinePlus, 2013; Scheinfeld, 2013)

Diagnosis HSP cont.
• Previous infections such as streptococcal • Rash: (not everyone) 1st defined as urticaria then
disseminates into purpura HALLMARK predominant on lower extremities, but may spread to face/trunk, may be preceded by joint or abd pain
• Abd pain: form of bleeding may occur, pain may continue for up to 2 wks after rash, intussusception may be a complication
• HTN: may be present• Orchitis: less common, can mimic testicular torsion• Joints: examine for swelling & ROM• CNS: HA, seizures, behavioral changes
(Domino, 2013; Reamy, Williams, & Lindsay, 2009; UpToDate, 2014)

Infectious Agents Associated • Mononucleosis• Group A streptococcal infection
(most common)• Hepatitis• Mycoplama infection• Camphylobacter enteritis• Subacute bacterial endocarditis• H-pylori infection• Yersinia infection• Shigella infection• Salmonella infection• Brucellosis• Legionella species• Parvovirus• Adenovirus• EBV infection• VZV infection• Glomerulocystic kidney disease
• Vaccinations that may precede HSP▫ Typhoid & paratyphoid A
and B▫ Measles▫ Yellow fever▫ Cholera
• Environmental factors▫ Drugs (ampicillin,
erythromycin, PCN, quinidine, quinine, losartan, & cytarabine)
▫ Foods▫ Horse serum▫ Cold exposures▫ Insect bites
(Scheinfeld, 2013)

Treatment per Symptoms
Symptom Severity Treatment
Minimal Supportive care
Mild arthralgias or abd pain Acetaminophen or NSAIDS
Moderate with significant arthritis, abd pain, or early renal involvement
Corticosteroids (pediatric dose 1-2 mg/kg X 2 wks followed by a taper)Consider a subspecialty referral
Severe with progressive renal disease, pulmonary hemorrhage
Corticosteroids (as above) plus adjunctive immunosuppressant (azathioprine [Imuran], cyclophosphamide [Cytoxan], IV immunoglobuline) or plasmapheresisSubspecialty referral needed (nephrology, gastroenterology, surgeon, rheumatology; depending on presenting symptoms or organ involvement)
(Reamy, Williams, & Lindsay, 2009)

Management• Blood pressure measurements and urinalysis
should be performed at the time of HSP dx for a baseline
• Serum BUN/Cr (if hematuria or proteinuria) monthly for 6 mo. to detect early renal involvement, facilitating consultation and steroid treatment
• Scheinfeld (2013) suggests that drugs such as acetaminophen, ibuprofen, flurbiprofen, ketoprofen, and naproxen can be causative agents; this is contraindicative of all other resources considering acetaminophen & NSAIDS are used to treat pain
(Reamy, Williams, & Lindsay, 2009)

Complications• Glomerulonephritis• Hemorrhagic cystitis• Nephrotic syndrome• Renal failure• Bowel infarction• Bowel perforation• Duodenal obstruction• Gastrointestinal
hemorrhage• Intestinal stricture• Alveolar hemorrhage• Interstitial infiltrate• Pulmonary effusion• Aphasia• Ataxia
• Cerebral hemorrhage• Chorea• Cortical blindness• Neuropathy• Paresis• Seizure• Anterior uveitis• Myocarditis• Myositis• Orchitis• Scrotal edema• Testicular torsion
(Reamy, Williams, & Lindsay, 2009)

Analysis• Recurrences of HSP can occur in up to 1/3 of the
patients within the 1st 6 mo. after onset (more common in patients who had renal involvement)
• Long-term prognosis depends on severity of renal involvement, 1-5% will end up with ESRD▫ Eighty five percent of patient with HSP developed renal
involvement within 4 wks of onset, 91% in 2 wks, 97% in 6 mo. With ESRD occurring in 19.5% of patients with nephritic or nephrotic syndrome
▫ Fifty percent of the patients will have recurrences within 6 wks & up to 7 yrs which will likely leave renal impairment
▫ Patients with normal urinalysis at 6 mo. do not go on to develop renal problems
(Reamy, Williams, & Lindsay, 2009; Scheinfeld, 2013)

HSP IgA Nephropathy
• Mostly children▫ Skin & connective tissue▫ GI tract▫ Joints▫ Scrotum▫ Kidneys
• Familiar occurrences• Patients with HPS who
under go renal transplantation develop IgA deposits in the graft
• Cystic changes in the ovaries of prepubertal females have been recorded
• Both have similar pathological findings
• Complete remission 72.5% at an average of 20 mo.
• Exclusively involves young adults▫ Affecting only the
kidneys• Has developed in patients
with a hx of HSP• Familiar occurrences
▫ In a study surveying 40 patients with 2 or more members who had IgA nephropathy, 5 presented with HPS
• Both have similar pathological findings
• Complete remission 19.4% after 34 mo. with consistant hematuria & proteinuria, and 16.1% active nephritides
(Scheinfeld, 2013)

Facts HSP• Ninety four percent of children & 89% of adults
only need supportive treatment (purpura may worsen without rest)
• Goal is to evaluate labs to identify complications & exclude other diseases (Renal func., CBC, PT/aPTT, IgA)
• HSP (IgAV) usually goes away in about a month but it can cause lasting problems with the kidneys (especially adults)
• Biopsy of the skin is the best diagnostic criteria (shows leukocytoclastic vasculitis) - this is unnecessary as the rash usually is enough to dx HSP
• Renal bx demonstrates a membranoproliferative glomerulonephritis similar to IgA nephropathy
(Reamy, Williams, & Lindsay, 2009)
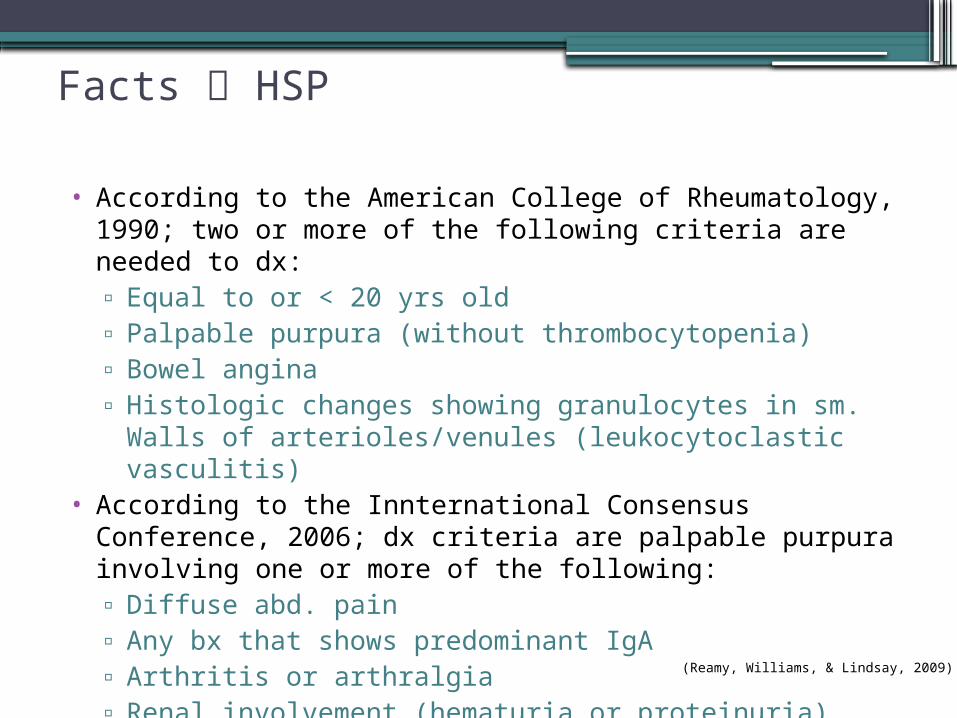
Facts HSP
• According to the American College of Rheumatology, 1990; two or more of the following criteria are needed to dx: ▫ Equal to or < 20 yrs old▫ Palpable purpura (without thrombocytopenia)▫ Bowel angina ▫ Histologic changes showing granulocytes in sm. Walls of
arterioles/venules (leukocytoclastic vasculitis)• According to the Innternational Consensus Conference,
2006; dx criteria are palpable purpura involving one or more of the following:▫ Diffuse abd. pain▫ Any bx that shows predominant IgA ▫ Arthritis or arthralgia▫ Renal involvement (hematuria or proteinuria)
(Reamy, Williams, & Lindsay, 2009)

References• Domino, F. (2013). The 5-minute clinical consult, 21 ed.,
Philadelphia, PA: Lippincott Williams & Wilkins, Wolters Kluwer.
• MedlinePlus. (2013). Henoch-Schonlein purpura. Retrieved from http://www.nlm.nih.gov/medlinplus/ency/article/000425.ht
m• Reamy, B. V., Williams, P. M., & Lindsay, T. J. (2009). Henoch-
Schonlein purpura. American Family Physician, 80(7), 697- 704.• Scheinfeld, N. S. (2013). Henoch-Schonlein purpura. Retrieved
from http://www.emedicine.medscape.com/article/084105-overview
• UpToDate. (2014). Patient information: Henoch-Schonlein purpura (IgA vasculitis) (the basics). Retrieved from http://www.uptodate.com/contents/henoch-schonlein- purpura-iga-vasculitis-the-basics?