cacoub p hcv ehm & inflam pr cacoub du 15 01 15 (1)
TRANSCRIPT

HCV and its Extra Hepatic Manifestations: From Immune- to Inflammatory-Related
Manifestations
Pr Patrice CACOUBDept of Internal Medicine and Clinical Immunology
CNRS UMR 7087
Université Pierre et Marie Curie
Centre Référence Maladies Auto-immunes
Hôpital La Pitié-Salpêtrière, Paris, FRANCE
PC01

Disclosures
• Dr P. Cacoub has received consulting and lecturing fees from : Abbvie, Astra
Zeneca, Bristol-Myers Squibb, Gilead, Glaxo Smith Kline, Janssen, Merck
Sharp Dohme, Roche, Servier, Vifor.
• Dr P. Cacoub is an inventor of a patent application owned by his academic
institution and licensed to ILTOO pharma, a biotechnology company
developing low dose IL-2 in autoimmune diseases, in which in holds shares.
• Dr P. Cacoub has received grants from : CNRS , INSERM , Université Pierre et
Marie Curie, ANRS
PC02

Let’s vote
Do you think that extrahepatic manifestations are a major problem in chronic HCV infection?
1. Yes
2. No
PC03

Let’s vote
Which category of extra-hepatic manifestations of HCV represents the major problem?
1. Auto-immune manifestations
2. Fatigue, depression and cognitive impairment
3. Cardiovascular events
4. Insulin resistance and type 2 diabetes
5. I don’t consider any of the above to be a major problem
PC04

35
30
25
20
15
10
5
0
Chronic HCV Infection Increases Mortality from both Hepatic and Extra Hepatic Diseases
*P<0.001 for comparison among all 3 groups and P<0.001 for HCV RNA
detectable vs. undetectable. †P<0.001 for comparison among all 3 groups and
P=0.002 for HCV RNA detectable vs. undetectableLee MH, et al. J Infect Dis 2012;206:469–77
Follow-up
(Years)
20
18
16
14
12
10
2
0
8
6
4
Follow-up
(Years)
12
10
8
6
4
2
0
All causes(n=2,394)
Liver cancer(n=115)
Extrahepatic diseases(n=2,199)
Cu
mu
lati
ve
mo
rtali
ty (
%)
Follow-up
(Years)
30.1%*
12.8%
12.4%
10.4%*
1.6%
0.3%
19.8%†
12.2%
11.0%
Anti-HCV+, HCV RNA detectable Anti-HCV+, HCV RNA undetectable Anti-HCV-
0 2 4 6 8 10 12 14 16 18 20 0 2 4 6 8 10 12 14 16 18 20 0 2 4 6 8 10 12 14 16 18 20
PC05
• 23 820 adults, Taiwan
• 1095 anti-HCV positive
• 760 (69%) HCV-RNA detectable
HCV+, RNA+
HCV+, RNA-
HCV-

35
30
25
20
15
10
5
0
Chronic HCV Infection Increases Mortality from both Hepatic and Extra Hepatic Diseases
*P<0.001 for comparison among all 3 groups and P<0.001 for HCV RNA detectable vs.
undetectable. †P<0.001 for comparison among all 3 groups and P=0.002 for HCV RNA
detectable vs. undetectable
Follow-up
(Years)
20
18
16
14
12
10
2
0
8
6
4
Follow-up
(Years)
12
10
8
6
4
2
0
All causes(n=2,394)
Liver cancer(n=115)
Extrahepatic diseases(n=2,199)
Follow-up
(Years)
30.1%*
12.8%
12.4%
10.4%*
1.6%
0.3%
19.8%†
12.2%
11.0%
0 2 4 6 8 10 12 14 16 18 20 0 2 4 6 8 10 12 14 16 18 20 0 2 4 6 8 10 12 14 16 18 20
PC05
Lee MH, et al. J Infect Dis 2012;206:469–77
HCV+, RNA+
HCV+, RNA-
HCV-
Cu
mu
lati
ve
mo
rta
lity
(%
)

Chronic HCV Infection Increases Mortality from both Hepatic and Extra Hepatic Diseases
*P<0.001 for comparison among all 3 groups and P<0.001 for HCV RNA detectable
vs. undetectable. †P<0.001 for comparison among all 3 groups and P=0.002 for
HCV RNA detectable vs. undetectable
Follow-up
(Years)
20
18
16
14
12
10
2
0
8
6
4
Extrahepatic diseases
(n=2,199)
Cu
mu
lati
ve
mo
rta
lity
(%
)
19.8%†
12.2%
11.0%
0 2 4 6 8 10 12 14 16 18 20
PC05
Lee MH, et al. J Infect Dis 2012;206:469–77
HCV+, RNA+
HCV+, RNA-
HCV-

Chronic HCV Infection Increases Mortality from both Hepatic and Extra Hepatic Diseases
Compared with anti-HCV negative individuals, anti-HCV positive individuals had higher mortality
Higher mortality in individuals with detectable HCV RNA vs. those with undetectable HCV RNA
CI: confidence interval Lee MH, et al. J Infect Dis 2012;206:469–77
Hazard ratio [95% CI]
All causes 1.89 [1.66–2.15]
Hepatic diseases
Extrahepatic diseases
Circulatory diseases
Nephritis, nephrotic syndrome
Esophageal cancer
Prostate cancer
Thyroid cancer
12.48 [9.34–16.66]
1.35 [1.15–1.57]
1.50 [1.10–2.03]
2.77 [1.49–5.15]
4.08 [1.38–12.08]
4.19 [1.18–14.94]
8.22 [1.36–49.66]
PC05a

HEPATITIS C VIRUS:A WORLD-WIDE
INFECTION…
…and A BODY-WIDE DISEASE
2.35% (160 million) chronically infected
PC06
Lavanchy D. Clin Microbiol Infect 2011;17:107–115
Hepatitis C global prevalence 2010 (%)1

Auto-immune manifestations
PC07

HCV Chronic Infection: More than One Target Cell
1. Choo GL, et al. Science 1989;21;244:359–62.; 2. Zignego AL, et al.
J Hepatol 1992;15:382–6.; 3. Ferri C, et al. Blood. 1993;82:3701–4
• Hepatitis • Cirrhosis• Hepatocarcinoma
• Cryoglobulinaemia• Auto-Ab• B-NHL
Hepatocyte1 Lymphocyte2,3
PC08

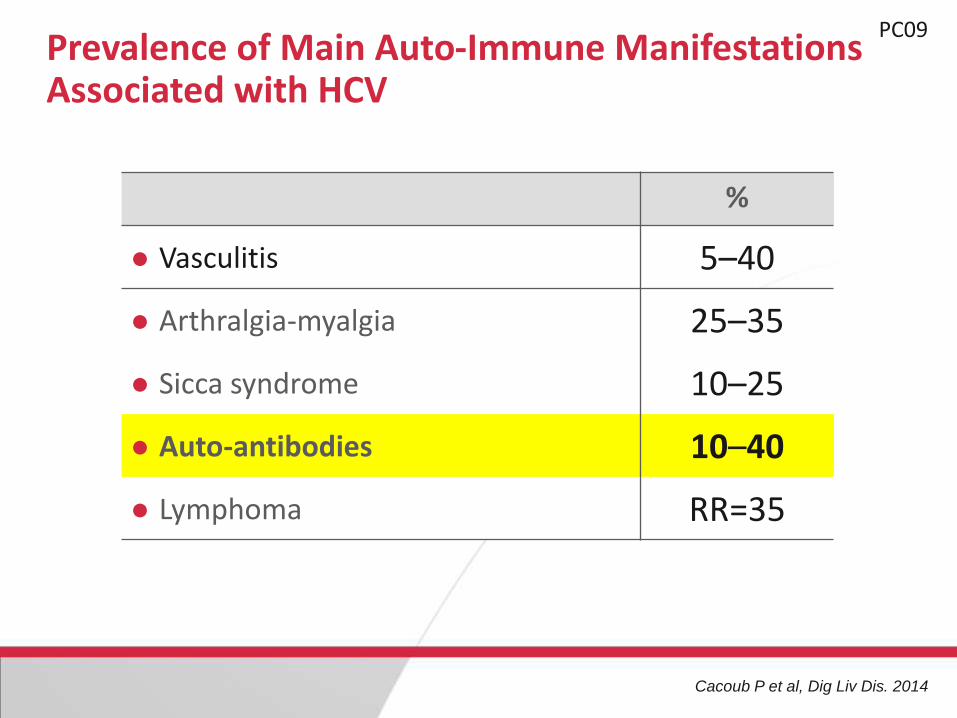
Prevalence of Main Auto-Immune Manifestations Associated with HCV
Cacoub P et al, Dig Liv Dis. 2014
%
Vasculitis 5–40
Arthralgia-myalgia 25–35
Sicca syndrome 10–25
Auto-antibodies 10–40
Lymphoma RR=35
PC09

Skin Purpura
MembranoproliferativeGlomerulonephritis
Neuropathy
Cryoglobulinaemia vasculitis
CNS Vasculitis
PC10
Jacobson IM et al, Clin Gastroenterol Hepatol. 2010 Dec;8(12):1017-29.
14
Rationale for
Rituximab treatment
in cryoglobulinemic
vasculitis
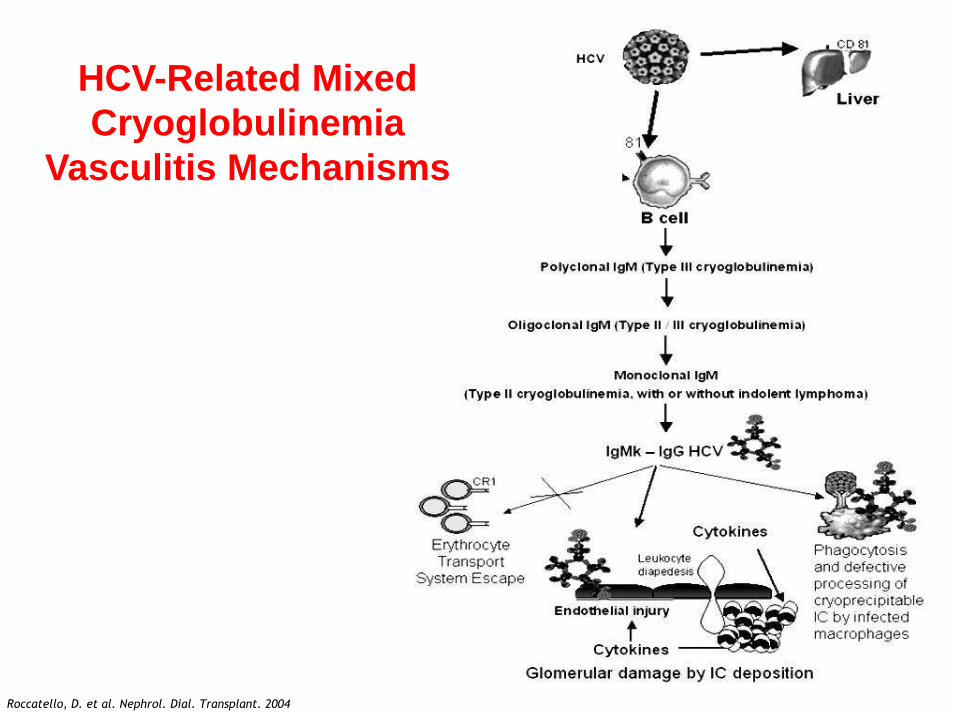
Rocatello D, Nephrol Dial Transplant, 2004Roccatello, D. et al. Nephrol. Dial. Transplant. 2004
HCV-Related Mixed
Cryoglobulinemia
Vasculitis Mechanisms

15
Age at disease onset (yrs) 54 ± 13 (29-72)
Female/Male ratio 3
Purpura 98%
Weakness 98%
Arthralgias 91%
Arthritis (non-erosive) 8%
Raynaud's phenomenon 32%
Sicca syndrome 51%
Peripheral neuropathy 81%
Renal involvement 31%
Features of Mixed Cryoglobulinemia Vasculitis
n=250 patients Ferri C, Mascia MT, Saadoun D, Cacoub P. 2009

16
Age at disease onset (yrs) 54 ± 13 (29-72)
Female/Male ratio 3
Purpura 98%
Weakness 98%
Arthralgias 91%
Arthritis (non-erosive) 8%
Raynaud's phenomenon 32%
Sicca syndrome 51%
Peripheral neuropathy 81%
Renal involvement 31%
B-cell non-Hodgkin's lymphoma 11%
Hepatocellular carcinoma 3%
Features of Mixed Cryoglobulinemia Vasculitis
n=250 patients Ferri C, Mascia MT, Saadoun D, Cacoub P. 2009
RR=34

17
Antigen-Insensitive
B Cell Proliferation
Oligo/Monoclonal
proliferation
Uncontrolled
proliferation
Antigen-Sensitive
B Cell Proliferation
Polyclonal
proliferation
B-cell lymphoma
Cytokines
BAFF
HyperglobulinemiaCryoglobulinemia
Vasculitis
B-cell lymphoma
IgH-bcl2? Other
oncogenic
events ?
CD81
HCV (E2)
B cell
Anti-E2 IgM/Rheumatoid factorIgG
HCV-Related Lymphoproliferative Disorders:
from Cryoglobulinemia to B-NHL
Treg deficit

Chronic HCV infection
Poly- oligoclonal B-cell expansion
AutoantibodiesRF - IC
Mixed cryoglobulins
Cryoglobulinaemic vasculitis
Monoclonal B-cellproliferation
Overt lymphoma
HCV eradication
Immunosuppressors
Chemotherapy
Plasma exchange
Steroids
PC14Strategies to Treat Auto-Immune Manifestations
IC: immune complexes; RF: rheumatoid factor Cacoub P et al, Dig Liv Dis. 2014

Zuckerman, J Rheumatol 2000. Naarendorp, J Rheumatol 2001. Cacoub, Arthritis Rheum 2002, Zaja F, Blood 2003. Sansonno D, Blood 2003 , Cacoub, Arthritis Rheum 2005, Saadoun,
Arthritis Rheum 2007; Saadoun, D et al , Ann Rheum Dis 2014
Non virological
response
Sustained virological
response
Clinical Remission in HCV-Cryoglobulinemia
Vasculitis Correlates with Virological Response
Prevalence of Main Auto-Immune Manifestations Associated with HCV
Cacoub P et al, Dig Liv Dis. 2014
%
Vasculitis 5–40
Arthralgia-myalgia 25–35
Sicca syndrome 10–25
Auto-antibodies 10–40
Lymphoma RR=35
PC09

Auto-antibody production in chronic HCV infection.
0
10
20
30
40
50
60
70
%
A-nuclear
A-phospholipid
A-thyroglobulin
A-smooth muscle
≥ one auto-Ab
≥ three auto-Ab
Pawlotsky JM, Hepatology 1994. Pawlotsky JM, Ann Intern Med 1994. Prieto J, Hepatology 1996. Cacoub P, J Rheumatol 1997. Cacoub P, Medicine 2000.

Extrahepatic manifestations associated with HCV infection.
(Prospective study in 321 HCV patients)
Autoantibody Number %
-----------------------------------------------------------------------------
Antinuclear 124 41
A-nucleosome 6 2
A-DNA 8 3
A-histone 9 3
A-ENA 10 3
Cacoub P et al. Medicine 2000

HCV & Health Related Quality of Life
Fatigue, depressionand cognitive impairment
PC16

HCV Infection, Fatigue and Depression
Fatigue
prevalence ranges from 50 to 67%
independently predicts poor HRQoL
Depression
documented in 28% of HCV patients prior to HCV therapy (DSM-IV).
predictive of HRQoL during HCV therapy with pegIFN/ribavirin.
HCV may directly affect the CNS:
through alterations in serotonergic and dopaminergicneurotransmission with resultant depressive symptoms.

Fatigue, Depression and ExtrahepaticManifestations (EM) in HCV patients
Poynard T, et al. J Viral Hepatitis 2002;9:295–303
% of patientsn=1614
% of controlsn=412
Fatigue without depression 48 0.7 Fatigue with depression 5 0
Depression without fatigue 2 0
No fatigue and no depression 45 99.3
TOTAL 100 100
Fatigue without EM 19 0.5
Fatigue with EM 35 0.2
EM without fatigue 21 3.4
No fatigue and no EM 25 96
TOTAL 100 100
Fatigue without depression 48 0.7
PC17

Fatigue, Depression and ExtrahepaticManifestations (EM) in HCV patients
Poynard T, et al. J Viral Hepatitis 2002;9:295–303
% of patientsn=1614
% of controlsn=412
Fatigue without depression 48 0.7 Fatigue with depression 5 0
Depression without fatigue 2 0
No fatigue and no depression 45 99.3
TOTAL 100 100
Fatigue without EM 19 0.5
Fatigue with EM 35 0.2
EM without fatigue 21 3.4
No fatigue and no EM 25 96
TOTAL 100 100
PC18

Baseline 18 months18 months vs
baseline
Non treated (n=72)
No fatigue
Moderate
Severe
39%35%26%
42%39%19%
P=0.74
Sustained responders (n=82)
No fatigue
Moderate
Severe
41%37%22%
69%24%7%
P<0.001
Non responders (n=224)
No fatigue
Moderate
Severe
40%42%18%
46%40%14%
P=0.18
PC19Decreased Fatigue Rate in HCV Patients with Sustained Response to IFN-RBV
IFN: interferon; RBV: ribavirin Cacoub P, et al. J Hepatol. 2002 Jun;36(6):812-8
Rates of moderate/severe fatigue decreased from 59% to 31% after SVR
FACIT-F: No SVR
0.55
0.65
0.75
0 4 8 12 16 20
Week
24 28
FACIT-F: SVR
FACIT-F: AllNo
rmal
ized
FA
CIT
-F
FACIT-F Scores During and Post-Treatment in FUSION
FACIT-F: No SVR
0.65
0.75
0 4 8 12 16 20
Week
24 28
FACIT-F: SVR
FACIT-F: AllNo
rmal
ized
FA
CIT
-F
FACIT-F Scores During and Post-Treatment in NEUTRINO
0.55
**
*
†
†
†
*
†
†
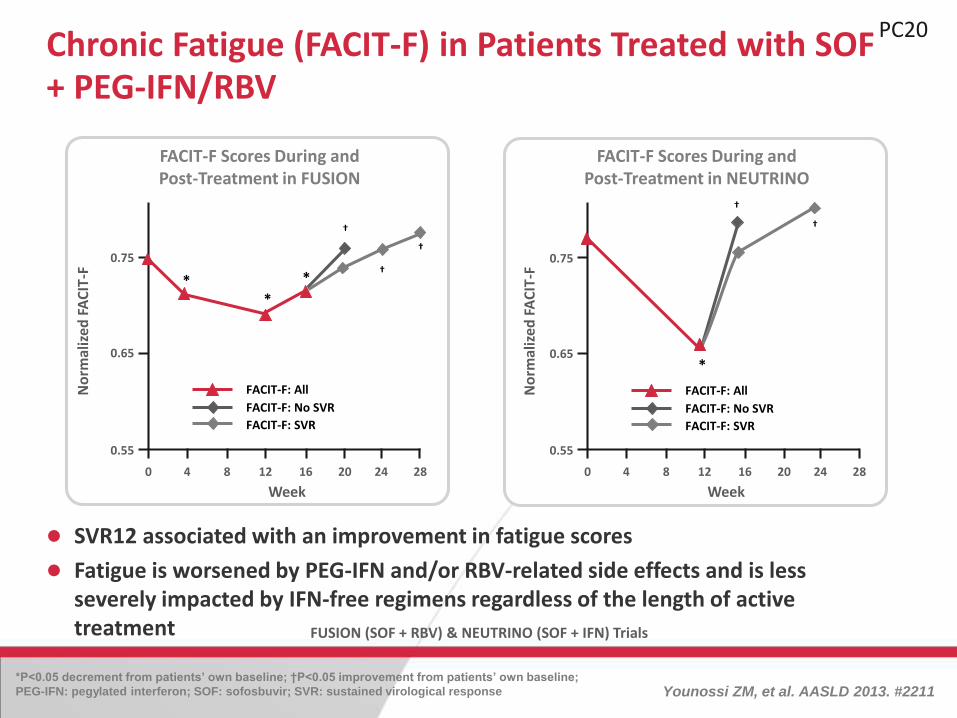
FUSION (SOF + RBV) & NEUTRINO (SOF + IFN) Trials
Chronic Fatigue (FACIT-F) in Patients Treated with SOF + PEG-IFN/RBV
SVR12 associated with an improvement in fatigue scores
Fatigue is worsened by PEG-IFN and/or RBV-related side effects and is less severely impacted by IFN-free regimens regardless of the length of active treatment
*P<0.05 decrement from patients’ own baseline; †P<0.05 improvement from patients’ own baseline;
PEG-IFN: pegylated interferon; SOF: sofosbuvir; SVR: sustained virological response Younossi ZM, et al. AASLD 2013. #2211
PC20

Actigraphy Parameters in HCV patientsActive at Night, Sleepy All Day !
Heeren M, et al. J Hepatol 2014;60:732–40
Monday 18.04.20
11
Tuesday 19.04.20
11Wednesd
ay 20.04.20
11Thursday 21.04.20
11
Friday 22.04.20
11
PC21

Cerebral MR Signal in HCV patients and Spectral Analysis
MR: magnetic resonance Byrnes V, et al. J Hepatol 2012;56:549–56
A
C
B
PC22

T1 vs. T3 in SVR; p<0.05
MR Signal in Basal Ganglia Myo-inositol/Creatininein HCV Patients According to Virological Response
Byrnes V, et al. J Hepatol 2012;56:549–56
Baseline (T1), week 12 t2), and for treatment candidates, 12 weeks post treatment with PEG-IFN and ribavirin (T3)
PC23
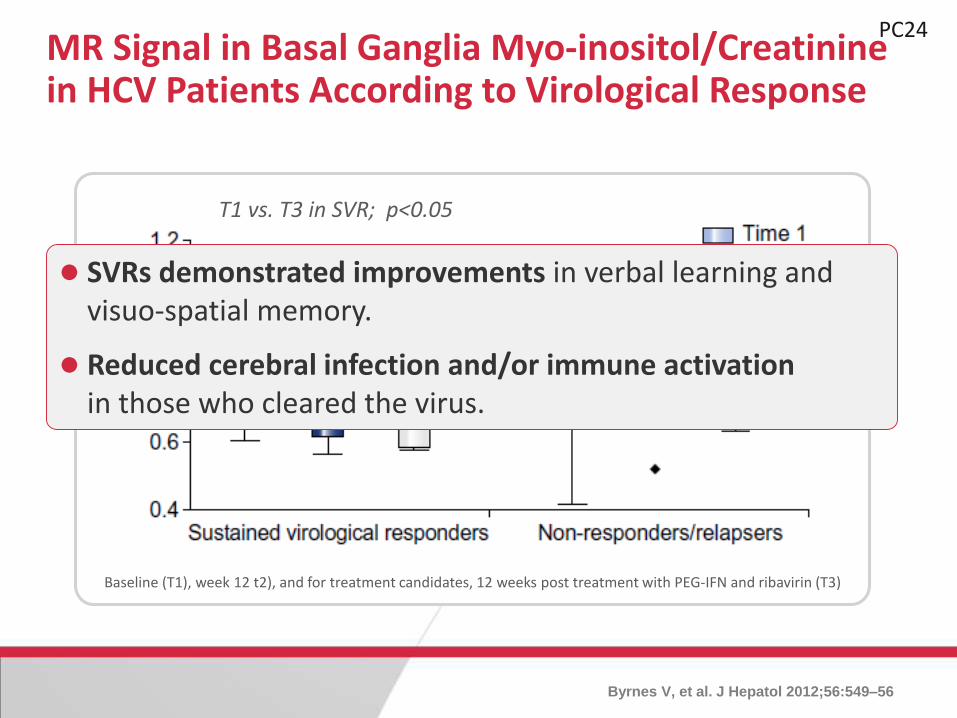
T1 vs. T3 in SVR; p<0.05
MR Signal in Basal Ganglia Myo-inositol/Creatininein HCV Patients According to Virological Response
Byrnes V, et al. J Hepatol 2012;56:549–56
Baseline (T1), week 12 t2), and for treatment candidates, 12 weeks post treatment with PEG-IFN and ribavirin (T3)
SVRs demonstrated improvements in verbal learning and visuo-spatial memory.
Reduced cerebral infection and/or immune activation in those who cleared the virus.
PC24

Chronic HCV infection : a new cardio-vascular risk
factor ?
PC25

Cumulative Incidence of End Stage Renal Disease three Diabetic Study Cohorts (death adjusted as a competing risk event)
Hsu YC et al, Hepatology, 2014 Apr;59(4):1293-302.
HCV+ non treated
HCV+ treated
Non HCV

Cumulative Incidence of Stroke in three Diabetic Study Cohorts (death adjusted as a competing risk event)
HCV+ non treated
HCV+ treated
Non HCV
Hsu YC et al, Hepatology, 2014 Apr;59(4):1293-302.

Risk Factors Associated with the Presence of Carotid Plaques in Geno1 HCV patients
Petta S, et al. Hepatology 2012;55:1317–23
P=0.008
N=21 CHCAge ≤55 yrs
F3-4
N=67 CHCAge ≤55 yrs
F0-2
N=43 CHCAge >55 yrs
F3-4
N=43 CHCAge >55 yrs
F0-2
P=0.51
Car
oti
dea
lPla
qu
es (
%)
00
20
80
60
40
100
PC29

IBT, interferon based therapy
Interferon-Based Therapy and Stroke-Free Survival in HCV patients
Hsu CS, et al. APT 2013;38:415–23
Log-rank test,p = 0.003
Stro
ke-f
ree
surv
ival
rat
e
0.80
0.85
0.95
0.90
100
0 1 2 3 4 5
Time (years)
Non-IBT
IBT
IFN-based therapy was associated with a 61% decreased riskof stroke in HCV patients, after adjusting for knownprognostic factors.
PC30

Studies assessing the association between HCV infection and ischemic cerebrovascular accident.
Domont F & Cacoub P, 2014
References, year Type of study Country HCV+ (n) HCV- (n)
Studies showing an association
Lee et al. (22), 2010 Prospective cohort Taiwan 1307 22,358
Liao et al. (24), 2012 Population Taiwan 4094 16,376
Hsu et al. (26), 2013 Retrospective cohort Taiwan 2875 12,450
Adinolfi et al. (23), 2013 Retrospective cohort Italy 79 741
Studies NOT showing an association
Younossi et al. (25), 2013 Retrospective
population
USA 173 19,568

References, year Type of study Country HCV + (n) HCV- (n)
Studies showing an association between HCV infection and carotid atherosclerosis
Ishizaka et al. (10), 2002 Population Japan 104 4784
Ishizaka et al. (11), 2003 Population Japan 25 1967
Tomiyawa et al. (12), 2003 Cohort Japan 87 7427
Fukui et al. (37), 2003 Cohort Japan 31 179
Boddi et al. (14), 2007 Cohort Italy 31 120
Targher et al. (15), 2007 Cohort Italy 60 60
Butt et al. (28), 2009 Observational USA 82,083 89,562
Mostafa et al. (16), 2010 Cohort Egypt 329 795
Petta et al. (38), 2012 Cross-over Italy 174 174
Adinolfi et al. (23) , 2013 Cohort Italy 326 477
Studies NOT showing an association between HCV infection and carotid atherosclerosis
Bilora et al. (19), 2008 Cohort Italy 40 40
Caliskan et al. (18), 2009 Cohort Turkey 36 36
Tien et al. (39), 2009 Cohort USA 273 1502
Masia et al. (40) , 2011 Cohort Spain 63 138

Myocardial Injury in HCV patients
BNP, brain natriuretic peptide; CPK: creatinine phosphokinase; HAI, histology activity index; HANP, human
atrial natriuretic peptide; LDH: lactate dehydrogenase; LVDd, left ventricular end diastolic dimension Maruyama S, et al. J Hepatol 2012;58:11–5
Characteristics Chronic hepatitis C (n = 217) Normal range
Age (yr) 57 + 9Sex 104/113
Liver function
Bilirubin (mg/dl) 0.7 + 0.3 0.2 - 1.0ALT (IU/L) 77 + 61 5 - 45Y-globulin (g/dl) 1.6 + 0.3 0.7- 1.2Prothrombin percent activity (%) 90 + 16 80 - 100IGC disappearance rate 0.172 + 0.041 0.158 - 0.232HAI score (point) 8.9 + 3.3
Cardiac function
Abnormal ECG (%) 9CPK (IU/L) 94 + 46 30 - 190LDH (IU/L) 172 + 38 107 - 230BNP (pg/ml) 22 + 18.8 Less than 18.4HANP (pg/ml) 19.6 + 12.5 Less than 43LVDd (mm) 48 + 5 39 - 55Ejection fraction (%) 66 + 7 55 - 80Severity score (point) 4.3 + 1.6 Less than 3Severity score > 3 (%) 87
Cardiac function HCV patients normal range
Abnormal ECG (%) 9
CPK (IU/L) 94 + 46 30 - 190
LDH (IU/L) 172 + 38 107 - 230
BNP (pg/ml) 22 + 18.8 Less than 18.4
HANP (pg/ml) 19.6 + 12.5 Less than 43
LVDd (mm) 48 + 5 39 - 55
Ejection fraction (%) 66 + 7 55 - 80
Severity score (point) 4.3 + 1.6 Less than 3
Severity score > 3 (%) 87
PC31

SVR
Before IFN therapy (M0; A), at the completion of IFN therapy (M6; B) and 6 months after the completion of IFN therapy (M12; C). The arrows show the regions of myocardial perfusion defects.
Myocardial SPECT Images in HCV Patients According to Virological Response
SPECT: single-photon emission computed tomography Maruyama S, et al. J Hepatol 2012;58:11–5
PC32
Before therapy
End of therapy
6 months after therapy

SVR Relapse
Myocardial SPECT Images in HCV Patients According to Virological Response
SPECT: single-photon emission computed tomography Maruyama S, et al. J Hepatol 2012;58:11–5
PC33
Before therapy
End of therapy
6 months after therapy
Before therapy
End of therapy
6 months after therapy
Before IFN therapy (M0; A), at the completion of IFN therapy (M6; B) and 6 months after the completion of IFN therapy (M12; C). The arrows show the regions of myocardial perfusion defects.

SVR Relapse Non Response
Myocardial SPECT Images in HCV Patients According to Virological Response
Maruyama S, et al. J Hepatol 2012;58:11–5
PC34
Before therapy
End of therapy
6 months after therapy
Before therapy
End of therapy
6 months after therapy
Before therapy
End of therapy
6 months after therapy
Before IFN therapy (M0; A), at the completion of IFN therapy (M6; B) and 6 months after the completion of IFN therapy (M12; C). The arrows show the regions of myocardial perfusion defects.

IFN
SVR group(n=30)
Relapse group(n=9)
NVR group(n=6)
Severity Score of Myocardial Perfusion Defects in HCV Patients After 48 weeks PEG-IFN/RBV
RBV: ribavirin; NVR: non-virological response Maruyama S, et al. J Hepatol 2012;58:11–5
PC35

IFN
SVR group(n=30)
Relapse group(n=9)
NVR group(n=6)
Severity Score of Myocardial Perfusion Defects in HCV Patients After 48 weeks PEG-IFN/RBV
RBV: ribavirin; NVR: non-virological response Maruyama S, et al. J Hepatol 2012;58:11–5
PC35

IFN
SVR group(n=30)
Relapse group(n=9)
NVR group(n=6)
Severity Score of Myocardial Perfusion Defects in HCV Patients After 48 weeks PEG-IFN/RBV
RBV: ribavirin; NVR: non-virological response Maruyama S, et al. J Hepatol 2012;58:11–5
PC35

Main studies assessing the association between HCV infection and ischemic heart disease.
References, year Type of study Country HCV+ (n) HCV- (n)
Studies showing an association
Vassalle et al. (9), 2004 Cross-over Italy 491 195
Völzke et al. (41), 2004 Transversal Germany 21 4033
Butt et al. (28), 2009 Cross-over USA 60 60
Tsui et al. (27), 2009 Cohort USA 84 -
Ramdeen et al. (41), 2010 Cohort USA 78 -
Studies NOT showing an association
Butt et al. (32), 2007 Cohort USA 126,926 126,926
Domont F & Cacoub P, 2014

HCV, Insulin-Resistanceand Type 2 Diabetes
Mellitus (T2DM)
PC36

PC37

PC38

PC39

ALT: alanine aminotransferase; AST: aspartate
aminotransferase; Arase Y, et al. Hepatology 2009;49:739–44
N 2.842
Body mass index 23.3 + 3.2
Staging (non LC/LC) 2.649/193
Efficacy of treatment (SVR/non-SVR) 1.175/1.667
PC41Type 2 Diabetes in HCV Patients Treated with IFN
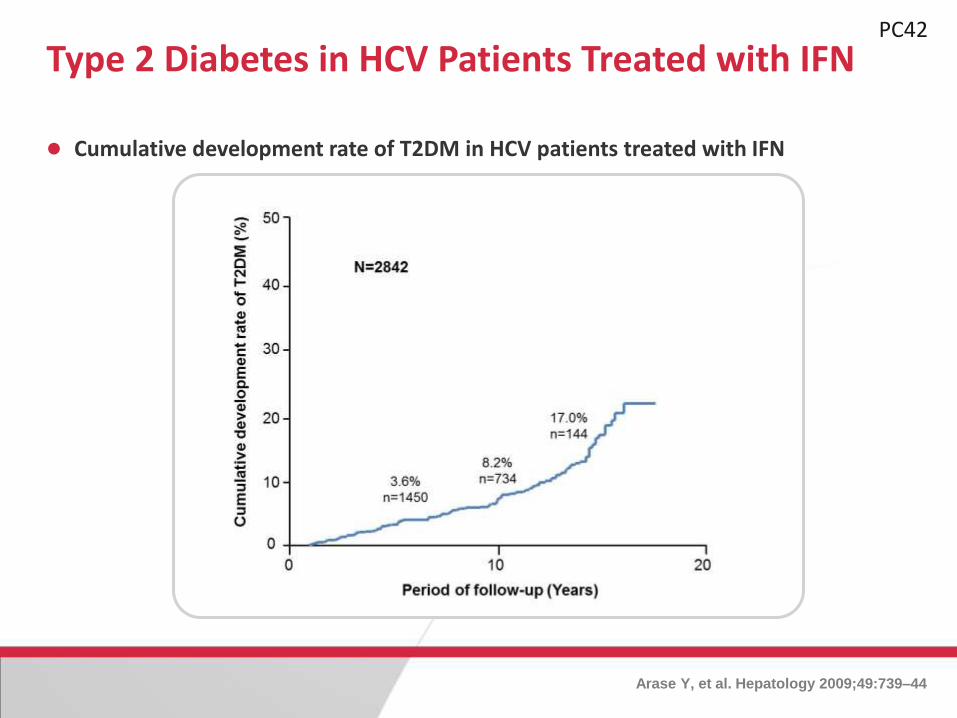
Type 2 Diabetes in HCV Patients Treated with IFN
Cumulative development rate of T2DM in HCV patients treated with IFN
Arase Y, et al. Hepatology 2009;49:739–44
PC42

Predictive factors for Type 2 Diabetes Development in HCV Patients Treated with IFN
Arase Y, et al. Hepatology 2009;49:739–44
Histological diagnosis (LC/non-LC) 4.03 (2.55 - 6.36) <0.0001 3.30 (2.06 - 5.28) <0.001
Efficacy (non-SVR/SVR) 2.73 (1.77 - 4.20) <0.0001 2.78 (1.75 - 4.41) <0.001
PC44

Age >50 yrs
Cumulative Development Rate of T2DM in HCV Patients with or without SVR after IFN
Arase Y, et al. Hepatology 2009;49:739–44
Cirrhotics
PC43
Extrahepatic Manifestations of HCV infectionSummary (1)
Chronic HCV infection increases mortality from both hepatic and extra hepatic diseases.
Extra-hepatic immunologic manifestations include vasculitis, lymphomas, and rheumatologic conditions.
Chronic HCV is associated with reduced health-related quality of life, in which depression, cognitive impairment and fatigue may be factors.
PC45

Increased risk of major cardiovascular events, chronic kidney disease and glucose related disorders require attention.
Healthcare costs imposed by these conditions must be considered in addition to those normally associated with chronic HCV infection.
Extrahepatic Manifestations of HCV infectionSummary (2)
PC46