bpco : epidemiologia ed inquadramento di una sindrome...
TRANSCRIPT

Leonardo M. Fabbri
Forth Mediterranean Congress Innovative Scenario in Internal Medicine
Palermo 7 Giugno 2014
Clinica di Malattie dell’Apparato Respiratorio
Università degli Studi di Modena e Reggio Emilia
BPCO : epidemiologia ed inquadramento di una sindrome complessa

CONFLICTS OF INTEREST
Leonardo M. Fabbri, 2014

BPCO : epidemiologia ed inquadramento di una sindrome complessa
Leonardo M. Fabbri
BPCO COME COMPONENTE POLMONARE DELLA
MULTIMORBIDITA’ CRONICA
ALTERAZIONI FUNZIONALI RESPIRATORIE IN
PAZIENTI CON CARDIOPATIE CRONICHE
INTERESSAMENTO POLMONARE NELLE MALATTIE
CRONICHE
COMPLESSITA’ DEL PAZIENTE CON DISPNEA ACUTA
IL MALATO CRITICO CRONICO

BPCO COME COMPONENTE POLMONARE DELLA
MULTIMORBIDITA’ CRONICA
ALTERAZIONI FUNZIONALI RESPIRATORIE IN
PAZIENTI CON CARDIOPATIE CRONICHE
INTERESSAMENTO POLMONARE NELLE MALATTIE
CRONICHE
COMPLESSITA’ DEL PAZIENTE CON DISPNEA ACUTA
IL MALATO CRITICO CRONICO
BPCO : epidemiologia ed inquadramento di una sindrome complessa
Leonardo M. Fabbri

Global Strategy for Diagnosis, Management and Prevention of COPD
Definition of COPD 2011
COPD, a common preventable and treatable disease, is characterized by persistent airflow
limitation that is usually progressive and associated with an enhanced chronic
inflammatory response in the airways and the lung to cigarette smoking
Exacerbations and comorbidities contribute to the overall severity in individual patients.

QUANTIFYING COMORBIDITY IN INDIVIDUALS WITH
CHRONIC OBSTRUCTIVE PULMONARY DISEASE: A
POPULATION STUDY
Among 7,241,591 adults
909,948 (12.6%) had COPD
50% of all lung cancer,
33% all lower respiratory tract infection
33% of all cardiovascular disease, a
25% of all low trauma fracture
20% all psychiatric, musculoskeletal,
non-lung cancer and diabetes
ambulatory care visits
emergency department visits
hospitalizations in Ontario
were used by people with COPD
Gershon A et al, Eur Respir J 2014; 7 june 2014, in press

COMORBIDITIES IN INDIVIDUALS WITH COPD
Gershon A et al, Eur Respir J 2014; 7 june 2014, in press
Individuals with COPD used about 5 times more health services for lung cancer and 2 times more health services
for lower respiratory tract infections and 2or cardiovascular disease than people without COPD

Pathogenesis of COPD
Adapted from PJ Barnes, 2000; Fabbri, Sinigaglia, Papi, Saetta 2002; Cosio,
Saetta and Cosio 2012
Cigarette smoke
or air pollutant
Alveolar
macrophage
Neutrophil
Proteases
? CD8+ T-cell
Alveolar wall destruction
EMPHYSEMA
Mucus hypersecretion
BRONCHIOLITIS
Inflammatory cytokines
(IL-8, LTB4) CXCL-10
CXCR3

Leading Causes of
Death in U.S.
1. Myocardial
Infarction
2. Cancer
3. Cerebrovascular
Diseases
4. COPD
Cigarette Related Diseases
Leading Causes of
Death Worldwide 2010

Rabe K. NEJM; 356:851-854 (2007)
COPD AS THE PULMONARY COMPONENT OF MULTIMORBIDITY

Global Strategy for Diagnosis, Management and Prevention of COPD
Definition of COPD 2011
COPD, a common preventable and treatable disease, is characterized by persistent airflow
limitation that is usually progressive and associated with an enhanced chronic
inflammatory response in the airways and the lung to noxious particles or gases
Exacerbations and comorbidities contribute to the overall severity in individual patients.

USING PULMONARY IMAGING TO
MOVE COPD BEYOND FEV1
Coxson HO et al, Am J Resp Cr Care Med, 5 June 2014
Thoracic imaging using MRI and CT provides
new opportunities to develop surrogate
measurements that improve our understanding
of COPD and its outcomes
The use of pulmonary imaging methods and
measurements has important implications for
COPD biomarker and therapy discovery and
development.

COMPLEX CHRONIC COMORBIDITIES OF COPD
Fabbri LM, Luppi F, Beghe B, and Rabe KF - Eur Respir J 2008;31:204-212

Courtesy of K.F. Rabe, 2014.
SIMULTANEOUS DEVELOPMENT OF
CHRONIC DISEASES

Chronic diseases represent a huge
proportion of human illness
58 million deaths in 2005:
Cardiovascular disease 30%
Cancer 13%
Chronic respiratory diseases 7%
Diabetes 2%
Beaglehole R et al. Lancet 2007;370:2152-57.

NUMBER OF CHRONIC DISORDERS BY AGE-GROUP
100
90
80
70
60
50
40
30
20
10
0
Age groups (years)
Pati
en
ts (
%)
0 disorders
1 disorder
2 disorders
3 disorders
4 disorders
5 disorders
6 disorders
7 disorders
≥ 8 disorders
Barnett, K et al, Lancet, 2012 Jul 7;380(9836):37-43

Martinis M et al. Exp. Mol. Pathol. 80 (3):219-227, 2006

BPCO COME COMPONENTE POLMONARE DELLA
MULTIMORBIDITA’ CRONICA
ALTERAZIONI FUNZIONALI RESPIRATORIE IN
PAZIENTI CON CARDIOPATIE CRONICHE
INTERESSAMENTO POLMONARE NELLE MALATTIE
CRONICHE
COMPLESSITA’ DEL PAZIENTE CON DISPNEA ACUTA
IL MALATO CRITICO CRONICO
BPCO : epidemiologia ed inquadramento di una sindrome complessa
Leonardo M. Fabbri

CARDIOVASCULAR MORTALITY IN COPD
For every 10% decrease in FEV1, cardiovascular mortality increases by approximately 28% and non-fatal coronary event
increases by approximately 20% in mild to moderate COPD
Sin DD et al, Proc Am Thorac Soc 2005;2:8-11

COPD vs. CHF
Up to 1\5 of elderly pts. with COPD have CHF
Up to 1\3 of elderly pts. with CHF have COPD
14 million Americans have
COPD and 5 million have
CHF
M. Padeletti-LeJemtel et al Int. J Cardiology, 2008
The risk ratio of developing HF in COPD pts is 4.5 The rate-adjusted hospital prevalence of CHF is 3 times greater among pts. discharged with a diagnosis of COPD compared with patients discharged without mention of COPD

How common is COPD in CHF?
Biagi P et al. Intern J Cardiol 2011;152:88-94
26.7
62,8
21
44,2
10,4
40,5
19,4
3,7 7,5
32,5
9,2
%

Roversi S et al. Eur J Clin Invest 2014;44:93
Common pathogenetic mechanisms of COPD and CVD

COPD only: 194 (48%)
CHF only: 33 (8%)
no CHF, no COPD: 128 (32)%
COPD + CHF: 50 (12%)
Rutten FH et al, Eur Heart J 2005
UNRECOGNIZED HEART FAILURE IN ELDERLY PATIENTS WITH STABLE COPD
405 elderly with a diagnosis of COPD, but no CHF by GPs
Echo + spiro reassessment
CHF only: 33 (8%)
COPD + CHF: 50 (12%)

29 %
71 %
Only 10 of 42 (<25%) pts. with both CHF and COPD were aware of
airflow limitation and properly treated
% o
f patients
0
10
20
30
40
50
60
GOLD I GOLD II GOLD III
CHF 34 CHF +
COPD
Echocardiography, Spirometry, and Systemic Acute- Phase Inflammatory Proteins in Smokers with COPD or CHF: An Observational Study
34 %
CHF patients
66%
Beghé B. et al. PlosOne 2013 Nov 11;8
66%
34%

hyperinflation reduces cardiothoracic ratio
pulmonary
vascular
remodeling
masks alveolar
shadowing
asymmetric
and regional
patterns
vascular bed
loss causes
upper lobe
venous
diversion
Gehlbach BK. Chest 2004; 125:669-82
radiology
COPD masks or mimics heart failure

Caution diagnosing COPD in HF
Airway compression
Bronchial hyper-responsiveness
always perform
Spirometry… and always
when euvolaemic
misdiagnosis overestimate severity
Inappropriate bronchodilators
Inappropriate avoidance of β-blockers

HIGH PREVALENCE AND UNDERDIAGNOSIS
OF LUNG FUNCTION ABNORMALITIES IN
PATIENTS WITH ISHEMIC HEART DISEASE
Soriano J ……. and Fabbri LM, 2014 in preparation
No AL
n=1,957
(70.5%)
AL
n=819
(29.5%)
No
Diagnosis
(70.3%)
Prior
Diagnosis *
(29.7%)

IMPACT OF COPD ON LONG-TERM OUTCOME AFTER STEMI RECEIVING PRIMARY PCI
Campo G., et al. Chest 2013 ;144:750-7
As compared to patients without COPD, patients with STEMI and concomitant COPD are at greater risk for
> death (25% vs 16.5%)
> hospital readmissions due to cardiovascular causes (recurrent MI, HF and bleedings)

AIRFLOW OBSTRUCTION, LUNG FUNCTION AND INCIDENCE OF ATRIAL FIBRILLATION
Li J et al Circulation 2014;129:971-80
In this large population-based study with a long-term follow-up, reduced FEV1 and obstructive respiratory disease were associated with a higher AF incidence after adjustment for measured confounders.

DIABETES AS A RISK FACTOR FOR STROKE IN WOMEN
COMPARED WITH MEN: A SYSTEMATIC REVIEW AND META-
ANALYSIS 775 385 INDIVIDUALS AND 12 539 STROKES
Peters SAE et al, Lancet 2014; 383: 1973–80
The excess risk of stroke
associated with diabetes
is > in women than men
Need for further work to
clarify
the biological,
behavioural, or social
mechanisms involved.

SYSTEMATIC REVIEW AND NETWORK META-ANALYSIS
COMPARING ANTITHROMBOTIC AGENTS FOR THE
PREVENTION OF STROKE AND MAJOR BLEEDING IN
PATIENTS WITH ATRIAL FIBRILLATION
Cameron C, Coyle D, Richter T, et al. BMJ Open 2014;4:e004301.
Compared with standard adjusted
dose of VKA, new oral
anticoagulants (NOA) were
associated with modest
reductions in the absolute risk of
stroke and major bleeding
People on antiplatelet drugs
experienced more strokes
compared with anticoagulant
drugs without any reduction in
bleeding risk

SYSTEMATIC REVIEW AND NETWORK META-ANALYSIS
COMPARING ANTITHROMBOTIC AGENTS FOR THE
PREVENTION OF STROKE AND MAJOR BLEEDING IN
PATIENTS WITH ATRIAL FIBRILLATION
Cameron C, Coyle D, Richter T, et al. BMJ Open 2014;4:e004301
Compared with VKA, new oral
anticoagulants (NOA) were
associated with modest
reductions in the absolute risk
of stroke and major bleeding
People on antiplatelet drugs
experienced more strokes
compared with anticoagulant
drugs without any reduction in
bleeding risk

OUTCOMES
Bronchodilators
Heart failure
Devices Smoking cessation
beta-blockers
Renin-angiotensin-aldosterone system inhibition
COPD
beta-agonists
Why is diagnosis important?

Exac
erb
atio
ns p
er
year
> 2
1
0
mMRC 0-1 CAT < 10
GOLD 4
mMRC > 2 CAT > 10
GOLD 3
GOLD 2
GOLD 1
SAMA prn or
SABA prn
LABA or
LAMA
ICS + LABA or
LAMA
Global Strategy for Diagnosis, Management and Prevention of COPD
Manage Stable COPD: Pharmacologic Therapy FIRST CHOICE
A B
D C ICS + LABA
and/or LAMA
GOLD 2013

Bronchodilators are associated with increased mortality
Hawkins NM. Eur J Heart Fail 2010: In Press.
0.7
0
.8
0.9
1.
0
Sur
viva
l R
ate
0 0.5 1.0 1.5 2.0 2.5 3.0 3.5
Time (years)
No bronchodilator and beta-blocker
No bronchodilator and no beta-blocker Bronchodilator and beta-blocker
Bronchodilator and no beta-blocker
CHARM trial: patients with HF receiving bronchodilators (n=674 of 7599)

Rutten FH et al, Arch Intern Med. 2010;170:880-7
Treatment with beta-blockers may reduce the risk of exacerbations and
improve survival in patients with COPD, possibly as a result of dual
cardiopulmonary protective properties

EFFECTS OF CARDIOVASCULAR DRUGS ON MORTALITY IN SEVERE COPD PATIENTS
(on Long Term Oxygen Therapy)
Ekström, M. et al. AJRCCM 2013,;187:715-20
Antiplatelet drugs improve survival
ACE inhibitors and statins may improve survival
Beta blockers may decrease survival

BPCO COME COMPONENTE POLMONARE DELLA
MULTIMORBIDITA’ CRONICA
ALTERAZIONI FUNZIONALI RESPIRATORIE IN
PAZIENTI CON CARDIOPATIE CRONICHE
INTERESSAMENTO POLMONARE NELLE MALATTIE
CRONICHE
COMPLESSITA’ DEL PAZIENTE CON DISPNEA ACUTA
IL MALATO CRITICO CRONICO
BPCO : epidemiologia ed inquadramento di una sindrome complessa
Leonardo M. Fabbri

HEART FAILURE AS A
SYSTEMIC DISEASE Myocardial infarction causes the release
of inflammatory cells from the spleen
and bone marrow and their myocardial
infiltration
This leads to an accumulation of
monocytes in the heart, predominantly
located in the infarct border zone, and a
decrease of monocytes in the spleen and
bone marrow
This may be mediated by activation of
the sympathetic nervous system,
angiotensin II, and/ or cytokine release.
Hofmasnn and Frantz. Eur Heart J 2014; 35: 314-5.

ASSOCIATION BETWEEN CHRONIC OBSTRUCTIVE
PULMONARY DISEASE AND CHRONIC KIDNEY
DISEASE IN VASCULAR SURGERY PATIENTS
The findings of this study indicate that COPD is
moderately associated with chronic kidney
diseases in a large cohort of vascular surgery
patients
Moderate and severe COPD are related to
increased long-term mortality in patients with
chronic kidney diseases
van Gestel Y. et al, Nephrol Dial Transplant (2009) 24: 2763–2767

METABOLIC SYNDROME IN COPD
A co-exisiting
metabolic
syndrome is
frequent in
patients with
COPD
Watz H, …., and H. Magnussen, Chest 2009

Liver-Related Causes of Dyspnea in a Patient with Chronic Liver Disease
Pulmonary - Parenchymal
Alveolar – Aspiration pneumonia
– Basal atelectasis
Interstitial lung disease – Lymphocytic interstitial
pneumonia
– Fibrosing alveolitis
– BOOP
– Noncardiogenic pulmonary edema
Vascular – Pulmonary hemorrhage
– Hepatopulmonary Syndrome
– Portal-Pulmonary Hypertension
Extraparenchymal
– Pleural effusions
– Restriction from tense ascites
Extrapulmonary
– Cirrhotic cardiomyopathy
– Cirrhotic myopathy
– Chronotropic dysfunction
– Muscle wasting
– Deconditioning from impaired mobility

Liver Lung Interaction
Liver Failure
Acute Liver Failure Chronic Liver Failure
ARDS
Vasodilatation Vasoconstriction
Hepato-pulmonary Syndrome
Portopulmonary Hypertnsion

PSORIASIS AND CHRONIC OBSTRUCTIVE
PULMONARY DISEASE: A CASE–
CONTROL STUDY
Dreiher J et al., Br J Derm 2008; 159: 956-960
In this large, population-based case–control study,
psoriasis was found to be associated with COPD
Dermatologists caring for patients with psoriasis
should be aware of this association, consult an
internist or pulmonologist, and advise the patients
to stop smoking and reduce additional risk factors
for COPD

BPCO COME COMPONENTE POLMONARE DELLA
MULTIMORBIDITA’ CRONICA
ALTERAZIONI FUNZIONALI RESPIRATORIE IN
PAZIENTI CON CARDIOPATIE CRONICHE
INTERESSAMENTO POLMONARE NELLE MALATTIE
CRONICHE
COMPLESSITA’ DEL PAZIENTE CON DISPNEA ACUTA
IL MALATO CRITICO CRONICO
BPCO : epidemiologia ed inquadramento di una sindrome complessa
Leonardo M. Fabbri

EXACERBATIONS OF RESPIRATORY SYMPTOMS IN PATIENTS WITH COPD MAY NOT BE EXACERBATIONS
OF COPD
Beghé B, Verduri A, Roca M and Fabbri LM. Eur Respir J 2013; 41: 993-5
Roca M, Verduri A, Clini EM, Fabbri LM and Beghé B. Eur J Clin Invest, 2013;43:510

BPCO COME COMPONENTE POLMONARE DELLA
MULTIMORBIDITA’ CRONICA
ALTERAZIONI FUNZIONALI RESPIRATORIE IN
PAZIENTI CON CARDIOPATIE CRONICHE
INTERESSAMENTO POLMONARE NELLE MALATTIE
CRONICHE
COMPLESSITA’ DEL PAZIENTE CON DISPNEA ACUTA
IL MALATO CRITICO CRONICO
BPCO : epidemiologia ed inquadramento di una sindrome complessa
Leonardo M. Fabbri
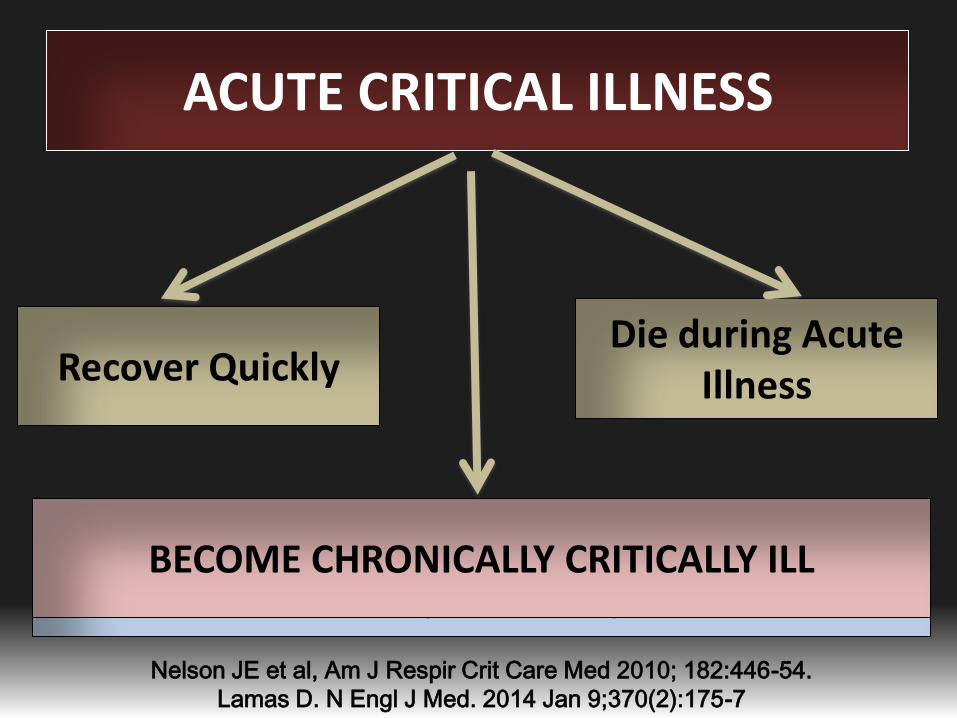
ACUTE CRITICAL ILLNESS
Recover Quickly Die during Acute
Illness
Require prolonged mechanical ventilation Elective tracheotomy
Continued High Levels of Nursing Care
BECOME CHRONICALLY CRITICALLY ILL
Nelson JE et al, Am J Respir Crit Care Med 2010; 182:446-54.
Lamas D. N Engl J Med. 2014 Jan 9;370(2):175-7

Risk Factors For Chronic Critical Illness
Acute Critical Illness Precipitants
Sepsis
Acute
Lung
Injury
Trauma
Chronic Critical Illness End Result
Weakness
Brain
Disfunction
Infection
Risk Factors • Age • Comorbidities • Genetics • Illness severity • Illness Type • Illness Management
Inflammatory Response?
Respir Care 2012; 57:859-864

Am J Respir Crit care med 2010; 182:446-454
CLINICAL FEATURES OF THE CRONIC CRITICAL ILLNESS SYNDROME
Profound Weakness
Myopathy, Neuropaty
Alterations of Body
Composition
Loss in lean body mass,
increased adiposity,
anasarca
Neuroendocrine
Changes
Brain Dysfunction
Coma, Delirium
Increased vulnerability
to infection
Skin Breakdown,
Nutritional Deficiencies,
Prolonged immobility

COPD and CHF often coexist, particularly in elderly
smokers, but often underdiagnosed
COPD increases risk of hospitalization and mortality in
CHF patients
Caution should be taken in spirometric diagnosis to
avoid overestimation of airflow limitation and
unjustified use bronchodilators
COPD is not a contraindication to β-blockers:
metoprololo, bisoprololo and nebivololo are candidates
. . . . Take home messages

BPCO COME COMPONENTE POLMONARE DELLA
MULTIMORBIDITA’ CRONICA
ALTERAZIONI FUNZIONALI RESPIRATORIE IN
PAZIENTI CON CARDIOPATIE CRONICHE
INTERESSAMENTO POLMONARE NELLE MALATTIE
CRONICHE
COMPLESSITA’ DEL PAZIENTE CON DISPNEA ACUTA
IL MALATO CRITICO CRONICO
BPCO : epidemiologia ed inquadramento di una sindrome complessa
Leonardo M. Fabbri

Leonardo M. Fabbri
Forth Mediterranean Congress Innovative Scenario in Internal Medicine
Palermo 7 Giugno 2014
Clinica di Malattie dell’Apparato Respiratorio
Università degli Studi di Modena e Reggio Emilia
BPCO : epidemiologia ed inquadramento di una sindrome complessa