caruth med app
DESCRIPTION
medicaid appTRANSCRIPT
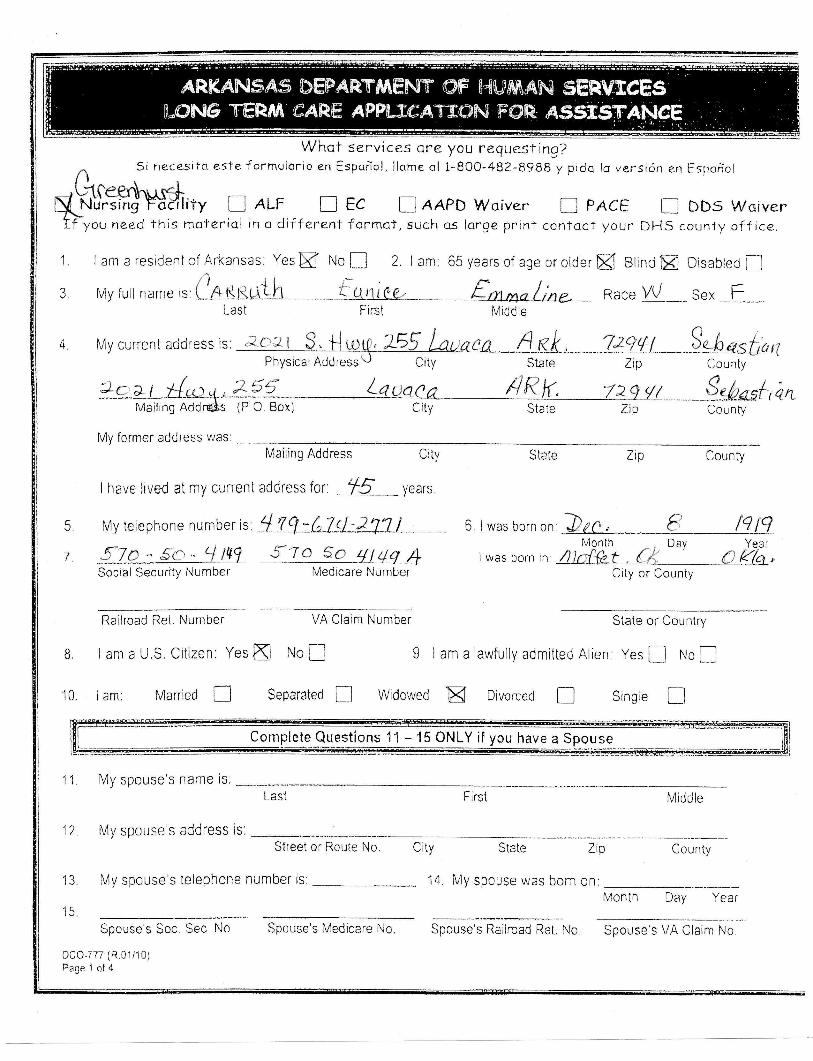
Whqt services qre you requesting?
#:ffi ;,. ;:#: ;ffi;H{d l*li{**,"I am a resident of Arkansas: Yes ffi No l] 2. I am. 65 years of age or older K gtind E Disabteo f]Myfuilnameis:Cee,*'dh---_-foni(uMRaceVU-_sex-F
1
?
Last First Middie
6
7
rMy currenr address is ao:tr 3. !|illq, 755 lauaco fr.Kk, ..- ?*9!l- "$*A -ast'rn:PhysicalAddre*su City State Zip County
570*-:.5c ^ Ll ttlg 57o so 4tua 4Yeer
Social Security Number Medicare Number
Railroad Ret Number VA Claim Number State or Country
I am a U.S. Citizen; Yes ffi No E I lam a lawfully admitted Alien: Yes I No I
lam: Married I Separated n Widowed X Dir,trced t]
*--.*,a i-t{* +, 45q - eggt - - S&as{,q.,tMailrng AddrgLs (P 0 8ox) City State Zip County
My forrner address was:Mailing Address Ciry State Zip Counly
I have lived at my cunent address lar f5 years.
My tetephone number is _179_:C*t:Za7l- 6. I was born on: ,.r " I lq fq
o
10. Single
City or County
Complete Questions 11 - 15 ONLY if you have a Spouse
My spouse's name is;
Last First Middle
13" My spouse's telePhone number is
12 My spouse s address is
Spo,,seb Soc.S.;N" "*
oco"777 (R 01/10)Page 1 ol 4
Street or Route No. City
14.
Srate Zip County
My spouse was bom on:Month Day Year
Spouse's Medicare No. Spouse s Railroad Ret. No Spouse's VA Claim No
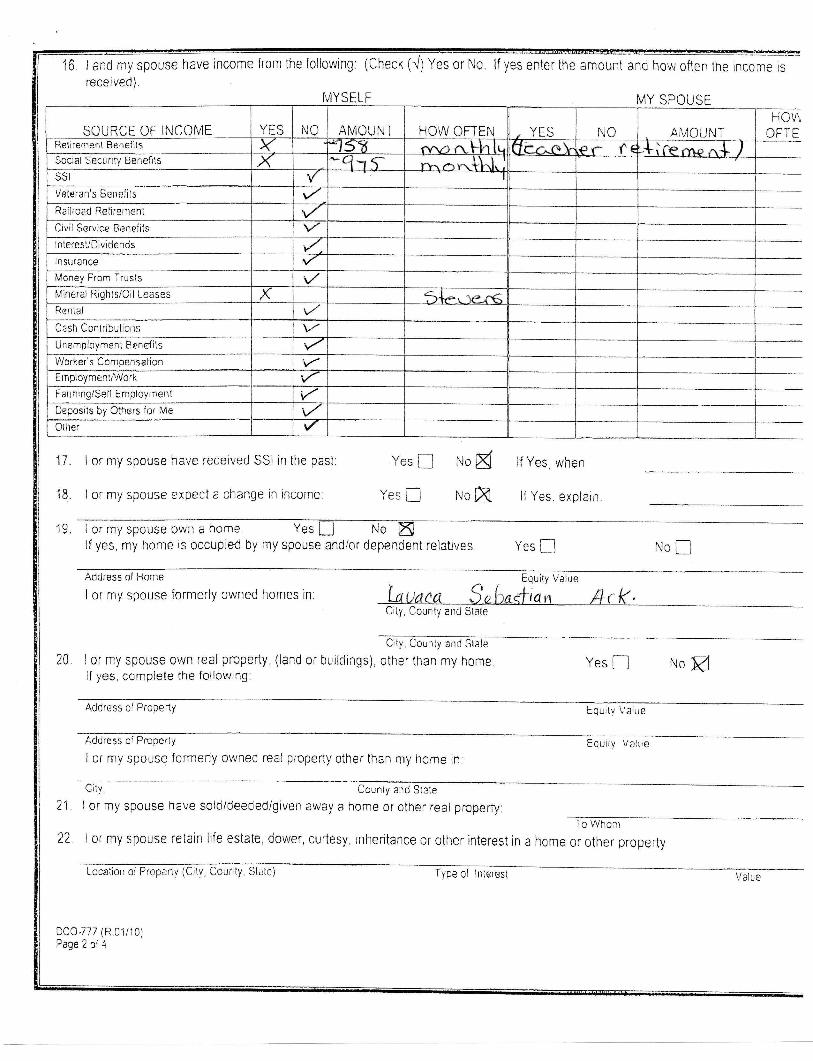
16 land my spouse have income {rom the following: (Check (./)Yes or No.
received) MysELF
lf yes enter the amount arrd how oflen the in.or. u
MY SPOUSE
SOURCE OF INCOME AMOUNT
Money From Trusts
Mineral Rights/Oil Leases
Cash Contributrons
Worl..er's Compen93lion
Fanning/Seli Employrnent
Deposits by Others for Me
17.
18.
19.
I or my spouse have received SSI in the past:
I or my spouse expect a change in incorne:
Yes D
Yes f
lf Yes, when
lf Yes, explain
r'roK
r.ro xI or my spouse own a home Yesl I No
lf yes, my home is occupied by my spouse and/or dependent relatives Yes L-l nNo
Address of Home
I or my spouse formerly owned homes in
I or my spouse own real property, (land or buildings),If yes, complete the following:
itv Value
qn
tu
Cily, Counly end State
, County and Slate
other than my home Yes fl NoM
Ac.idress ol Prope(y Equitv Value
Address ol Properly
I or my spouse formeriy owned real property other than my home in
Equily Valtre
Citv, County aud State
LI
t1
I or my spouse have sold/deeded/given away a home or other real prcperty:To Whonr
I or my spouse retain life estate, dower, curtesy, inhentance or other interest in a home or other prope(y
Locaiion ol Propertv (Cilv, Courrty, State)
DCO-777 (R.01/10)Page 2 of 4
Iype of Inleresi \/alue

23, I or rny spouse ovvn personal property such as cars, trucks, tractors or famr machinery, Irailers boats, etc,: (lf more thanthree, please list on a separate sheet)
Item (l/ako, Model, and Year) Equily \ralue
Item (lv1ake, Model, and Year) Equily Value
L+.
Iterrr (Make. Model, antj Year)
I or my spouse own IivestockYes tl No A
Equity Vslue
(cattle, poultry, cat{lsh minnows. cnckets, worms, etc )
lf yes, complete the lollowrng:
Type of Livestock and Nurnber Owned
I or my spouse have the following assets. (Check lrl) Yes or No. lf yes. enter the amounUvalue, tocation of theof joint owner, if any.)
Valtre
asset, and narne
TYPE YES NO AMTI/ALUE LOCATION OF ASSET
Cash ,/ o-:.*l- l)^{:r*.Checkino Account \/ e\k=B t.r.^oaSavinqs Account ,{Other Savinqs (Ce(ificates, eh.) \ZPromissory Notes r<Stocks gBonds
Patient Fund AccountMortgaqe wEurial PloUCrvot \,/ )rX.l\r ,( )crn (er.ror.eLleBurial Funds/l nsuranceLife lnsurance 1/.Trusts \-Other
NAME OF JOINTOWNER
26. lor my spouse ha-ve additional income andlor property (realor personal)lhat I was unable to list under rtems 16 through 23Yes [] rrro K lf yes, record your answeils)'orr a separate sheel
27 . I or my spouse.have other resources (real or personal properly) that are berng hetd {or me by a nother individualYes n No K lf yes, complete the following:
Type of Resource Location of Resource AmUValue
Type of Resource Location of Resource AmUValuts
28IA
or my spouse_have ical insurance coverage. Yes K{
Name and Address of lnsurance Company
I have unpaid medical expenses from the past three (3) monlhs. yes Il, or someone in my household, would like to learn to read, or lo read better
G. J r#'
6f4ilej!5rorrowr n'
,ED Y",/W31+722.Policv No
29.
30
31
No
Yes
Ktr
Do you have Long Term Care lnsurance? Yes I ru. dDC0-777 (R 01/10)P:ge 3 of 4
ruoH

,I understand tha( I must help establish my elrgibilrty by providing as much of the requested information as I can.I authortze the oepa(meni o{ Human Services to make any investigation conc,erning me and/or my spouse necessary to establish myelgibility lor assistance,I undersland thal no person may be denied long term care assistance or olher Medicaid assistance on the grounds of race, color, sex.national origin or disabilitY.lunderstand that lmay request a hearing be{ore the state agency represenlative if a decision is nol reached on my ffise within theappropriate time limit or it ldisagree uvtth the dectsion reeched.
lagree to notfy the Deparhent o[ Human Services within 10 days if lor my spouse receive additional income acqurre or dispose olproperty or if any oUter changes orcur in my circumstances,
I authorize the Department of Human Services to examine all records of mine, or records of those receivrng or having received tr4edicaidbenefils through me, for the purpose of investigaing whether or not any person may have cornnri6ed Medicaid fraud or for use in anylegal, administrative or ludicial proceeding,
I understand liat I must pro\'lde my Social Security Number as a condition ol my eligibi[ty, and I undersland that this nurnber nray beused by the Agency without rny express permission in a computer match to obtain informalion relatrve to my eligibilily for assistancefronr the Social Security Adrninistration, Departrnentof Workforce Services, lnternal Reventre Services, or other agenciesAS$IGNMENT OF MEDICAL SUPPORI, I authorize any holder ol medical or other inlorma[on about me to release infornrationneeded for a Medicaid claim to DHS i further authorize release of any in[orrnation to other parties who may be lrable for rly rnedicaiexpeilseS. As an eligibility conditron lautomalically assign rny rightto any settlement, ludgement, or awarcl which rnay be obtainedagainsl anythirdpartytoDHStothefull extentofanyamountwhichispaidbyDHsonmybehalf. lauhorizeandrequestthatfurrcjs.settlernent or other payments firade by or on behalf of third per(ies, inoludtng tortfeasors or insurers arising out of a Medicaid claim, bepaid directly to DHS My application for Medicaid benefits shall in itself constitute an assignment by operation of law and shalt beconsidered a statutory lien of any settlement. jlrdgement, or award received by me from a third parly, A third parry is any person, ontity,institution, organization or other source which rnay be liable for iniury, disease, disabilrty or death sustained by me or oihers nanredherein. irrcJuding estates of said individuals I aiso assign all rights in any sefllemeni made by me ot on my behalt ari5ing out of anyclairn to the exlent of medical expenses paid by DHS, whether or not a po(ion of such settJement is designated for medical expenses.Any such funds received by me shall be paid to DHS. A copy of this authoriradon may be used in pioce ol the originellunderstand the requirement to disclose, in my application for Long Term Care services, information regarding any rnterestthat I or my comrnunity spouse may have in an annuity.I understand the requirernentto name the state as a romainder beneficiary in which lor my spouse is the annuitant.lf you have questions or problems regarding your application or care, please call your State Long Term Care Ombudsman at501,682-8S52IMPORTANT ESTATE RECOVERY NOTICE:
lf you receive Medicaid in a nursing facility, ICFIMR facility, or under a hotne and community based waiver program, he totalsrnounl0fthe Medicaid benefits paid on your behalf will be a debt lo DHS and may be recovered from your €state or from the grantee of a
beneficiary deed after your death Your estate is the pioperty you o\{n atthe trme otyour death DHS will not make a claim against yorrrestate while you are living DHS will not make a claim against your eslate after your death if your spouse is still living, or if you havedependent children under age 21 or blind or disabled children DHS will collect the debl, if any, by filirrg a claim irr your eslateCollectionmaynotbemadeifit isnot cost effoctivetoDHSorifyourheirsapplyforahardshipwaiverafteryourdeath Ahgrd5hipqrsyexisl iF the estate property is the only source of income for your heirs, if that incorne is limrted, 0r it there are otlrer conrpellingcircumstances.CERTIFICATION: I H,AVE READ IHE ABOVE STATEMENTS AND I AGREE TO THEIR PROVISIONS.
FOR LONG TERM CARE FACILITY RECIPIENTSIAPPLICANTS 0NLY: After reviewing the alternatjves Io nursrrrq facrlity placementavailable through he Depsrtmentof HUman ServiCes, lunderstand that lam choosing to be served in a nursing facilityI understand that if lam admitted to a nursing facility based on conditional Medicaid approval and nry Medicaid case is denied, l, or myfamily, will be responsible for any indebtedness while in the nursing facilityI understand that this form is signed subject lo psnalties for perjury, I understarrd thal ii I receive assislance to which I am not entitled asa rosult of withholding informatjoll or providing inaccurate inlormation, such assisl ill be subioct lo recovery by the DepBrtmenI ofHurrran Services and I rnay be sublect to prosecution for fraud and
Wilness (if signed by mark)iDate
Address of Wilnessffelephone Number
Name of Person Who Helped Complete Form/Date
Dl/bl tZDate
477- 4571b07?Telephone Number
oQa-777 (R o1l10)
--.--Pagedof4
AlBq So jk,t 45, fa,oirut- AlLflqqlGuardian or Aulhonzed Rep. s Address

Arkansas Department of Human ServicesDivision of County Operations
DISPOSAL OF ASSETS DISCLOSURE
Si necesita este formulario en Espaflol, llame al l-800-482-8988 y pida la versi6n en Espafiol
lf you need this material in a different format, such as large print, contact your DHS county Office.
Medicaid rules require the complete disclosure of all asset transfers (real or personal property transfers)
made by yourself or your spouse since 02-08 -2006. Al1 such transfers must be documented by the local
Human Services Office to determine your eligibility for Medicaid assistance. Read each part of this form
carefully to determine parts which apply to you.You must complete and sign Part A or Part B.
Please complete another form to report additional transfers.
PART A. ASSETS TRANSFERRED
Please provide a copy of your trusttr I (or my spouse) established a trust or annuity onand/ or annuity documents. (Date)
tr I (or my spouse) have sold, transfeffed, assigned, or given away the following assets (cash, checkingaccounts, securiti real or , etc. since 02-08 -2006:
Address Telephone Number(Please use an additional sheet ofpaper ifneeded).
This statement is true to the best of my knowledge, and I understand that should I give a false statement, Imay be subject to criminal prosecution. I also understand that I will be liable for any overpayments made
on my behalf by the Arkansas Medicaid program due to my misrepresentation of fact(s).
Signature
PART B. NO ASSETS TRANSFERRED
I (or my spouse) have not established a trust or annuity, and have not sold, transferred, assigned,
or given away any assets (cash, checking accounts, savings accounts, securities, real or personalproperty, etc.) since 02-08-2006. This statement is true to the best of my knowledge, and Iunderstand that should I give a false statement, I may be subject to criminal prosecution. I also
understand that I will be liable for any overpayments made on my behalf by the Arkansas
Medicaid program due to my misrepresentation of fact(s).
DCO-727 (R.02l10)Page 1 of2
N
Transferred to(Name)
Provide the address and telephone number below for the person that received the item.
Signature -t?/te //3