bphc enrichment series for grantees: stopping a silent epidemic: policy and practice innovations to...
TRANSCRIPT

BPHC Enrichment Series for Grantees:Stopping a Silent Epidemic: Policy and
Practice Innovations to Treat and Prevent Viral Hepatitis
Thursday, January 26, 2012
2:00 PM – 3:30 PM ET
1
Learning Objectives
• Learn about viral hepatitis through a brief clinical review
• Learn about the HHS Viral Hepatitis Action Plan
• Describe several state and local health department hepatitis treatment partnerships with health centers
• Gain perspective and strategies from two current BPHC health center grantees who will discuss their approach to the treatment of Hepatitis B and C
• Learn about an innovative program, Project ECHO, that utilizes telehealth in the treatment of viral hepatitis.
2

Agenda in Brief
WelcomeJim Macrae, BPHC
Clinical Overview and HHS Viral Hepatitis Action PlanJohn Ward, CDC
State Support of Viral Hepatitis Action Plan
Chris Taylor, NASTADPerspectives from the Field
Hepatitis B: Caring for Asian & Pacific IslandersSu Wang, MD
Charles B. Wang Community Center, NY Hepatitis C: Caring for Homeless Individuals
Danielle Robertshaw, MD, Baltimore Health Center for the Homeless, MD
Innovative Program Presentation: Project ECHODr Saverio Sava, Chief Medical Officer and Primary Care PhysicianFirst Choice Community Healthcare, Albuquerque, NM
3

Clinical Overview and HHS Viral Hepatitis Action Plan
Dr. John WardDirector, Division of Viral Hepatitis, NCHHSTP
Centers for Disease Control and PreventionAtlanta, GA
4

Learning Objectives
• Describe HBV and HCV epidemiology
• Review HHS prevention priorities
• Describe opportunities for community health centers ( CHC) to improve viral hepatitis prevention care and treatment
• Highlight new opportunities for public health-CHC collaborations
5

6
Continued Transmission of HBV and HCV
– New infections continue to occur, 2009• Hepatitis B: 36,000 • Hepatitis C: ~20,000
– Hepatitis B vaccine-based interventions do not reach all at risk populations
• ~ 800 newborns infected with HBV/yr• Adults with risks represent 95% of new HBV infections
– HCV infection rates have plateaued since 2004 • Among young IDUs, annual incidence is > 10%• Increases in case reporting among young persons • Recent HCV sexual transmission among HIV+ MSM
– Healthcare-related outbreaks persist • In 2009; 115 infections; ~13,000 exposed patients • Settings: outpatient (HCV) and residential care (HBV)
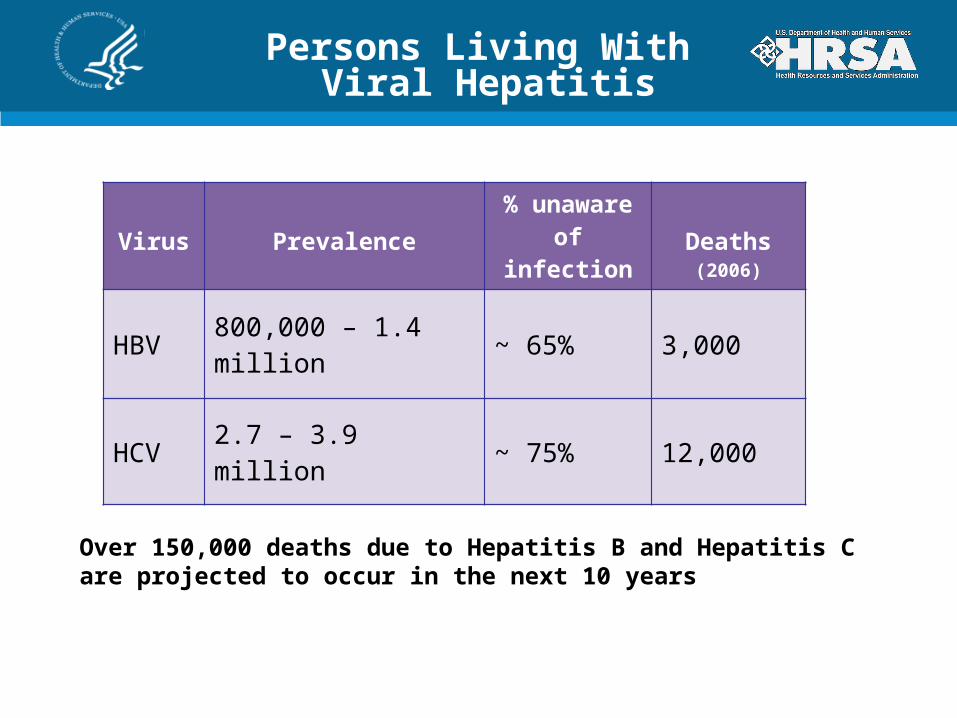
Persons Living With Viral Hepatitis
Virus Prevalence % unaware of infection
Deaths (2006)
HBV 800,000 – 1.4 million ~ 65% 3,000
HCV 2.7 – 3.9 million ~ 75% 12,000
Over 150,000 deaths due to Hepatitis B and Hepatitis C are projected to occur in the next 10 years
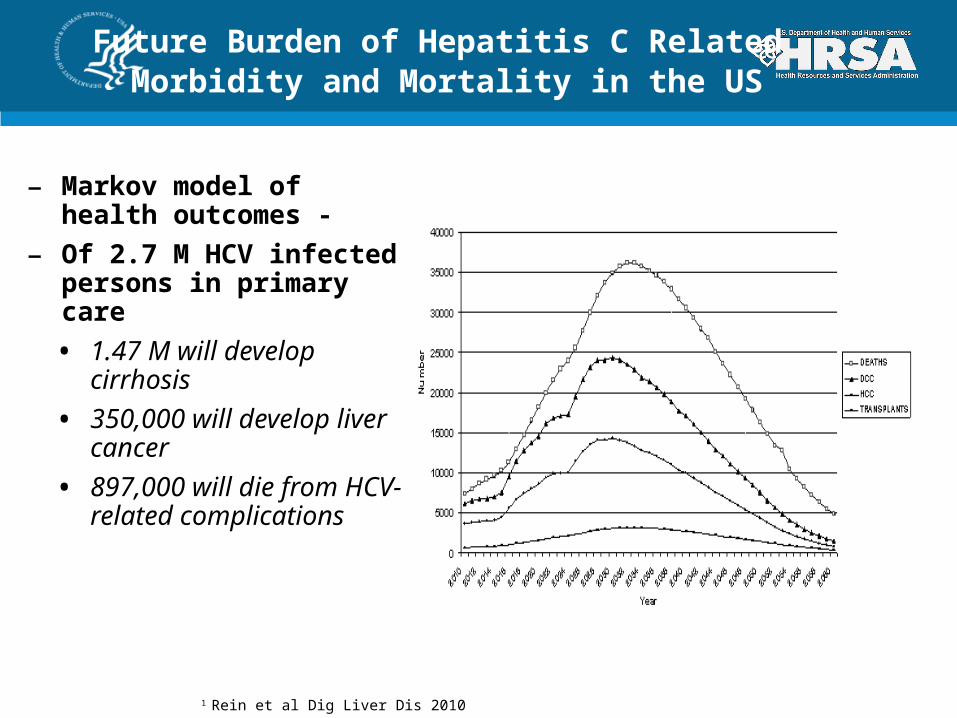
Future Burden of Hepatitis C Related Morbidity and Mortality in the US
– Markov model of health outcomes -
– Of 2.7 M HCV infected persons in primary care
• 1.47 M will develop cirrhosis
• 350,000 will develop liver cancer
• 897,000 will die from HCV-related complications
1 Rein et al Dig Liver Dis 2010

Viral Hepatitis and HIV/AIDS
HHS VIRAL HEPATITIS ACTION PLAN EDUCATING PROVIDERS AND COMMUNITIES TO
REDUCE HEALTH DISPARITIES
IMPROVING TESTING, CARE, AND TREATMENT TO PREVENT LIVER DISEASE AND CANCER
STRENGTHENING SURVEILLANCE TO DETECT VIRAL HEPATITIS TRANSMISSION AND DISEASE
ELIMINATING TRANSMISSION OF VACCINE-PREVENTABLE VIRAL HEPATITIS
REDUCING VIRAL HEPATITIS CASES CAUSED BY DRUG-USE BEHAVIORS
PROTECTING PATIENTS AND WORKERS FROM HEALTH-CARE-ASSOCIATED VIRAL HEPATITIS

HHS VIRAL HEPATITIS ACTION PLANHEALTH GOALS
Increase in the proportion of persons who are aware of their hepatitis B virus infection, from 33% to 66%
Increase in the proportion of persons who are aware of their hepatitis C virus infection, from 45% to 66%
A 25% reduction in incidence of HCV infection
Elimination of mother-to-child transmission of HBV

EDUCATE PROVIDERS AND COMMUNITIES TO REDUCE HEALTH DISPARITIES
Build a U.S. health-care workforce prepared to prevent, diagnose and treat viral hepatitis
Educate communities experiencing health disparities
Culturally appropriate
Community based
Recognize health events
World Hepatitis Day – July 28
National Hepatitis Testing Day- May 19, 2012

Improving Viral Hepatitis Testing, Care, and Treatment
– Update HHS guidelines; mandate coverage as health benefits • CDC recommends HBV testing for persons born in Asia, Africa and other
pops. > 2% prev• CDC recommends HCV testing for persons with hx of IDU, elev ALT;
considering one time testing for all persons born 1945-1965
– Include viral hepatitis testing and care coordination as standards for: • Health exchanges• Expanded Medicaid programs• Community health centers• Pre-existing condition insurance programs
– Implement performance measures in electronic medical records
– Develop and implement care models
– Build public health capacity for testing and care referral
13
STRENGTHEN SURVEILLANCE TO DETECT VIRAL HEPATITIS TRANSMISSION AND DISEASE
Build state and local surveillance systems
Automate case detection from electronic medical records
Gather data from non-traditional sources (e.g., clinical data sets)
Monitor provision of preventive and care services
Collect data to evaluate quality of prevention and care
Create data –sharing agreements across federal agencies
Provide data to support state/local case registries

REDUCE VIRAL HEPATITIS CAUSED BY DRUG USE BEHAVIORS
–Ensure IDUs have access to viral hepatitis preventive services
•Integrate viral hepatitis prevention within drug treatment and HIV prevention programs
–Provide persons who inject drugs access to care and substance abuse treatment
•Build network of primary care providers trained to provide prevention and care services for IDUs Promote continuity of care for releases inmates
•Strengthen partnerships between community re-entry programs and CHCs
Community Health Centers Programs to Improve
Viral Hepatitis Prevention, Care, and Treatment
– NACHC HCV Initiative- Keeping HCV Treatment at Home increased HCV treatment 178% in 18 CHCs*
– Project ECHO- telemedicine-based knowledge networks linking public health-CHC- tertiary care** improved care in underserved communities
– Possible opportunity in FY 12
• Prevention Public Health Fund available to support HCV and HBV testing and linkage to care
• Funding announcement in development
• Public health-CHC partnerships will be a priority
* http://www.iom.edu; ’**N Engl J Med. 2011 Jun 9;364(23):2199-207
16
Viral hepatitis “cause(s) substantial morbidity and mortality despite being preventable and treatable.”
Institute of Medicine, 2010

State Support of Viral Hepatitis Action Plan: Health Center and Public Health Collaborations
Chris Taylor
Associate Director, Viral Hepatitis
National Alliance of State and Territorial AIDS Directors (NASTAD)
18
Who is NASTAD?
• NASTAD is a non-profit national association of state health department HIV/AIDS program directors who administer HIV/AIDS and viral hepatitis prevention, care and treatment programs funded by state and federal governments. – Domestic Programs
o Health Care Accesso Prevention and Surveillanceo Health Equityo Viral Hepatitis
– Policy and Legislative Affairs– Global Program

NASTAD Mission and Vision
MissionNASTAD strengthens state and territory-based leadership, expertise and advocacy and brings them to bear on reducing the incidence of HIV and viral hepatitis infections and on providing care and support to all who live with HIV/AIDS and viral hepatitis.
VisionNASTAD’s vision is a world free of HIV/AIDS and viral hepatitis.

NASTAD and Viral Hepatitis
• Since 2000, NASTAD has been providing viral hepatitis support and technical assistance to health departments. – Due to the similarities in populations at risk, an emphasis on
integration of HIV, STD, VH and Immunization activities at the client level
• NASTAD’s viral hepatitis program has three major components– Technical assistance– Public policy– Coalition engagement
• 2010 Viral Hepatitis incorporated into Mission and Vision

• Adult Viral Hepatitis Prevention Coordinator
• Perinatal HBV Coordinator
• Adult Immunization Coordinator
• Vaccines for Children (VFC) Coordinator
• HIV/AIDS Program
Connecting with Public Health Department

• Staff In-service
• Brochures & Posters in Clinic/Agency
• Referral Guide
• Integrated Risk Assessments– Hepatitis Risk– Previous Testing– Vaccination History
• Prevention Interventions
• Integrated Presentations/Trainings
Short Term Strategies

• Hepatitis Workgroup/Committee
• Fee for Services– HBV/HCV Testing– HAV/HBV Vaccination
• Partner Services
• Support Group
• Include Hepatitis in Organization Mission
• Public Service Announcements
Medium Term Strategies

• Free Testing and Vaccination
• Medical Monitoring and Management
• Hepatitis Case Management
• Hepatitis Prevention Research
• Clinical Trials/Vaccine Development
• Successful Treatment! (Cure!)
Long Term Strategies

NASTAD report
26
http://www.NASTAD.org/care_and_treatment

Chris TaylorAssociate Director, Viral Hepatitis
[email protected] 202.434.8041
Follow NASTAD Online:
Contact Information

Hepatitis B: Caring for Asian & Pacific Islanders
Su Wang, MD MPH
Assistant Director of Medical Affairs
Charles B Wang Community Health Center, NY
28
Background on Hepatitis B Virus (HBV)
• HBV is transmitted perinatally(childbirth), blood and sex– Not transmitted by saliva, food, casual contact
• Hepatitis B Infection can be acute or chronic– Acute infections resolve and individual becomes immune (90% of
adult infections)– Chronic infections are usually lifelong (90% of childhood
infections)o Medications control disease but rarely “cure” it
• National Health Disparity– 1 out of 10 Asians has chronic HBV (5-15% in screening
programs), general population HBV rate is 0.3%– 2/3 of those infected in are unaware
• More than ½ of those with HBV in the US are Asians– Other areas of HBV infected origin
o 22% from Latin America, 13% from Africa, 7.5% from Europe

HBV: The Good, The Bad
• An effective vaccine prevents transmission (universal childhood vaccine in US since ‘91).
• HBV affects more people globally than HIV (350 vs 30 million) but gets less attention, less funding
• Most are asymptomatic, but 1 out of 4 may develop cirrhosis or liver cancer– Early intervention can prevent
complications and is cost effective– Liver cancer rates are increasing in the
US, largely due to chronic HBV and HCV infection
Post SE, Sodhi NK, Peng CH, Wan K, Pollack HJ. A simulation shows that early treatment of chronic hepatitis B infection can cut deaths and be cost-effective. Health Aff . 2011 Feb;30(2):340-8.

• Served 39,000 patients in 2010
• 89% served in language other than English – Mandarin, Cantonese,
Fujianese, Korean, Vietnamese
• 90% earn <200% of poverty
• 22% Uninsured, 72% Medicaid/Medicare, 6% Commercial insurance
• Hepatitis B Infection– 12.8% prevalence rate – 5,020 HBV+ patients in registry– 2800 are active within 18 mos
Charles B. Wang Community Health Center
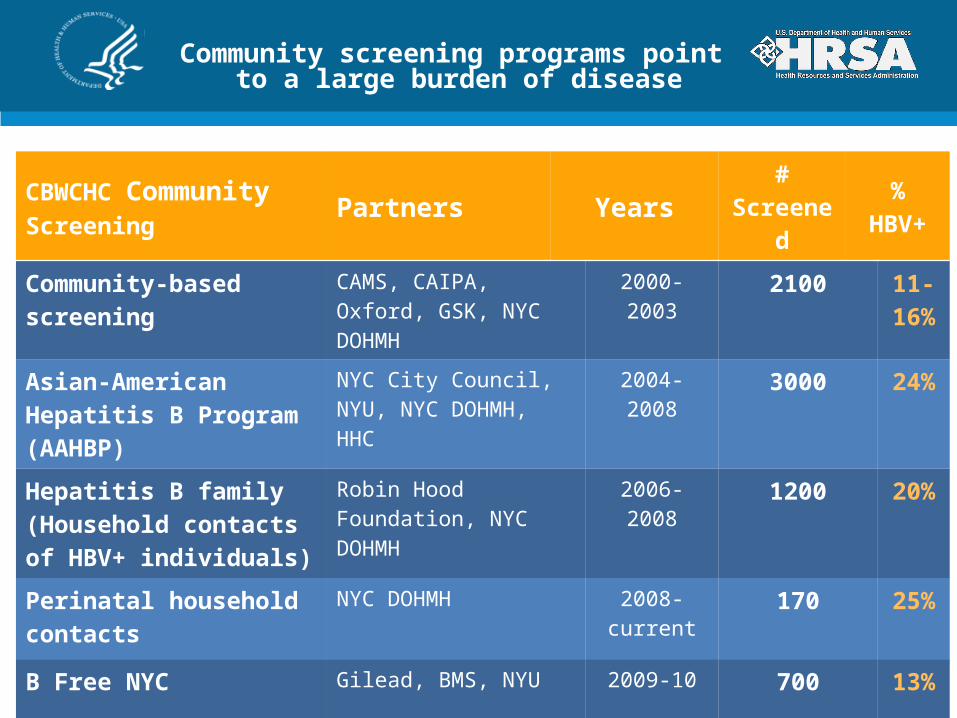
Community screening programs point to a large burden of disease
CBWCHC Community Screening Partners Years #
Screened % HBV+
Community-based screening CAMS, CAIPA, Oxford, GSK, NYC DOHMH
2000-2003 2100 11-16%
Asian-American Hepatitis B Program (AAHBP)
NYC City Council, NYU, NYC DOHMH, HHC
2004-2008 3000 24%
Hepatitis B family (Household contacts of HBV+ individuals)
Robin Hood Foundation, NYC DOHMH
2006-2008 1200 20%
Perinatal household contacts NYC DOHMH 2008-current 170 25%
B Free NYC Gilead, BMS, NYU 2009-10 700 13%
Total 6670

Developing our HBV Program
• Incorporated screening/vaccination into primary care.– Reminders built into EMR.– Case management strategy for vaccine completion– Collaborate w/ NYC DOHMH for perinatal household contact
screening
• Developed HBV care model for a primary are setting (many patients without access to specialist care and HBV very prevalent)– Train physicians:
o Screening/vaccination, interpretation of testso Evaluate HBV diseaseo Monitor for disease progressiono Treat with antivirals
– Support staffo Nurses educate, assist patient to apply for Patient Assistance
Programs for no cost antiviral medication.– Implement collaborative care model to improve patient engagement
and health care delivery
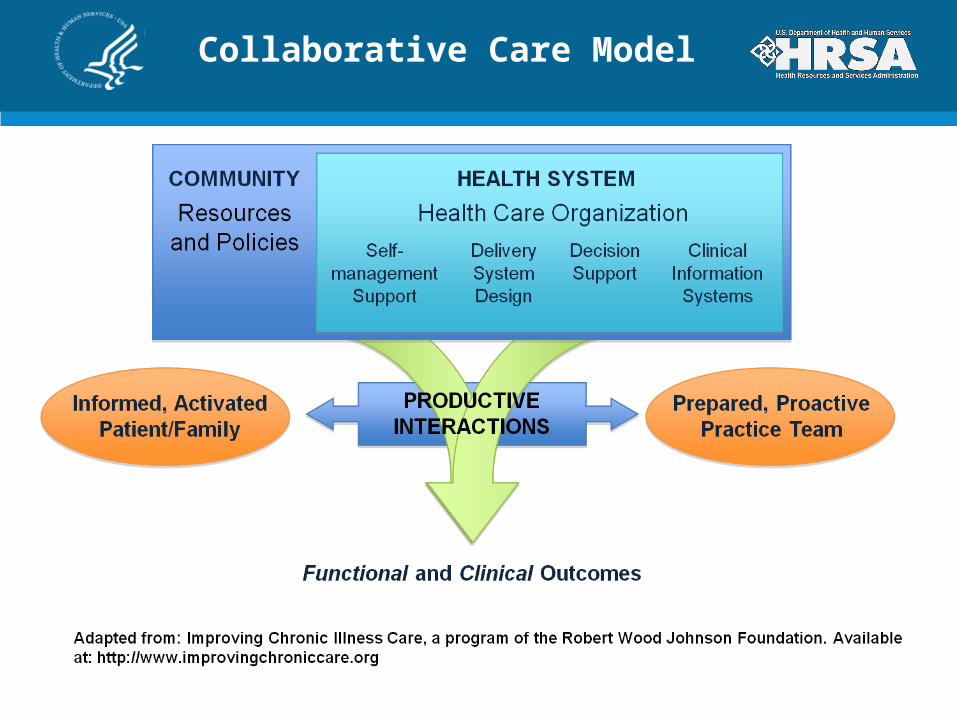
Collaborative Care Model

Health System Improvements for HBV

Provider Education:AASLD summary in exam rooms

Registry Form and HBV Flowsheet

Reminders of Overdue Tests Protocols utilize ICD9 code and last test date

Standardizing Patient Education

Hepatitis B Patient Tracker: Portable Medical Record & Education Tool

Take Home Messages
• FQHCs serve many populations at risk for HBV infection (i.e., foreign-born, HIV infected, MSM, IVDA)
• Screening needs to be increased
• Screening is simple– Hepatitis B surface Ag, Hepatitis B surface Ab, Hepatitis B core Ab– Identifies who is immune, infected and needs vaccine
• Early diagnosis and care of chronic hepatitis B infection can prevent complications of cirrhosis and cancer
• The Collaborative Care Model provides a thorough approach to improve delivery of care
41
IOM (Institute of Medicine). 2010. Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. Washington, DC: The National Academies Press http://www.iom.edu/Reports/2010/Hepatitis-and-Liver-Cancer-A-National-Strategy-for-Prevention-and-Control-of-Hepatitis-B-and-C.aspx
Questions?
Su Wang, MD MPHAssistant Director of Medical Affairs
Charles B Wang Community Health Center268 Canal St. NY NY 10013
[email protected], ext 2507
42

Danielle Robertshaw, MDMedical Officer
Family PhysicianHealth Care for the Homeless, Inc.
Baltimore, MD
Hepatitis C Virus (HCV)Caring for Homeless Individuals

Hepatitis C Virus (HCV) in the U.S.
• Most common blood borne infection in U.S.
• New infections annually: 16,000-19,000– Approximately 80% become chronic– Estimated that more than half are unaware
• CDC/NHANES: Chronic HCV estimated 1.3%-1.9% of general population (2.7-3.9 million) *Other estimates that include homeless, incarcerated
– increase to 5.2 million persons
HCV- Natural history
• Long-term– Nonspecific symptoms: fatigue, nausea, anorexia, chronic pain,
depression
– Chronic liver disease: 20-30% develop liver fibrosis, cirrhosis and liver failure over 20 years
– Cancer: 2-5% advance to Hepatocellular Carcinoma (HCC)
– In the United States:o HCV most common cause of liver transplanto Principal cause of death from liver disease – Est. 12,000
annuallyo All-cause mortality >2x higher for HCV infected patients

Health Care for the Homeless (HCH)
• Baltimore Health Care for the Homeless– Chronic HCV affects 21% of adults
E Chak, AH Talal, KE Sherman, et al. Hepatitis C virus infection in USA: an estimate of true prevalence. Liver International31(8): 1090-1101. September 2011
Prevalence in the general U.S. population 1.3-1.9%

Health Care for the Homeless
Patient demographics
Baltimore:• Race/Ethnicity – 77% African American, 18% Caucasian, 3% Hispanic• Gender – 64% male, 36% female• Age – 93% between 25-64 years• Uninsured - 75% (19% Medicaid, 6% Medicare)
Nationally: • Average 8 chronic, active medical problems• HIV - 3.4% of adults• Approximately 1/3 have Mental Health (MH) diagnoses• Estimated 2/3 meet criteria for Substance Abuse (SA)
– Co-occurring: 50% of mentally ill have a substance abuse disorder

Treatment of HCV – AASLD
Characteristics of persons for whom therapy
• Is widely accepted: – Willing to be treated and adhere to treatment
requirements
• Is currently contraindicated:– Major uncontrolled depressive illness– Severe concurrent medical disease
• Should be individualized– Current users of illicit drugs or alcohol– Coinfection with HIV
Barriers to HCV treatment
• Lack of insurance – Lack of primary medical care– Not screened/tested– Lack of specialty care– Lack of SA and MH
treatment– Medication access
• Substance abuse
• Psychiatric co-morbidity
• Medical co-morbidity
• Medication – Non-adherence – Side effects
Systemic and Individual
• Social circumstances– Housing, food, transportation– Support system
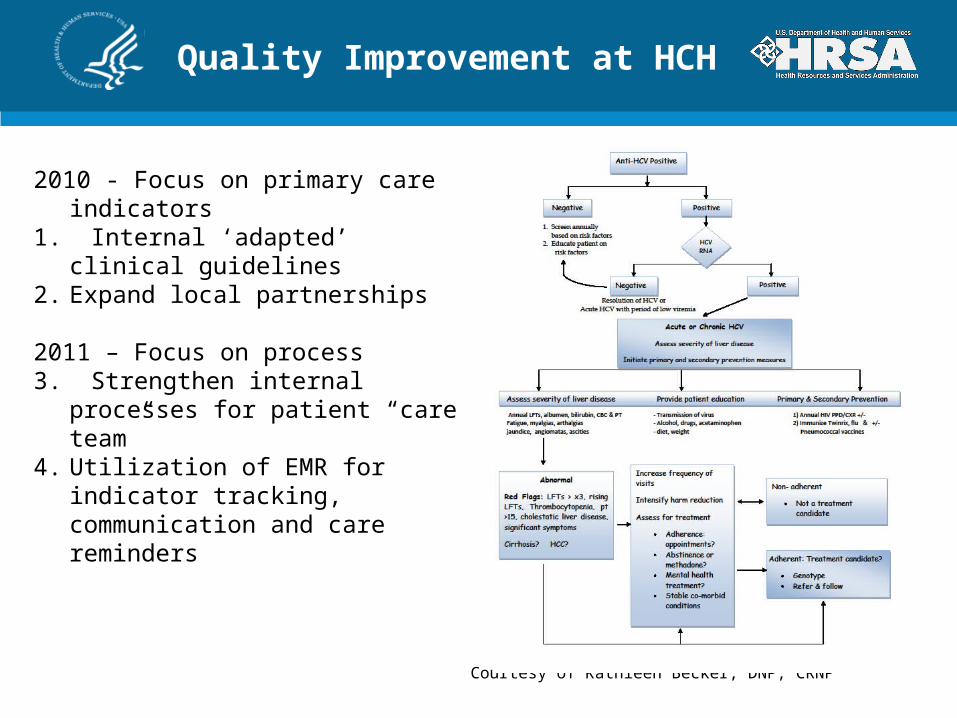
Quality Improvement at HCH
2010 - Focus on primary care indicators1. Internal ‘adapted’ clinical guidelines2. Expand local partnerships
2011 – Focus on process3. Strengthen internal processes for
patient “care team” 4. Utilization of EMR for indicator
tracking, communication and care reminders
Courtesy of Kathleen Becker, DNP, CRNP

HCV in a Primary Care setting
• Screen/test for Hepatitis C
• Educate– Hep C pos: diagnosis,
transmission and prevention, treatment options
– Hep C neg: prevention
• Counsel on – safe sex– good nutrition, weight
control– avoid hepatotoxins and– avoid sharing of
razors/toothbrushes
• Test for HIV, Hepatitis A and B
• Vaccinate: Hep A &B, flu and pneumonia
• Monitor for signs of liver disease
• Co-manage disease symptoms and treatment side effects
• Utilize peer/group support• Screen, counsel and treat for
substance abuse, depression/other psychiatric
• Refer for evaluation/treatment

Data from first phase – 16 weeks
Characteristic Baseline % Post-implementation %Diagnostic testing
Viremia 33 92Hep A & B 90 100Liver function 87 96HIV 67 71
VaccinationFlu 33 54Hep A & B 46 57
Currently working on improving and tracking (2011-2012)- Education and counseling – provision, standardization and documentation- Enhanced utilization of EMR - decision support and information sharing- Compliance – appointment and medication- Referral for specialty care - Treatment access and outcomes

Health Care for the Homeless – Lessons learned
• Multidisciplinary team approach • Medical (PCP, Nursing)
• Medication Adherence* Substance Abuse treatment* Mental Health treatment* Mobile and Street Outreach* Respite Care program * Social Work/Case Management
o Benefits assistanceo Housing assistance (obtaining
and maintaining)o Patient Assistance Programs for
medications• Considerations for Medications
– Access – Side effects (ex: diarrhea)– Instructions (3x/day with food)
• Partner with local service providers e.g., in Baltimore
o Health Dept for vaccineso Specialists/Hospital to access
evaluation and treatmento Specialists to assist in designing
protocol to improve quality of care in resource limited setting
• Harm reduction – ex: safe injecting, access to sterile injecting equipment
• Provide hygiene products– Toothbrushes– Razors
• Use of technology– EMR – Future ?text, email in improving
compliance and quality of care