bioethics sle in pregnancy san gabriel, saniano, sorreda
TRANSCRIPT

BIOETHICSSLE in Pregnancy
SAN GABRIEL, SANIANO, SORREDA

The patient is EG, a 21 year old female, who came in for chief complaint of seizures.
The patient is a diagnosed case of Systemic Lupus Erythematosus since December of 2008.
Patient Information

Initially presented with:malar rashphotosensitivityarthralgiahair loss and oral ulcersedema of both lower and upper extremities
weakness
Initial Presentation
ANA positive
Initially presented with:malar rashphotosensitivityarthralgiahair loss and oral ulcersedema of both lower and upper extremities
weakness
Systemic Lupus Erythematosus
ANA positive

Prednisone 10 mg once a dayHydrochloroquine 200 mg once a day
Medications
Regular Follow-upRheumatologyFamily Medicine

Pregnancy Uterine 14 1/7 weeks AOGG1P0
Systemic Lupus Erythematosus
Follow-upPGH Obstetrics High Risk ClinicLast Follow-up: February 17, 2010
2 WEEKS PTA(+) decreased appetite(+) gradually increasing generalized body weakness(-) interventions or consults
History of Present Illness

4 DAYS PTAgeneralized weakness now more prominent on both right upper and lower extremities(+) behavioral change (+) general decrease in activity (+) episodes of staring blankly into space(+) cough productive of whitish phlegm(+) febrile episodes (qualitative)(-) nasal congestion
History of Present Illness

2 HOURS PTA(-) rousability(+) seizure - upward rolling of the eyeballs, grinding of teeth and clenched fists (duration ~5 minutes)-> Promptly rushed to PGH, hence this admission
History of Present Illness

General(+) fever, (-) nausea and vomiting, (+) weakness, (+) weight loss
Integumentary(+) malar rash, (-) discoid rash,(-) hairloss
Eyes(–) blurring of vision
Ears(–) loss of hearing, tinnitus
Nervous(–) dysphagia, dysphonia, seizures, dizziness, (+) headache prior
Review of Systems

Respiratory(+) cough, (+) exertional dyspnea, (-) colds
Circulatory(–) chest pain, (-) bleeding
Digestive(-) melena, (-) constipation, (-) diarrhea, (-) abdominal pain
Urinary/ Reproductive System (-) urinary incontinence, (-) polyuria/nocturia, dysuria (-) dribbling, (-) tea colored urine, (+) vaginal spotting (Feb 14, 2010)
Review of Systems
(+) SLE, 2008 (-) HPN, DM, goiter, BA, PTB, CA (-) heart problems (-) allergy
Past Medical History

(-) SLE, HPN, DM, goiter, BA, Ca, heart problems
Family Medical HistoryPersonal and Social HistoryPt lives with live-in partner, a college graduate
(BA HRM), currently unemployed. Non-smoker, occasional alcoholic beverage drinker.(-) known exposure to chemicals, and radiation

G1P0 LMP: October 9, 2009 , PU 14 1/7 weeks AOG by late ultrasound
Obstetric History

Patient is awake, with regard, responds to name calling, inconsistently follows commands, with no verbal output
HR: 142 bpmBP: 100-110/60-70 mmHgRR: 40T: 38°C
Physical Examination

HEENT: (+) slight exophthalmos, anicteric sclerae, pink palpebral conjunctivae, (-) TPC, ANM, (-) NVE, (-) CLAD
Chest/Lungs: equal chest expansion, (+) bibasal and mid-field rhonchi, both lung fields ECE, (+) bibasal and mid-field rhonchi, both lung fields
CVS: adynamic precordium, distinct heart sounds, tachycardic, regular rhythm, (-) murmurs
Physical Examination
Abdomen: flat, normoactive bowel sounds, soft, (-) masses, (-) tenderness, liver edge not palpable
Genitourinary: deferred
Extremities: full and equal pulses, pink nailbeds, (-) edema/cyanosis, (+) blanching erythematous rash over extremities
Physical Examination

Pt is awake, with regard, responds to name calling, inconsistently follows commands, with no verbal output, uncooperative.
I – not assessed II – pupils 2/2 EBRTL, primary gaze midline, (-) preferential gaze III, IV, VI – (+) slight LR palsy, R; (+) visual threat, B V – brisk corneals VII – (-) facial assymetry VIII – gross hearing intact IX, X – good gag and swallow XII – refuses to protrude tongue
With spontaneous, purposeful movement of the extremities. Withdraws to pain, bilateral extremities (-) Babinski (-) clonus patient resists neck flexion. (-)dysmetria/dysdiadochokinesia (-) nystagmus Motor Strength: 3/5 on all extremities Sensory: WTP on all extremities
Neurologic Examination

CBC (2/28)
LaboratoriesWBC 14.1 HighHemoglobin 103 LowHematocrit 0.291 LowPlatelets 94 LowNeutrophils 0.764 ElevatedLymphocytes 0.197 NormalMonocytes 0.036 NormalEosinophils 0.002 NormalBasophils 0.001 Normal

Electrolytes (2/28)
LaboratoriesGlucose 5.83 NormalCreatinine 72 NormalSodium 134 LowPotassium 3.5 LowChloride 100 Normal

ABG (2/28)
LaboratoriesFiO2 60TemperatureHemoglobin 103pH 7.429PCO2 26.4PO2 63.5HCO3 17.9TCO2Base ExcessO2 saturation 92.9
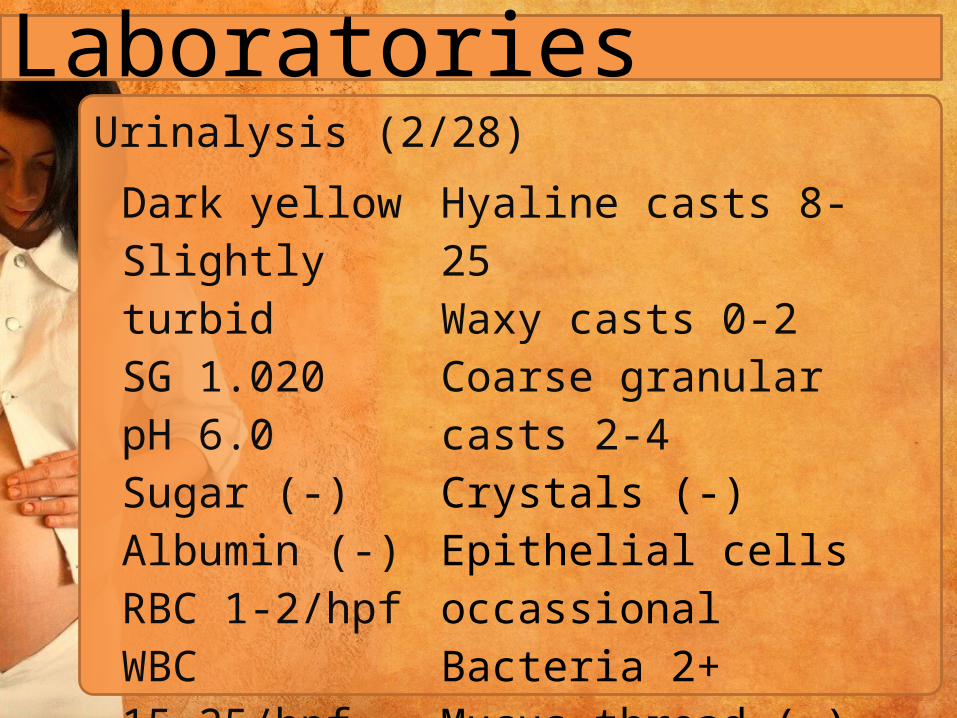
Urinalysis (2/28)
Laboratories
Dark yellowSlightly turbidSG 1.020pH 6.0Sugar (-)Albumin (-)RBC 1-2/hpfWBC 15-25/hpf
Hyaline casts 8-25Waxy casts 0-2Coarse granular casts 2-4Crystals (-)Epithelial cells occassionalBacteria 2+Mucus thread (-)
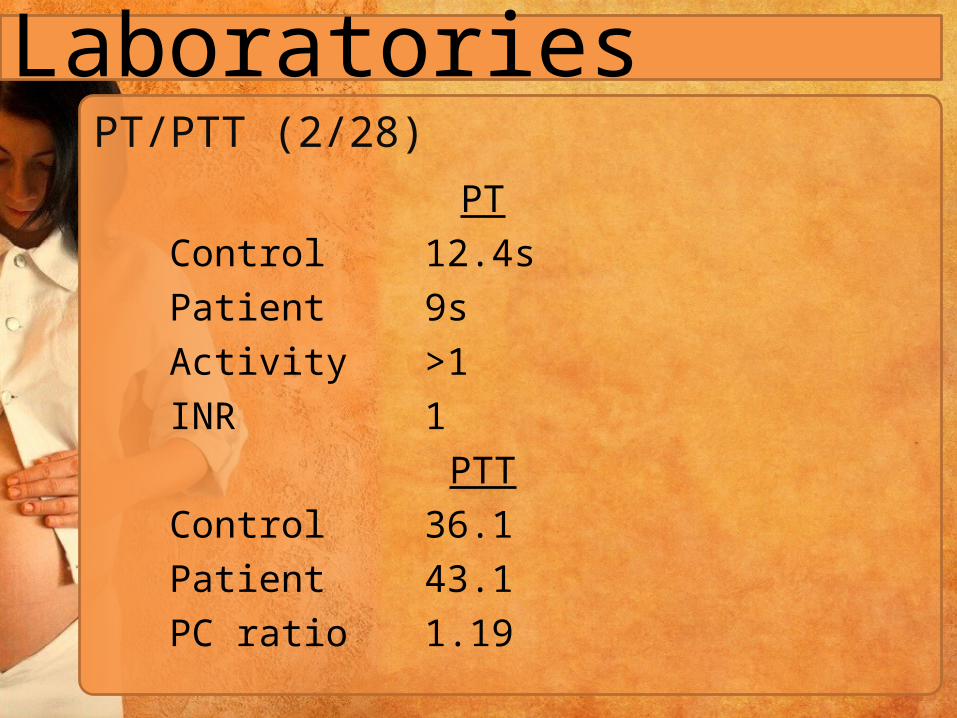
PT/PTT (2/28)
LaboratoriesPT
Control 12.4sPatient 9sActivity >1INR 1
PTTControl 36.1Patient 43.1PC ratio 1.19

ECG2/28: sinus tachycardia, normal axis, low voltage complexes 3/11: sinus tachycardia, normal axis, low voltage complexes 3/12: sinus tachycardia, normal axis, low voltage complexes
2D Echoconcentric LVH with good wall motion and contractility, EF=73% minimal pericardial effusion, mild pulmo HPN, incidental finding of pleural effusion, mild TR, PR.
Cranial CT Scan Normal findings
Laboratories

Systemic lupus erythematosus in activity t/c SLE cerebritis, myocarditis t/c sec APAS Community Acquired Pneumonia r/o SOL vs electrolyte imbalance vs CNS infection as cause of seizureAnemia of chronic diseaseComplicated UTI
Working Impression

content
Title
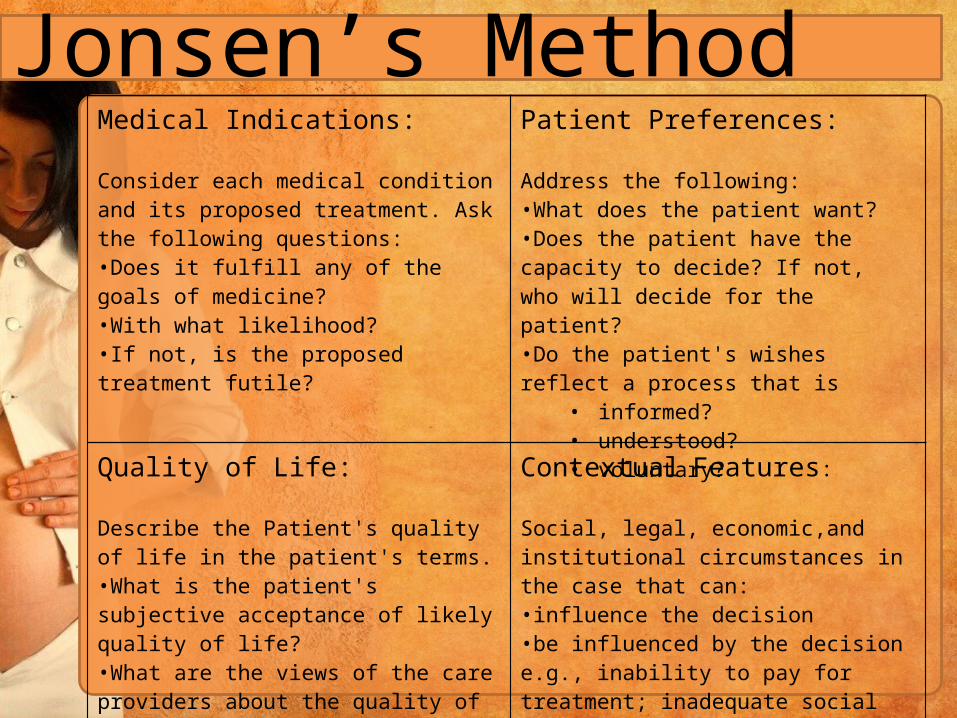
Jonsen’s MethodMedical Indications:
Consider each medical condition and its proposed treatment. Ask the following questions: •Does it fulfill any of the goals of medicine? •With what likelihood? •If not, is the proposed treatment futile?
Patient Preferences:
Address the following: •What does the patient want? •Does the patient have the capacity to decide? If not, who will decide for the patient? •Do the patient's wishes reflect a process that is
• informed? • understood? • voluntary?
Quality of Life:
Describe the Patient's quality of life in the patient's terms. •What is the patient's subjective acceptance of likely quality of life? •What are the views of the care providers about the quality of life? •Is quality of life "less than minimal?" (i.e., qualitative futility)
Contextual Features:
Social, legal, economic,and institutional circumstances in the case that can: •influence the decision •be influenced by the decision e.g., inability to pay for treatment; inadequate social support