case presentation - · pdf filecase presentation litong du m.d. ... after the first egd, ......
TRANSCRIPT

Case Presentation
Litong Du M.D.SUNY Downstate Medical Center

History
58 yo male 1 day history of black stools with No feverNo N/V, no hematemesisNo Abdomen pain

History
PMH: A-fib, no PUDSocial: smoking 1-2 ppd, no alcohol or illicit drug use Allergies: NKDAMedications: Coumadin, no NSAIDs
Physical Exam
T 98.7 P 80 R18 BP 155/86General: good, AA&Ox3Chest: CTABCVS: RRR, S1,S2ABD: soft, ND/NT, BS+, no mass, no surgical scar, stool guaic positiveNG lavage: positive for bloodNeuro: intact

Labs and studies
UA: Negative
EKG: WNL
CXR: WNL
8.8
5.712.1
34.2144 30.3 28
2.9
139 108 14
3.8 29 1.2134 6.9
4.2
30
21
66
1.6/0.3

Hospital Course
While patient in ER, passed 2 large BMHCT dropped to 28, then 25NPO, NGT, 2 large IV and foleyAggressive fluid, blood transfusion, and FFP/Vit K, and PPI dripSurgery and GI consultedAdmitted to ICUEmergent EGD scheduled

Hospital Course
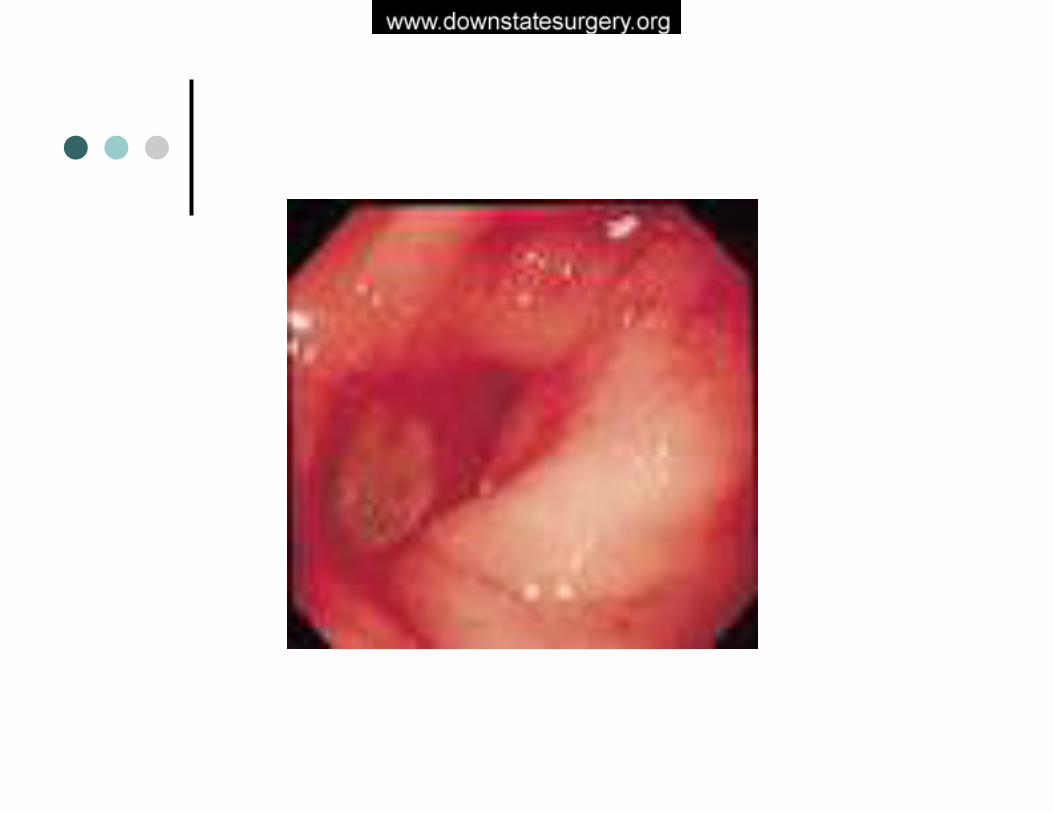
EGD showed large amount of blood was pooling in the bulb with clots, and a bleeding lesionThe area was washed and 1/10000 epinephrine was injected , bleeding stopped.Patient was transferred back to ICU for close observation. Patient remained hemodynamically stable.

Hospital CourseAfter the first EGD, Patient was stable for 8 hours with no active bleeding, responding well to blood transfusion.Then started another large BM with dropping of HCT to 20, though hemodynamically remained stable.Aggressive resuscitation and second EGD attempted.EGD showed deformed bulb, fresh blood oozing. Large blood clot. Epinephrine injected times 4 and bleeding stopped


Hospital Course4 hrs after the second EGD, patient started bleeding again and dropped HCT, although vital signs remained stablePatient was aggressively resuscitated with fluid and blood productsDecision was made to take the patient to the operating room.

First EGD Second EGD
OR

OR CoursePatient was taken to OR emergently Middle line incision madeTranspyloric incision made, a posterior wall ulcer with large blood clotOversewing of the base of ulcer in four quadrantsPyloroplasty and truncal vagotomy performedPatient tolerated the procedure well, was brought to ICU intubated

Hospital Course
POD#1: extubated and remained NPO and PPI dripPOD#2: OOBPOD#3: started clear and started PO antibiotics for H.pylori and PPIPOD#4: transfer to regular floorPOD#5: Gas and Bowel movement, advance to regular diet. Patient remained stable HCTPatient discharged home with H.pylori treatment and PPI for acid.

Pathology
Blood clot with organizationPosterior and anterior vagusspecimen: nerve present


Operative management of Duodenal UlcerLitong Du M.D.SUNY Downstate Medical Center

History and Evolution of ulcer surgery
350 B.C Dioceles gastric ulcer
1688 Muralto duodenal ulcer

History and Evolution of ulcer surgery
1881 Billroth distal gastrectomy and gastroduodenostomy (Billroth I)1882 Czerny Local ulcer excision1885 Billroth distal gastrectomy and gastorjejunostomy(Billroth II)

History and Evolution of ulcer surgery
1886 Heinekepyloroplasty1888 Mikulicz-Radecki performed the same operationHeineke-Mikulicz pyloroplsty

History and Evolution of ulcer surgery
1892 Jaboulaypyloroplasty
1902 Finney pyloroplasty

History and Evolution of ulcer surgery
First described byCellen-Jones in 19291937 Graham omental patch for perforated ulcer
Cellen-Jones C.J., A rapid method of treatment in perforated duodenal ulcer. BMJ (1929) 1 : pp 1076-
Graham R.R., The treatment of perforated duodenal ulcers. Surg Gynecol Obstet (1937) 64 : pp 235-.

History and Evolution of ulcer surgery
1945s Dragstedtand Owen truncal vagotomy1950 truncal vagotomy and drainage became a standard ulcer operation

History and Evolution of ulcer surgery
1952 Farmer and Smithwick truncal vagotomy and hemigastrectomy1953 Edwards and Herrington vagotomy and antrectomy

History and Evolution of ulcer surgery
1957 Griffith and Harkins described Parietal cell vagotomy (HSV)

History and Evolution of ulcer surgery
1977, histamine H2 antagonist introduced to market1988 Proton-pump inhibitor introduced to the market

History and Evolution of ulcer surgery
1982, Marshall BJ identified the association of H. pylori infections and peptic ulcerAntibiotics treatment standard
Marhsall BJ et al, Unidentified Curved bacilli in the stomach of patients with gastritis and peptic Ulceration. Lancet 1984;1:1311-1315

Operative “building blocks”
Acid reductionDrainageResection and reconstruction Omental patchOversewing

Acid Reduction: VagotomyTruncal vagotomy
Reduces output 85% and 50%Abolishes the receptive relaxationNeed drainage proceduresPost-vagotomy Syndrome
SelectivePreserves celiac and hepaticStill requires drainage procedures
High selectiveSelectively denervating acid producing parietal cell massNo need for drainage

Drainage procedures
Heineke-MikuliczJaboulayFinney Gastrojejunostomy

Resection and reconstruction
AntrectomySubtotalTotal
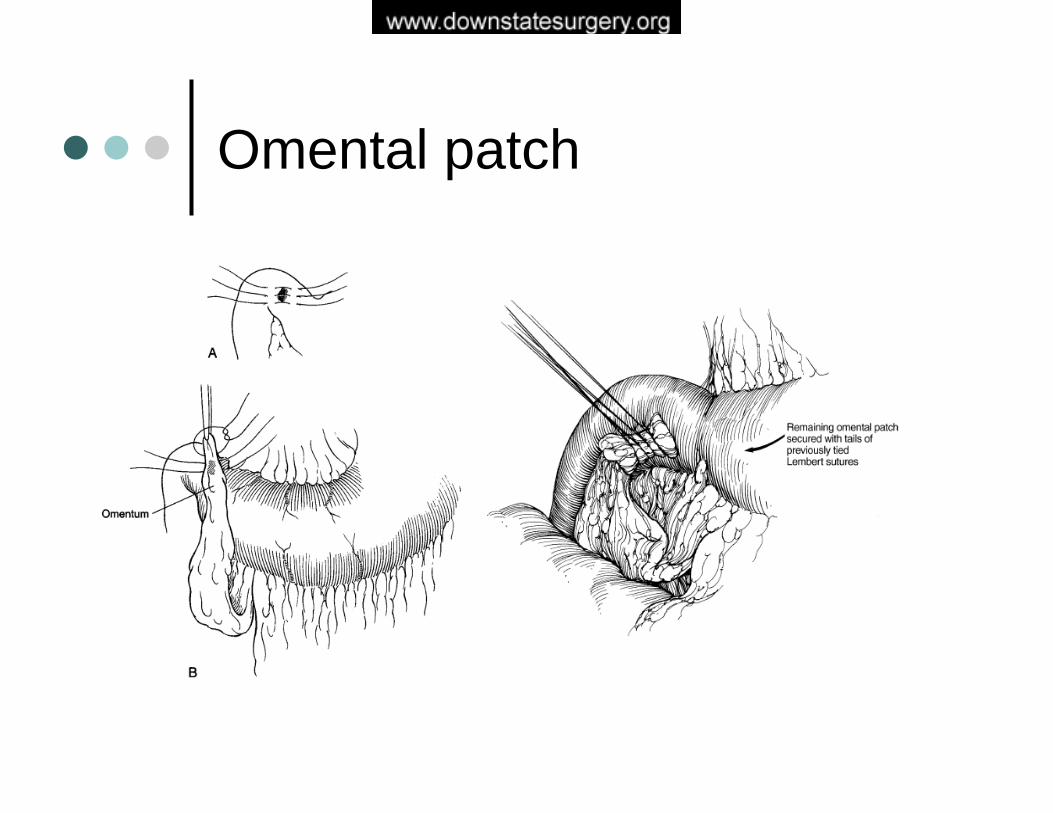
Omental patch

Oversewing
Longitudinal gastoduodenotomyOversewing Bleeding ulcer with “u” stitchSuture above, below the bleeding site, and pancreatic side for transverse pancreatic artery

Surgical options
HSVTV+DTV+A
HSVTV+DTV+A
Intractability
HSV+DTV+DTV+A
HSV+DTV+DTV+A
Obstruction
Omental patch+HSVTV+DTV+A
Omental PatchUlcer excision+patch
Perforation
Oversew+HSVOversew+TV+DTV+A
OversewOversew+TV+DTV+A
Bleeding
Ideal patientsCompromised patients

Surgical options
Highly selective vagotomy(HSV)Vagotomy and drainage(TV+D)Vagotomy and antrectomy(TV+A)

Mulholland MW, Debas HT: Chronic duodenal and gastric ulcer. Surg Clin North Am 67:489, 1987.
1-220Severe2025< 5Mild
Diarrhea (%)1-210Severe
10-1510< 5MildDumping (%)
< 25-155-15Ulcer recurrence rate (%)
<1<10Operative mortality rate (%)
TruncalVagotomy
andAntrectomy
TruncalVagotomy
andPyloroplasty
ParietalCell
Vagotomy
Clinical Results of Surgery for Duodenal Ulcer

Surgery complications

Indications for surgery
Bleeding PerforationObstructionIntractability

Indications for operation for bleeding duodenal ulcers
Hemodynamic instability despite vigorous resuscitation (>3 unit transfusion) Failure of endoscopic techniques to arrest hemorrhage Recurrent hemorrhage after initial stabilization (with up to two attempts at obtaining endoscopic hemostasis) Shock associated with recurrent hemorrhage Continued slow bleeding with a transfusion requirement exceeding three units per day
Surgical options for bleeding
Compromised patients:OversewingOversewing+TV+DTV+antrectomy
Ideal surgical candidates:Oversewing+HSVOversewing+TV+DTV+antrectomy
“The use of a definitive ulcer-curing operationis mandatory in patients who have hemorrhage”
Johnston D Duodenal and gastric ulcer. In: Schwartz SI, Maigot’sabdominal operations. 9th edition. Norwalk: Appleton-Lange; 1989. P.599


J Am Coll Surg, Vol. 202, No.1, January 2006


“With the new approach, surgery, if necessary, should aim at stopping the hemorrhage and not curing the disease.”
Ohmann C: Trends in peptic ulcer bleeding and surgical treatment. World J Surg 2000, 24:284

Indications for operation for perforated duodenal ulcers
Surgery is almost always indicatedUnless patient is stable with no peritonitis, and confirmed sealed perforation

Surgical options for perforation
Compromised patients:Simple omental patchUlcer excision with patch
Ideal surgical candidates:Simple omental patchUlcer excision with patchHSVT+DT+A


107 patients with perforated duodenal ulcer treated patch+HSVPatients followed up-up up to 21 yearsRecurrent rate 7.4% and reoperative rate 1.9%The study confirmed patch+HSV is an excellent choice.

Randomized studyAfter simple closure of perforation, patient either treated with quadruple anti-helicobacter therapy or omeprazole aloneUlcer relapse significantly less in the treated groupEradication of H. pylori prevents ulcer recurrence and immediate acid reduction surgery is unnecessary

Laparoscopic procedures
Taylor: posterior truncal vagotomy and anterior seromyotomyHill-Barker: posterior truncal and anterior highly selective vagotomyTruncal vagotomy and pyloromyotomy

Objective: to compare the results of open vs. lap repair for perforated ulcersMethods: From 1994 to June 1997, 130 patients were randomly assigned either groupConclusions: Lap repair is safe and reliable.

Siu et al: Laparoscopic repair for perforated peptic ulcer: a randomized controlled trial.Ann Surg. 2002 Mar;235(3):313-9

Siu et al: Laparoscopic repair for perforated peptic ulcer: a randomized controlled trial.Ann Surg. 2002 Mar;235(3):313-9

Are we ready?

Espat et al: J Gastrointest Surg. 2004 May-Jun;8(4):471-8.

Espat et al: J Gastrointest Surg. 2004 May-Jun;8(4):471-8.

Espat et al: J Gastrointest Surg. 2004 May-Jun;8(4):471-8.

Summary
Ulcer surgery has changed dramatically over the past 30 yearsSurgery is reserved for complicated ulcers or ulcer complicationsMost surgeons now favor a minimalist approach for perforations or bleeding