carotid artery disease: plaque features and vulnerability866385/fulltext01.pdf · carotid artery...
TRANSCRIPT

Carotid artery disease: plaque
features and vulnerability
Fisnik Jashari
Department of Public Health and Clinical Medicine
Umeå, 2015

Responsible publisher under Swedish law: the Dean of the Medical Faculty This work is protected by the Swedish Copyright Legislation (Act 1960:729) New Series No:1760 ISBN: 978-91-7601-364-9 ISSN: 0346-6612 Elektronisk version tillgänglig på http://umu.diva-portal.org/ Tryck/Printed by: Print & Media, Umeå University Umeå, Sweden, 2015

“Research is to see what everybody else has seen, and to think what nobody else has thought”
Albert Szent-Gyorgyi
To my family


i
Table of Contents
Abstract iv
List of Papers vi
Abbreviations vii
INTRODUCTION 1
Pathophysiology of atherosclerosis 1
Lesion types 2
Pathomechanisms of ischemic events 5
Risk factors 6
Epidemiology 6
CAROTID ARTERY STENOSIS 6
Who is at risk? 7
Degree of stenosis assessment 8
Carotid artery plaque features: the concept of plaque vulnerability 10
Imaging plaque features 10
Surface plaque morphology 10
Plaque composition 11
Thin cap fiboatheroma 12
Neovascularization and intraplaque hemorrhage 13
Arterial calcification 13
ASYMPTOMATIC CAROTID STENOSIS 14
Management of asymptomatic patients with carotid stenosis 15
Identifying high-risk asymptomatic patients 15
Bilateral carotid disease 16
“Silent” brain infarction 16
Multisite atherosclerosis disease 16

ii
Ultrasound markers of plaque vulnerability 17
Microembolic signals detection by transcranial Doppler 18
SYMPTOMATIC CAROTID STENOSIS 19
Management of symptomatic patients with carotid disease 20
Medical therapy 20
Interventional therapy 21
Identifying patients at high risk of symptom recurrence 23
Ultrasound imaging markers of vascular risk: subclinical atherosclerosis 24
Carotid artery wall measurements: intima-thickness and intima-media GSM 25
OBJECTIVES 28
METHODS 29
Preoperative patients evaluation 29
Definitions and clinical data of patients included in studies I, II and III 29
Carotid ultrasound examinations 30
Ultrasound data retrieval 30
Extraction of the carotid ultrasound examinations 31
Definitions of ultrasound derived plaque and intima-media complex features 31
Intima–media complex measurements 33
Cone Beam CT (CBCT) analysis 34
Carotid endarterectomy (CEA) procedure 34
Source of data 35
Inclusion/exclusion criteria 36
Statistical analysis 38
RESULTS 40
Study I 40
Study II 43
Study III 47

iii
Study IV 50
DISCUSSION 57
LIMITATIONS 64
CONCLUSIONS 66
Acknowledgement 68
References 70

iv
Abstract
Background: Atherosclerosis is an important cause of stroke. Ultrasound offers the
convenience of real-time and detailed assessment of carotid plaque features as well as
arterial wall thickening and composition. Evaluation of these features is important for
determining patients’ risk of suffering vascular events and also contributes to selecting
the best treatment strategy.
Methods: Using ultrasound data analysis we have determined plaque features in the
bifurcation and internal carotid artery (ICA), including: surface plaque irregularities,
calcification, echogenicity (grey scale median-GSM) and other textural plaque features
(Juxtaluminal black area, entropy, coarseness). In addition, intima media thickens (IMT)
and its grey scale median (IM-GSM) was measured in common carotid artery (CCA).
Using Cone Beam CT (CBCT) we have quantified calcification volume of the carotid
plaques extracted after carotid endarterectomy procedure. For the meta-analysis we have
used comprehensive meta-analysis software version 3.
Study I: We have included 39 patients and we compared carotid plaque features of the
contralateral arteries with those located ipsilateral to symptomatic side and arteries of
asymptomatic patients.
Study II: The accuracy of US to detect atherosclerosis calcification was assessed against
CBCT in 88 patients.
Study III: Based on the previous vascular events in coronary, carotid and lower extremity
arterial system, 87 patients were divided into three groups: asymptomatic, symptoms in
one vascular system and symptoms in more that one vascular system. IMT, IM-GSM and
plaque features were compared between groups.
Study IV: We have meta-analyzed ten cohort prospective studies evaluating carotid
plaque echogenicity for cerebrovascular symptoms prediction.
Results: Study I. Plaques of the contralateral to symptomatic arteries had similar features to those
in symptomatic and more vulnerable than asymptomatic arteries.
Study II. Carotid ultrasound was accurate in detecting calcification volumes of ≥8mm3
with very high sensitivity but it was less accurate in detecting lower calcification volumes

v
(<8mm3). Carotid calcification was not different between symptomatic and asymptomatic
patients.
Study III. Echogenicity of the intima-media complex (IM-GSM), but not its thickness
(IMT), was significantly decreased with increasing number of arterial systems affected by
atherosclerosis. IM-GSM was lower in patients with prior myocardial infarction and
stroke.
Study IV. Carotid plaque echogenicity evaluated by US could predict future
cerebrovascular events in patients with asymptomatic, relative risk RR 2.72 (95% CI,
1.86 to 3.96), and recurrent symptoms in symptomatic patients, RR 2.97 (95% CI, 1.85-
4.78).
Conclusion: Plaques located in the contralateral to symptomatic arteries have similar
features as symptomatic side and more vulnerable than asymptomatic arteries. Carotid
ultrasound could accurately detect larger but not smaller carotid plaque calcification
volumes (<8 mm3). Low IM-GSM could identify patients with multi-system
atherosclerosis disease, suggesting a better marker for determining systemic
atherosclerosis disease burden compared to conventional IMT. Finally, carotid plaque
echogenicity predicts future cerebrovascular events in patients with symptomatic and
asymptomatic carotid stenosis.
Keywords: Carotid atherosclerosis, ultrasound, plaque features, echogenicity, calcification, surface
plaque irregularities, subclinical atherosclerosis, cerebrovascular symptoms

vi
List of papers
I: Ibrahimi P, Jashari F, Johansson E, Gronlund C, Bajraktari G, Wester P, Henein
MY. Vulnerable plaques in contralateral carotid arteries in symptomatic patients:
A detailed ultrasound analysis. Atherosclerosis. 2014 Aug; 235(2):526-31.
II: Jashari F, Ibrahimi P, Johansson E, Ahlqvist J, Arnerlöv C, Garoff M,
Jäghagen EL, Wester P, Henein MY. Atherosclerotic Calcification Detection: A
Comparative Study of Carotid Ultrasound and Cone Beam CT. Int J Mol Sci. 2015
Aug 21;16(8):19978-88.
III: Jashari F, Ibrahimi P, Johansson E, Grönlund C, Bajraktari G, Wester P,
Henein MY. Carotid IM-GSM is more accurate than conventional IMT for
monitoring systemic nature of atherosclerosis. Manuscript.
IV: Jashari F, Ibrahimi P, Bajraktari G, Wester P, Henein MY. Carotid plaque
echogenicity predicts cerebrovascular symptoms: A systematic review and meta-
analysis. Manuscript submitted.

vii
Abbreviations ACAS Asymptomatic Carotid Atherosclerosis Study ACSRS Asymptomatic Carotid Stenosis and Risk of Stroke ACST Asymptomatic Carotid Surgery Trial ANSYSCAP Additional Neurological SYmptoms before Surgery of the Carotid Arteries ARIC Atherosclerosis Risk In Communities BMT Best Medical Treatment CAS Carotid Artery Stenting CAV Cardiovascular CBCT Cone Beam Computed Tomography CCA Common Carotid Artery CEA Carotid Endarterectomy CEUS Contrast Enhanced Ultrasound CV Cerebrovascular CT Computed Tomography CTA Computed Tomography Angiography DSA Digital subtraction angiography ECST European Carotid Surgery Trial GSM Grey Scale Median HDL High Density Lipoprotein HR Hazard Ratios ICA Internal Carotid Artery IMT Intima-Media Thickness IM-GSM Intima Media-Gray Scale Median IPH Intraplaque Hemorrhage JBA Juxtaluminal Black Area LDL Low Density Lipoprotein MES Microembolic Signal MI Myocardial Infarction MRA Magnetic Resonance Angiography MRI Magnetic Resonance Imaging NASCET North American Symptomatic Carotid Endarterectomy Trial NRI Net Reclassification Improvement OR Odds Ratios PET Positron Emission Tomography PT Plaque Type TCD Transcranial Doppler US Ultrasound VA Veteran’s Affairs

viii

1
INTRODUCTION
Atherosclerosis is a progressive inflammatory disease characterized by accumulation of
lipids, fibrous elements and inflammatory cells in large and middle-sized arteries. It is the
main cause cardiovascular (CAV) and important cause of cerebrovascular (CV) events
(1). Epidemiologically, ischemic heart disease and cerebral ischemia represent the main
cause of death and premature disability in developed countries (2). Moreover, due to the
aging of the population, the global burden of atherosclerosis, and thereby its clinical
consequences will continue to rise in the coming decades (3). The underlying
pathogenesis of atherosclerosis involves an imbalance between lipid metabolism and
maladaptive immune response and consequently chronic inflammation of the arterial wall
(4). Although several risk factors associated with arterial wall disease have been
identified, disease burden and ischemic events could not be predicted based on their
identification alone, thus leaving space for other methods (e.g. arterial imaging and
biomarkers) to be employed for better patients risk stratification. Advances in medical
and interventional treatment strategies have emphasized the importance of identifying
vulnerable patients, their risks and optimum treatment. Also, developments of different
imaging techniques have aided considerably in this aspect by making non-invasive
evaluation and quantification of atherosclerosis in-vivo possible, in particular ultrasound,
which is an established imaging modality in atherosclerosis research.
Pathophysiology of atherosclerosis
The term atherosclerosis is derived from the Greek "athero," meaning gruel, or wax, and
"sclerosis" for hardening (induration), with the former referring to the corresponding lipid
pool (necrotic core) and the latter referring to the fibrous cap of the plaque's luminal
edge. Arterial wall is composed of three layers: tunica intima, tunica media and
adventitia. The intima is the inner lining of the vessel, directly adjacent to blood flow, a
very dynamic layer which is composed of a monolayer of endothelial cells. The initial
step of the atherosclerosis pathology is the dysfunction of these endothelial cells that
allows the accumulation of low-density lipoprotein particles (LDL) into the intima.
Subsequently LDL particles undergo oxidative modifications that may trigger a local

2
inflammatory response that signals the following steps in the lesion formation. This is
followed by monocytes migration, accumulation into the intima and their conversion to
macrophages, which characterizes the initiation of early atherosclerotic lesion formation.
Upon occupying the intimal space, macrophages will uptake lipoprotein particles by
receptor mediated endocytosis and become lipid-laden foam cells. This stage of the
disease become macroscopically apparent as fatty streaks, that could be visible in the
large arteries even in the first decade of life, as confirmed by autopsy studies. (4, 5)
Although formation of fatty streaks commonly precedes the development of a more
advanced atherosclerotic plaque, not all of them will progress to atheroma formation.
Also, not all mechanisms involved in atherosclerosis process are “pro-atherogenic”, in
fact high-density lipoprotein (HDL) particles and M2-like phenotype macrophages have
“anti-atherogenic” properties (4). Based on the above, atherosclerotic plaque could follow
different ways: a) it could have stable progression (in most cases), b) it could have abrupt
progression that leads to plaque rupture with superimposed thrombosis or c) it could
regress, as shown in longitudinal follow-up imaging studies.
Lesion types
The pathogenesis of atherosclerotic lesions has been analyzed at different stages of
disease and in different age groups. There are many histological classification of
atherosclerotic lesions, however, we hereby present a simple one, which emphasizes the
link between morphology and clinical manifestations (6). In addition, this classification
could be properly related to plaque imaging during different stages of the disease. Figure
1, shows all plaque types presented on a graph together with corresponding ultrasound
images.
A. Adaptive intimal thickening: Characterized by smooth muscle cells accumulation
in a proteoglycan-rich matrix in the absence of lipids and inflammatory cells. This
may provide a soil for lesion development, initially at the branching points but
later could spread into adjacent parts.
B. Intimal xanthoma (“fatty streak”): Characterized by LDL accumulation into the
intima. Subsequently, LDL particles will modify and undergo process of

3
oxidation and start to act as chronic stimulator for immune response. They induce
endothelial cells to express adhesion molecules, which interact with receptors on
the surface of the monocytes and stimulate their adhesion and migration into the
intima. Macrophages could express several different phenotypes. Some of them
attain pro-inflammatory (M1-like phenotype), and the others that have an M2-like
phenotype may secret factors that favor resolution of the inflammation. These
types of lesions could be fully reversible if the stimuli that caused them dissipate.
They are present already in the aorta of some infants in the first 6 months,
probably reflecting risk factors of the mothers, then their number decline in the
subsequent years.
C. Pathological intimal thickening: Pathological intimal thickening is sometimes
refereed to in the literature as an “intermediate lesion.” True necrosis is not
apparent. The fibrous cap overlying the areas of lipid is rich in smooth muscle
cells and proteoglycans. Macrophages and lymphocytes may also be present, but
these are usually sparse.
D. Fibroatheroma: this corresponds to the formation of necrotic core. The foam
cells, macrophages and smooth muscle cells accumulated in the intima over time
could undergo apoptosis and secondary necrosis. The reason why necrosis
happens in some but not the other lesions is not known. At this stage of the
disease neovascularization and intraplaque hemorrhage are often present.
E. Fibrocalcific plaque: Calcification is common in progressive atherosclerosis and
its content increases with age. Plaque components that undergo calcification are:
apoptotic cells, extracellular matrix and necrotic core. Sometimes these structures
undergo complete calcification; so calcification may constitute most of the plaque
volume. The last two phases of the disease progression (D and E) can interchange
between each other under different internal and external factors, e.g. statin therapy
could increase fibrotic composition within the soft plaques and in high doses can
aggravate plaque calcification.

4
Figure 1. Stages of atherosclerosis development and ultrasound imaging samples.
In each box; top left- a cross sectional view of the carotid artery animation, top
right- more detailed animation focused at the more active disease process, bottom
right- ultrasound plaque features attempt to correlate with the plaque features
represented in the animations.
A-adaptive intimal thickening, that can be accurately measured by ultrasound; B-
Intimal xanthoma, there is an assumption, but it is not yet confirmed by direct
histological studies if an echolucent intima media complex (low IM-GSM)
represents the intimal xanthoma, characterized by accumulation of LDL and
inflammatory cell particles; C- Pathological intimal thickening (intermediate
lesion), early non-stenotic lesion on ultrasound; D-Fibroatheroma with typical
features vulnerable plaques, echolucent plaque with juxtaluminal black area on
US; E-Fibrocalcific plaque.

5
Pathomechanism of ischemic events
The most dramatic complication of atherosclerotic plaque progression is thrombosis,
which may be caused by three different mechanisms: a) plaque rupture, b) plaque erosion
or c) calcified nodule (7). The first and most common one is plaque rupture, which is
defined as a fibrous cap disruption when the overlying blood contents are in continuity
with the underlying necrotic core. Plaque erosion is identified when the thrombus is
superimposed on a plaque substrate primarily composed of smooth muscle cells and
proteoglycans, and without a communication between blood contents and the necrotic
core. Calcified nodules are characterized by protrusion of the eruptive dense calcified
bodies into the luminal space and represent the least frequent morphology associated with
luminal thrombosis (8). Following plaque rupture, the pathomechanisms by which the
disease is caused differs in different arterial systems. While in coronary arteries
myocardial infarction (MI) is attributed to in-situ thrombosis, in carotid artery
embolization is the most common mechanism causing ischemic stroke (1) (figure 2).
Figure 2. Stable and unstable plaque features. Pathomechanisms of ischemic events in
coronary and carotid artery
LUMEN
STABLE PLAQUE
UNSTABLEPLAQUE
Thin fibrous capLarge lipid pool
Neovascularization
Inflammatory cells
Neovascularization
LUMEN
In-situ thrombosis
Artery-to-artery embolization
Plaquerupture
Plaque thrombosisin coronary artery
Embolization aftercarotid plaque rupture
Thin fibrous cap

6
Risk factors
There are multiple factors that contribute to atherosclerotic plaque progression. As
described above, the processes involved in atherosclerosis include: endothelial cell injury,
lipid metabolism, inflammation, and smooth muscle cell proliferation. Factors affecting
these processes may inhibit or accelerate atherosclerosis. In general atherosclerosis risk
factors are divided into two groups: non-modifiable (family history, male gender) and
modifiable (hyperlipidemia, diabetes mellitus, cigarette smoking, hypertension, and
dietary deficiencies of antioxidants) (1).
Epidemiology
Atherosclerosis-related cardiovascular (CAV) and cerebrovascular (CV) events are the
most common causes of deaths in the West (2). The prevalence of atherosclerosis in
carotid and coronary arteries increases exponentially with age, and is more prevalent in
men than in women. According to the World Health Organization, 15 million people
suffer stroke annually worldwide and of them 5 million die. In Europe alone nearly
650.000 stroke deaths occur per year (9). Approximately 85% of strokes are ischemic and
15-20% of them are attributed to carotid artery disease (10).
CAROTID ARTERY STENOSIS
Carotid artery stenosis is an important cause of ischemic stroke (11). Atherosclerosis
could affect any segment of the carotid artery with a predilection at the point when it
bifurcates into internal and external artery. The arterial wall is normally highly dynamic
because its pulsations follow those caused by the cyclic heart contraction and relaxation.
Arterial expansion alters artery radius, shape and curvature, which together interact to
make the blood flow in the arteries (e.g. common carotid artery) laminar. Laminar blood
flow is characterized by concentric layers of blood moving in parallel down the length of
a blood vessel with the highest velocity in the center of the lumen. When blood separates
at an arterial bifurcation, a complex pattern of fluid velocities is created. The highest

7
velocities at the center of flow come in contact with the flow divider, and this flow
separation continues until some distance into the subsequent branches (figure 3). These
regions have a low wall shear stress that contributes to alterations of endothelial cells, by
inducing expression of endothelial leukocyte adhesion molecules that contribute to
leukocyte migration into the intima and hence the development of atherosclerosis (12).
Figure 3. Hemodynamics at the carotid artery bifurcation
Who is at risk?
Moderate to severe asymptomatic carotid stenosis is found in 2-5% of women and 2-8%
of men over the age of 60 years. However the risk is much higher in high-risk groups.
The prevalence of asymptomatic 50-90% carotid stenosis in patients over 60 years with
three CAV risk factors is estimated at 16%, and in those with concomitant coronary
artery disease and contralateral carotid disease is 15% and 6%, respectively. The
Framingham study showed that predictors of carotid stenosis over 12 years are (13):
8
Ø Age (odds ratio (OR) 1.6-1.7/10 year increase in age)
Ø Smoking (OR 1.3-1.5 per 10 cigarettes smoked/day)
Ø Systolic blood pressure (OR 1.2 per 10 mmHg increase)
Ø Total cholesterol (OR 1.1-1.2 per 0.5 mmol/L increase).
Clinical identification of carotid artery stenosis used to be based on auscultation skills
and the confirmation of a bruit. This clinical sign has recently been proven to be of low
accuracy in depicting 70-99% stenosis with a sensitivity of 57% and specificity of 70%
(14). This low accuracy of auscultation highlighted a need for other accurate imaging
screening modalities such as ultrasound. In addition, detection of calcification on
panorama radiograph or cone beam CT (CBCT), during patients’ evaluation for dental
procedures, has been found to be associated with significant carotid stenosis (15).
Recommending these patients for carotid US examination has made possible the
identification of those with significant stenosis and implementation of different treatment
strategies for stroke prevention.
Degree of Carotid stenosis assessment
The degree of carotid artery stenosis could be evaluated by different imaging techniques,
however the gold standard against which other methods accuracy is evaluated is
conventional angiography (16). Using angiography, the degree of stenosis could be
quantified by two methods: one suggested by North American Symptomatic Carotid
Endarterectomy Trial (NASCET) (17) and the other by European Carotid Surgery Trial
(ECST) (18). Both methods evaluate the degree of stenosis as the percentage reduction in
the linear diameter of the carotid artery. Because these two trials have used different
strategies to quantify the degree of stenosis, applying both of them in the same carotid
artery will demonstrate different values (e.g. 82% ECST usually corresponds to 70%
NASCET stenosis) (19). This difference between the trials degree of estimated stenosis
can be corrected using the formula: NASCET=(ESCET-40)/0.6 (20). Because
angiography is an invasive investigation and is also associated with 0.3-1% risk of peri-
procedural neurological events, a growing interest for other non-invasive modalities that
could accurately evaluate the degree of stenosis and identify other plaque features that

9
could be of importance for patients risk stratification has been developed (21). A meta-
analysis conducted by Koelemay et al. (22) reported a sensitivity of 97% and specificity
of 99% for CTA in characterizing the degree of carotid artery stenosis. In particular, CTA
was accurate for assessing 70-99% stenosis and for excluding total artery occlusions.
Carotid duplex ultrasound (US) has been shown to be accurately comparable with digital
subtraction angiography (DSA) and today it is the most widely used method for
evaluating carotid stenosis. Carotid US has the benefits of speed, safety, bedside and its
radiation free properties. Stenosis is measured using Doppler principles of blood velocity
at the tightest stenosis point, which could be translated to equivalent DSA measurements.
One of the methods recommended for grading stenosis is to use peak systolic velocity. A
velocity more than 125 cm/s corresponds to >50% stenosis and a velocity >230 mm/s
corresponds to greater than 70% stenosis (23).
A meta-analysis of individual patients data showed an inter-observer variability
agreement, for ultrasound, for 70-99% degree of stenosis of 86% (79%-91%) (24). In
clinical practice, an additional confirmatory investigation to ultrasound has been
recommended before carotid endartercomy (CEA); including another imaging modality
(CTA) or a repeat ultrasound examination (10). However, there are data that suggests that
ultrasound-only strategy is as effective as adding one more modality in patients with 70-
99% stenosis selected for surgical intervention within 14 days. Assessing moderate
symptomatic carotid stenosis by ultrasound has been shown to be less accurate (25). Also
the accuracy is limited in cases with moderate contralateral stenosis or occlusion as well
as in arteries with extensive calcification. In borderline cases, adding another modality,
CTA or contrast enhanced magnetic resonance angiography (MRA) can reduce
unnecessary CEA performed (26). It has been shown that symptomatic patients with
>70% stenosis benefit from CEA and is therefore very important to measure accurately
the degree of stenosis. However, it was later demonstrated that the risk of embolism and
thrombosis is not related only to the stenosis severity but also with its composition and
other plaque features.

10
Carotid artery plaque features: the concept of plaque vulnerability
Based on several morphological and histological characteristics, carotid plaques could be
defined as stable and unstable. In general, plaques that have been associated with
increased risk of ischemic events are defined as unstable or vulnerable. Vulnerable
plaques are characterized by the presence of a thin fibroatheromatous cap that overlies a
large lipid pool (>40% of the plaque), large necrotic core, intimal spotty calcification,
high inflammatory cell concentration, neovascularization and intraplaque hemorrhage.
While historically plaque features are evaluated histologically in autopsy studies or in the
arterial segments removed after surgical procedures, advances in imaging techniques
have made in vivo plaque visualization and identification of different components inside
the plaque possible.
Imaging plaque features
A number of non-invasive imaging modalities exist for reliably determining carotid
artery plaque features, including: ultrasound, magnetic resonance, computed tomography,
and positron emission tomography (PET) (16). Because studies included in this thesis are
mainly based on ultrasound technology, this section will be mostly focused on ultrasound
characterization of carotid plaque features, and also its strength and weakness will be
weighted against other non-invasive imaging modalities.
Surface plaque morphology
The surface morphology of the carotid plaques classified as smooth, mildly/markedly
irregular and ulcerated, is an important determinant of vascular events. A smooth surface
configuration is characterized by a regular luminal morphology which indicates a stable
plaque. Irregular surface morphology, especially marked irregularity has been shown to
be associated with increased risk of ischemic events (27). The third type of surface
morphology –ulceration, is significantly associated with increased risk of cerebral events,
and this was demonstrated in NASCET study (28). Of the different imaging techniques
that have been used to assess surface plaque morphology, computed tomography

11
angiography (CTA) has the greatest accuracy. Compared to ultrasound, CTA sensitivity
in detecting plaque ulceration has been shown the highest (93% vs. 37.5%) (29). Such
sensitivity of US for identification of ulceration is higher (77%) in plaques causing >50%
stenosis (27). Recently introduced ultrasound based techniques such as: contrast
enhanced US (CEUS) and ultrasound 3D reconstructions have been shown to have very
high accuracy for detecting ulceration (30, 31).
Plaque composition
As mentioned before, carotid plaques are composed of different components and the
relative proportion of these components can vary from one plaque to another, which
could determine its stability. Histologically, different plaque components have been
described and their association with ischemic events was determined. Carotid plaque
components most commonly found in patients with stroke and transient ischemic attack
(TIA) are: lipid pool, necrotic core and hemorrhage. The presence of calcium seems to
have a protective role, since it is found mostly in asymptomatic plaques. Because of the
clinical importance identifying such plaque features in vivo, many imaging modalities
have been employed (32, 33). Ultrasound as well as computed tomography (CT) and
magnetic resonance imaging (MRI) offer important information about carotid plaque
composition. On CT carotid plaques are classified based on the Hounsfield Units (HU)
density as fatty (<60 HU), mixed (60-130 HU) and calcified (>130 HU) (34). Very low
values (<0 HU) have been found to be associated with hemorrhage. Also MRI can depict
carotid plaque composition, especially plaque hemorrhage (35, 36).
On ultrasound, plaque echogenicity is the main parameter that reflects composition.
Plaque echogenicity has traditionally been evaluated by visual (subjective) grading
plaques echo reflection (e.g. echogenicity and echolucency), and its echo pattern
(heterogenous and homogenous). However, visual evaluation of plaque echogenicity has
some limitations because it is subjective and also plaque echogenicity could be affected
by ultrasound machine settings during the patients’ examination. Nevertheless, this
limitation could be overcome by computer assisted plaque normalization using image
processing and 2 references (blood and adventitia). The blood is scaled to zero, while the
brightest area of the adventitia is normalized to a grey scale of 190. Following

12
normalization, the plaque is outlined and its overall brightness evaluated by means of
grey scale median-GSM (grey scale range: 0-to-255; 0=black and 255= white). The lower
the GSM the more echolucent is the plaque. Conversely, echogenic plaques will have
higher GSM. However, because different studies have used different cut-off values to
define plaque echolucency, its use in clinical practice could not be suggested yet. In
addition to GSM evaluation, plaques could be objectively classified into four groups
based on Gray-Weal classification modified by Geroulakos (37):
Type 1: uniformly echolucent with <15% of the pixels in the plaque area being occupied
by pixel values >25;
Type 2: mainly echolucent where pixels with grey scale values >25 that occupy 15-50%
of the plaque;
Type 3: mainly echogenic with pixels >25 occupying 50-85% of the plaque;
Type 4: uniformly echogenic with grey scale >25, occupying >85% of the plaque.
Studies correlating US findings with plaque histology have revealed that echolucent
plaques are associated with lipids, necrotic core or intraplaque hemorrhage, while
echogenic plaques are associated with fibrous and calcified tissue. In addition to GSM
and plaque types there were other parameters developed such as: Juxtaluminal black area,
plaque coarseness and entropy.
Juxtaluminal black area (JBA) of the plaque is defined as the area of the plaque
components having grey-scale <25 without a visible echogenic cap. After imaging
normalization this area is outlined and expressed as mm2 (38). JBA <8 mm2 has been
shown to be associated with a 0.6 annual risk of stroke compared to 4.6% in patients with
JBA >8 mm2 (39).
Thin cap fibroatheroma
Histologically, fibrous cap is formed of smooth muscle cells relied within a collagen-
proteoglycan matrix, associated with macrophages and T lymphocytes (40). A thin
fibrous cap plays a critical role in determining plaque vulnerability. Following fibrous
cap rupture, the exposure of thrombogenic plaque components to the luminal blood flow

13
represents a critical step that eventually leads to thromboembolic complications. The best
non-invasive imaging modality to assess the status of the fibrous cap in carotid arteries is
MRI, which could define the fibrous cap as normal, thin or fissured/ruptured (41).
Currently, there are no imaging studies that have used ultrasonography to assess fibrous
cap, and CT proved not accurate for this purpose.
Neovascularization and intraplaque hemorrhage
Adventitia of the normal middle and large size arteries has a vasculature network (vasa
vasorum) that supplies the outermost part of the artery with oxygen and nutrition, while
the intima part is supplied with oxygen from the lumen through diffusion. In pathological
conditions (atherosclerosis), because the oxygen cannot achieve the deeper parts of the
plaque, some small vessels will proliferate from the adventitia towards the intima as
neovessels. The wall of these vessels lack pericytes and is very fragile and hence is prone
to rupture. It has been suggested that rupture of the neovessels is the cause of production
and expansion of intraplaque hemorrhage (IPH) (42). The presence of neovascularization
and/or intraplaque hemorrhage is considered a feature of vulnerability (43). The best
modality for visualizing IPH in the carotid arteries is magnetic resonance, which can
recognize the age of the hemorrhage as well (35). Using ultrasound, neovascularization
can be evaluated using microbubles based contrast, known as contrast enhanced
ultrasound (CEUS) (42). A recent study by Staub et al. concluded that the presence of
neovascularization inside the carotid plaque is associated with morphological features of
plaque instability (44).
Arterial Calcification
Calcium formation may be found in any arterial bed as well as in the microvessels. It may
be present in the intima and/or media, the latter being common in chronic kidney disease
or type II diabetes (16). The initial plaque calcification is associated with apoptotic
smooth muscle cell and appears as micro-calcifications bound to membrane vesicles.
Following plaque progression, the micro-calcifications combine together to form larger
calcium deposits. In patients with carotid atherosclerosis calcification is detected in 50-

14
60% of cases (45) and even often in significantly stenotic lesions (>50%) (15) but its
association with CV events is uncertain. Controversies exist as to the effect of
calcification on plaque nature with some evidence suggesting more stability (45) and
another indicating vulnerability, irrespective of the degree of stenosis (46). A systematic
review has shown that symptomatic plaques have less calcification than asymptomatic
ones (47). However, studies included in this review used wide range of methods to
quantify carotid calcification, highlighting the need for a well-validated, accurate and
reproducible technique for calcium quantification in patients with carotid atherosclerosis.
Plaque calcification in carotid arteries can be assessed by a number of imaging modalities
including: CT, ultrasound and MRI. While ultrasound may detect the presence of
calcification, it does not have the accurate means for quantifying its extent. Computed
tomography on the other hand has the ability to identify and quantify calcification. Even
calcification volumes of 1 mm3 can be detected and quantified by cone beam CT
(CBCT). Furthermore, it has been shown that the amount of calcification quantified by
carotid CT correlated with respective histology sections (48). Despite, such uncertainty
the extent of carotid calcification adds more accurate assessment to the plaque features.
Carotid US is an easy and economically favorable method to study different plaque
features and their potential association with symptoms. It has been reported that extensive
calcified carotid plaques are associated with adverse outcome 30 days after carotid artery
stenting (CAS), hence CEA should be recommended in such cases (49). Because many
centers today rely mainly on carotid US information before intervention, identification of
calcification and its severity seems to be important.
ASYMPTOMATIC CAROTID STENOSIS
Asymptomatic carotid stenosis refers to narrowing of the carotid artery caused by
atherosclerosis in patients who have not experienced a stroke or transient ischemic attack
in the brain related to cerebral circulation insufficiency. With the introduction of vascular
ultrasound in 1980s, investigation of carotid artery disease became easy, and on the
following years a high number of patients were diagnosed with a so-called asymptomatic
15
carotid disease. However, the prognosis and management of such patients remains
uncertain. Both natural history studies, as well as several large randomized trials showed
a low incidence of stroke in asymptomatic patients with carotid disease, only 1-2% per
year and a rather high incidence of cardiovascular morbidity and mortality (5-10% per
year) (50, 51).
Management of asymptomatic patients with carotid stenosis
The Asymptomatic Carotid Atherosclerosis Study (ACAS) (52) and the Asymptomatic
Carotid Surgery Trial (ACST) (53) provided evidence that CEA offers a 50% risk
reduction for ipsilateral stroke in patients with moderate to severe asymptomatic carotid
artery stenosis compared to medical treatment alone (annual stroke risk: 1% vs. 2%).
However, at the time when these trials were performed, patients had received a treatment
that today would be considered as suboptimal medical treatment, e.g. in the ACST statins
were used in only <10% of patients, while 20% of population was not taking antiplatelet
therapy. Furthermore, dietary modification, blood pressure control and statin dosage were
not close to those that are currently used in practice.
It has been suggested that up to 94% of CEA performed on the basis of these trials
recommendations are unnecessary. As compared to CEA for symptomatic stenosis, with
a number needed to treat (NNT) of 6 (or 3 for patients above 75 years old), to prevent a
stroke in asymptomatic patients the NNT were 83 (54). The advancement of the best
medical treatment (BMT) has questioned the invasive intervention (CEA or CAS) for
asymptomatic patients. Recently, a low risk of ipsilateral stroke in patients with
asymptomatic carotid stenosis has shown range from 0.4 to 1.0% per year (55).
Nevertheless, for a subgroup of patients at higher risk of stroke, invasive intervention
may still be justified. Identification of such high-risk patients who could benefit from
invasive intervention in addition to BMT is thus of crucial importance.
Identifying high-risk patients with asymptomatic carotid disease
In the past three years, it has become increasingly clear that BMT is the best choice for
the majority of patients with asymptomatic carotid disease, and there has been an
16
increasing effort in identifying factors that could stratify patients who may benefit of
intervention therapy (56). Many clinical and imaging features have been reported that are
associated with increased risk of stroke, and some of them will be described in the
following sections.
Bilateral carotid disease
Patients with bilateral carotid disease are at higher risk from suffering CV symptoms. In
asymptomatic carotid stenosis, it has been reported that patients with a history of
contralateral TIA/stroke were associated with a 3.4% annual risk of stroke compared to
1.2% in those with no previous symptoms (57). It has also been concluded that medically
treated patients with a history of contralateral symptoms prior to randomization were
significantly more likely to develop CV symptoms within 5 years follow-up in the
territory ipsilateral to asymptomatic stenosis compared to those without a history of
contralateral symptoms, 29% vs. 22%, respectively (58). In addition, patients with
bilateral carotid disease “vulnerable” textural features were confirmed in carotid plaques
of both sides compared to more stable features in patients with unilateral disease (59).
“Silent” brain infarction
About 20% of asymptomatic patients with carotid stenosis will have the evidence of
silent infarction on CT/MRI scans. Patients with ipsilateral “silent” infarction have been
shown to have a significantly higher annual risk of ipsilateral stroke compared to those
without, 3.6% vs. 1.0%, respectively (60). The same was confirmed in an ACST
subgroup analysis. Compared to patients with no evidence of brain infarction or prior
symptoms, those with ipsilateral infarction or a history of prior CV symptoms had a 5.8%
absolute risk increase for stroke in the subsequent 10 years (61).
Multisite atherosclerosis disease
Reduction of Atherosclerosis for Continued Health (REACH) (62) study analyzing
prospectively a cohort of 68,236 patients showed that after one year follow-up the rate of

17
vascular events is increased with the number of symptomatic diseased locations, ranging
from 5.31% in asymptomatic patients to 12.58%, 21.41% and 26.27% in patients with 1,
2 and 3 symptomatic arterial disease locations, respectively. Based on these results it
seems that the presence of multi-focal atherosclerosis disease has major clinical and
prognostic impact. However, the pathomechanism behind widespread atherosclerosis at
the level of distinct territories is complex; multiple risk factors, genetic, inflammatory
markers and loco-regional hemodynamics, all may play an important role (63, 64). The
impact of different risk factors on the disease prevalence in various locations is important
in predicting the affected arterial system: smoking is three times more likely to cause
lower extremity artery disease than coronary artery disease, compared to diabetes in
coronary artery disease and hypertension in carotid atherosclerosis (1, 65).
Ultrasound markers of plaque vulnerability
Degree of stenosis: There is conflicting evidence with regards to any relationship
between stenosis severity and future ischemic events. Subgroup analyses from the ECST
and NASCET showed that stenosis severity (but not near occlusion) was associated with
increased risk of stroke in medically treated patients. Also, the Asymptomatic Carotid
Stenosis and Risk of Stroke (ACSRS) study (57) has reported that the risk of stroke is
proportionally increased with the increase in the degree of stenosis from 0.8% to 1.4%
and 2.4%, for 50-69% to 70-89% and 90-99% stenosis, respectively. On the other hand,
neither ACAS (52) nor ACST (61) found any evidence that increasing stenosis severity is
a predictive of increased risk of stroke in the medically treated asymptomatic patients.
Stenosis progression: It has been assumed that progression of the stenosis severity as
shown with US could be associated with increased risk of stroke. Sabeti et al. (66)
showed that stenosis progression was associated with two-fold increase of stroke risk in
the 3-year follow-up period (OR 2.0; 95% CI 1.02-4.11). The ACSRS study (57) in a
subgroup analysis on this issue showed that at follow up stenosis severity remained
unchanged in 76%, regression was observed in 4% and stenosis progression in 20% of
patients. The 8-year cumulative risk of ipsilateral stroke was 0% for patients with US
evidence of stenosis regression, 9% in the group of patients with unchanged stenosis and

18
16% in patients with stenosis progression. Despite suggestions that stenosis progression
was associated with doubling rate of stroke per annum, 68% of the ischemic strokes
occurring during the follow-up affected patients with no evidence of stenosis progression,
thus indicating a low accuracy of the method for identifying high-risk patients.
Textural plaque features: As stated above, there are many ultrasound-derived textural
features that could be considered as a sign of plaque vulnerability. Soft (echolucent)
carotid plaques today could be evaluated using different cut-offs of GSM values (low
GSM=echolucent plaque) or by classifying plaques into plaque types (PT) as
recommended by Gray-Weale and Geroulakos (PT 1 and 2=echolucent plaque). In the
ACSRS study, asymptomatic patients with a GSM >30 had a very low annual rate of
stroke (0.6%), the annual stroke rate increased to 1.6% for those with a GSM of 15-30
and to 3.6% for those with GSM <15. The annual rate of stroke was progressively
increased when comparing plaque Types from 4 to 1, with Type 4 having a 0.4% annual
risk of stroke, compared to 0.8% and 3.0% for Type 3 and Type 1 or 2. Most studies that
used this classification to determine patients’ symptoms have defined plaques Type 1 and
2 as echolucent and plaque Types 3 and 4 as echogenic.
Microembolic signals detection by transcranial Doppler
Microembolic signal (MES) detection by transcranial Doppler (TCD) is another
important imaging modality that was used to identify patients at increased risk of stroke;
accordingly, consensus criteria have been established for interpreting these highintensity
transient signals (67). Several studies evaluated the predictive role of MES detected by
TCD ultrasonography in patients with asymptomatic stenosis. Asymptomatic Carotid
Emboli Study (ACES) showed that the presence of spontaneous embolization was
associated with a five-fold increase in the risk of ipsilateral stroke (68). In 2005, Spence
et al. (69) showed that asymptomatic carotid stenosis patients who had two or more
microemboli during an hour of monitoring had a 1-year stroke risk of 15.6% compared to
only 1% risk of stroke for patients with no microemboli. Furthermore, it was
demonstrated that an aggressive approach to medical therapy has significantly reduced
MES on TCD ultrasonography (70).

19
Figure 4. Proposed algorithm for the management of patients with asymptomatic carotid
stenosis, relied on clinical data and data acquired by ultrasound imaging. BMT - Best
Medical Treatment, CEA - Carotid Endarterectomy, CAS-Carotid Artery Stenting. Note:
To decide between CAS and CEA other clinical and imaging features acquired by
modalities other than US should be taken into consideration, e.g. intracranial extension
of carotid plaque, patients with previous irradiation of the cervical region, carotid artery
tortuosity, etc.
SYMPTOMATIC CAROTID STENOSIS
First descriptions of carotid stenosis related to cerebral ischemic events date back to T.
Willis (1621-1675) and J. Wepfer (1620-1695) (71). Symptomatic carotid stenosis is
defined as carotid artery disease associated with ischemic symptoms (Stroke, TIA or
amaurosis fugax) in the anterior brain circulation. After ischemic events, the presence of
carotid artery stenosis is confirmed during an US, CTA, MRA or conventional
Asymptomatic carotid stenosis
<60% stenosis
60-99%stenosis
BMT
One of the below:(1) Echolucent plaque (PT I or II),
(2) >2 MES on transcranial Doppler(3) markedly irregular/ulcerated
plaques
CEA + BMT CEA or CAS + BMT
One of the below:(1) >70 years old patient
(2) Echolucent plaque(3) Extensive calcification
Yes No
YesNo

20
angiography examination. During the US examination the degree of stenosis is measured
together with the description of exact plaque location and plaque morphology. After
confirmation of the carotid disease in most cases, unless contraindicated, patients will be
recommended carotid endarterectomy (CEA) intervention. CEA consists removal of the
carotid atheroma together with intima and media layers, leaving the adventitia
unattached.
Management of symptomatic patients with carotid disease
In patients with acute CV accidents associated with carotid stenosis the initial therapy
comprises antiplatelet, statins and risk factors management (72). In patients with carotid
stenosis an intervention should be performed within <2 weeks. Benefit of
revascularization is greater in men, in older patients, and in severe stenosis (70-99%)
(72). In addition, a subgroup of patients with moderate carotid stenosis (50-69%) might
also benefit of revascularization, particularly those with moderate carotid plaque
irregularities, ulceration and echolucency that are confirmed to be at higher risk for stroke
recurrence (73). In addition, it was recently shown that the incidence of stroke recurrence
is very high in the first 72 hours after initial symptoms and an emergency CEA
intervention would be of benefit in this subgroup of patients.
Medical therapy
Medical therapy of stroke or TIA related to a carotid stenosis consists of immediate
administration of secondary prevention with antiplatelet therapy. Either dipyridamole
plus aspirin (74), ���clopidogrel alone (75), or aspirin alone is recommended (76, 77). In
symptomatic patients with >50% carotid stenosis associated with microembolic signals
administration of dual antiplatelet therapy (aspirin + clopidogrel) resulted in decreased
risk of stroke recurrence (78). The Clopidogrel in High-risk patients with Acute Non-
disabling Cerebrovascular Events (CHANCE) trial showed that the combined treatment
of clopidogrel and aspirin for the first 21 days after TIA or stroke, followed by
clopidogrel alone decreases the 90-day risk of stroke [hazard ratio, 0.68, 95% (CI, 0.57–

21
0.81), p<0.001], without increasing the risk of hemorrhage in comparison with aspirin
alone (79).
In addition to antiplatelet therapy, statins have been found to be highly effective in stroke
prevention among medically managed patients with CAV disease (71). In a meta-analysis
the stabilizing effect of statin therapy on carotid plaque has been confirmed, and has been
proposed to be related to the non-cholesterol-lowering, so-called pleiotropic effects of
statins (80). Several studies have also demonstrated an independent benefit from statins
on outcomes before carotid endarterectomy (81). A three-fold reduction in the rate of
perioperative stroke, and five-fold reduction of perioperative mortality among 1,566
statin-treated patients undergoing carotid endarterectomy, has been shown (82). Stroke
Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial has confirmed
that in patients with recent stroke or TIA, 80 mg of atorvastatin daily reduced the overall
incidence of strokes and of CAV events, despite a small increase in the incidence of
hemorrhagic stroke (83).
Interventional therapy
It was not before 1950s when DeBakey and Estcot for the first time tried surgical
intervention in the carotid stenosis for secondary stroke prevention. Later on, several
large randomized studies demonstrated that CEA is associated with better clinical
outcome after ischemic stroke. Indeed, the results of ECST and NASCET trials showed
primarily that compared to medical treatment, CEA reduced the risk of stroke at 5 years
of 15% among patients with a 70–99% and of 7.8% among those with a 50–69% stenosis.
No benefit could be demonstrated in patients with 0-49% stenosis (17, 18). Also, surgery
conferred no benefit in patients with “near-occlusion”, defined as a 90-95% stenosis
when the distal internal carotid artery (ICA) lumen is collapsed, as shown on angiography
(84). In a pooled analysis including ECST and NASCET trials data, a higher benefit from
surgery in men has been reported (85). While CEA was clearly beneficial in women with
>70% symptomatic carotid stenosis, this was not the case for those with 50–69% stenosis
(85). Furthermore, women had a lower risk of ipsilateral ischemic stroke on medical
treatment than men. This observation is possibly a reflection of the differences in the
pathology of the atherosclerotic plaques, with men having unstable carotid plaques with

22
more pronounced features of inflammation compared to women (86). Because most of
the recurrences occur early after stroke, it was confirmed that earlier interventions are
associated with lower rate of adverse outcomes (87). In addition to CEA, carotid artery
stenting (CAS) is another optional treatment for patients with carotid artery disease.
Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST) (88), showed
that CEA and CAS can be performed with a procedural risk of <3% by carefully
credentialed surgeons and interventionists. However, it was demonstrated that CAS is
associated with inferior outcomes compared with CEA for patients with symptomatic
carotid disease (89). CAS was associated with higher rate of stroke, recurrent carotid
stenosis and considerably higher cost compared with CEA (89). For the present, CAS is
generally indicated for small proportion of symptomatic patients, those with: distal
lesions where CEA is more difficult to perform; scarred or infected neck; recurrent
stenosis following CEA; possibly contralateral internal carotid occlusion (90). However,
improvements in CAS technical skill and technology (membrane covered stents, newer
protection strategies) and better patient’s selection may alter this situation in the future.
One example is the use of the flow-reversal or flow-cessation embolic protection. A
meta-analysis of 4747 patients in 24 CAS studies found a significant benefit from
protected distal procedures with a relative risk reduction of 0.59 (95% CI, 0.47–0.73)
(91). Another important strategy is the avoidance of CAS in patients with echolucent
carotid disease or extensive calcification and in patients aged >70 who were shown to
have worse results with CAS (92). Several studies have confirmed that echolucent
plaques are associated with higher rates of emboli signals and in-stent restenosis
compared to echogenic plaques. There are controversial data according to CAS
interventions on echolucent plaques and recurrent symptoms. On the basis of this, we
undertook a systematic search on PubMed for studies evaluating associations between
carotid plaque echolucency and adverse outcomes (stroke, microembolization and in stent
restenosis). Out of 412 studies found after the first medical databases search, we
identified five studies appropriate to be qualitatively and quantitatively analyzed, which
evaluated different adverse outcomes in patients with echolucent plaques after CAS.
Pooled analysis showed that CAS in echolucent carotid plaques is associated with higher
risk of stroke (OR 2.33; 95% CI 1.73-4.65, p=0.015), microembolization (OR 2.77; 95%
CI 1.40-5.45, p=0.003), and in stent restenosis (OR 3.8; 95% CI 1.93-7.44, p<0.001).

23
In general, pooled OR of adverse outcomes for CAS performed in echolucent compared
to echogenic plaques was 2.92 (95% CI 1.97-4.32), p<0.001 (92-96).
Identifying patients at high risk for stroke recurrence
An analysis of pooled data of randomized clinical trials showed that the risk of stroke
recurrence is 21% at five years after symptoms (20). However, the risk of stroke in the
early period after onset of symptoms seems to be much higher than it was previously
thought, with contemporary natural history studies suggesting that within 72 hours of the
presenting symptom 8-15% of patients with a 50-99% stenosis may suffer a recurrent
stroke (97, 98). Accordingly, it would be of clinical benefit to identify this subgroup of
patients at increased risk and to deliver interventions as soon as possible (emergency
CEA) after onset of symptoms, accepting that benefit must always be balanced against
the potential for perioperative stroke.
ABCD2 (99) and ABCD2-I scoring system (100) that integrate clinical and brain imaging
data has been shown to have predictive value for symptom recurrences after TIA. In
addition, there are several imaging carotid plaque features that could also assist in
identifying high risk patients, more frequently associated with stroke recurrence
including: stenosis severity, plaque irregularity and ulceration and plaque echolucency
and the presence of contralateral occlusion. Even though, significant benefit of CEA
procedures was determined for 50-99% stenosis degree, a meta-analysis including more
than 6000 patients randomized in ECST, NASCET, and the Veteran’s Affairs (VA)
Study, revealed that for 1000 CEAs intervention only 78 strokes would be prevented at 5
years in patients with 50-69% stenosis, compared with 156 strokes prevented at 5 years in
patients with 70-99% stenosis (20). Plaque irregularity was associated with significantly
higher rates of ipsilateral stroke in patients randomized to BMT, compared with smooth
stenosis. In patients with smooth carotid plaques, CEA prevented about 100 strokes/1000
interventions at 5 years compared to 200 strokes/1000 CEAs at 5 years in patients with an
irregular plaque producing 75% stenosis (20, 28). Salem et al. reported that the presence
of plaques with GSM <25 were predictive of a significantly increased risk of recurrent
neurological events in the early period, prior to CEA (101). Furthermore, the presence of

24
contralateral occlusion is associated with a significant increase in the risk of late stroke
ipsilateral to the treated ICA stenosis in medically treated patients (85). In a recent
systematic review, it has been found that MES were highly predictive of stroke
recurrence in patients with carotid stenosis having an OR of 9.57; (95% CI, 1.54–59.38)
(102).
Figure 5. Proposed algorithm for the management of symptomatic patients with carotid
stenosis; BMT - best medical treatment, DUS - Duplex ultrasound, CEA - carotid
endarterectomy, CAS - carotid artery stenting.
Ultrasound imaging markers of vascular risk: subclinical atherosclerosis
Many large studies have confirmed the predictive value of carotid intima-media thickness
(IMT) for cardiovascular risk. On 2010 American Heart Association/American College
of Cardiology guidelines designated carotid IMT a class IIa recommendation for
Symptomatic carotid stenosis
0-49% stenosis
70-99%stenosis
BMT and regular DUS
Control
One of the below:(1) Echolucent plaque,
(2) >2 MES on transcranial Doppler(3) markedly irregular/ulcerated
plaques
Consider CEA + BMT
Consider CEA or CAS + BMT
One of the below:(1) >70 years old patient
(2) Echolucent plaque(3) Extensive calcification
Yes No
YesNo
50-69% stenosis

25
cardiovascular risk assessment in asymptomatic adults with intermediate risk of
cardiovascular disease (103). However, a careful evaluation of carotid IMT studies
recently together with quantitative assessment of their results revealed discrepancies in
methods with which IMT was assessed and suggested that IMT measurement in common
carotid artery (CCA) have only a minimal predictive power beyond traditional risk
factors, with no clinical importance (104, 105). Carotid plaque assessment appears to be a
better predictor of CAV and CV risk compared to IMT alone (106). In addition,
quantitative assessment of plaques such as plaque thickness, echogenicity, area, and
volume appears to be progressively more sensitive in predicting CV risk than assessment
of plaque presence alone (106). Recently, a new measure of carotid artery wall - intima-
media grey scale median (IM-GSM), that attempt to quantify the echogenicity of the
intima-media complex seems to have a better predictive value compared to IMT (107).
Carotid artery wall measurements: intima-media thickness and intima-media GSM
Carotid IMT is measured between intima-lumen interfaces and media-adventitia
interfaces of the arterial wall represented as a double-line density on carotid ultrasound
image (figure 6). Its accuracy for the measurement of far wall IMT in common carotid
artery was validated against histological specimens representing the true biological
thickness of the vessel wall (108). Otherwise, near-all assessment of IMT was associated
with systematic measurement error, because of the echogenicity of the adventitia layer,
the boundary between media and adventitia in the near wall, is not easy to be defined
(109). The differences of the IMT values between 25th and 75th percentile are very small
(<1mm) and therefore, for the measurement of IMT a high precision is required,
including, proper training of the sonographers and implementation of protocols for the
measurement of IMT. In general, IMT measurement has been shown to have a good intra
and interobserver correlation coefficient of >0.90. Furthermore, advances of US
technology have made possible automatic measurement of IMT, obviating the need to
perform manual measurements, and this have improved the reproducibility of the
measurements (110). These systems for IMT measurements incorporate IMT datasets
from large clinical studies that allow generation of carotid IMT percentile values for
individual patients (111).

26
Figure 6. A. Intima-media thickness (IMT) measured in common carotid artery (CCA). B.
Intima-media and adventitia differentiation on US images and C. Relevant histological
structure of carotid artery wall. 1 - Lumen-intima interface, 2 - media-adventitia
interface. (a) tunica-intima, (b) tunica media, (c) adventitia. Internal elastic membrane
separates intima from media and external elastic membrane separates media from
adventitia
One of the reasons behind the limitation of IMT measurements was the different
definition between studies. Some have used a cut-off of ≥0.9 mm or ≥1 mm (112, 113),
others defined an abnormal IMT as >75th percentile for age, ethnicity and sex, which is
also recommended by American Society of Echocardiography (114).
Salonen et al. were the first to demonstrate the association of carotid IMT with future
coronary events on 1991 (115). They showed that each 0.1 mm increment of IMT was
associated with 11% increased risk of MI on follow up. Subsequently, there were several
other large clinical studies, including: ARIC (Atherosclerosis Risk in Communities)
study (113), the CAPS (Carotid Atherosclerosis Progression Study) (116) the CHS
(Cardiovascular Health Study) (117), the MDCS (Malmo Diet and Cancer Study) (118)
and the Rotterdam Study (119), all showed that carotid IMT can be used to assess
incident CV disease risk. However, studies that evaluated the predictability of the IMT
over and above traditional risk factors (Framingham risk score) have been in most cases
negative. In the Multi-Ethnic Study of Atherosclerosis (MESA) (120), IMT measurement
in the CCA did not predict either MI or ischemic stroke after adjusting for Framingham
1 2
1
2
(a)
(b)
(c)
LUMEN
A B C

27
risk score. Lau et al. showed that the IMT measurements have an area under the curve of
0.69 for predicting CV events compared to 0.66 for Framingham risk score (121). These
data showed that IMT is not a highly predictive marker as it was thought, highlighting the
need for finding another measure (marker) on the carotid artery wall that could be a better
predictor of future risk. Measurement of echogenicity of the intima-media complex (IM-
GSM) was recently introduced as a possible marker of subclinical atherosclerosis. This
could probably differentiate between: adaptive intimal thickening (representing a hyper
reactivity of the smooth muscle cells in the tunica media) from intimal xanthoma or
pathological intimal thickening of the arterial wall (representing the accumulation of
LDL particles and inflammatory cells into intima) (figure 1). An echolucent IM-complex
(low IM-GSM) was associated with different risk factors of atherosclerosis and increased
risk of vascular events and mortality rate (122).
It has been shown that adding plaque and IMT data improved risk prediction in
intermediate risk patients but plaque presence in carotid artery is more effective than IMT
in predicting future ischemic events (106). A meta-analysis showed that compared to
IMT, carotid plaque had a 35% better predictive value of future ischemic events, after
adjusting for Framingham risk factors. In the ARIC study the model that performed best
for prediction of ischemic events, death and revascularization, included traditional risk
factors plus IMT plus carotid plaque (113). For intermediate risk patients NRI was 21%
and it was higher for women than man, 25.4% vs. 16.4% respectively. It was suggested
that carotid plaques grow faster in their length than thickness, and based on this it seems
that assessment of carotid plaque area is potentially a better indicator of disease burden.
In multivariable linear regression models, traditional risk factors explained only 15-17%
of the IMT compared to 52% of the carotid total plaque area. In addition, advancement of
US techniques has made possible assessment of carotid plaque volume by 3D images.
Early results showed plaque volume assessment is a more reliable and sensitive to
changes than cross-sectional area, and could be a better marker to evaluate the effects of
different treatments on the carotid plaque (123).

28
OBJECTIVES
Study I
To evaluate the status of the plaques located in the contralateral to symptomatic carotid
artery and to compare those plaques with plaques located in the same patients ipsilateral
side and also plaques located in asymptomatic carotid arteries.
Study II
To evaluate the accuracy of ultrasound in detecting carotid artery calcification as
compared to cone beam CT and in addition to compares calcification presence and
volume between different subgroup of patients and different risk factors.
Study III
To evaluate the ability of two different carotid arterial wall measures, IMT and IM-GSM
in differentiation between patients with and without prior vascular events in different
arterial systems and also between numbers of arterial systems affected by symptomatic
atherosclerosis disease.
Study IV
To evaluate the association between carotid plaque echogenicity and future
cerebrovascular ischemic events in asymptomatic and symptomatic patients, in a
systematic review and meta-analysis study.

29
METHODS
Preoperative patients evaluation
In all new cases presented with ischemic stroke a brain CTA, MRA or rarely
conventional angiography is performed and analyzed by experienced neuro-radiologists,
either at the Radiology department in Umeå University hospital or it would have been
performed at the referring hospital. Ultrasound examination is performed at the
department of Clinical Physiology at the Umeå University Hospital by experienced
vascular sonographers. All carotid scans are reported and also the images are illustrated
as a graph describing the location and the degree of stenosis and plaque calcification.
Ultrasound carotid imaging follows the NASCET-type protocol for assessing carotid
stenosis. All patients undergo a detailed neurological examination by a neurologist, who
determines if the symptoms are related to the diseased circulatory area in the brain. Also,
an echocardiogram is performed in these patients. Finally, the decision for CEA is
undertaken after discussion among the neurologist, internal medicine specialist and
vascular surgeon. For more complicated cases, there are meetings regularly organized,
“carotid rounds”, where cases are presented and discussed in detail by a group of multi-
disciplinary specialists (internal medicine, radiologists and vascular surgeons), and after
careful evaluation of risk and benefit the decision for BMT or invasive strategy (CEA vs.
CAS) is made.
Definitions and clinical data of patients included in Study I, II and III
Symptomatic patients with carotid stenosis were defined as those who had an ipsilateral
ischemic CV event (stroke, TIA or retinal artery embolization) within the 6 months prior
to the carotid scan, whereas asymptomatic patients were those with carotid
atherosclerosis but with no CV event within the same period (6 months).
Asymptomatic patients were identified because of a) objective or subjective bruit during
auscultation, b) a suspicion of CV symptoms which was later confirmed to be not of CV

30
origin, c) follow-up of a known carotid stenosis, d) previous known CV symptoms > 6
months before, e) detection of calcification in the territory of carotid artery by panorama
imaging, f) CV symptoms related to posterior circulation, or g) carotid disease detection
during evaluation of the thyroid gland.
Patients clinical data were prospectively analyzed to establish; a) the number and
duration of ischemic events; b) time of last symptom; c) risk factors (smoking, diabetes,
hypertension and dyslipidemia) and d) the surgical information. Data for coronary artery
disease, ongoing condition or prior events, were also collected. Routine biochemical data
were collected from the patient's clinical notes including lipid profile and glycated
hemoglobin (HbA1c).
Carotid ultrasound examinations
All patients included in Study I, II and III underwent preoperative carotid Doppler
ultrasound examinations, using a Siemens Acuson Sequoia 512® system with an 8L5
linear transducer. Using conventional Doppler ultrasound criteria the degree of carotid
stenosis was assessed (124).
Ultrasound data retrieval
Studies included in this thesis are retrospective analysis of the patients who were engaged
into two prospective studies:
1) Panorama arm of the SPACE study (15),
2) Additional Neurological SYmptoms before Surgery of the Carotid Arteries — a
Prospective study (ANSYSCAP) (125).
In the study I and II we used data of the Panorama arm of the SPACE study and in study
III we used only a subgroup of asymptomatic patients of the ANSYSCAP study. Over the
course of these studies, the ultrasound imaging storage process was upgraded from
analog to digital.

31
In study I and III, we aimed to obtain a detailed carotid plaque features analysis, we
decided not to combine in the same study data stored in digital and those stored in analog.
So in study I, we included only carotid ultrasound images stored in analog and for study
III we used only images of asymptomatic patients stored in digital. Because in study II
our intention was to only determine carotid plaque calcification (presence/absence), and
not undergoing detailed plaque analysis we decided to use both, data stored in analog as
well as those in digital.
Extraction of the carotid ultrasound examinations
The ultrasound images stored in analog or digital system were exported to the EchoPac
software (General Electric, EchoPac version 8.0.1, Waukesha, WI) and the IMT was
measured and the morphological features (plaque irregularities and calcification) were
assessed. We performed imaging normalization and measurements of the plaque and
intima-media complex features by using an in-house custom developed research software
package (Department of Biomedical Engineering — R&D, Umeå University Hospital,
Umeå, Sweden).
Definitions of ultrasound derived plaque and intima-media complex features
Plaque definition was taken as a focal protrusion that proved to be more than 50% the
thickness of the adjacent wall thickness (126). Each plaque was analyzed for plaque type,
calcification, irregularity, GSM, JBA, GSM of the JBA, DWAs, coarseness and entropy.
In the arteries with only one plaque, the feature of the latter was taken to represent the
artery. Arteries with more than one plaque were treated in a way that the congregated
information/measurements from all plaques represented that artery. When it came to
irregularity measurements, the worst abnormality of irregularity in all plaques was taken
to represent the artery. The presence of either calcification, JBA and DWA was marked
in all studied arteries too. An area-weighted average was taken for continuous features
(GSM, area of JBA and entropy) and used in relation to the size of the artery. The overall
plaque feature was assessed as an averaged sum of individual features multiplied by
plaque area and divided by the total plaque area.
32
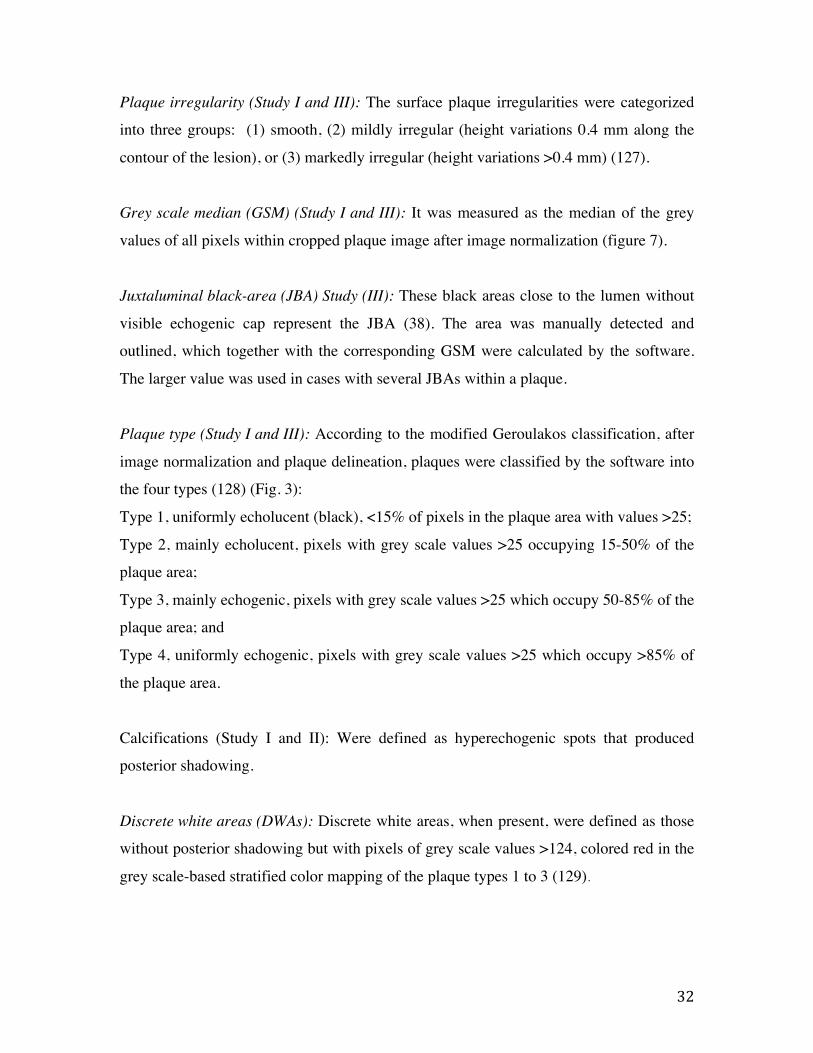
Plaque irregularity (Study I and III): The surface plaque irregularities were categorized
into three groups: (1) smooth, (2) mildly irregular (height variations 0.4 mm along the
contour of the lesion), or (3) markedly irregular (height variations >0.4 mm) (127).
Grey scale median (GSM) (Study I and III): It was measured as the median of the grey
values of all pixels within cropped plaque image after image normalization (figure 7).
Juxtaluminal black-area (JBA) Study (III): These black areas close to the lumen without
visible echogenic cap represent the JBA (38). The area was manually detected and
outlined, which together with the corresponding GSM were calculated by the software.
The larger value was used in cases with several JBAs within a plaque.
Plaque type (Study I and III): According to the modified Geroulakos classification, after
image normalization and plaque delineation, plaques were classified by the software into
the four types (128) (Fig. 3):
Type 1, uniformly echolucent (black), <15% of pixels in the plaque area with values >25;
Type 2, mainly echolucent, pixels with grey scale values >25 occupying 15-50% of the
plaque area;
Type 3, mainly echogenic, pixels with grey scale values >25 which occupy 50-85% of the
plaque area; and
Type 4, uniformly echogenic, pixels with grey scale values >25 which occupy >85% of
the plaque area.
Calcifications (Study I and II): Were defined as hyperechogenic spots that produced
posterior shadowing.
Discrete white areas (DWAs): Discrete white areas, when present, were defined as those
without posterior shadowing but with pixels of grey scale values >124, colored red in the
grey scale-based stratified color mapping of the plaque types 1 to 3 (129).

33
Entropy (Study I and III): Entropy was taken as a measure of the random nature of the
grey-tone values within the plaque (130), with low values for homogenous tissue and
high values for heterogeneous composition.
Coarseness (Study III): Coarseness quantifies the granularity of the plaque texture, which
is consistent with high degree of local uniformity in intensity for large areas. Coarseness
was calculated using the neighborhood grey-tone difference matrix method (131). It has
already been demonstrated that coarseness discriminates symptomatic from
asymptomatic plaques with low values in symptomatic plaques consistent with
heterogenic, more granular texture and less uniform composition (132).
Figure 7. Image normalization and plaque features assessment
Intima–media complex measurements (Study III)
Both IMT and IM-GSM were measured in the distal segment of the common carotid
artery within 1 cm (± 2 mm) distance starting from the carotid bifurcation at the right and
left carotid systems. When a plaque was present in this region, the IM-complex free-of-

34
plaque was selected, and if it was <8 mm long the artery was excluded from the study (n
= 8).
Carotid-intima media thickness (IMT)
IMT was conventionally defined as the distance between the media–adventitia interface
and the lumen–intima interface. One-centimeter long segments of the far wall were
measured and an average of three cycles was taken (133).
Intima–media grey scale median (IM-GSM)
The median of the grey values of all pixels within a one-centimeter length cropped intima
media complex image was measured to reflect IM-GSM. The distal intima-media
complex in the normalized and standardized image was manually outlined, prior to
feature calculation.
Cone Beam CT (CBCT) analysis
Excised plaques after CEA were examined by CBCT (Cone Beam Computed
Tomography, 3D Accuitomo 170, J Morita MFG Corporation, Kyoto, Japan; 60 kV, 1
mA, 360°). Volumes of 4 × 4 or 6 × 6 cm were used and they had a resolution of 0.08–
0.125 mm voxel size. The reconstructions were made with 0.5 mm slice thickness and 0.5
mm increment. A software program (General Electric Company, Barrington, IL, USA,
advantage workstation 4.3, Volume Viewer 2) for volume measurements was also used.
All calcification spots were measured in mm3, with resolution of the volume
reconstructions of 1 mm3. Plaques with multiple dispersed calcifications had the largest
calcification nodule volume used to represent the intra-plaque calcification.
Carotid endarterectomy (CEA) procedure
All patients were operated under general anesthesia. Common, internal and external
carotid arteries were exposed and a longitudinal incision was made in the common
carotid artery and then extended into the internal branch until a healthy area distal to the
plaque. The intimal thickening of the common carotid artery was divided and the plaque
was gently dissected from the artery, leaving the adventitial layer intact with careful

35
handling of the plaque. After excision, the plaque was immediately placed in a plastic
tube and stored in −20 °C, then transferred to a −80 °C freezer until later taken out for
CBCT analysis.
Source of data
Study I and II
This is a secondary analysis of the Ultrasound of the Panorama arm of the SPACE study
[15]. In the main study, 100 consecutive patients with symptomatic or asymptomatic
carotid stenosis (≥50%) who were eligible for CEA were included. All patients included
agreed to extensive preoperative evaluation and underwent CEA.
Study III
This is a secondary analysis of the ANSYSCAP study (125). In the main study
consecutive symptomatic and asymptomatic patients with 50-99% stenosis were included
between August 2007 and December 2009. In ANSYSCAP, consecutive patients with a
50-99% carotid stenosis eligible for CEA were prospectively included between August
2007 and December 2009.
Study IV
For the systematic review and meta-analysis we have systematically searched electronic
databases (PubMed, MEDLINE, EMBASE and Cochrane Center Register) up to January
2015 for studies evaluating the effect of carotid plaque echogenicity on CV symptoms.
The search terms used were: “carotid atherosclerosis”, “carotid plaque”, “echogenicity”
“ultrasound” “symptoms”, “Stroke”, “TIA” “amaurosis fugax” in various combinations.
Two researchers (FJ and PI) independently performed the literature search, study
selection and data extraction. There was no time or publication limit in the literature
search. The selected reports were manually searched, and relevant publications, obtained
from the reference lists, were retrieved.

36
Inclusion/exclusion criteria
Study I
Out of 47 cases with a preoperative ultrasound examination stored in the analog format
we analyzed 39. Eight patients were excluded because either the examinations could not
be retrieved and analyzed (n = 7) or the patient had an asymptomatic carotid stenosis but
a recent (<6 months) CV event on the contralateral side. Of the 39 patients included, 33
had symptomatic carotid stenosis (50-99%) and 6 had unilateral or bilateral
asymptomatic stenosis (50-99%). All patients had at least one atherosclerotic plaque on
both sides. We further excluded 12 arteries because of total occlusion (n=2) or because of
>50% of the plaque covered by shadow derived from extensive plaque calcification
(n=10). So, in total we analyzed 66 arteries (25 contralateral to symptomatic, 30
symptomatic and 11 asymptomatic). The contralateral arteries were compared with the
symptomatic and asymptomatic arteries.
Study II
Out of 101 carotid plaques (of 94 patients) we finally analyzed 94 plaques (from 88
patients). Seven patients were excluded, five because of suboptimal image quality and
two because there was no calcification in the internal carotid artery (ICA) plaque but a
distinct calcification in the external carotid artery (ECA). Since it was unclear whether
the ECA would be included in the extirpated plaque, it was impossible to make a
reasonable assessment without breaking the blinding.
Study III
Out of 87 asymptomatic patients stored in the digital system we finally analyzed 166
arteries. Seven arteries were excluded because the common carotid artery segment free of
plaque was <0.8mm.

37
Figure 8. Flowchart of the patients selections for study I, II and III
Study IV
Studies reporting results on US assessment of plaque echogenicity and their association
with CV symptoms (Stroke, TIA, amaurosis fugax) were included in our analysis.
Specific inclusion criteria for the systematic review were: (1) Cohort prospective studies;
(2) English language articles; (3) studies with ≥30 subjects, and (4) ultrasound based
characterization of carotid artery plaque, visually based on Gray-Weale, or using
computer-assisted analysis (Geroulakos classification or GSM). Studies that visually
categorized plaques in only two groups echogenic/echolucent, that evaluated plaque
heterogeneity, that used imaging techniques other than US (e.g. MRI, CT, IVUS, PET),
and those that analyzed plaque features other than echogenicity (volume, degree of

38
stenosis, plaque irregularities, ulceration, neovascularization) as predictors of CV
symptoms were excluded (figure 9).
Figure 9. Flowchart of the studies selection for the study IV
Statistical analysis
Study I, II and III. All statistical analyses were performed using IBM SPSS Statistics
22. Categorical variables were expressed as percentages and continuous variables as
mean ± SD (median). Mean values of the plaque texture features were compared between
groups, using independent samples t-test and Man-Whitney test. Baseline differences
between groups for each plaque texture feature were tested using one-way ANOVA, for
more than two groups in analysis. Post hoc analysis (Bonferroni) was also performed for
Records identified through databases searching
(n=1385)
Additional records identified through
related citations search(n=20)
Records after duplicates removed(n=1387)
Records screened(n=1387)
Full-text articles assessedfor eligibility
(n=30)
Recordsexcluded(n=1357)
Cross-sectional studies (n=12)Evaluated plaque hetero-genicity (n=6)Categorized carotid plaque echogenicity in two groups (n=2)
vio Iden
tifica
tion
Scre
enin
gEl
igib
ility
Incl
uded
Studies included in qualitative analysis (n=10)
Studies included in meta-analysis
(n=10)

39
continuous variables. If variables did not have normal distribution, the non-parametric
Kruskal-Wallis test was used. Fisher's exact probability test or the Chi-2-test was used
when comparing two sets of binary or categorical values, with a pre-selected significance
level of p < 0.05.
Quartile analyses were used for categorizing calcification volume into four groups.
Kappa values were calculated to determine the accuracy of US in detecting calcification.
Logistic regression analysis was used to determine the association of an echolucent
intima-media complex with multi-system atherosclerosis disease.
Study IV.
We have separately analyzed studies that evaluated asymptomatic and symptomatic
patients. I2 statistic was used to measure the heterogeneity. When there was a significant
variation between studies size, length and follow-up, as well as patient’s characteristics,
we used random-effect. Publication bias was examined using Begg–Mazumdar test. All
analyses were conducted using Comprehensive Meta Analysis version 3 software (Biostat
inc., Englewood, NJ, USA).

40
RESULTS
Study I
Clinical data
The severity of carotid artery stenosis and other risk factors are presented in figure 10 and
11. There was no difference between asymptomatic and symptomatic patients with
carotid stenosis.
Figure 10. Clinical data in symptomatic and asymptomatic patients. BP-blood pressure,
SD-standard deviation
0"
10"
20"
30"
40"
50"
60"
70"
80"
90"
Symptoma3c" Asymptoma3c"
Age,%mean%(SD)%
0"20"40"60"80"100"120"140"160"180"200"
Symptoma/c" Asymptoma/c"
Systolic)BP)(SD))
0"10"20"30"40"50"60"70"80"90"
100"
Symptoma3c" Asymptoma3c"
Diastolic)BP)(SD))
0"
1"
2"
3"
4"
5"
6"
7"
Symptoma1c" Asymptoma1c"
Total&cholesterol&(SD)&
0"
0.5"
1"
1.5"
2"
2.5"
Symptoma.c" Asymptoma.c"
HDL$cholesterol$(SD)$
0"
0.5"
1"
1.5"
2"
2.5"
3"
3.5"
4"
Symptoma0c" Asymptoma0c"
LDL#cholesterol#(SD)#mmol/L mmol/L
mmol/L
mmHgmmHg
mmHg

41
Figure 11. Distribution of the different risk factors, previous or ongoing ischemic events
and therapy in symptomatic and asymptomatic patients
Degree of stenosis
Based on the carotid Doppler velocities there was no difference in the degree of stenosis
between contralateral and asymptomatic arteries. In symptomatic arteries the degree of
stenosis was higher compared to contralateral (p<0.001) and asymptomatic arteries
(p=0.006).
Contralateral vs. Symptomatic
The GSM and JBA in the plaques located in the contralateral to symptomatic side had
similar features to those in the symptomatic side (26.2 ± 7.3 vs. 24.9 ± 7.8, p = 0.536)
(figure 12) and (5.0 ± 3.9 vs. 4.6 ± 3.0, p = 0.80), respectively. Also, the plaque
irregularities and PT were not different between these two groups. The only plaque
feature that differentiated between symptomatic and contralateral arteries was the
prevalence of JBA, which was higher in symptomatic arteries (p=0.001).
0"
10"
20"
30"
40"
50"
60"
70"
80"
90"
100"
Women"
Current"smoker"
Diabetes"
Previous"myocardial"infarcBon"
Current"angina"
Stroke"6"months"before"
ClaudicaBon"intermitent"
Previous"revascularizaBon"of"any"type"
Any"lipid"lowering"medicaBon"
33.3"
6.1"
30.3"
15.2"
3"
24.2"18.2"
27.3"
93.9"
33.3"
0"
33.3"
16.7"
0"
16.7"
33.3"
50"
100"
SymptomaBc" AsymptomaBc"%

42
Contralateral vs. Asymptomatic
Contralateral arteries had more vulnerable morphological and textural plaque features
compared to those in the asymptomatic arteries, with lower GSM (26.2 ± 7.3 vs. 49.4 ±
14.6, p < 0.001), lower GSM of the JBA (5.0 ± 3.9 vs. 11.4 ± 2.1, p = 0.001), higher
prevalence of plaque type 1 and 2 and lower prevalence of type 3 and 4 (p = 0.001) and
higher prevalence of mild (60% vs. 36%) and marked irregularities (28% vs. 9%), p =
0.03, (Figure 12).
Figure 12. Echogenicity (left) and surface plaque morphology (right) between
asymptomatic, contralateral to symptomatic and symptomatic arteries
Reproducibility analyses
Interobserver variability was expressed using intra-class correlation coefficient. For GSM
it was 0.928 (95% CI, 0.899-0.950) and for JBA it was 0.972 (95% CI, 0.848-0.965). The
interobserver agreement for JBA was (K=0.948, p<0.0001) and for PT was (0.843,
p<0.001).

43
Study II
Clinical data
Mean age of the patients included in this study was 70 ± 7 years and 33% were females.
Symptomatic carotid artery stenosis was observed in 73 patients and asymptomatic
carotid stenosis in the remaining 15 patients. Six of the symptomatic patients underwent
bilateral carotid endarterectomy (CEA). A stenosis severity of 50%–69% and 70-99%
was found in 6 and 85 cases, respectively, and near-occlusion in three arteries. Patient’s
baseline characteristics are presented in Table 1.
Baseline Study population (n=88) Age (years), mean±SD) Females, n (%)
70±7 29 (33)
Systolic blood pressure (mmHg), mean±SD 147±22.6 Diastolic blood pressure (mmHg), mean±SD 78±12 Total cholesterol (mmol/l), mean±SD 4.61±1.03 LDL (mmol/l), mean±SD 2.60±0.92 HDL (mmol/l), mean±SD 1.27±0.48 Creatinine (μmol/l), mean±SD 84±25 HBA1c (mmol/mol), mean±SD 52.5±12.7 Symptomatic carotid stenosis, n (%) 73 (83) Prior myocardial infarction, n (%) 14 (16) Current angina pectoris, n (%) 7 (8) Heart failure, n (%) 1 (1.1) Previous stroke (>6 months to the present evaluation), n (%) 14 (16) Claudication (lower extremity artery disease), n (%) 10 (11.4) Any previous revascularization for ischemia, n (%) 24 (27.3) Current smoker, n (%) 9 (10.2) Diabetes, n (%) 29 (33) Lipid lowering medicine, n (%) 82 (93.2) Platelet inhibiting or anticoagulation medicine, n (%) 88 (100) Blood pressure reducing medicine, n (%) 84 (95.5)
Table 1. Patients’ data

44
Ultrasound vs. CBCT
Carotid artery calcification was detected in 87.2% of cases in the preoperative ultrasound
examinations and in 98.9% in CBCT examinations after CEA. There was no difference
between the 50%–69% and the 70%–99% degree of stenosis groups (Table 2).
Furthermore, there was no difference in carotid calcification between different risk
factors (Table 2). In general, the sensitivity of carotid ultrasound in detecting the
presence of calcification was 88.2%. The calcification volumes acquired by CBCT were
divided into 4 groups using quartile analysis; <8, 8–35, 36–70 and >70 mm3 (Figure 13).
Calcification volumes ≥8 mm3 were accurately detectable by ultrasound with a higher
sensitivity of 96% compared to the sensitivity of 62% for the calcification volume of <8
mm3 (Table 2, Figure 13).
CBCT\Ultrasound Total
arteries, n
Calcification on CBCT
Calcification on US
US Sensitivity
Calcification 94 93 82 88.20% Calcification ≥8
mm3 72 72 69 96%
Calcification <8 mm3
22 21 13 62%
Table 2. Accuracy of Doppler ultrasound in detecting carotid calcification

45
Figure 13. Quartiles of calcification volumes detected and not detected by ultrasound
Calcification vs. Symptoms
The presence of calcification, evaluated by US was not different between symptomatic
and asymptomatic patients. In addition, we explored whether dispersed calcification
within the plaque could be associated with patient’s symptoms, but we didn’t find any
difference between groups. Even using quartiles of calcification volumes evaluated by
CBCT couldn’t discriminate between symptomatic and asymptomatic patients. In table 3
we have compared calcification volume (< and ≥ than 8 mm) between different risk
factors.
Reproducibility analyses
The inter-observer agreement for the presence of calcification in the carotid artery
plaques evaluated by US was good (K=0.905, p<0.001).

46
Subgroups Arteries n
<8mm3 calcification volumes on CBCT,
n (%) p
Age <75 68 18 (26.5) ≥75 26 4 (15.3) 0.21
Gender Female 30 7 (23.3) Male 64 15 (23.4) 0.99
Symptomatic 79 20 (25.3) Asymptomatic 15 2 (13.3) 0.31 Current smoker
Yes 10 4 (40.0) No 84 18 (21.4) 0.19
Diabetes Yes 31 8 (25.8) No 63 14 (22.2) 0.60
Previous stroke Yes 17 2 (11.8) No 77 20 (26.0) 0.21
Previous MI Yes 15 3 (20.0) No 79 19 (24.0) 0.73
Statin therapy Yes 87 21 (24.1) No 7 1 (14.3) 0.55
Degree of stenosis 50-69% 6 0 (0) 70-99% 85 20 (23.5)
near-occlusion 3 2 (66.7) 0.08 Table 3. Subgroup analysis

47
Study III
Clinical data
In this study we included 87 asymptomatic patients (166 carotid arteries). Mean age of
the patients was 69±6 year and 34.5% were females). 23% of patients had previous MI,
16% had angina, 21% had previous ischemic stroke, and 22% (n=19) had lower limb
atherosclerosis in the form of intermittent claudication (Table 4). 50% (n=43) of the
patients were asymptomatic, 34% (n=30) had previous disease in one arterial system and
16% (n=14) had previous disease in multi-arterial systems.
Age, years, mean±SD 69±6 Female, n (%) 30 (34.5) Current smoking, n (%) 18 (20.7) Diabetes, n (%) 25 (28.7) Previous MI, n (%) 20 (23) Current angina, n (%) 14 (16.1) Previous stroke, n (%) 18 (20.7) Intermittent claudication, n (%) 19 (21.8) SBP (mmHg), mean±SD 145.7±20 DBP (mmHg), mean±SD 77±12 Anti-platelet or anti-coagulation therapy, n (%) 84 (96.6) Blood pressure lowering therapy, n (%) 80 (92) Lipid lowering therapy, n (%) 78 (89.7) HbA1c (%), mean±SD 5.2±1.1 Total cholesterol (mmol/l), mean±SD 4.67±0.9 LDL (mmol/l), mean±SD 2.57±0.9 HDL (mmol/l), mean±SD 1.34±0.4
Table 4. Patients’ data
Intima-media measurements vs. previous vascular symptoms
In patients with previous MI the IMT was higher (1.06±0.2 vs. 0.95±0.2 mm, p=0.034)
and IM-GSM was lower (21±15 vs. 33±16, p=<0.001). Also, patients with previous
stroke had lower IM-GSM (24±12 vs. 33±16, p=0.007) but IMT was not different
between those with and without stroke (1.03±02 vs. 0.96±0.2 mm, p=0.195). IMT and

48
IM-GSM were not different in patients with and without previous atherosclerosis disease
in the lower extremity (Figure 14).
Figure 14. IM-GSM in patients with previous stroke, MI angina and claudication
intermittent
IMT and IM-GSM vs. multi-system atherosclerosis disease
IM-GSM was significantly different between groups, it decreased significantly with
increasing number of arterial systems affected by symptomatic atherosclerosis disease,
37.7±15.4 vs. 29.3±16.4 vs. 20.7±12.9, p<0.001, for asymptomatic, symptoms in one and
in multi-arterial system disease, respectively. When analyzing IM-GSM measured in the
artery-side with higher IMT the results were similar (Table 5). IMT was not significantly
different between groups, 0.95±0.2mm vs. 0.98±0.2mm vs. 1.02±0.02mm, p=0.49 (Table
5, Figure 15).

49
Asymptomatic (n=83)
Previous symptoms in one arterial system (n=58)
Previous symptoms in >one arterial system (n=25)
p
IM-GSM, mean±SD* IM-GSM, mean±SD#
37.7±15.4 35.0±15.7
29.3±16.4 29.5±18.6
20.7±12.9 17.4±13.9
<0.001 0.001
IMT, mean±SD 0.95±0.2 0.98±0.2 1.02±0.2 0.49 Plaque GSM, mean±SD 41.4±17.0 33.0±16.0 20.9±10.0 <0.001 Plaque Coarseness, mean±SD 13.7±4.4 11.4±5.1 7.6±3.9 <0.001 Plaque Entropy, mean±SD 3.5±0.2 3.6±0.2 3.6±0.2 0.13 Plaque JBA, n (%) 14 (19.4) 14 (28.6) 13 (72.2) <0.001 Plaque GSM of JBA 6.8±5.0 12.1±9.0 3.8±3.3 0.01
Table 5. Common carotid wall and bifurcation plaque measurements in different groups.
(*)IM-GSM mean of both sides. (#) IM-GSM measured on the side with higher IMT
Figure 15. IM-GSM, plaque GSM and plaque coarseness were significantly decreased
with increasing number of arterial systems affected by atherosclerosis
p<0.001p<0.001
p<0.001
p=0.137p=0.614
Asymptomatic Previous symptoms in one arterial system
Previous symptoms in >1 arterial system
0
10
20
30
40
50Plaque GSMIM-GSMPlaque coarsenessPlaque entropyIMT
Mea
n

50
Using ROC curve analysis we determined IM-GSM of 25 as the best cut-off value to
differentiate between numbers of arterial systems affected by the atherosclerosis disease.
Out of 25 arteries in the multi-system group, 16 (64%) had an IM-GSM <25, having an
OR of 3.23 (95%CI 1.33-7.85), p<0.01. Even after adjusting for IMT this association
remained significant with OR 2.65 (95%CI 1.56-6.67), p=0.03.
Reproducibility analyses
For intima-media complex and plaque measurements there was a good agreement
between the two observers. The interobserver variability for IMT measurements
expressed by intra-class correlation coefficient was 0.977 (95% CI, 0.963-0.988) and for
IM-GSM it was 0.934 (95% CI, 0.783-980). For plaque measurements intraclass
correlation was 0.921 (95% CI, 0.890-0.942) and for JBA it was 0.910 (95% CI, 0.871-
0.960). In addition we performed Bland-Altman test for the intima-media complex
measurements and there was not any proportional bias for IMT and IM-GSM
measurements, mean difference between the two observers measurements was not
significantly different from zero.
Study IV (Systematic review and meta-analysis)
Study selection
After the first searching of online medical databases we identified 1385 studies. In
addition ten studies were identified through related citations. After excluding duplicates,
1387 studies were screened (table 6). By reading the abstracts of the selected papers, we
first depicted 30 potentially eligible articles for further review, of these only 10 (101,
134-142) met the inclusion criteria for qualitative analysis. One of the studies (137) had
analyzed separately symptomatic and asymptomatic patients and we included both groups
in the meta-analysis. The remaining 20 studies were excluded (figure 9).

51
Qualitative assessment and study characteristics
There were considerable differences between reports in the degree of stenosis between
asymptomatic studies included in this analysis with 3 studies that have included patients
with mild to severe carotid stenosis (30-99%), 3 studies with moderate to severe stenosis
(50-99%) and 2 studies with severe carotid stenosis (≥70%) stenosis.
Author, year Number of subjects
No. of arteries
analyzed
Degree of carotid stenosis
Echolucency definition
Mean follow-up (months)
Outcome
1.Polak et al. 1998 (134) 4886 N/A 30-99% PT 1 and 2 39.6 Stroke, TIA 2.Mathiesen et al. 2001 (135) 223 N/A 35-99% PT 1 and 2 36 Stroke, TIA, AF 3.Liapis et al. 2001 (136) 332 442 30-95% PT 1 and 2 44 Stroke, TIA, AF 4a.Grønholdt et al. 2001 (137) 111 111 50-99% GSM<75 52.8 Stroke
4b.Grønholdt et al. 2001 135 135 50-99% GSM<75 52.8 Recurrent symptoms
5.Nicolaides et al. 2005 (138) 1115 N/A 50-99% PT 1, 2 ,3 37.1 Stroke, TIA, AF 6.Hashimoto et al. 2009 (139) 250 297 50-99% GSM<69 25 Stroke 7.Topakian et al. 2011 (140) 435 N/A 70-99% PT 1 and 2 24 Stroke, TIA
8.Salem et al. 2012 (101) 158 N/A 50-99% PT 1 and 2 2 weeks Recurrent symptoms
9. Silvestrini et al. 2013 (141) 621 N/A 70-99% PT 1 and 2 22 Stroke TIA
10. Singh et al. 2013 (142) 206 N/A 30-99% PT 1 and 2 6 Recurrent symptoms
Table 6. Studies included in the qualitative and qualitative analysis. GSM - grey scale
median, AF - amaurosis fugax, TIA - transient ischemic attack, PT - plaque type based on
Gray-Weale or Geroulakos classification
Four studies have visually (qualitatively) evaluated plaque echogenicity and four others
performed computer-assisted (quantitative) analysis of the plaque echogenicity. Two
studies defined plaque echolucency based on a cut-off value of GSM (<69 and <75) and
six studies defined plaque types (PT) 1 and 2 as echolucent and PT 3 and 4 as echogenic.
All studies have used longitudinal section US images for carotid echogenicity evaluation.
Patient’s clinical outcome was defined as stroke, TIA or amaurosis fugax (AF) in 8
studies and as recurrent CV accidents in 3 studies (Table 6).
Seven studies showed a higher risk of ipsilateral CV accidents in asymptomatic patients
with echolucent carotid plaques. Two studies showed higher risk of recurrent CV

52
accidents and one study showed that echolucent plaques could predict future events in
symptomatic but not asymptomatic patients.
Although, we observed a difference in the follow-up periods between different
symptomatic studies included in the analysis, the association between plaque
echolucency and recurrent ischemic events was determined even at only 2 weeks after
symptoms initiation. The degree of stenosis among symptomatic patients studies ranged
from 30-90%.
Meta-analysis results
We have meta-analyzed 8 studies with 7937 asymptomatic patients and 3 studies with
499 symptomatic patients. Among studies that met the set criteria for inclusion in the
meta-analysis, one has reported separately data for symptomatic and asymptomatic
patients and we included both of them in the analysis separately. Echolucent carotid
plaques predicted future CV accidents in asymptomatic patients with pooled relative risk
(RR) of 2.72 (95% CI, 1.86 to 3.96), p<0.001 (figure 16), and also recurrent symptoms in
symptomatic patients with pooled RR of 2.97 (95% CI, 1.85-4.78), p<0.001 (figure 17).
Figure 16. Forest plot of the studies evaluating the association between echolucent
plaques and future CV accidents in asymptomatic patinets. I2=39
Study name Statistics for each study Risk ratio and 95% CI
Risk Lower Upper ratio limit limit Z-Value p-Value
Polak et al. 1998 2.780 1.359 5.686 2.800 0.005Liapis et al. 2001 1.900 1.080 3.341 2.229 0.026Mathiesen et al. 2001 2.380 1.181 4.795 2.426 0.015Gronholdt et al 2001 1.010 0.430 2.371 0.023 0.982Nicolaides et al. 2005 4.800 2.256 10.215 4.071 0.000Hashimoto et al 2009 4.400 1.182 16.383 2.209 0.027Topakian et al. 2011 6.430 1.352 30.573 2.339 0.019Silvestrini et al. 2013 4.150 1.764 9.763 3.261 0.001
2.720 1.864 3.968 5.191 0.000
0.01 0.1 1 10 100
Favours A Favours B

53
Figure 17. Forest plot of the studies evaluating the association between echolucent
plaques and recurrent CV accidents in symptomatic patinets. I2=0, Kendall’s Tau=0.66,
p=0.29
Subgroup analysis
Based on the degree of carotid artery stenosis (mild-to-severe vs. moderate-to-severe vs.
severe), the time period during which patients were recruited in the studies and US
imaging was performed (before 2000 vs. since 2000) definition of the echolucent plaque
(GSM cut-off vs. PT 1 and 2), and the methods used for assessment of carotid plaque
types (visually vs. computer assisted), we have performed some comparison analyses
between subgroup (table 7).
There was clear association between echolucent plaques and future CV symptoms for all
degrees of stenosis categories, however, the highest RR was observed among studies with
severe stenosis 4.72 (95% CI, 1.86-12.00), p<0.001 (figure 18). Also, studies that
included US data collected after 2000 showed higher RR 4.65 (95% CI, 2.84-7.61) than
those before the year 2000, RR 1.97 (95% CI, 1.40-2.78) (figure 19). In addition,
analyzing separately only studies that have used a GSM cut-off to define carotid plaque
echolucency the prediction of future CV events was not significant (p=0.23), whereas RR
of the studies that defined echolucency as PT 1 and 2 was 3.01 (95% CI, 2.02-4.50),
p<0.001 and in cases when the PT was defined using computer-assisted Geroulakos
classification RR was even higher 3.56 (95% CI, 2.08-8.08), p<0.001 (table 7)
!
Study name Statistics for each study Risk ratio and 95% CI
Risk Lower Upper ratio limit limit Z-Value p-Value
Gronholdt et al 2001 3.100 1.308 7.346 2.570 0.010Salem et al. 2012 6.200 1.860 20.667 2.970 0.003Singh et al. 2013 2.360 1.240 4.491 2.616 0.009
2.977 1.853 4.782 4.509 0.000
0.01 0.1 1 10 100
Favours A Favours B
Meta Analysis

54
Figure 18. Subgroup analysis between different carotid stenosis
Figure 19. Subgroup analysis based on the year of patients’ recruitment and US image
analysis
Group byComparison
Study name Comparison Statistics for each study Risk ratio and 95% CI
Risk Lower Upper ratio limit limit Z-Value p-Value
Mild-severe Polak et al. 1998 Mild-severe 2.780 1.359 5.686 2.800 0.005
Mild-severe Liapis et al. 2001 Mild-severe 1.900 1.080 3.341 2.229 0.026
Mild-severe Mathiesen et al. 2001 Mild-severe 2.380 1.181 4.795 2.426 0.015
Mild-severe 2.292 1.311 4.006 2.911 0.004
Moderate-severe Gronholdt et al 2001 Moderate-severe 1.010 0.430 2.371 0.023 0.982
Moderate-severe Nicolaides et al. 2005 Moderate-severe 4.800 2.256 10.215 4.071 0.000
Moderate-severe Hashimoto et al 2009 Moderate-severe 4.400 1.182 16.383 2.209 0.027
Moderate-severe 2.647 1.347 5.201 2.824 0.005
Severe Topakian et al. 2011 Severe 6.430 1.352 30.573 2.339 0.019
Severe Silvestrini et al. 2013 Severe 4.150 1.764 9.763 3.261 0.001
Severe 4.725 1.860 12.003 3.264 0.001
Overall 2.801 1.756 4.469 4.321 0.000
0.01 0.1 1 10 100
Favours A Favours B
!
Stenosis
!
Group byOutcome
Study name Outcome Statistics for each study Risk ratio and 95% CI
Risk Lower Upper ratio limit limit Z-Value p-Value
Before 2000 Polak et al. 1998 Before 2000 2.780 1.359 5.686 2.800 0.005
Before 2000 Liapis et al. 2001 Before 2000 1.900 1.080 3.341 2.229 0.026
Before 2000 Mathiesen et al. 2001 Before 2000 2.380 1.181 4.795 2.426 0.015
Before 2000 Gronholdt et al 2001 Before 2000 1.010 0.430 2.371 0.023 0.982
Before 2000 1.976 1.402 2.785 3.893 0.000
Since 2000 Nicolaides et al. 2005 Since 2000 4.800 2.256 10.215 4.071 0.000
Since 2000 Hashimoto et al 2009 Since 2000 4.400 1.182 16.383 2.209 0.027
Since 2000 Topakian et al. 2011 Since 2000 6.430 1.352 30.573 2.339 0.019
Since 2000 Silvestrini et al. 2013 Since 2000 4.150 1.764 9.763 3.261 0.001
Since 2000 4.652 2.840 7.618 6.108 0.000
Overall 2.975 1.287 6.877 2.549 0.011
0.01 0.1 1 10 100
Favours A Favours B
Year

55
Relative risk
Lower limit
Upper limit Z value p value
Between subgroups
(p) Degree of stenosis Mild-to-severe 2.29 1.31 4 2.51 0.004 Moderate-to-Severe 2.64 1.34 5.2 2.82 0.005 Severe 4.72 1.86 12 3.26 <0.001 0.42 Period of ultrasound data collections Before 2000 1.97 1.4 2.78 3.89 <0.001 Since 2000 4.65 2.84 7.61 6.1 <0.001 0.005 Echolucency definition
GSM cut-off 1.66 0.71 3.92 1.19 0.23 PT 1 and 2 3.01 2.02 4.5 5.4 <0.001 0.21 PT assessment
Visual 2.56 1.64 4 4.15 <0.001 Computer assisted 3.56 2.08 6.08 4.65 <0.001 0.35
Table 7. Subgroup analysis of asymptomatic patients studies
In addition, we performed meta-regression analysis of the echolucent plaques and
different stenosis catogery on future ischemic events risk in asymptomatic patients.
Although there was an increasing trend of future events with increased stenosis severity,
the slope was not significant (p=0.19) (figure 20).
Figure 20. Meta-regression analysis. Regression of Log risk rato (RR) on carotid stenosis
severity in patients with echolucent plaques
!
!
!
Regression of Log risk ratio on grade
grade
0.5 0.8 1.0 1.3 1.5 1.8 2.0 2.3 2.5 2.8 3.0 3.3 3.5
Log
risk
rat
io
3.50
3.00
2.50
2.00
1.50
1.00
0.50
0.00
-0.50
-1.00
Mild to severe Moderate to severe Severe
Regression of Log RR on carotid stenosis severity
β=0.31 (95% CI, -0.16-0.80), p=0.19
Log
risk
ratio

56
Publication Bias
There was no publication bias reported for the studies included in the meta-analysis
(Figure 17 and 21).
Figure 21. Asymptomatic patients, funnel plot of the standard error by log risk ratio.
Kandall’s Tau=0.392, p=0.173
-0.5 0.0 0.5 1.5 2.0 2.5-1.0-1.5
0.0
0.2
0.4
0.6
0.8
Sta
ndar
d E
rror
Log Risk ratio

57
DISCUSION
Study I
Findings: This study shows that carotid plaques in the contralateral to symptomatic side
have similar features compared with the symptomatic ones but more vulnerable features
than the asymptomatic arteries. Contralateral plaques have lower GSM, lower GSM of
the JBA, higher prevalence of plaque type 1 and 2 compared with asymptomatic arteries.
In addition, they have more mild and marked irregular plaques, than the asymptomatic
ones. JBA presence was the only plaque features that showed difference between
contralateral and symptomatic arteries.
Data interpretation: It is generally believed that the pattern of carotid atherosclerosis is
unpredictable. The findings in this study show that symptomatic patients had more
aggressive disease, in both carotid sides, in the form of irregular contour and signs of
inconsistent texture, suggesting vulnerable plaque features compared to those seen in
asymptomatic patients. Even though the symptoms were unilateral, our results clearly
show that contralateral arteries have very similar features. However, the JBA was more
frequent in the ipsilateral carotid arteries and this could represent an additional feature for
plaque instability which could also help in better patient risk stratification. Previous
studies confirmed that vulnerable patients may have multiple unstable lesions, other than
the culprit ones, either distally or even in another territory (1, 143). These claims support
our results. However, despite our findings and the differences we identified between
symptomatic and asymptomatic arteries, it must be mentioned that identification of
vulnerable plaques remains a contentious issue in clinical practice. Quantitative
assessment of carotid plaque echogenicity and textural features analysis can identify
potentially unstable plaques, which are echolucent (low GSM) compared to echogenic
(high GSM) asymptomatic plaques. Again using histology as the gold standard, it has
been confirmed in imaging studies that echogenic plaques represent densely fibrotic and
calcific composition (144), whereas, Low GSM was associated with large hemorrhagic
areas and lower GSM values located in the juxtaluminal position that was associated with
predominant necrotic cores. Morphological plaque features (e.g. surface plaque

58
irregularities), GSM and JBA have been used in the prospective studies as an attempt to
predict future vascular events (145, 146). To our knowledge this is the first study that,
used computer based morphological and textural plaque features in providing information
on plaque vulnerability in contralateral carotid arteries.
Clinical implications: The findings of this study might have important clinical
implications, as it: (a) confirms the generalized nature of atherosclerosis in patients with
carotid disease, for not only involving more than one segment at the side of the symptoms
but also the contralateral side, (b) confirms the assessment of carotid plaque features by
computer assisted videodensitometric plaque features as a valuable analysis that could
reliably differentiate symptomatic from asymptomatic carotid disease, and (c) confirm
that the presence of JBA in carotid arteries could be of clinical relevance in addition to
plaque echogenicity, because it was the only feature that showed difference between the
two carotid sides of symptomatic patients. In addition, it may have therapeutic
implication since; being at high risk of recurrent events, symptomatic patients with
bilateral disease should receive aggressive secondary prevention treatment in addition to
revascularization.
Study II
Findings: The results of this study show the sensitivity of US for calcification detection
compared to CBCT images acquired in plaque specimens collected after CEA. US
sensitivity was high in identifying calcification volume ≥8 mm3 by CBCT, but,
calcification volumes <8 mm3 were inconsistently detected, with a sensitivity of only
62%. There was no difference for calcification between symptomatic and asymptomatic
patients, neither between other risk factors and degree of stenosis.
Data interpretation: The most accurate method for detection and quantification of carotid
artery calcification is computed tomography, which is highly correlated with the amount
of calcification evaluated by histology sections (48, 147). Because CT involves radiation
and is an expensive procedure, imaging plaque features, including calcification, by other

59
radiation free method that is more patient friendly such as US could have significant
clinical relevance. But, why is the detection of calcification important. Firstly, it has
been confirmed that the presence of calcification in carotid plaque is associated with
lower risk of future brain ischemic events, suggesting that the presence of calcification is
an indicator of plaque stability (47). Sometimes identifying vulnerability based on its
composition is time consuming, and demands expertise, in such circumstances detection
of calcium in the plaque could be a fast and important indicator of plaque stability.
However, it should be mentioned that calcification is not always a sign of stability. In the
contrary, intimal plaque microcalcification is an accepted sign of plaque vulnerability,
however detection of its presence is not possible with non-invasive imaging modalities,
but only with optical coherence tomography (OCT) (16). Secondly, detection of
calcification could be important in decision making for interventional treatment of carotid
atherosclerosis (CEA vs. CAS). It has been reported that implanting a stent in a calcified
carotid plaque is associated with increased risk of ipsilateral stroke, within days after
intervention (49). As many centers now rely mainly on the carotid US findings before
intervention, identification of calcification may guide towards better patient risk
stratification.
An attempt has been made to evaluate the accuracy of US in detecting plaque
calcification by quantifying the total plaque echogenicity (148), however, because the
carotid plaques are very frequently heterogenic, this method proved unreliable. We
believe that our study is the first to demonstrate the US accuracy for calcification
detection, defined as hyperechoic spots that produce posterior shadowing. Also, our
findings show that non-detectable calcifications are of lower volumes and usually
dispersed throughout the plaque. US was highly accurate in identifying carotid plaque
calcification volume of at least 8mm3. However, this volume seems to be relatively
significant when compared with normal intima-media thickness, which in most cases is
<1mm thick but yet reliably quantifiable by US. The same imaging method failed in
some cases to detect calcification volume of less than 8mm3 with reliable accuracy. In
addition, we did not find any difference in calcification presence and volume between
symptomatic and asymptomatic patients. It has been shown that statin therapy increases
carotid plaque echogenicity (149) and also coronary artery calcification (150) and we

60
wished to assess this effect in our study. However, we have been limited to undergo such
comparison since, 87.3% of our patients were already using statin therapy, limiting us in
carrying out a reliable comparison between groups.
Clinical implication: Our finding showed that calcification volumes of at least 8mm3 are
accurately detectable by US, that could be taken as a validation of this method to decide
for CAS intervention, since only extensive plaque calcification that was correlated with
adverse events after carotid stenting. US seems not well suited for the detection of
smaller calcium deposits, although they might play a role in plaque vulnerability.
Although the method we used to determine US accuracy is subjective in nature, it
establishes a potential foundation for the future development of quantitative models,
which could guide towards improved identification of plaque characteristics as a step
towards achieving plaque stabilization through optimum treatment. Determining a grey
scale media (GSM) cut-off of the hyperechoic spots that do not produce shadow but
otherwise represent calcification could enable detection of earlier stages of calcification
and reduce the need for advanced CT examinations and the resultant radiation for
patients.
Study III
Findings: This study demonstrates that common carotid artery measures, IMT and IM-
GSM are associated with significant differences in the severity of the disease and
distribution of other arterial systems. It was only IM-GSM, but not IMT that was able to
differentiate between the numbers of arterial systems affected by atherosclerosis. It was
proportionally decreased with increasing number of diseased arterial systems, starting
from asymptomatic to more than one vascular system. The conventional measure of
subclinical atherosclerosis, IMT, was less sensitive in showing similar differences
between groups.
Data interpretation: In general, patients suffering from atherosclerosis in any system are
at increased risk for recurrent events in the same arterial system or even symptomatic

61
disease in another territory. This is explained by the systemic inflammatory nature of
atherosclerosis. Patients with previous stroke have been shown to be at high risk of
suffering recurrent strokes but even higher risk of suffering a future MI (1). Patients with
symptomatic disease in one vascular system have been reported to have a 25% risk for
developing MI, stroke or even vascular death compared to >40% in those with multi-
system arterial disease (1). Based on these data patients with multisite atherosclerosis can
be described as vulnerable in the view of the high risk they carry for vascular events. It
was in the light of our findings, that IMT showed differences only when comparing
patients with and without previous MI. On the other hand IM-GSM proved much more
sensitive in showing significantly progressive lower values as patients went from
asymptomatic to symptomatic single arterial system and finally to symptomatic multi-
system disease. In addition IM-GSM was significantly different in patients with previous
stroke and MI, compared to those without.
Conventional carotid IMT has been widely used in many studies attempting to identify
patients at increased risk for future vascular events. On the other hand, measurements of
the composition of arterial wall free of plaque (IM-GSM) were only attempted in few
cases. The association between IM-GSM and future vascular events has recently been
demonstrated, as it was shown to be associated with a three-fold greater risk of all-cause
mortality and an eight-fold greater risk of cardiovascular mortality (122). Recently it has
been demonstrated that IMT represents an adaptive thickening of the arterial wall more
than real atherosclerosis pathology (16). It was confirmed that age and hypertension are
the dominant risk factors for increased IMT whereas low values of IM-GSM related to
low levels of HDL-C and increased level of CRP (151). Furthermore, it has been
suggested that IM-GSM could add incremental valued over and above IMT for patients
risk stratification, since they both were related to different plaque features in the distal
segments of the carotid artery (ICA and bifurcation) (59).
Clinical implication: The ability of the IM-GSM to differentiate between patients with
and without previous ischemic events suggests that it could also identify asymptomatic
patients at higher risk. Identifying such patients should warrant aggressive medical
management of modifiable risk factors in an attempt to reduce/prevent vascular events.

62
However our findings could find clinical implication once they are reproduced
prospectively and the reproducibility of the technique is confirmed in a number of
studies.
Study IV
Findings: Our analysis shows that atherosclerotic plaque echogenicity evaluated by
carotid ultrasound accurately predicts the development of CV symptoms in asymptomatic
and symptomatic patients. This prediction was preserved for all degrees of stenosis.
Data interpretation:
Asymptomatic patients
Although a small benefit of CEA was observed in asymptomatic carotid stenosis,
advances in medical therapies and the well-documented fall in stroke rates in such
patients over the last decade questioned the need of surgical treatment in these group of
patients (50, 52, 53, 152). However, there is a subgroup of high-risk asymptomatic
patients, which could benefit from CEA, and identification of such patients could have an
important clinical impact. The analysis we undertook in this study provides a strong
evidence for the additional value of plaque echogenicity in identifying asymptomatic
patients at higher risk of future CV events. To strengthen the argument further, such
accuracy for predicting future events, based on plaque echogenicity, stood firm even after
analyzing separately different categories of carotid artery stenosis, although
asymptomatic patients with severe stenosis again seem to be at a higher risk.
A higher association between plaque echolucency and future CV events was found
among studies that started patients’ recruitment and US data collection from 2000 and
thereafter, studies that defined plaques as PT 1 and 2 and when computer assisted
analysis was used to evaluate plaque echogenicity. Accordingly, more advanced US
devices and computer-assisted analysis of plaque echogenicity could help better
recognition of plaque echolucency and consequently, better prediction of future ischemic
events. Even if the cost-benefit of these findings is ignored, the clinical benefit to
patients cannot be over emphasized if our findings are implemented, particularly in
asymptomatic patients with severe stenosis. However, carotid plaque echogenicity

63
quantification is not real life analysis since it needs special software and expertise. It is
also an operator dependent technique with some potential technical difficulties in some
patients.
Symptomatic patients
Several large clinical randomized trials demonstrated a significant surgical benefit for
symptomatic patients, over and above medical treatment, particularly in those with 70-
99% stenosis (17, 153). However, there is a subgroup of patients with lower degree of
stenosis who carry a high risk of stroke recurrence. Although, our analysis showed that
plaque echogenicity analysis could predict recurrent ischemic events in symptomatic
patients with moderate to severe stenosis, the small number of studies and differences in
the follow-up periods between them limits us in providing a strong conclusion. A high
rate of stroke recurrence even within the first 72 hours of symptoms and within the
following two weeks has recently been reported (98). More studies are needed to confirm
the association between plaque echolucency and recurrent events in the early hours/days
after initial which could indicate a need for an emergency CEA in order to prevent
another stroke, as has been suggested (101).
Clinical implications: Quantification of carotid plaque echogenicity is a technique with
great potential in daily clinical service, which may result in better patient stratification
according to potential development of disease related complications. Such approach may
guide towards identifying high-risk patients with asymptomatic stenosis as well as
symptomatics with moderate stenosis and implement treatment strategy. Based on our
results plaque echolucency in asymptomatic patients, particularly in those with severe
stenosis, should be taken as a sign for vulnerability that supports the need for surgical
intervention.

64
LIMITATIONS
Study I
The small number of patients, particularly the asymptomatic and the retrospective nature
of the study are the most important limitations. When comparing different groups, the
small number of patients may carry the risk of false negative. In addition, lack of detailed
information for atherosclerosis burden in other arterial systems and lack of body mass
index data is another limitation. The images used for the analysis were slightly clouded,
however, applying standard image despeckle-filtering prior to the image analysis
minimized the noise (154). In general, the little noise that remained in the images for the
final analysis might influence the value of entropy and weaken its potential to
differentiate between groups.
Study II
The evaluation of US positive and negative predictive value was not possible; because
almost all (98.9%) carotid plaques were calcified in CBCT. During CEA procedure there
might be small-calcified material not excised, but we have been working on the
assumption that the largest plaque with the largest calcium volume was removed and
assessed by CBCT. Furthermore, we cannot be sure that the calcification detected and
quantified by CBCT was the same hyperechogenic nodule seen by US, particularly in
cases with multiple calcifications, however, we made a further assumption that the nodule
with the largest volume was the same that caused the posterior shadowing. In addition,
our subgroup comparisons were weak, since the number of asymptomatic patients was
small compared with symptomatic patients.
Study III
This is a retrospective study with known limitations. We have compared the two carotid
artery wall measures with previous symptoms in different arterial systems, an information

65
that was acquired from patients’ medical records. Another limitation is the lack of
imaging plaque features in other vascular territories (coronary and lower extremity
arteries). Assessing plaque/IMT and GSM in other arterial system, particularly the ones
related to the developed events, would have been of great interest but were not possible
with the retrospective nature of the study. In addition, information on the duration of
individual risk factors that could have influenced the results was not available.
Study IV
A systematic review based on relevant key words might have missed important
publications, but two investigators blinded to each other’s means of search checked the
search. We used only publications in the English language; other relevant ones in
different languages might have been missed. Studies included in the meta-analysis were
of different designs and different definitions to determine plaque echolucency were used,
however we tried to overcome this by using the random effect meta-analysis. Another
limitation is the low number of studies included in the meta-analysis, particularly those
with symptomatic patients.

66
CONCLUSIONS
Study I
Symptomatic patients with carotid atherosclerosis seem to have profound features of
plaque vulnerability in the contralateral arteries as well. Carotid plaques of asymptomatic
patients were more stable compared to symptomatic and contralateral to symptomatic
side. These findings, support the concept of generalized atherosclerotic pathology rather
than incidental unilateral disease, suggest increased relative vulnerability of the
contralateral plaques in symptomatic carotid stenosis and hence emphasize the need for
more aggressive treatment for secondary atherosclerosis prevention.
Study II
Carotid US accurately detected carotid artery calcification volumes of at least 8mm3, but
it was less accurate in detecting smaller volume calcified plaques, with relatively high
false negativity. We didn’t find any difference in calcification presence or volume
between symptomatic and asymptomatic patients. Since calcification is a dynamic
process, finding a method that can quantify atherosclerotic calcification by avoiding
radiation could be of importance for longitudinal assessment of its progression and
effects on plaque stability.
Study III
Our results showed that IM-GSM but not conventional IMT to differentiate between
patients with multiple system atherosclerosis disease. Because it was confirmed that
patients with multisite atherosclerosis are at higher risk of ischemic events in future,
measurement of intima-media complex echogenicity (IM-GSM) seems to be a promising
method to identify high-risk patients.

67
Study IV
There is a clear association between carotid plaque echolucency and future CV events in
asymptomatic and symptomatic patients. These findings if implemented, should result in
better management of vulnerable patients as well as early recruitment of those requiring
surgical intervention, who else would have been considered wrongly stable. Before
implementing such strategy for selecting asymptomatic patients for surgical intervention,
current results need to be confirmed in randomized clinical trials testing isolated medical
treatment in echogenic plaque against medical treatment plus CEA in asymptomatic
patients with echolucent plaque.

68
Acknowledgement
Though only my name appears on the cover of this dissertation, a great many people have
contributed to its production. I owe my gratitude to all those people who have made this
dissertation possible.
First and foremost I express my sincerest gratitude to my supervisor Professor Michael
Henein. I have been amazingly fortunate to have an advisor who gave me the freedom to
explore on my own, and at the same time the guidance to recover when my steps faltered.
Michael taught me how to question thoughts and express ideas. His patience and support
helped me overcome many difficult situations and complete this dissertation. I hope that
one day I would become as good an advisor to my students as Michael has been to me.
My co-supervisor Professor Per Wester deserve a special thanks for his help, very
professional comments that always made important changes in my scientific work and for
scholarly devotion to my work during realizing the thesis. So many things I have learned
from him will be very helpful for my academic career and also will help me for proper
diagnosis and treatment of stroke patients.
I would like to thank very much Elias Johansson who provided me the opportunity to
use the clinical patients’ data he collected very carefully making my scientific work much
easier, and also for his insightful discussions that helped me to do the best with the data
analysis and also to widen my knowledge in the carotid stenosis field.
This thesis couldn’t be possible without the help of Professor Christer Grönlund, who
made special software that I have used in my studies and also for his fruitful comments in
all of my studies.
Particularly, I would like to acknowledge, Professor Gani Bajraktari for helping me
during my entire scientific journey that started the time I was a medical student and
continued throughout my entire doctoral studies. I hope for a lifelong collaboration with
my tireless professor.

69
I would like to thank all the co-authors for their constructive and helpful criticism during
designing, analyzing and writing the papers for this thesis.
Special thanks to Kerstin Rosenqvist, for making all administrative issues during my
studies very easy and for making me feel at the Umeå University like my second home.
I would like to give a heartfelt thank to my grandfather Isak, my grandmother Taibe, my
parents Bedri and Shqipe and to my brothers Haki and Dardan. I am sure that I would
not have been able to complete this work without their help, encouragement, patience,
love and devotion for my work and myself.
And finally to my wife, Pranvera, for encouraging me to begin this scientific journey,
for being always by my side and help me to achieve what we intended, and to my
daughter Elena for her existence.

70
References
1. Jashari F, Ibrahimi P, Nicoll R, Bajraktari G, Wester P, Henein MY. Coronary
and carotid atherosclerosis: similarities and differences. Atherosclerosis.
2013;227(2):193-200.
2. Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, et al.
Heart disease and stroke statistics--2012 update: a report from the American Heart
Association. Circulation. 2012;125(1):e2-e220.
3. Svendsen A. The current status of cardiovascular disease in Canada--a call to
action. Canadian journal of cardiovascular nursing = Journal canadien en soins infirmiers
cardio-vasculaires. 2004;14(1):5-7.
4. Woollard KJ, Geissmann F. Monocytes in atherosclerosis: subsets and functions.
Nature reviews Cardiology. 2010;7(2):77-86.
5. Libby P, Ridker PM, Hansson GK, Leducq Transatlantic Network on A.
Inflammation in atherosclerosis: from pathophysiology to practice. Journal of the
American College of Cardiology. 2009;54(23):2129-38.
6. Virmani R, Kolodgie FD, Burke AP, Farb A, Schwartz SM. Lessons from sudden
coronary death: a comprehensive morphological classification scheme for atherosclerotic
lesions. Arteriosclerosis, thrombosis, and vascular biology. 2000;20(5):1262-75.
7. Bentzon JF, Otsuka F, Virmani R, Falk E. Mechanisms of plaque formation and
rupture. Circulation research. 2014;114(12):1852-66.
8. Badimon L, Vilahur G. Thrombosis formation on atherosclerotic lesions and
plaque rupture. J Intern Med. 2014;276(6):618-32.
9. Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, et al.
Executive summary: heart disease and stroke statistics--2014 update: a report from the
American Heart Association. Circulation. 2014;129(3):399-410.
10. Donnan GA, Fisher M, Macleod M, Davis SM. Stroke. Lancet.
2008;371(9624):1612-23.
11. de Weerd M, Greving JP, Hedblad B, Lorenz MW, Mathiesen EB, O'Leary DH,
et al. Prevalence of asymptomatic carotid artery stenosis in the general population: an
individual participant data meta-analysis. Stroke; a journal of cerebral circulation.
2010;41(6):1294-7.

71
12. Mathiesen EB, Joakimsen O, Bonaa KH. Prevalence of and risk factors associated
with carotid artery stenosis: the Tromso Study. Cerebrovascular diseases. 2001;12(1):44-
51.
13. Fine-Edelstein JS, Wolf PA, O'Leary DH, Poehlman H, Belanger AJ, Kase CS, et
al. Precursors of extracranial carotid atherosclerosis in the Framingham Study.
Neurology. 1994;44(6):1046-50.
14. Davies KN HP. Do carotid bruits predict disease of the internal carotid arteries?
Postgraduate Medical Journal. 1994;70(824):433-5.
15. Garoff M, Johansson E, Ahlqvist J, Jaghagen EL, Arnerlov C, Wester P.
Detection of calcifications in panoramic radiographs in patients with carotid stenoses
>/=50%. Oral surgery, oral medicine, oral pathology and oral radiology.
2014;117(3):385-91.
16. Ibrahimi P, Jashari F, Nicoll R, Bajraktari G, Wester P, Henein MY. Coronary
and carotid atherosclerosis: how useful is the imaging? Atherosclerosis. 2013;231(2):323-
33.
17. North American Symptomatic Carotid Endarterectomy Trial C. Beneficial effect
of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. The
New England journal of medicine. 1991;325(7):445-53.
18. Randomised trial of endarterectomy for recently symptomatic carotid stenosis:
final results of the MRC European Carotid Surgery Trial (ECST). Lancet.
1998;351(9113):1379-87.
19. Saba L, Mallarini G. A comparison between NASCET and ECST methods in the
study of carotids: evaluation using Multi-Detector-Row CT angiography. European
journal of radiology. 2010;76(1):42-7.
20. Rothwell PM, Eliasziw M, Gutnikov SA, Fox AJ, Taylor DW, Mayberg MR, et
al. Analysis of pooled data from the randomised controlled trials of endarterectomy for
symptomatic carotid stenosis. Lancet. 2003;361(9352):107-16.
21. Toepker M, Mahabadi AA, Heinzle G, Hofmann W, Mathies R, Schuster A, et al.
Accuracy of MDCT in the determination of supraaortic artery stenosis using DSA as the
reference standard. European journal of radiology. 2011;80(3):e351-5.

72
22. Koelemay MJ, Nederkoorn PJ, Reitsma JB, Majoie CB. Systematic review of
computed tomographic angiography for assessment of carotid artery disease. Stroke; a
journal of cerebral circulation. 2004;35(10):2306-12.
23. Oates CP, Naylor AR, Hartshorne T, Charles SM, Fail T, Humphries K, et al.
Joint recommendations for reporting carotid ultrasound investigations in the United
Kingdom. European journal of vascular and endovascular surgery : the official journal of
the European Society for Vascular Surgery. 2009;37(3):251-61.
24. Thapar A, Jenkins IH, Mehta A, Davies AH. Diagnosis and management of
carotid atherosclerosis. Bmj. 2013;346:f1485.
25. Chappell FM, Wardlaw JM, Young GR, Gillard JH, Roditi GH, Yip B, et al.
Carotid artery stenosis: accuracy of noninvasive tests--individual patient data meta-
analysis. Radiology. 2009;251(2):493-502.
26. Menke J. Diagnostic accuracy of contrast-enhanced MR angiography in severe
carotid stenosis: meta-analysis with metaregression of different techniques. European
radiology. 2009;19(9):2204-16.
27. Saba L, Anzidei M, Marincola BC, Piga M, Raz E, Bassareo PP, et al. Imaging of
the carotid artery vulnerable plaque. Cardiovascular and interventional radiology.
2014;37(3):572-85.
28. Eliasziw M, Streifler JY, Fox AJ, Hachinski VC, Ferguson GG, Barnett HJ.
Significance of plaque ulceration in symptomatic patients with high-grade carotid
stenosis. North American Symptomatic Carotid Endarterectomy Trial. Stroke; a journal
of cerebral circulation. 1994;25(2):304-8.
29. Saba L, Caddeo G, Sanfilippo R, Montisci R, Mallarini G. Efficacy and
sensitivity of axial scans and different reconstruction methods in the study of the
ulcerated carotid plaque using multidetector-row CT angiography: comparison with
surgical results. AJNR American journal of neuroradiology. 2007;28(4):716-23.
30. van den Oord SC, Akkus Z, Renaud G, Bosch JG, van der Steen AF, Sijbrands
EJ, et al. Assessment of carotid atherosclerosis, intraplaque neovascularization, and
plaque ulceration using quantitative contrast-enhanced ultrasound in asymptomatic
patients with diabetes mellitus. European heart journal cardiovascular Imaging.
2014;15(11):1213-8.

73
31. Heliopoulos J, Vadikolias K, Piperidou C, Mitsias P. Detection of carotid artery
plaque ulceration using 3-dimensional ultrasound. Journal of neuroimaging : official
journal of the American Society of Neuroimaging. 2011;21(2):126-31.
32. Kiechl S, Willeit J. The natural course of atherosclerosis. Part I: incidence and
progression. Arteriosclerosis, thrombosis, and vascular biology. 1999;19(6):1484-90.
33. Kiechl S, Willeit J. The natural course of atherosclerosis. Part II: vascular
remodeling. Bruneck Study Group. Arteriosclerosis, thrombosis, and vascular biology.
1999;19(6):1491-8.
34. de Weert TT, Ouhlous M, Meijering E, Zondervan PE, Hendriks JM, van
Sambeek MR, et al. In vivo characterization and quantification of atherosclerotic carotid
plaque components with multidetector computed tomography and histopathological
correlation. Arteriosclerosis, thrombosis, and vascular biology. 2006;26(10):2366-72.
35. Altaf N, Daniels L, Morgan PS, Auer D, MacSweeney ST, Moody AR, et al.
Detection of intraplaque hemorrhage by magnetic resonance imaging in symptomatic
patients with mild to moderate carotid stenosis predicts recurrent neurological events.
Journal of vascular surgery. 2008;47(2):337-42.
36. den Hartog AG, Bovens SM, Koning W, Hendrikse J, Luijten PR, Moll FL, et al.
Current status of clinical magnetic resonance imaging for plaque characterisation in
patients with carotid artery stenosis. European journal of vascular and endovascular
surgery : the official journal of the European Society for Vascular Surgery. 2013;45(1):7-
21.
37. Geroulakos G RG, Nicolaides A, James K, Labropoulos N, Belcaro G, Holloway
M. Characterization of symptomatic and asymptomatic carotid plaques using high-
resolution real-time ultrasonography. Br J Surg. 1993;80(10):1274-7.
38. Pedro LM, Pedro MM, Goncalves I, Carneiro TF, Balsinha C, Fernandes e
Fernandes R, et al. Computer-assisted carotid plaque analysis: characteristics of plaques
associated with cerebrovascular symptoms and cerebral infarction. European journal of
vascular and endovascular surgery : the official journal of the European Society for
Vascular Surgery. 2000;19(2):118-23.
39. Kakkos SK, Griffin MB, Nicolaides AN, Kyriacou E, Sabetai MM, Tegos T, et al.
The size of juxtaluminal hypoechoic area in ultrasound images of asymptomatic carotid

74
plaques predicts the occurrence of stroke. Journal of vascular surgery. 2013;57(3):609-18
e1; discussion 17-8.
40. Soloperto G, Casciaro S. Progress in atherosclerotic plaque imaging. World
journal of radiology. 2012;4(8):353-71.
41. Hatsukami TS, Ross R, Polissar NL, Yuan C. Visualization of fibrous cap
thickness and rupture in human atherosclerotic carotid plaque in vivo with high-
resolution magnetic resonance imaging. Circulation. 2000;102(9):959-64.
42. Kunte H, Schmidt C, Harms L, Ruckert RI, Grigoryev M, Fischer T. Contrast-
enhanced ultrasound and detection of carotid plaque neovascularization. Neurology.
2012;79(20):2081.
43. Adla T, Adlova R. Multimodality Imaging of Carotid Stenosis. The International
journal of angiology : official publication of the International College of Angiology, Inc.
2015;24(3):179-84.
44. Staub D, Partovi S, Schinkel AF, Coll B, Uthoff H, Aschwanden M, et al.
Correlation of carotid artery atherosclerotic lesion echogenicity and severity at standard
US with intraplaque neovascularization detected at contrast-enhanced US. Radiology.
2011;258(2):618-26.
45. Huang H, Virmani R, Younis H, Burke AP, Kamm RD, Lee RT. The impact of
calcification on the biomechanical stability of atherosclerotic plaques. Circulation.
2001;103(8):1051-6.
46. Nandalur KR, Baskurt E, Hagspiel KD, Finch M, Phillips CD, Bollampally SR, et
al. Carotid artery calcification on CT may independently predict stroke risk. AJR
American journal of roentgenology. 2006;186(2):547-52.
47. Kwee RM. Systematic review on the association between calcification in carotid
plaques and clinical ischemic symptoms. Journal of vascular surgery. 2010;51(4):1015-
25.
48. Ababneh B, Rejjal L, Pokharel Y, Nambi V, Wang X, Tung CH, et al.
Distribution of calcification in carotid endarterectomy tissues: comparison of micro-
computed tomography imaging with histology. Vascular medicine. 2014;19(5):343-50.
49. Setacci C, Chisci E, Setacci F, Iacoponi F, de Donato G, Rossi A. Siena carotid
artery stenting score: a risk modelling study for individual patients. Stroke; a journal of
cerebral circulation. 2010;41(6):1259-65.

75
50. Abbott AL. Medical (nonsurgical) intervention alone is now best for prevention of
stroke associated with asymptomatic severe carotid stenosis: results of a systematic
review and analysis. Stroke; a journal of cerebral circulation. 2009;40(10):e573-83.
51. Marquardt L, Geraghty OC, Mehta Z, Rothwell PM. Low risk of ipsilateral stroke
in patients with asymptomatic carotid stenosis on best medical treatment: a prospective,
population-based study. Stroke; a journal of cerebral circulation. 2010;41(1):e11-7.
52. Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee
for the Asymptomatic Carotid Atherosclerosis Study. Jama. 1995;273(18):1421-8.
53. Halliday A MA, Marro J, Peto C, Peto R, Potter J, Thomas D, MRC
Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Prevention of
disabling and fatal strokes by successful carotid endarterectomy in patients without recent
neurological symptoms: randomised controlled trial. Lancet. 2004;363(9420):1491-502.
54. Barnett HJ, Meldrum HE, Eliasziw M, North American Symptomatic Carotid
Endarterectomy Trial c. The appropriate use of carotid endarterectomy. CMAJ :
Canadian Medical Association journal = journal de l'Association medicale canadienne.
2002;166(9):1169-79.
55. Naylor AR. Time to rethink management strategies in asymptomatic carotid
artery disease. Nature reviews Cardiology. 2012;9(2):116-24.
56. Naylor AR, Schroeder TV, Sillesen H. Clinical and imaging features associated
with an increased risk of late stroke in patients with asymptomatic carotid disease.
European journal of vascular and endovascular surgery : the official journal of the
European Society for Vascular Surgery. 2014;48(6):633-40.
57. Nicolaides AN, Kakkos SK, Griffin M, Sabetai M, Dhanjil S, Tegos T, et al.
Severity of asymptomatic carotid stenosis and risk of ipsilateral hemispheric ischaemic
events: results from the ACSRS study. European journal of vascular and endovascular
surgery : the official journal of the European Society for Vascular Surgery.
2005;30(3):275-84.
58. Bogiatzi C, Cocker MS, Beanlands R, Spence JD. Identifying high-risk
asymptomatic carotid stenosis. Expert opinion on medical diagnostics. 2012;6(2):139-51.
59. Ibrahimi P, Jashari F, Johansson E, Gronlund C, Bajraktari G, Wester P, et al.
Common carotid intima-media features determine distal disease phenotype and

76
vulnerability in asymptomatic patients. International journal of cardiology. 2015;196:22-
8.
60. Kakkos SK, Sabetai M, Tegos T, Stevens J, Thomas D, Griffin M, et al. Silent
embolic infarcts on computed tomography brain scans and risk of ipsilateral hemispheric
events in patients with asymptomatic internal carotid artery stenosis. Journal of vascular
surgery. 2009;49(4):902-9.
61. Halliday A, Harrison M, Hayter E, Kong X, Mansfield A, Marro J, et al. 10-year
stroke prevention after successful carotid endarterectomy for asymptomatic stenosis
(ACST-1): a multicentre randomised trial. Lancet. 2010;376(9746):1074-84.
62. Steg PG, Bhatt DL, Wilson PW, D'Agostino R, Sr., Ohman EM, Rother J, et al.
One-year cardiovascular event rates in outpatients with atherothrombosis. Jama.
2007;297(11):1197-206.
63. European Stroke O, Tendera M, Aboyans V, Bartelink ML, Baumgartner I,
Clement D, et al. ESC Guidelines on the diagnosis and treatment of peripheral artery
diseases: Document covering atherosclerotic disease of extracranial carotid and vertebral,
mesenteric, renal, upper and lower extremity arteries: the Task Force on the Diagnosis
and Treatment of Peripheral Artery Diseases of the European Society of Cardiology
(ESC). European heart journal. 2011;32(22):2851-906.
64. Dormandy JA, Rutherford RB. Management of peripheral arterial disease (PAD).
TASC Working Group. TransAtlantic Inter-Society Consensus (TASC). Journal of
vascular surgery. 2000;31(1 Pt 2):S1-S296.
65. Price JF, Mowbray PI, Lee AJ, Rumley A, Lowe GD, Fowkes FG. Relationship
between smoking and cardiovascular risk factors in the development of peripheral arterial
disease and coronary artery disease: Edinburgh Artery Study. European heart journal.
1999;20(5):344-53.
66. Sabeti S, Schlager O, Exner M, Mlekusch W, Amighi J, Dick P, et al. Progression
of carotid stenosis detected by duplex ultrasonography predicts adverse outcomes in
cardiovascular high-risk patients. Stroke; a journal of cerebral circulation.
2007;38(11):2887-94.
67. Ringelstein EB, Droste DW, Babikian VL, Evans DH, Grosset DG, Kaps M, et al.
Consensus on microembolus detection by TCD. International Consensus Group on
Microembolus Detection. Stroke; a journal of cerebral circulation. 1998;29(3):725-9.
77
68. Markus HS, King A, Shipley M, Topakian R, Cullinane M, Reihill S, et al.
Asymptomatic embolisation for prediction of stroke in the Asymptomatic Carotid Emboli
Study (ACES): a prospective observational study. The Lancet Neurology. 2010;9(7):663-
71.
69. Spence JD, Tamayo A, Lownie SP, Ng WP, Ferguson GG. Absence of
microemboli on transcranial Doppler identifies low-risk patients with asymptomatic
carotid stenosis. Stroke; a journal of cerebral circulation. 2005;36(11):2373-8.
70. Spence JD, Coates V, Li H, Tamayo A, Munoz C, Hackam DG, et al. Effects of
intensive medical therapy on microemboli and cardiovascular risk in asymptomatic
carotid stenosis. Archives of neurology. 2010;67(2):180-6.
71. Momjian-Mayor I, Burkhard P, Murith N, Mugnai D, Yilmaz H, Narata AP, et al.
Diagnosis of and treatment for symptomatic carotid stenosis: an updated review. Acta
neurologica Scandinavica. 2012;126(5):293-305.
72. Paraskevas KI, Mikhailidis DP, Moore WS, Veith FJ. Optimal contemporary
management of symptomatic and asymptomatic carotid artery stenosis. Vascular.
2011;19(3):117-20.
73. Naylor AR, Sillesen H, Schroeder TV. Clinical and imaging features associated
with an increased risk of early and late stroke in patients with symptomatic carotid
disease. European journal of vascular and endovascular surgery : the official journal of
the European Society for Vascular Surgery. 2015;49(5):513-23.
74. De Schryver EL, Algra A, van Gijn J. Dipyridamole for preventing stroke and
other vascular events in patients with vascular disease. The Cochrane database of
systematic reviews. 2007(3):CD001820.
75. Sacco RL, Diener HC, Yusuf S, Cotton D, Ounpuu S, Lawton WA, et al. Aspirin
and extended-release dipyridamole versus clopidogrel for recurrent stroke. The New
England journal of medicine. 2008;359(12):1238-51.
76. Antithrombotic Trialists C, Baigent C, Blackwell L, Collins R, Emberson J,
Godwin J, et al. Aspirin in the primary and secondary prevention of vascular disease:
collaborative meta-analysis of individual participant data from randomised trials. Lancet.
2009;373(9678):1849-60.

78
77. Hennekens CH, Sechenova O, Hollar D, Serebruany VL. Dose of aspirin in the
treatment and prevention of cardiovascular disease: current and future directions. Journal
of cardiovascular pharmacology and therapeutics. 2006;11(3):170-6.
78. Markus HS, Droste DW, Kaps M, Larrue V, Lees KR, Siebler M, et al. Dual
antiplatelet therapy with clopidogrel and aspirin in symptomatic carotid stenosis
evaluated using doppler embolic signal detection: the Clopidogrel and Aspirin for
Reduction of Emboli in Symptomatic Carotid Stenosis (CARESS) trial. Circulation.
2005;111(17):2233-40.
79. Wang Y, Johnston SC, Investigators C. Rationale and design of a randomized,
double-blind trial comparing the effects of a 3-month clopidogrel-aspirin regimen versus
aspirin alone for the treatment of high-risk patients with acute nondisabling
cerebrovascular event. American heart journal. 2010;160(3):380-6 e1.
80. Makris GC, Lavida A, Nicolaides AN, Geroulakos G. The effect of statins on
carotid plaque morphology: a LDL-associated action or one more pleiotropic effect of
statins? Atherosclerosis. 2010;213(1):8-20.
81. Kennedy J, Quan H, Buchan AM, Ghali WA, Feasby TE. Statins are associated
with better outcomes after carotid endarterectomy in symptomatic patients. Stroke; a
journal of cerebral circulation. 2005;36(10):2072-6.
82. McGirt MJ, Perler BA, Brooke BS, Woodworth GF, Coon A, Jain S, et al. 3-
hydroxy-3-methylglutaryl coenzyme A reductase inhibitors reduce the risk of
perioperative stroke and mortality after carotid endarterectomy. Journal of vascular
surgery. 2005;42(5):829-36; discussion 36-7.
83. Goldstein LB, Amarenco P, Zivin J, Messig M, Altafullah I, Callahan A, et al.
Statin treatment and stroke outcome in the Stroke Prevention by Aggressive Reduction in
Cholesterol Levels (SPARCL) trial. Stroke; a journal of cerebral circulation.
2009;40(11):3526-31.
84. Fox AJ, Eliasziw M, Rothwell PM, Schmidt MH, Warlow CP, Barnett HJ.
Identification, prognosis, and management of patients with carotid artery near occlusion.
AJNR American journal of neuroradiology. 2005;26(8):2086-94.
85. Rothwell PM, Eliasziw M, Gutnikov SA, Warlow CP, Barnett HJ, Carotid
Endarterectomy Trialists C. Endarterectomy for symptomatic carotid stenosis in relation
to clinical subgroups and timing of surgery. Lancet. 2004;363(9413):915-24.

79
86. Hellings WE, Pasterkamp G, Verhoeven BA, De Kleijn DP, De Vries JP,
Seldenrijk KA, et al. Gender-associated differences in plaque phenotype of patients
undergoing carotid endarterectomy. Journal of vascular surgery. 2007;45(2):289-96;
discussion 96-7.
87. Ballotta E, Meneghetti G, Da Giau G, Manara R, Saladini M, Baracchini C.
Carotid endarterectomy within 2 weeks of minor ischemic stroke: a prospective study.
Journal of vascular surgery. 2008;48(3):595-600.
88. Brott TG, Hobson RW, 2nd, Howard G, Roubin GS, Clark WM, Brooks W, et al.
Stenting versus endarterectomy for treatment of carotid-artery stenosis. The New
England journal of medicine. 2010;363(1):11-23.
89. Yavin D, Roberts DJ, Tso M, Sutherland GR, Eliasziw M, Wong JH. Carotid
endarterectomy versus stenting: a meta-analysis of randomized trials. The Canadian
journal of neurological sciences Le journal canadien des sciences neurologiques.
2011;38(2):230-5.
90. Bain S, Moheet AM, Rasmussen P. Which patients benefit from carotid stenting?
What recent trials show. Cleveland Clinic journal of medicine. 2008;75(10):714-20.
91. Garg N, Karagiorgos N, Pisimisis GT, Sohal DP, Longo GM, Johanning JM, et al.
Cerebral protection devices reduce periprocedural strokes during carotid angioplasty and
stenting: a systematic review of the current literature. Journal of endovascular therapy :
an official journal of the International Society of Endovascular Specialists.
2009;16(4):412-27.
92. Biasi GM, Froio A, Diethrich EB, Deleo G, Galimberti S, Mingazzini P, et al.
Carotid plaque echolucency increases the risk of stroke in carotid stenting: the Imaging in
Carotid Angioplasty and Risk of Stroke (ICAROS) study. Circulation. 2004;110(6):756-
62.
93. Reiter M, Bucek RA, Effenberger I, Boltuch J, Lang W, Ahmadi R, et al. Plaque
echolucency is not associated with the risk of stroke in carotid stenting. Stroke; a journal
of cerebral circulation. 2006;37(9):2378-80.
94. Kitta Y, Obata JE, Takano H, Nakamura T, Kodama Y, Fujioka D, et al.
Echolucent carotid plaques predict in-stent restenosis after bare metal stenting in native
coronary arteries. Atherosclerosis. 2008;197(1):177-82.

80
95. Rosenkranz M, Wittkugel O, Waiblinger C, Thomalla G, Krutzelmann A,
Havemeister S, et al. Cerebral embolism during carotid artery stenting: role of carotid
plaque echolucency. Cerebrovascular diseases. 2009;27(5):443-9.
96. Giannakopoulos TG, Moulakakis K, Sfyroeras GS, Avgerinos ED, Antonopoulos
CN, Kakisis JD, et al. Association between plaque echogenicity and embolic material
captured in filter during protected carotid angioplasty and stenting. European journal of
vascular and endovascular surgery : the official journal of the European Society for
Vascular Surgery. 2012;43(6):627-31.
97. Marnane M, Prendeville S, McDonnell C, Noone I, Barry M, Crowe M, et al.
Plaque inflammation and unstable morphology are associated with early stroke
recurrence in symptomatic carotid stenosis. Stroke; a journal of cerebral circulation.
2014;45(3):801-6.
98. Ois A, Cuadrado-Godia E, Rodriguez-Campello A, Jimenez-Conde J, Roquer J.
High risk of early neurological recurrence in symptomatic carotid stenosis. Stroke; a
journal of cerebral circulation. 2009;40(8):2727-31.
99. Johnston SC, Rothwell PM, Nguyen-Huynh MN, Giles MF, Elkins JS, Bernstein
AL, et al. Validation and refinement of scores to predict very early stroke risk after
transient ischaemic attack. Lancet. 2007;369(9558):283-92.
100. Merwick A, Albers GW, Amarenco P, Arsava EM, Ay H, Calvet D, et al.
Addition of brain and carotid imaging to the ABCD(2) score to identify patients at early
risk of stroke after transient ischaemic attack: a multicentre observational study. The
Lancet Neurology. 2010;9(11):1060-9.
101. Salem MK SR, Bown MJ, West K, Moore D, Nicolaides A, Robinson TG, Naylor
AR. Patients with recurrent ischaemic events from carotid artery disease have a large
lipid core and low GSM. European journal of vascular and endovascular surgery : the
official journal of the European Society for Vascular Surgery. 2012;43(2):147-53.
102. Ritter MA, Dittrich R, Thoenissen N, Ringelstein EB, Nabavi DG. Prevalence and
prognostic impact of microembolic signals in arterial sources of embolism. A systematic
review of the literature. Journal of neurology. 2008;255(7):953-61.
103. Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, Fayad ZA, et al.
2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic
adults: a report of the American College of Cardiology Foundation/American Heart

81
Association Task Force on Practice Guidelines. Journal of the American College of
Cardiology. 2010;56(25):e50-103.
104. Den Ruijter HM, Peters SA, Anderson TJ, Britton AR, Dekker JM, Eijkemans
MJ, et al. Common carotid intima-media thickness measurements in cardiovascular risk
prediction: a meta-analysis. Jama. 2012;308(8):796-803.
105. Lorenz MW, Polak JF, Kavousi M, Mathiesen EB, Volzke H, Tuomainen TP, et
al. Carotid intima-media thickness progression to predict cardiovascular events in the
general population (the PROG-IMT collaborative project): a meta-analysis of individual
participant data. Lancet. 2012;379(9831):2053-62.
106. Naqvi TZ, Lee MS. Carotid intima-media thickness and plaque in cardiovascular
risk assessment. JACC Cardiovascular imaging. 2014;7(10):1025-38.
107. Jung M, Parrinello CM, Xue X, Mack WJ, Anastos K, Lazar JM, et al.
Echolucency of the carotid artery intima-media complex and intima-media thickness have
different cardiovascular risk factor relationships: the Women's Interagency HIV Study.
Journal of the American Heart Association. 2015;4(2).
108. Pignoli P, Tremoli E, Poli A, Oreste P, Paoletti R. Intimal plus medial thickness
of the arterial wall: a direct measurement with ultrasound imaging. Circulation.
1986;74(6):1399-406.
109. Wendelhag I, Gustavsson T, Suurkula M, Berglund G, Wikstrand J. Ultrasound
measurement of wall thickness in the carotid artery: fundamental principles and
description of a computerized analysing system. Clinical physiology. 1991;11(6):565-77.
110. Kanters SD, Algra A, van Leeuwen MS, Banga JD. Reproducibility of in vivo
carotid intima-media thickness measurements: a review. Stroke; a journal of cerebral
circulation. 1997;28(3):665-71.
111. Naqvi TZ, Mendoza F, Rafii F, Gransar H, Guerra M, Lepor N, et al. High
prevalence of ultrasound detected carotid atherosclerosis in subjects with low
Framingham risk score: potential implications for screening for subclinical
atherosclerosis. Journal of the American Society of Echocardiography : official
publication of the American Society of Echocardiography. 2010;23(8):809-15.
112. Price JF, Tzoulaki I, Lee AJ, Fowkes FG. Ankle brachial index and intima media
thickness predict cardiovascular events similarly and increased prediction when
combined. Journal of clinical epidemiology. 2007;60(10):1067-75.

82
113. Chambless LE, Heiss G, Folsom AR, Rosamond W, Szklo M, Sharrett AR, et al.
Association of coronary heart disease incidence with carotid arterial wall thickness and
major risk factors: the Atherosclerosis Risk in Communities (ARIC) Study, 1987-1993.
American journal of epidemiology. 1997;146(6):483-94.
114. Stein JH, Korcarz CE, Hurst RT, Lonn E, Kendall CB, Mohler ER, et al. Use of
carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular
disease risk: a consensus statement from the American Society of Echocardiography
Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular
Medicine. Journal of the American Society of Echocardiography : official publication of
the American Society of Echocardiography. 2008;21(2):93-111; quiz 89-90.
115. Salonen JT, Salonen R. Ultrasonographically assessed carotid morphology and
the risk of coronary heart disease. Arteriosclerosis and thrombosis : a journal of vascular
biology / American Heart Association. 1991;11(5):1245-9.
116. Lorenz MW, Schaefer C, Steinmetz H, Sitzer M. Is carotid intima media thickness
useful for individual prediction of cardiovascular risk? Ten-year results from the Carotid
Atherosclerosis Progression Study (CAPS). European heart journal. 2010;31(16):2041-8.
117. O'Leary DH, Polak JF, Kronmal RA, Kittner SJ, Bond MG, Wolfson SK, Jr., et
al. Distribution and correlates of sonographically detected carotid artery disease in the
Cardiovascular Health Study. The CHS Collaborative Research Group. Stroke; a journal
of cerebral circulation. 1992;23(12):1752-60.
118. Rosvall M, Janzon L, Berglund G, Engstrom G, Hedblad B. Incident coronary
events and case fatality in relation to common carotid intima-media thickness. J Intern
Med. 2005;257(5):430-7.
119. Bots ML, Hoes AW, Koudstaal PJ, Hofman A, Grobbee DE. Common carotid
intima-media thickness and risk of stroke and myocardial infarction: the Rotterdam
Study. Circulation. 1997;96(5):1432-7.
120. Yeboah J, McClelland RL, Polonsky TS, Burke GL, Sibley CT, O'Leary D, et al.
Comparison of novel risk markers for improvement in cardiovascular risk assessment in
intermediate-risk individuals. Jama. 2012;308(8):788-95.
121. Lau KK, Chan YH, Yiu KH, Tam S, Li SW, Lau CP, et al. Incremental predictive
value of vascular assessments combined with the Framingham Risk Score for prediction
83
of coronary events in subjects of low-intermediate risk. Postgrad Med J.
2008;84(989):153-7.
122. Wohlin M, Sundstrom J, Andren B, Larsson A, Lind L. An echolucent carotid
artery intima-media complex is a new and independent predictor of mortality in an
elderly male cohort. Atherosclerosis. 2009;205(2):486-91.
123. Shai I, Spence JD, Schwarzfuchs D, Henkin Y, Parraga G, Rudich A, et al.
Dietary intervention to reverse carotid atherosclerosis. Circulation. 2010;121(10):1200-8.
124. Hansen F, Bergqvist D, Lindblad B, Lindh M, Matzsch T, Lanne T. Accuracy of
duplex sonography before carotid endarterectomy--a comparison with angiography.
European journal of vascular and endovascular surgery : the official journal of the
European Society for Vascular Surgery. 1996;12(3):331-6.
125. Johansson EP, Arnerlov C, Wester P. Risk of recurrent stroke before carotid
endarterectomy: the ANSYSCAP study. International journal of stroke : official journal
of the International Stroke Society. 2013;8(4):220-7.
126. Touboul PJ, Hennerici MG, Meairs S, Adams H, Amarenco P, Bornstein N, et al.
Mannheim carotid intima-media thickness consensus (2004-2006). An update on behalf
of the Advisory Board of the 3rd and 4th Watching the Risk Symposium, 13th and 15th
European Stroke Conferences, Mannheim, Germany, 2004, and Brussels, Belgium, 2006.
Cerebrovascular diseases. 2007;23(1):75-80.
127. Polak JF, O'Leary DH, Kronmal RA, Wolfson SK, Bond MG, Tracy RP, et al.
Sonographic evaluation of carotid artery atherosclerosis in the elderly: relationship of
disease severity to stroke and transient ischemic attack. Radiology. 1993;188(2):363-70.
128. Geroulakos G, Ramaswami G, Nicolaides A, James K, Labropoulos N, Belcaro
G, et al. Characterization of symptomatic and asymptomatic carotid plaques using high-
resolution real-time ultrasonography. Br J Surg. 1993;80(10):1274-7.
129. Carra G, Visona A, Bonanome A, Lusiani L, Pesavento R, Bortolon M, et al.
Carotid plaque morphology and cerebrovascular events. International angiology : a
journal of the International Union of Angiology. 2003;22(3):284-9.
130. Mazzone AM, Urbani MP, Picano E, Paterni M, Borgatti E, De Fabritiis A, et al.
In vivo ultrasonic parametric imaging of carotid atherosclerotic plaque by
videodensitometric technique. Angiology. 1995;46(8):663-72.

84
131. Amadasun M KR. Texural Features Corresponding to Texural Properties. IEEE
Transactions on Systems, Man and Cybernetics. 1989;19(5):1264-74.
132. Christodoulou CI, Pattichis CS, Pantziaris M, Nicolaides A. Texture-based
classification of atherosclerotic carotid plaques. IEEE transactions on medical imaging.
2003;22(7):902-12.
133. Gepner AD, Keevil JG, Wyman RA, Korcarz CE, Aeschlimann SE, Busse KL, et
al. Use of carotid intima-media thickness and vascular age to modify cardiovascular risk
prediction. Journal of the American Society of Echocardiography : official publication of
the American Society of Echocardiography. 2006;19(9):1170-4.
134. Polak JF SL, O'Leary DH, Lefkowitz D, Price TR, Savage PJ, Brant WE, Reid C.
Hypoechoic plaque at US of the carotid artery: an independent risk factor for incident
stroke in adults aged 65 years or older. Cardiovascular Health Study. Radiology.
1998;208(3):649-54.
135. Mathiesen EB, Bonaa KH, Joakimsen O. Echolucent plaques are associated with
high risk of ischemic cerebrovascular events in carotid stenosis: the tromso study.
Circulation. 2001;103(17):2171-5.
136. Liapis CD, Kakisis JD, Kostakis AG. Carotid stenosis: factors affecting
symptomatology. Stroke; a journal of cerebral circulation. 2001;32(12):2782-6.
137. Gronholdt ML, Nordestgaard BG, Schroeder TV, Vorstrup S, Sillesen H.
Ultrasonic echolucent carotid plaques predict future strokes. Circulation. 2001;104(1):68-
73.
138. Nicolaides AN, Kakkos SK, Griffin M, Sabetai M, Dhanjil S, Thomas DJ, et al.
Effect of image normalization on carotid plaque classification and the risk of ipsilateral
hemispheric ischemic events: results from the asymptomatic carotid stenosis and risk of
stroke study. Vascular. 2005;13(4):211-21.
139. Hashimoto H, Tagaya M, Niki H, Etani H. Computer-assisted analysis of
heterogeneity on B-mode imaging predicts instability of asymptomatic carotid plaque.
Cerebrovascular diseases. 2009;28(4):357-64.
140. Topakian R, King A, Kwon SU, Schaafsma A, Shipley M, Markus HS, et al.
Ultrasonic plaque echolucency and emboli signals predict stroke in asymptomatic carotid
stenosis. Neurology. 2011;77(8):751-8.

85
141. Silvestrini M, Altamura C, Cerqua R, Pasqualetti P, Viticchi G, Provinciali L, et
al. Ultrasonographic markers of vascular risk in patients with asymptomatic carotid
stenosis. Journal of cerebral blood flow and metabolism : official journal of the
International Society of Cerebral Blood Flow and Metabolism. 2013;33(4):619-24.
142. Singh AS, Atam V, Jain N, Yathish BE, Patil MR, Das L. Association of carotid
plaque echogenicity with recurrence of ischemic stroke. North American journal of
medical sciences. 2013;5(6):371-6.
143. Kato K, Yonetsu T, Kim SJ, Xing L, Lee H, McNulty I, et al. Nonculprit plaques
in patients with acute coronary syndromes have more vulnerable features compared with
those with non-acute coronary syndromes: a 3-vessel optical coherence tomography
study. Circulation Cardiovascular imaging. 2012;5(4):433-40.
144. Baroncini LA PFA, Murta Junior LO, Martins AR, Ramos SG, Cherri J, Piccinato
CE. Ultrasonic tissue characterization of vulnerable carotid plaque: correlation between
videodensitometric method and histological examination. Cardiovascular Ultrasound.
2006;4(1):32.
145. Nicolaides AN, Kakkos SK, Kyriacou E, Griffin M, Sabetai M, Thomas DJ, et al.
Asymptomatic internal carotid artery stenosis and cerebrovascular risk stratification.
Journal of vascular surgery. 2010;52(6):1486-96 e1-5.
146. Griffin MB, Kyriacou E, Pattichis C, Bond D, Kakkos SK, Sabetai M, et al.
Juxtaluminal hypoechoic area in ultrasonic images of carotid plaques and hemispheric
symptoms. Journal of vascular surgery. 2010;52(1):69-76.
147. Miralles M, Merino J, Busto M, Perich X, Barranco C, Vidal-Barraquer F.
Quantification and characterization of carotid calcium with multi-detector CT-
angiography. European journal of vascular and endovascular surgery : the official journal
of the European Society for Vascular Surgery. 2006;32(5):561-7.
148. Denzel C, Lell M, Maak M, Hockl M, Balzer K, Muller KM, et al. Carotid artery
calcium: accuracy of a calcium score by computed tomography-an in vitro study with
comparison to sonography and histology. European journal of vascular and endovascular
surgery : the official journal of the European Society for Vascular Surgery.
2004;28(2):214-20.

86
149. Ibrahimi P, Jashari F, Bajraktari G, Wester P, Henein MY. Ultrasound assessment
of carotid plaque echogenicity response to statin therapy: a systematic review and meta-
analysis. International journal of molecular sciences. 2015;16(5):10734-47.
150. Henein M, Granasen G, Wiklund U, Schmermund A, Guerci A, Erbel R, et al.
High dose and long-term statin therapy accelerate coronary artery calcification.
International journal of cardiology. 2015;184:581-6.
151. Andersson J, Sundstrom J, Gustavsson T, Hulthe J, Elmgren A, Zilmer K, et al.
Echogenecity of the carotid intima-media complex is related to cardiovascular risk
factors, dyslipidemia, oxidative stress and inflammation: the Prospective Investigation of
the Vasculature in Uppsala Seniors (PIVUS) study. Atherosclerosis. 2009;204(2):612-8.
152. Raman G, Moorthy D, Hadar N, Dahabreh IJ, O'Donnell TF, Thaler DE, et al.
Management strategies for asymptomatic carotid stenosis: a systematic review and meta-
analysis. Annals of internal medicine. 2013;158(9):676-85.
153. Barnett HJ, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes RB, et al.
Benefit of carotid endarterectomy in patients with symptomatic moderate or severe
stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. The
New England journal of medicine. 1998;339(20):1415-25.
154. Loizou CP, Pattichis CS, Christodoulou CI, Istepanian RS, Pantziaris M,
Nicolaides A. Comparative evaluation of despeckle filtering in ultrasound imaging of the
carotid artery. IEEE transactions on ultrasonics, ferroelectrics, and frequency control.
2005;52(10):1653-69.