breast cancer staging singpore 2013 · breast cancer staging pathology issues ... 09/11/2013 2 0 30...
TRANSCRIPT

09/11/2013
1
Breast Cancer Staging
Ian Ellis
Molecular Medical Sciences, University of Nottingham
Department of Histopathology, Nottingham University Hospitals NHS Trust
Breast Cancer StagingPathology Issues
• Tumour Size
• Vascular Invasion
• Lymph Node Status
0
50
100
150
200
250
300
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Maximum diameter (mm)
No
.o
fp
ath
olo
gis
ts
Case No. 8
Submitted - size range 8-20 - median 13Measured size range on first, middle and last section, 13, 13 and 13mm
Circulation 2001/1 Case 8Invasive Ca, grade 1, NST
0
50
100
150
200
250
300
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Maximum diameter (mm)
No
.o
fpa
tho
log
ists
Case No. 11
Submitted - size range 7-26 - median 20Measured size range on first, middle and last section, 21, 21 and 19mm
Circulation 2001/1 Case 11Invasive Ca, grade 2, Lobular

09/11/2013
2
0
30
60
90
120
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32
Maximum diameter (mm)
No
.o
fp
ath
olo
gis
ts
Case No. 7
Submitted - size range 2-26, median 21Measured size range 1st, 35th and 70th sections, 24, 23 and 22mm
Circulation 2001/1 Case 7 Low grade DCIS
Distribution of measures of agreement for NHSBSP pathologists
(403 pathologists)
243
60
32 34
215 13
1 1 1 1
0
10
20
30
40
50
60
70
80
90
100
100 97 94 91 88 85 82 79 76 73 70 67 64
Measure of agreement (%)
% of readers
0
40
80
120
160
200
240
280
320
360
400Number of readers
A B C D0
50
100
150
200
250
300
350
400
450
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38Maximum diameter (mm)
No
.o
fp
ath
olo
gis
ts
Object A
0
50
100
150
200
250
300
350
400
450
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38
Maximum diameter (mm)
No
.o
fp
ath
olo
gis
ts
Object D

09/11/2013
3
Breast CancerMinimum Data Set
Pathological Size
Microscopic - impalpable & diffuse tumoursMacroscopic verified by microscopy
MRI
Ultrasound
Mammography
Clinical
Size measurement hierarchy
VI in Breast Cancer
Prognostic significance
Close correlation with loco regional lymph node statusRosen et al, 1983; Davis et al, 1985; Orbö et al, 1990;Pinder et al, 1994
Correlation with early recurrence in lymph node negative patientsRosen et al, 1982; Bettelheim et al, 1984
Predicts for long term survival, independent of nodal statusRosen et al, 1982; Pinder et al, 1994
Predicts for local recurrence following breast conservation therapyNealon et al, 1981; Rosen, 1983; Locker et al, 1989
Predicts for flap recurrence after mastectomyO’Rourke et al, 1994
Vascular Invasion in Breast CancerFrequency
Study % cases
Fisher et al 1975 33
Roses et al, 1982 21
Davis et al, 1985 59
Dawson et al, 1986 (a) 25 yr survivors 57
(b) short term survivors 67
Orbo et al, 1990 24
Pinder et al, 1994 23
• Tumour emboli must be present within clear spaceswhich are lined by endothelial cells
• No distinction is made between lymphatics, capillariesand post-capillary venules
• Assessment is made in breast tissue adjacent to themain primary tumour and not within it
• Topographic patterns are helpful in identifying involvedvessels
Vascular Invasion in Breast Cancer
Diagnostic Criteria

09/11/2013
4
LVI for LN neg
Cumulative Proportion Surviving (Kaplan-Meier)
Complete Censored
Group 0.Group 1.0 50 100 150 200 250
Time
0.65
0.70
0.75
0.80
0.85
0.90
0.95
1.00
1.05
Cu
mu
lative
Pro
po
rtio
nS
urv
ivin
g
p = .00017
LVI contribution and nodalstatus contribution to hazard
Cumulative Proportion Surviving (Kaplan-Meier)
Complete Censored
LVInegLNnegLVIposLNnegonetwothreefourplus
020
4060
80100
120140
160180
200220
240260
280300
Time
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Cu
mu
lative
Pro
po
rtio
nS
urv
ivin
g
Merging LVI pos 1 and 2
Cumulative Proportion Surviving (Kaplan-Meier)
Complete Censored
LVInegLNnegthreefourplusLVIpos 1and 20 50 100 150 200 250 300
Time
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Cu
mu
lative
Pro
po
rtio
nS
urv
ivin
g

09/11/2013
5
Background and rationale including theresults from clinical trials
Optimal handing of the specimen andanalysis
Role of Immunohistochemical analysis?Role of Intraoperative Examination?
Alternatives and future directions
Lymph node Staging
Background and rationale including theresults from clinical trials
Optimal handing of the specimen andanalysis
Role of Immunohistochemical analysis?Role of Intraoperative Examination?
Alternatives and future directions
Lymph node Staging Lymph Node Involvementin Breast Cancer
• Palpable loco-regional lymph nodes form an importantpart of TNM clinical staging - notoriously inaccurate -
Barr & Baum, 1992
• Presence of histologically confirmed axillarymetastases indicates a poor prognosis e.g. 10 yearsurvival reduced from 75% to 30% -
Cutler et al, 1969
• The greater the number of nodes involved, the poorerthe prognosis -
Fisher et al, 1984; Galea et al, 1992
Nottingham Tenovus Primary BreastCancer Study
Lymph Node Stage
Stage 1 - LN Neg
Stage 2 - Up to 3 lowaxillary LN +, or internalmammary LN + alone
0
.2
.4
.6
.8
1
Cu
m.
Su
rviv
al
0 48 96 144 192 240
Time
553.146 2 <.0001
Chi-Square DF P-Value
2360 909 207 Stage 1
973 192 34 Stage 2
385 56 13 Stage 3
0 4 8 12 16 20 Time (years)
Stage 3: 4 or more axillary LN +, apical LN +,or low axillary AND internal mammary +
Axillary Surgery
• Staging
• Loco-regional control
• Survival

09/11/2013
6
Staging and Prognosis
• ALND
– Widely accepted
– Qualitative
– Quantitative
• Axillary Node Sample
• SLNB
Loco-regional Control
Local disease control is essential
NSAPB – 04
– 10 year axillary recurrence rate
• 1% node negative
• 3% node positive with ALND
• 17% node positive, no dissection
• However no survival difference
Survival
• Variations between studies
• No difference - NSABP B-04
• Advantage
– Cabanes et al - 5 year
– Guys hospital, Edinburgh - long term
• May have some impact but quality ofevidence poor
Advantages of ALND
• Most important prognostic variable
• Planning of adjuvant systemic therapy
• DFS and OS are related to number ofinvolved nodes
• Node positivity increases with tumoursize
• But screening detects smaller cancerslikely to be node negative
Disadvantages of ALND
Seroma
Wound infection @10%
Reduced shoulder mobility
Damage to motor nerves
Medial pectoral
Long thoracic
Thoracodorsal
Numbness and paraesthesia
Lymphoedema - 10 - 25% (30 - 40% if ALND + RT)
Sentinel Lymph Node
• Definition
– “Any node receiving directlymphatic drainage from theprimary tumour”

09/11/2013
7
SLNB
• Constant afferent channel to SLN
• Assumes skip metastases do not occur
(< 5%)
• Negative SLN implies negative entirelymphatic basin
• Minimally invasive
• Less morbidity
– ALMANAC trial
Operative Appearance
• a blue node
• a hot node
• a palpable node
What to do if SLNB +ve?
• In 50 - 70% the SLN is the only involved node
– Staged and treated by SLNB
• 30 - 50% have micro or macro-mets in nonsentinel nodes
• ALND or RT?
• Consider volume of nodal disease, patientsfactors, patient wishes
• Discuss pros and cons of each procedure fully
• No right or wrong answer!
Natural History of Nodal Mets
• May progress and lead to relapse anddecreased survival
• May be adequately treated by adjuvantsystemic therapy
• May be ablated by radiotherapy
• ACOSOG - Z0011 – no survivaladvantage to ALND if SLNB +ve
Conclusions
• SLNB has largely replaced ALND formost early breast cancer patients
• ALND will increasingly be limited topatients with more extensive axillarydisease and to those with localrecurrence
• Further study is needed to evaluate theclinical significance of IHC-detectedisolated tumour cells and micro-metastases in sentinel nodes.
Background and rationale including theresults from clinical trials
Optimal handing of the specimen andanalysis
Role of Immunohistochemical analysis?Role of Intraoperative Examination?
Alternatives and future directions
Sentinel lymph node biopsy
09/11/2013
8
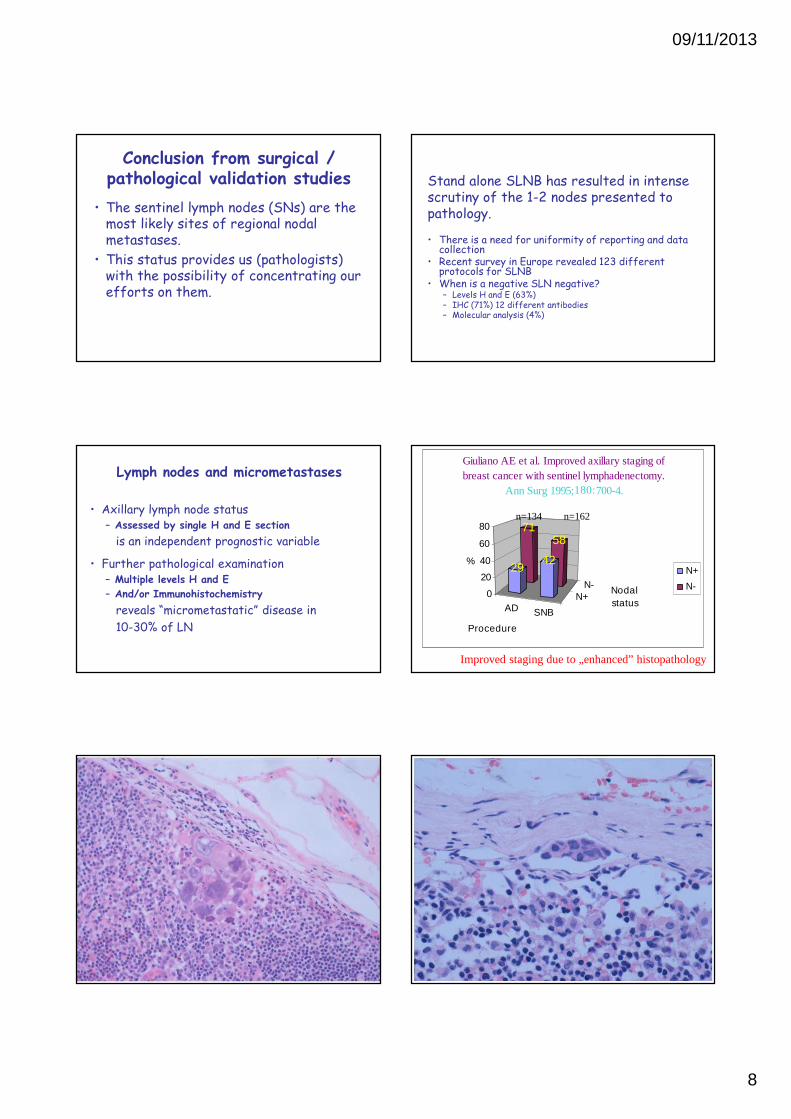
Conclusion from surgical /pathological validation studies
• The sentinel lymph nodes (SNs) are themost likely sites of regional nodalmetastases.
• This status provides us (pathologists)with the possibility of concentrating ourefforts on them.
Stand alone SLNB has resulted in intensescrutiny of the 1-2 nodes presented topathology.
• There is a need for uniformity of reporting and datacollection
• Recent survey in Europe revealed 123 differentprotocols for SLNB
• When is a negative SLN negative?– Levels H and E (63%)– IHC (71%) 12 different antibodies– Molecular analysis (4%)
Lymph nodes and micrometastases
• Axillary lymph node status
– Assessed by single H and E section
is an independent prognostic variable
• Further pathological examination
– Multiple levels H and E
– And/or Immunohistochemistry
reveals “micrometastatic” disease in
10-30% of LN
AD SNB
N+N-
7158
2942
0
20
40
60
80
%
Procedure
Nodal
status
Giuliano AE et al. Improved axillary staging of
breast cancer with sentinel lymphadenectomy.
Ann Surg 1995;180:700-4.
N+
N-
n=134 n=162
Improved staging due to „enhanced” histopathology

09/11/2013
9
Methods of increasing detectionof nodal metastases
• Identifying more nodes in specimen
• Cutting node into smaller pieces
• Step sections or levels
• Immunohistochemistry
• Reverse transcriptase polymerase chainreaction (RT-PCR)
Trends and possibilities in SNassessment
SLN assessment
Standard histopathology Enhanced histopathology
Limited sampling with or without IHC Thorough (systematic) sampling
Trends and possibilities in SNassessment
SLN assessment
Standard histopathology Enhanced histopathology
Limited sampling with or without IHC Thorough (systematic) sampling
“Standard” assessment
• “Standard” histopathology
– Many of the earliest reports, and someclinical trials use this approach.
• “Standard” is often 1 level / SN, but can bemultiple levels / SN depending on theinstitution. Rarely is it specified.
“Standard” histology of LNs
At some places standard assessment is multilevel, at othersit is 1 HE.
Pickren JW.Cancer 1961;14:1266-71.
Trends and possibilities in SNassessment
SLN assessment
Standard histopathology Enhanced histopathology
Limited sampling with or without IHC Thorough (systematic) sampling

09/11/2013
10
“Enhanced” histopathology
• Multilevel assessment:– Serial sectioning (at least 3 meanings) –
prefered terminology:• Slicing (gross)
• Step sectioning
• Serial sectioning (microscopic)
• Immunohistochemistry (CKs):– Generally containing CK8/18 (e.g. AE1/AE3,
MNF116, CAM5.2…etc)
• Combination of these two
Multilevel assessment I.
• This means the assessment of an HE section pereach level from a few tissue blocks (oftenembedded in one cassette).
• Terms: - Slicing, macroslicing, macroscopic slicing
A few mm thick slices
2-3 mm apart
Multilevel assessment II.
• This means the assessment of microscopiclevels at specified distances from each other(complete or incomplete assessment of theblocks).
• Terms: - Step sectioning
Tissue block withembedded LN(piece) in it
Sectioning with amicrotome(microscopic) at stepsof … mm.
1 2 3 4
Multilevel assessment III.
• This means the assessment of microscopiclevels separated by the thickness of one (or afew) sections (complete or incompleteassessment of the blocks).
• Terms: - Serial sectioning, microscopic serialsectioning
Tissue block withembedded LN(piece) in it
Sectioning with amicrotome(microscopic) at stepsof 3-5 um.
1 2 3 …
Multilevel assessment IV.A combination of slicing and step sectioning
4 slices of an obviously positive SN, not requiring stepsectioning
3 slices step sectioned at 250 mm

09/11/2013
11
CAM5.2
Immunohistochemistry
• Increases detection of metastasesby 10 to 30%
• Quicker for technician andpathologist
• Can assess morphology
• Pitfalls
sentinel node trial
• ACOSOG Z0010
• 5539 patients
• BCT and SNB (AxCl if LN+(H&E))
• 5 year OS not related to nodal metsdiscovered with immuno (trend for BMmets) on multivariate analysis
Trends and possibilities in SNassessment
SLN assessment
Standard histopathology Enhanced histopathology
Limited sampling with or without IHC Thorough (systematic) sampling
Limited sampling with or withoutIHC
• A few levels separated by a givendistance.
• Results in upstaging but leaves aproportion of the SN unexplored
• E.g. the Santa Monica protocol
The Santa Monica protocol(2004)
Halving of the lymph node in its hilar plane, which they claimto be the most likely site of metastases.
Hilum Efferent lymphatics
• 1 HE frozen• 1 HE paraffin• 1 CK IHC
separated by 200 mmfrom the initiallyassessed level (perhalf)
Rather large proportion of theSN not investigated

09/11/2013
12
Trends and possibilities in SNassessment
SLN assessment
Standard histopathology Enhanced histopathology
Limited sampling with or without IHC Thorough (systematic) sampling
Thorough (complete)sampling
• The whole thickness of the SN isinvestigated at given distances,depending on the size of the metastaseswe are looking for.
• Complete (?) investigation of the lymphnode. (Loss of diagnostic material)
2a = 2[r2-(d/2)2]1/2
Complete step sectioning ofSNs at 250 mm + IHC /750
mm
Number of levels assessed for identification of metastases
%
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 >9
J Clin Pathol 2002; 55:926-931.
Thorough sampling (Model)
• To detect a spherical metastasis of 2 mm indiameter as a metastasis of 2 mm, levelsseparated by 1 mm should be examined.
J Clin Pathol 2004; 57:467-471.
2a = 2[r2-(d/2)2]1/2d: distance between sectioning levels
Statements on handling
• Thorough (systematic) sampling mayyield the best results.
• The largest metastases are generallydetected by limited sampling.
• IHC may sometimes be of help inidentifying larger metastases, but itgenerally helps detectingmicrometastases and ITCs.
• All SLN assessed separately
• Management of– Nodes <4mm
– Nodes >4mm
• Standardised reporting
Pathology assessment ofSLN:
National guidelines

09/11/2013
13
Single H & E section
• Suspicious or metastatic cells seen?
• Further levels and/or ICC to establish natureand size (classification) of deposit
• IHC may be helpful but not mandatory
• Identification of ITC not the aim ofassessment
Pathology assessment ofSLN:
National guidelines
12
1
2
Group of metastatic cells2 mm diameter
Lymph node <4mm
Pathology assessment ofSLN:
National guidelines
2mm
1 2 3 4 5
1 2
3
4
5
Lymph node >4mm
Pathology assessment of SLN:National guidelines
Micrometasis vs ITC
?
Micrometastasis
• Term introduced by Andrew Huvos;<2mm, as this was felt the size thatgenerally needed microscopy fordetection. Larger metastases couldmore often be picked up by experiencednaked eye examination.
• However the term is used differentlyby different authors.
The current definitions ofITC
(and micrometastasis)

09/11/2013
14
• TNM categories are arbitrarily chosen(have some evidence in support), but areused on the basis of a consensus. Theyhave DEFINITIONS, but these are notsufficient to assure an acceptablereproducibility.
Micrometastasis (UICC)pN1mi
• Larger than 0.2 mm, but none largerthan 2 mm in greatest dimension
Sobin LH, Wittekind C (eds).
TNM Classification of Malignant Tumours,6th edition, 2002.
pN0 & isolated tumor cell clusters (ITC)• ! Approximately 1,000 tumor cells are contained in a three-
dimensional 0.2-mm cluster. Thus, if more than 200 individual tumorcells are identified as single dispersed tumor cells or as a nearlyconfluent elliptical or spherical focus in a single histologic section ofa lymph node there is a high probability that more than 1,000 cellsare present in the lymph node. In these situations, the node shouldbe classified as containing a micrometastasis (pN1mi).
• ! … the 200 cells must be in a single node profile even if the node hasbeen thinly sectioned into multiple slices.
• It is recognized that there is substantial overlap between the upperlimit of the ITC and the lower limit of the micrometastasiscategories due to inherent limitations in pathologic nodal evaluationand detection of minimal tumor burden in lymph nodes. Thus, thethreshold of 200 cells in a single cross-section is a guideline to helppathologists distinguish between these two categories. Thepathologist should use judgment regarding whether it is likely thatthe cluster of cells represents a true micrometastasis or is simply asmall group of isolated tumor cells.
• ! Metastatic characteristics no longer considered in the distinctionbetween micrometastasis and ITC.
Studies of occultmetastases with at least40 events or 150 patients
Weaver et al. Effect of OccultMetastases on Survival
in Node-Negative Breast Cancer.N Engl J Med 2011;364:412-21
3887 women (NSABP-B32), median follow up 95 monthsSentinel node (+/- Axillary Clearance)2mm slices, H&E negativeImmuno at 0.5mm and 1mm, but clinicians not informedOccult metastases 16%5 year overall survival:Occult metastases present 94.6%Occult metastases not seen 95.8%Multivariate analysis (with size and grade, but no VI):Occult metastases RR 1.4 (95% 1.05 – 1.86)Conclusion: ‘do not indicate a clinical benefit of additionalevaluation, including immunohistochemical analysis’
Pathology evaluation of sentinel lymphnodes in breast cancer: protocolrecommendations and rationale.
Weaver. Mod Pathol 2010
“All protocols that use serial sectionsand IHC must be consideredexperimental until validated withoutcome data”
Sectioning nodes at 2mm intervals
Embedding all the sections
Examine one section

09/11/2013
15
Intraoperative Assessment
• Frozen section
• Imprint cytology
• Intraoperative immunohistochemistry
• Molecular asessment
Background and rationale including theresults from clinical trials
Optimal handing of the specimen andanalysis
Role of Immunohistochemical analysis?Role of Intraoperative Examination?
Alternatives and future directions
Sentinel lymph node biopsy
Imaging modalities forassessing the axilla
• Mammography
• CT
• MRI
• PET
• Scintimammography
• Ultrasound

09/11/2013
16
Cortex
Benign Malignant
• Normal 94% 10%
• Abnormal 6% 90%P<0.0001
In vitro high Resolution Helical CT of small axillary LymphNodes in Patients with Breast Cancer. Uematsu et al AJR2001;176:1069-1074
Pre-operative Biopsyof Axillary Lymph
Nodes
Study Total no. ofpts
No. with LNmets (%)
FNA/ Core Criteria used pre-opdiagnosis rate(%)
Bonnema et al(1997)
150 62 (41) FNA No 63
de Kanter et al(1997)
185 87 (47) FNA No 36
Kuenen-Boomeester(2002)
183 85 (46) FNA No 44
Duerloo et al(2003)
268 121(45) FNA Yes 31
Sapino et al(2003)
267 88 (33) FNA Yes 55
Damera et al(2003)
166 64 (39) Core Yes 42
Ciatto et al
(2006) **
491 298 (61) FNA Yes 73
Britton et al
(2009)
139 73 (53) Core No 53
Pre-operative biopsy of axillary nodes
Node positive patients
No. of positivenodes
No. of patients % diagnosed bypre-op biopsy
1 26 15
2 12 17
3 5 60
3 or more 26 77
4 or more 20 90
Nottingham data
STUDY CONCLUSIONS
• A pre-operative diagnosis of nodalmetastases can be made in 42% ofnode positive patients
• US guided core biopsy is moresensitive in patients with extensivenodal involvement
Nottingham data
Summary of guidelines
Slicing Step sectioning IHC
US/CAP Yes No No
US/Philadelphia Yes 3 levels No
UK Yes No No
Germany Yes Yes (500 mm) No
Austria Yes Yes (200 mm) Yes (up to 4)
Australia Yes Yes (4 at 200 mm) Yes (1st)
EU Guidelines Yes Yes
Minimum: 1 mm
Optimum: 200 mm
No (possible)

09/11/2013
17