case report - matheuspithon · carlos ventura de oliveira ruellas, dds antÔnio carlos de oliveira...
TRANSCRIPT

Diabetes mellitus is a metabol-ic disorder characterized by
either partial or total deficiencyof insulin or by a resistance tothat hormone, leading to an in-crease in blood glucose levelsand subsequent complications.1
Most cases of diabetes mellitusfall into two categories: type 1(insulin-dependent) and type 2(some combination of insulin-deficient and insulin-resistant).2
Type 1 diabetes mellitus isdistinguished by a complete lackof insulin production, usually ac-companied by intense hyper-glycemia and ketoacidosis. Mostpatients develop the disease dur-ing childhood and require exoge-nous insulin injections to sur-vive.1
The five classic complica-tions of diabetes are microan-
giopathy, neuropathy, nephropa-thy, macrovascular diseases, andwound-healing delay.3-5 TheWorld Health Organization ad-ded periodontal disease as a sixthclassic complication in 1993.
The increased risk of perio-dontitis in diabetic patients is as-sociated with multiple factors,including the patient’s age, theduration of the diabetes,2,6,7,16-18
the presence or absence of meta-bolic controls, and the level ofbacterial plaque.2,8,9 Adults withtype 1 diabetes have been foundto be more susceptible than non-diabetic adults to gingivitis andperiodontitis.11,12 Over a long pe-riod of time, type 1 diabetes canalter the periodontal tissue andthus speed up the clinical loss ofperiodontal ligament insertion.10
Bone metabolism is adversely
affected by both the direct im-pact of hyperglycemia and thelong-term effects of vascular dis-ease.13-15 Furthermore, patientswhose diabetes is inadequatelycontrolled tend to show a greaterloss of insertion and alveolarbone than patients with well-controlled diabetes.7,19-21
These findings are signifi-cant for the orthodontist, becauseif a diabetic patient presents withadvanced periodontal disease, itwill be necessary to use the leasttraumatic treatment possible toavoid a worsening of the alreadydeficient periodontium. The pre-sent article reports an orthodon-tic treatment involving the ex-traction of four second premolarsin an adult patient with type 1 di-abetes mellitus and a widespreadloss of supporting bone.
VOLUME XXXIX NUMBER 7 © 2005 JCO, Inc. 435
CASE REPORT
Orthodontic Treatment of a Patientwith Type 1 Diabetes MellitusMATHEUS MELO PITHON, DDSCARLOS VENTURA DE OLIVEIRA RUELLAS, DDSANTÔNIO CARLOS DE OLIVEIRA RUELLAS, DDS, MS, PHD
Dr. Pithon is a student and Dr. Antônio Ruellas is a Visiting Pro-fessor in the Orthodontics Specialization Course, Escola de Far-mácia e Odontologia de Alfenas/Centro Universitário Federal,Alfenas, MG, Brazil. Dr. Antônio Ruellas is also an Assistant Pro-fessor, Department of Orthodontics, Federal University of Rio deJaneiro, Brazil. Dr. Carlos Ruellas is a postgraduate student inoral rehabilitation, USP, Ribeirão Preto, Brazil. Contact Dr.Pithon at Rua Mexico 78, Bairro Recreio, 45020-390 Vitória daConquista, Bahia, Brazil; e-mail: [email protected].
Dr. Carlos RuellasDr. Pithon Dr. Antônio Ruellas

Diagnosis
A 38-year-old female pre-sented with the chief complaintof poor dental esthetics. Hermedical history involved type 1diabetes mellitus, with daily in-sulin injections needed to controlher glucose levels. The patientreported neither hypoglycemicnor hyperglycemic crises, whichgave us an indication of her abil-ity to cooperate with orthodontictreatment. She displayed goodoral hygiene and an absence ofactive cavity lesions.
In the clinical examination,the patient showed normal facialsymmetry, a labial seal at rest,and a mesocephalic facial pattern(Fig. 1). Her profile was concave(LS-S = –2mm; LIS = –3mm),but her lip relationship was good.She had a Class I molar and ca-nine relationship with moderateupper and lower crowding, a4mm overjet, and a 5% overbite.Widespread bone loss was con-firmed radiographically, sug-gesting a periodontal complica-tion of diabetes.
Cephalometrically, the pa-tient showed a normal anteropos-terior and transverse jaw rela-
436 JCO/JULY 2005
Orthodontic Treatment of a Patient with Type 1 Diabetes Mellitus
Fig. 1 38-year-old female patient with type 1 diabetes mellitus and widespread loss of supporting bone beforetreatment.
VOLUME XXXIX NUMBER 7 437
Pithon, Ruellas, and Ruellas
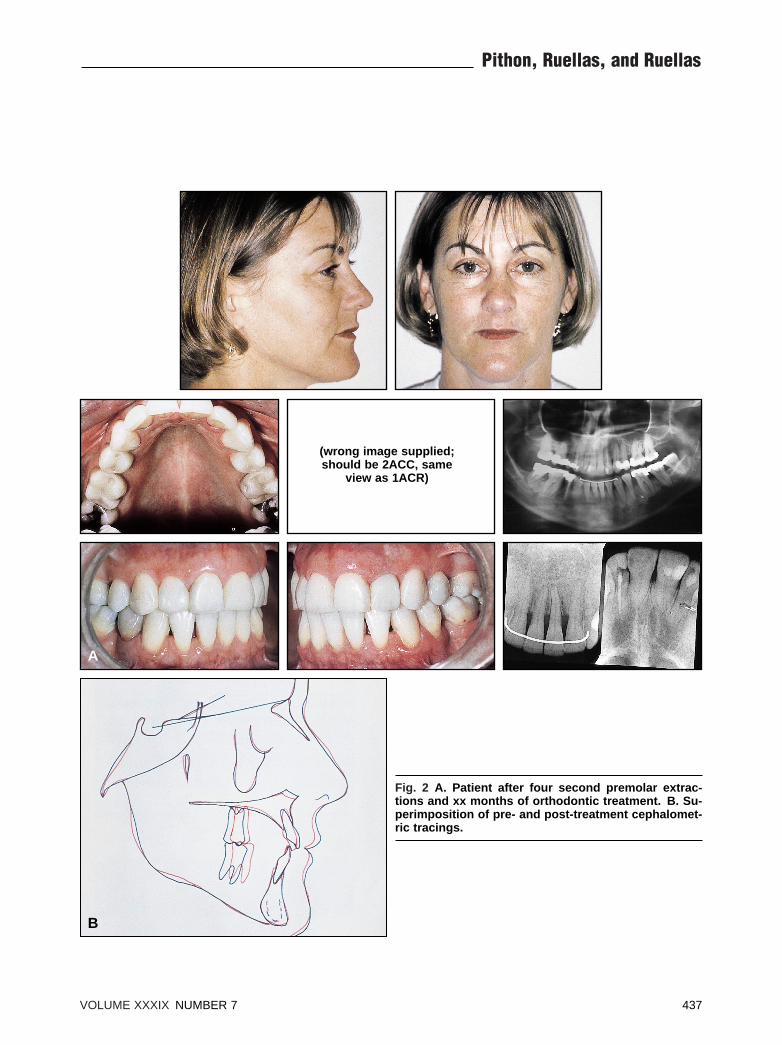
Fig. 2 A. Patient after four second premolar extrac-tions and xx months of orthodontic treatment. B. Su-perimposition of pre- and post-treatment cephalomet-ric tracings.
(wrong image supplied;should be 2ACC, same
view as 1ACR)
A
B

tionship (SNA = 78°; SNB =76°) with a skeletal Class I pat-tern (ANB = 2°). The upper andlower incisors were well posi-tioned (1-NA = 23°, 5mm; 1-NB= 22°, 4mm; 1-1 = 131°).
Treatment Plan
Premolar extractions wereproposed because of the patient’ssatisfactory lower incisor posi-tion and 7mm arch-length dis-crepancy. The second premolarswere chosen, since extraction ofthe first premolars would haveresulted in more repositioning ofthe incisors, further increasingthe concavity of the lower thirdof the face. A dose of amoxy-cillin was prescribed one hourbefore the extraction surgery toprevent infection.
Prior to orthodontic treat-ment, the patient was referred toan endocrinologist for evalua-tion of her glycemic level and toa periodontist for bacterialplaque control and oral hygieneinstruction. The patient was toldto maintain her daily dosage ofinsulin and to return to the en-docrinologist and periodontistevery three months throughoutthe orthodontic therapy, empha-sizing the need for multidiscipli-nary cooperation in the treatmentof diabetic patients. Once the pa-tient’s glycemic rate and degreeof bone loss were verified, theinitial upper and lower edgewiseappliances were placed.
Treatment Progress
Leveling and alignmentwere carried out with segmentedarches from second molar to thecanine, and the first premolarsand canines were partially re-tracted with elastic chain. Con-tinuous .016", .018", .020", and.019" ↔ .025" archwires werethen used to complete the level-ing and alignment and close theremaining spaces. An .019" ↔.025" finishing archwire withtorque and ideal bends was usedto complete the case.
After xx months of treat-ment, the appliances were re-moved. A 3-3 lower lingual re-tainer was bonded, and an upperwraparound retainer was pre-scribed.
Results
Satisfactory occlusal re-sults were achieved, with canineguidance in lateral movementsand incisor guidance in protru-sive movements (Fig. 2). Ceph-alometrically, as consequencesof the extraction space closure, aretroclination and retrusion ofthe upper and lower incisors (1-NA = 12°, 3mm; 1-NB = 21°,3mm) and a loss of molar anch-orage could be seen.
The patient’s lower facialconcavity increased because ofthe repositioning of the incisorsand aging of the soft tissues. Aslight loss of periodontal support
was observed, mainly at the ex-traction sites, which would beconsistent with the susceptibilityof diabetic patients to bone lossand inflammation.
The slow, gradual increasein orthodontic forces,22 properglycemic control, and good oralhygiene by the patient all con-tributed to the successful results.Five years after treatment, whenthe patient returned for a re-eval-uation, her occlusal and perio-dontal conditions had remainedstable.
Discussion
Orthodontic treatment of apatient with type 1 diabetes mel-litus should not begin until thedisease is properly controlled,since a diabetic patient is moresusceptible to infection and per-iodontal disease, and a hypo-glycemic crisis could lead to acoma. The maintenance of ade-quate oral hygiene is importantin avoiding bacterial plaque re-tention, especially with the pa-tient’s increased risk of cariesand periodontal disease.23
As we have shown, con-ventional orthodontic treatmentof a diabetic patient is possible,requiring only strict control ofthe force intensity and constantevaluation of the patient’s gly-cemic and periodontal condi-tions.
438 JCO/JULY 2005
Orthodontic Treatment of a Patient with Type 1 Diabetes Mellitus

1. Neville, B.W.; Damm, D.D.; Allen,C.M.; and Bouquot, J.E.: Manifestaçõesorais de doenças sistêmicas, inPatologia Oral e Maxilofacial,Guanabara Koogan, Rio de Janeiro,Brazil, 1998, p. 600.
2. Nishimura, F.; Takahashi, K.; Kurihara,M.; Takashiba, S.; and Murayama, Y.:Periodontal disease as a complication ofdiabetes mellitus, Ann. Periodontol.3:20-29, 1998.
3. Taylor, G.W.; Burt, B.A.; Becker, M.P.;Genco, R.J.; and Shlossman, M.: Gly-cemic control and alveolar bone lossprogression in type 2 diabetes, Ann.Periodontol. 3:30-39, 1998.
4. Inoue, H.; Shinohara, M.; and Ohura,K.: The effect of leukocyte function ofstreptozotocin-induced diabetes in natu-rally occurring gingivitis rat, J. OsakaDent. Univ. 31:47-54, 1997.
5. Iacopino, A.M.: Diabetic periodontitis:Possible lipid-induced defect in tissuerepair through alteration of macrophagephenotype and function, Oral Dis.1:214-229, 1995.
6. Salvi, G.E.; Beck, J.D.; and Offenbach-er, S.: PGE2, IL-1 beta, and TNF-alpharesponses in diabetics as modifiers ofperiodontal disease expression, Ann.Periodontol. 3:40-50, 1998.
7. Oliver, R.C. and Tervonen, T.: Diabe-tes—A risk factor for periodontitis inadults? J. Periodontol. 65:530-538,1994.
8. Grossi, S.G. and Genco, R.J.: Periodont-al disease and diabetes mellitus: A two-way relationship, Ann. Periodontol.3:51-61, 1998.
9. Emingil, G.: Darcan, S.; Keskinoglu, A.;Kutukculer, N.; and Atilla, G.: Localizedaggressive periodontitis in a patient withtype 1 diabetes mellitus: A case report, J.Periodontol. 72:1265-1270, 2001.
10. Firatli, E.: The relationship betweenclinical periodontal status and insulin-dependent diabetes mellitus: Result after5 years, J. Periodontol. 68:136-137,1997.
11. Cohen, D.W.; Friedman, L.A.; Shapiro,J.; Kyle, G.C.; and Franklin, S.:Diabetes mellitus and periodontal dis-ease: Two year longitudinal observa-tions, Part I, J. Periodontol. 41:709-712,1970.
12. Cianciola, L.J.; Park, B.H.; Bruck, E.;Mosovich, L.; and Genco, R.J.: Preva-lence of periodontal disease in insulin-dependent diabetes mellitus (juvenilediabetes), J. Am. Dent. Assoc. 104:653-660, 1970.
13. Nevins, M.L.; Karimbux, N.Y.; Weber,H.P.; Giannobile, W.V.; and Fiorellini,J.P.: Wound healing around endosseousimplants in experimental diabetes, Int. J.Oral Maxillofac. Implants, 13:620-629,1998.
14. Shyng, Y.C.; Devlin, H.; and Sloan, P.:The effect of streptozotocin-inducedexperimental diabetes mellitus on cal-varial defect healing and bone turnoverin the rat, Int. J. Oral Maxillofac. Surg.30:70-74, 2001.
15. Krakauer, J.C.; McKenna, M.J.; Buder-er, N.F.; Rao, D.S.; Whitehouse, F.W.;and Parfitt, A.M.: Bone loss and boneturnover in diabetes, Diabetes 44:775-782, 1995.
16. Glavind, L.; Lund, B.; and Loe, H.: Therelationship between periodontal stateand diabetes duration, insulin dosageand retinal changes, J. Periodontol.39:341-347, 1968.
17. Hugoson, A.; Thorstensson, H.; Falk,H.; and Kuylenstierna, J.: Periodontalconditions in insulin-dependent diabet-ics, J. Clin. Periodontol. 16:215-223,1989.
18. Thorstensson, H. and Hugoson, A.:Periodontal disease experience in adultlong-duration insulin-dependent diabet-ics, J. Clin. Periodontol. 20:352-358,1993.
19. Tervonen, T. and Knuuttila, M.: Relationof diabetes control to periodontal pock-eting and alveolar bone level, Oral Surg.Oral Med. Oral Pathol. 61:346-349,1986.
20. Safkan-Seppala, B. and Ainamo, J.:Periodontal conditions in insulin-depen-dent diabetes mellitus, J. Clin. Perio-dontol. 19:24-29, 1992.
21. Tervonen, T.; Karjalainen, K.; Knuuttila,M.; and Huumonen, S.: Alveolar boneloss in type 1 diabetic subjects, J. Clin.Periodontol. 27:567-571, 2000.
22. Rey, A.C.: Movimento ortodôntico emratos “wistar” com diabetes mellitusinduzido, UFRJ/Faculdade de Odonto-logia, Rio de Janeiro, Brazil, 2003.
23. Bensch, L.; Braem, M.; Van Acker, K.;and Willems, G.: Orthodontic treatmentconsiderations in patients with diabetesmellitus, Am. J. Orthod. 123:74-78,2003.
REFERENCES
VOLUME XXXIX NUMBER 7 439
Pithon, Ruellas, and Ruellas