blood society the journal of and thrombocytopenia are unusual at presentation. coagulation...
TRANSCRIPT

BLOOD The Journal of The American Society of Hematology
VOL 75, NO 3 FEBRUARY 1, 1990
REVIEW ARTICLE
Amyloidosis: A Final Common Pathway for Protein Deposition in Tissues
By Marvin J. Stone
MYLOID IS A N eosinophilic substance which under A the light microscope has a hyaline appearance and which is deposited in the walls of small blood vessels and extracellularly in various organs. These deposits, when exten- sive, interfere with normal function. Many controversies arose about the cause and composition of amyloid for a century after it was named by Rudolph Virchow in 1854.Is2 The first major breakthrough regarding the nature of amy-
of the amyloid diseases. They are of interest to hematologists for a t least three reasons: (a) Many of the precursor proteins circulate in the blood, (b) one of the more common types of amyloidosis is a plasma cell dyscrasia, and (c) many patients with amyloid disorders require hematological evaluation a t some time during the course of their disease.
DIAGNOSIS AND CLINICAL FINDINGS
loid occurred in 1959 when electron microscopy showed that this apparently structureless material was actually fibrillar.3 The ability to solubilize the fibrils enabled subsequent characterization of their major protein const i t~ents .~ Analyt- ical protein chemistry techniques have elucidated several distinct chemical forms of amyloid although all of them share the common physical properties of polarization birefrin- gence after Congo red staining, nonbranching fibrils with a diameter of 70 to 100 A by electron microscopy, and a twisted P-pleated sheet conformation by x-ray diffra~t ion.~ Except for intracerebral amyloid plaques, all deposits of amyloid also contain a nonfibrillar glycoprotein moiety, the P component.6 This amyloid P (AP) component is derived from a normal serum precursor (SAP) structurally related to one of the acute-phase reactants, C-reactive protein (CRP). Both SAP and C R P belong to the pentraxin family of plasma protein^.^
In the past decade, monographs resulting from four international symposia have reflected the accelerated activity and progress in amyloid research.'." Several chemical types of amyloid have been identified, most of which circulate in the blood before being deposited in extracellular sites. Except for their common morphologic and physical properties, the various amyloid diseases are widely disparate and occur in diverse clinical settings. A classification of amyloidosis based on the major protein subunits present in the fibrils is shown in Table 1.
Historically, amyloidosis was classified according to whether it occurred de novo ("primary") or was "secondary" to a recognizable preexisting or coexisting chronic infectious or inflammatory disease. In the past 60 years, rare hereditary amyloid syndromes have been well documented. Most pri- mary, secondary, and hereditary syndromes are systemic, ie, they involve more than one organ system. Isolated or tumor- like collections of amyloid in various organs also have been described. Recently, new amyloid disorders were recognized.
This review summarizes recent advances in understanding
The diagnosis of amyloidosis is based on biopsy of involved tissue." Apple-green birefringence under polarized light after Congo red staining and/or the typical fibrillar structure evident by electron microscopy constitute the most reliable methods. Biopsy of any involved site may yield the diagnosis. Because of the propensity for amyloid to involve the walls of small blood vessels, biopsies of internal organs such as liver, kidney, or gastrointestinal tract may lead to hemorrhage. Rectal biopsy provides a positive diagnosis in most patients with primary systemic amyloid~sis, '~ but the specimen must include submucosa. Recent experience with abdominal fat aspiration suggests that this simple low-risk method is the diagnostic procedure of choice in evaluation for systemic amyloidosis with a 60% to 85% positive yield.'4-16 Patients presenting with carpal tunnel syndrome have a lower inci- dence (0% to 17%) of positive abdominal fa t aspi- ra te~. '~ ' ' ' Tenosynovial amyloid is often unrecognized on routine histology, emphasizing the need to request the Congo red stain if amyloid is suspected.
Clinical manifestations of amyloidosis vary widely and depend on the organ system predominantly i n v ~ l v e d . l ~ ~ ' ~ ~ - ~ ~ Renal involvement with proteinuria associated with the nephrotic syndrome and/or Bence Jones proteinuria is ~ o m m o n ~ ~ . ~ ' ; the latter finding is restricted to the AL type of
From the Charles A. Sammons Cancer Center and the Depart- ments of Internal Medicine, Oncology. and Pathology, Baylor University Medical Center. Dallas, TX.
Dedicated to the memory of Elliott F. Osserman, MD. Submitted July 17,1989; accepted October 10, 1989. Supported in part by the Tri Delta Cancer Research Fund and the
Baylor Research Foundation. Address reprint requests to Marvin J. Stone, MD. Charles A .
Sammons Cancer Center, Baylor University Medical Center, 3500 Gaston Ave, Dallas, TX 75246. 0 1990 by The American Society of Hematology. 0006-4971/90/7503-0032$3.00/0
53 1 Blood, Vol 75, No 3 (February 1). 1990: pp 531-545
532 MARVIN J. STONE
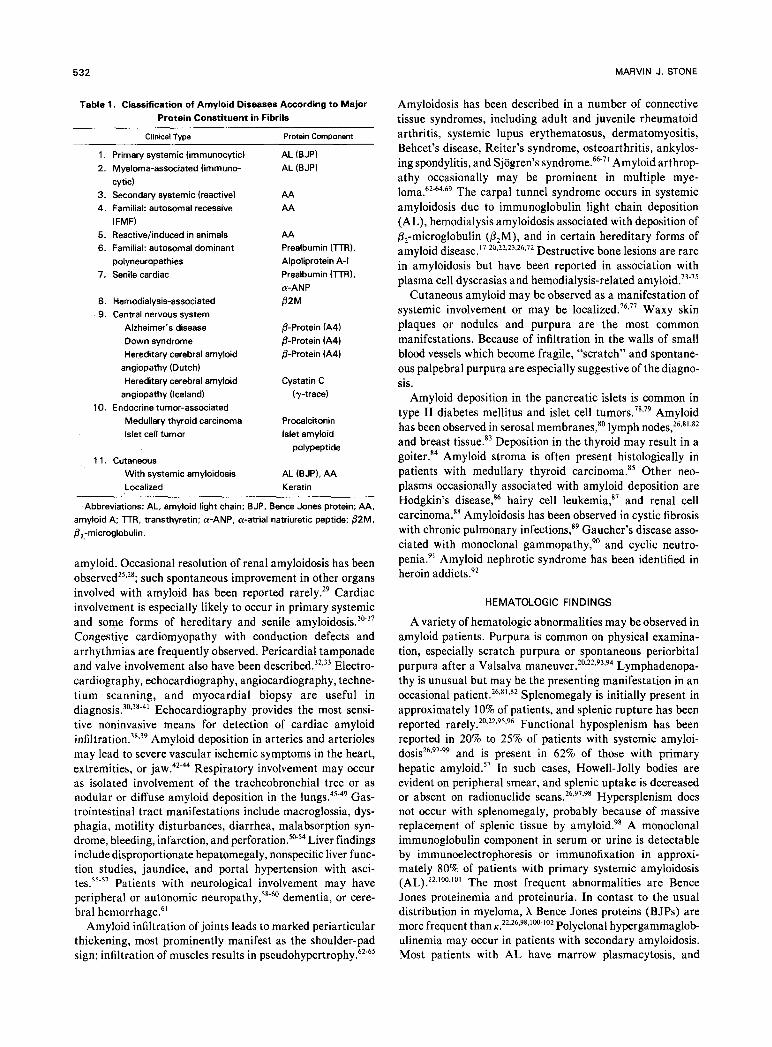
Table 1. Classification of Amyloid Diseases According to Major Protein Constituent in Fibrils
~
Clinical Type Protein Component
1. Primary systemic (immunocytic) 2. Myeloma-associated (immune
3. Secondary systemic (reactive) 4 . Familial: autosomal recessive
5. Reactive/induced in animals 6. Familial: autosomal dominant
7. Senile cardiac
cytic)
(FMF)
polyneuropathies
8. Hemodialysis-associated 9. Central nervous system
Alzheimer’s disease Down syndrome Hereditary cerebral amyloid
angiopathy (Dutch) Hereditary cerebral amyloid
angiopathy (Iceland) 10. Endocrine tumor-associated
Medullary thyroid carcinoma Islet cell tumor
1 1. Cutaneous With systemic amyloidosis Localized
AL (BJP) AL (B JP)
AA AA
AA Prealbumin (l-rR), Alpoliprotein A-I Prealbumin (TTR),
82M a-ANP
0-Protein (A4) @-Protein (A41 &Protein (A41
Cystatin C (7-trace)
Procalcitonin Islet amyloid
polypeptide
AL (BJP), AA Keratin
Abbreviations: AL, amyloid light chain; BJP, Bence Jones protein; AA, amyloid A: l-rR. transthyretin: a-ANP, a-atrial natriuretic peptide: 02M, &-microglobulin.
amyloid. Occasional resolution of renal amyloidosis has been o b s e r ~ e d ~ ~ s ~ ~ ; such spontaneous improvement in other organs involved with amyloid has been reported rarely.29 Cardiac involvement is especially likely to occur in primary systemic and some forms of hereditary and senile amyloido~is . ’~-~~ Congestive cardiomyopathy with conduction defects and arrhythmias are frequently observed. Pericardial tamponade and valve involvement also have been described.32s33 Electro- cardiography, echocardiography, angiocardiography, techne- tium scanning, and myocardial biopsy are useful in d i a g n o s i ~ . ~ ~ - ~ ~ - ~ ~ Echocardiography provides the most sensi- tive noninvasive means for detection of cardiac amyloid i n f i l t r a t i ~ n . ~ ~ . ~ ~ Amyloid deposition in arteries and arterioles may lead to severe vascular ischemic symptoms in the heart, extremities, or jaw.42-44 Respiratory involvement may occur as isolated involvement of the tracheobronchial tree or as nodular or diffuse amyloid deposition in the I~ngs .4’ -~~ Gas- trointestinal tract manifestations include macroglossia, dys- phagia, motility disturbances, diarrhea, malabsorption syn- drome, bleeding, infarction, and Liver findings include disproportionate hepatomegaly, nonspecific liver func- tion studies, jaundice, and portal hypertension with asci- tes.55-57 Patients with neurological involvement may have peripheral or autonomic n e u r ~ p a t h y , ’ ~ - ~ ~ dementia, or cere- bral hemorrhage.61
Amyloid infiltration of joints leads to marked periarticular thickening, most prominently manifest as the shoulder-pad sign; infiltration of muscles results in pse~dohypertrophy.~~.~’
Amyloidosis has been described in a number of connective tissue syndromes, including adult and juvenile rheumatoid arthritis, systemic lupus erythematosus, dermatomyositis, Behcet’s disease, Reiter’s syndrome, osteoarthritis, ankylos- ing spondylitis, and Sjogren’s ~yndrome!~.~’ Amyloid arthrop- athy occasionally may be prominent in multiple mye- loma.62-64369 The carpal tunnel syndrome occurs in systemic amyloidosis due to immunoglobulin light chain deposition (AL), hemodialysis amyloidosis associated with deposition of P,-microglobulin (P2M), and in certain hereditary forms of amyloid disease.17-20.22,23.26~72 Destructive bone lesions are rare in amyloidosis but have been reported in association with plasma cell dyscrasias and hemodialysis-related a m y l ~ i d . ~ ’ . ~ ~
Cutaneous amyloid may be observed as a manifestation of systemic involvement or may be l o ~ a l i z e d . ~ ~ , ~ ’ Waxy skin plaques or nodules and purpura are the most common manifestations. Because of infiltration in the walls of small blood vessels which become fragile, “scratch” and spontane- ous palpebral purpura are especially suggestive of the diagno- sis.
Amyloid deposition in the pancreatic islets is common in type I1 diabetes mellitus and islet cell t ~ m o r s . ~ ~ , ~ ~ Amyloid has been observed in serosal membranes,” lymph nodes,26.s1,s2 and breast tissue.” Deposition in the thyroid may result in a goiter.84 Amyloid stroma is often present histologically in patients with medullary thyroid carcinoma.” Other neo- plasms occasionally associated with amyloid deposition are Hodgkin’s disease,86 hairy cell le~kemia,~’ and renal cell carcinoma.88 Amyloidosis has been observed in cystic fibrosis with chronic pulmonary infection^,'^ Gaucher’s disease asso- ciated with monoclonal gammopathy?’ and cyclic neutro- penia.” Amyloid nephrotic syndrome has been identified in heroin addicts.92
HEMATOLOGIC FI NDl NGS
A variety of hematologic abnormalities may be observed in amyloid patients. Purpura is common on physical examina- tion, especially scratch purpura or spontaneous periorbital purpura after a Valsalva Lymphadenopa- thy is unusual but may be the presenting manifestation in an occasional patient.26.81,82 Splenomegaly is initially present in approximately 10% of patients, and splenic rupture has been reported rarely.20.22~95.96 Fu nctional hyposplenism has been reported in 20% to 25% of patients with systemic amyloi-
and is present in 62% of those with primary hepatic amyloid.57 In such cases, Howell-Jolly bodies are evident on peripheral smear, and splenic uptake is decreased or absent on radionuclide scans.26.97s98 Hypersplenism does not occur with splenomegaly, probably because of massive replacement of splenic tissue by amyloid.98 A monoclonal immunoglobulin component in serum or urine is detectable by immunoelectrophoresis or immunofixation in approxi- mately 80% of patients with primary systemic amyloidosis (AL) ,223100.101 The most frequent abnormalities are Bence Jones proteinemia and proteinuria. In contast to the usual distribution in myeloma, X Bence Jones proteins (BJPs) are more frequent than K . ~ ~ . ~ ~ , ~ ~ , ’ ~ - ~ ~ ~ Polyclonal hypergammaglob- ulinemia may occur in patients with secondary amyloidosis. Most patients with AL have marrow plasmacytosis, and
dosiS26,97-99

AMYLOIDOSIS 533
some have sheets or clusters of plasma cells.22326s1o3 Amyloid deposits are occasionally found in the walls of small blood vessels on marrow biopsy or rarely in the aspirate; 30% of patients with A L amyloidosis have a positive bone marrow.22 Rouleau is commonly observed in patients with monoclonal or polyclonal hypergammaglobulinemia. Ten to 15% of patients have anemia; it is normocytic in those with coexist- ing myeloma or secondary amyloid, and microcytic in pa- tients with hemorrhage and associated iron deficiency. Leu- kopenia and thrombocytopenia are unusual a t presentation. Coagulation abnormalities are often present in patients with hepatic amyloid~sis.~’ Acquired factor X deficiency is an unusual but well-documented complication of amyloidosis; the clotting factor appears to be rapidly cleared from the circulation and bound by amyloid deposit^.'^-'^^ Factor X deficiency has been reported to resolve after splenectomy or chemotherapy. 108~109 Rarely, increased fibrinolytic activity may lead to a hemorrhagic diathesis; in such a circumstance amino caproic acid may be of Lytic bone lesions of the type characteristic of myeloma rarely occur in a m y l o i d ~ s i s . ~ ” ~ ~ ~ ~ ~ ’ ~ ~
IMMUNOGLOBULIN LIGHT CHAIN-DERIVED AMYLOID (AL)
An interesting historical parallel exists between amyloid and BJP. Amyloid was named and popularized by Virchow in the mid-nineteenth century. Its structural features were not elucidated for more than 100 years, however, and its chemical nature remained controversial until the early 1970s. Similarly, BJP was described in 1848112 and was used by clinicians as a diagnostic test for multiple myeloma for more than a century before its structure was clarified. Not until 1962 was it shown that BJP was the monoclonal immu- noglobulin (Ig) light (L) chain portion of the serum M-component, which was often present in excess of heavy (H) chains and thus appeared commonly in the urine of patients with mye10ma.I’~ A short time later, it was demon- strated that both H and L chains could be split by proteolytic enzymes into common (C) and variable (V) regions. The association between amyloid, BJP, and marrow plasmacyto- sis had been stressed by Apitz and Magnus-Levy for more than 40 In the 1960s, studies by Osserman et al l 16.1 17 and the Mayo Clinic group118 provided further evidence of this association and called attention to the relationship between myeloma and “primary” systemic amy- loidosis. More recently, it has become clear that most patients presenting with the clinical manifestations of de novo systemic deposits of amyloid of the nonhereditary type (ie, primary) have an identifiable monoclonal Ig abnormality in serum, urine, or both. Amyloid deposition in these individ- uals tends to be distributed in the heart, tongue, gastrointes- tinal tract, skin, ligaments, and peripheral nerves.20-24,26*100 Involvement of liver, kidneys, spleen, and adrenals, a distribu- tion more characteristic of “secondary” systemic amyloid, also may occur, however. Because of the overlap in amyloid deposition, differentiation into primary and secondary types on the basis of organ involvement or anatomic location is often unreliable in the individual patient.
The role of Ig components in the pathogenesis of nonhered- itary primary systemic amyloidosis was clearly demonstrated
by Glenner et al, who established by amino acid sequence studies the identity of monoclonal Ig L chains (BJPs) and certain amyloid fibril proteins.1’9-’21 In patients with nonfamil- ial primary systemic amyloidosis or plasma cell dyscrasia associated with amyloidosis, the major protein constituent of the isolated amyloid fibril protein usually consists of intact monoclonal Ig L chains (BJPs), fragments from their amino- terminal (V) region, or both. Therefore, the amyloid in these patients (AL) consists of extracellular deposits of intact molecules or fragments of BJP.5s1222123 In some patients with AL, the V-region L fragments may be aberrantly secreted from the plasma cell monoclone in vitro and perhaps in vivo.124 In addition, free monoclonal L chain synthesis has been identified in vitro even in patients without evidence of an M-protein in serum or urine. Tetramers or larger poly- mers of BJPs are selectively retained in the circulation and may predispose to amyloid d e p o s i t i ~ n . ~ ~ ~ ~ ~ ~ - ’ ~ ~ Amyloid has been rarely observed in patients with y heavy chain disease, a disorder typically unaccompanied by evidence of monoclonal L chain production.I2* Because immunoglobulin heavy chains are not known to form amyloid, this finding has been unexplained. The recent demonstration of abnormal L chain genes in both y and a heavy-chain disease may be pertinent in this regard.129,’30 Low-level production of L chain frag- ments that are difficult to detect could, nevertheless, lead to amyloid deposition. Patients with primary systemic amyloido- sis occasionally have been shown to have chemical types of amyloid other than AL.1313132 Approximately 80% of patients with nonhereditary primary (ie, without evidence of coexist- ing chronic infections or inflammatory disease) systemic amyloidosis have an identifiable M-protein in serum, urine, or both. Exclusive identification of BJPs, especially A, has been especially common. Thus, accurate characterization of urinary protein by immunological techniques is critically important in this group of patients. Approximately 15% to 20% of BJPs appear to be amyloidogenic in that they have the property of precipitating as fibrillar material resembling amyloid after in vitro proteolytic This amyloidogenic property is associated with the V, region and is more commonly observed with h than with K monoclonal L chains, a finding in accord with the L-chain distribution noted in amyloid patients. The V region of the X subclass VI appears to be especially amyloidogenic, although all h subclasses have been i d e r ~ t i f i e d . ’ ~ ~ - I ~ ~ AL amyloid is com- posed of intact molecules or fragments of monoclonal L chains (ie, BJPs), and the amino-acid sequence of each BJP [molecular weight (mol wt) 23,000 daltons] is unique. N o specific amino-acid sequence common to all amyloidogenic BJPs or AL proteins has yet been BJP dimers may function as a primitive antibody; if so, such antigen- binding activity may be important in etiology and pathogen-
141.142 The experimental studies relating BJPs to amyloid explain the rather high incidence of amyloidosis in patients with “light chain d i ~ e a s e . ” * ~ . ~ * ~ ~ ~ ~ Although it certainly oc- curs, amyloidosis has been infrequent in patients with the typical symptoms and signs of overt m y e l ~ m a . ~ ~ . ’ ~ ~ . ’ ~ ~
These data are consistent with the hypothesis that patients with plasma cell dyscrasias who secrete intact BJPs or fragments thereof that possess amyloidogenic properties

534 MARVIN J. STONE
have a clinical picture dominated by the features of primary systemic amyloidosis instead of the usual manifestations observed in typical myeloma. The resulting clinical illness, therefore, would be more dependent on the molecular struc- ture of the individual BJP synthesized than on any intrinsic difference between primary systemic amyloidosis and multi- ple myeloma.26 Such a hypothesis does not dictate that every patient producing amyloidogenic L chains necessarily need develop clinical amyloidosis; some clearly do not, suggesting that additional factors play an important role in tissue deposition of amyloid Whether the BJP is transformed into amyloid fibrils intra- or extracellularly is not ~ l e a r . ’ ~ ’ - ‘ ~ ~ Monoclonal antibodies (MoAbs) directed to non-light-chain antigens on plasma cells react with certain tissue amyloid deposits from patients with plasma cell dyscrasia-related amyloid~sis.’~” The tendency for some L-chain monomers or dimers to associate into high-mol wt polymers as well as biosynthetic studies demonstrating se- creted L-chain fragments may have a bearing on whether incorporation into amyloid fibrils O C C U ~ S . ~ ~ ~ ’ ~ ~ ~ ’ ~ ~ ~ ’ ~ ’ B 0th clinical types of AL, nonhereditary primary systemic and plasma cell dyscrasia-associated, have been termed immuno- cyte-derived amyloidosis by Glenner .’
The relationship of systemic light-chain deposition and light-chain nephropathy to amyloidosis is ~ n c l e a r . ” ~ ~ ~ ~ ~ ~ ” ~ ~ ’ ~ ~ About 150 cases of light-chain deposition disease have been reported, most of which have had evidence of myeloma or an asymptomatic plasma cell d y s c r a ~ i a . ’ ~ ~ ~ ’ ’ ~ Nearly all cases have been associated with K L hai ins."^^'^^^'^^^^^ The deposits may occur in virtually any organ, especially the kidney. The monoclonal L chains in the deposits have been identified by immunohistochemical methods but do not show polarization birefringence after Congo red staining or a fibrillar structure by electron microscopy. Although systemic light-chain depo- sition has been observed with myeloma and Bence Jones proteinuria, serum M-components are frequently absent and the concentration of monoclonal L chains in urine is low. Marrow plasmacytosis usually is mild, but its monoclonal nature has been d e m o n ~ t r a t e d . ” ~ ~ ’ ~ ~ The most prominent findings usually are in the kidneys, in which glomerular and tubular deposits have been observed. A nodular type of glomerular involvement, resembling diabetic glomeruloscle- rosis, has been a striking finding in some patient^.'^^^''^.^'^^'^' Most patients develop renal failure. An amyloidlike glomeru- lopathy without monoclonal L-chain deposits also has been described.I6’ There is some evidence indicating that the monoclonal L chains in light-chain deposition disease are either abnormally large or small and perhaps are glycosy- lated and synthesized as S U C ~ . ” ~ . ~ ’ ~ K BJPs have a lesser tendency to form amyloid fibrils than their X counterparts. Monoclonal K chains in L-chain deposition disease may not contain an amino-acid sequence that permits a /3-pleated sheet conformation in tissues and thus may not form amy- loid.
AMYLOID A (AA)
In contrast to primary amyloidosis, patients with systemic amyloidosis secondary or reactive to chronic infections or inflammatory disorders and certain tumors have as the major
protein constituent in their amyloid fibrils a protein (AA) that is not derived from immunoglobulin L hai ins.'^^^'^^ Recurrent infections in patients with tuberculosis, leprosy, chronic osteomyelitis, bronchiectasis, decubitus ulcers, para- plegia, chronically infected burns, chronic skin infections associated with parenteral drug abuse, hypogammaglobulin- emia, and Whipple’s disease are associated with AA.164 In addition, chronic inflammatory diseases, especially rheuma- toid arthritis and juvenile chronic arthritis, are occasionally associated with amyloidosis of this type. Patients with other connective tissue disorders and Crohn’s disease rarely de- velop AA.’64 Neoplasms associated with AA include Hodgkin’s disease, renal cell carcinoma and, very rarely, other tumors. AA appears to be derived by proteolytic cleavage of a heterogeneous minor component of normal plasma (SAA), which has a mol wt of -12,500 daltons, is transported in association with high-density lipoprotein, and behaves as an acute-phase r e a ~ t a n t . ’ ~ ~ ” ~ ~ An increased con- centration of SAA appears to be necessary for formation of AA; the apoprotein precursor protein is elevated in inflamma- tory and neoplastic disease^.'^' The function of SAA is obscure; however, recent evidence indicates that it may play a role in modulating synthesis of collagenase.’68 AA is a single polypeptide chain usually consisting of 76 amino acids and having a mol wt of approximately 8,500 d a l t ~ n s . ’ ~ ~ . ’ ~ ’ Larger and smaller sizes of the protein have been identified as well.’63 AA has been found in fibroblasts, plasma cells, Kupffer cells, and polymorphonuclear leukocytes, but ap- pears to be synthesized by hepatocytes. Loss of affinity for Congo red after treatment with potassium permanganate is characteristic of AA; this histochemical property has proved useful in distinguishing AA from AL.” The amyloid related to P,-microglobulin deposition in chronic hemodialysis pa- tients also is permanganate-sensitive, however. Immunohis- tochemistry using MoAbs specific for AA protein appears to be the method of choice for diagnosis of this type of amyloid~sis.’~’
In addition to chronic infectious or inflammatory diseases and occasional tumors, AA also is the fibrillar protein in the only type of hereditary amyloidosis inherited as an autosomal recessive, familial Mediterranean fever (FMF). The amy- loidosis of FMF occurs primarily in Sephardic Jews and persons of Turkish descent and may be the presenting manifestation of the di~order.’’~,’’~ Gertz et a1 described an FMF-like syndrome in a kindred in which the disorder appeared to be transmitted in an autosomal dominant att tern."^ The AA protein has been identified in amyloid fibrils from a patient with the Muckle-Wells syndrome, a type of hereditary amyloidosis characterized by nerve deaf- ness, fever, urticaria, and the nephrotic syndrome.’” AA also is the chemical type that occurs in a variety of animal species with reactive or experimentally induced amyl~idos is . ’~~~’’~
Lavie et a1 showed that AA may form from faulty processing of SAA by peripheral blood monocyte^.'^^ More- over, defective macrophage (Kupffer cell) function precedes development of amyloidosis in mice.’” Reduced SAA- degrading activity has been described in patients with secondary amy1oidosis;the decrease in such activity parallels the serum albumin le~e1.I’~ In mice, one of three SAA

AMYLOIDOSIS 535
isotypes appears to be the precursor of amyloid fibril protein AA; this isotype (SAA,) is selectively removed from the circulation.lS0 Mice resistant to amyloidosis have defective expression of the gene for SAA,."' A genetic marker for susceptibility to reactive systemic amyloidosis in patients with juvenile arthritis has been described; its applicability to other inflammatory disorders associated with amyloidosis is unknown."'
PREALBUMIN (TRANSTHYRETIN [iTRl)-DERIVED AMYLOID
A number of heredofamilial amyloid syndromes have been described; an excellent review of these disorders appeared recently."' Unlike FMF, all other hereditary amyloidoses show an autosomal dominant mode of inheritance. Most are late-onset disorders with slow progression over a number of years; they are manifest as polyneuropathies, cardiomyopa- thies, or nephropathie~.'~'~' '~ In most of these syndromes as well as in some types of senile cardiac amyloid, the major protein in the fibrils has been thyroxine-binding prealbumin, also known as TTR. This transport protein, which also binds retinol binding protein, has a normal plasma concentration of 20 to 40 mg/dL and is synthesized by the liver as a single polypeptide chain of 127 amino acids."' Prealbumin is a negative acute-phase reactant (ie, its concentration decreases with inflammation); serum levels of the protein are also low in many patients with prealbumin a m y l o i d o ~ i s . ' ~ ~ ~ ' ' ~ The normal circulating molecule has an extensive @ structure and is composed of a tetramer of noncovalently linked subunits, each of which has a mol wt of 14,000 daltons. A variant protein has been found in most types of familial amyloid polyneuropathy; both the normal and the abnormal forms of prealbumin are found in the deposits, but the latter appears to p r e d ~ m i n a t e . ' ~ ~ " ~ ~ Single amino-acid substitutions have been identified at positions 30, 33,60,77,84, 1 1 1, and 122 of the prealbumin molecule in the different types of hereditary amyloid~ses. '~' Six of these seven substitutions have been shown to result from single nucleotide changes in the prealbumin gene. In Portuguese, Japanese, United States, and Swedish families with familial amyloidotic polyneuropa- thy type I, the variant protein differs from normal plasma prealbumin in having a substitution of methionine for valine at position 30. Immunological, chemical, and direct DNA tests have been developed for detection of the specific mutations in the prealbumin variants; these assays are useful in identification of family members a t risk while still in the preclinical phase of the disease.'83.192-194 Such methods also are valuable for genetic counseling purposes. The ability to identify affected family members before clinical onset of disease will allow assessment of potentially valuable therapeu- tic regimens for these unusual disorders.
Not all of the familial amyloidotic polyneuropathy syn- dromes are associated with prealbumin deposits. In the Iowa type characterized by lower limb neuropathy, peptic ulcers and nephrotic syndrome, a variant form of apolipoprotein A-I has been demonstrated in the amyloid fibrils."' Apoli- poproteins occur in other types of amyloid. The precursor (SAA) of reactive systemic amyloidosis is an apolipoprotein. In addition, apolipoprotein A-I1 is present in the amyloid of mice with early senescence.'63
AMYLOID SECONDARY TO DEPOSITION OF PPM IN CHRONIC HEMODIALYSIS PATIENTS
During the past decade, a number of groups have reported that some patients on long-term hemodialysis develop the carpal tunnel ~ y n d r o m e . ' ' * ~ ~ ~ ~ ' ~ ~ This finding occurs primarily in patients who have been on dialysis for 7 to 10 years. The carpal tunnel syndrome usually is bilateral. Cystic bone lesions or pathological fractures occur in some patients, and such lesions may be observed in the carpal bone^.^^.'^^''^^ These symptoms and findings are the result of amyloid deposition in synovium and bone. Systemic involvement has been observed in some patients.'99 The fibrillar protein in this circumstance has the usual tinctorial properties of amyloid. The electron microscopic appearance of the fibrils tends to be curvilinear rather than ~traight. '~'.~" The major protein constituent in this type of hemodialysis-associated amyloid consists of monomers and dimers of @2M.200-202 Like AA, @,M-derived amyloid is permanganate sensitive. This protein is normally present on all cell membranes other than erythro- cytes and trophoblastic cells and is a component of the HLA class I molecule. The primary structure of B2M is homolo- gous to that of the constant domains of immunoglobulin H and L chains.203 @,M binds preferentially to collagen; this property may be important in the pathogenesis of amyloid- osis in patients on long-term hemodialysis.204 Like SAA, P2M may function in regulating collagen breakdown.16' &M is a low-mol-wt protein (1 1,800 daltons) and, like immunoglobu- lin L chains and other small proteins, is filtered at the glomerulus and reabsorbed in the proximal t ~ b ~ l e . ~ ~ . ~ ~ * ~ ~ ~ @,M is too large to pass through most dialysis membranes; thus, it accumulates in the plasma of patients with chronic renal failure. The serum @,M concentration in chronic hemodialysis patients is 40 to 50 times higher than normal, but the elevated levels alone do not correlate well with the risk for developing a m y l ~ i d . ~ ' . ' ~ ~ Thus, other systemic or local tissue factors may be important in determining whether amyloid deposition occurs. The use of polysulfone dialysers or extracorporeal adsorbents may increase the clearance of &M and thus reduce the likelihood of amyloid deposition in this patient g r o ~ p . ~ ' . ' ~ ~
AMYLOIDOSIS INVOLVING THE CENTRAL NERVOUS SYSTEM: ALZHEIMER'S DISEASE, DOWN'S SYNDROME, AND HEREDITARY CEREBRAL AMYLOID ANGIOPATHY
Alzheimer's disease, formerly believed to be a rare cause of dementia, is now recognized as the fourth leading cause of death in the United States and may be the most common type of amyloid-associated d i s e a ~ e . ~ ' ~ ~ ~ ~ Amyloid is present in three types of lesions in the brain of patients with Alz- heimer's disease: neurofibrillary tangles, senile (neuritic) plaques, and blood v e ~ ~ e l ~ . ~ ' ~ ~ ~ ' ~ ~ ~ ~ As is usual, amyloid deposition in the plaques and vessels is extracellular but the neurofibrillary tangle with its paired helical filaments is a unique form of intracellular a m y l ~ i d . ~ ' , * ~ ~ Similar though less frequent amyloid lesions have been found in brains of normal elderly persons, patients with other neurodegenerative disor- ders, and several species of aged mammals. The major component of the fibrils in all three sites is @-protein (also

536 MARVIN J. STONE
known as A4), a unique 28- to 43-amino acid polypeptide with a mol wt of approximately 4,200 daltons.61~206~20s In virtually all individuals with Down’s syndrome aged more than 35 years, the same lesions occur in the brain and are also composed of 6-protein. 6’s205*206,209 The gene for P-protein and that for familial Alzheimer’s disease have been localized to chromosome 21 but these two genes do not appear to be
Because Down’s syndrome is characterized by trisomy of chromosome 2 1, a third copy of the /%protein gene exists in these patients and may account for an overproduc- tion of the protein which, after many years, leads to amyloid deposition in the brain.2’2,2’3 As with other chemical types of amyloid, the P-protein originates from a larger precursor (BAPP or PreA4); in this case, the precursor molecule appears to be a 695-amino acid glycoprotein of about 79,000 daltons.61 ,206.2 I4 The /3-protein sequence is near the C-terminal region of the precursor sequence; the precursor protein has been suggested to be a glycosylated cell receptor2I4 and related to the core protein of a heparan sulfate proteogly~an.~’~ The mRNA for P-protein has been identified in multiple cell types in the brain as well as other sites, including heart, kidney, and spleen.2063210,216 Im munoreactivity for BAPP has been identified in the same nonneural sites as well as in adrenal gland and liver.217 Native DAPP occurs as a heteroge- neous group of membrane-associated proteins in brain and other tissues. The cellular source of OAPP and its function remain to be determined.217 The widespread distribution of the precursor protein as well as the elevated ratio of serum BAPP (PreA4) to cerebrospinal fluid BAPP (PreA4) suggest that it circulates in the blood before it is incorporated into vessels, plaques, and tangles in the brain.61*206*208 Serum levels of BAPP (PreA4) are increased in patients with Down’s syndrome but are normal in Alzheimer’s patients.613212 Al- though the role of p-protein in Alzheimer’s disease is still unclear, the finding that a preamyloid Congo red-negative type of amorphous nonfibrillar 0-protein appears to precede development of neuritic plaques and neurofibrillary tangles in both Alzheimer’s disease and Down’s syndrome argues strongly for its importance in pathogenesis of the brain lesion^.^^^,^'^.^'^ No evidence exists for production of an abnormal protein precursor in either Alzheimer’s disease or Down’s syndrome; nevertheless, this remains a possibility.206 A processing abnormality or catabolic defect constitutes another potential mechanism for amyloid d e p o ~ i t i o n . ~ ~ ~ . ~ ’ ~ . ~ ~ ~ A serine protease inhibitor, a,-antichymotrypsin, is a compo- nent of amyloid deposits in neuritic plaques and blood vessel walls from brains of Alzheimer’s disease patient^.^" Alter- ations in the local concentration of inhibitor could promote deposition of P-protein into amyloid by inhibiting its clear- ance (excess activity) or by permitting increased proteolytic cleavage of OAPP and formation of 0-protein (decreased activity).
Amyloid has been identified in Creutzfeldt-Jakob disease and other transmissible spongiform encephal~pathies.~~~~~’~ The amino acid sequence of the “prion” fibrillar protein in these disorders differs from that of P-protein found in Alzheimer’s disease and Down’s syndrome.
Cerebral amyloid angiopathy occurs in nearly all patients with Alzheimer’s disease and aged Down’s syndrome. In
linked. 206.2 10.2 I I
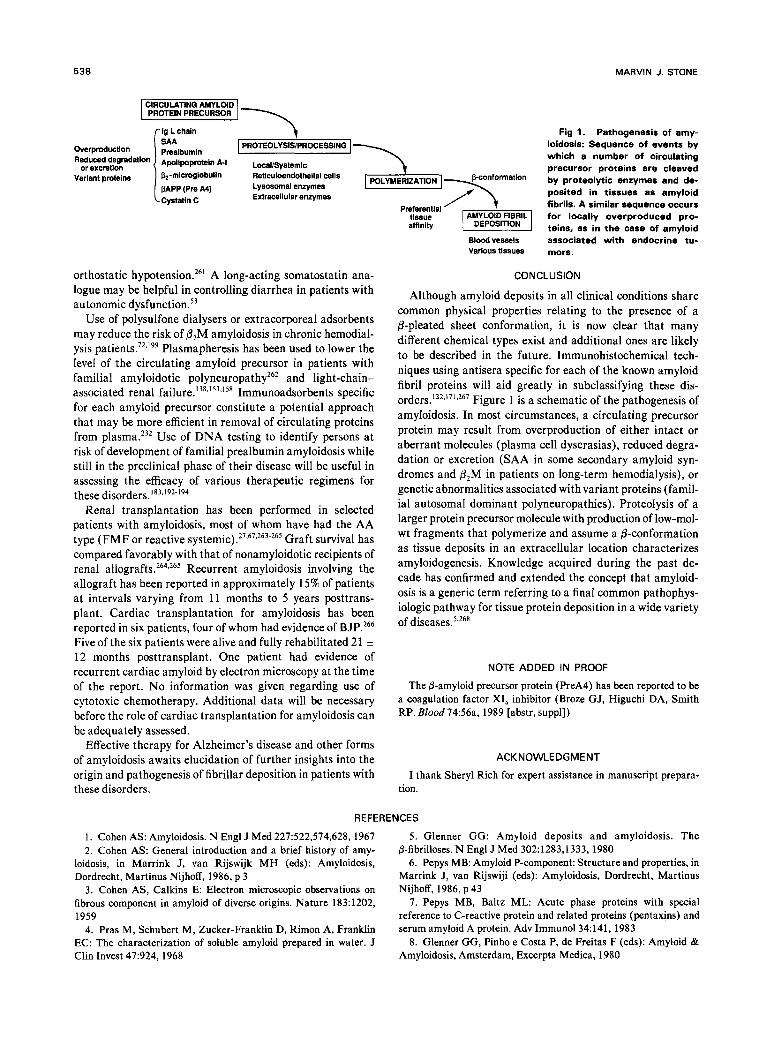
addition, cerebral amyloid angiopathy is a significant cause of spontaneous cerebral hemorrhage and has been described in kindreds from Iceland and the Netherlands in which it is transmitted as an autosomal dominant trait.61,220-222 Amyloid from the Dutch patients is biochemically identical to the P-protein seen in Alzheimer’s disease and Down’s syndrome.223 The Icelandic form of cerebral amyloid angiopathy is charac- terized by a protein closely related to the cysteine protease inhibitor cystatin C (previously known as y-trace) which is found deposited in blood vessels. This protein is a 120-amino acid polypeptide with a mol wt of 13,000 daltons and is present in body fluids, especially the cerebrospinal fluid. It is produced by neuroendocrine cells within and outside the central nervous system. A variant protein has been identified in the cerebrovascular amyloid deposits, which is 10 residues shorter than the native protein and has an amino-acid substitution of glutamine for leucine at residue 58.224 As with other chemical types of amyloid, monomers and polymers of the protein are present in the deposits. Variant proteins reported in human amyloid diseases are shown in Table 2.
AMYLOID OF OTHER TYPES: ENDOCRINE AND CUTANEOUS
Certain tumors of endocrine glands (eg, medullary thyroid carcinoma and pancreatic islet cell tumors) have an amyloid stroma on histological examination. The localized amyloid of medullary thyroid carcinoma is composed of a precursor form of the hormone secreted by the tumor; ie, procalci- t ~ n i n . ~ ’ , ~ ~ ~ Amyloid also may be found in other types of calcitonin-producing tumors.226 The amyloid present in pa- tients with islet cell tumors appears to be a protein distinct from insulin or proinsulin and has been termed islet amyloid polypeptide (IAPP).79 This molecule also may be involved in the pancreatic islet amyloid observed in elderly persons and persons with type I1 d i a b e t e ~ . ~ ~ . ~ ~ A form of senile cardiac amyloid in which the deposits are restricted to the atria (isolated atrial amyloid or IAA) is composed of a atrial natriuretic peptide (cxANP).’~’ This peptide is the C-terminal 28-amino acid fragment derived from a larger prohormone
Table 2. Variant Proteins in Human Amyloidosis
Protein Variant. Clinical Syndrome
Monoclonal L chains Multiple unique variants
Prealbumin Methionine 3 0 (transthyretin)
Isoleucine 33 Alanine 6 0
Tyrosine 77
Serine 84 Methionine 1 1 1 Isoleucine 122
Apolipoprotein A-I Arginine 26 Cystatin C Glutamine 58
Primary systemic, m yeloma-associated (immunocytic)
FAP I
Jewish hereditary Appalachian
hereditary lllinois/German
hereditary FAP II Danish hereditary Senile cardiac FAP 111 Iowa Hereditary cerebral
amyloid angiopathy (Iceland)
Abbreviation: FAP, familial amyloidotic polyneuropathy “Amino acid substitutions.
AMYLOIDOSIS 537
molecule (126 amino acid residues) and has potent natri- uretic and diuretic effects.
Cutaneous involvement with amyloid occurs commonly as part of systemic deposition or may be localized to the skin.76.77 The lesions may be macular, papular, or nodular. Studies to date indicate that Ig L chains or AA protein are present in the skin of patients with systemic a m y l o i d ~ s i s . ~ ~ Immunoreactivity to keratin has been reported in some patients with localized cutaneous amyloidosis.228
THERAPEUTIC CONSIDERATIONS
Therapy of amyloidosis is unsatisfactory, and evaluation of various approaches has been hindered by the lack of ability to determine accurately its extent in an individual ~ a t i e n t . ’ ~ ~ . ~ ~ ’ Despite the inert nature of amyloid fibrils and their presence in a relatively inaccessible extracellular location, amyloidosis occasionally is reversible.25*28329s145*23i Th us, the fibrils can be mobilized and apparently dissolved under some circum- stances. Potential therapeutic approaches consist of those directed to prevention of amyloid precursor protein synthesis, prevention of amyloid fibril deposition, and removal or dissolution of amyloid deposits from t i s s ~ e s . ~ ~ ~ . ~ ~ ~
Colchicine has been shown to block production of second- ary AA amyloid in mice.234 For more than a decade, colchicine has been known to prevent or abort febrile attacks in most patients with FMF.235-237 Israeli investigators subse- quently showed that this agent can prevent amyloidosis in F M F patients.238 Moreover, colchicine can prevent addi- tional deterioration of renal function in F M F patients with amyloidosis who have proteinuria but who have not pro- gressed to the overt nephrotic syndrome. The effect of colchicine in prevention of amyloidosis in F M F patients appears to be independent of the drug’s action on ameliora- tion or prevention of the febrile attacks.238 The potential salutary effect of colchicine in other AA disorders associated with secondary (reactive) amyloidosis is unclear, but cer- tainly needs to be examined.
Results of treatment in AL, usually with a myeloma-type chemotherapy regimen, have been unimpressive, although occasional successes have been reported.22,26,75,’26,138,140.229, 239-250 This approach is predicated on the rationale that treatment of such patients with alkylating agents and cor- ticosteroids has as its objective reduction of the circulating monoclonal L-chain precursor by reducing the number of plasma cells synthesizing that protein in the bone marrow or e l ~ e w h e r e . ~ ~ . ~ ~ . ~ ~ ~ Such an approach is aimed a t retarding further deposition of amyloid in tissues rather than reversing amyloid that is already present. The median survival of patients with this plasma cell dyscrasia is 12 months, although long survival has been reported rarely.22*98,247.250 Congestive heart failure, urinary light chain excretion, hepatomegaly, and the presence of overt multiple myeloma are adverse prognostic factors within the first year.247 Ele- vated serum creatinine, overt multiple myeloma, orthostatic hypotension, and monoclonal serum component are adverse variables for those patients surviving more than 1 year.247
Chemotherapy has been of benefit in occasional patients with AL and the nephrotic syndrome. i26,229,239-2413244.245 Im- provement was evident within 1 year after institution of
treatment and consisted of reduction in proteinuria and disappearance of edema. Hepatomegaly resolved in the four patients in whom it was initially present. Remission of the nephrotic syndrome, disappearance of serum and urine M-protein, stable renal function, and resolution of hepato- megaly may occur after chemotherapy despite advancing renal amyloidosis on subsequent b i o ~ s y . ’ ~ ~ , ~ ~ ~ Thus, repeat biopsy of previously involved tissue is important in assessing the efficacy of therapy for AL. This point is further empha- sized by reports of spontaneous remission in amyloid neph- rotic syndrome.25.281251~252 Occasional patients with histologi- cally proven amyloidosis but without nephrotic syndrome have improved after chemotherapy, including one in whom histological regression of hepatic amyloid was demonstrated after melphalan-prednisone treatment.98*243.249.250
In a randomized trial, 55 patients with primary systemic amyloidosis received either melphalan-prednisone or placebo.242 Although laboratory parameters improved in 10 patients receiving chemotherapy, survival was not signifi- cantly different in the two groups.
Because of its efficacy in FMF, colchicine also has been used in AL patients.75.246.250.Z53.2S4 Two groups of investigators have demonstrated improved survival in colchicine-treated patients as compared with historical ~ o n t r o l s . ~ ~ ~ . ~ ~ ~ Kyle et a1 compared melphalan-prednisone with colchicine in a prospec- tively randomized cross-over No significant differ- ence in survival was demonstrated when the two groups were analyzed in aggregate. Melphalan-prednisone-treated pa- tients fared significantly better, however, when patients receiving only one regimen were analyzed or when survival was determined from the time of entry into the study until death or disease progression. These results suggested that melphalan-prednisone was superior to colchicine for treat- ment of AL amyloidosis. Use of melphalan-prednisone plus or minus colchicine should be compared in a randomized trial in patients with AL.
Dimethylsulfoxide (DMSO) administered either orally or transdermally has been reported to benefit occasional amy- loid patients, but the agent has been difficult to tolerate orally and the results, in general, have been d i ~ a p p o i n t i n g . ~ ~ ~ . ~ ’ ~
Several other pharmacologic agents have been reported to have toxic or beneficial effects in experimental and clinical amyloid disorders. Various immunosuppressive drugs, includ- ing several cytotoxic chemotherapeutic agents in clinical use, accelerate casein-induced amyloidosis in mice.257 Such find- ings sound a note of caution regarding use of these drugs in non-AL types of amyloid, especially reactive (AA) systemic amyloidosis. Patients with amyloid cardiomyopathy have long been considered to be sensitive to digitalis. Isolated amyloid fibrils bind digoxin; such binding may be related to the enhanced toxicity of digitalis in patients with amyloid heart disease.258 Calcium channel-blocking agents can aggra- vate congestive heart failure in patients with cardiac amyloidosis.259 Gertz et a1 reported selective binding of nifedipine to isolated amyloid fibrils; the binding was largely irreversible and not calcium dependent.260 Autonomic neu- ropathy may result in incapacitating symptoms in amyloid patients. A norepinephrine precursor, ~-threo-3, 4-dihy- droxyphenylserine, appears to be effective in treatment of
538 MARVIN J. STONE
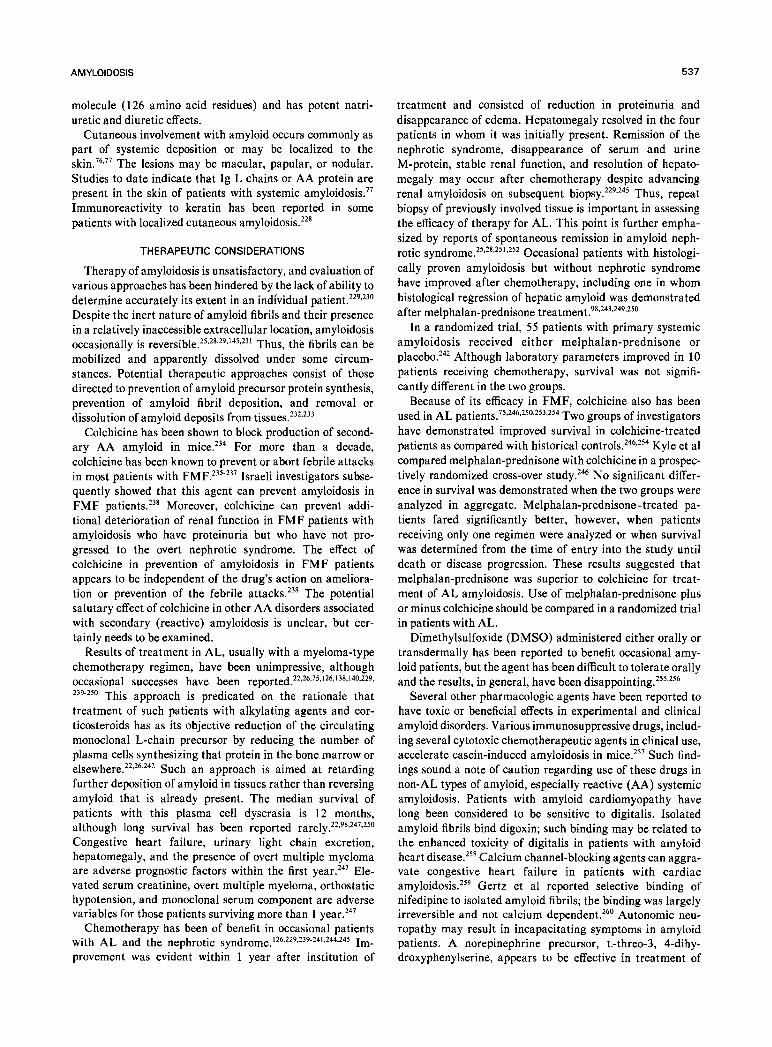
ig L chain Fig 1. Pathogenesis of amy- loidosis: Sequence of events by which a number of circulating precursor proteins are cleaved by proteolytic enzymes and de- posited in tissues as amyloid
PROTEOLYSiSiPROCESSiNG
BAPP (Pre A41 Lysosomal enzymes cells POLYMERIZATION
Preferential tlssue affinity
fibrils. A similar sequence occurs for locally overproduced pro- teins, as in the case of amyloid
Blood vessels associated with endocrine tu- Various tissues mors.
DEPoSITloN
I Cystati" c Extracellular enzymes
orthostatic hypotension.26' A long-acting somatostatin ana- logue may be helpful in controlling diarrhea in patients with autonomic d y s f ~ n c t i o n . ~ ~
Use of polysulfone dialysers or extracorporeal adsorbents may reduce the risk of P2M amyloidosis in chronic hemodial- ysis Plasmapheresis has been used to lower the level of the circulating amyloid precursor in patients with familial amyloidotic polyneuropathy262 and light-chain- associated renal f a i l ~ r e . ' ~ ~ ~ ' ~ ~ . ' ~ * Immunoadsorbents specific for each amyloid precursor constitute a potential approach that may be more efficient in removal of circulating proteins from plasma.232 Use of DNA testing to identify persons a t risk of development of familial prealbumin amyloidosis while still in the preclinical phase of their disease will be useful in assessing the efficacy of various therapeutic regimens for these disorder^.'^^^'^^-'^^
Renal transplantation has been performed in selected patients with amyloidosis, most of whom have had the AA type (FMF or reactive systemic).27*673263-26s Graft survival has compared favorably with that of nonamyloidotic recipients of renal allograft^.^^^.^^^ Recurrent amyloidosis involving the allograft has been reported in approximately 15% of patients a t intervals varying from 11 months to 5 years posttrans- plant. Cardiac transplantation for amyloidosis has been reported in six patients, four of whom had evidence of BJP.266 Five of the six patients were alive and fully rehabilitated 21 * 12 months posttransplant. One patient had evidence of recurrent cardiac amyloid by electron microscopy at the time of the report. N o information was given regarding use of cytotoxic chemotherapy. Additional data will be necessary before the role of cardiac transplantation for amyloidosis can be adequately assessed.
Effective therapy for Alzheimer's disease and other forms of amyloidosis awaits elucidation of further insights into the origin and pathogenesis of fibrillar deposition in patients with these disorders.
CONCLUSION
Although amyloid deposits in all clinical conditions share common physical properties relating to the presence of a @-pleated sheet conformation, it is now clear that many different chemical types exist and additional ones are likely to be described in the future. Immunohistochemical tech- niques using antisera specific for each of the known amyloid fibril proteins will aid greatly in subclassifying these dis- orders. 132.1 7 1.267 Figure 1 is a schematic of the pathogenesis of amyloidosis. In most circumstances, a circulating precursor protein may result from overproduction of either intact or aberrant molecules (plasma cell dyscrasias), reduced degra- dation or excretion (SAA in some secondary amyloid syn- dromes and &M in patients on long-term hemodialysis), or genetic abnormalities associated with variant proteins (famil- ial autosomal dominant polyneuropathies). Proteolysis of a larger protein precursor molecule with production of low-mol- wt fragments that polymerize and assume a @-conformation as tissue deposits in an extracellular location characterizes amyloidogenesis. Knowledge acquired during the past de- cade has confirmed and extended the concept that amyloid- osis is a generic term referring to a final common pathophys- iologic pathway for tissue protein deposition in a wide variety of disease^.^^^^^
NOTE ADDED IN PROOF
The @-amyloid precursor protein (PreA4) has been reported to be a coagulation factor XI, inhibitor (Broze GJ, Higuchi DA, Smith RP. Blood 74:56a, 1989 [abstr, suppl])
ACKNOWLEDGMENT
I thank Sheryl Rich for expert assistance in manuscript prepara- tion.
REFERENCES
1. Cohen AS: Amyloidosis. N Engl J Med 227522,574,628, 1967 2. Cohen AS: General introduction and a brief history of amy-
loidosis, in Marrink J, van Rijswijk MH (eds): Amyloidosis, Dordrecht, Martinus Nijhoff, 1986, p 3
3. Cohen AS, Calkins E: Electron microscopic observations on fibrous component in amyloid of diverse origins. Nature 183:1202, 1959
4. Pras M, Schubert M, Zucker-Franklin D, Rimon A, Franklin EC: The characterization of soluble amyloid prepared in water. J Clin Invest 47:924, 1968
5. Glenner GG: Amyloid deposits and amyloidosis. The P-fibrilloses. N Engl J Med 302:1283,1333, 1980
6. Pepys MB: Amyloid P-component: Structure and properties, in Marrink J, van Rijswiji (eds): Amyloidosis, Dordrecht, Martinus Nijhoff, 1986, p 43
7. Pepys MB, Baltz ML: Acute phase proteins with special reference to C-reactive protein and related proteins (pentaxins) and serum amyloid A protein. Adv Immunol34:141, 1983
8. Glenner GG, Pinho e Costa P, de Freitas F (eds): Amyloid & Amyloidosis, Amsterdam, Excerpta Medica, 1980
AMYLOIDOSIS 539
9. Glenner GG, Osserman EF, Benditt EP, Calkins E, Cohen AS, Zucker-Franklin D (eds): Amyloidosis, New York, Plenum, 1986
10. Marrink J, van Rijswijk MH (eds): Amyloidosis, Dordrecht, Martinus Nijhoff, 1986
11. Isobe T, Araki S, Uchino F, Kit0 S, Tsubura E (eds): Amyloid and Amyloidosis. New York, Plenum, 1988
12. Cohen AS, Skinner M: The diagnosis of amyloidosis, in Cohen AS (ed): Laboratory Diagnostic Procedures in the Rheu- matic Diseases, ed. 3. Boston, Little, Brown, 1985, p 377
13. Kyle RA, Spencer RJ, Dahlin DC: Value of rectal biopsy in the diagnosis of primary systemic amyloidosis. Am J Med Sci 251:501, 1966
14. Westermark P, Stenkvist B: A new method for the diagnosis of systemic amyloidosis. Arch Intern Med 132522, 1973
15. Duston MA, Skinner M, Shirahama T, Cohen AS: Diagnosis of amyloidosis by abdominal fat aspiration. Analysis of four years’ experience. Am J Med 82:412,1987
16. Duston MA, Skinner M, Meenan RF, Cohen AS: Sensitivity, specificity, and predictive value of abdominal fat aspiration for the diagnosis of amyloidosis. Arthritis Rheum 32:82, 1989
17. Varga J, Idelson BA, Felson D, Skinner M, Cohen AS: Lack of amyloid in abdominal fat aspirates from patients undergoing long-term hemodialysis. Arch Intern Med 147:1455, 1987
18. Gertz MA, Li CY, Shirahama T, Kyle RA: The subcutaneous fat aspirate: A controlled and blinded evaluation of the technique in the diagnosis of primary amyloidosis (AL). In Isobe T, Araki S, Uchino F, Kit0 S, Tsubura E (eds): Amyloid and Amyloidosis. New York, Plenum, 1988, p 801
19. Kyle RA, Eilers SG, Linscheid RL, Gaffey TA: Amyloid localized to tenosynovium at carpal tunnel release. Am J Clin Pathol 91:393, 1989
20. Kyle RA, Bayrd ED: Amyloidosis: A review of 236 cases. Medicine 54:27 1 , 1975
21. Wright JR, Calkins E: Clinical-pathologic differentiation of common amyloid syndromes. Medicine 60:429, 198 1
22. Kyle RA, Greipp PR: Amyloidosis (AL). Clinical and labora- tory features in 229 cases. Mayo Clin Proc 58:665, 1983
23. Browning MJ, Banks RA, Tribe CR, Hollingworth P, Kings- wood C, Mackenzie JC, Bacon PA: Ten years’ experience of an amyloid clinic-A clinicopathological survey. Q J Med 54:213, 1985
24. Janssen S, van Rijswijk MH, Meijer S, Ruinen L, van der Hem GK: Clinical evaluation of AA and AL amyloid disease, in Marrink J, van Rijswijk MH (eds): Amyloidosis. Dordrecht, Marti- nus Nijhoff, 1986, p 61
25. Triger DR, Joekes AM: Renal amyloidosis-A fourteen year follow-up. Q J Med 42:15, 1973
26. Stone MJ, Frenkel EP: The clinical spectrum of light chain myeloma. A study of 35 patients with special reference to the occurrence of amyloidosis. Am J Med 58:601, 1975
27. Cohen AS, Bricetti AB, Harrington JT, Mannick JA: Renal transplantation in two cases of amyloidosis. Lancet 2:5 13, 1971
28. Dikman SH, Kahn T, Gribetz D, Churg J: Resolution of renal amyloidosis. Am J Med 63:430, 1977
29. WaldenstriSm H: On the formation and disappearance of amyloid in man. Acta Chir Scand 63:479, 1928
30. Buja LM, Khoi NB, Roberts WC: Clinically significant cardiac amyloidosis. Clinicopathologic findings in 15 patients. Am J Cardiol26:394, 1970
3 1. Roberts WC, Waller BF: Cardiac amyloidosis causing car- diac dysfunction: Analysis of 54 necropsy patients. Am J Cardiol 52:137, 1983
32. Brodarick S, Paine R, Higa E, Carmichael KA: Pericardial tamponade, a new complication of amyloid heart disease. Am J Med 73:133, 1982
33. Cooper JH: Localized dystrophic amyloidosis of heart valves. Hum Pathol 14:649, 1983
34. Cornwell GG, Murdoch WL, Kyle RA, Westermark P, Pitkanen P: Frequency and distribution of senile cardiovascular amyloid. A clinicopathological correlation. Am J Med 75:618, 1983
35. Pitkanen P, Westermark P, Cornwell GG: Senile systemic amyloidosis.Am J Pathol 117:391, 1984
36. Lie JT, Hammond PI: Pathology of the senescent heart: Anatomic observations on 237 autopsy studies of patients 90 to 105 years old. Mayo Clin Proc 63:552, 1988
37. Morley JE, Reese SS: Clinical implications of the aging heart. Am J Med 86:77, 1989
38. Cueto-Garcia L, Tajik AJ, Kyle RA, Edwards WD, Greipp PR, Callahan JA, Shub C, Seward JB: Serial echocardiographic observations in patients with primary systemic amyloidosis: An introduction to the concept of early (asymptomatic) amyloid infiltra- tion of the heart. Mayo Clin Proc 59:589,1984
39. Falk RH, Plehn JF, Deering T, Schick EC, Boinay P, Rubinow A, Skinner M, Cohen AS: Sensitivity and specificity of the echocardiographic features of cardiac amyloidosis. Am J Cardiol 59:418, 1987
40. Gertz MA, Brown ML, Hauser MF, Kyle RA: Utility of technetium Tc 99m pyrophosphate bone scanning in cardiac amy- loidosis. Arch Intern Med 147:1039, 1987
41. Naggar CZ: Rapid amyloid infiltration of the heart. Am J Med 80:276,1986
42. Capone R, Amsterdam EA, Mason DT, Zelis R: Systemic amyloidosis, funtional coronary insufficiency, and autonomic impair- ment. Ann Intern Med 76:599, 1972
43. Zelis R, Mason DT, Barth W: Abnormal peripheral vascular dynamics in systemic amyloidosis. Ann Intern Med 70:1167, 1969
44. Gertz MA, Kyle RA, Griffing WL, Hunder GG: Jaw claudi- cation in primary systemic amyloidosis. Medicine 65:173, 1986
45. Attwood HD, Price CG, Riddell RJ: Primary diffuse tracheo- bronchial amyloidosis. Thorax 27:620, 1972
46. Laden SA, Cohen ML, Harley RA: Nodular pulmonary amyloidosis with extrapulmonary involvement. Hum Pathol 15:594, 1984
47. Gonzalez-Cueto DM, Rigoli M, Gioseffi LM, Lancelle B, Martinez A: Diffuse pulmonary amyloidosis. Am J Med 48:668, 1970
48. Kanada DJ, Sharma O P Long-term survival with diffuse interstitial pulmonary amyloidosis. Am J Med 67379, 1979
49. Eisenberg R, Sharma O P Primary pulmonary amyloidosis. An unusual case with 14 years’ survival. Chest 89:889, 1986
SO. Lesser BA, Leeper KV, Conway W: Obstructive sleep apnea in amyloidosis treated with nasal continuous positive airway pres- sure. Arch Intern Med 148:2285, 1988
51. Battle WM, Rubin MR, Cohen S, Snape WJ: Gastrointestinal- motility dysfunction in amyloidosis. N Engl J Med 301:24, 1979
52. Rubinow A, Burakoff R, Cohen AS, Harris LD: Esophageal manometry in systemic amyloidosis. Am J Med 75:951, 1983
53. OConner CR, O’Dorisio TM: Amyloidosis, diarrhea and a somatostatin analogue. Ann Intern Med 110:665, 1989 (letter)
54. French JM, Hall G, Parish DJ, Smith WT: Peripheral and autonomic nerve involvement in primary amyloidosis associated with uncontrollable diarrhea and steatorrhea. Am J Med 39:277, 1965
55. Levine RA: Amyloid disease of the liver. Correlation of clinical, functional and morphologic features in forty-seven patients. Am J Med 33:349, 1962
56. Rubinow A, Koff RS, Cohen AS: Severe intrahepatic cholesta- sis in primary amyloidosis. A report of four cases and a review of the literature. Am J Med 64:937, 1978
57. Gertz MA, Kyle RA: Hepatic amyloidosis (primary [AL],

540 MARVIN J. STONE
immunoglobulin light chain): The natural history in 80 patients. Am J Med 85:73,1988
58. Kelley JJ, Kyle RA, O’Brien PC, Pyck PJ: The natural histroy of peripheral neuropathy in primary systemic amyloidosis. Ann Neurol6:1, 1979
59. Kyle RA, Kottke BA, Schirger A: Orthostatic hypotension as a clue to primary systemic amyloidosis. Circulation 34383, 1966
60. Hines S, Houston M, Robertson D: The clinical spectrum of autonomic dysfunction. Am J Med 70:1091, 1981
61. Vinters HV, Miller BL, Pardridge WM: Brain amyloid and Alzheimer’s disease. Ann Intern Med 109:41, 1988
62. Wiernik PH: Amyloid joint disease. Medicine 51:465, 1972 63. Katz GA, Peter JB, Pearson CM, Adams WS: The shoulder-
pad sign-A diagnostic feature of amyloid arthropathy. N Engl J Med 288:354,1973
64. Hickling P, Wilkins M, Neuman GR, Pritchard MH, Jessop J, Whittaker J, Nuki G: A study of amyloid arthropathy in multiple myeloma. Q J Med 200:417,1981
65. Santiago RM, Scharnhorst D, Ratkin G , Crouch EC: Respi- ratory muscle weakness and ventilatory failure in AL amyloidosis with muscular pseudohypertrophy. Am J Med 83:175, 1987
66. Ozdemir AI, Wright JR, Calkins E: Influence of rheumatoid arthritis on amyloidosis of aging. Comparison of 47 rheumatoid patients and 47 controls matched for age and sex. N Engl J Med 285:534, 1971
67. Light PD, Hall-Craggs M: Amyloid deposition in a renal allograft in a case of amyloidosis secondary to rheumatoid arthritis. Am J Med 66:532,1979
68. Huston DP, McAdam KPWJ, Balow JB, Bass R, Debellis RA: Amyloidosis in systemic lupus erythematosus. Am J Med 70:320, 198 1
69. Zilko PJ, Dawkins RL: Amyloidosis associated with dermato- myositis and features of multiple myeloma. The progression of amyloidosis associated with corticosteroid and cytotoxic drug ther- apy. Am J Med 59:448,1975
70. Egan MS, Goldenberg DL, Cohen AS, Segal D: The associa- tion of amyloid deposits and osteoarthritis. Arthritis Rheum 25:204, 1982
7 1. Ludmerer KM, Kissane JM: Subcutaneous masses and ade- nopathy in a 77 year-old man with Sjogren’s syndrome and amyloid- osis. Am J Med 86:585, 1989
72. Kleinman KS, Coburn JW: Amyloid syndromes associated with hemodialysis. Kidney Int 35:567, 1989
73. Grossman RE, Hensley GT: Bone lesions in primary amy- loidosis. AJR 1012372, 1967
74. Lai KN, Chan KW, Siu DLS, Wong CC, Yeung D: Patho- logic hip fractures secondary to amyloidoma. Am J Med 77:937, 1984
75. Schattner A, Varon D, Green L, Hurwitz N, Bentwich Z : Primary amyloidosis with unusual bone involvement: Reversibility with melphalan, prednisone, and colchicine. Am J Med 86:347, 1989
76. Rubinow A, Cohen AS: Skin involvement in generalized amyloidosis. Ann Intern Med 88:781, 1978
77. Okuzono Y, Gondoh T, Kawano H, Nagasawa T, Uchino F Histopathology of cutaneous amyloid: A comparative study on 144 cases of localized cutaneous amyloidosis and 20 cases of systemic amyloidosis, in Glenner GG, Osserman EF, Benditt EP, Calkins E, Cohen AS, Zucker-Franklin D (eds): Amyloidosis. New York, Plenum, 1986, p 821
78. Clark A, Cooper GJS, Lewis CE, Morris JF, Willis AC, Reid KMB, Turner RC: Islet amyloid formed from diabetes-associated peptide may be pathogenic in type 2 diabetes. Lancet 2:231, 1987
79. Johnson KH, O’Brien TD, Betsholtz C, Westermark P: Islet amyloid, islet-amyloid polypeptide, and diabetes mellitus. N Engl J Med 321:513,1989
80. Weinrach LA, Desautels RE, Christlieb AR, Kaldany A, DElia JA: Amyloid deposition in serosal membranes. Its occurrence with cardiac tamponade, bilateral ureteral obstruction, and gas- trointestinal bleeding. Arch Intern Med 144:630, 1984
81. Newland JR, Linke RP, Lennert K: Amyloid deposits in lymph nodes: A morphologic and immunohistochemical study. Hum Pathol 17:1245,1986
82. Brown S, Armstrong WM, Moses D, Fordtran JS: Unknown case discussion: A 49-year-old man with recurrent tender lymph nodes. Baylor Univ Med Ctr Proc 2:25, 1989
83. OConnor CR, Rubinow A, Cohen AS: Primary (AL) amy- loidosis as a cause of breast masses. Am J Med 77:98 l , 1984
84. Daoud FS, Nieman RE, Vilter RW: Amyloid goiter in a case of generalized primary amyloidosis. Am J Med 43:604, 1967
85. Hill CS, Ibanez MI, Samaan NA, Ahearn MJ, Clark RL: Medullary (solid) carcinoma of the thyroid gland: An analysis of the MD Anderson Hospital experience with patients with the tumor, its special features, and its histogenesis. Medicine 52:141, 1973
86. Kaplan HS: Hodgkin’s Disease, 2nd ed. Cambridge, Harvard University Press, 1980, p 220
87. Linder J, Silberman HR, Croker BP: Amyloidosis complicat- ing hairy cell leukemia. Am J Clin Pathol78:864, 1982
88. Pras M, Franklin EC, Shibolet S, Frangione B: Amyloidosis associated with renal cell carcinoma of the AA type. Am J Med 73:426, 1982
89. Biberstein M, Wolf P, Pettross B, Fanestil D, Vasquez M: Amyloidosis complicating cystic fibrosis. Am J Clin Pathol 80:752, 1983
90. Hanash SM, Rucknagel DL, Heidelberger KP, Radin NS: Primary amyloidosis associated with Gaucher’s disease. Ann Intern Med 89:639,1978
91. Shiomura T, Ishida Y, Matsumoto N, Sasaki K, Ishihara T, Miwa S: A case of generalized amyloidosis associated with cyclic neutropenia. Blood 54:628, 1979
92. Neugarten J, Gallo GR, Buxbaum J, Katz LA, Rubenstein J, Baldwin DS: Amyloidosis in subcutaneous heroin abusers (“skin poppers’ amyloidosis”). Am J Med 81:635, 1986
93. Milutinovich J, Wu W, Savory J: Periorbital purpura after renal biopsy in primary amyloidosis. JAMA 242:2555, 1979 (letter)
94. Yood RA, Skinner M, Rubinow A, Talarico L, Cohen AS: Bleeding manifestations in 100 patients with amyloidosis. JAMA 249:1322,1983
95. Barth WF, Willerson JT, Waldmann TA, Decker JL: Pri- mary amyloidosis. Clinical, immunochemical and immunoglobulin metabolism studies in fifteen patients. Am J Med 47:259, 1969
96. Hurd WW, Katholi RE: Acquired functional asplenia: Asso- ciation with spontaneous rupture of the spleen and fatal spontaneous rupture of the liver in amyloidosis. Arch Intern Med 140:844,1980
97. Gertz MA, Kyle RA, Greipp PR: Hyposplenism in primary systemic amyloidosis. Ann Intern Med 98:475, 1983
98. Stone MJ, Hirsch VJ: Splenic function in amyloidosis, in Glenner GG, Osserman EF, Benditt EP, Calkins E, Cohen AS, Zucker-Franklin D (eds): Amyloidosis. New York, NY, Plenum, 1986, p 583
99. Frank JM, Palomino NJ: Primary amyloidosis with diffuse splenic infiltration presenting as fulminant pneumococcal sepsis. Am J Clin Pathol87:405, 1987
100. Isobe T, Osserman EF: Patterns of amyloidosis and their association with plasma-cell dyscrasia, monoclonal immunoglobu- lins and Bence-Jones proteins. N Engl J Med 290:473, 1974
101. Stone MJ: Monoclonal gammopathies: Clinical aspects, in SE Ritzmann (ed): Pathology of Immunoglobulins: Diagnostic and Clinical Aspects. Protein Abnormalities, vol2. New York, NY, Liss, 1982, p 161
102. Isobe T: Lambda predominance of Bence Jones protein
AMYLOIDOSIS 54 1
(BJP) in AL amyloidosis among Japanese patients, in Isobe T, Araki S, Uchino F, Kit0 S, Tsubura E (eds): Amyloid and Amyloidosis. New York, Plenum, 1988, p 175 103. Wolf BC, Kumar A, Vera JC, Nieman RS: Bone marrow
morphology and immunology in systemic amyloidosis. Am J Clin Pathol 86:84, 1986
104. Pechet L, Kastrul JJ: Amyloidosis associated with factor X (Stuart) deficiency. Ann Intern Med 61:315,1964 105. Greipp PR, Kyle RA, Bowie EJW: Factor-X deficiency in
amyloidosis: A critical review. Am J Hematol 11:443, 1981 106. Furie B, Greene E, Furie BC: Syndrome of acquired factor
X deficiency and systemic amyloidosis. In vivo studies of the metabolic fate of factor X. N Engl J Med 297:81,1977 107. Furie B, Voo L, McAdam KPWJ, Furie BC: Mechanism of
factor X deficiency in systemic amyloidosis. N Engl J Med 304:827, 1981 108. Rosenstein ED, Itzkowitz SH, Penziner AS, Cohen JI,
Mornaghi RA: Resolution of factor X deficiency in primary amy- loidosis following splenectomy. Arch Intern Med 143597, 1983 109. Camoriano JK, Greipp PR, Bayer GK, Bowie EJW: Resolu-
tion of acquired factor X deficiency and amyloidosis with melphalan and prednisone therapy. N Engl J Med 3 16:1133, 1987 110. Redleaf PD, Davis RB, Krichinski C, Hoilund L, Cans H:
Amyloidosis with an unusual bleeding diathesis. Observations on the use of epsilon amino caproic acid. Ann Intern Med 58:347, 1963
1 1 1. Liebman H, Chinowsky M, Valdin J, Kenoyer G, Feinstein D: Increased fibrinolysis and amyloidosis. Arch Intern Med 143:678, 1983 112. Jones HB: On a new substance occurring in the urine of a
patient with mollities ossium. Philos Trans R Soc Lond [Biol] 13855, 1848 113. Edelman GM, Gally JA: The nature of Bence Jones pro-
teins. Chemical similarities to polypeptide chains of myeloma globulins and normal y-globulins. J Exp Med 116:207, 1962 114. Apitz K: Die Paraproteinosen. Uber die Stdrung des Eiweiss-
stoffwechsels be Plasmocytom. Virchows Arch Path Anat 306:63 1, 1940
1 15. Magnus-Levy A: Amyloidosis in multiple myeloma. Progress noted in 50 years of personal observation. J Mt Sinai Hosp 19:8, 1952
1 16. Osserman E F Amyloidosis: Tissue proteinosis: Gammaloid- osis. Ann Intern Med 55:1033, 1961 117. Osserman EF, Takatsuki K, Tala1 N: The pathogenesis of
“amyloidosis”: Studies on the role of abnormal gamma globulins and gamma globulin fragments of the Bence Jones (I-polypeptide) type in the pathogenesis of “primary” and “secondary amyloidosis,” and the “amyloidosis” associated with plasma cell myeloma. Semin Hematol 1:3, 1964 118. Kyle RA, Bayrd ED: “Primary” systemic amyloidosis and
myeloma. Discussion of relationship and review of 81 cases. Arch Intern Med 107:344, 1961 119. Glenner GG, Terry W, Harada M, Isersky C, Page D:
Amyloid fibril proteins. Proof of homology with immunoglobulin light chains by sequence analyses. Science 172:1150, 1971 120. Glenner GG, Ein D, Eanes ED, Bladen HA, Terry W, Page
DL: Creation of “amyloid” fibrils from Bence Jones proteins in vitro. Science 174:7 12, 197 1 121. Terry WD, Page DL, Kimura S, Isobe T, Osserman EF,
Glenner GG: Structural identity of Bence Jones and amyloid fibril proteins in a patient with plasma cell dyscrasia and amyloidosis. J Clin Invest 52:1276, 1973 122. Osserman EF, Merlini G, Butler VP: Multiple myeloma and
related plasma cell dyscrasias. JAMA 258:2930, 1987 123. Feiner HD: Pathology of dysproteinemia: Light chain amy-
loidosis, non-amyloid immunoglobulin deposition disease, cryoglobu-
linemia syndromes, and macroglobulinemia of Waldenstrom. Hum Pathol 19:1255, 1988 124. Buxbaum J: Aberrant immunoglobulin systhesis in light
chain amyloidosis. Free light chain and light chain fragment production by human bone marrow cells in short-term tissue culture. J Clin Invest 78:798, 1986 125. Parr DM, Pruzanski W, Scott JG, Mills DM: Primary
amyloidosis with plasmacytic dyscrasia and a tetramer of Bence Jones lambda globulin in the serum and urine. Blood 37:473, 1971 126. Buxbaum JN, Hurley ME, Chuba J, Spito T: Amyloidosis of
the AL type. Clinical, morphologic and biochemical aspects of the response to therapy with alkylating agents and prednisone. Am J Med 67:867,1979 127. Kosaka M, Iishi Y, Okakawa K, Saito S, Sugihara J, Muto
Y: Tetramer Bence Jones protein in the immunoproliferative dis- eases. Angioimmunoblastic lymphadenopathy, primary amyloidosis, and multiple myeloma. Am J Clin Pathol 91:639, 1989 128. Kyle RA, Greipp PR, Banks PM: The diverse picture of
gamma heavy-chain disease. Report of seven cases and review of literature. Mayo Clin Proc 56:439, 198 1 129. Cogne M, Bakhshi A, Korsmeyer SJ, Guglielmi P: Gene
mutations and alternate RNA splicing result in truncated Ig L chains in human y H chain disease. J Immunol 141:1738, 1988 130. Matuchansky C, Cogne M, Lemaire M, Babin P, Trouchard
G, Chamaret S, Preud‘homme JL: Nonsecretory a-chain disease with immunoproliferative small intestinal disease. N Engl J Med 320:1534,1989 131. Pras M, Zaretzky J, Frangione B, Franklin EC: AA protein
in a case of “primary” or “idiopathic” amyloidosis. Am J Med 68:291, 1980 132. Cornwell GG, Thomas B, Kyle RA, Sletten K, Westermark
P Immunohistochemical typing of tissues from 100 patients with systemic amyloidosis, in Isobe T, Araki S, Uchino F, Kit0 S, Tsubura E (eds): Amyloid and Amyloidosis. New York, Plenum, 1988, p 179
133. Linke RP, Tischendorf FW, Zucker-Franklin D, Franklin EC: The formation of amyloid-like fibrils in vitro from Bence Jones proteins of the VXl subclass. J Immunol 11 1:24, 1973 134. Linke RP, Zucker-Franklin D, Franklin EC: Morphologic,
chemical, and immunologic studies of amyloid-like fibrils formed from Bence Jones proteins by proteolysis. J Immunol 1 1 l:lO, 1973 135. Epstein WV, Tan M, Wood IS: Formation of “amyloid”
fibrils in vitro by action of human kidney lysosomal enzymes on Bence Jones protein. J Lab Clin Med 84:107, 1974 136. Solomon A, Frangione B, Franklin EC: Bence Jones proteins
and light chains of immunoglobulins. Preferential association of the VhVl subgroup of human light chains with amyloidosis AL(X). J Clin Invest 70:453, 1982 137. Solomon A: Light chains of immunoglobulins: Structural-
genetic correlates. Blood 68:603, 1986 138. Solomon A: Clinical implications of monoclonal light chains.
SeminOncol13:341,1986 139. Benson MD, Dwulet FE, Madura D, Wheeler G: Structural
analysis of a lambda IV primary amyloid protein, in Isobe T, Araki S, Uchino F, Kito S, Tsubura E (eds): Amyloid and Amyloidosis. New York, NY, Plenum, 1988, p 163 140. Cornwell GG: Progress in multiple myeloma, amyloidosis,
and related monoclonal dysproteinemias. Curr Hematol Oncol 5:121, 1987 141. Glenner GG, Terry WD, Isersky C: Amyloidosis: Its nature
and pathogenesis. Semin Hematol 10:65, 1973 142. Merlini G, Farhangi M, Osserman E F Monoclonal immuno-
globulins with antibody activity in myeloma, macroglobulinemia and related plasma cell dyscrasias. Semin Oncol 13:350, 1986 143. Hobbs JR: Immunochemical classes of myelomatosis. Br J
Hematol 16:599, 1969
542 MARVIN J. STONE
144. Kyle RA: Amyloidosis, in Wiernik PH, Canellos GP, Kyle RA, Schiffer CA, (eds): Neoplastic Diseases of the Blood, vol2. New York, Churchill Livingstone, 1985, p 607
145. Franklin EC: Some unsolved problems in the amyloid diseases. Am J Med 66:365, 1979
146. Pras M: Systemic amyloidosis: Tissue specific variability in the primary structure of amyloid proteins, in Isobe T, Arab S, Uchino F, Kito S, Tsubura E (eds): Amyloid and Amyloidosis. New York, NY, Plenum, 1988, p 41
147. Zucker-Franklin D, Franklin EC: Intracellular localization of human amyloid by fluorescence and electron microscopy. Am J Pathol59:23,1970
148. Durie BGM, Persky B, Soehnlen BJ, Grogan TM, Salmon SE: Amyloid production in human myeloma stem-cell culture, with morphologic evidence of amyloid secretion by associated macro- phages. N Engl J Med 307:1689,1982
149. Nomura S, Kanoh T, Uchino H: Intracellular formation of amyloid fibrils in myeloma. Cytochemical, immunochemical, and electron microscopic observations. Cancer 54:303, 1984
150. Tong AW, Lee JC, Stone MJ: Expression of plasma cell- associated non-light chain antigens in patients with plasma cell dyscrasia and amyloidosis, in Isobe T, Araki S, Uchino F, Kito S, Tsubura E (eds): Amyloid and Amyloidosis. New York, NY, Plenum, 1988, p 185
15 1. Picken MM, Gallo G, Buxbaum J, Frangione B: Character- ization of renal amyloid derived from the variable region of the lambda light chain subgroup 11. Am J Pathol 124:82, 1986
152. Randall RE, Williamson WC, Mullinax F, Tung MY, Still WJS: Manifestations of systemic light chain deposition. Am J Med 60:293, 1976
153. Preud’homme JL, Morel-Maroger L, Bronet JC, Cerf M, Mignon F, Guglielmi P, Seligmann M: Synthesis of abnormal immunoglobulins in lymphoplasmacytic disorder with visceral light chain deposition. Am J Med 69:703,1980
154. Ganeval D, Noel LH, Preud’homme JL, Droz D, Grunfeld JP: Light-chain deposition disease: Its relation with AL-type amy- loidosis. Kidney Int 26:1, 1984
155. Gallo G, Picken M, Buxbaum J, Frangione B: The spectrum of monoclonal immunoglobulin deposition disease associated with immunocytic dyscrasias. Semin Hematol26:234, 1989
156. Silva FG, Meyrier A, Morel-Maroger L, Pirani C L Prolifer- ative glomerulonephropathy in multiple myeloma. J Pathol 130229, 1980
157. Gallo GR, Feiner HD, Katz LA, Feldman GM, Correa EB, Chuba JV, Buxbaum JN: Nodular glomerulopathy associated with nonamyloidotic kappa light chain deposits and excess immunoglobu- lin light chain synthesis. Am J Pathol99:621, 1980
158. Fang LST: Light-chain nephropathy. Kidney Int 27:582, 1985
159. Palant CE, Bonitati J, Bartholomew WR, Brentjens JR, Walshe JI, Bentzel CJ: Nodular glomerulosclerosis associated with multiple myeloma. Role of light chain isoelectric point. Am J Med 80:98, 1986
160. Venkataseshan VS, Faraggiana T, Hughson MD, Buchwald D, Olesnicky L, Goldstein MH: Morphologic variants of light-chain deposition disease in the kidney. Am J Nephrol8:272, 1988
161. Sturgill BC, Bolton WK, Griffith KM: Congo red-negative amyloidosis-like glomerulopathy. Hum Pathol 16:220, 1985
162. Benditt EP, Eriksen M, Hermodsen MA, Ericsson LH: The major proteins of human and monkey amyloid substance: Common properties including unusual N-terminal amino acid sequences. FEBS Lett 19:169, 1971
163. Husby G, Sletten K. Chemical and clinical classification of amyloidosis 1985: Scand J Immunol 23:253, 1986
164. Hind CRK, Baltz ML, Pepys MB: Amyloidosis, in Dela- more IW (ed): Multiple myeloma and other paraproteinaemias. Edinburgh, UK, Churchill Livingstone, 1986, p 234
165. Eriksen N, Benditt EP: Isolation and characterization of the amyloid-related apoprotein (SAA) from human high density lipopro- tein. Proc Natl Acad Sci USA 77:6860, 1980
166. Bausserman LL, Herbert PN, McAdam KPWJ: Heteroge- neity of human serum amyloid A proteins. J Exp Med 152:641, 1980
167. De Beer FC, Mallya RK, Fagan EA, Lanham JG, Hughes GRV, Pepys MB: Serum amyloid-A protein concentration in inflam- matory diseases and its relationship to the incidence of reactive systemic amyloidosis. Lancet 2:231, 1982
168. Brinckerhoff CE, Mitchell TI, Karmilowicz MJ, Kluve- Beckerman B, Benson MD: Autocrine induction of collagenase by serum amyloid A-like and 0,-microglobulin-like proteins. Science 243:655,1989
169. Levin M, Franklin EC, Frangione B, Pras M: The amino acid sequence of a major nonimmunoglobulin component of some amyloid fibrils. J Clin Invest 51:2773, 1972
170. Sletten K, Husby G: The complete amino-acid sequence of nonimmunoglobulin amyloid fibril protein AS in rheumatoid arthri- tis. Eur J Biochem 41:117, 1974
171. Linke RP, Huhn D, Nathrath WBJ: Diagnosis of AA- amyloidosis using monoclonal antibodies: Application to paraffin and ultrathin sections as well as to urinary sediments, in Isobe T, Araki S, Uchino F, Kit0 S, Tsubura E (eds): Amyloid and Amyloid- osis. New York, NY, Plenum, 1988, p 247
172. Meyerhoff J: Familial Mediterranean fever: Report of a large family, review of the literature, and discussion of the frequency of amyloidosis. Medicine 59:66,1980
173. Blum A, Gafni J, Sohar E, Shibolet S, Heller H: Amyloid- osis as the sole manifestation of familial Mediterranean fever (FMF). Further evidence of its genetic nature. Ann Intern Med 57:795, 1962
174. Gertz MA, Petitt RM, Perrault J, Kyle RA: Autosomal dominant familial Mediterranean fever-like syndrome with amy- loidosis. Mayo Clin Proc 62:1095, 1987
175. Linke RP, Heilman KL, Nathrath WBJ, Eulitz M: Identifi- cation of amyloid A protein in a sporadic Muckle-Wells syndrome. Lab Invest 48:698, 1983
176. Gorevic PD, Greenwald M, Frangione B, Pras M, Franklin EC: The amino acid sequence of duck amyloid A (AA) protein. J Immunol118:1113,1977
177. Lavie G, Zucker-Franklin D, Franklin EC: Degradation of serum amyloid A protein by surface-associated enzymes of human blwd monocytes. J Exp Med 148:1020,1978
178. Fuks A, Zucker-Franklin D: Impaired Kupffer cell function precedes development of secondary amyloidosis. J Exp Med 161: 1013,1985
179. Maury CPJ, Teppo AM: Mechanism of reduced amyloid-A- degrading activity in serum of patients with secondary amyloidosis. Lancet 2:234, 1982
180. Meek RL, Hoffman JS, Benditt EP: Amyloidogenesis. One serum amyloid A isotype is selectively removed from the circulation. J Exp Med 163:499,1986
181. Yamamoto KI, Shiroo M, Migita S: Diverse gene expression for isotypes of murine serum amyloid A protein during acute phase reaction. Science 232:227, 1986
182. Woo P, OBrien J, Robson M, Ansell BM: A genetic marker for systemic amyloidosis in juvenile arthritis. Lanet 2:767, 1987
183. Benson MD, Wallace MR: Amyloidosis, in Scriver CR, Beaudet AL, Sly WS, Valle D (eds): The Metabolic Basis of Inherited Disease, ed 6, vol 2. New York, NY, McGraw-Hill, 1989, p 2439
AMYLOIDOSIS 543
184. Andrade C, Araki S, Block WD, Cohen AS, Jackson CE, Kuroiwa Y, McKusick VA, Nissim J, Sohar E, Van Allen MW: Hereditary amyloidosis. Arthritis Rheum 13:902, 1970
185. Benson MD, Dwulet FE: Prealbumin and retinol binding protein serum concentrations in the Indiana type hereditary amy- loidosis. Arthritis Rheum 26:1493, 1983
186. Westermark P, Pitkanen P, Benson L, Vahlquist A, Olofsson BO, Cornwell GG: Serum prealbumin and retinol-binding protein in the prealbumin-related senile and familial forms of systemic amy- loidosis. Lab Invest 52:314,1985
187. Saraiva MJM, Birken S, Cost PP, Goodman DS: Amyloid fibril protein in familial amyloidotic polyneuropathy, Portuguese type. Definition of molecular abnormality in transthyretin (prealbu- min). J Clin Invest 74104,1984
188. Dwulet FE, Benson MD: Characterization of a transthyretin (prealbumin) variant associated with familial amyloidotic polyneu- ropathy type I1 (Indiana/Swiss). J Clin Invest 78:880,1986
189. Benson MD, Wallace MR, Tejada E, Baumann H, Page E Hereditary amyloidosis: Description of a new American kindred with late onset cardiomyopathy. Appalachian amyloid. Arthritis Rheum 30:195,1987
190. Staunton H, Dervan P, Kale R, Linke RP, Kelly P: Heredi- tary amyloid polyneuropathy in northwest Ireland. Brain 1 1 0 123 1, 1987
191. Maury CPJ, Teppo AM, Karinemi AL, Koeppen AH: Amyloid fibril protein in familial amyloidosis with cranial neuropa- thy and corneal lattice dystrophy (FAP type IV) is related to transthyretin. Am J Clin Pathol89:359, 1988
192. Wallace MR, Dwulet FE, Williams EC, Conneally PM, Benson MD: Identification of a new hereditary amyloidosis prealbu- min variant, Tyr-77, and detection of the gene by DNA analysis. J Clin Invest 81:189,1988
193. Wallace MR, Benson MD: DNA tests for four prealbumin mutations in hereditary amyloidosis, in Isobe T, Araki S, Uchino F, Kito S, Tsubura E (4s): Amyloid and Amyloidosis. New York, NY, Plenum, 1988, p 355
194. Holt IJ, Harding AE, Middleton L, Chrysostomou G, Said G, King RHM, Thomas PK: Molecular genetics of amyloid neurop athy in Europe. Lancet 1524, 1989
195. Nichols WC, Dwulet FE, Liepnieks J, Benson MD: Variant apolipoprotein AI as a major constituent of a human hereditary anyloid. Biochem Biophys Res Commun 156:762, 1988
196. Fenves AZ, Emmett M, White MG, Greenway G, Michaels DB: Carpal tunnel syndrome with cystic bone lesions secondary to amyloidosis in chronic hemodialysis patients. Am J Kidney Dis 7:130, 1986
197. Bardin T, Zingraff J, Shirahama T, Noel LH, Droz D, Voisin MC, Drueke T, Dry11 A, Skinner M, Cohen As, Kuntz D: Hemodialysis-associated amyloidosis and beta-2 microglobulin. Clin- ical and immunohistochemical study. Am J Med 83:419,1987
198. Casey TT, Stone WJ, DiRaimondo CR, Brantley BD, DiRaimondo CV, Gorevic PH, Page DL: Tumoral amyloidosis of bone of beta,-microglobulin origin in association with long-term hemodialysis: A new type of amyloid disease. Hum Pathol 17:731, 1986
199. Ullian ME, Hammond WS, Alfrey AC, Schultz A, Molito- ris BA: Beta-2-microglobulin-associated amyloidosis in chronic hemodialysis patients with carpal tunnel syndrome. Medicine 68: 107,1989
200. Gorevic PD, Casey TT, Stone WJ, DiRaimondo CR, Prelli FC, Frangione B: Beta-2 microglobulin is an amyloidogenic protein in man. J Clin Invest 76:2425,1985
201. Gejyo F, Yamada T, Odani S, Nakagawa Y, Arakawa M, Kunitomo T, Kataoka H, Suzuki M, Hirasawa Y, Shirahama T,
Cohen AS, Schmid K: A new form of amyloid protein associated with chronic hemodialysis was identified as @,-microglobulin. Bio- chem Biophys Res Commun 129:701, 1985
202. Gorevic PD, Munoz PC, Casey TT, DiRaimondo CR, Stone WJ, Prelli FC, Rodrigues MM, Poulik MD, Frangione B: Polymer- ization of intact &-microglobulin in tissue causes amyloidosis in patients on chronic hemodialysis. Proc Natl Acad Sci USA 83:7908, 1986
203. Cunningham BA, Wang SL, Berggard I, Peterson PA: The complete amino acid sequence of @,-microglobulin. Biochemistry 12:4811, 1973
204. Homma N, Gejyo F, Isemura M, Arakawa M: 82- Microglobulin binding to collagen: An amyloidogenic factor in chronic hemodialysis patients. In Isobe T, Araki S, Uchino F, Kit0 S , Tsubura E (eds): Amyloid and Amyloidosis. New York, NY, Plenum, 1988, p 623
205. Mozar HN, Bal DG, Howard JT: Perspectives on the etiology of Alzheimer’s disease. JAMA 257:1503, 1987
206. Glenner GG: The pathobiology of Alzheimer’s disease. Ann Rev Med 40:45,1989
207. Selkoe DJ: Altered structural proteins in plaques and tangles: What do they tell us about the biology of Alzheimer’s disease? Neurobiol Aging 7:425, 1986
208. Glenner GG, Wong CW: Alzheimer’s disease: Initial report of the purification and characterization of a novel cerebrovascular amyloid protein. Biochem Biophys Res Commun 120885, 1984
209. Friedland RP, Koss E, Haxby JV, Grady CL, Luxenberg J, Schapiro MB, Kaye J: Alzheimer disease: Clinical and biological heterogeneity. Ann Intern Med 109:298, 1988
210. Tanzi RE, Gusella JF, Watkins PC, Bruns GAP, St George- Hyslop P, Van Keuren ML, Patterson D, Pagan S, Kumit DM, Neve RL: Amyloid @ protein gene: cDNA, mRNA distribution and genetic linkage near the Alzheimer locus. Science 235880, 1987
211. Tanzi RE, Bird ED, Latt SA, Neve RL: The amyloid @-protein gene is not duplicated in brains from patients with Alzheimer’s disease. Science 238:666, 1987
212. Rumble B, Retallack R, Hilbich C, Simms G, Multhaup G, Martin R, Hockey A, Montgomery P, Beyreuther K, Masters CL: Amyloid A4 protein and its precursor in Down’s syndrome and Alzheimer’s disease. N Engl J Med 320:1446, 1989
213. Selkoe DJ: Aging, amyloid, and Alzheimer’s disease. N Engl J Med 320:1484,1989
214. Kang J, Lemaire HG, Unterbeck A, Salbaum JM, Masters CL, Grzeschik KH, Multhaup G, Beyreuther K, Muller-Hill B: The precursor of Alzheimer’s disease amyloid A4 protein resembles a cell-surface receptor. Nature 325:733, 1987
215. Schubert D, Schroeder R, LaCorbiere, Saitoh T, Cole G: Amyloid j3 protein precursor is possibly a heparan sulfate proteogly- can core protein. Science 241:223, 1988
216. Palmert MR, Golde TE, Cohen ML, Kovacs DM, Tanzi RE, Gusella JF, Usiak MF, Younkin LH, Younkin SG: Amyloid protein precursor messenger RNAs: Differential expression in Alzheimer’s disease. Science 241:1080, 1988
217. Selkoe DJ, Podlisny MB, Joachim CL, Vickers EA, Lee G, Fritz LC, Oltersdorf T: @-Amyloid precursor protein of Alzheimer disease occurs as 110- to 135-kilodalton membrane-associated pro- teins in neural and nonneural tissues. Proc Natl Acad Sci USA 85:7341,1988
218. Giaccone G, Tagliavini F, Linoli G, Bouras C, Frigerio L, Frangione B, Bugiani 0: Down patients: Extracellular preamyloid deposits precede neuritic degeneration and senile plaques. Neurosci Lett 97:232, 1989
219. Abraham CR, Selkoe DJ, Potter H: Immunochemical iden-
544 MARVIN J. STONE
tification of the serine protease inhibitor a,-antichymotrypsin in the brain amyloid deposits of Alzheimer’s disease. Cell 52:487, 1988
220. Gudmundsson G, Hallgrimsson J, Jonasson TA, Bjarnason 0: Hereditary cerebral hemorrhage with amyloidosis. Brain 95:387, 1972
221. Wattendorf AF, Botts GTAM, Went LN, Endtz LJ: Famil- ial cerebral amyloid angiopathy presenting as recurrent cerebral hemorrhage. J Neurol Sci 55:121, 1982
222. Vinters HV: Cerebral amyloid angiopathy. A critical review. Stroke 18:311,1987
223. Van Duinen SG, Castano EM, Prelli F, Bots GTAB, Luyendijk W, Frangione B: Hereditary cerebral hemorrhage with amyloidosis in patients of Dutch origin is related to Alzheimer’s disease. Proc Natl Acad Sci USA 84:5991, 1987
224. Ghiso J, Jensson 0, Frangione B: Amyloid fibrils in heredi- tary cerebral hemorrhage with amyloidosis of Icelandic type is a variant of y-trace basis protein (cystatin C). Proc Natl Acad Sci USA 83:2974,1986
225. Sletten K, Westermark P, Natvig JB: Characterization of amyloid fibril proteins from medullary carcinoma of the thyroid. J Exp Med 143:993,1976
226. Dayal Y, Tahjian AH, Wolfe HJ: Immunocytochemical localization of calcitonin-producing cells in a stromal carcinoid with amyloid stroma. Cancer 43:1331, 1979
227. Johansson B, Wernstedt C, Westermark P Isolated atrial amyloid (IAA): A cardiac amyloid of endocrine origin, in Isobe T, Araki S, Uchino F, Kit0 S, Tsubura E (eds): Amyloid and Amyloid- osis. New York, NY, Plenum, 1988, p 661
228. Yoneda K, Watanabe H, Yanagihara M, Mori S: Immuno- histochemical staining properties of cutaneous amyloidosis using anti-keratin monoclonal antibodies, in Isobe T, Araki S, Uchino F, Kito S, Tsubura E (eds): Amyloid and Amyloidosis. New York, NY, Plenum, 1988, p 709
229. Kyle RA: Diagnosis and management of multiple myeloma and related disorders. Prog Hematol 14:257,1986
230. Hazenberg BPC, van Rijswijk MH, Meijer S, Marrink J, Limberg PC, Janssen S: Systemic amyloidosis: A clinical survey of 162 cases, in Isobe T, Araki S, Uchino F, Kito S, Tsubura E (eds): Amyloid and Amyloidosis. New York, NY, Plenum, 1988, p 821
231. Fields M, Polliack A, Laufer A: Resorption of amyloid and enzymatic studies in amyloidosis. Israel J Med Sci 92375, 1973
232. Glenner GG, Future directions in amyloid research, in Marrink J, van Rijswijk MH (eds): Amyloidosis. Dordrecht, Marti- nus Nijhoff, 1986, p 357
233. Natvig JB, Skogan B, Amundsen E: Enhanced degradation of serum amyloid protein SAA in vivo by proteolytic enzymes, in Isobe T, Araki S, Uchino F, Kit0 S, Tsubura E (eds): Amyloid and Amyloidosis. New York, NY, Plenum, 1988, p 119
234. Shirahama T, Cohen AS: Blockage of amyloid induction of colchicine in an animal model. J Exp Med 140:1102, 1974
235. Zemer D, Revach M, Pras M, Modan B, Schor S, Sohar E, Gafri J: A controlled trial of colchicine in preventing attacks of familial Mediterranean fever. N Engl J Med 291:932, 1974
236. Dinarello CA, Wolff SM, Goldfinger SE, Dale DC, Alling DW: Colchicine therapy for familial Mediterranean fever. A double- blind trial. N Engl J Med 291:934, 1974
237. Wright DG, Wolff SM, Fauci AS, Alling DW: Efficacy of intermittent colchicine therapy in familial Mediterranean fever. Ann Intern Med 86:162,1977
238. Zemer D, Pras M, Sohar E, Modan M, Cabili S, Gafni J: Colchicine in the prevention and treatment of the amyloidosis of familial Mediterranean fever. N Engl J Med 314:1001,1986
239. Jones NF, Hilton PJ, Tighe JR, Hobbs JR: Treatment of “primary” renal amyloidosis with melphalan. Lancet 2:616,1972
240. Cohen HJ, Lessin LS, Hallal J, Burkholder P Resolution of
primary amyloidosis during chemotherapy. Studies in a patient with nephrotic syndrome. Ann Intern Med 82:466, 1973
241. Horne M K Improvement in amyloidosis. Ann Intern Med 83:281, 1975 (letter)
242. Kyle RA, Greipp PR: Primary systemic amyloidosis: Com- parison of melphalan and prednisone versus placebo. Blood 52:818, 1978
243. Corkery J, Bern MM, Tullis JL: Resolution of amyloidosis and plasma-cell dyscrasia with combination chemotherapy. Lancet 2:425, 1978 (letter)
244. Schwartz RS, Cohen JR, Schrier SL Therapy of primary amyloidosis with melphalan and prednisone. Arch Intern Med 139:1144,1979
245. Kyle RA, Wagoner RD, Holley K E Primary systemic amyloidosis. Resolution of the nephrotic syndrome with melphalan and prednisone. Arch Intern Med 142:1445, 1982
246. Kyle RA, Greipp PR, Garton JP, Gertz MA: Primary systemic amyloidosis. Comparison of melphalan/prednisone versus colchicine. Am J Med 79:708, 1985
247. Kyle RA, Greipp PR, OFallon WM: Primary systemic amyloidosis: Multivariate analysis for prognostic factors in 168 cases. Blood 68:220, 1986
248. Fielder K, Durie BGM: Primary amyloidosis associated with multiple myeloma. Predictors of successful therapy. Am J Med 80:413, 1986
249. Gertz MA, Kyle RA: Response of primary hepatic amyloido- sis to melphalan and prednisone: A case report and review of the literature. Mayo CIin Proc 61:218, 1986
250. Fritz DA, Luggen ME, Hess EV: Unusual longevity in primary systemic amyloidosis: A 19-year survivor. Am J Med 86:245, 1989
25 1. Mery JP, Mostefa S: Remission in renal amyloidosis. Ann Intern Med 83581, 1975
252. Michael J, Jones N F Spontaneous remissions of nephrotic syndrome in renal amyloidosis. Br Med J 1:1592, 1978
253. Benson MD: Treatment of AL amyloidosis with melphalan, prednisone, and colchicine. Arthritis Rheum 29:683,1986
254. Cohen AS, Rubinow A, Anderson JJ, Skinner M, Mason JH, Libbey C, Kayne H: Survival of patients with primary (AL) amyloidosis. Colchicine-treated cases from 1976 to 1983 compared with cases seen in previous years (1961 to 1973). Am J Med 82:1182, 1987
255. Osserman EF, Sherman WF, Kyle RA: Further studies of therapy of amyloidosis with dimethylsulfoxide (DMSO), in Glenner GG, Pinho e Costa P, de Freitas F (eds) Amyloid and Amyloidosis. Amsterdam, Excerpta Medica, 1980, p 563
256. Isobe T, Matsumoto J, Schimizu S, Fujita T, Kashiwabara T: DMSO therapy using dermal application to patients with sys- temic amyloidosis, in Isobe T, Araki S , Uchino F, Kito S, Tsubura (4s) : Amyloid and Amyloidosis. New York, NY, Plenum, 1988, p 815
257. Hardt F: Acceleration of casein induced amyloidosis in mice by immunosuppressive agents. Acta Pathol Microbiol Scand [A] 79:61, 1971
258. Rubinow A, Skinner M, Cohen AS: Digoxin sensitivity in amyloid cardiomyopathy. Circulation 63:1285, 1981
259. Gertz MA, Falk RH, Skinner M, Cohen AS, Kyle R A Worsening of congestive heart failure in amyloid heart disease treated by calcium channel-blocking agents. Am J Cardiol 55:1645, 1985
260. Gertz MA, Skinner M, Connors LH, Falk RH, Cohen AS, Kyle RA: Selective binding of nifedipine to amyloid fibrils. Am J Cardiol55:1646, 1985
261. Suzuki T, Azuma T, Araki S, Ikegawa S, Kito S, Matsuba- yashi H, Yanagisawa N, Ikeda S: Treatment of autonomic dysfunc-

AMYLOIDOSIS 545
tion with ~-threo-3,4-dihydroxyphenylserine in patients with famil- ial amyloidotic polyneuropathy: A multicenter study, in Isobe T, Araki S, Uchino F, Kit0 S, Tsubura E (eds): Amyloid and Amyloid- osis. New York, NY, Plenum, 1988, p 851
262. Coutinho P, Macedo E, Estacio A, Saraiva A, Costa PP, Saraiva JM: Periodic plasma exchanges in the treatment of familial amyloid polyneuropathy: Preliminary results, in Isobe T, Araki S, Uchino F, Kit0 S, Tsubura E (eds): Amyloid and Amyloidosis. New York, NY, Plenum, 1988, p 845
263. Benson MD, Skinner M, Cohen AS: Amyloid deposition in a renal transplant in familial Mediterranean fever. Ann Intern Med 87:31, 1977
264. Jacob ET, Bar-Nathan N, Shapira Z, Gafni J: Renal
transplantation in the amyloidosis of familial Mediterranean fever. Experience in ten cases. Arch Intern Med 139:1135, 1979
265. Pasternack A, Ahonen J, Kuhlback B: Renal transplantation in 45 patients with amyloidosis. Transplantation 42598, 1986
266. Hosenpud JD, Uretsky BF, O’Connell JB, Olivari M: Cardiac transplantation for amyloidosis: Results of a multicenter survey. J Heart Transplant 8:99, 1989 (abstract 63)
267. Gallo GR, Feiner HD, Chuba JV, Beneck D, Marion P, Cohen DH: Characterization of tissue amyloid by immunofluores- ence microscopy. Clin Immunol Immunopathol39:479,1986
268. Heller H, Gafni J, Sohar E The inherited systemic amy- loidosis, in Stanbury JB, Wyngaarden JB, Fredrickson DS (eds): The Metabolic Basis of Inherited Disease, ed 3. New York, NY, McGraw-Hill, 1966, p 995