case reports cheiro-oral syndrome due to lesions in the corona
TRANSCRIPT
599
Case Reports
Cheiro-Oral Syndrome Due to Lesionsin the Corona Radiata
Tsuyoshi Omae, MD; Takashi Tsuchiya, MD; and Takenori Yamaguchi, MD
Background and Purpose: We describe three patients with cheiro-oral syndrome caused by a small lesionin the corona radiata confirmed by high-resolution magnetic resonance imaging.
Case Descriptions: Case 1: A 56 -year-old hypertensive man who developed hypesthesia and paresthesiain the left perioral area and hand was found to have a small hematoma just lateral to the right internalcapsule. Case 2: A 67-year-old man noticed hypesthesia around the left mouth angle and thumb and indexfinger. Magnetic resonance imaging revealed a lesion in the right corona radiata. Case 3: A 45-year-oldhypertensive man developed numbness in his perioral region and left hand that later spread to hisshoulder. Magnetic resonance imaging revealed a recent small infarct in the lower lateral aspect of theright corona radiata.
Conclusions: A small lesion in the corona radiata can cause cheiro-oral syndrome, whose pathogeneticmechanism in such patients may be explained by the somatotopical location or by the differingvulnerability of the neuropils in the corona radiata. (Stroke 1992;23:599-601)
KEY WORDS • hypesthesia • magnetic resonance imaging
Cheiro-oral syndrome is a unilateral sensory dis-turbance limited to the hand or fingers and theipsilateral perioral region. This syndrome was
initially attributed to a lesion in the contralateral post-central gyrus of the parietal lobe by Sittig.1 Later, thisunusual distribution of sensory abnormalities was re-lated to thalamic lesions.2"5 Recently, cases associatedwith brain stem lesions have been reported.6"10 Wereport three patients with a cheiro-oral syndromecaused by small lesions in the contralateral coronaradiata, confirmed by high-resolution magnetic reso-nance imaging (MRI).
Case ReportsCase 1
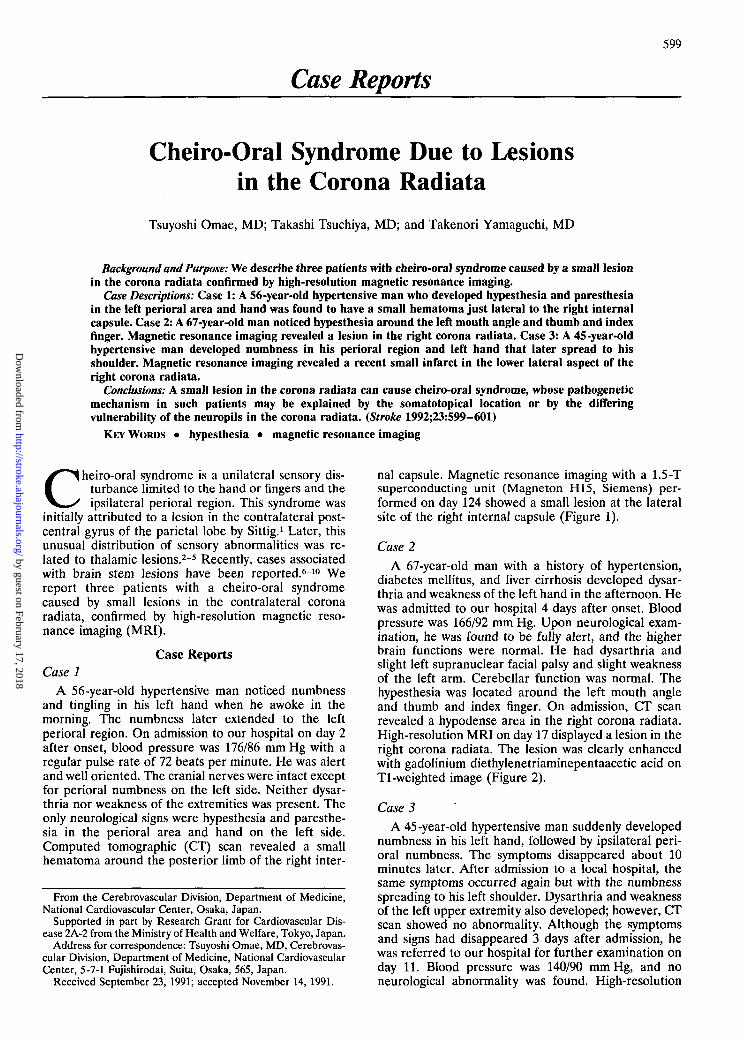
A 56-year-old hypertensive man noticed numbnessand tingling in his left hand when he awoke in themorning. The numbness later extended to the leftperioral region. On admission to our hospital on day 2after onset, blood pressure was 176/86 mm Hg with aregular pulse rate of 72 beats per minute. He was alertand well oriented. The cranial nerves were intact exceptfor perioral numbness on the left side. Neither dysar-thria nor weakness of the extremities was present. Theonly neurological signs were hypesthesia and paresthe-sia in the perioral area and hand on the left side.Computed tomographic (CT) scan revealed a smallhematoma around the posterior limb of the right inter-
From the Cerebrovascular Division, Department of Medicine,National Cardiovascular Center, Osaka, Japan.
Supported in part by Research Grant for Cardiovascular Dis-ease 2A-2 from the Ministry of Health and Welfare, Tokyo, Japan.
Address for correspondence: Tsuyoshi Omae, MD, Cerebrovas-cular Division, Department of Medicine, National CardiovascularCenter, 5-7-1 Fujishirodai, Suita, Osaka, 565, Japan.
Received September 23, 1991; accepted November 14, 1991.
nal capsule. Magnetic resonance imaging with a 1.5-Tsuperconducting unit (Magneton H15, Siemens) per-formed on day 124 showed a small lesion at the lateralsite of the right internal capsule (Figure 1).
Case 2
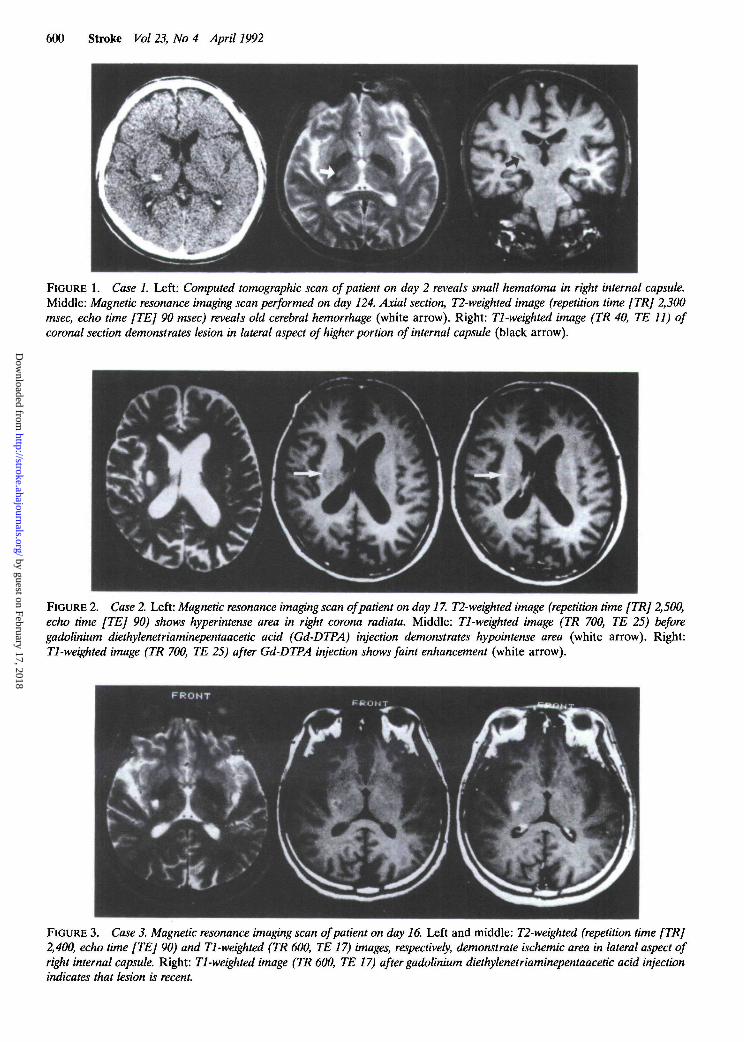
A 67-year-old man with a history of hypertension,diabetes mellitus, and liver cirrhosis developed dysar-thria and weakness of the left hand in the afternoon. Hewas admitted to our hospital 4 days after onset. Bloodpressure was 166/92 mm Hg. Upon neurological exam-ination, he was found to be fully alert, and the higherbrain functions were normal. He had dysarthria andslight left supranuclear facial palsy and slight weaknessof the left arm. Cerebellar function was normal. Thehypesthesia was located around the left mouth angleand thumb and index finger. On admission, CT scanrevealed a hypodense area in the right corona radiata.High-resolution MRI on day 17 displayed a lesion in theright corona radiata. The lesion was clearly enhancedwith gadolinium diethylenetriaminepentaacetic acid onTl-weighted image (Figure 2).
Case 3
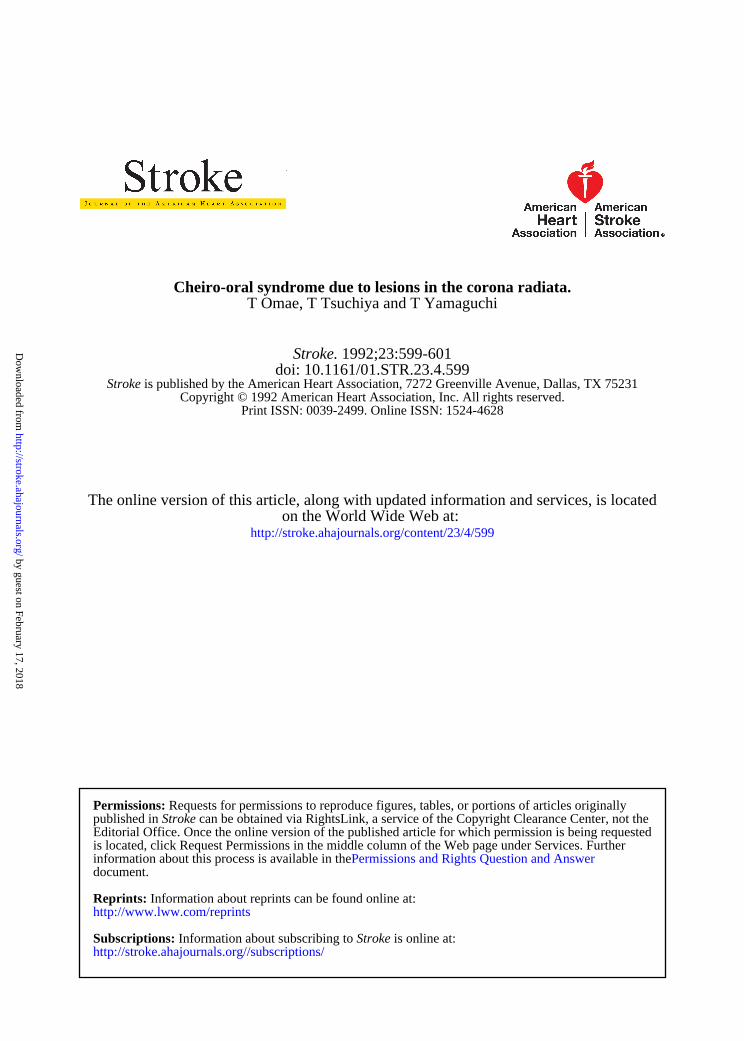
A 45-year-old hypertensive man suddenly developednumbness in his left hand, followed by ipsilateral peri-oral numbness. The symptoms disappeared about 10minutes later. After admission to a local hospital, thesame symptoms occurred again but with the numbnessspreading to his left shoulder. Dysarthria and weaknessof the left upper extremity also developed; however, CTscan showed no abnormality. Although the symptomsand signs had disappeared 3 days after admission, hewas referred to our hospital for further examination onday 11. Blood pressure was 140/90 mm Hg, and noneurological abnormality was found. High-resolution
by guest on February 17, 2018http://stroke.ahajournals.org/
Dow
nloaded from
600 Stroke Vol 23, No 4 April 1992
FIGURE 1. Case 1. Left: Computed tomographic scan of patient on day 2 reveals small hematoma in right internal capsule.Middle: Magnetic resonance imaging scan performed on day 124. Axial section, T2-weighted image (repetition time [TR] 2,300msec, echo time [TE] 90 msec) reveals old cerebral hemorrhage (white arrow). Right: Tl-weighted image (TR 40, TE 11) ofcoronal section demonstrates lesion in lateral aspect of higher portion of internal capsule (black arrow).
FIGURE 2. Case 2. Left: Magnetic resonance imaging scan of patient on day 17. T2-weighted image (repetition time [TR] 2,500,echo time [TE] 90) shows hyperintense area in right corona radiata. Middle: Tl-weighted image (TR 700, TE 25) beforegadolinium diethylenetriaminepentaacetic acid (Gd-DTPA) injection demonstrates hypointense area (white arrow). Right:Tl-weighted image (TR 700, TE 25) after Gd-DTPA injection shows faint enhancement (white arrow).
FIGURE 3. Case 3. Magnetic resonance imaging scan of patient on day 16. Left and middle: T2-weighted (repetition time [TR]2,400, echo time [TE] 90) and Tl-weighted (TR 600, TE 17) images, respectively, demonstrate ischemic area in lateral aspect ofright internal capsule. Right: Tl-weighted image (TR 600, TE 17) after gadolinium diethylenetriaminepentaacetic acid injectionindicates that lesion is recent.
by guest on February 17, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Omae et al Cheiro-Oral Syndrome 601
MRI revealed a recent small infarct at the lower lateralaspect of the right corona radiata (Figure 3).
DiscussionThe mechanism causing the peculiar distribution of
sensory impairment in cheiro-oral syndrome resultingfrom a single lesion has been explained as a closesomatotopical location in the postcentral gyrus of theparietal lobe,1-4 thalamic sensory nuclei,3 and mediallemniscus of the brain stem.5-6 The somatotopical local-ization of the hand and the mouth is close in thethalamic nuclei and medial lemniscus of the brain stem.However, the cortical topography of these regions wasfound by electrophysiological and anatomic studies tobe separated by that of the upper portion of the face.11
This finding makes a simple anatomic explanation ofthis syndrome based on a single parietal lesion difficult.In the case of the somatic motor cortex, the corticalareas representing these regions were reported to bemore sensitive to electrical stimulation than other re-gions.12 The areas in the somatosensory cortex are alsothought to be so sensitive to stimuli that sensory impair-ment restricted to the hand and the corner of the mouthcan be produced by a single lesion.13
In one case of cheiro-oral syndrome in which Kino-shita et al14 reported a lesion in the corona radiata,there was no discussion of the pathogenetic mechanism.Although Bogousslavsky et al15 recently reported casesof this syndrome due to opercular infarct involving theunderlying white matter, their discussion focusedmainly on the rarity of cortical cheiro-oral syndromecaused by stroke and on the anatomic consideration.
In an experimental neuropathologic study, Jones andPowell16 demonstrated antegrade axonal degenerationresulting from a lesion in the ventroposterior nucleus ofthe thalamus in a rhesus monkey. They also found thatfibers from the medial part of the ventral posterolateralnucleus and the lateral part of the ventral posterome-dial nucleus run together and project to the somatosen-sory cortex. This study indicates the possibility that thethalamocortical fibers from the hand are adjacent tothose from the mouth in the corona radiata. Thus, asingle small lesion can cause cheiro-oral syndrome in
such a region. On the other hand, if the fibers from thehand and mouth are more vulnerable than other fibers,as is speculated to be the case in the cortex, a singlelesion in the corona radiata can cause cheiro-oralsyndrome.
References1. Sittig O: Klinische Beitrage zur Lehre von der Lokalisation der
sensiblen Rindenzentren. Prager Med Wochenschr 1914;45:548-550
2. Garcin R, Lapresle J: Syndrome sensitif de type thalamique et &topographie cheiro-orale par lesion localisee du thalamus. RevNeurol (Paris) 1954;90:124-129
3. Garcin R, Lapresle J: Deuxieme observation personnelle desyndrome sensitif de type thalamique et a topographie cheiro-oralepar lesion localisee du thalamus. Rev Neurol (Paris) 1960;103:474-481
4. Strauss H: Ober Sensibilitatsstorungen an Hand und Gesicht,Gaschmacksstorugen und ihre lokalisatorische Bedeutung.Monatsschr Psychiatr Neurol 1925;58:265-276
5. Kawakami Y, Chikama M, Tanimoto T, Shimamura Y: Radiolog-ical studies of the cheiro-oral syndrome. J Neurol 1989;236:177-181
6. Tawara S, Shirabe T, Terao A, Araki S: Unilateral MLF syndromewith palm-oral sensory disturbance: Report of a case. Clin Neurol(Tokyo) 1974;14:745-751
7. Ono S, Inoue K: Cheiro-oral syndrome following midbrain haem-orrhage. J Neurol 1985;232:304-306
8. Araga S, Fukada M, Kagimoto H, Takahashi K: Pure sensorystroke due to pontine haemorrhage. J Neurol 1987;235:116—117
9. Holter JT, Tijssen C: Cheiro-oral syndrome: Does it have a specificlocalizing value? Eur Neurol 1988;28:326-330
10. Matsumoto S, Kaku S, Yamasaki M, Imai T, Nabatame H,Kameyama M: Cheiro-oral syndrome with bilateral oral involve-ment: A study of pontine lesions by high-resolution magneticresonance imaging. J Neurol Neurosurg Psychiatry 1989;52:792-794
11. Penfield W, Boldrey E: Somatic motor and sensory representationin the cerebral cortex of man as studied by electrical stimulation.Brain 1937;60:389-443
12. Liddle EGT, Phillips CG: Threshold of cortical representation.Brain 1950;73:125-140
13. Noda S, Umezaki H, Nagata S, Kuromatsu C: Cortical cheiro-oralsyndrome due to convexity meningioma. Neurol Med (Tokyo)1983;18:506-509
14. Kinoshita I, Iwanaga K, Muta K, Ohe H, Ohe N: Radial cheiro-oral syndrome: A case report. Neurol Med (Tokyo) 1991;34:490-492
15. Bogousslavsky J, Dizerens K, Regli F, Despland PA: Opercularcheiro-oral syndrome. Arch Neurol 1991;48:658-661
16. Jones EG, Powell TPS: Connexions of the somatic sensory cortexof the rhesus monkey: III. Thalamic connexions. Brain 1970;93:37-56
by guest on February 17, 2018http://stroke.ahajournals.org/
Dow
nloaded from
T Omae, T Tsuchiya and T YamaguchiCheiro-oral syndrome due to lesions in the corona radiata.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1992 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.23.4.599
1992;23:599-601Stroke.
http://stroke.ahajournals.org/content/23/4/599on the World Wide Web at:
The online version of this article, along with updated information and services, is located
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document.
Permissions and Rights Question and Answer information about this process is available in theis located, click Request Permissions in the middle column of the Web page under Services. Further
requestedEditorial Office. Once the online version of the published article for which permission is being can be obtained via RightsLink, a service of the Copyright Clearance Center, not theStrokepublished in
Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on February 17, 2018http://stroke.ahajournals.org/
Dow
nloaded from