c ollaborative hi v p aediatric s tudy ( chips )
DESCRIPTION
Older and wiser: continued improvements in clinical outcome and highly active antiretroviral therapy (HAART) response in HIV-infected children in the UK and Ireland, 1996-2005. C ollaborative HI V P aediatric S tudy ( CHIPS ) - PowerPoint PPT PresentationTRANSCRIPT

Older and wiser: continued improvements in clinical outcome and highly active
antiretroviral therapy (HAART) response in HIV-infected children in the UK and Ireland,
1996-2005
Collaborative HIV Paediatric Study (CHIPS)
A Judd, T Duong, KJ Lee, AS Walker, PA Tookey, M Sharland,A Riordan, H Lyall, J Masters, E Menson, G Tudor-Williams,
K Butler, S Donaghy, V Novelli, C Peckham, DM Gibb

Introduction to CHIPS & NSHPC
• Surveillance of obstetric and paediatric HIV in the UK and Ireland is carried out through the National Study of HIV in Pregnancy and Childhood (NSHPC)
• CHIPS is a multicentre cohort study of HIV infected children under care in 39 hospitals in the UK & Ireland since 1996 90% children currently in NSHPC are also in CHIPS
– detailed annual follow up questionnaires
• For those not in CHIPS, NSHPC collects limited annual follow up data

Aim
• Describe changes over time in demographics, morbidity and mortality, and exposure and response to HAART
• HIV infected children in the UK & Ireland• 1996 - 2005

Methods
• HAART exposure and response data are for CHIPS children only (n=1065). All other analyses include all diagnosed children (n=1439)
• Logistic regression to explore 12 month viral load and CD4% responses to HAART in ART naïve children
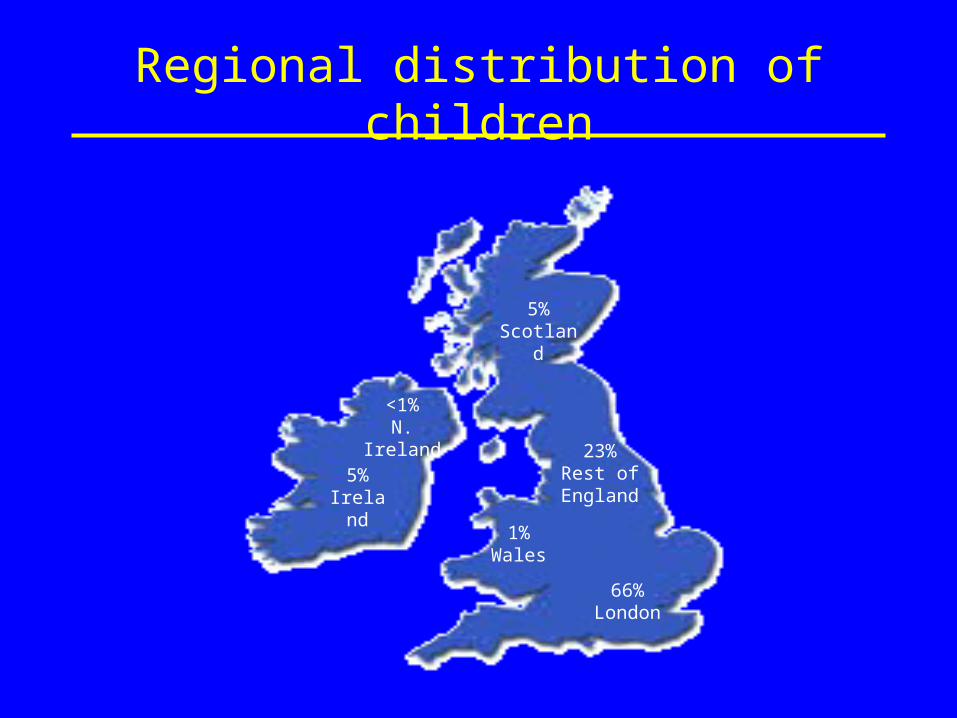
Regional distribution of children
5%Ireland
1%Wales
66%London
23%Rest of England
5% Scotland
<1%N. Ireland

Sociodemographics
Sex: How child was identified:
Female 50% Prospectively 13%
Before AIDS 68%
Ethnicity: AIDS diagnosis 19%
Black African 72%
White 13% Source of infection:
Other 16% Vertical 94%
Blood transfusion 3%
% born abroad: Other 3%
Early 1990s ~30%
2000+ ~65%
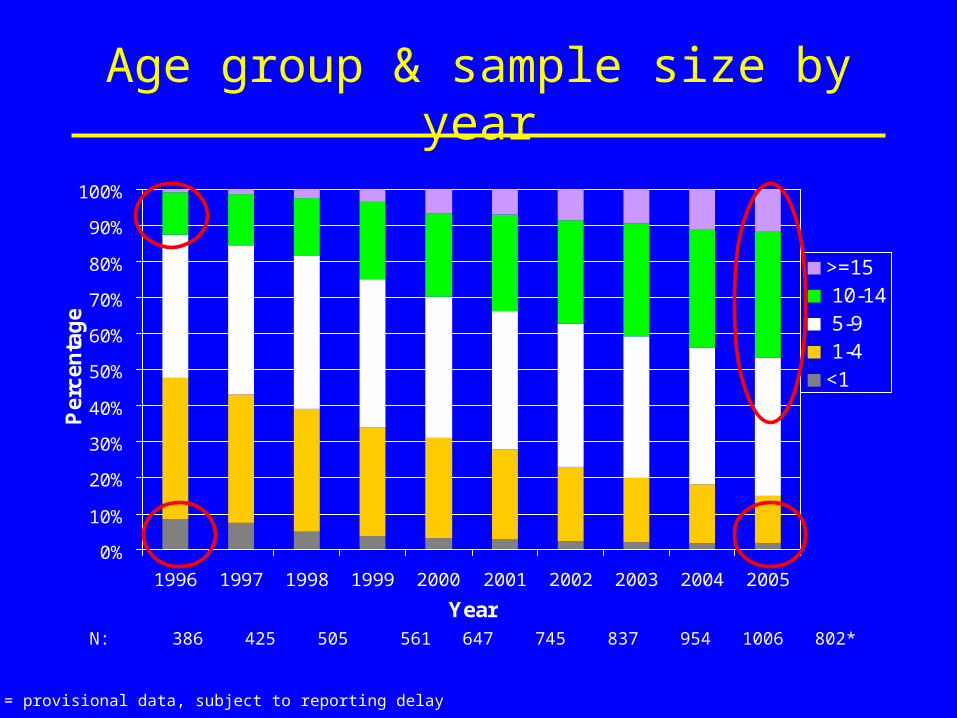
Age group & sample size by year
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Year
Perc
en
tag
e
>=15 10-14 5-9 1-4<1
N: 386 425 505 561 647 745 837 954 1006 802*
* 2005 = provisional data, subject to reporting delay

HAART exposure and switching
• 595 children started a HAART regimen since 1997 and were ART naïve before HAART– median age = 5 years (IQR 2-9)
• Median time to switching to 2nd line =7.2 yrs– [switching = 2 drugs substituted because of failure (CD4/ VL/
clinical/ resistance), or all drugs changed]
• At last follow up:– 33% of 10-14 year olds and 41% aged 15 were
triple class exposed– 9% of 10-14 year olds and 14% aged 15 were
off all ART, after previously receiving HAART

VL decrease <400 c/ml at 12 months
Variable % Odds ratio(95%CI)
Year started HAART
1997/9 (baseline) 51% 1.00
2000/2 70% 2.27 (1.30-3.96)
2003/5 76% 2.99 (1.60-5.59)
• No effect of age, or viral load at HAART
All ORs are adjusted for: age, CD4% and HIV-1 RNA at HAART initiation; sex; CDC B/C events prior to HAART; number of drugs in the initial HAART regimen; year started HAART; and timing of response measurements

CD4% increase >10% at 12 months
Variable Odds ratio(95%CI)
Age at HAART (per year)0.85 (0.78-0.92)
CD4% at HAART (per 5%) 0.55 (0.47-0.64)
Sex
Male (baseline) 1.00
Female 1.68 (1.01-2.81)
• No effect of calendar yearAll ORs are adjusted for: age, CD4% and HIV-1 RNA at HAART initiation; sex; CDC B/C events prior to HAART; number of drugs in the initial HAART regimen; year started HAART; and timing of response measurements

Rates of progression to AIDS/ death
0
2
4
6
8
10
12
14
16
18
-1996 1997/99 2000/02 2003/05
Year
Ra
te/ 1
00
pe
rso
n y
ea
rs AIDS/deaths
Deaths

Deaths in 2003/5
• 18 children died between 2003/5. Of these:• 7 presented with AIDS/ died within one month• Of the remaining 11:
– only 3 were on HAART for 6+ months prior to death– primary cause of death was opportunistic infections
(2), HIV encephalopathy (1), sepsis (1), lung disease (1), gastrointestinal bleeding (1), chickenpox/ cardiovascular (1), neurocysticercosis
– cause of 3 deaths unknown:• 1 was diagnosed at 4 months & died 6 weeks later; 2 were
diagnosed at birth but subsequently returned to Africa and died there

Conclusions
• Mortality and rates of progression to AIDS have continued to decline since HAART
• Viral load suppression 12 months after HAART initiation improved with time
• Low rates of switching to 2nd line therapy• Increased triple class exposure complicates
clinical management• Provision of transitional services and
continued monitoring essential as the cohort ages into adolescence and adulthood
Acknowledgements
• We thank:– staff and families from the hospitals collaborating in
CHIPS, and Gill Wait, CHIPS Data Manager– all paediatricians and other health professionals
reporting to the NSHPC, and the British Paediatric Surveillance Unit of the Royal College of Paediatrics and Child Health
– UK Department of Health, HPA, Bristol-Myers Squibb, Boehringer-Ingelheim, GlaxoSmithKline, Roche, Abbott and Gilead for financial support
• www.chipscohort.ac.uk