biotherapy interferon- : introna 3–5 muxiii–v/week peginterferon alpha 50–100 gxi/week –...
TRANSCRIPT

Biotherapy
• Interferon-: IntronA 3–5 MUxIII–V/week• PegInterferon alpha 50–100 gxI/week
– Adjust the dose according to tolerance and leukocyte count <3.0
• Octreotide, Lanreotide: – Sandostatin 100–500 gx2–3– Sandostatin LAR 20–30 mg/3–4 weeks i.m.– Somatuline Autogel 90–120 mg/4 weeks s.c.

Biotherapy
Treatment Objective response
Stable disease
Biochemical/symptomatic
alpha-interferon 10–15% 40–60% ≤50%
octreotide/lanreotide <10% 30–50% 60–90%
Treatment Objective response
Stable disease
Biochemical/symptomatic
alpha-interferon 10–20% 33–100% ≤50%
octreotide/lanreotide <10% 24–57% 40–80%
EPT
Carcinoids

TreatmentTreatment Disease Objective
response
alpha-interferon EPT, carcinoids 12–15%
octreotide/lanreotide EPT, carcinoids 0–6%
streptozocin + 5-FU/doxorubicin EPT 6–69%
cisplatin + etoposide EPT, foregut 7–39%
DTIC + 5-FU + epirubicin EPT 27%
Paclitaxel EPT, carcinoids 4%
Docetaxel Carcinoids 0
Topotecan EPT, carcinoids 0
Gemcitabine EPT, carcinoids 0
Granberg 2007

TreatmentTreatment Disease Objective
response
Temozolomide EPT, carcinoids 17%
Temozolomide + capecitabine EPT 59%
Temozolomide + thalidomide EPT, carcinoids 45%, 7%
Temozolomide + bevacizumab EPT, carcinoids 14%
Sunitinib EPT, carcinoids 10%
Temsirolimus EPT, carcinoids 5%
Bortezomib EPT, carcinoids 0
Endostatin EPT, carcinoids 0
Granberg 2007

Temozolomide
All patients (n=36)
EPT (n=12)
Bronchial carcinoids
(n=13)
Thymic carcinoids
(n=7)
Other (n=4)
PR 5 (14%) 1 (8%) 4 (31%) 0 0
SD 19 (53%) 8 (67%) 4 (31%) 5 (71%) 2 (50%)
PD 12 (33%) 3 (25%) 5 (38%) 2 (29%) 2 (50%)
Ekeblad 2007

Temozolomide – before and after
Decrease of the endocrine panceatic tumor

Temozolomide – before and after
Decrease of the liver metastases

Temozolomide + capecitabine
Isacoff 2006
Patients:• 17 patients with advanced NET
Treatment: • Capecitabine 1000 mg b.i.d. day 1–14• Temozolomide 150–200 mg/m2 day 10–14• Cycle length 28 days
Results:• CR 1/17 (6%)• PR 9/17 (53%)
– Median response duration 9 months• Biochemical response 6/7 (86%)
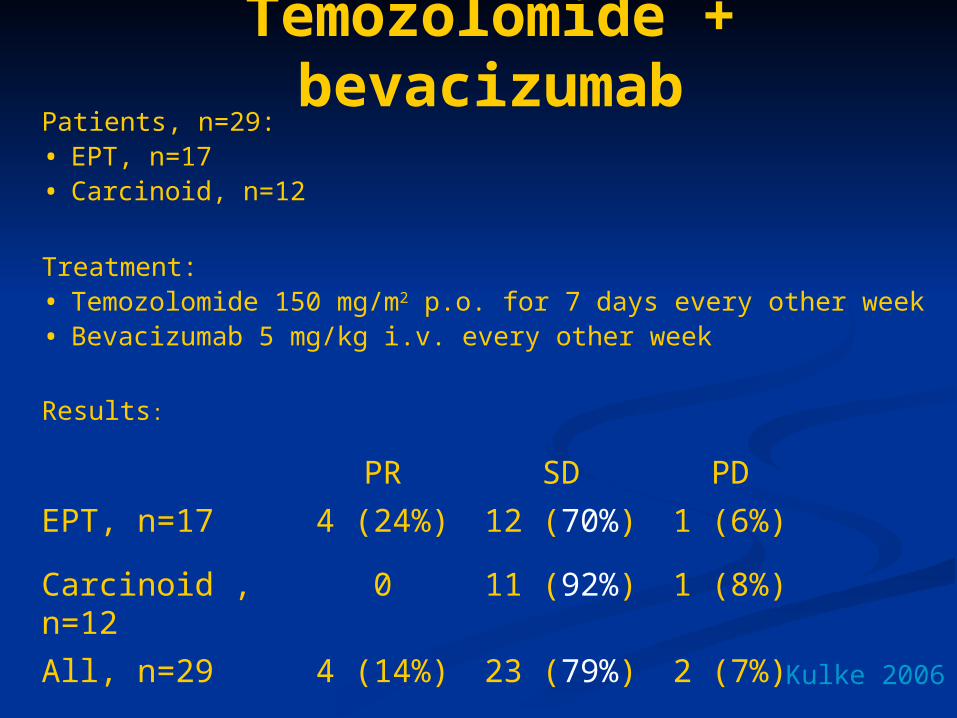
Temozolomide + bevacizumab
Kulke 2006
Patients, n=29:• EPT, n=17• Carcinoid, n=12
Treatment: • Temozolomide 150 mg/m2 p.o. for 7 days every other week• Bevacizumab 5 mg/kg i.v. every other week
Results:PR SD PD
EPT, n=17 4 (24%) 12 (70%) 1 (6%)
Carcinoid , n=12 0 11 (92%) 1 (8%)
All, n=29 4 (14%) 23 (79%) 2 (7%)

Temozolomide + thalidomide
Kulke 2006
Patients, n=28 (carcinoid, n=14 EPT, n=11, pheo, n=3)
Treatment: Temozolomide 150 mg/m2 for 7 days every 2 week Thalidomide 50–400 mg daily (median 100 mg)
Results: CR PR CR+PR SD PD
Carcinoid, n=14 1 1 (14%)
EPT, n=11 1 4 5 (45%)
All, n=28 7 (25%) 19 (68%) 2 (7%)
Conclusions: • Temozolomide + thalidomide is active in NETs• Temozolomide + thalidomide seems more active in EPTs
than in carcinoids

Sunitinib
Kulke 2006
Patients:• EPT, n=52• Carcinoid, n=41
Treatment: • Sunitinib 50 mg/day for 4 weeks, followed by a 2 week break
Results: PR SD PD
EPT, n=52 7 (13.5%) 40 (77%) 3 (5.5%)
Carcinoid , n=41 2 (5.1%) 36 (92.3%) 1 (2.6%)

Treatment
Liver embolization Objective response
Carcinoids 38–81%
EPT 25–60%
All 25–81%
Chemo-embolization
Carcinoids 7–44%
EPT 11–50%
All 7–50%

Treatment
Liver embolization Objective response
% no
Carcinoids 81% 34/42
EPT 25% 8/32
Chemo-embolization Objective response
% no
Carcinoids 44% 12/27
EPT 50% 11/22
Gupta 2005

Targeted irradiation therapy
• 111In-DTPA0 -octreotide• 90Y-DOTA0 ,Tyr3 -octreotide• 177Lu-DOTA0,Tyr3-octreotate• 131I-MIBG• 90Y-SIR-Spheres

Isotopes• 111Indium
– -emitter
– T1/2 2.83 days
• 90Yttrium– - emitter
– T1/2 2.67 days
• 177Lutetium– - emitter(+ weak - emitter)
– T1/2 6.71 days
• 131Iodine– - emitter + - emitter
– T1/2 8.02 days

Isotopes
T1/2 (days) Range in tissue
Average Max
111In 2.83 10 m
90Y 2.67 4 mm 12 mm
177Lu 6.71 0.5 mm 2 mm
Breeman 2001

Grading of radionuclide uptake at somatostatin receptor scintigraphy
Grade Appearance of somatostatin receptor scintigraphy
0 No radionuclide accumulation in known tumor lesions 1 Suspected but not certain uptake in known tumor lesions 2 Accumulation in known tumor lesions, intensity less or equal to normal liver uptake 3 Clear uptake in known tumor lesions, higher than liver uptake 4 Intense uptake in known metastases

177Lu-DOTA-octreotate therapyThe Rotterdam experience
• Patients, n=131– 70 carcinoid (64 small bowel, 4 lung, 1 thymic, 1 gastric)– 33 EPT non-functioning– 8 gastrinoma– 2 insulinoma– 18 unknown
• Treatments:– Dosage 100–200 mCi– Cumulative dose 600–800 mCi (22.2 to 29.6 GBq)– Interval 6–10 weeks
Kwekkeboom 2005

177Lu-DOTA-octreotate therapyThe Rotterdam experience
CR 3 (2%)
PR 32 (26%)
MR 24 (19%)
SD 44 (35%)
PD 22 (18%)
• Higher remission rates: – higher uptake– limited no. of liver metastases– gastrinomas
• PD: low performance status extensive disease
Median time to progression: 36 mo
Serious adverse events:
• renal insufficiency (1 patient)
• liver failure (1 patient)Kwekkeboom et al, JCO, 2005
Results:Results:

177Lu-DOTA-octreotate therapyThe Uppsala experience
• 56 patients, (27 MGC, 11 EPT non-functioning, 5 gastrinoma)
• 152 treatments (1–6): Dose 200 mCi (7.4 GBq), interval 6–12 weeks
• Results, n=34, mean follow-up 7.6 months (2,8–22,6):
– 1 CR, 6 PR (21% CR+PR), 1 MR, 25 SD, 1 PD, 3 dead
• Toxicity: 26 hematological grade 3–4 (24 lymfopenia, 5 neutropenia, 3 leucopenia, 1 thrombopenia), 9 renal grade 1

Before After 15 months

Tumor responses in patients with GEP tumors, treated with different radiolabelled somatostatin analogs
Tumor Response
Center Ligand Pats. CR+PR SD PD
Rotterdam (111In-DTPA0)octr 26 0(0%) 16(62%) 10(38%)
New Orleans (111In-DTPA0)octr 26 2(8%) 21(81%) 3(12%)
Milan (90Y-DOTA0,Tyr3)octr 21 6(29%) 11(52%) 4(19%)
Basel (90Y-DOTA0,Tyr3)octr 74 18(24%) 48(65%) 8(11%)
Basel (90Y-DOTA0,Tyr3)octr 33 11(33%) 19(57%) 3(9%)
Rotterdam (90Y-DOTA0,Tyr3)octr 54 4(7%) 40(74%) 10(19%)
Rotterdam (177Lu-DOTA0,Tyr3)octr 76 23(30%) 39(51%) 14(18%)
Rotterdam (177Lu-DOTA0,Tyr3)octr 125 35(28%) 68(54%) 22(18%)
Kwekkeboom 2005

Tumor responses according to tumor type in patients with GEP tumors, treated with different radiolabelled
somatostatin analogs
Tumor Response (CR + PR)
EPT Carcinoid Unknown
Center Ligand Funct Total G-I Bronch origin Total
Basel (90Y-DOTA0,Tyr3)octr NA 37% 5% 20% 29% 24%
Basel (90Y-DOTA0,Tyr3)octr NA 33% 25% 0% 36% 33%
Milan (90Y-DOTA0,Tyr3)octr 63% 51% 35% 14% 21% 38%
Rotterdam (177Lu-DOTA0,Tyr3)octr 71% 36% 20% 100% 42% 30%
Kwekkeboom 2005

Side effects in patients with GEP tumors, treated with different radiolabelled somatostatin analogs
Grade 3/4 hematologic
Center Ligand Pats. Platelets Hb WBC Other
Rotterdam (111In-DTPA0)octr 50 10% 15% 2% 3 AML or MDS
New Orleans (111In-DTPA0)octr 27 7% 11% 7% 3 liver, 1 renal
Milan (90Y-DOTA0,Tyr3)octr 40 7% 3% 7%
Basel (90Y-DOTA0,Tyr3)octr 29 3% 7% 0% 4 renal
Basel (90Y-DOTA0,Tyr3)octr 39 0% 3% 0% 1 renal
Rotterdam (90Y-DOTA0,Tyr3)octr 60 12% 8% 13% 1 liver, 1 renal
Rotterdam (177Lu-DOTA0,Tyr3)octr 200 3% 1% 2% 1 MDS, 1 renal
Kwekkeboom 2005

Conclusion
• Somatostatin receptor mediated treatment provides a feasible, widely well tolerated therapeutic option for patients with neuroendocrine tumors
• beta emitters are promising
• Treatment with combination of 90Y and 177Lu seem to provide even better tumor control
• Best time for radioisotopes in the treatment of these patients is still to be established

131I-MIBG-treatment
Carcinoid Pheochromocytoma/paraganglioma
Response: No % No %
Radiologic 10/75 13 8/21 38
Biochemical 19/52 37 12/20 60
Symptomatic 35/72 49 19/22 86
Toxicity:
Hematologic 13/98 13 4/33 12
Nausea/vomiting 4/98 4 2/33 6
Deaths 2/98 2 3/33 9
Safford 2003–2004
Results:

Treatment
SIRT = Selective Internal Radiation Therapy
• Liver embolization with SIR-Spheres®
• SIR-Spheres® = 90Yttrium-labelled resin
microspheres
• Size ≈ 30–35 m

Selective Internal Radiation Therapy
• High dose of radioactivity delivered selectively to liver metastases
• Pre-treatment angiography to clarify the vascular anatomy
• Pre-treatment scintigraphy with 99Tc macroalbumin to assess lung shunt (≤20%)
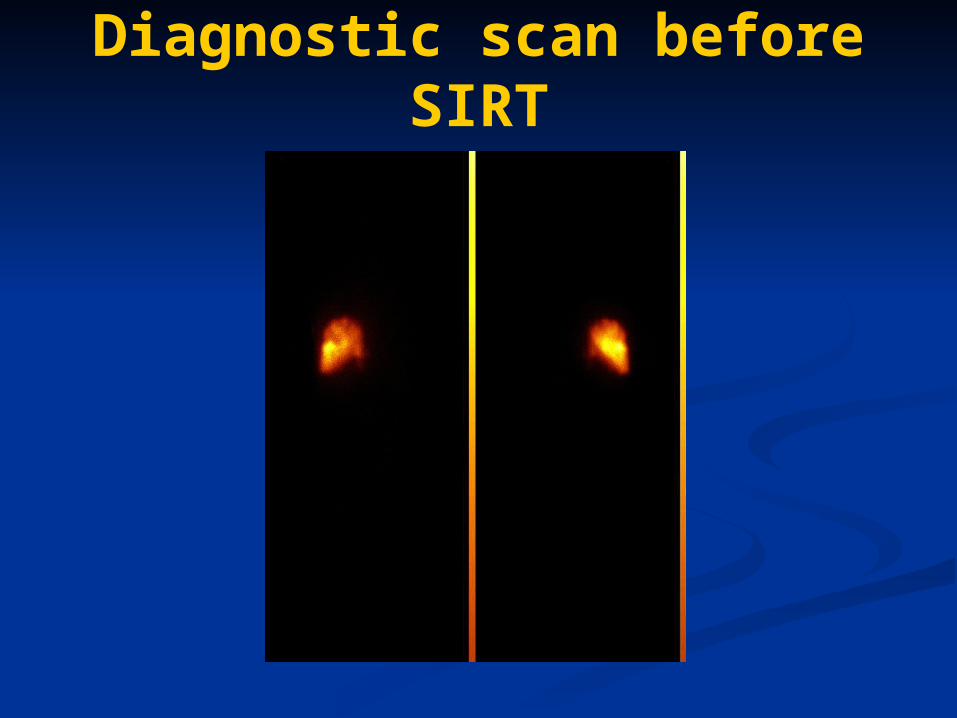
Diagnostic scan before SIRT

Selective Internal Radiation Therapy
Patients, n=34:• 15 carcinoids (10 small bowel, 2 cecum, 1 bonchial, 1
gastric, 1 rectum)• 8 endocrine pancreatic tumor• 2 medullary thyroid carcinoima• 9 unknown
Treatment:• Single injection of SIR-Spheres® in the hepatic artery• Concomitant single 7 day systemic infusion of 5-FU 225
mg/m2
Median follow-up 9.8 monthsKing 2005

Selective Internal Radiation Therapy
Results: PR PR SD SD
No % No %
1 month (n=34) 8 24% 23 68%
3 months (n=29) 6 21% 19 66%
12 months (n=10) 2 20% 6 60%
18 months (n=7) 1 14% 5 71%
King 2005
4 patients died from progresssive disease
Complications: 3 duodenal ulcers, 1 pancreatitis, 2 jaundiceAll patients experienced abdominal pain, nausea and lethargy

Selective Internal Radiation Therapy
Conclusion:
SIRT appears to have efficacy in treating unresectable neuroendocrine liver metastases
King 2005

pre 6 month9 month
SIRT in NET – Pilot Study
Patient 2: Morphological Response
El-Sheik, Barcelona 2006

SIRT – before and after

Diagnosis of midgut carcinoids
• Biochemistry– Plasma chromogranin A– U-5’HIAA
• Radiology– CT– Ultrasonography + biopsy
• Octreoscan• PET• Echocardiography

Treatment of midgut carcinoids• Cytoreductive procedures
– Surgery: Primary tumour, lymph nodes, liver metastases– Radiofrequency ablation– Liver embolisation: Particles, SIRT
• Biotherapy: interferon-, somatostatin analogs• Surgery of carcinoid heart disease
• Progression– Liver embolisation: Particles, SIRT– 177Lu-octreotate, 90Y-octreotide– Experimental: RAD001, antiangiogenesis

Diagnosis of lung carcinoids• Biochemistry
– Plasma chromogranin A• Radiology
– CT• Octreoscan• Bronchoscopy + biopsy (Ki67, CD44)• PET

Treatment of lung carcinoids
Radical surgery• Primary tumour• Lymph node metastases• Frozen sections
Long-term follow-up, at least 10 years

Treatment of lung carcinoidsLow proliferative rate (Ki67<2–3%):• Biotherapy –interferon-, somatostatin analogs• Chemotherapy – temozolomide, STZ + 5-FU• 177Lu-octreotate, 90Y-octreotide
Intermediate proliferative rate (Ki67 5–10%):• Chemotherapy – temozolomide, STZ + dox• 177Lu-octreotate, 90Y-octreotide
High proliferative rate (Ki67 >15–20%):• cisplatin/carboplatin + etoposide • temozolomide + capecitabine/bevacizumab• taxanes + dox
Experimental: RAD001, tyrosine kinase/angiogenesis inhibitors

Diagnosis of EPT
• Biochemistry– Chromogranin A– PP, glucagon, insulin, proinsulin, gastrin, calcitonin, VIP– Sectetin test– 72-hour gasting– Meal stimulation test
• Radiology– CT– Ultrasonography– Endoscopic ultrasonography
• Octreoscan• PET

Treatment of EPTLow proliferative rate (Ki67<2–3%):• Chemotherapy – STZ + 5-FU• Biotherapy –interferon-, somatostatin analogs• 177Lu-octreotate, 90Y-octreotide
Intermediate proliferative rate (Ki67 5–10%):• Chemotherapy –, STZ + 5-FU/dox, temozolomide• 177Lu-octreotate, 90Y-octreotide
High proliferative rate (Ki67 >15–20%):• cisplatin/carboplatin + etoposide • taxanes + dox • temozolomide + capecitabine/bevacizumab
Experimental: RAD001, tyrosine kinase/angiogenesis inhibitors

Treatment of EPT• Cytoreductive procedures
– Surgery: Primary tumour, lymph nodes, liver metastases– Radiofrequency ablation– Liver embolisation: Particles, chemoembolisation, SIRT
• Symptomatic– Proton pump inhibitors– Somatostatin analogs– Interferon-– Ketoconazole– Metyrapone

Malignant neuroendocrine GEP-tumours
DiagnosisHistopathology,tumour biology, localisation and staging
Cytoreductive proceduresSurgery, RF
Low proliferating tumours (Ki-67 <3%)Biotherapy: SMS ± IFN
STZ + 5 FU (EPT)Tumour targeted therapy: 90Y, 177Lu
High proliferating tumours (Ki-67 5-10%)Cytotoxic therapy:
STZ + 5 FU/doxorubicin, TemozolomideTumour targeted therapy: 90Y, 177LuCisplatin + Etoposide (Ki-67 >20%)
Progression
Tumour targeted therapy: 90Y-DOTA-Octreotide, 177Lu-DOTA-OctreotateEmbolisation, chemoembolisation, SIRT
Experimental: RAD001, taxanes, tyrosine kinase/angiogenesis inhibitors

AcknowledgementsDept of Endocrine Oncology, Uppsala
• Barbro Eriksson
• Kjell Öberg
• Britt Skogseid
Dept of Nuclear Medicine, Uppsala
• Ulrike Garske
• Lars-Göran Andersson
Dept of Radiology, Uppsala
• Anders Sundin
• Rickard Nyman
SIRTEX Medical, Bonn
• Ralph Peters

