booklet contents - healthnow new york much does medicare deposit into my msa bank account? medicare...
TRANSCRIPT

ActiveSaver MSA (H9788) Summary of Benefits
SmartSaver Rx PDP (S1140) Summary of Benefits
Additional information regarding your coverage
Booklet Contents
3503_09_2014_R1
MEDICARE ADVANTAGE
2015


Summary of Benefits
H9788
2015 ActiveSaver MSA


Sum
mar
y of
Ben
efits
AC
TIVE
SAVE
R M
SA (M
SA)
Ja
nuar
y 1,
201
5 - D
ecem
ber 3
1, 2
015
(a M
edic
al S
avin
gs A
ccou
nt (M
SA) o
ffere
d by
HEA
LTHN
OW
NEW
YO
RK IN
C. w
ith a
M
edic
are
cont
ract
)
This
book
let g
ives
you
a su
mm
ary
of w
hat w
e co
ver a
nd w
hat y
ou p
ay. I
t doe
sn't
list e
very
serv
ice
that
we
cove
r or l
ist e
very
lim
itatio
n or
exc
lusio
n. T
o ge
t a c
ompl
ete
list o
f ser
vice
s we
cove
r, ca
ll us
and
ask
for t
he "E
vide
nce
of C
over
age.
"
You
have
cho
ices
abo
ut h
ow to
get
you
r Med
icar
e be
nefit
s
One
cho
ice
is to
get
you
r Med
icar
e be
nefit
s thr
ough
Orig
inal
Med
icar
e (fe
e-fo
r-se
rvic
e M
edic
are)
. Orig
inal
Med
icar
e is
run
dire
ctly
by
the
Fede
ral g
over
nmen
t.
Anot
her c
hoic
e is
to g
et y
our M
edic
are
bene
fits b
y jo
inin
g a
Med
ical
Sav
ings
Acc
ount
(suc
h as
Act
iveS
aver
MSA
(MSA
)).
MSA
pla
ns c
ombi
ne a
hig
h-de
duct
ible
hea
lth p
lan
with
a b
ank
acco
unt.
Med
icar
e de
posit
s mon
ey in
to th
e ac
coun
t (u
sual
ly le
ss th
an th
e de
duct
ible
). Yo
u ca
n us
e th
e m
oney
to p
ay fo
r you
r hea
lth c
are
serv
ices
dur
ing
the
year
. Onl
y M
edic
are-
cove
red
expe
nses
cou
nt to
war
d yo
ur d
educ
tible
. Ref
er to
the
"Med
icar
e &
You
" ha
ndbo
ok fo
r Med
icar
e-co
vere
d se
rvic
es. F
or m
ore
info
rmat
ion
abou
t MSA
s, re
fer t
o th
e "Y
our G
uide
to M
edic
are
Med
ical
Sav
ings
Acc
ount
Pl
ans"
pub
licat
ion
by v
isitin
g w
ww
.Med
icar
e.go
v, c
licki
ng "P
ublic
atio
ns" u
nder
"Tak
e Ac
tion"
and
sear
ch fo
r pub
licat
ion
num
ber 1
1206
. Or,
call
1-80
0-M
EDIC
ARE
to re
ques
t a c
opy.
Enr
ollm
ent i
s gen
eral
ly fo
r a fu
ll ca
lend
ar y
ear u
nles
s you
m
eet c
erta
in e
xcep
tions
. Tho
se w
ho d
isenr
oll d
urin
g th
e ca
lend
ar y
ear w
ill o
we
a po
rtio
n of
the
acco
unt d
epos
it ba
ck to
th
e pl
an.
You
have
cho
ices
abo
ut h
ow to
get
you
r Med
icar
e be
nefit
s Th
is Su
mm
ary
of B
enef
its b
ookl
et g
ives
you
a su
mm
ary
of w
hat A
ctiv
eSav
er M
SA (M
SA) c
over
s and
wha
t you
pay
.
If
you
wan
t to
com
pare
our
pla
n w
ith o
ther
Med
icar
e he
alth
pla
ns, a
sk th
e ot
her p
lans
for t
heir
Sum
mar
y of
Ben
efits
bo
okle
ts. O
r, us
e th
e M
edic
are
Plan
Fin
der o
n ht
tp:/
/ww
w.m
edic
are.
gov.
If yo
u w
ant t
o kn
ow m
ore
abou
t the
cov
erag
e an
d co
sts o
f Orig
inal
Med
icar
e, lo
ok in
you
r cur
rent
"M
edic
are
& Y
ou"
hand
book
. Vie
w it
onl
ine
at h
ttp:
//w
ww
.med
icar
e.go
v or
get
a c
opy
by c
allin
g 1-
800-
MED
ICAR
E (1
-800
-633
-422
7), 2
4 ho
urs a
day
, 7 d
ays a
wee
k. T
TY u
sers
shou
ld c
all 1
-877
-486
-204
8.
H978
8_CO
M34
7 Ac
cept
ed
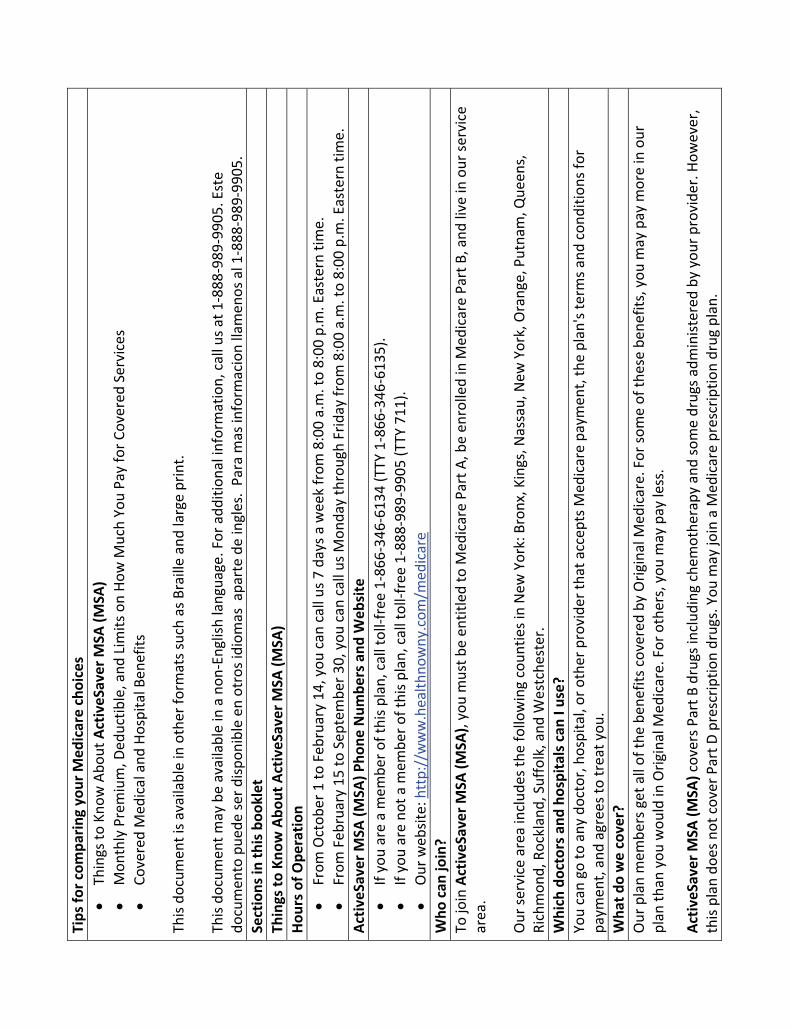
Tips
for c
ompa
ring
your
Med
icar
e ch
oice
s
Thin
gs to
Kno
w A
bout
Act
iveS
aver
MSA
(MSA
)
Mon
thly
Pre
miu
m, D
educ
tible
, and
Lim
its o
n Ho
w M
uch
You
Pay
for C
over
ed S
ervi
ces
Co
vere
d M
edic
al a
nd H
ospi
tal B
enef
its
This
docu
men
t is a
vaila
ble
in o
ther
form
ats s
uch
as B
raill
e an
d la
rge
prin
t. Th
is do
cum
ent m
ay b
e av
aila
ble
in a
non
-Eng
lish
lang
uage
. For
add
ition
al in
form
atio
n, c
all u
s at 1
-888
-989
-990
5. E
ste
docu
men
to p
uede
ser d
ispon
ible
en
otro
s idi
omas
apa
rte
de in
gles
. Pa
ra m
as in
form
acio
n lla
men
os a
l 1-8
88-9
89-9
905.
Se
ctio
ns in
this
boo
klet
Th
ings
to K
now
Abo
ut A
ctiv
eSav
er M
SA (M
SA)
Hour
s of O
pera
tion
Fr
om O
ctob
er 1
to F
ebru
ary
14, y
ou c
an c
all u
s 7 d
ays a
wee
k fr
om 8
:00
a.m
. to
8:00
p.m
. Eas
tern
tim
e.
Fr
om F
ebru
ary
15 to
Sep
tem
ber 3
0, y
ou c
an c
all u
s Mon
day
thro
ugh
Frid
ay fr
om 8
:00
a.m
. to
8:00
p.m
. Eas
tern
tim
e.
Activ
eSav
er M
SA (M
SA) P
hone
Num
bers
and
Web
site
If yo
u ar
e a
mem
ber o
f thi
s pla
n, c
all t
oll-f
ree
1-86
6-34
6-61
34 (T
TY 1
-866
-346
-613
5).
If
you
are
not a
mem
ber o
f thi
s pla
n, c
all t
oll-f
ree
1-88
8-98
9-99
05 (T
TY 7
11).
O
ur w
ebsit
e: h
ttp:
//w
ww
.hea
lthno
wny
.com
/med
icar
e W
ho c
an jo
in?
To jo
in A
ctiv
eSav
er M
SA (M
SA),
you
mus
t be
entit
led
to M
edic
are
Part
A, b
e en
rolle
d in
Med
icar
e Pa
rt B
, and
live
in o
ur se
rvic
e ar
ea.
Our
serv
ice
area
incl
udes
the
follo
win
g co
untie
s in
New
Yor
k: B
ronx
, Kin
gs, N
assa
u, N
ew Y
ork,
Ora
nge,
Put
nam
, Que
ens,
Ri
chm
ond,
Roc
klan
d, S
uffo
lk, a
nd W
estc
hest
er.
Whi
ch d
octo
rs a
nd h
ospi
tals
can
I us
e?
You
can
go to
any
doc
tor,
hosp
ital,
or o
ther
pro
vide
r tha
t acc
epts
Med
icar
e pa
ymen
t, th
e pl
an's
term
s and
con
ditio
ns fo
r pa
ymen
t, an
d ag
rees
to tr
eat y
ou.
Wha
t do
we
cove
r?
Our
pla
n m
embe
rs g
et a
ll of
the
bene
fits c
over
ed b
y O
rigin
al M
edic
are.
For
som
e of
thes
e be
nefit
s, y
ou m
ay p
ay m
ore
in o
ur
plan
than
you
wou
ld in
Orig
inal
Med
icar
e. F
or o
ther
s, y
ou m
ay p
ay le
ss.
Activ
eSav
er M
SA (M
SA) c
over
s Par
t B d
rugs
incl
udin
g ch
emot
hera
py a
nd so
me
drug
s adm
inist
ered
by
your
pro
vide
r. Ho
wev
er,
this
plan
doe
s not
cov
er P
art D
pre
scrip
tion
drug
s. Y
ou m
ay jo
in a
Med
icar
e pr
escr
iptio
n dr
ug p
lan.
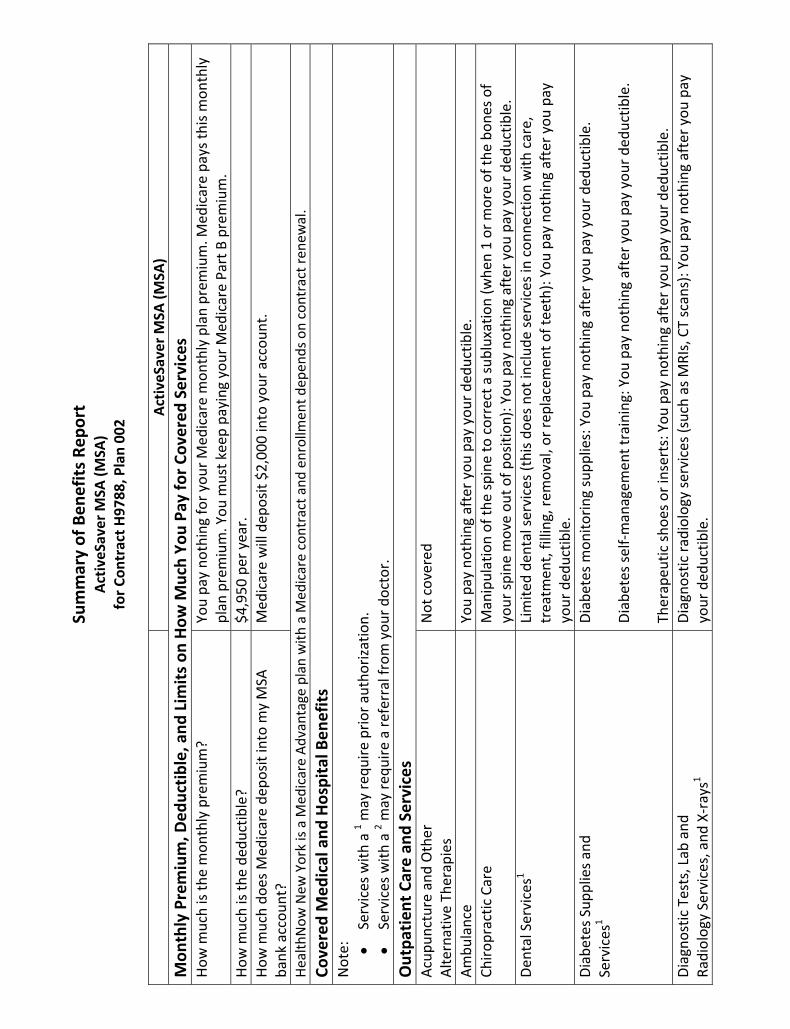
Sum
mar
y of
Ben
efits
Rep
ort
Activ
eSav
er M
SA (M
SA)
for C
ontr
act H
9788
, Pla
n 00
2
Ac
tiveS
aver
MSA
(MSA
) M
onth
ly P
rem
ium
, Ded
uctib
le, a
nd L
imits
on
How
Muc
h Yo
u Pa
y fo
r Cov
ered
Ser
vice
sHo
w m
uch
is th
e m
onth
ly p
rem
ium
? Yo
u pa
y no
thin
g fo
r you
r Med
icar
e m
onth
ly p
lan
prem
ium
. Med
icar
e pa
ys th
is m
onth
ly
plan
pre
miu
m. Y
ou m
ust k
eep
payi
ng y
our M
edic
are
Part
B p
rem
ium
. Ho
w m
uch
is th
e de
duct
ible
? $4
,950
per
yea
r.Ho
w m
uch
does
Med
icar
e de
posit
into
my
MSA
ba
nk a
ccou
nt?
Med
icar
e w
ill d
epos
it $2
,000
into
you
r acc
ount
.
Heal
thN
ow N
ew Y
ork
is a
Med
icar
e Ad
vant
age
plan
with
a M
edic
are
cont
ract
and
enro
llmen
t dep
ends
on
cont
ract
rene
wal
.Co
vere
d M
edic
al a
nd H
ospi
tal B
enef
itsN
ote:
Serv
ices
with
a 1 m
ay re
quire
prio
r aut
horiz
atio
n.
Se
rvic
es w
ith a
2 may
requ
ire a
refe
rral
from
you
r doc
tor.
Out
patie
nt C
are
and
Serv
ices
Ac
upun
ctur
e an
d O
ther
Al
tern
ativ
e Th
erap
ies
Not
cov
ered
Ambu
lanc
e Yo
u pa
y no
thin
g af
ter y
ou p
ay y
our d
educ
tible
.Ch
iropr
actic
Car
e M
anip
ulat
ion
of th
e sp
ine
to c
orre
ct a
subl
uxat
ion
(whe
n 1
or m
ore
of th
e bo
nes o
f yo
ur sp
ine
mov
e ou
t of p
ositi
on):
You
pay
noth
ing
afte
r you
pay
you
r ded
uctib
le.
Dent
al S
ervi
ces1
Lim
ited
dent
al se
rvic
es (t
his d
oes n
ot in
clud
e se
rvic
es in
con
nect
ion
with
car
e,
trea
tmen
t, fil
ling,
rem
oval
, or r
epla
cem
ent o
f tee
th):
You
pay
noth
ing
afte
r you
pay
yo
ur d
educ
tible
. Di
abet
es S
uppl
ies a
nd
Serv
ices
1 Di
abet
es m
onito
ring
supp
lies:
You
pay
not
hing
aft
er y
ou p
ay y
our d
educ
tible
. Di
abet
es se
lf-m
anag
emen
t tra
inin
g: Y
ou p
ay n
othi
ng a
fter
you
pay
you
r ded
uctib
le.
Ther
apeu
tic sh
oes o
r ins
erts
: You
pay
not
hing
aft
er y
ou p
ay y
our d
educ
tible
.Di
agno
stic
Tes
ts, L
ab a
nd
Radi
olog
y Se
rvic
es, a
nd X
-ray
s1 Di
agno
stic
radi
olog
y se
rvic
es (s
uch
as M
RIs,
CT
scan
s): Y
ou p
ay n
othi
ng a
fter
you
pay
yo
ur d
educ
tible
.

Ac
tiveS
aver
MSA
(MSA
) Di
agno
stic
Tes
ts, L
ab a
nd
Radi
olog
y Se
rvic
es, a
nd X
-ray
s1 (c
ontin
ued)
Di
agno
stic
test
s and
pro
cedu
res:
You
pay
not
hing
aft
er y
ou p
ay y
our d
educ
tible
. La
b se
rvic
es: Y
ou p
ay n
othi
ng a
fter
you
pay
you
r ded
uctib
le.
Out
patie
nt X
-ray
s: Y
ou p
ay n
othi
ng a
fter
you
pay
you
r ded
uctib
le.
Ther
apeu
tic ra
diol
ogy
serv
ices
(suc
h as
radi
atio
n tr
eatm
ent f
or c
ance
r): Y
ou p
ay n
othi
ng
afte
r you
pay
you
r ded
uctib
le.
Doct
or's
Offi
ce V
isits
Pr
imar
y ca
re p
hysic
ian
visit
: You
pay
not
hing
aft
er y
ou p
ay y
our d
educ
tible
. Sp
ecia
list v
isit:
You
pay
noth
ing
afte
r you
pay
you
r ded
uctib
le.
Dura
ble
Med
ical
Equ
ipm
ent (
whe
elch
airs
, oxy
gen,
et
c.)1
You
pay
noth
ing
afte
r you
pay
you
r ded
uctib
le.
Also
incl
udes
cov
erag
e fo
r phy
sicia
n-pr
escr
ibed
ost
omy
supp
lies,
cru
tche
s, w
heel
chai
rs,
cane
s, C
PAP
mac
hine
s, e
tc.
Emer
genc
y Ca
re
You
pay
noth
ing
afte
r you
pay
you
r ded
uctib
le.
Foot
Car
e (p
odia
try
serv
ices
) Fo
ot e
xam
s and
trea
tmen
t if y
ou h
ave
diab
etes
-rel
ated
ner
ve d
amag
e an
d/or
mee
t ce
rtai
n co
nditi
ons:
You
pay
not
hing
aft
er y
ou p
ay y
our d
educ
tible
. He
arin
g Se
rvic
es
Exam
to d
iagn
ose
and
trea
t hea
ring
and
bala
nce
issue
s: Y
ou p
ay n
othi
ng a
fter
you
pay
yo
ur d
educ
tible
.Ho
me
Heal
th C
are
You
pay
noth
ing
afte
r you
pay
you
r ded
uctib
le.
Cove
red
whe
n pr
ovid
ed b
y a
Med
icar
e pa
rtic
ipat
ing
hom
e he
alth
age
ncy.
Ben
efic
iarie
s m
ust b
e (1
) con
fined
to th
e ho
me;
(2) u
nder
a tr
eatm
ent p
lan
from
a p
hysic
ian;
and
(3)
in n
eed
of in
term
itten
t ski
lled
nurs
ing
care
, phy
sical
ther
apy,
spee
ch th
erap
y, o
r co
ntin
ued
occu
patio
nal t
hera
py.
Men
tal H
ealth
Car
e1
Inpa
tient
visi
t: O
ur p
lan
cove
rs u
p to
190
day
s in
a lif
etim
e fo
r inp
atie
nt m
enta
l hea
lth c
are
in a
ps
ychi
atric
hos
pita
l. Th
e in
patie
nt h
ospi
tal c
are
limit
does
not
app
ly to
inpa
tient
men
tal
serv
ices
pro
vide
d in
a g
ener
al h
ospi
tal.

Ac
tiveS
aver
MSA
(MSA
) M
enta
l Hea
lth C
are1
(con
tinue
d)
You
pay
noth
ing
afte
r you
pay
you
r ded
uctib
le.
Out
patie
nt g
roup
ther
apy
visit
: You
pay
not
hing
aft
er y
ou p
ay y
our d
educ
tible
. O
utpa
tient
indi
vidu
al th
erap
y vi
sit: Y
ou p
ay n
othi
ng a
fter
you
pay
you
r ded
uctib
le.
Out
patie
nt R
ehab
ilita
tion1
Card
iac
(hea
rt) r
ehab
serv
ices
(for
a m
axim
um o
f 2 o
ne-h
our s
essio
ns p
er d
ay fo
r up
to
36 se
ssio
ns u
p to
36
wee
ks):
You
pay
noth
ing
afte
r you
pay
you
r ded
uctib
le.
Occ
upat
iona
l the
rapy
visi
t: Yo
u pa
y no
thin
g af
ter y
ou p
ay y
our d
educ
tible
. Ph
ysic
al th
erap
y an
d sp
eech
and
lang
uage
ther
apy
visit
: You
pay
not
hing
aft
er y
ou p
ay
your
ded
uctib
le.
Out
patie
nt S
ubst
ance
Abu
se1
Grou
p th
erap
y vi
sit: Y
ou p
ay n
othi
ng a
fter
you
pay
you
r ded
uctib
le.
Indi
vidu
al th
erap
y vi
sit: Y
ou p
ay n
othi
ng a
fter
you
pay
you
r ded
uctib
le.
Out
patie
nt S
urge
ry1
Ambu
lato
ry su
rgic
al c
ente
r: Yo
u pa
y no
thin
g af
ter y
ou p
ay y
our d
educ
tible
. O
utpa
tient
hos
pita
l: Yo
u pa
y no
thin
g af
ter y
ou p
ay y
our d
educ
tible
. O
ver-
the-
Coun
ter I
tem
s N
ot c
over
edPr
osth
etic
Dev
ices
(bra
ces,
art
ifici
al li
mbs
, etc
.)1Pr
osth
etic
dev
ices
: You
pay
not
hing
aft
er y
ou p
ay y
our d
educ
tible
. Re
late
d m
edic
al su
pplie
s: Y
ou p
ay n
othi
ng a
fter
you
pay
you
r ded
uctib
le.
Rena
l Dia
lysis
Yo
u pa
y no
thin
g af
ter y
ou p
ay y
our d
educ
tible
. Tr
ansp
orta
tion
Not
cov
ered
U
rgen
t Car
e Yo
u pa
y no
thin
g af
ter y
ou p
ay y
our d
educ
tible
.Vi
sion
Serv
ices
Ex
am to
dia
gnos
e an
d tr
eat d
iseas
es a
nd c
ondi
tions
of t
he e
ye (i
nclu
ding
yea
rly
glau
com
a sc
reen
ing)
: You
pay
not
hing
aft
er y
ou p
ay y
our d
educ
tible
. Ey
egla
sses
or c
onta
ct le
nses
aft
er c
atar
act s
urge
ry: Y
ou p
ay n
othi
ng a
fter
you
pay
you
r de
duct
ible
. Pr
even
tive
Care
You
pay
noth
ing
afte
r you
pay
you
r ded
uctib
le.

Ac
tiveS
aver
MSA
(MSA
) Pr
even
tive
Care
(con
tinue
d)
Our
pla
n co
vers
man
y pr
even
tive
serv
ices
, inc
ludi
ng:
Ab
dom
inal
aor
tic a
neur
ysm
scre
enin
g
Alco
hol m
isuse
cou
nsel
ing
Bo
ne m
ass m
easu
rem
ent
Br
east
can
cer s
cree
ning
(mam
mog
ram
)
Card
iova
scul
ar d
iseas
e (b
ehav
iora
l the
rapy
)
Card
iova
scul
ar sc
reen
ings
Cerv
ical
and
vag
inal
can
cer s
cree
ning
Colo
nosc
opy
Co
lore
ctal
can
cer s
cree
ning
s
Depr
essio
n sc
reen
ing
Di
abet
es sc
reen
ings
Feca
l occ
ult b
lood
test
Flex
ible
sigm
oido
scop
y
HIV
scre
enin
g
Med
ical
nut
ritio
n th
erap
y se
rvic
es
O
besit
y sc
reen
ing
and
coun
selin
g
Pros
tate
can
cer s
cree
ning
s (PS
A)
Se
xual
ly tr
ansm
itted
infe
ctio
ns sc
reen
ing
and
coun
selin
g
Toba
cco
use
cess
atio
n co
unse
ling
(cou
nsel
ing
for p
eopl
e w
ith n
o sig
n of
toba
cco-
rela
ted
dise
ase)
Vacc
ines
, inc
ludi
ng fl
u sh
ots,
Hep
atiti
s B sh
ots,
Pne
umoc
occa
l sho
ts
W
elco
me
to M
edic
are"
pre
vent
ive
visit
(one
-tim
e)
Ye
arly
"Wel
lnes
s" v
isit
Any
addi
tiona
l pre
vent
ive
serv
ices
app
rove
d by
Med
icar
e du
ring
the
cont
ract
yea
r will
be
cov
ered
. Ho
spic
e Yo
u pa
y no
thin
g fo
r hos
pice
car
e fr
om a
Med
icar
e-ce
rtifi
ed h
ospi
ce. Y
ou m
ay h
ave
to
pay
part
of t
he c
ost f
or d
rugs
and
resp
ite c
are.

Ac
tiveS
aver
MSA
(MSA
) In
patie
nt H
ospi
tal C
are1
The
copa
ys fo
r hos
pita
l and
skill
ed n
ursin
g fa
cilit
y (S
NF)
ben
efits
are
bas
ed o
n be
nefit
pe
riods
. A b
enef
it pe
riod
begi
ns th
e da
y yo
u're
adm
itted
as a
n in
patie
nt a
nd e
nds w
hen
you
have
n't r
ecei
ved
any
inpa
tient
car
e (o
r ski
lled
care
in a
SN
F) fo
r 60
days
in a
row
. If
you
go in
to a
hos
pita
l or a
SN
F af
ter o
ne b
enef
it pe
riod
has e
nded
, a n
ew b
enef
it pe
riod
begi
ns. Y
ou m
ust p
ay th
e in
patie
nt h
ospi
tal d
educ
tible
for e
ach
bene
fit p
erio
d.
Ther
e's n
o lim
it to
the
num
ber o
f ben
efit
perio
ds.
Our
pla
n co
vers
90
days
for a
n in
patie
nt h
ospi
tal s
tay.
O
ur p
lan
also
cov
ers 6
0 "li
fetim
e re
serv
e da
ys."
The
se a
re "e
xtra
" day
s tha
t we
cove
r. If
your
hos
pita
l sta
y is
long
er th
an 9
0 da
ys, y
ou c
an u
se th
ese
extr
a da
ys. B
ut o
nce
you
have
use
d up
thes
e ex
tra
60 d
ays,
you
r inp
atie
nt h
ospi
tal c
over
age
will
be
limite
d to
90
days
. Yo
u pa
y no
thin
g af
ter y
ou p
ay y
our d
educ
tible
.In
patie
nt M
enta
l Hea
lth C
are
For i
npat
ient
men
tal h
ealth
car
e, se
e th
e "M
enta
l Hea
lth C
are"
sect
ion
of th
is bo
okle
t.Sk
illed
Nur
sing
Faci
lity
(SN
F)
Our
pla
n co
vers
up
to 1
00 d
ays i
n a
SNF
as lo
ng a
s you
pre
viou
sly st
ayed
in a
hos
pita
l for
3
days
. Yo
u pa
y no
thin
g af
ter y
ou p
ay y
our d
educ
tible
.Ho
w m
uch
do I
pay?
Fo
r Par
t B d
rugs
such
as c
hem
othe
rapy
dru
gs: Y
ou p
ay n
othi
ng a
fter
you
pay
you
r de
duct
ible
O
ther
Par
t B d
rugs
: You
pay
not
hing
aft
er y
ou p
ay y
our d
educ
tible

Medical Savings Account Qualified Medical ExpensesQualified medical expenses are the same types of services and products that otherwise could be deducted as medical expenses on your yearly income tax return. Not all qualified medical expenses as defined by the Internal Revenue Service (IRS) will count toward your Medicare medical savings account (MSA) plan’s annual deductible (see lists below).
Only Medicare-covered Part A and Part B services will count toward your Medicare MSA plan’s annual deductible. Please consult the Medicare and You handbook for a complete list of Medicare-covered services.
MSA plans do not include prescription drug coverage, but funds from Medicare MSAs can be used toward drug copays. However, these expenses will not count toward the Medicare MSA plan’s annual
deductible. If you join a Medicare MSA plan, you can also join a Medicare prescription drug plan (standalone PDP) to obtain drug coverage.
Below is a quick reference list of qualified medical expenses that can be reimbursed from a Medicare MSA and will count toward your annual deductible on MSA plans.
• Ambulance services• Blood• Cardiac rehabilitation• Chiropractic services (to correct subluxation only)• Clinical laboratory services• Contact lenses (after cataract surgery only)• Defibrillator (implantable, automatic)• Diabetes supplies*• Doctor services• Durable medical equipment
(also known as DME; includes but not limited to hospital beds, oxygen, walkers, wheelchairs, etc.)• Emergency services• Eyeglasses (after cataract surgery only)• Flu shots• Hearing exams (must be medically necessary)• Home care (excludes custodial care)• Hospital bills• Kidney disease services and supplies (end-stage renal disease patients only)• Mental health care• Physical exams• Physical therapy• Preventive services
(see the Medicare and You handbook for a complete list of services covered)• Pneumococcal shot• Prosthetic/orthotic items• Pulmonary rehabilitation (COPD patients only)• Tests, other than lab tests (includes, but is not limited to X-rays, MRIs, CT scans, EKGs)• Transplants and immunosuppressive drugs**• Urgent care
* Some diabetes supplies are covered under Part D and would not count toward your annual deductible. See the Medicare and You handbook for more information.
**Organ transplant needs to be performed in a Medicare-approved facility
H9788_MRK985 rev Accepted

Below is a quick reference list of qualified medical expenses that can be reimbursed through a Medicare MSA and will NOT count toward the annual deductible on MSA plans.
• Acupuncture• Artificial teeth• Chiropractor (routine)• Contact lenses (not related to
cataract surgery)• Dental services• Eyeglasses (not related to cataract surgery)
• Hearing aids• Insurance premiums • Long-term care• Medicines• Transportation• Wigs
The above lists do not include all qualified medical expenses as defined by the IRS. For a complete list of qualified services and products and for other tax information, call the IRS at 1-800-TAX-FORM (1-800-829-3676). Ask for a free copy of the IRS publication #502, Medical and Dental Expenses.
You can also request the IRS publication #969 to get more information about the tax Form 8853, or visit www.irs.gov on the web and select Forms and Publications to view or print copies of the publications.
You must file Form 1040, U.S. Individual Income Tax Return, along with Form 8853, Archer MSA and Long-Term Care Insurance Contracts, with the IRS for any distributions made from your Medicare MSA account to ensure you are not taxed on your MSA account withdrawals. You must file these tax forms for any year in which an MSA account withdrawal is made, even if you have no taxable income or other reason for filing a Form 1040. MSA account withdrawals for qualified medical expenses are tax-free; account withdrawals for non-medical expenses are subject to both income tax and a fifty (50) percent tax penalty.
Non-Qualified Medical ExpensesThe following list includes items that the IRS deems as non-qualified expenses and cannot be included in calculating your annual medical expense deduction. For a complete list and clarification regarding these items, call the IRS at 1-800-TAX-FORM (1-800-829-3676). Ask for a free copy of the IRS publication #502, Medical and Dental Expenses. You can also request the IRS publication #969 to get more information about the tax Form 8853, or visit www.irs.gov and select Forms and Publications to view or print copies of the publications.
If you use the money in your MSA for non-qualified expenses, it will be taxed as part of your income and will also be subject to an additional fifty percent tax penalty.
• Babysitting and childcare• Controlled substances• Cosmetic surgery• Dancing lessons• Diaper service • Electrolysis or hair removal• Flexible spending account (FSA)• Funeral expenses• Future medical care• Hair transplant• Health club dues• Health coverage tax credit
• Health savings account (HSA)• Household help• Illegal operations and treatments• Maternity clothes• Archer medical savings account (MSA)• Medicine and drugs from other countries• Non-prescription drugs and medicines• Nutritional supplements• Personal use items• Swimming lessons• Teeth whitening• Veterinary fees

HealthNow New York is a Medicare Advantage and PDP plan with a Medicare contract and enrollment depends on contract renewal.
MSA Plans combine a high deductible Medicare Advantage Plan and a trust or custodial savings account (as defined and/or approved by the IRS). The plan deposits money from Medicare into the account. You can use this money to pay for your health care costs, but only Medicare-covered expenses count toward your deductible. The amount deposited is usually less than your deductible amount, so you generally have to pay out-of-pocket before your coverage begins. Medicare MSA Plans don’t cover prescription drugs. If you join a Medicare MSA Plan, you can also join any separate Medicare Prescription Drug Plan. There are additional restrictions to join an MSA plan, and enrollment is generally for a full calendar year unless you meet certain exceptions. Those who disenroll during the calendar year will owe a portion of the account deposit back to the plan. Contact the plan at 1-888-989-9905 (TTY 711) for additional information.
This information is available for free in other languages. Please call our customer service number at 1-888-989-9905 (TTY 711). We’re available 8 a.m. to 8 p.m., 7 days a week from October 1 to February 14, and 8 a.m. to 8 p.m., Monday-Friday, from February 15 to September 30.
Esta información se encuentra disponible gratis en otros idiomas. Comuníquese con nuestros Servicios para Miembros al 1-888-989-9905 para obtener información adicional. Los usuarios de TTY deben llamar al 711. Las horas de atención son 8 a.m. a 8 p.m. los siete dias de las semana, desde Octubre 1 a Febrero 14, y 8 a.m. a 8 p.m. Lunes a Viernes desde Febrero 15 a Septiembre 30.

Medicare Medical Savings Account Fee and Rate Schedule
Interest Rate, Set-Up and Monthly Fee Interest Rate ………………………………………………………………………………… 0.05%
Annual Percentage Yield (APY) …………………………………………………………... 0.05%
Account Set-up Fee …………………………………………………………………… $15.00
Monthly Service Charge for average monthly balance of $1,000 or less...………… Setup and monthly maintenance fees will be paid for you by your health plan during active coverage. If you leave your sponsored plan, but retain your MSA you will be responsible for the monthly service fee of $3.50.
$ 3.50
Requests for Debit Card, Checkbook or Copies of Documents Replacement/Additional Debit Card ……………………………………………………… $ 5.00
Checkbook Reorder Fee …………………………………………………………………... $ 5.00
Copy of Check, Statement or Other Document (per item) ...…………………………… $ 5.00
Other Banking Fees when Applicable ATM Usage Fee (per usage)…………………………………………………..………….
Stop Payment (per request) ……………………………………………..………………… $ 2.00
$ 25.00
Returned Item (per instance) ……….……………………………………………………... $ 25.00
Custodian Check Issuance Fee (deducted from account balance) …………………… $ 25.00
Excess Contribution Reimbursement (deducted from account balance) ………..…… $ 25.00
Attachments/levies/legal requests/subpoenas (per request) ………………………….. $100.00
Statement Reconciliation/Account Research …………………. $20.00 per hr/$10 min charge
See your Medical Savings Account Deposit Agreement and Disclosures for the complete terms and conditions related to your account. Note the fees disclosed will remain in effect until further notice. Interest is credited to participant accounts on the last business day of the month. Monthly service charge is debited from participant accounts on last business day of the month. For additional information regarding these fees, contact your health plan or our service center. Other fees will be deducted from the balance of your Medical Savings Account when incurred. If the account balance is less than $25 at the time of a check issuance request, a fee equal to the account balance will be deducted from the Medical Savings Account balance.
THE BANK OF NEW YORK MELLON MEDICAL SAVINGS ACCOUNT
DEPOSIT AGREEMENT & DISCLOSURE STATEMENT
A Medicare Advantage Medical Savings Account (“MSA” or “Medical Savings Account”) is an individually owned checking-with-interest account at The Bank of New York Mellon (referred to in this document as “us” “we”, “our” and similar terms). Medical Savings Account holders (referred to in this document as “you”, “your”, and similar terms) cannot make deposits into the Medical Savings Account. Medicare, by way of your Medicare Advantage Health Plan, will deposit funds (as part of your Medicare Advantage benefits) by check or electronic transfer into your MSA. Your Medicare Advantage Health Plan, on behalf of the Centers for Medicare and Medicaid Services (“CMS”), is the only entity that can make this deposit; such deposits will be made only once per year. Withdrawals from the Medical Savings Account can be made by way of check or electronic transfer. By opening a Medical Savings Account with us (your “Account”) and providing us with a signed Medical Savings Account Master Signature Card, you agree to be bound by (a) this Deposit Agreement and Disclosure Statement as it may be amended from time to time (this “Agreement”), and (b) our policies and procedures regarding Medical Savings Accounts.
Section 1 General Deposits. Only one deposit per year can be made to your Account; such deposit will be made by your Medicare Advantage Health Plan and will be comprised of funds provided to it by CMS. We may, at our sole discretion, refuse to accept particular instruments as deposits. Deposits are handled by us according to our usual collection practices. Funds deposited to your Account are available in accordance with the Funds Availability provisions below. You agree to accept our account of the amount of any deposit of cash, checks, or other items. If a deposit or part of a deposit is returned unpaid, we will debit your Account and adjust any interest earned. You are liable to us for the amount of any item deposited to your account that is returned and all costs and expenses related to the collection of some or all of the amount from you. Collection of Deposit Items. In receiving items for deposit or collection, we act only as your agent and assume no responsibility beyond the exercise of ordinary care. All items are credited subject to final settlement in cash or credits. If we permit you to withdraw funds from your Account before final settlement has been made for any deposited item, and final settlement is not made, we have the right to charge your Account or obtain a refund from you. In addition, we may charge back any deposited items at any time before settlement for whatever reason. We shall not be liable for any damages resulting from the exercise of these rights. Except as may be attributable to our lack of good faith or failure to exercise ordinary care, we shall not be liable for dishonor resulting from any reversal of credit, return of deposited items or for any damages resulting from any of those actions. Custodial Accounts. You acknowledge that your Account is setup as a custodial account as contemplated by 26 U.S.C. Sections 223 and 408(h) and it is your sole responsibility to

determine the legal effects of opening and maintaining an account of this nature. Interactive Voice Response (IVR). Account information provided on the IVR system may not reflect recent intraday transactions. Power of Attorney. If you wish to name another person to act as your attorney in fact or agent in connection with your Account, you must use our form of Power of Attorney. Fees, Service Charges and Balance Requirements. You agree you are responsible for any fees, charges, balance, or deposit requirements as stated in our fee and rate schedule as amended from time to time. Non-Sufficient Funds. If your Account lacks sufficient available funds to pay a check or preauthorized transfer presented for payment, we may return such check or preauthorized transfer for non-sufficient funds. We may process checks in any order, including from highest dollar amount to lowest dollar amount. Amendments and Alterations. We can change any provision of this Agreement, add new terms to it, and delete terms from it (including but not limited to the Medical Savings Account Rate and Fee Schedule) from time to time. We will give you advance notice of a changed term, new term or deletion in accordance with applicable law. Notices. You are responsible for notifying us of any address or name changes, or other information affecting your Account. Unless we agree otherwise, your notices to us must be in writing, signed by you, and must contain enough information to allow us to identify the Account. Notice sent by you to us is not effective until we have received it and have a reasonable opportunity to act on it. Written notice sent by us to you is effective when mailed to the last address supplied to us in writing. Closing Account. We may close the Account at any time, with or without cause, by sending you notice and a check for the balance in our possession to which you are entitled. We will close your Account if it is in overdraft status for 60 consecutive days. At our discretion, we have the authority to pay an otherwise properly payable check, which is presented after the closing of your Account. Beneficiary Designations. You may designate one or more persons or entities as death beneficiary of your Account (referred to as “Primary Beneficiaries”) and may also designate one or more persons to receive your Account if no Primary Beneficiary survives you (referred to as “Contingent Beneficiaries”). Beneficiary designations can be made only on a form provided by or acceptable to us and will only be effective when filed with us during your lifetime. If you die before you receive all of the amounts in your Account, payments from your Account will be made according to your beneficiary designation(s). The following procedures will be used in processing beneficiary designations: 1. If no percentages are assigned to beneficiaries in a Beneficiary classification (Primary or Contingent), the Beneficiaries within such class will share equally.

2. If the percentage total for each Beneficiary classification (Primary and Contingent) does not equal 100%, any remaining percentages will be divided equally among the Beneficiaries within such class. 3. If in a Beneficiary classification (Primary or Contingent) a Beneficiary dies before distribution of the account is made, that deceased Beneficiary’s designated share shall be divided equally among the surviving Beneficiary(ies) within the class. 4. If no Beneficiaries are named or if all the named Beneficiaries predecease the account holder, the Account will be paid to the spouse of the account holder if then living or if the spouse is not then living to the estate of the account holder. Transfers and Assignments. You cannot assign or transfer any interest in your Account unless we first agree in writing. Applicable Laws and Regulations. You understand that this Agreement is governed by the laws of the Commonwealth of Massachusetts, unless federal law controls. Changes in these laws may change the terms and conditions of your Account. Automated Clearing House (ACH) Transactions. If you are a party to an Automated Clearing House (ACH) entry, you acknowledge and agree that any such entry will be governed by the National Automated Clearing House Association (NACHA) Operating Rules, Rules of any local ACH, and the Rules of any other system through which the entry is made. Other payments orders you make may be governed by Article 4A of the Uniform Commercial Code. Under NACHA Rules, we are not required to give you next day notice of the receipt of an ACH entry and we will not do so. We will notify you in your Account Statement. If we credit your Account for an ACH entry the credit is provisional until we receive the final settlement for the item or payment order. We are entitled to a refund of the amount credited if we do not receive the final settlement or if we credit your Account by mistake. You agree that we may exercise our option to reverse the credit or require that you reimburse us by way of direct payment. Stop Payments. If you request us to stop payment on a check you have written, you will give us a written request within 14 days of making the request. If you fail to confirm an oral stop payment request in writing within 14 days, we reserve the right to cancel the request. We must receive the request in a time and way that gives us a reasonable opportunity to act on it. Stop payments are effective for twelve (12) months. You will be charged a fee every time you request a stop payment, even if it is a continuation of a previous stop payment request. Only the person who requested the stop payment can release a stop payment request. Our acceptance of a stop payment request does not constitute a representation by us that the item has not already been paid or that we have had a reasonable opportunity to act on the request. Checks. All negotiable paper (“checks”) presented for deposit must be in a format that can be processed by our processing system and we may refuse to accept any check that does not meet this requirement. All endorsements on the reverse side of any check deposited into your Account or on any check issued by you must be placed on the left side of the check when looking at it from the front, and must be placed so as to not go beyond an area located 1 ½ inches

from the left edge of the check when looking at if from the front. It is your responsibility to ensure that this requirement is met and you are responsible for any loss incurred by us for failure of an endorsement to meet this requirement. Stale, Postdated or Overdraft Checks. We reserve the right to pay or dishonor a check more than six (6) months old without prior notice to you. You agree not to postdate any check drawn on the Account; if you do and the check is presented for payment before the date of the check, we may pay it or return it unpaid. We are not liable for paying any stale, postdated or overdraft check. Any damages you incur that we may be liable for are limited to actual damages not to exceed the amount of the check. Check Safekeeping. Unless we indicate otherwise, your canceled checks will be retained by us and destroyed after a reasonable time period or as required by law. If for any reason we cannot provide you with a copy of a check, our liability, to the extent permitted by law, will be limited to the lesser of the face amount of the check or the actual damages sustained by you. Statements. We will provide you with a periodic statement showing the Account activity. You will notify us within 30 days after we mail or otherwise make the statement available to you of any discrepancies. If you fail to notify us, you will have no claim against us. However, if the discrepancy is the result of an electronic fund transfer, the provisions of this Agreement regarding such transfers will control its resolution. If you do not receive a statement from us because you have failed to claim it or have supplied us with an incorrect address, we may stop sending your statements until you specifically make written request that we resume sending your statements and you supply us with a proper address. We will send Account statements for your Accounts to the latest address shown on our records for the Account to which the statement relates. In preparing your statement we rely upon and incorporate information about your Account that we receive from third parties. We shall have no liability to you for (i) errors on your statement resulting from inaccurate information provided to us by a third party or (ii) delays in posting transactions on your statement due to the actions or failure to act of third parties. Restrictive Legends. We are not required to honor any restrictive legend on checks you write unless we have agreed to the restriction in a writing signed by one of our officers. Examples of restrictive legends are “must be presented within 90 days” or “not valid for more than $1,000.00.” No Waiver. You understand and agree that no delay or failure on our part to exercise any right, remedy, power or privilege available to us under this Agreement or law shall affect or preclude our future exercise of that right, remedy, power or privilege. Information Sharing. You authorize us to make any inquiries not prohibited by law about your deposit account experience at other financial institutions. You authorize us to share information about your Account with third parties routinely requesting that we verify the existence and nature of your Account and our experience concerning your management of your Account. We may share Account information with your Medicare Advantage health plan insurer and our service providers for Account administration and processing purposes. Also, see the section on

Electronic Fund Transfers below. Subject to any limitations imposed by law, you also authorize us to provide our affiliates, and others with a legal privilege, with other information about you, such as information obtained from deposit or loan applications, consumer reporting agencies, or other outside sources. Withdrawal Notice Requirements. We have the right to require seven (7) days’ prior written notice of your intent to withdraw any funds from your Account. Contribution Limits. Except in the case of certain rollover contributions, and except as otherwise permitted by law or guidance issued by the U.S. government, no contribution will be accepted unless it is from CMS through your Medicare Advantage Health Plan for a Medical Savings account. Use of Funds. We are not required to determine whether the distribution is for the payment or reimbursement of qualified medical expenses. Only you are responsible for substantiating that the distribution is for qualified medical expenses and you must maintain records sufficient to show that the distribution is tax-free. Account Assets. No part of the Account assets will be invested in life insurance contracts. The assets of the Account will not be commingled with other property except in a common trust fund or common investment fund. Forfeiture. Your interest in your Account balance is nonforfeitable. Deposits and Payments. We may (a) accept deposits to your Account via wire or other electronic fund transfers from your Medicare Advantage Health Plan, on behalf of CMS, and (b) make payments from your Account via electronic fund transfer to any person you have authorized to receive such payments; we are not responsible for determining whom you have authorized to make electronic withdrawals from your Account. To the extent permitted by law, you agree that we will not have any liability for losses you incur as a result of such wire or electronic fund transfers. Information. Unless you direct us otherwise, we will permit your Medicare Advantage Health Plan or third party administrator to initiate electronic withdrawals from your Account to pay qualified medical expenses on your behalf. Not all Health Plans have this capacity; check with your Medicare Advantage Health Plan regarding this. If you do not wish your Health Plan to have such access or to make such withdrawals, please contact us at 888-769-4788, M-F, 8 a.m. to 11 p.m. Eastern Time. Business Day. For purposes of this Agreement, Business Days are any day except Saturday, Sunday, federal holidays, and any day we are not open in the U.S. to conduct substantially all of our business functions. Communication and Service. If we need to contact you to service your Account, you authorize us (and our affiliates, agents and contractors) to contact you at any number you provide, from which

you call us, or at which we believe we may reach you. We may contact you in any way, such as calling or texting. We may contact you using an automated dialer or prerecorded messages. We may contact you on a mobile, wireless or similar device even if you are charged for it. We may monitor and record any calls between you and us. We may also email you at email address(es) you provide to us. Cross Border Transactions and Currency Conversion Assessment. A Cross-border Transaction refers to any transaction on your Medical Savings Account Debit Card that is processed by MasterCard in which the country code of the Issuer differs from the country code of the merchant. The transaction amount shall be itemized on your statement. The charges are (1) the Cross-border Assessment, and (2) the Currency Conversion Assessment. The Cross-border Assessment is the amount that U.S. card issuers are required to pay MasterCard on all Cross-border Transactions; it will be in an amount equal to 8/10ths of 1 percent of the amount of the transaction, as calculated by MasterCard. The Currency Conversion Assessment is the currency conversion procedure selected by MasterCard, and may differ from the applicable currency conversion on the date of the transaction or when the transaction is posted to your account; it will be in an amount equal to 2/10ths of 1 percent of the transaction amount, as calculated by MasterCard. Return of Incorrect Distribution. Requests for the return of an incorrect distribution must be submitted to us on the forms we specify before we can process such requests. We will not accept a return of a distribution that was made from an account at another institution or that was made from an account that was closed after the distribution was made. Adjustments. You agree that the Medicare Advantage Health Plan that deposited funds to your Account on your behalf may debit your Account to correct errors in such deposits. Other Fees. We and our service provider, a company independent from us, work together to make MSAs available to you and other account holders; in doing so we and our service provider perform various services for each other for which each pays the other a fee. State Abandoned and Unclaimed Property Laws. The funds in your Account may be transferred to the appropriate state if no activity occurs in the account within the time period specified by state law.
Section 2 -- Truth in Savings Variable Rate Information �� Your interest rate and annual percentage yield (“APY”) may change. �� At our discretion, we may change the interest rate on your Account at any time. �� There are no maximum or minimum interest rate limits for your Account.

Compounding and Crediting �� Interest will be compounded monthly and will be paid to your Account monthly. �� If you close your Account before accrued interest is credited, you will NOT receive this
accrued interest. Minimum Balance Computation � In instances where a minimum balance service charge applies (see the Medical Savings
Account Fee and Rate Schedule for information on whether this applies to your Account), we calculate the monthly balance for the minimum balance service charge by adding up the current ledger balance for your Account as of the end of the day for each calendar day in the month, and then dividing the sum by the number of calendar days in the month.
Balance Computation Method �� We use the daily balance method to calculate the interest on your Account. This method
applies a daily periodic rate to the principal in the Account each day. Accrual on Noncash Deposits �� Interest begins to accrue no later than the business day after the day we post the deposit. Fees and Charges �� Please see the Medical Savings Account Fee and Rate Schedule for information on fees and
charges that may be assessed against your Account.
Section 3 – Customer Identification Program Notice Important Information About Procedures
for Opening a New Account To help the government fight the funding of terrorism and money laundering activities, Federal Law requires all financial institutions to obtain, verify and record information that identifies each individual or entity that opens an Account. What this means for you: When you open an Account, we will ask for your name, address, date of birth, and other information that will allow us to identify you. We also may ask to see your driver’s license, or other identifying documents.
Section 4 -- Electronic Funds Transfers The Term electronic fund transfer means any transfer of funds that is initiated through an electronic terminal, telephone, computer, or magnetic tape for the purposes of directing a financial institution to debit or credit an account. You can arrange with third parties for electronic transfers from or to your Account if they are willing to enter into such arrangements

with you. The only electronic fund transfer service involving your Account that you can arrange for directly with us is the use of a Debit Card. The types of electronic fund transfers that can occur with your Account are listed below. Types of Electronic Fund Transfers �� Debit Card - Purchases By opening an Account, you are requesting, and will be provided
with, a Debit Card (or simply “Card”) for use with your Account; you may use it to purchase goods and services from certain health care providers and pharmacies that have arranged to accept your Card as a means of payment. You may authorize us to issue a Debit Card to someone you specify (an “Authorized User”); use of the Debit Card by the Authorized User will be subject to all the provisions of this Agreement. Purchases made with your Card are referred to as “Point of Sale” or “POS” transactions, and will cause your Account to be debited for the amount of the purchase. We have the right to return any check or other item drawn on your Account to ensure there are funds available to pay for the Card transactions. We will not pay a Card transaction if your Account does not have funds sufficient to pay for the entire transaction. You will be provided with a Personal Identification Number (“PIN”) for use with the Card, which you can change.
�� Debit Card – Automated Teller Machines This service is available only to members of
certain health plans; please review the cover letter from the welcome kit for further information. If this service is available to you, then you can use your Debit Card at an Automated Teller Machine (“ATM”) to withdraw cash from your Account, and check your Account balance. Some of these services may not be available at all ATMs. We do not own or operate any ATMs, so you will use ATMs owned and operated by other institutions. When you use your Debit Card at an ATM, you may be charged a fee by the ATM operator or any network used, and you may be charged a balance inquiry fee even if you do not complete a fund transfer. Account balance information disclosed to you at an ATM may not reflect recent transactions.
�� Electronic Check Conversion In this service, you may authorize a merchant or other payee
to make a one-time electronic payment from your Account using information from your check to (i) pay for purchases; (ii)pay bills.
�� Electronic Check Conversion -- Re-Presented Check If your paper check has been returned
unpaid to a payee due to insufficient or unavailable funds, the payee may re-present the paper check as an electronic check transaction which will be debited against your Account.
�� Preauthorized Transfer Services You may arrange with a third party for the preauthorized
automatic payment of funds to or from your Account. � Transfer Services (Note: this service is not available at present - you will be advised when it
is offered).

Limitations on Transactions �� You may buy up to $3,000 worth of goods and services each day by way a POS transaction
with your Card. �� You may withdraw no more than $500 per day using your Card at one or more ATMs. Some
ATM operators or networks may set a lower limit for withdrawals. �� We reserve the right to impose limitations for security purposes at any time. �� Unless we tell you otherwise, you can use your Card for POS transactions only from vendors
we believe provide products or services that constitute qualified medical expenses as defined by section 223 of the Internal Revenue Code. This limitation does not apply to the use of your checks.
Right to Receive Documentation of Your Transfers
Transaction Receipts. Upon completing a POS transaction, you will receive a printed receipt documenting the transaction (unless you have chosen not to get a paper receipt). These receipts should be retained to verify that a transaction was performed. You may not receive receipts for transactions you make by telephone, mail or via the internet. Receipts may not be provided for Purchases of $15.00 or less, or for transactions performed outside the United States.
ATM Receipts. ATM operators should provide you with a receipt when you use your Debit
Card at any of their ATMs. These receipts should be retained to verify that a transaction was performed. Receipts may not be provided for transactions performed outside the United States.
Periodic Statements. You will get a periodic account statement.
Rights Regarding Preauthorized Transfers From Your Account
Right to Stop Payment and Procedure for Doing so. If you arranged in advance to make regular payments out of your Account, you can stop any of these payments. To stop a payment:
Call us at 888-769-4788, or write us at BenefitWallet MSA Contact Center, P..O Box 1584, Secaucus, NJ 07094-1584 in time for us to receive your request 3 business days or more before the payment is scheduled to be made. If you call, we may also require you to put your request in writing and get it to us within 14 days after you call.
Notice of Varying Amounts. If these regular payments may vary in amount, the person you are going to pay will tell you, 10 days before each payment, when it will be made and how much it will be. You may choose instead to get this notice only when the payment would differ by more than a certain amount from the previous payment, or when the amount would

fall outside certain limits you set.
Our Liability for Failure to Stop Payment of Preauthorized Transfer. If you order us to stop one of these payments 3 business days or more before the transfer is scheduled, and we do not do so, we will be liable for your losses or damages.
Loss or Theft of Your Account Debit Card
Your Responsibility to Notify us of Loss or Theft. If you believe your The Bank of New York Mellon Card or PIN has been lost or stolen, call us at 888-769-4788, M-F 8 a.m. to 11 p.m. Eastern Time, or write us at BenefitWallet MSA Contact Center, PO Box 1584, Secaucus, NJ 07094-1584. After hours, you may report a lost of stolen card by calling 800-264-5578. You should also call the number or write to the address listed above if you believe a transfer has been made using information from your check without your permission.
Zero Liability Rules. If you notify us of an unauthorized transaction involving your Card,
and the unauthorized transaction took place on the MasterCard or Maestro network, zero liability will be imposed on you for the unauthorized transaction. In order to qualify for zero liability, you must have exercised reasonable care in safeguarding your card from the risk of loss or theft, you must not have reported two or more incidents of unauthorized use within the preceding 12 months, and your Account must be in good standing. If you do not qualify for the Zero Liability Rule, the rules below will apply.
Your Liability in Other Cases. (If you do not qualify for the Zero Liability Rules listed
above, then this paragraph and the next two paragraphs apply.) Tell us AT ONCE if you believe your Card or PIN has been lost or stolen, or if you believe that an electronic fund transfer has been made without your permission using information from your check. Telephoning is the best way of keeping your possible losses down. You could lose all the money in your Account. If you tell us within two (2) business days after you learn of the loss or theft of your card or PIN, you can lose no more than $50 if someone used your Card or PIN without your permission. If you do NOT tell us within two (2) business days after you learn of the loss or theft of your Card or PIN, and we can prove we could have stopped someone from using your Card or PIN without your permission if you had told us, you could lose as much as $500. Also, if your statement shows transfers that you did not make, including those made by card, code or other means, tell us at once. If you do not tell us within 60 days after the statement was mailed to you, you may not get back any money you lost after the 60 days if we can prove that we could have stopped someone from taking the money if you had told us in time. If a good reason (such as a long trip or a hospital stay) kept you from telling us, we will extend the time periods.

Illegal Use of Your Account Debit Card
You agree not to use your Card for any illegal transactions. Errors or Questions About Your Electronic Fund Transactions
In Case of Errors or Questions About Your Electronic Transfers Telephone us at 888-769-4788, or write us at BenefitWallet MSA Contact Center, PO Box 1584, Secaucus, NJ 07094-1584 as soon as you can, if you think your statement or receipt is wrong or if you need more information about a transfer listed on the statement or receipt. We must hear from you no later than 60 days after we sent the FIRST statement on which the problem or error appeared. (1) Tell us your name and Account number (if any). (2) Describe the error or the transfer you are unsure about, and explain as clearly as you can why you believe it is an error or why you need more information. (3) Tell us the dollar amount of the suspected error.
�� If you tell us orally, we may require that you send us your complaint or question in writing within 10 business days.
�� We will determine whether an error occurred within 10 days after we hear from you and will correct any error promptly. If we need more time, however, we may take up to 45 days to investigate your complaint or question. If we decide to do this, we will credit your Account within 10 days for the amount you think is in error, so that you will have the use of the money during the time it takes us to complete our investigation. If we ask you to put your complaint or question in writing and we do not receive it within 10 business days, we may not credit your Account.
�� We will tell you the results within three (3) business days after completing our investigation. If we decide that there was no error, we will send you a written explanation. You may ask for copies of the documents that we used in our investigation.
�� Unless otherwise provided in this Agreement, you may not stop payment of electronic fund transfers. Therefore, you should not employ electronic access for purchases or services unless you are satisfied that you will not need to stop payment.
Liability for Failure to Complete Transaction �� If we do not complete a transfer to or from your Account on time or in the correct amount
according to our agreement with you, we will be liable for your losses or damages. �� However, there are some exceptions. We will NOT be liable, for instance-
o If, through no fault of ours, you do not have enough money in your Account to make

the transfer.
o If the electronic terminal or system was not working properly and you knew about the breakdown when you started the transfer.
o If circumstances beyond our control (such as fire or flood) prevent the transfer, despite reasonable precautions that we have taken.
o If the ATM you use does not have enough cash.
o If we have terminated our agreement with you.
o When your Card has been reported lost or stolen or we have reason to believe that something is wrong with a transaction.
o If we received inaccurate or incomplete information needed to complete a transaction.
o In the case of preauthorized transfers, we will not be liable where there is a breakdown of the system that would normally handle the transfer.
o If the funds in the Account are subject to legal action preventing a transfer from or to your Account.
o There may be other exceptions provided by applicable law.
Charges for Transfers or the Right to Make Transfers �� We reserve the right to impose a fee and to change fees upon notice to you.
Amending or Terminating Your Electronic Fund Transfer Service � We can terminate your use of the Debit Card at any time, without giving you prior notice
(unless prior notice is required by law). In such event, you will promptly surrender the Card to us.
Miscellaneous � Your initiation of certain electronic fund transfers from your Account will, except as
otherwise noted in this document, effectively eliminate your ability to stop payment of the transfer.
Section 5-- Funds Availability
Definitions � The term “check” does not include checks not payable in U.S. money or checks drawn on
offices of organizations or banks outside the U.S.

General Availability Rule � Our policy is to make funds from cash and check deposits made to your account available to
you on the first business day after the day we receive the deposit. Electronic direct deposits will be available on the first business day after the day we receive the deposit. Once the funds are available, you can withdraw them in cash and we will use them to pay checks that you have written.
Determining the Availability of a Deposit � If a deposit is made before 1:00 pm Eastern Time on a business day that we are open, we will
consider that day to be the day of the deposit. However, if a deposit is made on or after 1:00 pm Eastern Time or on a day we are not open, we will consider that the deposit was made on the next business day we are open.
Section 6 Check 21 Information
Substitute Checks and Your Rights What is a substitute check? To make check processing faster, federal law permits banks to replace original checks with “substitute checks.” These checks are similar in size to original checks with a slightly reduced image on the front and back of the original check. The front of a substitute check states: “This is a legal copy of your check. You can use it the same way you would use the original check.” You may use a substitute check as proof of payment just like the original check. Some or all of the checks that you receive back from us may be substitute checks. This notice describes rights you have when you receive substitute checks from us. The rights in this notice do not apply to original checks or to electronic debits to your Account. However, you have rights under other law with respect to those transactions. What are my rights regarding substitute checks? In certain cases, federal law provides a special procedure that allows you to request a refund for losses you suffer if a substitute check is posted to your Account (for example, if you think that we withdrew the wrong amount from your Account or that we withdrew money from your Account more than once for the same check). The losses you may attempt to recover under this procedure may include the amount that was withdrawn from your Account and fees that were charged as a result of the withdrawal (for example, bounced checks fees). The amount of your refund under this procedure is limited to the amount of your loss or the amount of the substitute check, whichever is less. You also are entitled to interest on the amount of your refund if your Account is an interest-bearing account. If your loss exceeds the amount of the substitute check, you may be able to recover additional amounts under other law.

If you use this procedure, you may receive up to $2,500 of your refund (plus interest if your Account earns interest) within 10 business days after we receive your claim and the remainder of your refund (plus interest if your Account earns interest) not later than 45 calendar days after we received your claim. We may reverse the refund (including any interest on the refund) if we later are able to determine that the substitute check was correctly posted to your Account. How do I make a claim for a refund? If you believe you have suffered a loss relating to a substitute check that you received and that was posted to your Account, please contact us at 888-769-4788, or write us at BenefitWallet MSA Contact Center, PO Box 1584, Secaucus, NJ 07094-1584. You must contact us within 40 calendar days of the date that we mailed (or otherwise delivered by a means to which you agreed) the substitute check in question or the Account statement showing that the substitute was posted to your Account, whichever is later. We will extend this time period if you were not able to make a timely claim because of extraordinary circumstances. Your claim must include: � A description of why you have suffered a loss (for example, you think the amount withdrawn
was incorrect); � An estimate of the amount of your loss; � An explanation of why the substitute check you received is insufficient to confirm that you
suffered a loss; and � A copy of the substitute check and/or the following information to help us identify the
substitute check: the check number, the name of the person to whom you wrote the check and the amount of the check.
7/31/2014

FACTS WHAT DOES THE BANK OF NEW YORK MELLON DO WITH YOUR PERSONAL INFORMATION?
Rev. June 2014
Why?
Financial companies choose how they share your personal information. Federal law gives consumers the right to limit some but not all sharing. Federal law also requires us to tell you how we collect, share, and protect your personal information. Please read this notice carefully to understand what we do.
What?
The types of personal information we collect and share depend on the product or service you have with us. This information can include:
• Social Security number• Account balances• Payment history• Transaction history• Checking account information
When you are no longer our customer, we continue to share your information as described in this notice.
How?
All financial companies need to share customers’ personal information to run their everyday business. In the section below, we list the reasons financial companies can share their customers’ personal information; the reasons The Bank of New York Mellon chooses to share; and whether you can limit this sharing.
Reasons we can share your personal information Does The Bank of New York Mellon share?
Can you limit this sharing?
For our everyday business purposes— such as to process your transactions, maintain your account(s), respond to court orders and legal investigations, or report to credit bureaus
Yes No
For our marketing purposes— to offer our products and services to you Yes No
For joint marketing with other financial companies No No
For our affiliates’ everyday business purposes— information about your transactions and experiences
Yes No
For our affiliates’ everyday business purposes— information about your creditworthiness No No
For our affiliates to market to you No NoFor nonaffiliates to market to you No No
Questions? Call 888-769-4788

Page 2
Who we areWho is providing this notice? The Bank of New York Mellon is providing this notice to
customers of Medicare Medical Savings Accounts.
What we doHow does The Bank of New York Mellon protect my personal information?
To protect your personal information from unauthorized access and use, we use security measures that comply with federal law. These measures include computer safeguards and secured files and buildings.
How does The Bank of New York Mellon collect my personal information?
We collect your personal information, for example, when you• Open an account• Make deposits or withdrawals from your account • Use your credit or debit card • Provide account information • Give us your contact information
We also collect your personal information from other parties, such as credit bureaus, affiliates, or other companies.
Why can’t I limit all sharing? Federal law gives you the right to limit only• Sharing for affiliates’ everyday business purposes—
information about your creditworthiness• Affiliates from using your information to market to you• Sharing for nonaffiliates to market to you
State laws and individual companies may give you additional rights to limit sharing.
DefinitionsAffiliates Companies related by common ownership or control. They can
be financial and nonfinancial companies.Nonaffiliates Companies not related by common ownership or control. They
can be financial and nonfinancial companies.• The Bank of New York Mellon does not share
information with nonaffiliates so they can market to you.
Joint marketing A formal agreement between nonaffiliated financial companies that together market financial products or services to you.
• The Bank of New York Mellon doesn’t jointly market.
Other important informationThis notice applies to individual consumers who are customers or former customers. This notice replaces all previous notices of our consumer privacy policy, and may be amended at any time. We will keep you informed of changes or amendments as required by law.


Summary of Benefits
S1140
2015 SmartSaver Rx PDP


Sum
mar
y of
Ben
efits
SM
ARTS
AVER
RX
PDP
VALU
E (P
DP) A
ND
SMAR
TSAV
ER R
X PD
P (P
DP)
Janu
ary
1, 2
015
- Dec
embe
r 31,
201
5 (a
Med
icar
e Pr
escr
iptio
n Dr
ug p
lan
(PDP
) offe
red
by H
EALT
HNO
W N
EW Y
ORK
INC.
with
a M
edic
are
cont
ract
) Th
is bo
okle
t giv
es y
ou a
sum
mar
y of
wha
t we
cove
r and
wha
t you
pay
. It d
oesn
't lis
t eve
ry se
rvic
e th
at w
e co
ver o
r list
eve
ry
limita
tion
or e
xclu
sion.
To
get a
com
plet
e lis
t of s
ervi
ces w
e co
ver,
call
us a
nd a
sk fo
r the
"Evi
denc
e of
Cov
erag
e."
You
have
cho
ices
abo
ut h
ow to
get
you
r Med
icar
e pr
escr
iptio
n dr
ug b
enef
its
O
ne c
hoic
e is
to g
et p
resc
riptio
n dr
ug c
over
age
thro
ugh
a M
edic
are
Pres
crip
tion
Drug
Pla
n, li
ke S
mar
tSav
er R
x PD
P Va
lue
(PDP
) and
Sm
artS
aver
Rx
PDP
(PDP
).
An
othe
r cho
ice
is to
get
you
r pre
scrip
tion
drug
cov
erag
e th
roug
h a
Med
icar
e Ad
vant
age
Plan
(lik
e an
HM
O o
r PPO
) or
anot
her M
edic
are
heal
th p
lan
that
offe
rs M
edic
are
pres
crip
tion
drug
cov
erag
e. Y
ou g
et a
ll of
you
r Par
t A a
nd P
art B
co
vera
ge, a
nd p
resc
riptio
n dr
ug c
over
age
(Par
t D),
thro
ugh
thes
e pl
ans.
Ti
ps fo
r com
parin
g yo
ur M
edic
are
choi
ces
This
Sum
mar
y of
Ben
efits
boo
klet
giv
es y
ou a
sum
mar
y of
wha
t Sm
artS
aver
Rx
PDP
Valu
e (P
DP) a
nd S
mar
tSav
er R
x PD
P (P
DP)
cove
r and
wha
t you
pay
.
If
you
wan
t to
com
pare
our
pla
n w
ith o
ther
Med
icar
e he
alth
pla
ns, a
sk th
e ot
her p
lans
for t
heir
Sum
mar
y of
Ben
efits
bo
okle
ts. O
r, us
e th
e M
edic
are
Plan
Fin
der o
n ht
tp:/
/ww
w.m
edic
are.
gov.
If yo
u w
ant t
o kn
ow m
ore
abou
t the
cov
erag
e an
d co
sts o
f Orig
inal
Med
icar
e, lo
ok in
you
r cur
rent
"M
edic
are
& Y
ou"
hand
book
. Vie
w it
onl
ine
at h
ttp:
//w
ww
.med
icar
e.go
v or
get
a c
opy
by c
allin
g 1-
800-
MED
ICAR
E (1
-800
-633
-422
7), 2
4 ho
urs a
day
, 7 d
ays a
wee
k. T
TY u
sers
shou
ld c
all 1
-877
-486
-204
8.
Sect
ions
in th
is b
ookl
et
Th
ings
to K
now
Abo
ut S
mar
tSav
er R
x PD
P Va
lue
(PDP
) and
Sm
artS
aver
Rx
PDP
(PDP
)
Mon
thly
Pre
miu
m, D
educ
tible
, and
Lim
its o
n Ho
w M
uch
You
Pay
for C
over
ed S
ervi
ces
Pr
escr
iptio
n Dr
ug B
enef
its
This
docu
men
t is a
vaila
ble
in o
ther
form
ats s
uch
as B
raill
e an
d la
rge
prin
t.
This
docu
men
t may
be
avai
labl
e in
a n
on-E
nglis
h la
ngua
ge. F
or a
dditi
onal
info
rmat
ion,
cal
l us a
t 1-8
88-9
89-9
905.
Est
e do
cum
ento
pue
de se
r disp
onib
le e
n ot
ros i
diom
as a
part
e de
ingl
es.
Para
mas
info
rmac
ion
llam
enos
al 1
-888
-989
-990
5 Th
ings
to K
now
Abo
ut S
mar
tSav
er R
x PD
P Va
lue
(PDP
) and
Sm
artS
aver
Rx
PDP
(PDP
) Y0
086_
COM
348
Acce
pted

Hour
s of O
pera
tion
Fr
om O
ctob
er 1
to F
ebru
ary
14, y
ou c
an c
all u
s 7 d
ays a
wee
k fr
om 8
:00
a.m
. to
8:00
p.m
. Eas
tern
tim
e.
Fr
om F
ebru
ary
15 to
Sep
tem
ber 3
0, y
ou c
an c
all u
s Mon
day
thro
ugh
Frid
ay fr
om 8
:00
a.m
. to
8:00
p.m
. Eas
tern
tim
e.
Smar
tSav
er R
x PD
P Va
lue
(PDP
) and
Sm
artS
aver
Rx
PDP
(PDP
) Pho
ne N
umbe
rs a
nd W
ebsi
te
If
you
are
a m
embe
r of t
his p
lan,
cal
l tol
l- fr
ee 1
-888
-787
-239
0 (T
TY 7
11).
If
you
are
not a
mem
ber o
f thi
s pla
n, c
all t
oll-
free
1-8
88-9
89-9
905
(TTY
711
).
Our
web
site:
htt
p://
ww
w.h
ealth
now
ny.c
om/m
edic
are
Who
can
join
? To
join
Sm
artS
aver
Rx
PDP
Valu
e (P
DP) o
r Sm
artS
aver
Rx
PDP
(PDP
), yo
u m
ust b
e en
title
d to
Med
icar
e Pa
rt A
, be
enro
lled
in
Med
icar
e Pa
rt B
, and
live
in o
ur se
rvic
e ar
ea. O
ur se
rvic
e ar
ea in
clud
es th
e fo
llow
ing:
New
Yor
k.
Whi
ch d
rugs
are
cov
ered
? Yo
u ca
n se
e th
e co
mpl
ete
plan
form
ular
y (li
st o
f Par
t D p
resc
riptio
n dr
ugs)
and
any
rest
rictio
ns o
n ou
r web
site
(htt
p://
ww
w.h
ealth
now
ny.c
om/m
edic
are)
. Or,
call
us a
nd w
e w
ill se
nd y
ou a
cop
y of
the
form
ular
y.
How
will
I de
term
ine
my
drug
cos
ts?
Our
pla
n gr
oups
eac
h m
edic
atio
n in
to o
ne o
f fiv
e "t
iers
." Y
ou w
ill n
eed
to u
se y
our f
orm
ular
y to
loca
te w
hat t
ier y
our d
rug
is on
to
det
erm
ine
how
muc
h it
will
cos
t you
. The
am
ount
you
pay
dep
ends
on
the
drug
's tie
r and
wha
t sta
ge o
f the
ben
efit
you
have
re
ache
d. L
ater
in th
is do
cum
ent w
e di
scus
s the
ben
efit
stag
es th
at o
ccur
aft
er y
ou m
eet y
our d
educ
tible
: Ini
tial C
over
age,
Co
vera
ge G
ap, a
nd C
atas
trop
hic
Cove
rage
. W
hich
pha
rmac
ies c
an I
use?
W
e ha
ve a
net
wor
k of
pha
rmac
ies a
nd y
ou m
ust g
ener
ally
use
thes
e ph
arm
acie
s to
fill y
our p
resc
riptio
ns fo
r cov
ered
Par
t D
drug
s.
You
can
see
our p
lan'
s pha
rmac
y di
rect
ory
at o
ur w
ebsit
e (h
ttp:
//w
ww
.hea
lthno
wny
.com
/med
icar
e). O
r, ca
ll us
and
we
will
send
yo
u a
copy
of t
he p
harm
acy
dire
ctor
y.

Sum
mar
y of
Ben
efits
Rep
ort
for C
ontr
act S
1140
, Pla
ns 0
01 a
nd 0
02
Smar
tSav
er R
x PD
P Va
lue
(PDP
) Sm
artS
aver
Rx
PDP
(PDP
) M
ON
THLY
PRE
MIU
M, D
EDU
CTIB
LE, A
ND
LIM
ITS
ON
HO
W M
UCH
YO
U P
AY F
OR
COVE
RED
SERV
ICES
Ho
w m
uch
is th
e m
onth
ly p
rem
ium
? $8
0.20
per
mon
th.
$82.
10 p
er m
onth
.
How
muc
h is
the
dedu
ctib
le?
$320
per
yea
r for
Par
t D p
resc
riptio
n dr
ugs.
Th
is pl
an d
oes n
ot h
ave
a de
duct
ible
.
Heal
thN
ow N
ew Y
ork
is a
stan
d-al
one
pres
crip
tion
drug
pla
n pl
an w
ith a
Med
icar
e co
ntra
ct. E
nrol
lmen
t in
Heal
thN
ow d
epen
ds o
n co
ntra
ct re
new
al.
PRES
CRIP
TIO
N D
RUG
BEN
EFIT
S
Initi
al C
over
age
Afte
r you
pay
you
r yea
rly d
educ
tible
, you
pay
the
follo
win
g un
til y
our t
otal
yea
rly d
rug
cost
s rea
ch $
2,96
0.
Tota
l yea
rly d
rug
cost
s are
the
tota
l dru
g co
sts p
aid
by
both
you
and
our
Par
t D p
lan.
Yo
u m
ay g
et y
our d
rugs
at n
etw
ork
reta
il ph
arm
acie
s and
m
ail o
rder
pha
rmac
ies.
St
anda
rd R
etai
l Cos
t-Sh
arin
g
Tier
O
ne-m
onth
su
pply
Th
ree-
mon
th
supp
ly
Tier
1 (P
refe
rred
Ge
neric
) $1
0 co
pay
$30
copa
y
Tier
2 (N
on-
Pref
erre
d Ge
neric
) $2
0 co
pay
$60
copa
y
Tier
3 (P
refe
rred
Br
and)
$4
4 co
pay
$132
cop
ay
Tier
4 (N
on-
Pref
erre
d Br
and)
$9
0 co
pay
$270
cop
ay
Tier
5 (S
peci
alty
Ti
er)
25%
of t
he
cost
25
% o
f the
co
st
You
pay
the
follo
win
g un
til y
our t
otal
yea
rly d
rug
cost
s re
ach
$2,9
60. T
otal
yea
rly d
rug
cost
s are
the
tota
l dru
g co
sts p
aid
by b
oth
you
and
our P
art D
pla
n.
You
may
get
you
r dru
gs a
t net
wor
k re
tail
phar
mac
ies
and
mai
l ord
er p
harm
acie
s.
Stan
dard
Ret
ail C
ost-
Shar
ing
Tier
O
ne-m
onth
su
pply
Th
ree-
mon
th
supp
ly
Tier
1 (P
refe
rred
Ge
neric
) $5
cop
ay
$15
copa
y
Tier
2 (N
on-
Pref
erre
d Ge
neric
) $1
5 co
pay
$45
copa
y
Tier
3 (P
refe
rred
Br
and)
$4
0 co
pay
$120
cop
ay
Tier
4 (N
on-
Pref
erre
d Br
and)
$7
5 co
pay
$225
cop
ay
Tier
5 (S
peci
alty
Ti
er)
33%
of t
he
cost
33
% o
f the
co
st

Initi
al C
over
age
(con
tinue
d)
Stan
dard
Mai
l Ord
er C
ost-
Shar
ing
Tier
O
ne-m
onth
su
pply
Th
ree-
mon
th
supp
ly
Tier
1 (P
refe
rred
Ge
neric
) $1
0 co
pay
$25
copa
y
Tier
2 (N
on-
Pref
erre
d Ge
neric
) $2
0 co
pay
$50
copa
y
Tier
3 (P
refe
rred
Br
and)
$4
4 co
pay
$110
cop
ay
Tier
4 (N
on-
Pref
erre
d Br
and)
$9
0 co
pay
$225
cop
ay
Tier
5 (S
peci
alty
Ti
er)
25%
of t
he
cost
25
% o
f the
co
st
If yo
u re
side
in a
long
-ter
m c
are
faci
lity,
you
pay
the
sam
e as
at a
reta
il ph
arm
acy.
Yo
u m
ay g
et d
rugs
from
an
out-
of-n
etw
ork
phar
mac
y an
d pa
y th
e sa
me
as a
n in
-net
wor
k ph
arm
acy,
but
you
will
get
le
ss o
f the
dru
g.
Stan
dard
Mai
l Ord
er C
ost-
Shar
ing
Tier
O
ne-m
onth
su
pply
Th
ree-
mon
th
supp
ly
Tier
1 (P
refe
rred
Ge
neric
) $5
cop
ay
$12.
50 c
opay
Tier
2 (N
on-
Pref
erre
d Ge
neric
) $1
5 co
pay
$37.
50 c
opay
Tier
3 (P
refe
rred
Br
and)
$4
0 co
pay
$100
cop
ay
Tier
4 (N
on-
Pref
erre
d Br
and)
$7
5 co
pay
$187
.50
copa
y Ti
er 5
(Spe
cial
ty
Tier
) 33
% o
f the
co
st
33%
of t
he
cost
If
you
resid
e in
a lo
ng-t
erm
car
e fa
cilit
y, y
ou p
ay th
e sa
me
as a
t a re
tail
phar
mac
y.
You
may
get
dru
gs fr
om a
n ou
t-of
-net
wor
k ph
arm
acy
and
pay
the
sam
e as
an
in-n
etw
ork
phar
mac
y, b
ut y
ou
will
get
less
of t
he d
rug.
Co
vera
ge G
ap
Mos
t Med
icar
e dr
ug p
lans
hav
e a
cove
rage
gap
(also
ca
lled
the
"don
ut h
ole"
). Th
is m
eans
that
ther
e's a
te
mpo
rary
cha
nge
in w
hat y
ou w
ill p
ay fo
r you
r dru
gs.
The
cove
rage
gap
beg
ins a
fter
the
tota
l yea
rly d
rug
cost
(in
clud
ing
wha
t our
pla
n ha
s pai
d an
d w
hat y
ou h
ave
paid
) rea
ches
$2,
960.
Af
ter y
ou e
nter
the
cove
rage
gap
, you
pay
45%
of t
he
plan
's co
st fo
r cov
ered
bra
nd n
ame
drug
s and
65%
of t
he
plan
's co
st fo
r cov
ered
gen
eric
dru
gs u
ntil
your
cos
ts to
tal
$4,7
00, w
hich
is th
e en
d of
the
cove
rage
gap
. Not
ev
eryo
ne w
ill e
nter
the
cove
rage
gap
.
Mos
t Med
icar
e dr
ug p
lans
hav
e a
cove
rage
gap
(also
ca
lled
the
"don
ut h
ole"
). Th
is m
eans
that
ther
e's a
te
mpo
rary
cha
nge
in w
hat y
ou w
ill p
ay fo
r you
r dru
gs.
The
cove
rage
gap
beg
ins a
fter
the
tota
l yea
rly d
rug
cost
(inc
ludi
ng w
hat o
ur p
lan
has p
aid
and
wha
t you
ha
ve p
aid)
reac
hes $
2,96
0.
Afte
r you
ent
er th
e co
vera
ge g
ap, y
ou p
ay 4
5% o
f the
pl
an's
cost
for c
over
ed b
rand
nam
e dr
ugs a
nd 6
5% o
f th
e pl
an's
cost
for c
over
ed g
ener
ic d
rugs
unt
il yo
ur
cost
s tot
al $
4,70
0, w
hich
is th
e en
d of
the
cove
rage
ga
p. N
ot e
very
one
will
ent
er th
e co
vera
ge g
ap.

Cata
stro
phic
Cov
erag
e Af
ter y
our y
early
out
-of-p
ocke
t dru
g co
sts (
incl
udin
g dr
ugs p
urch
ased
thro
ugh
your
reta
il ph
arm
acy
and
thro
ugh
mai
l ord
er) r
each
$4,
700,
you
pay
the
grea
ter o
f:
5%
of t
he c
ost,
or
$2
.65
copa
y fo
r gen
eric
(inc
ludi
ng b
rand
dru
gs
trea
ted
as g
ener
ic) a
nd a
$6.
60 c
opay
men
t for
all
othe
r dru
gs.
Afte
r you
r yea
rly o
ut-o
f-poc
ket d
rug
cost
s (in
clud
ing
drug
s pur
chas
ed th
roug
h yo
ur re
tail
phar
mac
y an
d th
roug
h m
ail o
rder
) rea
ch $
4,70
0, y
ou p
ay th
e gr
eate
r of
:
5% o
f the
cos
t, or
$2.6
5 co
pay
for g
ener
ic (i
nclu
ding
bra
nd d
rugs
tr
eate
d as
gen
eric
) and
a $
6.60
cop
aym
ent f
or
all o
ther
dru
gs.


Additional information regarding your coverage


HN Sales Y0086 H9788_MRK1192 Accepted
Multi-language Interpreter Services
English: We have free interpreter services to answer any questions you may have about our health or drug plan. To get an interpreter, just call us at 1-888-989-9905. Someone who speaks English/Language can help you. This is a free service.
Spanish: Tenemos servicios de intérprete sin costo alguno para responder cualquier pregunta que pueda tener sobre nuestro plan de salud o medicamentos. Para hablar con un intérprete, por favor llame al 1-888-989-9905. Alguien que hable español le podrá ayudar. Este es un servicio gratuito.
Chinese Mandarin: 我们提供免费的翻译服务,帮助您解答关于健康或药物保险的任何疑 问。如果您需要此翻译服务,请致电 1-888-989-9905。 我们的中文工作人员很乐意帮助您。 这是一项免费服务。
Chinese Cantonese: 您對我們的健康或藥物保險可能存有疑問,為此我們提供免費的翻譯 服務。如需翻譯服務,請致電 1-888-989-9905。 我們講中文的人員將樂意為您提供幫助。這 是一項免費服務。
Tagalog: Mayroon kaming libreng serbisyo sa pagsasaling-wika upang masagot ang anumang mga katanungan ninyo hinggil sa aming planong pangkalusugan o panggamot. Upang makakuha ng tagasaling-wika, tawagan lamang kami sa 1-888-989-9905. Maaari kayong tulungan ng isang nakakapagsalita ng Tagalog. Ito ay libreng serbisyo. French: Nous proposons des services gratuits d'interprétation pour répondre à toutes vos questions relatives à notre régime de santé ou d'assurance-médicaments. Pour accéder au service d'interprétation, il vous suffit de nous appeler au 1-888-989-9905. Un interlocuteur parlant Français pourra vous aider. Ce service est gratuit. Vietnamese: Chúng tôi có dịch vụ thông dịch miễn phí để trả lời các câu hỏi về chương sức khỏe và chương trình thuốc men. Nếu quí vị cần thông dịch viên xin gọi 1-888-989-9905 sẽ có nhân viên nói tiếng Việt giúp đỡ quí vị. Đây là dịch vụ miễn phí . German: Unser kostenloser Dolmetscherservice beantwortet Ihren Fragen zu unserem Gesundheits- und Arzneimittelplan. Unsere Dolmetscher erreichen Sie unter 1-888-989-9905. Man wird Ihnen dort auf Deutsch weiterhelfen. Dieser Service ist kostenlos.
Korean: 당사는 의료 보험 또는 약품 보험에 관한 질문에 답해 드리고자 무료 통역 서비스를 제공하고 있습니다. 통역 서비스를 이용하려면 전화1-888-989-9905 번으로 문의해 주십시오. 한국어를 하는 담당자가 도와 드릴 것입니다. 이 서비스는 무료로 운영됩니다.

Russian: Если у вас возникнут вопросы относительно страхового или медикаментного плана, вы можете воспользоваться нашими бесплатными услугами переводчиков. Чтобы воспользоваться услугами переводчика, позвоните нам по телефону 1-888-989-9905. Вам окажет помощь сотрудник, который говорит по-pусски. Данная услуга бесплатная.
Arabic:
فوري، مترجم على للحصول. لدينا األدوية جدول أو بالصحة تتعلق أسئلة أي عن لإلجابة المجانية الفوري المترجم خدمات نقدم إنناعلى بنا االتصال سوى عليك ليس العربية يتحدث ما شخص سيقوم. 1-888-989-9905 مجانية خدمة ھذه. بمساعدتك .
Hindi: हमारे वा य या दवा की योजना के बारे म आपके िकसी भी प्र न के जवाब देने के िलए हमारे पास
मु त दभुािषया सेवाएँ उपल ध ह. एक दभुािषया प्रा त करने के िलए, बस हम 1-888-989-9905 पर फोन
कर. कोई यिक्त जो िह दी बोलता है आपकी मदद कर सकता है. यह एक मु त सेवा है. Italian: È disponibile un servizio di interpretariato gratuito per rispondere a eventuali domande sul nostro piano sanitario e farmaceutico. Per un interprete, contattare il numero 1-888-989-9905. Un nostro incaricato che parla Italianovi fornirà l'assistenza necessaria. È un servizio gratuito.
Portugués: Dispomos de serviços de interpretação gratuitos para responder a qualquer questão que tenha acerca do nosso plano de saúde ou de medicação. Para obter um intérprete, contacte-nos através do número 1-888-989-9905. Irá encontrar alguém que fale o idioma Português para o ajudar. Este serviço é gratuito.
French Creole: Nou genyen sèvis entèprèt gratis pou reponn tout kesyon ou ta genyen konsènan plan medikal oswa dwòg nou an. Pou jwenn yon entèprèt, jis rele nou nan 1-888-989-9905. Yon moun ki pale Kreyòl kapab ede w. Sa a se yon sèvis ki gratis.
Polish: Umożliwiamy bezpłatne skorzystanie z usług tłumacza ustnego, który pomoże w uzyskaniu odpowiedzi na temat planu zdrowotnego lub dawkowania leków. Aby skorzystać z pomocy tłumacza znającego język polski, należy zadzwonić pod numer 1-888-989-9905. Ta usługa jest bezpłatna.
Japanese: 当社の健康 健康保険と薬品 処方薬プランに関するご質問にお答えするため に、無料の通訳サービスがありますございます。通訳をご用命になるには、1-888-989-9905 にお電話ください。日本語を話す人 者 が支援いたします。これは無料のサー ビスです。

How to Get Extra HelpYou may be able to get Extra Help to pay for your prescription drug premiums and costs. To see if you qualify for Extra Help, call: 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048, 24 hours a day/ 7 days a week; the Social Security Office at 1-800-772-1213 between 7 a.m. and 7 p.m., Monday through Friday. TTY users should call 1-800-325-0778; or Your Medicaid Office.
Contract RenewalPlease note that a plan may not be available to beneficiaries the following contract year because by law, plan sponsors can choose to not renew their contract with CMS or reduce their service area and CMS may also refuse to renew the contract, thus, resulting in a termination or non-renewal of your plan.
1-888-989-9905 (TTY 711)
Call Us
October 1-February 148 a.m. to 8 p.m., 7 days a week
February 15-September 308 a.m. to 8 p.m., Monday-Friday
We are available:
H9788 Y0086_MRK1197 Accepted
HealthNow New York is a Medicare Advantage and PDP plan with a Medicare contract and enrollment depends on contract renewal.
