chemotherapy biotherapy & targeted therapies
TRANSCRIPT
1
ChemotherapyBiotherapy &Targeted Therapies
MiKaela Olsen RN, MS, OCN
Oncology and BMT Clinical Nurse Specialist
Objectives
State the dose limiting toxicity of chemotherapy
Describe the mechanism of action of 2Describe the mechanism of action of 2 different biotherapy drugs
State the theory behind targeted therapies
Why Use Chemotherapy?
Characteristics of malignant cells Uncontrolled growth
Decreased ability to repair DNA damage Decreased ability to repair DNA damage
Need for systemic treatment Metastatic tumors
Cancers that are systemic by nature
2
Goals of Chemotherapy
Cure = No evidence of disease: Normal life span
Control = Increase in survival and quality of life
Palliation = Increase in comfort
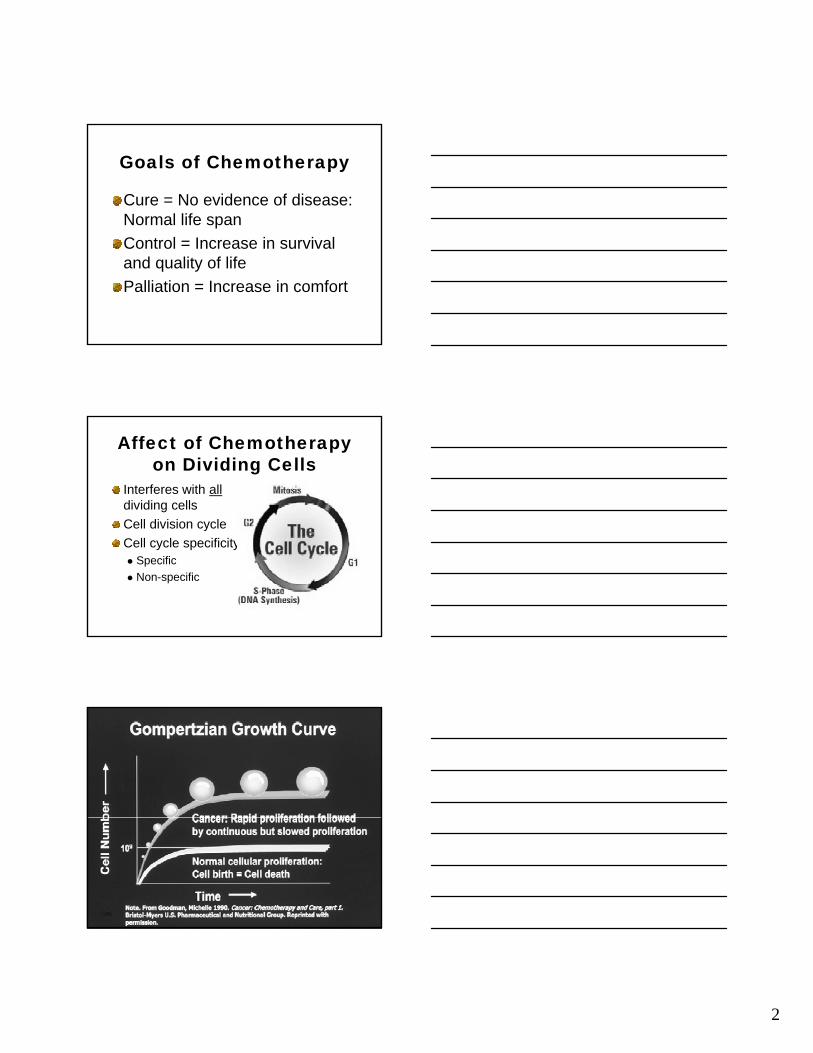
Affect of Chemotherapy on Dividing Cells
Interferes with alldividing cells
Cell division cycleCell division cycle
Cell cycle specificity Specific
Non-specific
3
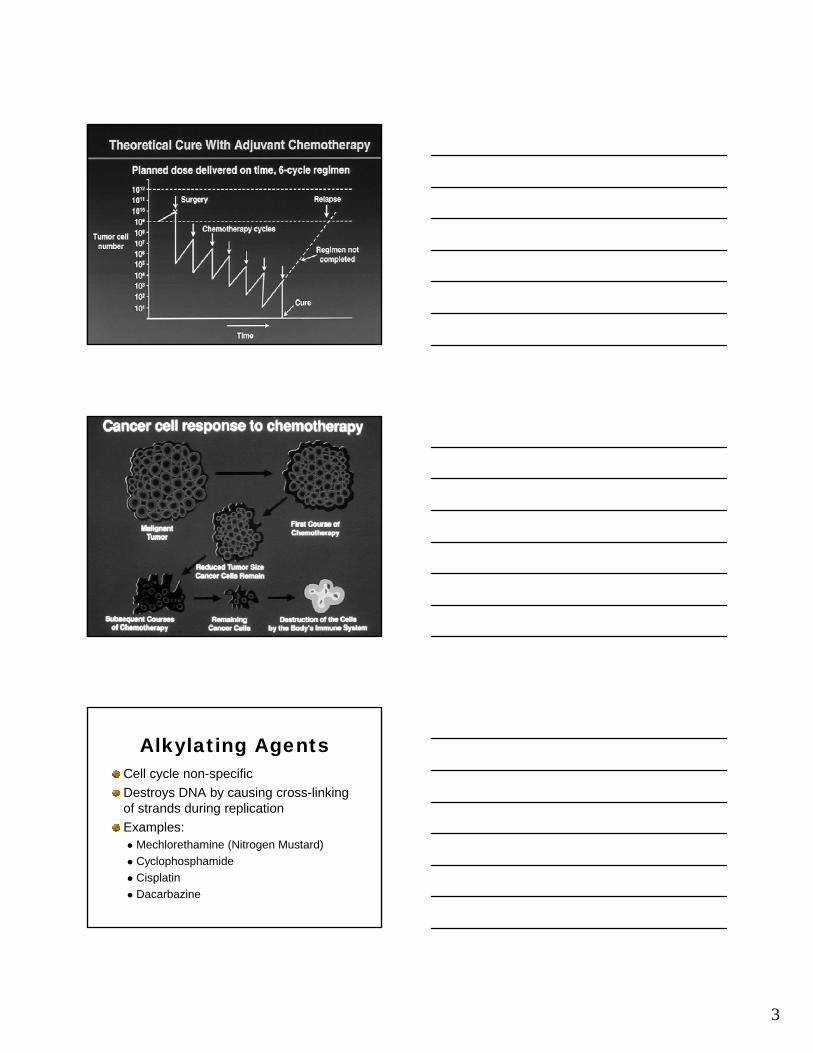
Alkylating AgentsCell cycle non-specific
Destroys DNA by causing cross-linking of strands during replication
Examples: Mechlorethamine (Nitrogen Mustard)
Cyclophosphamide
Cisplatin
Dacarbazine

4
Anti-tumor Antibiotics
Cell cycle non-specific
Interferes with DNA and RNA synthesis
Examples:Examples: Doxorubicin
Daunorubicin
Bleomycin
Mitomycin
Antimetabolites
Cell cycle specific (S phase)Block DNA synthesis by substituting for normal enzymes or other cellular ycomponentsExamples: Fluourouracil Methotrexate Cytarabine
Nitrosureas
Cell cycle non-specific
Cross the BBB
SterilitySterility
Second malignancies
Examples: BCNU, CCNU
5
Plant AlkaloidsCell cycle specific (M phase)
Block mitosis by interfering with the integrity of the mitotic apparatusintegrity of the mitotic apparatus
Examples: Vincristine
Etoposide
Paclitaxel
Hormones and Hormone Antagonists
Cell cycle non-specificInterfere with cellular division by altering the intracellular environmentExamples: Corticosteroids Megestrol acetate Tamoxifen Luprolide
Chemotherapy Side Effects

6
Chemotherapy Adverse Effects: Myelosuppression
Mechanism of OccurrencePotential problems Leukopenia: Infection Thrombocytopenia: Bleedingy p g Anemia: Fatigue
At risk populations Myelosuppressive chemotherapy regimens Previous/concurrent myelosuppressive therapies Hematologic malignancies Source of infection Cardiopulmonary compromise
ABSOLUTE NEUTROPHIL COUNT (ANC)
Polys + Bands X WBC = ANC100
Example: WBC = 4.5, Polys = 77, Bands = 3
77 + 3 X 4.5 = 10080% X 4.5 = 3600 normal count
7
ANC AND RISK OF INFECTION
1,000 - 1,500 Minimal Risk
500 - 1,000
< 500
Moderate Risk
Severe Risk
CLINICAL MANIFESTATION
Fever > 38oC (100.4o F)
Reliable & often only sign of infectionReliable & often only sign of infection
If extremely neutropenic, they may not be able to manifest the usual sign
Chemotherapy Adverse Effects: Nausea and Vomiting
Mechanism of occurrence
P ttPatterns Acute
Delayed
Anticipatory

8
Chemotherapy Adverse Effects: Nausea and Vomiting
Potential Problems Dehydration Inadequate nutritional intake
F ti Fatigue
At Risk Populations Emetogenic chemotherapy drugs History of nausea/vomiting Gastrointestinal/pelvic tumors Other medications (e.g. opioids, antibiotics)
Emetogenic Potential of Select Chemotherapy Drugs
HighestCisplatinDacarbazineMechlorethamineCyclophosphamideDoxorubicin/Daunorubicin
Lowest
Doxorubicin/DaunorubicinCytarabinePaclitaxelEtoposideMethotrexateBleomycinVincristineFluorouracilHormones

9
Chemotherapy Adverse Effects: Mucositis/Stomatitis
Mechanism of Occurrence
Potential Problems Pain
Decreased food and fluid intake
Increased risk for infection
At risk populations Causative agents
Intensive treatment regimens
History alcohol/tobacco use
Poor oral hygiene
Head and neck tumors
Chemotherapy Adverse Effects: Peripheral Neuropathies
Mechanism of occurrence
Potential problems Discomfort (pain hyperesthesias) Discomfort (pain, hyperesthesias)
Increased risk of injury
At risk populations Causative agents
History of alcoholism or diabetes
10
Chemotherapy Adverse Effects: Renal Toxicity
Mechanism of occurrencePotential problems Electrolyte wastingy g Decreased ability to clear
toxins/drugs
At risk populations Causative agents
(chemotherapy, antibiotics)
Dehydration Preexisting renal disease
Chemotherapy Adverse Effects: Cardiac Toxicity
Mechanism of OccurrencePotential problems
A ti it i t l Activity intolerance Congestive heart failure
At risk populations Causative agents Children and elderly Pre-existing heart disease
Chemotherapy Adverse Effects: Pulmonary Toxicity
Mechanism of occurrencePotential problems Shortness of breath/DOE Activity intolerancey Oxygen dependence
At risk populations Causative agents Concurrent radiation therapy Pre-existing lung disease
Primary or metastatic cancer History of smoking
11
Chemotherapy Adverse Effects: Fatigue
Mechanism of occurrence
Potential problems Activity tolerance
Decreased treatment tolerance
At risk populations Intensive treatment
regimens
Impaired activity tolerance prior to treatment
Chemotherapy Adverse Effects: Alopecia
Mechanism of occurrence
Potential Problems Alteration in self concept Alteration in self concept
At risk populations Causative agents
Intensive treatment regimens
Safe Handling of Hazardous Drugs
What is a hazardous drug? Any drug which poses a significant risk to
healthcare workers because of a potentialt t t i t ito cause teratogenic, mutagenic, carcinogenic or reproductive toxicity as well as other serious organ damage.
Includes antineoplastic agents, as well as some biologic, anti-viral and anti-infective agents.
12
Safe Handling of Hazardous Drugs
How might I be exposed to hazardous drugs? Healthcare workers can be exposed toHealthcare workers can be exposed to
hazardous drugs during preparation, transportation, administration, disposal of administration equipment, or disposal of body excreta from patients who have received hazardous drugs.
Decreasing Risk of Exposure to Hazardous Drugs
Wear protective gown and gloves when handling hazardous drugs or contaminated body fluids/excreta.Change gloves and wash hands before and after working withbefore and after working with hazardous drugs.Wear goggles or facial splash guard when there is risk of splashing of drug or body fluids.Avoid hand to mouth or eye contact while working with hazardous drugs or contaminated body fluids.
Chemotherapy Pretreatment AssessmentPatient knowledge of: Disease and treatment plan
Reason for using chemotherapy
Specific agents to be administered
Laboratory data Complete blood count with WBC differential
Liver function test
Renal function test
13
Chemotherapy Pretreatment AssessmentHistory and Physical Assessment Side effects of previous treatments
Signs/symptoms of infection
Nutritional status
Integrity of skin and mucosal barriers
Cardiopulmonary status
Energy level
Emotional response to disease and treatment
Social support
BiotherapyBiological therapy is the therapeutic use of agents derived from biologic sources and/or affecting biologic responses.
Also called “immunotherapy” and “biotherapy.”
Modifies the body’s biologic/immune response resulting in therapeutic effects.
Types
Interferons
InterleukinsInterleukins
Hematopoietic Growth Factors

14
Immune System ReviewComplex system of cells and creation of antibodies Retains memory of previous encounters with immunogens and mounts responses on new challenges Differentiates between “self” and “foreign”In many cancers, may not recognize the cancer as “foreign” and/or the immune system does not act against it Some biological therapies stimulate the immune system to attack cancer.
Hematopoietic Growth Factors
Hematopoietic Growth Factors (HGFs) – proteins that interact with specific receptors to regulate the production, maturation, and function of blood cells.maturation, and function of blood cells.
Usually used to ameliorate side effects of chemotherapy, although some are under investigation for anti-tumor properties.
15
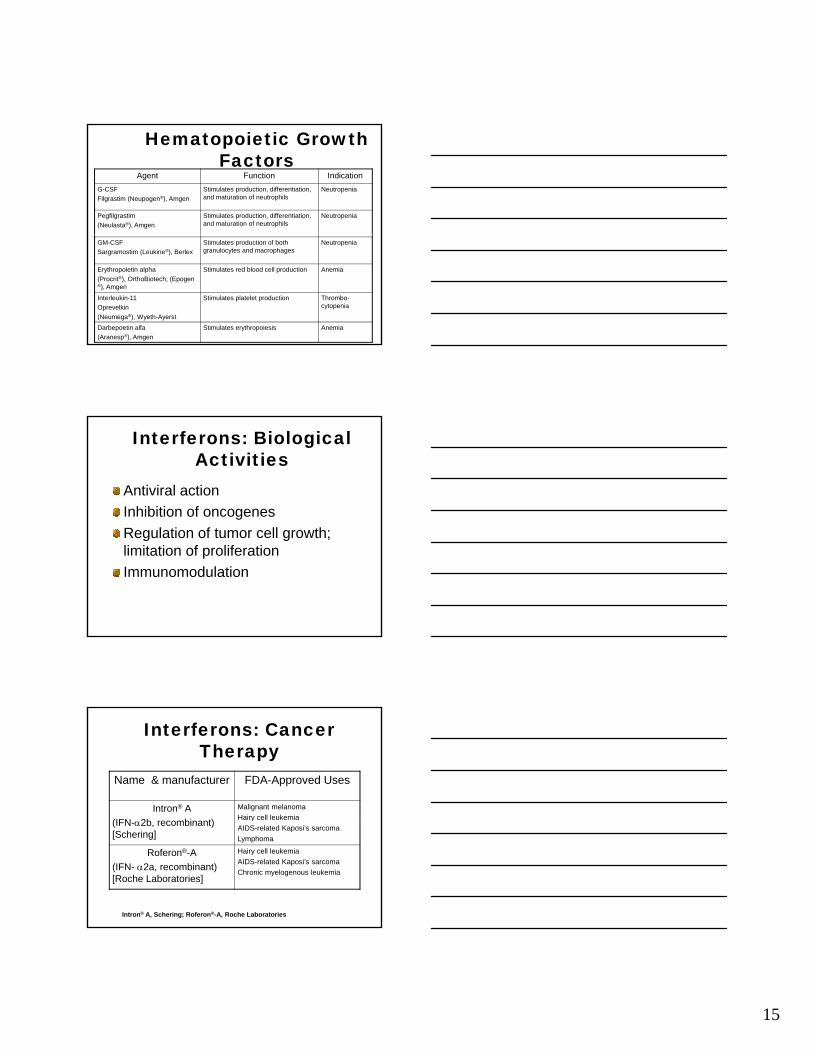
Hematopoietic Growth Factors
Agent Function Indication
G-CSF
Filgrastim (Neupogen®), Amgen
Stimulates production, differentiation, and maturation of neutrophils
Neutropenia
Pegfilgrastim
(Neulasta®), Amgen
Stimulates production, differentiation, and maturation of neutrophils
Neutropenia
GM-CSF
Sargramostim (Leukine®), Berlex
Stimulates production of both granulocytes and macrophages
Neutropenia
Erythropoietin alpha
(Procrit®), OrthoBiotech; (Epogen ®), Amgen
Stimulates red blood cell production Anemia
Interleukin-11
Oprevelkin
(Neumega®), Wyeth-Ayerst
Stimulates platelet production Thrombo-cytopenia
Darbepoetin alfa
(Aranesp®), Amgen
Stimulates erythropoiesis Anemia
Interferons: Biological Activities
Antiviral action
Inhibition of oncogenes
Regulation of tumor cell growth; limitation of proliferation
Immunomodulation
Interferons: Cancer Therapy
Name & manufacturer FDA-Approved Uses
Intron® A Malignant melanoma
Hairy cell leukemia(IFN-2b, recombinant) [Schering]
Hairy cell leukemia
AIDS-related Kaposi’s sarcoma
Lymphoma
Roferon®-A
(IFN- 2a, recombinant) [Roche Laboratories]
Hairy cell leukemia
AIDS-related Kaposi’s sarcoma
Chronic myelogenous leukemia
Intron® A, Schering; Roferon®-A, Roche Laboratories

16
Interleukins: Biological Activities
•Autocrine action (T helper cells)•Monocyte/macrophage activation•Promotion of cell division and release of mediators (T cells)•Activation and promotion of cell division (B cells)•Activation of Natural Killer (NK) cells
Interleukin-2: Indications/ Administration
Interleukin-2
[Aldeskeukin]
Proleukin® (Chiron)
Renal cell cancer
Metastatic melanoma Subcutaneous
Because of the possible severity of high-dose side effects, administration of high-dose therapy should take place in the hospital setting and not in out-patient clinics.
Standard regimen, Interleukin-2: 600,000 IU/kg (0.037 mg/kg) administered every 8 hours by a 15-minute IV infusion for a maximum of 14 doses. Following 9 days of rest, schedule is repeated for another 14 doses, for maximum of 28 doses per course, as tolerated. During clinical trials, doses were frequently withheld for toxicity.
Proleukin®, Chiron
Molecular Targeted Therapies
Tyrosine Kinase Inhibitors
Proteasome InhibitorsProteasome Inhibitors
Monoclonal antibodies (MoAbs)
17
Tyrosine Kinase Inhibitors (TKI)
Imatinib Mesylate (Gleevec®), Novartis
Gefitinib (Iressa®), AstraZeneca
TKIs are enzymes within the cell that block the ability y yof the protein tyrosine kinase to function, limiting cancerous cell growth.
Certain leukemias, as well as cancer of the breast, prostate, ovary, bladder, liver, and lung may be successfully treated with tyrosine kinase inhibitors.
Proteasome InhibitorsBlock activity of proteasomes, enzymes that help regulate cell function and growth
Proteasomes are involved in the cell cycle, growth of new blood vessels (angiogenesis), cellgrowth of new blood vessels (angiogenesis), cell adhesion, cytokine production, and apoptosis.
Blockade can lead to cell death in cancers.
Bortezomib (Velcade™)Indications and Dosing
Indicated for patients with Multiple Myeloma (MM) who have received 2 prior therapies and have shown disease progression since the last therapy
IV injection: 1.3 mg/m2 twice weekly for 2 weeks
Administered on days 1,4, 8, and 11, with a 10 day rest period before the next cycle.
Velcade™ (Millennium Pharmaceuticals, Inc.)

18
Monoclonal Antibodies
MoAbs are artificially produced in the laboratory and are designed to bind to the antigens expressed on the surface of malignant cells
Block the growth of the tumor and/or recruit theBlock the growth of the tumor and/or recruit the body’s immune system to attack the cancer cells
Can be given as a monotherapy, in combination with chemotherapy, and with other targeted therapies under clinical trial
Differences Between Chemotherapy and Monoclonal Antibody Therapy
Traditional Chemotherapy
Injury to cancer cells and normal cellsSid ff t /t i it
Monoclonal AntibodiesSpecifically target tumor cellsFewer side effects to
l llSide effects/toxicity can be cumulative and may lead to long term sequelae
Multi-drug resistance
normal cellsLess chance of drug resistance Fewer cumulative side effectsFew dose-limiting side effects
19
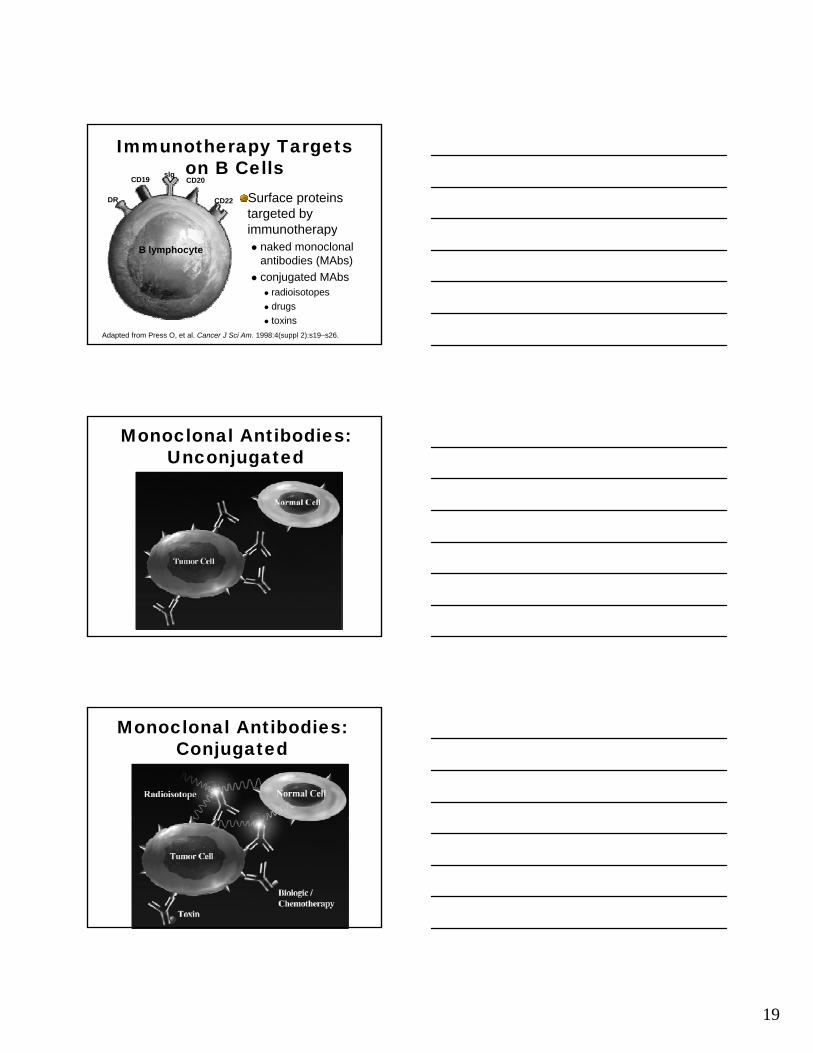
Immunotherapy Targets on B Cellsslg
DR
CD19 CD20
CD22 Surface proteins targeted by immunotherapy
B lymphocyte
py naked monoclonal
antibodies (MAbs)
conjugated MAbs radioisotopes
drugs
toxins
Adapted from Press O, et al. Cancer J Sci Am. 1998:4(suppl 2):s19–s26.
Monoclonal Antibodies: Unconjugated
Monoclonal Antibodies: Conjugated

20
Efficacy of Unlabeled Tositumomab Enhanced Through the Crossfire
Effect of Iodine-131
Unlabeled “cold” Antibody Radiolabeled Antibody
Courtesy of Andrew Zelenetz, MD.
MoAbs FDA-Approved for Cancer Therapy
Monoclonal Antibody Function Indication
Alemtuzumab
(Campath®), Berlex
Targets 21-28 kD cell surface glycoprotein, CD52
B-cell lymphocytic leukemia
Bevacizumab
(Avastin™) Genentech
Targets VEGF, prevents
Metastatic colorectal cancer, first line(Avastin ), Genentech prevents
angiogenesiscancer, first line
Cetuximab
(Erbitux™), Imclone/Bristol-Meyers Squibb
Targets EGFR receptor
Metastatic colorectal cancer, relapsed
Gemtuzumab ozogamicin (Mylotarg®), Wyeth-Ayerst
Targets the CD33 antigen; conjugated with calicheamicin (antibiotic)
Acute myeloid leukemia, relapsed
21
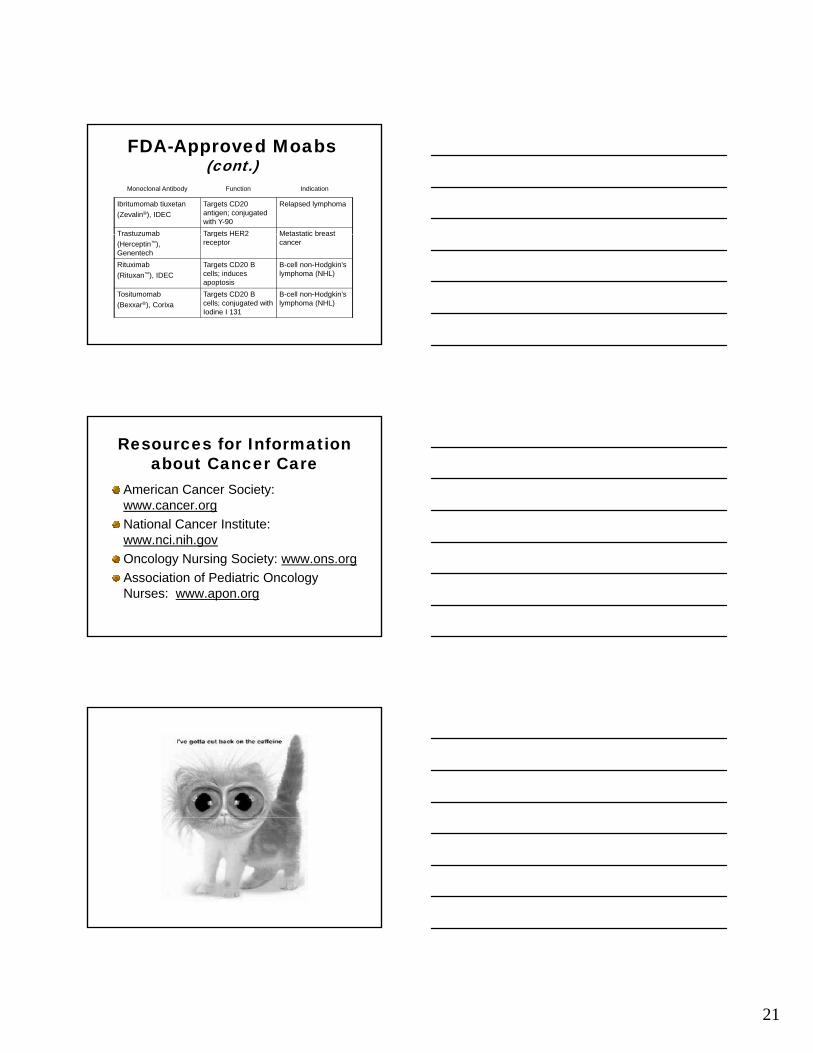
FDA-Approved Moabs (cont.)
Monoclonal Antibody Function Indication
Ibritumomab tiuxetan
(Zevalin®), IDEC
Targets CD20 antigen; conjugated with Y-90
Relapsed lymphoma
Trastuzumab Targets HER2 Metastatic breastTrastuzumab
(Herceptin™), Genentech
Targets HER2 receptor
Metastatic breast cancer
Rituximab
(Rituxan™), IDEC
Targets CD20 B cells; induces apoptosis
B-cell non-Hodgkin’s lymphoma (NHL)
Tositumomab
(Bexxar®), Corixa
Targets CD20 B cells; conjugated with Iodine I 131
B-cell non-Hodgkin’s lymphoma (NHL)
Resources for Information about Cancer Care
American Cancer Society: www.cancer.org
National Cancer Institute:National Cancer Institute: www.nci.nih.gov
Oncology Nursing Society: www.ons.org
Association of Pediatric Oncology Nurses: www.apon.org