benefit information guide - vbgov.com...office hours: mon. – fri. 8 a.m. to 6 p.m. after business...
TRANSCRIPT

v9.2018
Benefit Information Guide
POS PlansA D M I N I S T E R E D B Y S E N TA R A H E A LT H P L A N S , I N C .

Visit www.optimahealth.com/members to:
If you are considering Optima Health or are new to the plan and do not have a member ID card, please call us toll-free at 1-877-552-7401.
• View a list of Plan providers• Change your Plan primary care physician (PCP)• Update your home address, phone number, or email address• Order a new member ID card or print member ID card• View your claims history• View your benefits• View your authorizations• Download member forms
• Learn about member discounts• Manage your pharmacy benefit (if administered by Optima Health)• Research drug options and pricing• Choose to receive your Explanation of Benefits (EOB) electronically• Research conditions, treatment options, and hospital quality
Optima Health Member Services4417 Corporation LaneVirginia Beach, VA 23462
[email protected] note: Members who register and sign in to optimahealth.com can contact Member Services securely using the Contact Us form.
Member Services
Call the number listed on the back of your member ID card.Office hours: Mon. – Fri. 8 a.m. to 6 p.m.After business hours, please leave a message.
After Hours Nurse Advice Line
Call the number listed on the back of your member ID card.
Behavioral Health Services
1-800-648-8420
Language services for non-English speaking
members
Call 1-855-687-6260 for assistance in languages other than English.
TYY/TDD line for the hearing impaired
Optima Health uses the Virginia Relay Service 1-800-828-1140 or 711
Optima Health Mobile App
On the Go? Download the Optima Health Mobile App to your smartphone or tablet and access your member ID card, benefits, claims, and more, anywhere, anytime, anyplace.
Optima Health Individual & Family Plans
Customer Service (for current members)1-866-514-5916
For new sales inquiries and quotes:
Phone: 1-800-741-4825Website: optimahealth.com/individual
You will need to register on optimahealth.com/members in order to access your secure member information, as well as special tools available only to Optima Health members.

Section 1: Uniform Summary of Benefits and Coverage (SBC) ……………………………………2
Section 2: Welcome to Optima Health…………………………………………………………………23
Section 3: Summary of Benefits (SOB) ……………………………………………………………….48POS PremierPOS StandardPOS Basic
Section 4: Pharmacy Benefits ………………………………………………………………………...97Savings with GenericsOptumRx Home Delivery FAQsOptumRx Mailorder FormProprium Pharmacy FAQs
Section 5: Mental/Behavioral Health/Substance Use Disorder Services …………………………107
Section 6: Other Health Insurance Information ……………………………...................................109HSA Plan FAQsVision Care and Materials RiderVision Discount Fee ScheduleDiabetes TreatmentHearing Aid RiderChiropractic Care RiderComplementary Alternative Medicine Discount ProgramGym Network 360 Discount Program
Section 7: Additional Items …………………………………………………………………………….122MDLIVE FlyerOptions for Care FlyerSentara Quality Care Network FlyerPreventive Services Covered Under Health Care ReformTreatment Cost Calculator FlyerMyLife MyPlan FlyersEPIC Hearing FlyersProgeny Health Flyer
Section 8: BEWell Flyers…………………………………………………………………….………….150Cardiovascular Disease Management ProgramDiabetes Management ProgramRespiratory Disease Management ProgramPartners in Pregnancy ProgramAccordantCareTM Program
Group Name:
City of VA Beach and VA Beach City Public Schools
Effective Date:
01/01/2019
Table of Contents

Un
ifo
rm
Su
mm
ary o
f B
en
efi
ts a
nd
Co
verag
e (
SB
C)
2

Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 POS Premier Coverage for: Individual/Family | Plan Type: POSVA Beach Schools/City
1 of 6
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan wouldshare the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately.
This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, visit optimahealth.com or call 1-866-509-7567. For general definitions of common terms, such as allowed amount, balance billing, coinsurance, copayment, deductible, provider, or other underlined terms see the Glossary. You can view the Glossary at healthcare.gov/sbc-glossary or call 1-866-509-7567 to request a copy.Important Questions Answers Why This Matters:
What is the overall deductible?
$850/Individual or $1,700/familyin-network. $1,700/Individual or $3,400/family out-of-network
Generally, you must pay all of the costs from providers up to the deductible amount before this plan begins to pay. If you have other family members on the plan, each family member must meet their own individual deductible until the total amount of deductible expenses paid by all family members meets the overall family deductible.
Are there services covered before you meet your deductible?
Yes. Preventive care, Vision Careand Materials are covered before you meet your deductible.
This plan covers some items and services even if you haven’t yet met the deductible amount. But a copayment or coinsurance may apply. For example, this plan covers certain preventive serviceswithout cost-sharing and before you meet your deductible. See a list of covered preventive services at https://www.healthcare.gov/coverage/preventive-care-benefits/.
Are there otherdeductibles for specific services?
No. You don’t have to meet deductibles for specific services.
What is the out-of-pocket limit for this plan?
For in-network providers $3,000individual / $6,000 family. For out-of-network providers, $4,500individual / $9,000 family
The out-of-pocket limit is the most you could pay in a year for covered services. If you have other family members in this plan, they have to meet their own out-of-pocket limits until the overall family out-of-pocket limit has been met.
What is not included inthe out-of-pocket limit?
Premiums, balance-billed charges, healthcare this plan doesn’t cover, ancillary drug charges and pre-authorization penalties.
Even though you pay these expenses, they don’t count toward the out–of–pocket limit.
Will you pay less if you use a network provider?
Yes. See optimahealth.com or call 1-866-509-7567 for a list of network providers.
This plan uses a provider network. You will pay less if you use a provider in the plan’s network.You will pay the most if you use an out-of-network provider, and you might receive a bill from a provider for the difference between the provider’s charge and what your plan pays (balance billing). Be aware, your network provider might use an out-of-network provider for some services (such as lab work). Check with your provider before you get services.
Do you need a referral to see a specialist? No. You can see the specialist you choose without a referral.
3

2 of 6 * For more information about limitations and exceptions, see the plan or policy document at optimahealth.com.
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common Medical Event Services You May Need
What You Will PayLimitations, Exceptions, & Other Important
InformationIn-Network Provider(You will pay the least)
Out-of-Network Provider
(You will pay the most)
If you visit a health care provider’s office or clinic
Primary care visit to treat an injury or illness
$20 copayment/SQCNDeductible does not apply$40 copayment/all otherDeductible does not apply
40% coinsurance --none--
Specialist visit$40 copayment/SQCNDeductible does not apply$60 copayment/all otherDeductible does not apply
40% coinsurance --none--
Preventive care/screening/ immunization
No chargeDeductible does not apply 40% coinsurance
You may have to pay for services that aren't preventive. Ask your provider if the services you need are preventive. Then check what your plan will pay for.
If you have a test
Diagnostic test (x-ray, blood work) 15% coinsurance 40% coinsurance --none--
Imaging (CT/PET scans, MRIs) 15% coinsurance 40% coinsurance Benefits may be denied or reduced without pre-authorization
If you need drugs to treat your illness or conditionMore information about prescription drug coverage is available at www.optimahealth.com
Selected Generic drugs (Tier 1)$10 copayment/preferred network/$25 copayment retail /$25 copayment mail order
$10 copayment/preferred network/$25 copayment retail / mail order not covered
Coverage is limited to maximum $150 ancillary cap per prescription per month in addition to applicable Copayment/Coinsurance. Coverage is limited to FDA-approved prescription drugs. If brand drugs are used when a generic is available, you must pay the difference in cost plus the Copayment or Coinsurance amount. Covers up to a 31-day supply (retail); up to a 90-day supply for 3 copayments (Preferred Pharmacies only); 31- to 90-day supply (mail order). Not all drugs are available through a mail order program.
Selected brand and other generic drugs (Tier 2)
$25 copayment/preferred network/$45 copayment retail /$60 copayment mail order
$25 copayment/preferred network/$45 copayment retail / mail order not covered
Non-selected brand drugs(Tier 3)
25% Coinsurance: $50 max preferred network/$75 max retail/$125 max mail order
25% Coinsurance: $50 max preferred network/$75 max retail/mail order not covered
Specialty drugs (Tier 4) 25% coinsurance retail 25% coinsurance retail
4

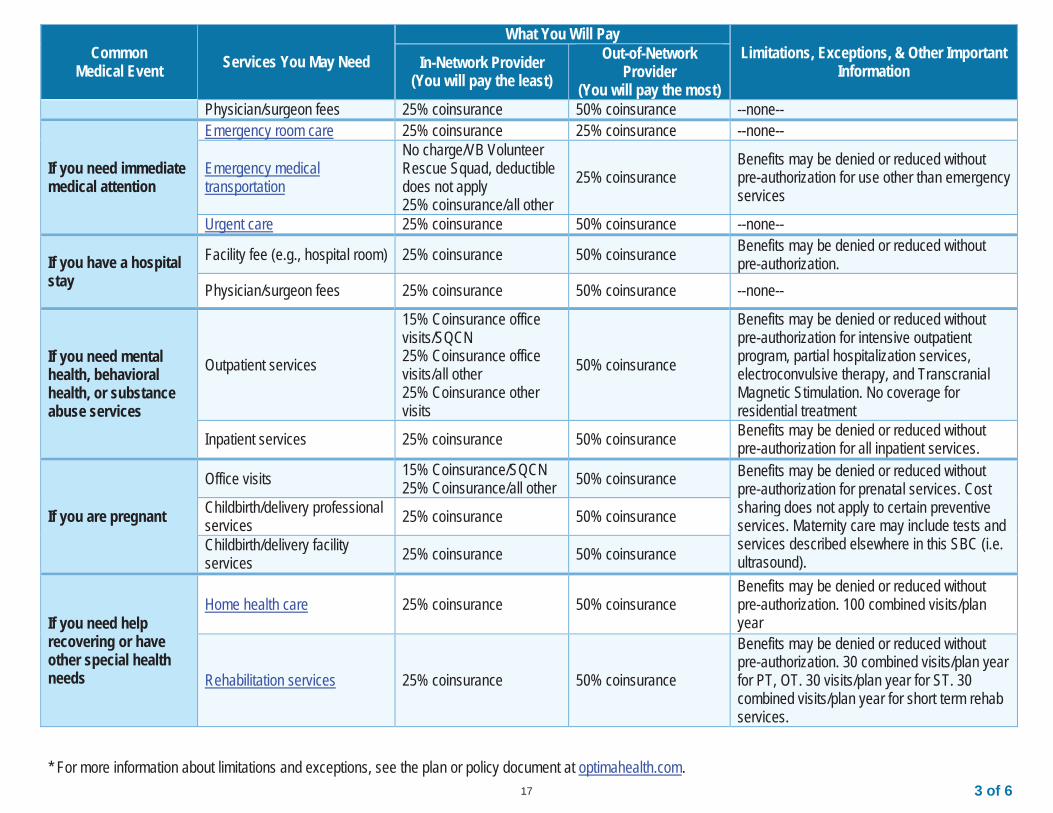
3 of 6 * For more information about limitations and exceptions, see the plan or policy document at optimahealth.com.
Common Medical Event Services You May Need
What You Will PayLimitations, Exceptions, & Other Important
InformationIn-Network Provider(You will pay the least)
Out-of-Network Provider
(You will pay the most) $200 max/ mail order not covered
$200 max/ mail order not covered
If you have outpatient surgery
Facility fee (e.g., ambulatory surgery center) 15% coinsurance 40% coinsurance Benefits may be denied or reduced without
pre-authorizationPhysician/surgeon fees 15% coinsurance 40% coinsurance --none--
If you need immediate medical attention
Emergency room care 15% coinsurance 15% coinsurance --none--
Emergency medical transportation
No charge/VB Volunteer Rescue Squad, deductible does not apply15% coinsurance/all other
15% coinsuranceBenefits may be denied or reduced without pre-authorization for use other than emergency services
Urgent care 15% coinsurance 40% coinsurance --none--
If you have a hospital stay
Facility fee (e.g., hospital room) 15% coinsurance 40% coinsurance Benefits may be denied or reduced without pre-authorization.
Physician/surgeon fees 15% coinsurance 40% coinsurance --none--
If you need mental health, behavioral health, or substance abuse services
Outpatient services
$20 copayment office visits/SQCNDeductible does not apply$40 copayment office visits/all otherDeductible does not apply15% coinsurance other visits
40% coinsurance
Benefits may be denied or reduced without pre-authorization for intensive outpatient program, partial hospitalization services, electroconvulsive therapy, and Transcranial Magnetic Stimulation. No coverage for residential treatment
Inpatient services 15% coinsurance 40% coinsurance Benefits may be denied or reduced without pre-authorization for all inpatient services.
If you are pregnant
Office visits$350 global copayment/SQCN$500 global copayment/all other
40% coinsurance Benefits may be denied or reduced without pre-authorization for prenatal services. Cost sharing does not apply to certain preventive services. Maternity care may include tests and services described elsewhere in this SBC (i.e. ultrasound).
Childbirth/delivery professional services 15% coinsurance 40% coinsurance
Childbirth/delivery facility services 15% coinsurance 40% coinsurance
5

4 of 6 * For more information about limitations and exceptions, see the plan or policy document at optimahealth.com.
Common Medical Event Services You May Need
What You Will PayLimitations, Exceptions, & Other Important
InformationIn-Network Provider(You will pay the least)
Out-of-Network Provider
(You will pay the most)
If you need help recovering or have other special health needs
Home health care 15% coinsurance 40% coinsuranceBenefits may be denied or reduced without pre-authorization. 100 combined visits/plan year
Rehabilitation services 15% coinsurance 40% coinsurance
Benefits may be denied or reduced without pre-authorization. 30 combined visits/plan year for PT, OT. 30 visits/plan year for ST. 30combined visits/plan year for short term rehabservices.
Habilitation services Not covered Not covered --none--
Skilled nursing care 15% coinsurance 40% coinsuranceBenefits may be denied or reduced without pre-authorization. 100 combined days/plan year
Durable medical equipment 15% coinsurance 40% coinsuranceBenefits may be denied or reduced without pre-authorization for single items over $750, all rental items, and repair and replacement.
Hospice services 15% coinsurance 40% coinsurance Benefits may be denied or reduced without pre-authorization.
If your child needs dental or eye care
Children’s eye exam$20 copayment/spectacles$40 copayment/contact lensesDeductible does not apply
$40 reimbursementDeductible does not apply
Coverage limited to one exam/plan year from participating EyeMed providers
Children’s glassesAllowances: $100/spectacles$95/contact lensesDeductible does not apply
Not covered Coverage limited to one pair/plan year from participating EyeMed providers
Children’s dental check-up Not covered Not covered --none--
Excluded Services & Other Covered Services:Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
AcupunctureBariatric surgeryCosmetic surgeryDental care (Adult)
Habilitation servicesInfertility treatmentLong-term carePediatric dental check-up
Private-duty nursingRoutine foot careWeight loss programs
6

5 of 6 * For more information about limitations and exceptions, see the plan or policy document at optimahealth.com.
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)Chiropractic careHearing aids
Non-emergency care when traveling outside theU.S. (under out-of-network benefit) Routine eye care (Adult)
Your Rights to Continue Coverage: For more information on your rights to continue coverage, contact the plan at 1-866-509-7567. There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is: Virginia State Corporation Commission, Life & Health Division, Bureau of Insurance, at 1-877-310-6560 or [email protected]; the U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa/healthreform; or the U.S. Department of Health and Human Services at 1-877-267-2323 x61565 or www.cciio.cms.gov. Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For more information about the Marketplace,visit www.HealthCare.gov or call 1-800-318-2596.
Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact: Member Services at the number on the back of your member ID card. You may also contact the Department of Labor's Employee Benefits Security Administration at 1-866-444-EBSA (3272) or www.dol.gov/ebsa/healthreform; or your state department of insurance at the Virginia State Corporation Commission, Life & Health Division, Bureau of Insurance, P.O. Box 1157, Richmond, VA, 23218, 1-877-310-6560 or [email protected].
Additionally, a consumer assistance program can help you file your appeal. Contact the Virginia State Corporation Commission, Life & Health Division, Bureau of Insurance, P.O. Box 1157, Richmond, VA, 23218, 1-877-310-6560, or [email protected].
Does this plan provide Minimum Essential Coverage? YesIf you don’t have Minimum Essential Coverage for a month, you’ll have to make a payment when you file your tax return unless you qualify for an exemption from the requirement that you have health coverage for that month.
Does this plan meet the Minimum Value Standards? YesIf your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next section.––––––––––––––––––––––
7

6 of 6 The plan would be responsible for the other costs of these EXAMPLE covered services.
Peg is Having a Baby(9 months of in-network pre-natal care and a
hospital delivery)
Mia’s Simple Fracture(in-network emergency room visit and follow
up care)
Managing Joe’s type 2 Diabetes(a year of routine in-network care of a well-
controlled condition)
The plan’s overall deductible $850Specialist copayment $350Hospital (facility) coinsurance 15%Other coinsurance 15%
This EXAMPLE event includes services like: Specialist office visits (prenatal care)Childbirth/Delivery Professional ServicesChildbirth/Delivery Facility ServicesDiagnostic tests (ultrasounds and blood work)Specialist visit (anesthesia)
Total Example Cost $12,800
In this example, Peg would pay:Cost Sharing
Deductibles $850Copayments $430Coinsurance $1,500
What isn’t coveredLimits or exclusions $0The total Peg would pay is $2,780
The plan’s overall deductible $850Specialist copayment $40Hospital (facility) coinsurance 15%Other coinsurance 15%
This EXAMPLE event includes services like: Primary care physician office visits (including disease education)Diagnostic tests (blood work)Prescription drugs Durable medical equipment (glucose meter)
Total Example Cost $7,400
In this example, Joe would pay:Cost Sharing
Deductibles $850Copayments $875Coinsurance $120
What isn’t coveredLimits or exclusions $55The total Joe would pay is $1,900
The plan’s overall deductible $850Specialist copayment $40Hospital (facility) coinsurance 15%Other coinsurance 15%
This EXAMPLE event includes services like: Emergency room care (including medical supplies)Diagnostic test (x-ray)Durable medical equipment (crutches)Rehabilitation services (physical therapy)
Total Example Cost $1,900
In this example, Mia would pay: Cost Sharing
Deductibles $850Copayments $120Coinsurance $160
What isn’t coveredLimits or exclusions $0The total Mia would pay is $1,130
About these Coverage Examples:
This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost sharingamounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.
Note: These numbers assume the patient does not participate in the plan’s wellness program. If you participate in the plan’s wellness program, you may be able to reduce your costs. For more information about the wellness program, please contact: 1-877-817-3037.
8

Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 POS Standard Coverage for: Individual/Family | Plan Type: POSVA Beach Schools/City
1 of 6
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan wouldshare the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately.
This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, visit optimahealth.com or call 1-866-509-7567. For general definitions of common terms, such as allowed amount, balance billing, coinsurance, copayment, deductible, provider, or other underlined terms see the Glossary. You can view the Glossary at healthcare.gov/sbc-glossary or call 1-866-509-7567 to request a copy.Important Questions Answers Why This Matters:
What is the overall deductible?
$1,350/Individual or $2,700/familyin-network. $2,600/Individual or $5,200/family out-of-network
Generally, you must pay all of the costs from providers up to the deductible amount before this plan begins to pay. If you have other family members on the policy, the overall family deductiblehas to be met before the plan begins to pay.
Are there services covered before you meet your deductible?
Yes. Preventive care, Vision Careand Materials are covered before you meet your deductible.
This plan covers some items and services even if you haven’t yet met the deductible amount. But a copayment or coinsurance may apply. For example, this plan covers certain preventive serviceswithout cost-sharing and before you meet your deductible. See a list of covered preventive services at https://www.healthcare.gov/coverage/preventive-care-benefits/.
Are there otherdeductibles for specific services?
No. You don’t have to meet deductibles for specific services.
What is the out-of-pocket limit for this plan?
For in-network providers $3,500individual / $7,000 family. For out-of-network providers, $5,500individual / $11,000 family
The out-of-pocket limit is the most you could pay in a year for covered services. If you have other family members in this plan, they have to meet their own out-of-pocket limits until the overall family out-of-pocket limit has been met.
What is not included inthe out-of-pocket limit?
Premiums, balance-billed charges, healthcare this plan doesn’t cover, ancillary drug charges and pre-authorization penalties.
Even though you pay these expenses, they don’t count toward the out–of–pocket limit.
Will you pay less if you use a network provider?
Yes. See optimahealth.com or call 1-866-509-7567 for a list of network providers.
This plan uses a provider network. You will pay less if you use a provider in the plan’s network.You will pay the most if you use an out-of-network provider, and you might receive a bill from a provider for the difference between the provider’s charge and what your plan pays (balance billing). Be aware, your network provider might use an out-of-network provider for some services (such as lab work). Check with your provider before you get services.
Do you need a referral to see a specialist? No. You can see the specialist you choose without a referral.
9

2 of 6 * For more information about limitations and exceptions, see the plan or policy document at optimahealth.com.
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common Medical Event Services You May Need
What You Will PayLimitations, Exceptions, & Other Important
InformationIn-Network Provider(You will pay the least)
Out-of-Network Provider
(You will pay the most)
If you visit a health care provider’s office or clinic
Primary care visit to treat an injury or illness
10% Coinsurance/SQCN20% Coinsurance/all other 50% coinsurance --none--
Specialist visit 10% Coinsurance/SQCN20% Coinsurance/all other 50% coinsurance --none--
Preventive care/screening/ immunization
No chargeDeductible does not apply 50% coinsurance
You may have to pay for services that aren't preventive. Ask your provider if the services you need are preventive. Then check what your plan will pay for.
If you have a test
Diagnostic test (x-ray, blood work) 20% coinsurance 50% coinsurance --none--
Imaging (CT/PET scans, MRIs) 20% coinsurance 50% coinsurance Benefits may be denied or reduced without pre-authorization
If you need drugs to treat your illness or conditionMore information about prescription drug coverage is available at www.optimahealth.com
Selected Generic drugs (Tier 1)$10 copayment/preferred network/$25 copayment retail /$25 copayment mail order
$10 copayment/preferred network/$25 copayment retail / mail order notcovered
Medical deductible applies. Coverage is limited to maximum $150 ancillary cap per prescription per month in addition to applicable Copayment/Coinsurance. Coverage is limited to FDA-approved prescription drugs. If brand drugs are used when a generic is available, you must pay the difference in cost plus the Copayment or Coinsurance amount. Covers up to a 31-day supply (retail); up to a 90-day supply for 3 copayments (Preferred Pharmacies only); 31- to 90-day supply (mail order). Not all drugs are available through a mail order program.
Selected brand and other generic drugs (Tier 2)
$25 copayment/preferred network/$45 copayment retail /$60 copayment mail order
$25 copayment/preferred network/$45 copayment retail / mail order not covered
Non-selected brand drugs(Tier 3)
25% Coinsurance: $50 max preferred network/$75 max retail/$125 max mail order
25% Coinsurance: $50 max preferred network/$75 max retail/mail order not covered
Specialty drugs (Tier 4)25% coinsurance retail$200 max/ mail order not covered
25% coinsurance retail$200 max/ mail order not covered
If you have outpatient surgery
Facility fee (e.g., ambulatory surgery center) 20% coinsurance 50% coinsurance Benefits may be denied or reduced without
pre-authorizationPhysician/surgeon fees 20% coinsurance 50% coinsurance --none--
10

3 of 6 * For more information about limitations and exceptions, see the plan or policy document at optimahealth.com.
Common Medical Event Services You May Need
What You Will PayLimitations, Exceptions, & Other Important
InformationIn-Network Provider(You will pay the least)
Out-of-Network Provider
(You will pay the most)
If you need immediate medical attention
Emergency room care 20% coinsurance 20% coinsurance --none--
Emergency medical transportation
No charge/VB Volunteer Rescue Squad, deductibledoes not apply20% coinsurance/all other
20% coinsuranceBenefits may be denied or reduced without pre-authorization for use other than emergency services
Urgent care 20% coinsurance 50% coinsurance --none--
If you have a hospital stay
Facility fee (e.g., hospital room) 20% coinsurance 50% coinsurance Benefits may be denied or reduced without pre-authorization.
Physician/surgeon fees 20% coinsurance 50% coinsurance --none--
If you need mental health, behavioral health, or substance abuse services
Outpatient services
10% Coinsurance office visits/SQCN20% Coinsurance office visits/all other 20% Coinsurance other visits
50% coinsurance
Benefits may be denied or reduced withoutpre-authorization for intensive outpatient program, partial hospitalization services, electroconvulsive therapy, and Transcranial Magnetic Stimulation. No coverage for residential treatment
Inpatient services 20% coinsurance 50% coinsurance Benefits may be denied or reduced without pre-authorization for all inpatient services.
If you are pregnant
Office visits 10% Coinsurance/SQCN20% Coinsurance/all other 50% coinsurance Benefits may be denied or reduced without
pre-authorization for prenatal services. Cost sharing does not apply to certain preventive services. Maternity care may include tests and services described elsewhere in this SBC (i.e. ultrasound).
Childbirth/delivery professional services 20% coinsurance 50% coinsurance
Childbirth/delivery facility services 20% coinsurance 50% coinsurance
If you need help recovering or have other special health needs
Home health care 20% coinsurance 50% coinsuranceBenefits may be denied or reduced without pre-authorization. 100 combined visits/plan year
Rehabilitation services 20% coinsurance 50% coinsurance
Benefits may be denied or reduced without pre-authorization. 30 combined visits/plan year for PT, OT. 30 visits/plan year for ST. 30combined visits/plan year for short term rehab services.
Habilitation services Not covered Not covered --none--
11

4 of 6 * For more information about limitations and exceptions, see the plan or policy document at optimahealth.com.
Common Medical Event Services You May Need
What You Will PayLimitations, Exceptions, & Other Important
InformationIn-Network Provider(You will pay the least)
Out-of-Network Provider
(You will pay the most)
Skilled nursing care 20% coinsurance 50% coinsuranceBenefits may be denied or reduced without pre-authorization. 100 combined days/plan year
Durable medical equipment 20% coinsurance 50% coinsuranceBenefits may be denied or reduced without pre-authorization for single items over $750, all rental items, and repair and replacement.
Hospice services 20% coinsurance 50% coinsurance Benefits may be denied or reduced without pre-authorization.
If your child needs dental or eye care
Children’s eye exam$20 copayment/spectacles$40 copayment/contact lensesDeductible does not apply
$40 reimbursementDeductible does not apply
Coverage limited to one exam/plan year from participating EyeMed providers
Children’s glasses Allowances: $100/spectacles$95/contact lensesDeductible does not apply
Not covered Coverage limited to one pair/plan year from participating EyeMed providers
Children’s dental check-up Not covered Not covered --none--
Excluded Services & Other Covered Services:Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
AcupunctureBariatric surgeryCosmetic surgeryDental care (Adult)
Habilitation servicesInfertility treatmentLong-term carePediatric dental check-up
Private-duty nursingRoutine foot careWeight loss programs
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)Chiropractic careHearing aids
Non-emergency care when traveling outside theU.S. (under out-of-network benefit) Routine eye care (Adult)
12

5 of 6 * For more information about limitations and exceptions, see the plan or policy document at optimahealth.com.
Your Rights to Continue Coverage: For more information on your rights to continue coverage, contact the plan at 1-866-509-7567. There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is: Virginia State Corporation Commission, Life & Health Division, Bureau of Insurance, at 1-877-310-6560 or [email protected]; the U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa/healthreform; or the U.S. Department of Health and Human Services at 1-877-267-2323 x61565 or www.cciio.cms.gov. Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For more information about the Marketplace,visit www.HealthCare.gov or call 1-800-318-2596.
Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact: Member Services at the number on the back of your member ID card. You may also contact the Department of Labor's Employee Benefits Security Administration at 1-866-444-EBSA (3272) or www.dol.gov/ebsa/healthreform; or your state department of insurance at the Virginia State Corporation Commission, Life & Health Division, Bureau of Insurance, P.O. Box 1157, Richmond, VA, 23218, 1-877-310-6560 or [email protected].
Additionally, a consumer assistance program can help you file your appeal. Contact the Virginia State Corporation Commission, Life & Health Division, Bureau of Insurance, P.O. Box 1157, Richmond, VA, 23218, 1-877-310-6560, or [email protected].
Does this plan provide Minimum Essential Coverage? YesIf you don’t have Minimum Essential Coverage for a month, you’ll have to make a payment when you file your tax return unless you qualify for an exemption from the requirement that you have health coverage for that month.
Does this plan meet the Minimum Value Standards? YesIf your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next section.––––––––––––––––––––––
13

6 of 6 The plan would be responsible for the other costs of these EXAMPLE covered services.
Peg is Having a Baby(9 months of in-network pre-natal care and a
hospital delivery)
Mia’s Simple Fracture(in-network emergency room visit and follow
up care)
Managing Joe’s type 2 Diabetes(a year of routine in-network care of a well-
controlled condition)
The plan’s overall deductible $1350Specialist coinsurance 10%Hospital (facility) coinsurance 20%Other coinsurance 20%
This EXAMPLE event includes services like: Specialist office visits (prenatal care)Childbirth/Delivery Professional ServicesChildbirth/Delivery Facility ServicesDiagnostic tests (ultrasounds and blood work)Specialist visit (anesthesia)
Total Example Cost $12,800
In this example, Peg would pay:Cost Sharing
Deductibles $1,350Copayments $40Coinsurance $2,110
What isn’t coveredLimits or exclusions $0The total Peg would pay is $3,500
The plan’s overall deductible $1350Specialist coinsurance 10%Hospital (facility) coinsurance 20%Other coinsurance 20%
This EXAMPLE event includes services like: Primary care physician office visits (including disease education)Diagnostic tests (blood work)Prescription drugs Durable medical equipment (glucose meter)
Total Example Cost $7,400
In this example, Joe would pay:Cost Sharing
Deductibles $1,350Copayments $635Coinsurance $135
What isn’t coveredLimits or exclusions $55The total Joe would pay is $2,175
The plan’s overall deductible $1350Specialist coinsurance 10%Hospital (facility) coinsurance 20%Other coinsurance 20%
This EXAMPLE event includes services like: Emergency room care (including medical supplies)Diagnostic test (x-ray)Durable medical equipment (crutches)Rehabilitation services (physical therapy)
Total Example Cost $1,900
In this example, Mia would pay: Cost Sharing
Deductibles $1,095Copayments $0Coinsurance $240
What isn’t coveredLimits or exclusions $0The total Mia would pay is $1,335
About these Coverage Examples:
This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost sharingamounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.
Note: These numbers assume the patient does not participate in the plan’s wellness program. If you participate in the plan’s wellness program, you may be able to reduce your costs. For more information about the wellness program, please contact: 1-877-817-3037.
14

Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2019-12/31/2019 POS Basic Coverage for: Individual/Family | Plan Type: POSVA Beach Schools/City
1 of 6
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan wouldshare the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately.
This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, visit optimahealth.com or call 1-866-509-7567. For general definitions of common terms, such as allowed amount, balance billing, coinsurance, copayment, deductible, provider, or other underlined terms see the Glossary. You can view the Glossary at healthcare.gov/sbc-glossary or call 1-866-509-7567 to request a copy.Important Questions Answers Why This Matters:
What is the overall deductible?
$2,000/Individual or $4,000/familyin-network. $4,000/Individual or $8,000/family out-of-network
Generally, you must pay all of the costs from providers up to the deductible amount before this plan begins to pay. If you have other family members on the policy, the overall family deductiblehas to be met before the plan begins to pay.
Are there services covered before you meet your deductible?
Yes. Preventive care, Vision Care and Materials are covered before you meet your deductible.
This plan covers some items and services even if you haven’t yet met the deductible amount. But a copayment or coinsurance may apply. For example, this plan covers certain preventive serviceswithout cost-sharing and before you meet your deductible. See a list of covered preventive services at https://www.healthcare.gov/coverage/preventive-care-benefits/.
Are there otherdeductibles for specific services?
No. You don’t have to meet deductibles for specific services.
What is the out-of-pocket limit for this plan?
For in-network providers $4,000individual / $8,000 family (not to exceed $7,900 for one individual).For out-of-network providers,$6,500 individual / $13,000 family
The out-of-pocket limit is the most you could pay in a year for covered services. If you have other family members in this plan, they have to meet their own out-of-pocket limits until the overall family out-of-pocket limit has been met.
What is not included inthe out-of-pocket limit?
Premiums, balance-billed charges, healthcare this plan doesn’t cover, ancillary drug charges and pre-authorization penalties.
Even though you pay these expenses, they don’t count toward the out–of–pocket limit.
Will you pay less if you use a network provider?
Yes. See optimahealth.com or call 1-866-509-7567 for a list of network providers.
This plan uses a provider network. You will pay less if you use a provider in the plan’s network.You will pay the most if you use an out-of-network provider, and you might receive a bill from a provider for the difference between the provider’s charge and what your plan pays (balance billing). Be aware, your network provider might use an out-of-network provider for some services (such as lab work). Check with your provider before you get services.
Do you need a referral to see a specialist? No. You can see the specialist you choose without a referral.
15

2 of 6 * For more information about limitations and exceptions, see the plan or policy document at optimahealth.com.
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common Medical Event Services You May Need
What You Will PayLimitations, Exceptions, & Other Important
InformationIn-Network Provider(You will pay the least)
Out-of-Network Provider
(You will pay the most)
If you visit a health care provider’s office or clinic
Primary care visit to treat an injury or illness
15% Coinsurance/SQCN25% Coinsurance/all other 50% coinsurance --none--
Specialist visit 15% Coinsurance/SQCN25% Coinsurance/all other 50% coinsurance --none--
Preventive care/screening/ immunization
No chargeDeductible does not apply 50% coinsurance
You may have to pay for services that aren't preventive. Ask your provider if the services you need are preventive. Then check what your plan will pay for.
If you have a test
Diagnostic test (x-ray, blood work) 25% coinsurance 50% coinsurance --none--
Imaging (CT/PET scans, MRIs) 25% coinsurance 50% coinsurance Benefits may be denied or reduced without pre-authorization
If you need drugs to treat your illness or conditionMore information about prescription drug coverage is available at www.optimahealth.com
Selected Generic drugs (Tier 1)$10 copayment/preferred network/$25 copayment retail /$25 copayment mail order
$10 copayment/preferred network/$25 copayment retail / mail order not covered
Medical deductible applies. Coverage is limited to maximum $150 ancillary cap per prescription per month in addition to applicable Copayment/Coinsurance. Coverage is limited to FDA-approved prescription drugs. If brand drugs are used when a generic is available, you must pay the difference in cost plus the Copayment or Coinsurance amount. Covers up to a 31-day supply (retail); up to a 90-day supply for 3 copayments (Preferred Pharmacies only); 31- to 90-day supply (mail order). Not all drugs are available through a mail order program.
Selected brand and other generic drugs (Tier 2)
$25 copayment/preferred network/$45 copayment retail /$60 copayment mail order
$25 copayment/preferred network/$45 copayment retail / mail order not covered
Non-selected brand drugs(Tier 3)
25% Coinsurance: $50 max preferred network/$75 max retail/$125 max mail order
25% Coinsurance: $50 max preferred network/$75 max retail/mail order not covered
Specialty drugs (Tier 4)25% coinsurance retail$200 max/ mail order not covered
25% coinsurance retail$200 max/ mail order not covered
If you have outpatient surgery
Facility fee (e.g., ambulatory surgery center) 25% coinsurance 50% coinsurance Benefits may be denied or reduced without
pre-authorization
16
3 of 6 * For more information about limitations and exceptions, see the plan or policy document at optimahealth.com.
Common Medical Event Services You May Need
What You Will PayLimitations, Exceptions, & Other Important
InformationIn-Network Provider(You will pay the least)
Out-of-Network Provider
(You will pay the most) Physician/surgeon fees 25% coinsurance 50% coinsurance --none--
If you need immediate medical attention
Emergency room care 25% coinsurance 25% coinsurance --none--
Emergency medical transportation
No charge/VB Volunteer Rescue Squad, deductible does not apply25% coinsurance/all other
25% coinsuranceBenefits may be denied or reduced without pre-authorization for use other than emergency services
Urgent care 25% coinsurance 50% coinsurance --none--
If you have a hospital stay
Facility fee (e.g., hospital room) 25% coinsurance 50% coinsurance Benefits may be denied or reduced without pre-authorization.
Physician/surgeon fees 25% coinsurance 50% coinsurance --none--
If you need mental health, behavioral health, or substance abuse services
Outpatient services
15% Coinsurance office visits/SQCN25% Coinsurance office visits/all other 25% Coinsurance other visits
50% coinsurance
Benefits may be denied or reduced without pre-authorization for intensive outpatient program, partial hospitalization services, electroconvulsive therapy, and Transcranial Magnetic Stimulation. No coverage for residential treatment
Inpatient services 25% coinsurance 50% coinsurance Benefits may be denied or reduced without pre-authorization for all inpatient services.
If you are pregnant
Office visits 15% Coinsurance/SQCN25% Coinsurance/all other 50% coinsurance Benefits may be denied or reduced without
pre-authorization for prenatal services. Cost sharing does not apply to certain preventive services. Maternity care may include tests and services described elsewhere in this SBC (i.e. ultrasound).
Childbirth/delivery professional services 25% coinsurance 50% coinsurance
Childbirth/delivery facility services 25% coinsurance 50% coinsurance
If you need help recovering or have other special health needs
Home health care 25% coinsurance 50% coinsuranceBenefits may be denied or reduced without pre-authorization. 100 combined visits/plan year
Rehabilitation services 25% coinsurance 50% coinsurance
Benefits may be denied or reduced without pre-authorization. 30 combined visits/plan year for PT, OT. 30 visits/plan year for ST. 30combined visits/plan year for short term rehab services.
17

4 of 6 * For more information about limitations and exceptions, see the plan or policy document at optimahealth.com.
Common Medical Event Services You May Need
What You Will PayLimitations, Exceptions, & Other Important
InformationIn-Network Provider(You will pay the least)
Out-of-Network Provider
(You will pay the most) Habilitation services Not covered Not covered --none--
Skilled nursing care 25% coinsurance 50% coinsuranceBenefits may be denied or reduced without pre-authorization. 100 combined days/plan year
Durable medical equipment 25% coinsurance 50% coinsuranceBenefits may be denied or reduced without pre-authorization for single items over $750, all rental items, and repair and replacement.
Hospice services 25% coinsurance 50% coinsurance Benefits may be denied or reduced withoutpre-authorization.
If your child needs dental or eye care
Children’s eye exam$20 copayment/spectacles$40 copayment/contact lensesDeductible does not apply
$40 reimbursementDeductible does not apply
Coverage limited to one exam/plan year from participating EyeMed providers
Children’s glassesAllowances: $100/spectacles$95/contact lensesDeductible does not apply
Not covered Coverage limited to one pair/plan year from participating EyeMed providers
Children’s dental check-up Not covered Not covered --none--
Excluded Services & Other Covered Services:Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
AcupunctureBariatric surgeryCosmetic surgeryDental care (Adult)
Habilitation servicesInfertility treatmentLong-term carePediatric dental check-up
Private-duty nursingRoutine foot careWeight loss programs
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)Chiropractic careHearing aids
Non-emergency care when traveling outside theU.S. (under out-of-network benefit) Routine eye care (Adult)
Your Rights to Continue Coverage: For more information on your rights to continue coverage, contact the plan at 1-866-509-7567. There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is: Virginia State Corporation Commission, Life & Health Division, Bureau of Insurance, at 1-877-310-6560 or [email protected]; the U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or
18

5 of 6 * For more information about limitations and exceptions, see the plan or policy document at optimahealth.com.
www.dol.gov/ebsa/healthreform; or the U.S. Department of Health and Human Services at 1-877-267-2323 x61565 or www.cciio.cms.gov. Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For more information about the Marketplace,visit www.HealthCare.gov or call 1-800-318-2596.
Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact: Member Services at the number on the back of your member ID card. You may also contact the Department of Labor's Employee Benefits Security Administration at 1-866-444-EBSA (3272) or www.dol.gov/ebsa/healthreform; or your state department of insurance at the Virginia State Corporation Commission, Life & Health Division, Bureau of Insurance, P.O. Box 1157, Richmond, VA, 23218, 1-877-310-6560 or [email protected].
Additionally, a consumer assistance program can help you file your appeal. Contact the Virginia State Corporation Commission, Life & Health Division, Bureau of Insurance, P.O. Box 1157, Richmond, VA, 23218, 1-877-310-6560, or [email protected].
Does this plan provide Minimum Essential Coverage? YesIf you don’t have Minimum Essential Coverage for a month, you’ll have to make a payment when you file your tax return unless you qualify for an exemption from the requirement that you have health coverage for that month.
Does this plan meet the Minimum Value Standards? YesIf your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next section.––––––––––––––––––––––
19

6 of 6 The plan would be responsible for the other costs of these EXAMPLE covered services.
Peg is Having a Baby(9 months of in-network pre-natal care and a
hospital delivery)
Mia’s Simple Fracture(in-network emergency room visit and follow
up care)
Managing Joe’s type 2 Diabetes(a year of routine in-network care of a well-
controlled condition)
The plan’s overall deductible $2000Specialist coinsurance 15%Hospital (facility) coinsurance 25%Other coinsurance 25%
This EXAMPLE event includes services like: Specialist office visits (prenatal care)Childbirth/Delivery Professional ServicesChildbirth/Delivery Facility ServicesDiagnostic tests (ultrasounds and blood work)Specialist visit (anesthesia)
Total Example Cost $12,800
In this example, Peg would pay:Cost Sharing
Deductibles $2,000Copayments $40Coinsurance $1,960
What isn’t coveredLimits or exclusions $0The total Peg would pay is $4,000
The plan’s overall deductible $2000Specialist coinsurance 15%Hospital (facility) coinsurance 25%Other coinsurance 25%
This EXAMPLE event includes services like: Primary care physician office visits (including disease education)Diagnostic tests (blood work)Prescription drugs Durable medical equipment (glucose meter)
Total Example Cost $7,400
In this example, Joe would pay:Cost Sharing
Deductibles $2,000Copayments $635Coinsurance $195
What isn’t coveredLimits or exclusions $55The total Joe would pay is $2,885
The plan’s overall deductible $2000Specialist coinsurance 15%Hospital (facility) coinsurance 25%Other coinsurance 25%
This EXAMPLE event includes services like: Emergency room care (including medical supplies)Diagnostic test (x-ray)Durable medical equipment (crutches)Rehabilitation services (physical therapy)
Total Example Cost $1,900
In this example, Mia would pay: Cost Sharing
Deductibles $1,030Copayments $0Coinsurance $310
What isn’t coveredLimits or exclusions $0The total Mia would pay is $1,340
About these Coverage Examples:
This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost sharingamounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.
Note: These numbers assume the patient does not participate in the plan’s wellness program. If you participate in the plan’s wellness program, you may be able to reduce your costs. For more information about the wellness program, please contact: 1-877-817-3037.
20

Optima Health Alternative Language Options for Notices and other Written Information English: ATTENTION: If you speak English, language assistance services, free of charge, are available to you. Call 1-855-687-6260.
Amharic:
1-855-687-6260 Arabic:
6260-687-855-1
Bengali/Bangla:
, - 1-855-687-6260 Chinese (Mandarin):
1-855-687-6260 French: ATTENTION : Si vous parlez français, les services d'assistance linguistique sont à votre disposition sans aucun frais. Appelez le 1-855-687-6260. German: ACHTUNG: Wenn Sie deutsch sprechen, stehen Ihnen Sprachhilfsdienste kostenlos unter der Rufnummer 1-855-687-6260 zur Verfügung. Gujarati:
: . 1-855-687-6260 . Hindi:
: , : 1-855-687-6260
Hmong: CIM CIA: Yog tias koj hais lus Hmoob, kev pab cuam txais lus tau muaj rau koj ua tsis them nqi. Hu rau 1-855-687-6260. Igbo: GEE NT : b r na na-as Igbo, ga-enweta enyemaka n’efu site n’aka nd ga-enyere gi aka inweta ya. Kp 1-855-687-6260 Japanese:
1-855-687-6260
Korean:
: , . 1-855-687-6260.
21
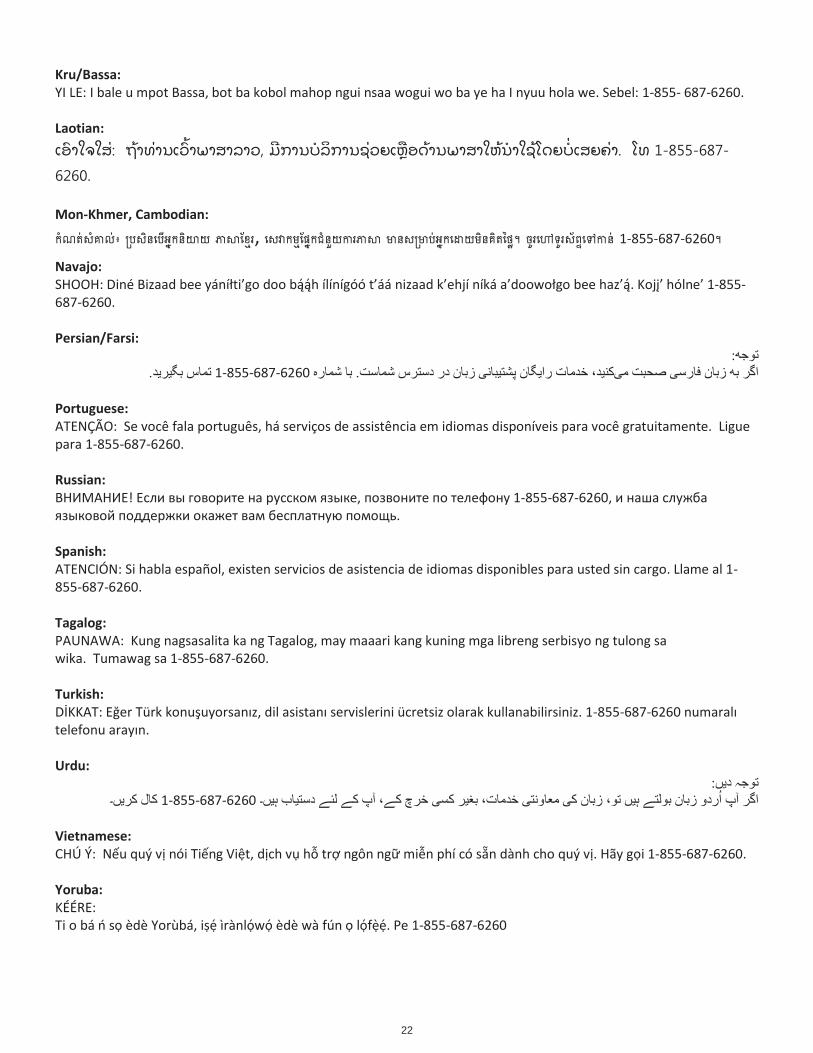
Kru/Bassa: YI LE: I bale u mpot Bassa, bot ba kobol mahop ngui nsaa wogui wo ba ye ha I nyuu hola we. Sebel: 1-855- 687-6260. Laotian:
Mon-Khmer, Cambodian:
, 1-855-687-6260
Navajo: -855-
687-6260. Persian/Farsi:
1-855-687-6260
Portuguese: ATENÇÃO: Se você fala português, há serviços de assistência em idiomas disponíveis para você gratuitamente. Ligue para 1-855-687-6260. Russian:
! , 1-855-687-6260
Spanish: ATENCIÓN: Si habla español, existen servicios de asistencia de idiomas disponibles para usted sin cargo. Llame al 1-855-687-6260. Tagalog: PAUNAWA: Kung nagsasalita ka ng Tagalog, may maaari kang kuning mga libreng serbisyo ng tulong sa wika. Tumawag sa 1-855-687-6260. Turkish:
-855-687-
Urdu:
1-855-687-6260
Vietnamese: CHÚ Ý: N u quý v ng Vi t, d ch v h tr ngôn ng mi n dành cho quý v . Hãy g i 1-855-687-6260. Yoruba: KÉÉRE:
èdè Yorùbá, i ìrànl w èdè wà fún l f . Pe 1-855-687-6260
22

Welc
om
e t
o O
pti
ma H
ealt
h
23

�
Welcome to Optima Health
Our Plans This Benefit Information Guide outlines basic information and answers to common questions about the POS health plan. Remember, specific infor such as copay, coinsurance and applicable deductibles is referenced in your specific plan benefit, a benefit structure that is chosen by your employer. Refer to your employer plan-specific document located in this book for more details.
POS Pla Optima POS is a plan in which you
In-network/ PHCS network: The in-network benefit option means you can lower your out-of-pocket costs by seeing primary care physician, specialist, therapist and other health-care professionals who have met all of Optima Health's credentialing require-ments, and are part of the network.
Out-of-network: If you choose to use your out-of-network benefit option for covered services, it means you and your family members can select doctor or medical facility you want , regardless of whether or not they are providers.
.Provider Network Optima Health members can receive care from any provider they choose; however, coverage will depend upon the plan you have and the participation status of the doctor you choose to see. It is important to understand your plan and your plan's network in order to ensure your care is covered by Optima Health.
Participating Providers Doctors, hospitals and other healthcare professionals who sign an agreement with Optima Health are participating, or in-network, providers. These providers have agreed to accept a set fee for services rendered to our health plan members.
Non-participating Providers Doctors, hospitals and other healthcare professionals who do not have a signed agreement with Optima Health are considered non-participating, or out-of-net- work, providers. These providers can charge whatever they want for their ser- vices. Typically, when plan members who have out-of-network benefits receive covered services from these out-of-network providers, we will pay a set percent- age of the amount we pay in-network providers for the same service. The mem- ber will pay the rest. If what the out-of-network providers charge is more than what Optima Health pays, they can bill you, the member, for the difference between the two amounts.
This Benefit
Information Guide
answers frequently
asked questions
about primary care
physicians (PCPs),
referrals,
emergencies, urgent
care, and more.
24

Member ID Cards
You may receive a new member ID card when you enroll or renew in a plan. You can request one online or from Member Services, or view and/or print it from our website. The following abbreviations might help you read your card.
Member ID Card Abbreviations: Coins: Coinsurance OV: SOV: Specialist Copayment or Coinsurance UCC: Urgent Care Center Copayment or Coinsurance ED: Emergency Department Copayment or Coinsurance DX1: Radiological and diagnostic tests performed outside the physician’s office, excluding lab work DX2: Outpatient Advanced Imaging and Testing Procedures performed in a physician’s Examples: MRI, MRA, PET Scans, CT Scans, CTA Scans, Sleep Studies OP: Outpatient Copayment or Coinsurance IP: Inpatient Copayment or Coinsurance RxDed: Prescription Drug Deductible Rx: Applicable Prescription Drug Copayment according to drug Tier
Note: Your card is designed according to the plan you have elected and may not contain all of the codes mentioned above.
Your member ID card identifies you as a covered member of Optima Health and provides information about your Plan.
Office Visit (Primary Care Physician) Copayment or Coinsurance
office, a freestanding outpatient facility, or a hospital outpatient facility.
25

What is a plan primary care physician and why do I need one?Your plan primary care physician (PCP) is your point of contact to coordinate your healthcare needs. They can pro ide oth the rst contact for an undia nosed health concern as ell as continuin care of aried medical conditions. ependin on your PCP for routine medical care and uidance hen see in care ithin the ptima
ealth net or can increase your satisfaction ith the plan and ith your care. You ill e as ed to select an in net or or plan PCP for yourself and each of your eli i le dependents hen you enroll.
How do I choose or change a plan PCP?hen you enroll in an ptima ealth Plan you ill e as ed to choose a PCP for yourself and each of your
dependents. e mem ers can often continue relationships ith their present doctor or select a doctor ith an of ce more con enient to their home or or addresses. You ha e the ri ht to choose any PCP ho participates in our net or and ho is a aila le to accept you and or your dependents. or children you may choose a participatin pediatrician as their PCP.You can re ie a list of participatin pro iders for your plan online at optimahealth.com mem ers. You can choose or chan e your PCP online y si nin in selectin Chan e Primary Care Physician from the y ptima menu and follo in the on screen instructions. n most cases your PCP selection ill e effecti e the ne t business day.Please note you do not need prior authori ation from ptima ealth or from any other person includin your PCP to access obstetrical or ynecolo ical or other specialty care from a healthcare professional in our net or . The healthcare professional may be re uired to comply ith certain procedures includin obtainin prior authori ation for certain ser ices follo in a pre appro ed treatment plan or other Plan re uirements.f you ha e not seen your desi nated PCP ithin the last months please contact your PCP s of ce or ember er ices to ensure that the of ce still lists you as a patient. a in your correct PCP on le ensures that any
correspondence or other outreach to your PCP is accurate.
What about my spouse and children? Do we all have the same PCP?dult members ha e the ri ht to choose a eneral family practice or an internal medicine doctor as their PCP
and a family practice doctor or a pediatrician for their children.
How do new federal health reform changes affect my access to PCPs and OB/GYNs?You ha e the ri ht to choose any PCP ho participates in our net or and ho is a ailable to accept you and or your family members. or children you may choose a pediatrician as the PCP.You do not need pre authori ation from ptima ealth or from any other person (includin a PCP) in order to obtain access to obstetrical or ynecolo ical care from a healthcare professional in our net or ho speciali es in obstetrics or ynecolo y. The healthcare professional ho e er may be re uired to comply ith certain procedures includin obtainin pre authori ation for certain ser ices follo in a pre appro ed treatment plan or procedures for ma in referrals. or a list of participatin healthcare professionals ho speciali e in obstetrics or ynecolo y contact ember er ices at the number on the bac of your member card or si n in to optimahealth.com members.
What if my plan doctor leaves the Optima Health network?f your plan doctor lea es the net or ptima ealth ill notify and assist you in ndin a ne doctor or facility. f you are in acti e treatment ith a doctor ho lea es the net or you can re uest to continue recei in
healthcare ser ices from the doctor for at least days. f you are beyond the rst trimester of pre nancy you may be able to remain ith that doctor throu h the pro ision of postpartum care directly related to the deli ery.
or a terminal illness treatment may continue for the remainder of the member s life for care directly related to the terminal illness.
PCP FAQs
26

What if I need to see a plan specialist?You do not need a referral from your PCP for specialist care. f you and your PCP ma e the decision for you to see a plan specialist your PCP ill coordinate your care and you can ma e your o n appointment. efore you see a specialist you should con rm that the plan specialist is in the ptima ealth net or . isit optimahealth.commembers or contact ember er ices at the number on the bac of your member card to ma e sure that your specialist is in the net or .
What if my plan doctor directs my care to a non-plan provider?t is your responsibility to ensure that you are usin in net or or plan doctors and facilities. f you ha e an ptima P plan you ha e the option of usin plan pro iders or non plan pro iders. Claims from non plan
pro iders ill be paid at a reduced benefit le el and you ill usually pay a hi her deductible copayment andor coinsurance amounts. You may also be balance billed for any char es in e cess of the plan s allo able char es. To find a plan pro ider use the ind a octor or ind a acility search feature or do nload a Pro ider
irectory from optimahealth.com members. You may also contact ember er ices at the number on the bac of your member card.
Is my plan specialist authorized to order diagnostic or X-ray tests for me?Yes. o e er some tests may re uire pre authori ation by the plan.
Do I need a referral for my annual GYN exam?o. Your Plan does not re uire referrals. emale members may schedule an appointment for a routine annual
e am ith any Y in the ptima ealth net or .
Can an OB serve as PCP while I am pregnant?Yes. urin your pre nancy your can ser e as your PCP. s a Plan member you are automatically eli ible for the ptima ealth Partners in Pre nancy pro ram. This pro ram is desi ned to pro ide education and support to pre nant omen. f you ould li e more information about the pro ram simply call option .
Who is responsible for making sure the plan providers I see and the services I receive are covered under my health plan?t is up to you to no hich doctors and medical facilities are ptima ealth pro iders. To con rm plan
participation use the ind a octor feature on optimahealth.com members do nload a Pro ider irectory from optimahealth.com members or call ember er ices at the number on the bac of your member card.
emember hile you do not need a referral to see care you do need to ensure that you are seein a plan pro ider.
FAQs Specialist Care
27

What is pre-authorization and when is it necessary?Pre authori ation is a clinical re ie of all pertinent medical information to determine medical necessity and your Plan s bene t criteria for co era e. The pro ider of the ser ice is responsible for obtainin pre authori ation.
icensed medical professionals such as P s s beha ioral health professionals clinicians and medical doctors perform the process of pre authori ation by the Plan.
edical ser ices typically re uirin pre authori ation include but are not limited to hospitali ations outpatient sur eries certain dia nostic tests ad anced ima in ser ices ( CT P T) home health ser ices hospice therapies (physical therapy occupational therapy speech therapy) rehabilitation ser ices certain durable medical e uipment prosthetics s illed nursin facilities certain in ectable dru s and scheduled ambulance transportation.
What happens if certain services are not pre-authorized?f your Plan pro ider s re uest for pre authori ation of a medical ser ice is denied by the health plan ptima ealth ill not pay for any cost associated ith the re uested ser ice. f you ish to appeal the denial you may
call ember er ices to initiate the appeal process. Please eep in mind that if you recei e medical ser ices that ptima ealth has denied you must pay all char es for the ser ices.
f you belie e the denial of pre authori ation ill result in the loss of life limb or permanent in ury be sure to tell the representati e at the time you re uest an appeal. n these situations you may re uest an e pedited appeal.P embers f you are a P member ho chooses to use your out of net or bene ts you ha e the responsibility of ensurin that your non Plan pro ider has obtained pre authori ation from ptima ealth prior to the procedure. l ays chec ith ember er ices or o online to optimahealth.com members to ensure that your ser ices ha e been pre authori ed before see in treatment.
Do I need services pre-authorized if I have primary coverage under another health plan?Your pro ider must still call the Plan for pre authori ation e en if you ha e primary co era e under another insurance plan and ha e ptima ealth as secondary insurance. Claims that re uire coordination of bene ts
ith another health plan must still recei e pre authori ation to be eli ible to recei e ma imum bene ts from ptima ealth.
How far in advance should my provider obtain pre-authorization?Your pro ider should obtain electi e pre authori ation at least days or as soon as you are a are prior to the ser ices bein scheduled or pro ided.
How do I ensure pre-authorization has been obtained?To ensure pre authori ation has been obtained isit y ptima on optimahealth.com members contact ember
er ices at the number on the bac of your member card or call your pro ider.
What if I need to be hospitalized?f you need to be hospitali ed for an electi e procedure your Plan doctor must notify ptima ealth business days prior to your admission. f you are hospitali ed due to an emer ency you or a family member should contact
ptima ealth ithin hours (t o business days) of admission or as soon as medically possible.
Pre-Authorization FAQs
28

FAQs After Hours Nurse Advice LineWhat should I do if I get sick or hurt after business hours or during the weekend?f you ha e an illness in ury or condition that occurs durin an e enin or ee end you should call your PCP or plan doctor s of ce or the ptima ealth fter ours urse d ice ine number located on the bac of your member card.
What happens when I call the After Hours Nurse Advice Line?hen you call the fter ours urse d ice ine a re istered nurse ill as you to describe your medical
situation in as much detail as possible. e sure to mention any other medical conditions you ha e such as diabetes or hypertension.
ependin on the situation you may be ad ised about appropriate home treatments or ad ised to isit your plan doctor. f necessary the nurse may direct you to an ur ent care center or emer ency department.The nurses for our fter ours urse d ice ine ha e trainin in emer ency medicine acute care Y and pediatric care. They are ell prepared to ans er your medical or beha ioral health uestions. o e er since they are unable to access medical records they cannot dia nose or medically treat conditions order labs
rite prescriptions order home health ser ices or initiate hospital admissions or dischar es.
Need After Hours Nurse Advice?Call the number on the bac
of your member card. Remember, in an emergencyalways call 911,
or go to the nearest emergency
department.
29

Emergency Care FAQsWhat should I do if I have an emergency?n any life threatenin emer ency al ays o to the closest emer ency department or call . f you received emer ency care and are admitted you or a family member should contact ptima Health ithin
hours (t o business days) or as soon as medically possible. This enables ptima Health to arran e for appropriate follo up care if necessary. n this type of situation care may be revie ed retrospectively to ma e sure it met the criteria for covera e of emer ency ur ent care treatment.
How can I tell if it is an emergency?An emer ency is the sudden onset of a medical condition ith such severe symptoms or pain that an avera e person ith an avera e no led e of health and medicine (prudent layperson) ould see medical care immediately because there may be serious ris to your physical or mental health or that of your unborn child.
ome e amples of situations that ould re uire the use of an emer ency department include but are not limited to
Heart attac severe chest pain oss of pulse or breathintro e Poisonin
• Loss of consciousness • Convulsions
What conditions generally do not require emergency department treatment?The follo in conditions do not ordinarily re uire emer ency department treatment and may be more appropriately treated in your doctor s of ce or at an ur ent care center
• Sprains or strains• Chronic conditions such as arthritis bursitis or bac aches• inor in uries and puncture ounds of the s in
What is the difference between an emergency department and an urgent care center?An emer ency department is desi ned staffed and e uipped to treat life threatenin conditions. An ur ent care center is a more appropriate place to see treatment for sudden acute illness and minor in uries hen your plan doctor s office is closed or not available. opayments and coinsurance amounts for emer ency department visits are enerally hi her than copayments for ur ent care visits. f you are transferred to an emer ency department from an ur ent care center you ill be char ed an emer ency department copaymentcoinsurance.
Do I need to contact Optima Health or my PCP before going to the emergency department/urgent care center?No. f you are unsure hether to visit an emer ency department or ur ent care center you can call your PCP of ce or the After Hours Nurse Advice Line at the number on the bac your member card.
Are there any special emergency care policies I should know about?Yes. ptima Health may revie all emer ency care retrospectively or after the fact to determine if a true medical emer ency did e ist. This retrospective revie policy is desi ned to protect you and all other ptima Health members from the hi h costs associated ith unnecessary use of emer ency departments and ur ent care centers. f you handle nonemer encies as if they are emer encies by see in treatment at an emer ency department or ur ent care center hen a visit to your doctor s of ce ould suf ce you could be responsible for payin a reater portion or all of the char es.
30

What if I become ill when I am outside of the Optima Health service area?Your Plan includes covera e for emer ency services hen you are outside the service area. f you have an une pected illness or in ury hen outside of the service area you should call the After Hours Nurse Advice Line at the number on the bac of your member card.n any life threatenin emer ency al ays o to the closest emer ency department or call .
emember ptima Health may revie all emer ency department care retrospectively or after the fact to determine if a medical emer ency did e ist. f an emer ency did not e ist you could be responsible for payment for all services.
What if I need to be hospitalized?f you received emer ency care and are admitted you or a family member should contact ptima Health ithin hours (t o business days) or as soon as medically possible. This enables ptima Health to revie your care immediately and to arran e for appropriate follo up care. emember all emer ency care may be revie ed retrospectively to ma e sure it met the criteria for covera e of emer ency ur ent care treatment.f you are admitted to a hospital outside of the ptima Health service area call ember Services or the After Hours Nurse Advice Line at the number on the bac your member card.
e prepared to ive the follo in information • ember name • Reason for treatment • Hospital name • City and state here treatment is occurrin • Name of treatin doctor.The doctor or hospital may also call Clinical Care Services.
What happens once I am admitted to the hospital?As part of your ptima Health covera e a RN case mana er ill follo your case from be innin to end. He or she ill revie your medical record chec your pro ress and arran e for your continuin care needs after you leave the hospital.
FAQs Emergency Care
ptima Health mayrevie all emer encydepartment careretrospectively todetermine if amedical emer encydid e ist. f anemer ency did note ist you could beresponsible forpayment for allservices.
31

Pharmacy FAQs
How will my prescription drugs be covered under Optima Health?ptima Health uses a prescription dru formulary. The formulary is a list of dru s that are covered under your
plan. ost ptima Health plans have a four ( ) tier formulary. The tier your dru is placed in ill determine your copayment or coinsurance amount. ru s on tier ill have the lo est out of poc et cost to you. ru s on hi her tiers may cost you more. To vie an abbreviated version of this list or calculate dru costs si n in to optimahealth.com members and select Pharmacy Resources.
Some dru s re uire pre authori ation by ptima Health in order to be covered. Your prescribin provider is responsible for initiatin pre authori ation. You should also chec your plan documents to see hat medications may be e cluded from covera e. ptima Health may also establish monthly uantity limits for selected medications.
Specialty dru s may only be available throu h ptima Health specialty mail order pharmacy. You can chec the ptima Health ebsite for a listin of specialty medications.
How does Optima Health determine my prescription drug tier?ptima Health has a Pharmacy and Therapeutics Committee hich is composed of doctors and pharmacists.
The committee revie s all dru s includin enerics for ef cacy safety overall disease factors and lastly cost. ru s are placed in tiers based on their revie and recommendation. ost eneric dru s usually fall into the
Selected eneric ru s tier (tier ) more e pensive eneric dru s ill be available in Select rand and ther eneric ru s tier (tier ).
How much will I have to pay out-of-pocket for my prescription drug?Your copayments deductibles or coinsurance that may apply to your pharmacy cost are outlined in your plan bene t documents. You must pay your applicable copayment coinsurance hen you pic up your dru from the retail pharmacy. f your plan includes bene ts for mail order prescription dru s you may be able to et certain maintenance dru s by your Plan s net or mail order pharmacy for lo er out of poc et costs.
Is it possible that I would ever pay less than my Copayment/Coinsurance for a prescription?Yes. f the pharmacy s usual and customary cost is less than your copayment coinsurance you ill pay the lesser amount.
There are several thin s to eep in mind before havin your prescriptions lled
. Re istered members of optimahealth.com can locate a participatin pharmacy by si nin in tooptimahealth.com members and selectin Pharmacy Resources.
. f you choose to have your prescription lled at a non participatin pharmacy you ill have to pay thefull cost of the prescription upfront and le for reimbursement from ptima Health. You ill beresponsible for payin all char es in e cess of the ptima Health allo able char e in addition to anycopayment deductible or coinsurance amounts speci ed in your plan documents.
. Some dru s re uire pre authori ation by ptima Health in order to be covered. Your prescribinprovider is responsible for initiatin pre authori ation.
. ptima Health may limit uantities of certain medications.
. f you or your prescribin provider re uests a brand medication hen a eneric e uivalent is availableyou are responsible for the difference in the cost bet een the eneric and the brand name dru inaddition to your copayment coinsurance and or deductible.
As a registered member of optimahealth.com/
members, you can:
• Calculate the cost for a speci c dru or see hichcopayment applies
• See if your dru has a eneric e uivalent• ie the status of your pharmacy claims• Learn about dru s that can treat your condition• se the ru nformation Center to learn about dosa e
stren th side effects and potential dru interactions
• ie your deductibles and out of poc et ma imums (if applicable)
• Locate and et directions to participatin pharmacies
32

What does Optima Health do to assist members with communication disabilities?
ptima Health uses various means to facilitate healthcare services for members ith physical mental lan ua e and cultural barriers.
or members ho may be hearin impaired ptima Health uses the ir inia Relay Service ( ).
embers ho are non n lish spea in can connect to a lan ua e interpretation service by callin the number on the bac of their member card. Additionally members may re uest documents that contain bene t plan premium and appeals information in non
n lish versions includin Amharic Arabic en ali Chinese rench erman Hindi bo orean ru assa Nava o Persian arsi
Russian Spanish Ta alo rdu ietnamese and Yoruba. f you need assistance ith any accommodations in accessin healthcare contact ember Services at the number on the bac of your member
card.
How do I make changes to my membership information?No one else can ma e chan es to or vie your information ithout your consent. n accordance ith privacy la s
e re uire an Authori ation of esi nated A ent form henever anyone other than the ptima Health member needs to obtain and or chan e health information. This form must be si ned and returned to ptima Health. isit optimahealth.com members to do nload a esi nated A ent form or contact ember Services at the number on the bac of your member card to re uest a form.
When and how can I add a newborn or adopted child?You must add ne borns or adopted children to the plan ithin days of birth or placement for adoption. The application and supportin documents for these additions must be submitted directly to your employer for processin . ailure to provide information re uested by ithin
days from the birth or adoption ill result in your dependent bein ineli ible for covera e until the ne t open enrollment period or ualifyin event.
When and how can I enroll my dependent up to age 26?ependents up to a e can be enrolled durin the month of the roup s rene al re ardless of the dependent s
student status. The subscriber has days to add the dependent. f the child is added ithin the day period covera e ill be in on the plan rene al date. f the child is not added ithin the day period the child ill have to ait until the ne t open enrollment or a ualifyin event.
FAQs Member Services
33

Member Services FAQsDo I have to present any additional information to have my application processed?You may need to provide additional information
• f you have dependents ith a different last name from your o n you may need to produce le aldocumentation to support your relationship (e. . birth certi cate marria e certi cate court orderadoption papers etc.).
• f you have dependents that e ceed the ma imum dependent a e you ill be as ed to provide currentdocumentation to support their disabled status.
ailure to provide information re uested by may result in your dependent bein ineli ible for covera e.
Why do you need social security numbers for me and my dependents?Social security numbers (SSN) are re uired on all individuals includin children to comply ith federal la related to coordination of bene ts. f you do not have a social security number or do not ish to provide one a refusal form must be completed annually for each family member not providin a social security number. Ne enrollin members ho do not provide their SSN and do not send a refusal form ill not be enrolled and ill be ineli ible for covera e until your employer s ne t open enrollment period. f you are the subscriber and do not provide the documentation then none of your dependents ill be enrolled.
You do not need to le for reimbursement hen usin your in net or bene ts throu h plan providers. f you use an out of net or provider ho does not le on your behalf you ill need to mail ori inals of your medical bills for reimbursement to
CAL CLA SP. . o Troy
The itemi ed bill should contain the name address ta number and NP number of the provider the name of the member receivin services the date dia nosis and type of services the member received and the char e for each type of service. Your claim ill be processed in accordance ith out of net or bene ts.
34

How is utilization of healthcare services determined?The Clinical Care Services epartment at ptima Health may use any or all of the follo in procedures to determine your healthcare services covera e
• Pre Authori ation (authori ation for covera e from ptima Health prior to receivin services)• Concurrent revie (on oin medical revie of your care and treatment hile services are bein
rendered) or re uest for an e tension of previously approved services. Services include hospitali ations illed nursin facility stays therapies rehabilitation home health and durable medical e uipment.
• Retrospective revie (medical revie for covera e after services have been received)• Case mana ement (individual revie and follo up for on oin speciali ed services)
ptima Health staff (nurses and doctors) ma e covera e decisions based on medical ud mentand evidence based criteria and policies. ur staff does not receive incentives from ptimaHealth based on decisions re ardin covera e.
How does Optima Health pay providers?ptima Health uses a fee for service payment to reimburse doctors for the care they provide. ee for service
payment means doctors are paid for medical care each time it is delivered hether it is for an of ce visit or another form of treatment. sually fee for service payments are at a discounted rate hich has been ne otiated in advance. octors al ays have the ri ht to discuss all medical care and treatment options ith their patients.
What is the Optima Health Quality Improvement Program designed to do?The purpose of the ptima Health uality mprovement Pro ram is to provide a foundation for the development of pro rams and activities directed to ards improvin the health of our members. t is desi ned to implement monitor evaluate and improve processes that are ithin the scope of the health plan. Several committees ithin the or ani ation or on uality mprovement ( ) issues. Committee membership includes ptima Health staff and Plan providers and may include representatives from other or ani ations. ach year ptima Health develops a pro ram and or plan that outlines our efforts to improve clinical care and service to our members.
e identify areas for improvin service by analy in member complaint data and conductin an annual member satisfaction survey. f you ould li e a copy of the current pro ram and or plan or information on other activities please call .
How does Optima Health evaluate and determine coverage for new medical technologies?Since healthcare is constantly chan in the ptima Health team of health professionals are al ays researchin and evaluatin ne medical technolo ies and applications of e istin technolo ies by the follo in
• Revie in current medical literature and research studies• Consultin ith national technolo y rms• Researchin clinical and national state overnment uidelines• Consultin ith members local doctors and other providers in the ptima Health net or
FAQs Utilization Management
35

Important Regulatory Information FAQs
nce you are enrolled as an ptima Health member you are entitled to receive a Plan and a niform Summary of enefits and Covera e (S C). Your is an important document provided
to you by your employer. Read it carefully to understand hat services are covered under ptima Health. Your copayments coinsurances and deductibles are also listed on the facesheet of the . Your S C is a federally mandated document that contains clear consistent and comparable information about your health plan benefits. hen you enroll e ill send you instructions on ho to access your S C online at optimahealth.com members or to request a paper copy.
You are entitled to a list of providers that are in the plan s net or . You can nd this list on optimahealth.commembers or you can call ember Services at anytime to nd out if your provider is in the plan s net or .
How does Optima Health use my personal information?e understand that medical information about you and your health is personal and e are committed to protectin
it. e use information about you to administer your bene ts process your claims provide education and clinical care coordinate your bene ts ith other insurance carriers and other transactions related to providin you and your dependents healthcare covera e.
How does Optima Health protect my personal information?The Health nsurance Portability and Accountability Act of (H PAA) requires that health plans protect the con dentiality of your private health information. ptima Health ill not use or further disclose H PAA protected health information (PH ) e cept as necessary for treatment payment and health plan operations as permitted or required by la or as authori ed by you. A complete description of your ri hts under H PAA can be found in the Sentara Healthcare nte rated Notice of Privacy Practices. You can also o to optimahealth.com members to see a copy of our privacy notice. The Common ealth of ir inia also has la s in place to protect the privacy of our members insurance information.
e ill not release data about you unless you have authori ed it or as permitted or required by la . ptima Health requires an Authori ation of esi nated A ent form henever anyone other than the ptima Health member needs to obtain and or chan e health information. You can do nload a copy of the form at optimahealth.com members under ana e y Plan ember orms or by callin ember Services at the number on the bac on your member card.
nder H PAA and ir inia la you have certain ri hts to see and copy health information about you. nder H PAA you have the ri ht to request an accountin of certain disclosures of the information and under certain circumstances amend the information. You have the ri ht to le a complaint ith ptima Health or ith the Secretary of the .S. epartment of Health and Human Services if you believe your ri hts under H PAA have been violated.
What if I decide not to enroll with Optima Health at this time? Will my dependents or I be able to enroll later?f you are declinin enrollment for yourself or your dependents (includin your spouse) because of other health
insurance or roup health plan covera e you may be able to enroll yourself and your dependents ith ptima Health
.
36

Optima Health offers special enrollment for employees and dependents that lose eligibility under Medicaid or CHIP coverage.
mployees or dependents ho are eli ible for roup covera e ill be permitted to enroll late if they ( ) lose eli ibility for edicaid or CH P covera e or ( ) become eli ible to participate in a premium assistance pro ram under edicaid or CH P. n both cases the employee must request special enrollment ithin days of the loss of edicaid CH P or of the eli ibility determination.To request special enrollment or obtain more information contact your employer roup bene ts administrator or contact ptima Health ember Services at the number located on the bac of your member card.
What if I have coverage under more than one health plan?f you have covera e under another health plan that plan may have primary responsibility for the covered
e penses of you or your family members. ptima Health uses order of bene t rules to determine hether it is the primary or secondary plan. enerally the plan that covers the person as a subscriber pays rst. f your dependents are covered under more than one healthcare plan ptima Health has rules based on subscriber date of birth len th of covera e and custody obli ations that determine primary responsibility.
What are my rights under the Women’s Health and Cancer Rights Act?nder the omen s Health and Cancer Ri hts Act of and accordin to ir inia State La ptima Health
provides bene ts for the mastectomy related services listed belo in a manner determined in consultation ith the attendin doctor and the member • All sta es of reconstruction of the breast on hich the mastectomy has been performed • Sur ery and reconstruction of the other breast to produce a symmetrical appearance • Prosthesis and any physical complications resultin from the mastectomy includin lymphedema.Covera e for breast reconstruction bene ts is sub ect to deductibles copayments and or coinsurance consistent ith those established for other bene ts under ptima Health. Call ember Services at the number on the bac of your member card for more information.
FAQs Important Regulatory Information
37

nder ederal and ir inia State La you have certain ri hts and protections re ardin your maternity bene ts ith ptima Health.nder federal la no n as the Ne borns and others Health Protection Act of (Ne borns Act) roup health
plans and health insurance issuers enerally may not restrict bene ts for any hospital len th of stay in connection ith childbirth for the mother or ne born child to less than hours follo in a va inal delivery or less than hours
follo in a cesarean section. Ho ever federal la enerally does not prohibit the mother s or ne born s attendin provider after consultin ith the mother from dischar in the mother or her ne born earlier than hours (or hours as applicable). n any case plans and issuers may not under ederal La require that a provider obtain authori ation from the Plan or the issuer for prescribin a len th of stay not in e cess of hours (or hours).
nder ir inia State La if your Plan provides bene ts for obstetrical services your bene ts ill include covera e for postpartum services. Covera e ill include bene ts for inpatient care and a home visit or visits hich shall be in accordance ith the medical criteria outlined in the most current version of or an of cial update to the uidelines for Perinatal Care prepared by the American Academy of Pediatrics and the American Colle e of bstetricians and ynecolo ists or the Standards for bstetric ynecolo ic Services prepared by the American Colle e of
bstetricians and ynecolo ists. Covera e for obstetrical services as an inpatient in a eneral hospital or obstetrical services by a physician shall provide such bene ts ith durational limits eductibles Coinsurance factors and Copayments that are enerally no less favorable than for physical illness.
What can I do to prevent Healthcare Fraud?raud increases the cost of healthcare for everyone. Here are some thin s that you can do to prevent fraud
• o not ive your plan identi cation ( ) number or other personal information over the telephone or email it to people you do not no e cept for your healthcare providers or ptima Health representatives. • o not o to a doctor ho says that an item or service is not usually covered but they no ho to bill the health plan to et it paid. o not as your doctor to ma e false entries on certi cates bills or records in order to et us to pay for an item or service. • Carefully revie e planation of bene ts ( ) statements that you receive from the health plan. f you suspect a provider has char ed you for services you did not receive billed you t ice for the same service or misrepresented any information contact the provider for an e planation. There may be an error.
ptima Health provides its members a ay to report situations or actions they thin may be potentially ille al unethical or improper. f you ant to report fraudulent or abusive practices you can call the raud and Abuse Hotline at the number belo . You can also send an email or for ard your information to the address belo . All referrals may remain anonymous. Please be sure to leave your name and number if you ish to be contacted for follo up. f appropriate the necessary overnmental a ency (e. . AS C S etc.) ill be noti ed as required by la .
FAQs Important Regulatory Information
Optima Health Fraud & Abuse Hotline: 1-866-826-5277 Email: [email protected] Mail: Optima Health c/o Special Investigations Unit 4417 Corporation Lane Virginia Beach, VA 23462
38

Flu and Pneumonia PreventionFlu VaccineThe u vaccine is covered for members ith medical and or pharmacy bene ts administered by ptima Health. The Centers for isease Control and Prevention (C C) recommends a yearly u vaccine for everyone si months of a e and older as the rst and most important step in protectin a ainst this serious disease. hile there are many different u viruses the u vaccine is desi ned to protect a ainst the main u strains that research indicates ill cause the most illness durin each u season.
ptima Health members may visit the follo in locations to receive a u shotYour doctor • Chec ith your physician to see if he or she offers the u vaccine. • A physician of ce Copayment may apply.Your local pharmacy • embers should visit optimahealth.com members to do nload a list of participatin pharmacies. • e recommend that you call the pharmacy in advance to chec the availability of the u vaccine.
f you need additional assistance ndin a location to receive the u vaccine contact ptimaHealth ember Services at the number on the bac of your member card.
Pneumonia VaccineThe C C de nes pneumonia as an infection of the lun s that can cause mild to severe illness in people of all a es. Si ns of pneumonia can include cou hin fever fati ue nausea vomitin rapid breathin or shortness of breath chills or chest pain. Certain people are more li ely to become ill ith pneumonia. This includes adults years of a e or older and children youn er than ve years of a e. People up throu h years of a e ho have underlyin medicalconditions (li e diabetes or H A S) and people throu h ho smo e ci arettes or have asthma are also at increased ris for ettin pneumonia.
The pneumococcal con u ate vaccine (PC or Prevnar ) protects a ainst the types of pneumococcal bacteria that cause most of the severe illness in children and adults. The vaccine can also help prevent some ear infections. PC is recommended for all children at and throu h months old. PC is also recommended for adults years or older ith certain medical conditions and in all adults years or older.
The pneumococcal polysaccharide vaccine (PPS or Pneumova ) protects a ainst types of pneumococcal bacteria. t is recommended for all adults years or older and for anyone ho is years or older at hi h ris for disease. PPS is also recommended for adults throu h years old ho smo e ci arettes or ho have asthma.
ptima amily Care and A S members are ineli ible for the ptima Health pharmacy administered lu accination Pro ram.
Please see your provider for information on receivin the u or pneumonia vaccine.
39

Health and Preventive ServicesOverviewHealth and Preventive Services of ptima Health provides individual and roup pro rams to improve health and prevent disease. The department offers a ide ran e of services includin direct mail reminders health screenin s self learnin pro rams online education u shots and selected classes.
Personal Health Assessment & Health CoachingThe completion of a Personal Health Assessment (PHA) includes the identi cation of health ris s for members and tar eted interventions to reduce ris s and improve health. embers receive health ris information tar eted at their readiness to chan e.
ptima Health has a po erful resource yLife yPlan Connection to help members adopt healthy behaviors reduce health ris s and lo er their lifetime cost of care. yLife yPlan Connection offers our members e ible pro rams e pert uidance and inspiration to ta e char e of their o n health hether they are continuin healthy behaviors or ma in a chan e to improve their health. t all be ins hen the member completes a Personal Health Assessmentand creates the foundation for their Health Record and coachin pro ram. ur health coachin partner offers a comprehensive online activities tool no n as the i ital Health Assistant ( HA). The HA delivers a personali ed interactive and motivational e perience to help members ta e action and sustain healthy behaviors in a fun ay.
Healthy Publicationsembers can request Health ise Handboo a self care manual ith valuable information about health
improvement common illnesses and preventive health care.
The Patient denti cation ana er Reminder System informs members of recommended immuni ations and preventive health screenin s that help ht communicable disease and dia nose cancer in the earliest most treatable sta es. Healthy Pro rams ive members valuable and current information and encoura ement to reduce health ris s.
mployees ho improve their health can reduce their healthcare needs reduce absenteeism and reduce healthcare costs. nitiatives of this system include
• ammo raphy reminders omen and older ho have not had a mammo ram in the previous monthsreceive a postcard durin their birthday month. This card informs them of the recommended mammo raphy schedule and the importance of mammo raphy and cervical cancer screenin .
• Cervical cancer screenin reminders omen and older ho have not had a cervical cancer screenin inthe previous months receive a postcard durin their birthday month. This card informs them of Pap smear recommendations and the importance of cervical cancer and mammo raphy screenin .
• Healthy pre nancy mailin s nce the health plan learns of a member s pre nancy she receives the follo in. The Plannin a Healthy Pre nancy Self Care Handboo. A letter and ma net featurin the childhood immuni ation schedule and our ishes for a healthy
delivery (sent once member is in her seventh month of pre nancy)• mmuni ation postcards and letters Parents receive a postcard re ardin basic immuni ation schedule for
children at and months of a e.• irthday cards All plan members a e and over receive a birthday card durin their birthday month from the
plan. Part of this mailin includes a boo mar er that serves to remind members of the preventive health uidelines they should follo to achieve their personal best health.
• Physician noti cations Physicians receive monthly lists of their patients (our members) ho ere reminded throu h the P System and have still not completed their preventive screenin s.
To determine if you have access to telephonic Health Coachin chec ith your bene ts administrator or call ember Services.
40

Health and Preventive Servicesased on health screenin ndin s members receive roup individual and self paced pro rams to reduce
cardiovascular health ris s and promote health.
Healthy Programs
Eating for Life is an a ard innin educational pro ram that helps participants develop healthy eatin and e ercise habits.
Get Off Your Butt: Stay Smokeless for Life is an educational pro ram offerin support for anyone ho ants to quit tobacco use.
Guided Meditation is a pro ram that invites listeners to e perience a calm peaceful retreat from everyday stressors.
Healthy Habits Healthy You is a pro ram that offers helpful ays to prevent Type diabetes and heart disease ith healthy food choices mana in body ei ht e ercisin and ndin ays to rela and et more sleep.
Movement Programs
Tai Chi is a pro ram that helps your body to mentally and physically rela . The movements enhance your blood o release muscle tension and improve your balance.
WalkAbout with Healthy Edge is a pro ram that focuses on increasin re ular activity. t includes a step trac in device and encoura es participants to start movin and be in al in their ay to better health.
Yoga pro rams include stretchin and stren thenin e ercises to help improve e ibility stren th and cardiovascular health. Chair Yo a is also available.
Health and Preventive Services by ptima Health provides individual and roup pro rams to improve health and prevent disease.
embers have access to direct mail reminders health screenin sself learnin pro rams nternet resources and more.
41

An appeal is e pedited if a member s life health or the ability to re ain ma imum function is in eopardy or if a physician believes a member ould be sub ected to severe pain that could not be adequatelymana ed ithout therequested care ortreatment.
Resolving Member Complaints and Appealsf you have a problem or concern about ptima Health and or the quality of care services and or policies and procedures of ptima Health call ember Services at the number on the bac of your member card.
ptima Health has a formal process that allo s your concern to be addressed ith the appropriate departmentspersons ithin ptima Health. Research into your concerns is conducted in a timely manner to accommodate any clinical ur ency of the situation. pon research and revie you ill be noti ed of the resolution to your concern.
f your concern involves a denial of a covered service or claim ptima Health includes a formal internal and ur ent appeals process. e also have an independent e ternal appeal process. o nload an appeal pac et from the ana e
y Plan section on optimahealth.com members or contact ember Services to initiate the appeals procedure.
The .S. epartment of Labor Pension and elfare ene ts Administration can assist members in ndin out hat other voluntary alternative dispute resolutions are available.
U.S. Department of LaborToll ree SA L ( ) or
Other resources to help you:or questions about your appeal ri hts or for assistance you can contact the mployee ene ts Security
Administration at SA ( )
Did you know that you could download an Appeals Packet
from optimahealth.com/members?
42

Member Rights and ResponsibilitiesAs a member of ptima Health you are entitled to all covered bene ts ho ever you must learn ho the health plan or s follo the proper procedures and use the proper net or (i.e. Plan doctors hospitals mental health providers and other Plan specialists participatin ith ptima Health).
Optima Health Plan Members have the right to:. Timely and uality of Carea. Access to Protected Health nformation (PH ) medical records physicians and other healthcare professionals
and referrals to specialists hen medically necessary.b. Continuity of care and to no in advance the time and location of an appointment as ell as the physicians and
other health care professionals providin care.c. Receive the medical care that is necessary for the proper dia nosis and treatment of any covered illness or
in uryd. Participate ith physicians and healthcare professionals in
i. iscussin their dia nosis the pro nosis of the condition and instructions required for follo up careii. nderstandin the health problems and assistin to develop mutually a reed upon oals for treatmentiii. ecision ma in re ardin their healthcare and treatment plannin andiv. A candid discussion of appropriate or medically necessary treatment options for their condition re ardless
of cost or bene t covera e.e. The ri ht to af rm that all practitioners providers and employees ho ma e utili ation mana ement ( )
decisionsi. ase decisions on appropriateness of care services and e istence of covera eii. Are not re arded for issuin medical denials of covera e andiii. o not encoura e decisions that result in underutili ation throu h nancial incentives.
. Treatment ith i nity and Respect embers illa. e treated ith respect di nity compassion and the ri ht to privacy.b. ercise these ri hts re ardless of race physical or mental ability ethnicity ender se ual orientation creed
a e reli ion or their national ori in cultural or educational bac round economic or health status n lishpro ciency readin s ills or source of payment for their care. pect this ri ht by both Plan and contractinphysicians.
c. pect protection of all oral ritten and electronic information across the Plan and information to plan sponsorsand employers.
d. tend their ri hts to any person ho may have le al responsibility to ma e decisions on the member s behalfre ardin medical care.
e. e free from any form of restraint or seclusion used as a means of coercion discipline convenience or retaliation.f. e able to refuse treatment or to si n a consent form if the member feels they do not clearly understand its
purpose or crossout any part of the form they do not ant applied to their care or chan e their mind about anytreatment for hich they have previously iven consent and be informed of the medical consequences of thisaction.
. Receive Health Plan nformation embers illa. Receive information about their health plan its services its physicians other health care professionals facilities
clinical uidelines and member ri hts and responsibilities statements and collection use and disclosure of PH .b. no by name title and or ani ation the physicians nurses or other health care professionals providin care.c Receive information about medications ( hat they are ho to ta e them and possible side effects) and pharmacy bene t information (effective date of formulary chan e ne dru s available or recalled medications).
43

Member Rights and Responsibilitiesd. Receive clear information re ardin bene ts and e clusions of their policy ho medical treatment decisions are
made authori ed by the health plan or contracted medical roups payment structure and the ri ht to approvethe release of information.
e e advised if a practitioner proposes to en a e in e perimentation affectin care or treatment. The member may have the ri ht to refuse to participate in such research.
f. e informed of policies re ardin Advance irectives (livin ills) as required by state and federal la s.. embers Solve Problems in a Timely anner bya. Presentin questions concerns or complaints to a customer service specialist ithout discrimination
and e pect problems to be fairly e amined and appropriately addressed.b. oicin concerns or complaints to ptima Health about their health plan if the care provided as inadequate
or feel their ri hts have been compromised. This includes the ri ht to appeal an action or denial and the processinvolved.
c. a in recommendations re ardin the health plan members ri hts and responsibilities policies.
44

Member Rights and ResponsibilitiesMember ResponsibilitiesOptima Health Plan Members, in addition to their rights, subscribers and their enrolled dependents have the responsibility:
. To identify themselves and their family members as an ptima Health enrollee and present their identi cation card(s) hen requestin healthcare services.
. To be on time for appointments and contact the physician or other healthcare personnel at once if there is a need to cancel or if they are oin to be late for an appointment. f the physician other healthcare personnel or facility has a policy assessin char es re ardin late cancellations or no sho s the member ill be responsible for such char es.
. To provide information about their health to physicians and other health care professionals so they may provide appropriate medical care.
. To actively participate and understand improvin their health condition(s) by follo in the plans and instructions for care and treatment oals that they a reed upon ith the physician or healthcare professional.
. To act in a manner that supports the care provided to other patients and the eneral functionin of the of ce or facility.
. To revie the employee handboo and Plan documentation a. To ma e sure the services are covered under the plan b. To approve release of information and have services properly authori ed before receivin medical attention c. To follo proper procedures for illness before and after business hours and d. or materials concernin health bene ts (e. . issues) and educate other covered family members.
. To accept nancial responsibility for any copayment or coinsurance associated ith services received hile under the care of a physician or other healthcare professional or hile a patient at a facility.
. To contact ptima Health if they have concerns or if they feel their ri hts have been compromised.
or questions concerns or additional information please visit .optimahealth.com or contact ember Services at the number on the bac of your member card. T TTY services and lan ua e assistance are available.
Code of ederal Re ulations. Revised as of Au ust . C. .R. . . Retrieved from https . po. ov . National Committee for uality Assurance (NC A) ( ). Standards and uidelines for the Accreditation of Health Plans. HP Standards and uidelines. ashin ton C. NC A.Common ealth of ir inia. epartment of edical Assistance Services. ( ). edallion . ana ed Care Contract Section . .
45

Advance DirectivesFederal Law requires Optima Health to provide enrolled members 18 years of age or older the opportunity to make decisions concerning their right to accept or refuse medical or surgical treatment and their right to formulate written instructions called an Advance Directive.
An Advance Directive consists of three parts: a living will, designation of healthcare agent, and wishes regarding anatomical gift or organ donation. Advance Directives are recognized under State Law and Federal Law and are to provide for the wishes of individuals who are unable to make medical care decisions on their own.
The law requires that the care you receive from any Plan provider will not be affected by your making (or not making) an Advance Directive, unless your Advance Directive states that medical care should not be given to you.
In compliance with Federal Law, Optima Health is providing you with information about the Patient Self-Determination Act. The following is a summary of our policies regarding patients’ rights and Advance Directives. It means you have a chance to make important life choices. You may never need to exercise these choices, but making them ahead of any event can give peace of mind to you and your family.
You may want to take this opportunity to discuss and document your wishes with your family, attorney, and/or a close friend. It is also important to talk with your Plan doctor about your choices, so he or she is informed and understands your wishes.
We will gladly send you advance care planning guide, which tells more about Advance Directives, and information on a Virginia living will, designation of healthcare agent, and wishes regarding anatomical gift or organ donation form.
If you have an Advance Directive, take a copy of the member statement to your next Plan doctor appointment. You may download an Advance Directive from optimahealth.com/members. If you would like more information, call Member Services at the number on the back of your member ID card.
Summary of Policies on Patient Rights and Advance DirectivesPurposeThis policy is intended to enable ptima Health to comply ith the Patient Self etermination Act. The purpose of the act is to protect each adult patient s ri ht to participate in healthcare decision ma in to the ma imum e tent of his or her ability and to prevent discrimination based on hether the patient has e ecuted an Advance irective for healthcare.
Practice Statementptima Health supports a patient s ri ht to participate in healthcare decision ma in . Throu h education and inquiry
about Advance irectives this health plan ill encoura e patients to communicate their healthcare preferences and values to others. Such communication ill uide others in healthcare decision ma in for the patient if the patient is incapacitated.
46

Advance DirectivesProceduresAt enrollment you ill be provided information about your ri hts under ir inia la to • a e decisions about your medical care includin your ri ht to accept or refuse medical and sur ical treatment. • a e an Advance irective such as a livin ill or durable po er of attorney for healthcare if you choose to do so. • You ill be as ed if you have made an Advance irective. • f you have you ill need to ive this form to your plan doctor so it ill be made part of your medical record. You ill need to eep an additional copy for yourself. • f you have not and ish to do so you ill be provided additional information upon request in order to ma e an Advance Directive. • You ill be encoura ed to discuss your Advance Directive ith your family plan doctor cler y attorney or a close friend. • f you do not have an Advance Directive do not ant to ma e one and do not ant more information you ill not be as ed any more questions.
You may revo e your Advance Directive at any time in ritin or by oral declaration. Your ma in (or not ma in ) an Advance Directive ill not affect the care you receive from any plan provider unless your Advance Directive states that medical care should not be iven to you. Your Advance Directive ill be follo ed unless it requests medical care that is inappropriate unethical or is of no medical bene t or harmful to you.
f your plan doctor is un illin to comply ith your Advance Directive or ith the decision of a person you desi nate to ma e decisions for you he or she ill ma e a reasonable effort to transfer your care to another plan doctor ithin
days. Durin this period your plan doctor must continue any life sustainin care.
47

Su
mm
ary o
f B
en
efi
ts
48

OOptima Health
Point of Service (POS)
PREMIER PLAN
49

ADMINISTERED BY SENTARA HEALTH PLANS, INC.Plus2080p_0114
OPTIMA POINT OF SERVICE (POS) PREMIER 2019 SUMMARY OF BENEFITS
City of Virginia Beach & Virginia Beach City Public SchoolsThis document is not a contract or policy with Optima Health. It is a summary of benefits and services available through the Plan. If there are any differences between this summary and the employer group Plan Document, the provisions of those documents will prevail for all benefits, conditions, limitations and exclusions.
Deductibles, Maximum Out-of-Pocket LimitsOPTIMA NETWORK / PHCS NETWORK OUT-OF-NETWORK
Deductibles per Calendar Year3 $ 850 per Individual $ 1,700 per Family
$1,700 per Individual $3,400 per Family
Maximum Out-of-Pocket Limit per Calendar Year $3,000 per Individual4
$6,000 per Family4$4,500 per Individual5
$9,000 per Family5
Physician ServicesIncludes Covered Services performed in the Physician’s office during the Physician office visit. Includes, but is not limited to, office consults and exams; In-office surgery; In-office lab, x-ray, injections, and diagnostic and treatment services. Family planning services including injectables and vasectomy; Physical, Occupational, and Speech Therapy; Cardiac, Pulmonary, and Vascular Rehabilitation Services; Chemo, Radiation, IV, and Respiratory therapy services; Dialysis treatments. Pre-Authorization is required for in-office surgery6
Physician Office Visits OPTIMA NETWORK / PHCS NETWORK Copayment/Coinsurance2
OUT-OF-NETWORK Copayment/Coinsurance2
MDLIVE Services $10 Copayment then covered at 100% Not ApplicableSentara Quality Care Network (SQCN) Primary Care Physician (PCP) Office Visit SQCN providers are currently available in Hampton Roads, Charlottesville and Rockingham zip codes only. Members who do not reside in those areas will pay the SQCN provider copay.
Non-Sentara Quality Care Network (SQCN) Primary Care Physician (PCP) Office Visit
$20 Copayment then covered at 100%
$40 Copayment then covered at 100%
After Deductible Covered at 60%
Sentara Quality Care Network (SQCN) Specialist Office Visit SQCN providers are currently available in Hampton Roads, Charlottesville and Rockingham zip codes only. Members who do not reside in those areas will pay the SQCN provider copay.
Non-Sentara Quality Care Network (SQCN) Specialist Office Visit
$40 Copayment then covered at 100%
$60 Copayment then covered at 100%
After Deductible Covered at 60%
Physician ServicesPreventive Care10 OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Routine Annual Physical Exams Well Baby Exams Annual GYN Exams and Pap Smears11 PSA Tests Colorectal Cancer Tests Routine Adult and Childhood Immunizations Screening Colonoscopy Screening Mammograms (including 3-D mammograms) Women’s Preventive Services
Covered at 100% After Deductible Covered at 60%
50

ADMINISTERED BY SENTARA HEALTH PLANS, INC.Plus2080p_0114
Outpatient Therapy and Rehabilitation ServicesShort Term Therapy Services7 OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Physical Therapy Occupational Therapy Pre-Authorization is required.6
Physical and Occupational Therapy are limited to a maximum combined benefit with In-Network and Out-of-Network benefits and for all places of service of 30 visits per calendar year.7 Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 85% After Deductible Covered at 60%
Speech Therapy Pre-Authorization is required.6
Speech Therapy is limited to a maximum combined benefit with In-Network and Out-of-Network benefits and for all places of service of 30 visits per calendar year.7 Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 85% After Deductible Covered at 60%
Short Term Rehabilitation Services7 OPTIMA NETWORK / PHCS NETWORK Copayment/Coinsurance2
OUT-OF-NETWORK Copayment/Coinsurance2
Cardiac Rehabilitation Pulmonary Rehabilitation Vascular Rehabilitation Vestibular Rehabilitation Pre-Authorization is required.6
Services are limited to a maximum combined benefit with In-Network and Out-of-Network benefits and for all places of service of 30 visits per calendar year.7 Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 85% After Deductible Covered at 60%
Other Outpatient Treatments OPTIMA NETWORK / PHCS NETWORK Copayment/Coinsurance2
OUT-OF-NETWORK Copayment/Coinsurance2
Chemotherapy Radiation Therapy IV Therapy Inhalation Therapy
Physician’s Office Visit: $20 Copayment
Specialist office visit: $40 Copayment
Outpatient Facility: After Deductible Covered at 85%
Physician’s Office Visit: Covered at 60%
Specialist office visit: Covered at 60%
Outpatient Facility: After Deductible Covered at 60%
Outpatient Therapy and Rehabilitation ServicesOther Outpatient Treatments OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Pre-Authorized Injectable and Infused Medications Includes injectable and infused medications, biologics, and IV therapy medications that require prior authorization. Coinsurance applies when medications are provided in a Physician’s office, outpatient facility, or in the Member’s home as part of Skilled Home Health Care Services benefit. Coinsurance is in addition to any applicable office visit or outpatient facility Copayment or Coinsurance.
After Deductible Covered at 85% After Deductible Covered at 60%
51

ADMINISTERED BY SENTARA HEALTH PLANS, INC.Plus2080p_0114
Outpatient Dialysis ServicesOutpatient Dialysis Services OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Dialysis Services Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 85% After Deductible Covered at 60%
Outpatient SurgeryOutpatient Surgery OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Outpatient Surgery Pre-Authorization is required.6
Coinsurance or Copayment applies to services provided in a free-standing ambulatory surgery center or hospital outpatient surgical facility.
After Deductible Covered at 85% After Deductible Covered at 60%
Outpatient Diagnostic ProceduresCopayment or Coinsurance will apply when a procedure is performed in a free-standing outpatient facility or lab, or a hospital outpatient facility or lab.Outpatient Diagnostic Procedures OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Outpatient Diagnostic Procedures After Deductible Covered at 85% After Deductible Covered at 60%Outpatient X-Ray Ultrasound Doppler Studies
After Deductible Covered at 85% After Deductible Covered at 60%
Outpatient Lab Work After Deductible Covered at 85% After Deductible Covered at 60%
Outpatient Advanced Imaging and Testing ProceduresOutpatient Advanced Imaging and Testing Procedures OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Magnetic Resonance Imaging (MRI) Magnetic Resonance Angiography (MRA) Positron Emission Tomography (PET Scans) Computerized Axial Tomography (CT Scans) Computerized Axial Tomography Angiogram (CTA Scans) Sleep Studies Pre-Authorization is required.6
Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 85% After Deductible Covered at 60%
Maternity CareMaternity Care OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Maternity Care 8,10,11
Pre-Authorization is required for prenatal services.6
Includes prenatal, delivery, postnatal, postpartum services, and home health visits. Copayment or Coinsurance is in addition to any applicable inpatient hospital Copayment or Coinsurance. Sentara Quality Care Network (SQCN) SQCN providers are currently available in Hampton Roads, Charlottesville and Rockingham zip codes only. Members who do not reside in those areas will pay the SQCN provider coinsurance.
Non-Sentara Quality Care Network (SQCN)
$350 Copayment, then covered at 100%
$500 Copayment, then covered at 100%
After Deductible Covered at 60%
52

ADMINISTERED BY SENTARA HEALTH PLANS, INC.Plus2080p_0114
Inpatient ServicesInpatient Services OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Inpatient Hospital Services Pre-Authorization is required.6
Transplants are covered at contracted facilities only.
After Deductible Covered at 85% After Deductible Covered at 60%
Skilled Nursing Facilities/Services7 Pre-Authorization is required.6
Following inpatient hospital care or in lieu of hospitalization. Covered Services include up to 100 days combined in and out-of-network per calendar year that in the Plan’s judgment requires Skilled Nursing Facility Services.7
After Deductible Covered at 85% After Deductible Covered at 60%
Ambulance ServicesAmbulance Services OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Ambulance Services9
Pre-Authorization is required for non-emergent transportation only. Includes air and ground ambulance for emergency transportation, or non-emergent transportation that is Medically Necessary and Pre-Authorized by the Plan. Copayment or Coinsurance is applied per transport each way.
Covered at 85% *If transported by a Virginia BeachVolunteer Rescue Squad – Covered at 100%
Covered at 85%
Emergency ServicesEmergency Services OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Emergency Services9
Pre-Authorization is not required. Includes Emergency Services, Physician, and Ancillary Services provided in an emergency department facility. Coinsurance waived for facility charges if admitted. Inpatient copayment / coinsurance will apply if admitted.
After Deductible Covered at 85% After Deductible covered at 85%
Urgent Care Center ServicesUrgent Care Center Services OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Urgent Care Services9
Pre-Authorization is not required. Includes Urgent Care Services, Physician services, and other Ancillary Services received at an Urgent Care facility. If You are transferred to an emergency department from an Urgent Care center, You1 will pay an Emergency Services Copayment or Coinsurance.
Covered at 85% Covered at 60%
53

ADMINISTERED BY SENTARA HEALTH PLANS, INC.Plus2080p_0114
Mental/Behavioral Health Care Includes inpatient and outpatient services for the treatment of mental health and substance abuse. Also includes services for Biologically Based Mental Illnesses for the following diagnoses: schizophrenia, schizoaffective disorder, bipolar disorder, major depressive disorder, panic disorder, obsessive-compulsive disorder, attention deficit hyperactivity disorder, autism, and drug and alcoholism addiction.
Mental/Behavioral Health Care OPTIMA NETWORK / PHCS NETWORK Copayment/Coinsurance2
OUT-OF-NETWORK Copayment/Coinsurance2
Inpatient Services Pre-Authorization is required.6
Residential Treatment is not covered.
After Deductible Covered at 85% After Deductible Covered at 60%
Sentara Quality Care Network (SQCN) Outpatient Office Visits Pre-Authorization may be required.6 SQCN providers are currently available in Hampton Roads, Charlottesville and Rockingham zip codes only. Members who do not reside in those areas will pay the SQCN provider copay.
Non-Sentara Quality Care Network (SQCN) Outpatient Office Visits Pre-Authorization may be required.6
$20 Copayment then covered at 100%
$40 Copayment then covered at 100%
Covered at 60%
Other Outpatient Visits (Includes Hospital Outpatient and Freestanding Outpatient Centers) Pre-Authorization may be required.6
After Deductible Covered at 85% Covered at 60%
Other Covered ServicesOther Covered Services OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Allergy Care Includes Allergy testing, Injections, Serum and RAST testing.
Covered at 85% After Deductible Covered at 60%
54

ADMINISTERED BY SENTARA HEALTH PLANS, INC.Plus2080p_0114
Other Covered ServicesOther Covered Services OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Autism Spectrum Disorder Pre-Authorization is required.6 Covered Services include “diagnosis” and “treatment” of Autism Spectrum Disorder in children from age two through 10.
“Autism Spectrum Disorder” means any pervasive developmental disorder, including (i) autistic disorder, (ii) Asperger’s Syndrome, (iii) Rett syndrome, (iv) childhood disintegrative disorder, or (v) Pervasive Developmental Disorder – Not Otherwise Specified, as defined in the most recent edition of the Diagnostic and Statistical Manual of Mental Disorders of the American Psychiatric Association.
“Diagnosis of autism spectrum disorder” means medically necessary assessments, evaluations, or tests to diagnose whether an individual has an autism spectrum disorder.
“Treatment for autism spectrum disorder” shall be identified in a treatment plan and includes the following care prescribed or ordered for an individual diagnosed with autism spectrum disorder by a licensed physician or a licensed psychologist who determines the care to be medically necessary: (i) behavioral health treatment, (ii) pharmacy care, (iii) psychiatric care, (iv) psychological care, (v) therapeutic care, and (vi) applied behavioral analysis when provided or supervised by a board certified behavioral analyst licensed by the Board of Medicine.
“Applied behavioral analysis” means the design, implementation, and evaluation of environmental modifications, using behavioral stimuli and consequences, to produce socially significant improvement in human behavior, including the use of direct observation, measurement, and functional analysis of the relationship between environment and behavior. Coverage for applied behavioral analysis under this benefit is limited to an annual maximum benefit of $35,000.6
Coverage for Autism Spectrum Disorder will not be subject to any visit limits, and will be neither different nor separate from coverage for any other illness, condition, or disorder for purposes of determining Deductibles, lifetime dollar limits, Copayment and Coinsurance factors, and benefit year maximum for Deductibles and Copayment and Coinsurance factors.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of treatment or service listed on the Summary of Benefits.
Coverage for Autism Spectrum Disorder will not be subject to any visit limits, and will be neither different nor separate from coverage for any other illness, condition, or disorder for purposes of determining Deductibles, lifetime dollar limits, Copayment and Coinsurance factors, and benefit year maximum for Deductibles and Copayment and Coinsurance factors.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of treatment or service listed on the Summary of Benefits.
55

ADMINISTERED BY SENTARA HEALTH PLANS, INC.Plus2080p_0114
Other Covered ServicesOther Covered Services OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Prosthetic Limbs and Components7
Pre-Authorization is required.6
Services include coverage for medically necessary prosthetic devices. This also includes repair, fitting, replacement and components.
Definitions: “Component” means the materials and equipment needed to ensure the comfort and functioning of a prosthetic device. “Limb” means an arm, a hand, a foot, or any portion of an arm, hand, a leg or foot. “Prosthetic device” means an artificial device to replace, in whole or in part, a limb. Prosthetic device coverage does not mean or include repair and replacement due to enrollee neglect, misuse, or abuse. Coverage also does not mean or include prosthetic devices designed primarily for an athletic purpose.
After Deductible Covered at 85% After Deductible Covered at 60%
Chiropractic Care7
Optima Health contracts with American Specialty Health Group (ASH) to administer this benefit6. Pre-Authorization is required by ASH for all chiropractic care services. 6
To receive services, contact ASH's Member Services at 1-800-678-9133. Representatives are available from 8:00 AM to 9:00 PM Monday-Friday. Coverage is limited to a combined maximum benefit with in- and out-of-network benefits of 30 visits per Person, per calendar year. This benefit also includes coverage of Chiropractic appliances up to a combined maximum benefit with in-and out-of-network benefits of 1 appliance per Person per calendar year when medically necessary.
For providers not in the ASH network the Member will be responsible for payment of all charges in excess of ASH’s allowable charge in addition to any coinsurance amount. Allowable charge is the lesser of the provider’s actual charge or ASH’s In-Network fee schedule for the same services.
Covered at 85% of ASH’s fee schedule Covered at 60% of ASH’s fee schedule
56

ADMINISTERED BY SENTARA HEALTH PLANS, INC.Plus2080p_0114
Other Covered ServicesOther Covered Services OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Diabetic Supplies and Equipment Includes FDA approved equipment and supplies for the treatment of diabetes and in-person outpatient self-management training and education including medical nutrition therapy.
Insulin, syringes, and needles are covered under the Plan’s Prescription Drug Benefit for the applicable Copayment or Coinsurance per 31 day supply.
An annual diabetic eye exam is covered from an Optima Health Plan Provider, a participating EyeMed Provider, or a Non-Plan Provider at the applicable office visit Copayment or Coinsurance amount.
For more information about how to access this benefit for meters, strips and lancets, please call one of the following providers: Home Care Delivered: 1-800-867-4412 EdgePark Medical Supplies: 1-888-394-5375
You may also call 757-552-7200 or 1-800-SENTARA for information on educational classes.
Blood glucose monitoring equipment and supplies including home glucose monitors, lancets, blood glucose test strips, and insulin pump infusion sets if prescribed by your physician: Covered at 100%
Insulin pumps: Covered at 100%.
Outpatient self-management training and education, including medical nutritional therapy: Covered at 100%
Blood glucose monitoring equipment and supplies including home glucose monitors, lancets, blood glucose test strips, and insulin pump infusion sets if prescribed by your physician: Covered at 60%
Insulin pumps: Covered at 60%.
Outpatient self-management training and education, including medical nutritional therapy: Covered at 60%
Durable Medical Equipment (DME) and Supplies7
Orthopedic Devices and Prosthetic Appliances7 Pre-Authorization is required for single items over $750.6
Pre-Authorization is required for all rental items.6
Pre-Authorization is required for repair and replacement.6
Covered Services include durable medical equipment, orthopedic devices, prosthetic appliances other than artificial limbs, colostomy, ileostomy and tracheostomy supplies, suction and urinary catheters, and repair/replacement.
After Deductible Covered at 85% After Deductible Covered at 60%
Early Intervention Services Pre-Authorization is required.6
Covered for Dependents from birth to age three who are certified as eligible by the Virginia Department of Behavioral Health and Developmental Services.
Covered Services include: Medically Necessary speech and language therapy, occupational therapy, physical therapy and assistive technology services and devices.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of service.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of service.
57

ADMINISTERED BY SENTARA HEALTH PLANS, INC.Plus2080p_0114
Other Covered ServicesOther Covered Services OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Family Planning Depo-Provera Injection:
Lunelle Injection:
Tubal Ligation: Pre-authorization required
Vasectomy:
Covered at 100%
Covered at 100%
Covered at 100%
After Deductible Covered at 100%
Subject to any applicable outpatient/inpatient surgery copayment
After Deductible Covered at 60%
After Deductible Covered at 60%
After Deductible Covered at 60%
After Deductible Covered at 60%
Subject to any applicable outpatient/inpatient surgery copayment
Hearing Aid Rider Pre-Authorization is required.6
The following services are covered up to the annual maximum benefit of $1,250 :
the hearing aid(s);audiometric specialist office visits for fitting,
including molds and dispensing; repair, replacement or refurbishment of the
hearing aid(s) Replacement is covered only every 36 months from date of acquisition. Batteries are not covered. Supplies are not covered.
After Deductible $40 Copayment per visit
After Deductible Covered at 60%
Home Health Care Skilled Services7
Pre-Authorization is required.6
Services are covered up to a maximum combined benefit with In-Network and Out-of-Network benefits of 100 visits per calendar year for Members who are home bound, and in the Plan’s judgment require Home Health Skilled Services.7
You will pay a separate outpatient therapy Copayment or Coinsurance amount for physical, occupational, and speech therapy visits received at home. Therapy visits received at home will count toward Your Plan’s annual outpatient therapy benefit limits.
You will pay a separate outpatient rehabilitation services Copayment or Coinsurance amount for cardiac, pulmonary, vascular, and vestibular rehabilitation visits received at home. Rehabilitation visits received at home will count toward Your Plan’s annual outpatient rehabilitation benefit limits.
After Deductible Covered at 85% After Deductible Covered at 60%
Hospice Care Pre-Authorization is required.6
After Deductible Covered at 85% After Deductible Covered at 60%
58

ADMINISTERED BY SENTARA HEALTH PLANS, INC.Plus2080p_0114
Other Covered ServicesOther Covered Services OPTIMA NETWORK / PHCS NETWORK
Copayment/Coinsurance2OUT-OF-NETWORK
Copayment/Coinsurance2
Vision Care and Materials 7
Optima Health contracts with EyeMed Vision Care to administer this benefit.
Coverage includes one examination every 12 months when done by a participating EyeMed Provider.
To locate a participating EyeMed provider, please call 1-888-610-2268 or visit www.optimahealth.com.
Medical conditions related to the eye, such as glaucoma, are covered under the medical plan.
Spectacle Exam: $20 Copayment then covered at 100% OR
Contact Lens Exam: $40 Copayment then covered at 100%
Limited to one exam every 12 months (from the date of last exam) by a participating EyeMed Provider
Materials – By a participating EyeMed Provider: Lenses (single vision, bifocal, trifocal) covered in full. Frames: Covered in full up to $100 retail Contact Lenses (in lieu of glasses) covered in full up to $95 retail.
If you choose contact lenses when they are not medically indicated, you will receive an allowance of $95 toward the purchase price. (Contact lenses are deemed medically necessary following cataract surgery, to correct extreme visual acuity problems not correctable with spectacle lenses, or if you have certain conditions of anisometropia or keratoconus). If contact lenses are obtained, they are in lieu of spectacles.
For eye examinations from Out-of-Network providers, Members will be reimbursed up to $40 for an eye examination only every 12 months (from date of last exam).
No coverage for eyeglasses/contacts out-of-network.
Telemedicine Services Telemedicine Services means the use of interactive audio, video, or other electronic media used for the purpose of diagnosis, consultation, or treatment. Telemedicine services do not include an audio-only telephone, electronic mail message, or facsimile transmission.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of treatment or service. Your out-of-pocket deductible, copayment, or coinsurance amounts will not exceed the deductible, copayment or coinsurance amount You would have paid if the same services were provided through face-to-face diagnosis, consultation, or treatment.
59

Premier POSOutpatient Prescription Drug Rider Schedule of Benefits
ADMINISTERED BY SENTARA HEALTH PLANS, INC.
This schedule of benefits describes Your outpatient prescription drug coverage. All drugs must be Food and DrugAdministration (FDA) approved and you must have a prescription. You will need to pay Your Copayment or Coinsurancewhen you fill your prescription at the pharmacy. If Your Plan has a Deductible you must meet that amount before yourcoverage begins. Some drugs require Pre-Authorization by Your Physician, and some quantities may be limited. Your drugcoverage has specific Exclusions and Limitations, so please read the next few pages carefully. Optima Health’s Pharmacyand Therapeutics Committee places covered drugs into the following Tiers. You will pay Your Copayment or Coinsurancedepending on which Tier Your Drug is in.
This Plan has a closed formulary and covers a specific list of drugs and medications. Drugs not included on the Plan’s formulary will be excluded from coverage.
Selected Generic (Tier 1) includes commonly prescribed generic drugs. Other drugs may be included in Tier 1if the Plan recognizes they show documented long-term decreases in illness.
Selected Brand & Other Generic (Tier 2) includes brand-name drugs, and some generic drugs with highercosts than Tier 1 generics, that are considered by the Plan to be standard therapy.
Non-Selected Brand (Tier 3) includes brand name drugs not included by the Plan on Tier 1 or Tier 2. Thesemay include single source brand name drugs that do not have a generic equivalent or a therapeutic equivalent.Drugs on this tier may be higher in cost than equivalent drugs, or drugs determined to be no more effective thanequivalent drugs on lower tiers.
Specialty Drugs (Tier 4) includes those drugs classified by the Plan as Specialty Drugs. Tier 4 also includescovered compound prescription medications. Specialty Drugs have unique uses and are generally prescribedfor people with complex or ongoing medical conditions. Specialty Drugs typically require special dosing,administration, and additional education and support from a health care professional. Specialty Drugs includethe following:
Medications that treat certain patient populations including those with rare diseases;
Medications that require close medical and pharmacy management and monitoring;
Medications that require special handling and/or storage;
Medications derived from biotechnology and/or blood derived drugs or small molecules; and
Medications that can be delivered via injection, infusion, inhalation, or oral administration.
Specialty Drugs are only available through Proprium Pharmacy at 757-553-3568 or 1-855-553-3568 (toll free). Specialty Drugs will be delivered to Your home address from Our Specialty mail order pharmacy. If You have a question or need to find out if Your drug is considered a Specialty Drug please call Member Services at thenumber on Your Optima Health ID Card. You can also log onto optimahealth.com for a list of Specialty Drugs.
A compound prescription medication is used to meet the needs of a specific individual and must have at leastone ingredient requiring a physician’s authorization by State or Federal Law. Compound prescriptions canusually be filled at Your local pharmacy.
Your Copayment, Coinsurance, and Deductible amounts for each Tier are listed on the following page. Your MaximumOut-of-Pocket Amount is also listed. If You need help please call Member Services or log on to optimahealth.com to findout which of the following Tiers Your drug is in.
60

Premier POSOutpatient Prescription Drug Rider Schedule of Benefits
ADMINISTERED BY SENTARA HEALTH PLANS, INC.
Maximum Out-of-Pocket LimitMaximum Out-of-Pocket Limit
Outpatient Prescription Drug Copayments or Coinsurance apply to the Plan’s Maximum MedicalOut-of-Pocket LimitAncillary charges which result from a request for a brand name outpatient prescription drug whena generic drug is available are not Covered, do not count toward the Plan’s Maximum Out-of-Pocket Limit and must continue to be paid after the maximum out-of-pocket Limit has been met.
Non-Preferred Pharmacy (all retail other than Walgreens, Walmart or Sam’s Club). You may purchase up to a 30-day supply.Selected Generic (Tier 1) $25 Copayment (or the plan’s negotiated cost of the drug, if less)Selected Brand & Other Generic (Tier 2) $45 Copayment (or the plan’s negotiated cost of the drug, if less)Non-Selected Brand (Tier 3) Covered at 75% (maximum $75)
Specialty Drugs (Tier 4) Covered at 75% (maximum $200)
Mail Order Pharmacy Benefit Copayments and CoinsurancesSome Outpatient prescription drugs are available through the Plan’s Mail Order Provider. This does not include Tier4 Specialty Drugs. You may call OptumRx Home Delivery at 866-244-9113 to find out if a drug is available. If Yourdrug is available You may purchase up to a 90-day supply for the Copayment or Coinsurance amount.Selected Generic (Tier 1) $25 Copayment (or the plan’s negotiated cost of the drug, if less)Selected Brand & Other Generic (Tier 2) $60 Copayment (or the plan’s negotiated cost of the drug, if less)Non-Selected Brand (Tier 3) Covered at 75% (maximum $125)Specialty Drugs (Tier 4) No 90 day mail order benefits are available for Tier 4 Specialty Drugs
Non-formulary requests. You have the right to request a non-formulary prescription drug if You believe that You need a prescription drug that is not on the Plan’s list of covered drugs (formulary), or You have been receiving a specific non-formulary prescription drug for at least six months previous to the development or revision of the formulary and Your prescribing physician has determined that the formulary drug is inappropriate for Your condition or that changing drug therapy presents a significant health risk to You. Your physician must complete a medical necessity form and deliver it to the Optima Health pharmacy authorization department. After reasonable investigation and consultation with the prescribing physician, Optima Health will make a determination. Optima Health will act on such requests within one business day of receipt of the request. You will be responsible for all applicable Copayments, Coinsurance, or Deductibles depending upon which Tier a drug is placed in by the Plan.
PREFERRED NETWORK – You will pay a lower Copayment if you fill your prescriptions at a Walgreens, Walmart or Sam’sClub Preferred Pharmacy. You may purchase up to a 90-day supply for 3 Copayments or Coinsurance amounts.Selected Generic (Tier 1) $10 Copayment (or the plan’s negotiated cost of the drug, if less)Selected Brand & Other Generic (Tier 2) $25 Copayment (or the plan’s negotiated cost of the drug, if less)Non-Selected Brand (Tier 3) Covered at 75% (maximum $50)
Copayments and CoinsurancesFor a single Copayment or Coinsurance charge You may receive up to a consecutive 31-day supply of a covereddrug. A Copayment is a flat dollar amount. A Coinsurance is a percent of Optima Health’s Allowable Charge. Certainprescription drugs will be covered at a generic product level established by the Plan. If a generic product level has beenestablished for a drug and You or Your prescribing Physician requests the brand-name drug or a higher costing generic, Youmust pay the difference between the cost of the dispensed drug and the generic product level in addition to the Copaymentcharge (not to exceed $150 per each 31-day supply prescription).
61

ADMINISTERED BY SENTARA HEALTH PLANS, INC.Plus2080p_0114
The Covered Services herein are subject to the terms and conditions set forth in the Plan Document. Words that are capitalized are defined terms listed in the Definitions section of the Plan Document. Optima Health has an internal claims appeal process and an external review process. Please look in Your Plan Document for details about how to file a complaint or an appeal. Under certain circumstances Your coverage can be terminated. However, Your Coverage can only be rescinded for fraud or intentional misrepresentation of material fact. Please look in Your Plan Document in the section on When Your Coverage Will End. For Optima Health plans that require that You choose a primary care provider (PCP), You have the right to choose any PCP who participates in our network and who is available to accept new patients. For children, You may choose a pediatrician as the PCP.
1. You or Your means the Subscriber and each family member who is a Covered Person under the Plan.
2. Copayment and Coinsurance are out of pocket amounts You pay directly to a Provider for a Covered Service. A Copayment is aflat dollar amount. A Coinsurance is a percent of Optima Health’s Allowable Charge (AC) for the Covered Service You receive.
Allowable Charge is the amount the Plan determines will be paid to a Provider for a Covered Service. When You useIn-Network benefits the Allowable Charge is the lesser of: (1) the Provider’s contracted rate with the Plan or its third partyadministrator or (2) the Provider’s actual charge for the Covered Service. When You use an Out-of-Network Provider, theAllowable Charge is the lesser of the usual and customary charge for the service as determined by the Plan or the actualcharge.
Medically Necessary Covered Services provided by a Non-Plan Provider during an Emergency, or during an authorizedAdmission to a Plan Facility, will be Covered under In-Network benefits. All other Covered Services received from Non-PlanProviders will be Covered under Your Out of Network benefits.
When You use Out-of Network benefits from Non-Plan Providers Allowable Charge may be a negotiated rate; or if there is nonegotiated rate Allowable Charge is Optima Health’s In-Network contracted rate for the same service performed by the sametype of Provider or the Provider’s actual charge for the service, whichever is less. Non-Plan Providers may not accept thisamount as payment in full. If You use a Non-Plan Provider who charges more than our allowable amount the Provider maybalance bill You for the difference. You will have to pay the difference to the Provider in addition to Your Copayment orCoinsurance amount. Charges from Non-Plan Providers will be higher than the Plan’s Allowable Charge so You will usuallypay more out of pocket when You use Out of Network benefits.
3. Deductible means the dollar amount You must pay out of pocket each calendar year for Covered Services before the Planbegins to pay for Your benefits. Your Plan may have different Deductibles to meet for In Network Covered Services and for Outof Network Covered Services. Amounts applied to an In Network Deductible will apply toward the Plan’s In Network MaximumOut of Pocket Limit. Amounts applied to an Out of Network Deductible will apply toward the Plan’s Out of Network MaximumOut of Pocket Limit. Amounts which You are required to pay for outpatient prescription drugs, preventive vision, or visionmaterials, will not be applied to any Deductible amount in the Plan. Deductibles will not be reimbursed under the Plan. Anypart of the calendar year Deductible that is satisfied in the last three months of a calendar year can be carried forward to thenext calendar year.
4. Maximum Out of Pocket Limit for In-Network Benefits means the total dollar amount You pay out of pocket for mostIn-Network Covered Services during a calendar year. Your Plan has a separate out of pocket limit for Covered Services Youreceive under the Plan’s Out of Network Benefits. Copayments and Coinsurance amounts that You pay for most In-NetworkCovered Services will count toward Your In-Network Maximum Out of Pocket Limit. If a service does not count toward YourMaximum Out of Pocket Limit You must continue to pay Your Copayments, Coinsurance and any other charges for theseservices after Your Maximum Out of Pocket Limit has been met. Copayments, Coinsurance, or any other charges for thefollowing will not count toward Your In-Network Maximum Out of Pocket Limit:
1) Amounts You pay for services not covered under Your Plan;2) Amounts You pay for Out of Network Benefits;3) Amounts You pay for Vision care;4) Amounts You pay for any benefits covered under a plan rider;5) Amounts You pay for Reduction Mammoplasty benefits, except for procedures associated with reconstructive breast
surgery following mastectomy;6) Ancillary charges which result from Your request for a brand name outpatient prescription drug when a generic drug is
available. Ancillary charges are not Covered Services;7) Amounts You pay for any services after a benefit limit has been reached;8) Amounts You pay as a penalty for failure to comply with the Plan’s Pre-authorization procedures;9) Amounts applied to Your Out-of-Network Deductible.
Notes
62

ADMINISTERED BY SENTARA HEALTH PLANS, INC.Plus2080p_0114
5. Maximum Out of Pocket Limit for Out-of-Network Benefits means the total dollar amount You will pay during a calendaryear for most Out of Network Covered Services. Your Plan has a separate out of pocket limit for Covered Services Youreceive under the Plan’s In- Network Benefits. Copayments and Coinsurance amounts that You pay for mostOut-of-Network Covered Services will count toward Your Out-of-Network Maximum Out of Pocket Limit. If a service doesnot count toward Your Maximum Out of Pocket Limit You must continue to pay Your Copayments or Coinsurance forthese services after Your Maximum Out of Pocket Limit has been met. Copayments, Coinsurance, or any other chargesfor the following will not count toward Your Out-of-Network Maximum Out of Pocket Limit:
1) Amounts You pay for services not covered under Your Plan;2) Amounts You pay for In- Network Benefits; 3) Amounts You pay for Vision care;4) Amounts You pay for any benefits covered under a plan rider;5) Amounts You pay for Reduction Mammoplasty benefits, except for procedures associated with reconstructive breast
surgery following mastectomy;6) Ancillary charges which result from Your request for a brand name outpatient prescription drug when a generic drug is
available. Ancillary charges are not Covered Services; 7) Amounts You pay for any services after a benefit limit has been reached;8) Amounts You pay as a penalty for failure to comply with the Plan’s Pre-authorization procedures;9) Amounts applied to Your In-Network Deductible;
10) Amounts that exceed the Plan’s Allowable Charge for a Covered Service
6. This benefit requires Pre-Authorization before You receive services. Your benefits for Covered Services may be reduced ordenied if You do not comply with the Plan's Pre-Authorization requirements. The Plan may also apply a penalty of up to$500 to any benefits paid for Covered Services if You do not comply with the Plan’s Pre-Authorization requirements.
7. Coverage for this benefit or service is limited by a dollar amount and/or visit or day limits as stated. Maximum amounts arecombined maximums of both In Network and Out-Of Network Covered Services unless otherwise stated. The Plan will notcover any additional services after the limits have been reached. You will be responsible for payment for all services aftera benefit limit has been reached. Amounts You pay for any services after a benefit limit has been reached areexcluded from Coverage and will not count toward Your Maximum Out of Pocket Maximum Limit.
8. Coverage for obstetrical services as an inpatient in a general hospital or obstetrical services by a physician shall providesuch benefits with durational limits, deductibles, coinsurance factors, and Copayments that are no less favorable than forphysical illness generally. If the Plan charges a Global Copayment for prenatal, delivery, and postpartum services You areentitled to a refund from the Delivering Obstetrician if the total amount of the Global Copayment for prenatal, delivery,and postpartum services is more than the total Copayments You would have paid on a per visit or per procedure basis.
9. All Emergency, Urgent Care, Ambulance, and Emergency Mental/Behavioral Health Services may be subject toRetrospective Review to determine the Plan’s responsibility for payment. If the Plan determines that the condition treatedwas not an Emergency Service, the Plan will have no responsibility for the cost of the treatment and You will be solelyresponsible for payment. Members who receive Emergency Services from Non-Plan Providers may be responsible forcharges in excess of what would have been paid had the Emergency Services been received from Plan Providers. In noevent will the Plan be responsible for payment for services from Non-Plan Providers where the service would not have beencovered had the member received care from a Plan Provider.
10. Preventive Care includes recommended preventive care services under the Patient Protection and Affordable Care Act(PPACA) listed below. You may be responsible for an office visit copayment or coinsurance when you receive preventivecare. Some services may be administered under Your prescription drug benefit under the Plan.
1) Evidence-based items or services that have in effect a rating of A or B in the recommendations of the U.S.Preventive Services Task Force as of September 23, 2010, with respect to the individual involved;
2) Immunizations for routine use in children, adolescents, and adults that have in effect a recommendation from theAdvisory Committee on Immunization Practices of the Centers for Disease Control and Prevention with respect to theindividual involved. For purposes of this subdivision, a recommendation from the Advisory Committee on ImmunizationPractices of the Centers for Disease Control and Prevention is considered in effect after it has been adopted by theDirector of the Centers for Disease Control and Prevention, and a recommendation is considered to be for routine useif it is listed on the Immunization Schedules of the Centers for Disease Control and Prevention;
3) With respect to infants, children, and adolescents, evidence-informed preventive care and screenings in theRecommendations for Preventive Pediatric Health by the American Academy of Pediatrics and the RecommendedUniform Screening Panels by the Secretary's Advisory Committee on Heritable Disorders in Newborns and Children;and
63

ADMINISTERED BY SENTARA HEALTH PLANS, INC.Plus2080p_0114
4) With respect to women, evidence-informed preventive care and screenings recommended in comprehensive guidelinessupported by the Health Resources and Services Administration. Services include well-woman visits, screening forgestational diabetes, human papillomavirus, testing (HPV), counseling for sexually transmitted infections, counseling andscreening for human immunodeficiency virus (HIV), FDA-approved contraception methods, sterilization procedures,and patient education and counseling for women, breastfeeding support, supplies, and counseling,screening and counseling for interpersonal and domestic violence.
11. You do not need prior authorization from Optima Health or from any other person (including a Primary Care Provider) inorder to obtain access to obstetrical or gynecological care from a health care professional in our network who specializes inobstetrics or gynecology. The health care professional, however, may be required to comply with certain procedures,including obtaining prior authorization for certain services, following a pre-approved treatment plan, or procedures formaking referrals. Look in Your Plan Document in the Utilization Management section for more information on Pre-Authorization.
64

OOptima Health
Point of Service (POS)
STANDARD PLAN
65

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
OPTIMA POINT OF SERVICE (POS) STANDARD 2019 Summary of Benefits
City of Virginia Beach & Virginia Beach City Public SchoolsThis document is not a contract or policy with Optima Health. It is a summary of benefits and services available through the Plan. If there are any differences between this summary and the employer group Plan Document, the provisions of those documents will prevail for all benefits, conditions, limitations and exclusions. This plan is a Qualified High Deductible plan compatible with a Health Savings Account.
Deductibles, Maximum Out-of-Pocket LimitsOptima Network/PHCS Network Out-of-Network
Deductibles per Calendar Year3 $1,350 Employee only coverage $2,700 per Family
$2,600 Employee only coverage $5,200 per Family
Maximum Out-of-Pocket Limit per Calendar Year
$3,500 Employee only coverage
$7,000 Family4$5,500 Employee only coverage5
$11,000 per Family 5
Physician ServicesIncludes Covered Services performed in the Physician’s office during the Physician office visit. Includes, but is not limited to, office consults and exams; In-office surgery; In-office lab, x-ray, injections, and diagnostic and treatment services. Family planning services including injectables and vasectomy; Physical, Occupational, and Speech Therapy; Cardiac, Pulmonary, and Vascular Rehabilitation Services; Chemo, Radiation, IV, and Respiratory therapy services; Dialysis treatments. Pre-Authorization is required for in-office surgery6.Physician Office Visits Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
MDLIVE Services After Deductible Covered at 90% Not applicable
Sentara Quality Care Network (SQCN) Primary Care Physician (PCP) Office Visit SQCN providers are currently available in Hampton Roads, Charlottesville and Rockingham zip codes only. Members who do not reside in those areas will pay the SQCN provider coinsurance.
Non-Sentara Quality Care Network (SQCN) Primary Care Physician (PCP) Office Visit
After Deductible Covered at 90%
After Deductible Covered at 80%
After Deductible Covered at 50%
Sentara Quality Care Network (SQCN) Specialist Office Visit SQCN providers are currently available in Hampton Roads, Charlottesville and Rockingham zip codes only. Members who do not reside in those areas will pay the SQCN provider coinsurance.
Non-Sentara Quality Care Network (SQCN) Specialist Office Visit
After Deductible Covered at 90%
After Deductible Covered at 80%
After Deductible Covered at 50%
Physician ServicesPreventive Care10 Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Routine Annual Physical Exams Well Baby Exams Annual GYN Exams and Pap Smears11 PSA Tests Colorectal Cancer Tests Routine Adult and Childhood Immunizations Screening Colonoscopy Screening Mammograms (including 3-D mammograms) Women’s Preventive Services
Covered at 100% After Deductible Covered at 50%
66

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Outpatient Therapy and Rehabilitation ServicesShort Term Therapy Services7 Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Physical Therapy Occupational Therapy Pre-Authorization is required.6
Physical and Occupational Therapy are limited to a maximum combined benefit with In-Network and Out-of-Network benefits and for all places of service of 30 visits per calendar year.7 Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 80% After Deductible Covered at 50%
Speech Therapy Pre-Authorization is required.6
Speech Therapy is limited to a maximum combined benefit with In-Network and Out-of- Network benefits and for all places of service of 30 visits per calendar year.7 Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 80% After Deductible Covered at 50%
Short Term Rehabilitation Services7 Optima Network/PHCS Network Copayment/Coinsurance2
Out-of-Network Copayment/Coinsurance2
Cardiac Rehabilitation Pulmonary Rehabilitation Vascular Rehabilitation Vestibular Rehabilitation Pre-Authorization is required.6
Services are limited to a maximum combined benefit with In-Network and Out-of-Network benefits and for all places of service of 30 visits per calendar year.7 Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 80% After Deductible Covered at 50%
Other Outpatient Treatments Optima Network/PHCS Network Copayment/Coinsurance2
Out-of-Network Copayment/Coinsurance2
Chemotherapy Radiation Therapy IV Therapy Inhalation Therapy
After Deductible covered at 80% After Deductible covered at 50%
Outpatient Therapy and Rehabilitation ServicesOther Outpatient Treatments Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Pre-Authorized Injectable and Infused Medications Includes injectable and infused medications, biologics, and IV therapy medications that require prior authorization. Coinsurance applies when medications are provided in a Physician’s office, outpatient facility, or in the Member’s home as part of Skilled Home Health Care Services benefit. Coinsurance is in addition to any applicable office visit or outpatient facility Copayment or Coinsurance.
After Deductible Covered at 80% After Deductible Covered at 50%
67

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Outpatient Dialysis ServicesOutpatient Dialysis Services Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Dialysis Services Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 80% After Deductible Covered at 50%
Outpatient SurgeryOutpatient Surgery Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Outpatient Surgery Pre-Authorization is required.6
Coinsurance or Copayment applies to services provided in a free-standing ambulatory surgery center or hospital outpatient surgical facility.
After Deductible Covered at 80% After Deductible Covered at 50%
Outpatient Diagnostic ProceduresCopayment or Coinsurance will apply when a procedure is performed in a free-standing outpatient facility or lab, or a hospital outpatient facility or lab.Outpatient Diagnostic Procedures Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Outpatient Diagnostic Procedures After Deductible Covered at 80% After Deductible Covered at 50%Outpatient X-Ray Ultrasound Doppler Studies
After Deductible Covered at 80% After Deductible Covered at 50%
Outpatient Lab Work After Deductible Covered at 80% After Deductible Covered at 50%Outpatient Advanced Imaging and Testing Procedures
Outpatient Advanced Imaging and Testing Procedures Optima Network/PHCS Network Copayment/Coinsurance2
Out-of-Network Copayment/Coinsurance2
Magnetic Resonance Imaging (MRI) Magnetic Resonance Angiography (MRA) Positron Emission Tomography (PET Scans) Computerized Axial Tomography (CT Scans) Computerized Axial Tomography Angiogram (CTA Scans) Sleep Studies Pre-Authorization is required.6
Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 80% After Deductible Covered at 50%
Maternity CareMaternity Care Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Maternity Care 8,10,11
Pre-Authorization is required for prenatal services.6
Includes prenatal, delivery, postnatal, postpartum services, and home health visits. Copayment or Coinsurance is in addition to any applicable inpatient hospital Copayment or Coinsurance. Sentara Quality Care Network (SQCN) SQCN providers are currently available in Hampton Roads, Charlottesville and Rockingham zip codes only. Members who do not reside in those areas will pay the SQCN provider coinsurance.
Non-Sentara Quality Care Network (SQCN)
After Deductible Covered at 90%
After Deductible Covered at 80%
After Deductible Covered at 50%
68

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Inpatient ServicesInpatient Services Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Inpatient Hospital Services Pre-Authorization is required.6
Transplants are covered at contracted facilities only.
After Deductible Covered at 80% After Deductible Covered at 50%
Skilled Nursing Facilities/Services7
Pre-Authorization is required.6
Following inpatient hospital care or in lieu of hospitalization. Covered Services include up to 100 days combined in and out-of-network per calendar year that in the Plan’s judgment requires Skilled Nursing Facility Services.7
After Deductible Covered at 80% After Deductible Covered at 50%
Ambulance ServicesAmbulance Services Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Ambulance Services9
Pre-Authorization is required for non-emergent transportation only.6
Includes air and ground ambulance for emergency transportation, or non-emergent transportation that is Medically Necessary and Pre-Authorized by the Plan. Copayment or Coinsurance is applied per transport each way.
After Deductible Covered at 80% *If transported by a Virginia BeachVolunteer Rescue Squad – Covered at 100%
After Deductible Covered at 80%
Emergency ServicesEmergency Services Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Emergency Services9
Pre-Authorization is not required. Includes Emergency Services, Physician, and Ancillary Services provided in an emergency department facility. Coinsurance waived for facility charges if admitted. Inpatient copayment / coinsurance will apply if admitted.
After Deductible Covered at 80% After Deductible Covered at 80%
Urgent Care Center ServicesUrgent Care Center Services Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Urgent Care Services9
Pre-Authorization is not required. Includes Urgent Care Services, Physician services, and other Ancillary Services received at an Urgent Care facility. If You1 are transferred to an emergency department from an Urgent Care center, You1 will pay an Emergency Services Copayment or Coinsurance.
After Deductible Covered at 80% After Deductible Covered at 50%
69

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Mental/Behavioral Health CareIncludes inpatient and outpatient services for the treatment of mental health and substance abuse. Also includes services for Biologically Based Mental Illnesses for the following diagnoses: schizophrenia, schizoaffective disorder, bipolar disorder, major depressive disorder, panic disorder, obsessive-compulsive disorder, attention deficit hyperactivity disorder, autism, and drug and alcoholism addiction.Mental/Behavioral Health Care Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Inpatient Services Pre-Authorization is required.6
Residential treatment is not covered.
After Deductible Covered at 80% After Deductible Covered at 50%
Sentara Quality Care Network (SQCN) Outpatient Office Visits Pre-Authorization may be required.6
SQCN providers are currently available in Hampton Roads, Charlottesville and Rockingham zip codes only. Members who do not reside in those areas will pay the SQCN provider coinsurance.
Non-Sentara Quality Care Network (SQCN) Outpatient Office Visits Pre-Authorization may be required.6
After Deductible Covered at 90%
After Deductible Covered at 80%
After Deductible Covered at 50%
Other Outpatient Visits (Includes Hospital Outpatient and Freestanding Outpatient Centers) Pre-Authorization may be required.6
After Deductible Covered at 80% After Deductible Covered at 50%
Other Covered ServicesOther Covered Services Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Allergy Care Includes Allergy testing, Injections, Serum and RAST testing.
After Deductible Covered at 80% After Deductible Covered at 50%
70

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Other Covered ServicesOther Covered Services Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Autism Spectrum Disorder Pre-Authorization is required.6 Covered Services include “diagnosis” and “treatment” of Autism Spectrum Disorder in children from age two through 10.
“Autism Spectrum Disorder” means any pervasive developmental disorder, including (i) autistic disorder, (ii) Asperger’s Syndrome, (iii) Rett syndrome, (iv) childhood disintegrative disorder, or (v) Pervasive Developmental Disorder – Not Otherwise Specified, as defined in the most recent edition of the Diagnostic and Statistical Manual of Mental Disorders of the American Psychiatric Association.
“Diagnosis of autism spectrum disorder” means medically necessary assessments, evaluations, or tests to diagnose whether an individual has an autism spectrum disorder.
“Treatment for autism spectrum disorder” shall be identified in a treatment plan and includes the following care prescribed or ordered for an individual diagnosed with autism spectrum disorder by a licensed physician or a licensed psychologist who determines the care to be medically necessary: (i) behavioral health treatment, (ii) pharmacy care, (iii) psychiatric care, (iv) psychological care, (v) therapeutic care, and (vi) applied behavioral analysis when provided or supervised by a board certified behavioral analyst licensed by the Board of Medicine.
“Applied behavioral analysis” means the design, implementation, and evaluation of environmental modifications, using behavioral stimuli and consequences, to produce socially significant improvement in human behavior, including the use of direct observation, measurement, and functional analysis of the relationship between environment and behavior. Coverage for applied behavioral analysis under this benefit is limited to an annual maximum benefit of $35,000.6
Coverage for Autism Spectrum Disorder will not be subject to any visit limits, and will be neither different nor separate from coverage for any other illness, condition, or disorder for purposes of determining Deductibles, lifetime dollar limits, Copayment and Coinsurance factors, and benefit year maximum for Deductibles and Copayment and Coinsurance factors.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of treatment or service listed on the Summary of Benefits.
Coverage for Autism Spectrum Disorder will not be subject to any visit limits, and will be neither different nor separate from coverage for any other illness, condition, or disorder for purposes of determining Deductibles, lifetime dollar limits, Copayment and Coinsurance factors, and benefit year maximum for Deductibles and Copayment and Coinsurance factors.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of treatment or service listed on the Summary of Benefits.
71

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Other Covered ServicesOther Covered Services Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Prosthetic Limbs and Components7 Pre-Authorization is required.6
Services include coverage for medically necessary prosthetic devices. This also includes repair, fitting, replacement and components.
Definitions: “Component” means the materials and equipment needed to ensure the comfort and functioning of a prosthetic device. “Limb” means an arm, a hand, a foot, or any portion of an arm, hand, a leg or foot. “Prosthetic device” means an artificial device to replace, in whole or in part, a limb. Prosthetic device coverage does not mean or include repair and replacement due to enrollee neglect, misuse, or abuse. Coverage also does not mean or include prosthetic devices designed primarily for an athletic purpose.
After Deductible Covered at 80% After Deductible Covered at 50%
Chiropractic Care7
Optima Health contracts with American Specialty Health Networks (ASHN) to administer this benefit6. Pre-Authorization is required by ASHN for all chiropractic care services. 6
To receive services, contact ASHN's Member Services at 1-800-678-9133. Representatives are available from 8:00 AM to 9:00 PM Monday-Friday. Coverage is limited to a combined maximum benefit with in and out-of-network benefits of 30 visits per Person, per calendar year. This benefit also includes coverage of Chiropractic appliances up to a combined maximum benefit with in-and out-of-network benefits of 1 appliance per Person per calendar year when medically necessary.
For providers not in the ASHN network the Member will be responsible for payment of all charges in excess of ASHN’s allowable charge in addition to any coinsurance amount. Allowable charge is the lesser of the provider’s actual charge or ASHN’s in-network fee schedule for the same services.
After Deductible Covered at 80% of ASHN fee schedule
After Deductible Covered at 50 % of ASHN fee schedule
72

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Other Covered ServicesOther Covered Services Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Diabetic Supplies and Equipment Includes FDA approved equipment and supplies for the treatment of diabetes and in-person outpatient self-management training and education including medical nutrition therapy.
Insulin, syringes, and needles are covered under the Plan’s Prescription Drug Benefit for the applicable Copayment or Coinsurance per 31 day supply.
An annual diabetic eye exam is covered from an Optima Health Plan Provider, a participating EyeMed Provider, or a Non-Plan Provider at the applicable office visit Copayment or Coinsurance amount.
For more information about how to access this benefit for meters, strips and lancets, please call one of the following providers:
Home Care Delivered at 1-800-867-4412 EdgePark Medical Supplies at 1-888-394-5375
You may also call 552-7200 or 1-800-SENTARA for information on educational classes.
Blood glucose monitoring equipment and supplies including home glucose monitors, lancets, blood glucose test strips, and insulin pump infusion sets if prescribed by your physician: After Deductible Covered at 100%
Insulin pumps: After Deductible covered at 100%
Outpatient self-management training and education, including medical nutritional therapy: After Deductible covered at 100%
Blood glucose monitoring equipment and supplies including home glucose monitors, lancets, blood glucose test strips, and insulin pump infusion sets if prescribed by your physician: After Deductible Covered at 50%
Insulin pumps: After Deductible covered at: 50%
Outpatient self-management training and education, including medical nutritional therapy: After Deductible covered at: 50%
Durable Medical Equipment (DME) and Supplies7
Orthopedic Devices and Prosthetic Appliances7 Pre-Authorization is required for single items over $750.6
Pre-Authorization is required for all rental items.6
Pre-Authorization is required for repair and replacement.6
Covered Services include durable medical equipment, orthopedic devices, prosthetic appliances other than artificial limbs, colostomy, ileostomy, and tracheostomy supplies, suction and urinary catheters, and repair/replacement.
After Deductible Covered at 80% After Deductible Covered at 50%
Early Intervention Services Pre-Authorization is required.6
Covered for Dependents from birth to age three who are certified as eligible by the Virginia Department of Behavioral Health and Developmental Services.
Covered Services include: Medically Necessary speech and language therapy, occupational therapy, physical therapy and assistive technology services and devices.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of service.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of service.
73

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Other Covered ServicesOther Covered Services Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Family Planning Depo-Provera Injection:
Lunelle Injection:
Tubal Ligation: Pre-authorization required
Vasectomy:
Covered at 100%
Covered at 100%
Covered at 100%
After Deductible Covered at 100% Subject to any applicable outpatient/inpatient surgery copayment
After Deductible Covered at 50%
After Deductible Covered at 50%
After Deductible Covered at 50%
After Deductible Covered at 50% Subject to any applicable outpatient/inpatient surgery copayment/coinsurance.
Hearing Aid Rider Pre-Authorization is required.6
The following services are covered up to the annual maximum benefit of $1,250 :
the hearing aid(s);audiometric specialist office visits for fitting,
including molds and dispensing; repair, replacement or refurbishment of the
hearing aid(s) Replacement is covered only every 36 months from date of acquisition. Batteries are not covered. Supplies are not covered.
After Deductible Covered at 80% After Deductible Covered at 50%
Home Health Care Skilled Services7
Pre-Authorization is required.6
Services are covered up to a maximum combined benefit with In-Network and Out-of-Network benefits of 100 visits per calendar year for Members who are home bound, and in the Plan’s judgment require Home Health Skilled Services.7
You will pay a separate outpatient therapy Copayment or Coinsurance amount for physical, occupational, and speech therapy visits received at home. Therapy visits received at home will count toward Your Plan’s annual outpatient therapy benefit limits. You will pay a separate outpatient rehabilitation services Copayment or Coinsurance amount for cardiac, pulmonary, vascular, and vestibular rehabilitation visits received at home. Rehabilitation visits received at home will count toward Your Plan’s annual outpatient rehabilitation benefit limits.
After Deductible Covered at 80% After Deductible Covered at 50%
Hospice Care Pre-Authorization is required.6
After Deductible Covered at 80% After Deductible Covered at 50%
74

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Other Covered ServicesOther Covered Services Optima Network/PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Vision Care and Materials7
Optima Health contracts with EyeMed Vision Care to administer this benefit. Medical conditions related to the eye, such as glaucoma, are covered under the medical plan.
Coverage includes one examination every 12 months when done by a participating EyeMed Provider.
To locate a participating EyeMed provider, please call 1-888-610-2268 or visit www.optimahealth.com.
Spectacle Exam: $20 Copayment then covered at 100% OR
Contact Lens Exam: $40 Copayment then covered at 100%
Limited to one exam every 12 months (from the date of last exam) by a participating EyeMed Provider.
Materials – By a participating EyeMed Provider: Lenses (single vision, bifocal, trifocal) covered in full. Frames: Covered in full up to $100 retail Contact Lenses (in lieu of glasses) covered in full up to $95 retail.
If you choose contact lenses when they are not medically indicated, you will receive an allowance of $95 toward the purchase price. (Contact lenses are deemed medically necessary following cataract surgery, to correct extreme visual acuity problems not correctable with spectacle lenses, or if you have certain conditions of anisometropia or keratoconus). If contact lenses are obtained, they are in lieu of spectacles.
For eye examinations from Out-of-Network providers, Members will be reimbursed up to $40 for an eye examination (once every 12 months from date of last exam).
No coverage for eyeglasses/contacts out-of-network.
Telemedicine Services Telemedicine Services means the use of interactive audio, video, or other electronic media used for the purpose of diagnosis, consultation, or treatment. Telemedicine services do not include an audio-only telephone, electronic mail message, or facsimile transmission.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of treatment or service. Your out-of-pocket deductible, copayment, or coinsurance amounts will not exceed the deductible, copayment or coinsurance amount You would have paid if the same services were provided through face-to-face diagnosis, consultation, or treatment.
75

Standard POSOutpatient Prescription Drug Rider Schedule of Benefits
ADMINISTERED BY SENTARA HEALTH PLANS, INC.
This schedule of benefits describes Your outpatient prescription drug coverage. All drugs must be Food and DrugAdministration (FDA) approved and you must have a prescription. You will need to pay Your Copayment or Coinsurancewhen you fill your prescription at the pharmacy. If Your Plan has a Deductible you must meet that amount before yourcoverage begins. Some drugs require Pre-Authorization by Your Physician, and some quantities may be limited. Your drugcoverage has specific Exclusions and Limitations, so please read the next few pages carefully. Optima Health’s Pharmacyand Therapeutics Committee places covered drugs into the following Tiers. You will pay Your Copayment or Coinsurancedepending on which Tier Your Drug is in.
This Plan has a closed formulary and covers a specific list of drugs and medications. Drugs not included on the Plan’s formulary will be excluded from coverage.
Selected Generic (Tier 1) includes commonly prescribed generic drugs. Other drugs may be included in Tier 1if the Plan recognizes they show documented long-term decreases in illness.
Selected Brand & Other Generic (Tier 2) includes brand-name drugs, and some generic drugs with highercosts than Tier 1 generics, that are considered by the Plan to be standard therapy.
Non-Selected Brand (Tier 3) includes brand name drugs not included by the Plan on Tier 1 or Tier 2. Thesemay include single source brand name drugs that do not have a generic equivalent or a therapeutic equivalent.Drugs on this tier may be higher in cost than equivalent drugs, or drugs determined to be no more effective thanequivalent drugs on lower tiers.
Specialty Drugs (Tier 4) includes those drugs classified by the Plan as Specialty Drugs. Tier 4 also includescovered compound prescription medications. Specialty Drugs have unique uses and are generally prescribedfor people with complex or ongoing medical conditions. Specialty Drugs typically require special dosing,administration, and additional education and support from a health care professional. Specialty Drugs includethe following:
Medications that treat certain patient populations including those with rare diseases;
Medications that require close medical and pharmacy management and monitoring;
Medications that require special handling and/or storage;
Medications derived from biotechnology and/or blood derived drugs or small molecules; and
Medications that can be delivered via injection, infusion, inhalation, or oral administration.
Specialty Drugs are only available through Proprium Pharmacy at 757-553-3568 or 1-855-553-3568 (toll free). Specialty Drugs will be delivered to Your home address from Our Specialty mail order pharmacy. IfYou have a question or need to find out if Your drug is considered a Specialty Drug please call MemberServices at the number on Your Optima Health ID Card. You can also log onto optimahealth.com for alist of Specialty Drugs.
A compound prescription medication is used to meet the needs of a specific individual and must have at leastone ingredient requiring a physician’s authorization by State or Federal Law. Compound prescriptions canusually be filled at Your local pharmacy.
Your Copayment, Coinsurance, and Deductible amounts for each Tier are listed on the following page. Your MaximumOut-of-Pocket Amount is also listed. If You need help please call Member Services or log on to optimahealth.com to findout which of the following Tiers Your drug is in.
76

Standard POSOutpatient Prescription Drug Rider Schedule of Benefits
ADMINISTERED BY SENTARA HEALTH PLANS, INC.
Specialty Drugs (Tier 4) After Deductible Covered at 75% (maximum $200)
Non-Preferred Pharmacy (all retail other than Walgreens, Walmart or Sam’s Club). You may purchase up to a 30-day supply.Selected Generic (Tier 1) After Deductible $25 Copayment (or the plan’s negotiated cost of the drug, if less)Selected Brand & Other Generic(Tier 2)
After Deductible $45 Copayment (or the plan’s negotiated cost of the drug, if less)
Non-Selected Brand (Tier 3) After Deductible Covered at 75% (maximum $75)
PLEASE NOTE: Prescription medications used to prevent any of the following medical conditions are not subject to thedeductible including medications for Hypertension, high cholesterol, diabetes, asthma, osteoporosis, stroke, prenatalnutrient deficiency.
Mail Order Pharmacy Benefit Copayments and CoinsurancesSome Outpatient prescription drugs are available through the Plan’s Mail Order Provider. This does not include Tier4 Specialty Drugs. You may call OptumRx Home Delivery at 866-244-9113 to find out if a drug is available. If Yourdrug is available You may purchase up to a 90-day supply for the Copayment or Coinsurance amount.Selected Generic (Tier 1) After Deductible $25 Copayment (or the plan’s negotiated cost of the drug, if less)Selected Brand & Other Generic(Tier 2)
After Deductible $60 Copayment (or the plan’s negotiated cost of the drug, if less)
Non-Selected Brand (Tier 3) After Deductible Covered at 75% (maximum $125)Specialty Drugs (Tier 4) No 90 day mail order benefits are available for Tier 4 Specialty Drugs
Non-formulary requests. You have the right to request a non-formulary prescription drug if You believe that You need a prescription drug that is not on the Plan’s list of covered drugs (formulary), or You have been receiving a specific non-formulary prescription drug for at least six months previous to the development or revision of the formulary and Your prescribing physician has determined that the formulary drug is inappropriate for Your condition or that changing drug therapy presents a significant health risk to You. Your physician must complete a medical necessity form and deliver it to the Optima Health pharmacy authorization department. After reasonable investigation and consultation with the prescribing physician, Optima Health will make a determination. Optima Health will act on such requests within one business day of receipt of the request. You will be responsible for all applicable Copayments, Coinsurance, or Deductibles depending upon which Tier a drug is placed in by the Plan.
Deductibles and Maximum Out-of-Pocket LimitYou must meet the medical Deductible listed on the Your Plan’s Schedule of Benefits.
Maximum Out-of-Pocket Outpatient Prescription Drug Copayments or Coinsurance apply to the Plan’s Maximum MedicalOut-of-Pocket Limit. Ancillary charges which result from a request for a brand name outpatient prescription drugwhen a generic drug is available are not Covered, do not count toward the Plan’s MaximumOut-of-Pocket Limit and must continue to be paid after the maximum out-of-pocket Limit hasbeen met.
Copayments and CoinsurancesFor a single Copayment or Coinsurance charge You may receive up to a consecutive 31-day supply of a covereddrug. A Copayment is a flat dollar amount. A Coinsurance is a percent of Optima Health’s Allowable Charge. Certainprescription drugs will be covered at a generic product level established by the Plan. If a generic product level has beenestablished for a drug and You or Your prescribing Physician requests the brand-name drug or a higher costing generic, Youmust pay the difference between the cost of the dispensed drug and the generic product level in addition to the Copaymentcharge (not to exceed $150 per each 31-day supply prescription).
PREFERRED NETWORK – You will pay a lower Copayment if you fill your prescriptions at a Walgreens, Walmart or Sam’sClub Preferred Pharmacy. You may purchase up to a 90-day supply for 3 Copayments or Coinsurance amounts.Selected Generic (Tier 1)Selected Brand & Other Generic(Tier 2)Non-Selected Brand (Tier 3)
After Deductible $10 Copayment (or the plan’s negotiated cost of the drug, if less)After Deductible $25 Copayment (or the plan’s negotiated cost of the drug, if less)
After Deductible Covered at 75% (maximum $50)
77

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
The Covered Services herein are subject to the terms and conditions set forth in the Plan Document. Words that are capitalized are defined terms listed in the Definitions section of the Plan Document. Optima Health has an internal claims appeal process and an external review process. Please look in Your Plan Document for details about how to file a complaint or an appeal. Under certain circumstances Your coverage can be terminated. However, Your Coverage can only be rescinded for fraud or intentional misrepresentation of material fact. Please look in Your Plan Document in the section on When Your Coverage Will End. For Optima Health plans that require that You choose a primary care provider (PCP), You have the right to choose any PCP who participates in our network and who is available to accept new patients. For children, You may choose a pediatrician as the PCP.
1. You or Your means the Subscriber and each family member who is a Covered Person under the Plan.
2. Copayment and Coinsurance are out-of-pocket amounts You pay directly to a Provider for a Covered Service. A Copayment is aflat dollar amount. A Coinsurance is a percent of Optima Health’s Allowable Charge (AC) for the Covered Service You receive.
Allowable Charge is the amount the Plan determines will be paid to a Provider for a Covered Service. When You use In-Networkbenefits the Allowable Charge is the lesser of: (1) the Provider’s contracted rate with the Plan or its third party administrator or(2) the Provider’s actual charge for the Covered Service. When You use an Out-of-Network Provider, the Allowable Charge is thelesser of the usual and customary charge for the service as determined by the Plan or the actual charge.
Medically Necessary Covered Services provided by a Non-Plan Provider during an Emergency at a Plan Facility, or during anauthorized Admission to a Plan Facility, will be Covered under In-Network benefits. All other Covered Services received fromNon-Plan Providers will be Covered under Your Out-of-Network benefits.
When You use Out-of Network benefits from Non-Plan Providers the Allowable Charge may be a negotiated rate; or if there is nonegotiated rate the Allowable Charge is Optima Health’s In-Network contracted rate for the same service performed by the sametype of Provider or the Provider’s actual charge for the service, whichever is less. Non-Plan Providers may not accept this amountas payment in full. If You use a Non-Plan Provider who charges more than Optima Health’s allowable amount the Provider maybalance bill You for the difference. You will have to pay the difference to the Provider in addition to Your Copayment orCoinsurance amount. Charges from Non-Plan Providers will be higher than the Plan’s Allowable Charge so You will usually paymore out-of-pocket when You use Out-of-Network benefits.
3. Deductible means the dollar amount You must pay out-of-pocket each calendar year for Covered Services before the Plan beginsto pay for Your benefits. If You have individual coverage You must satisfy the individual member Deductible before Coveragebegins. If You have family coverage You must satisfy the family coverage Deductible. Your Plan has a non-embeddedindividual deductible. Non-embedded means if one covered family member meets the individual member deductible hisor her benefits will not begin until the entire family deductible is satisfied. Once the total family coverage deductible ismet benefits are available for all covered family members. A Plan may have separate individual and family Deductibles forIn-Network Covered Services and for Out-of-Network Services. Deductibles will not be reimbursed under the Plan. TheDeductible does not apply to Preventive Care Visits and Screenings, Preventive Drugs, or Preventive Vision Services and Youare required to pay Your office visit Copayment or Coinsurance only. Amounts applied to Your In-Network Deductible willapply toward Your Plan’s In-Network Maximum Out-of-Pocket Limit. Amounts applied to Your Out-of-Network Deductible will apply toward Your Out-of-Network Maximum Limit. Should the Federal Government adjust the deductible for highdeductible health plans as defined by the Internal Revenue Service, the deductible amount in the Policy will be adjustedaccordingly.
4. Maximum Out-of-Pocket Limit for In-Network Benefits means the total dollar amount You pay out-of-pocket for mostIn-Network Covered Services during a calendar year. Your Plan has a separate out-of-pocket limit for Covered Services Youreceive under the Plan’s Out-of-Network Benefits. Copayments and Coinsurance amounts that You pay for most In-NetworkCovered Services will count toward Your In-Network Maximum Out-of-Pocket Limit. Amounts applied to Your In-NetworkDeductible will apply to Your In-Network Maximum Out-of-Pocket Limit. Copayments or Coinsurance for Outpatient PrescriptionDrug Coverage will count toward Your In-Network Maximum Out-of-Pocket Limit. If a service does not count toward YourMaximum Out-of-Pocket Limit You must continue to pay Your Copayments, Coinsurance and any other charges for theseservices after Your Maximum Out-of-Pocket Limit has been met. Copayments, Coinsurances, or any other charges for thefollowing will not count toward Your In-Network Maximum Out-of-Pocket Limit:
1. Amounts You pay for services not covered under Your Plan;2. Amounts You pay for Out-of-Network Benefits;3. Amounts You pay for Vision care;
Notes
78

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
4. Amounts You pay for any benefits covered under a plan rider;5. Amounts You pay for Reduction Mammoplasty benefits, except for procedures associated with reconstructive
breast surgery following mastectomy;6. Ancillary charges which result from Your request for a brand name outpatient prescription drug when a generic
drug is available. Ancillary charges are not Covered Services;7. Amounts You pay for any services after a benefit limit has been reached;8. Amounts You pay as a penalty for failure to comply with the Plan’s Pre-authorization procedures;9. Amounts applied to Your Out-of-Network Deductible.
5. Maximum Out-of-Pocket Limit for Out-of-Network Benefits means the total dollar amount You will pay during a calendar yearfor most Out-of-Network Covered Services. Your Plan has a separate Out-of-Pocket limit for Covered Services You receive underthe Plan’s In-Network Benefits. Copayments and Coinsurance amounts that You pay for most Out-of-Network Covered Serviceswill count toward Your Out-of-Network Maximum Out-of-Pocket Limit. Amounts applied to Your Out-of-Network Deductible willapply to Your Out-of-Network Maximum Out-of-Pocket Limit. If a service does not count toward Your Maximum Out-of-PocketLimit You must continue to pay Your Copayments or Coinsurance for these services after Your Maximum Out-of-Pocket Limithas been met. Copayments, Coinsurances, or any other charges for the following will not count toward Your Out-of-NetworkMaximum Out-of-Pocket Limit:
1. Amounts You pay for services not covered under Your Plan;2. Amounts You pay for In- Network Benefits;3. Amounts You pay for Vision care;4. Amounts You pay for any benefits covered under a plan rider;5. Amounts You pay for Reduction Mammoplasty benefits, except for procedures associated with reconstructive
breast surgery following mastectomy;6. Ancillary charges which result from Your request for a brand name outpatient prescription drug when a generic
drug is available. Ancillary charges are not Covered Services;7. Amounts You pay for any services after a benefit limit has been reached;8. Amounts You pay as a penalty for failure to comply with the Plan’s Pre-authorization procedures;9. Amounts applied to Your In-Network Deductible;10. Amounts that exceed the Plan’s Allowable Charge for a Covered Service
6. This benefit requires Pre Authorization before You receive services. Your benefits for Covered Services may be reduced ordenied if You do not comply with the Plan's Pre-Authorization requirements. The Plan may also apply a penalty of up to $500 toany benefits paid for Covered Services if You do not comply with the Plan’s Pre-Authorization requirements.
7. Coverage for this benefit or service is limited by a dollar amount and/or visit or day limits as stated. Maximum amounts arecombined maximums of both In-Network and Out-Of Network Covered Services unless otherwise stated. The Plan will not coverany additional services after the limits have been reached. You will be responsible for payment for all services after a benefitlimit has been reached. Amounts You pay for any services after a benefit limit has been reached are excluded from Coverage andwill not count toward Your Maximum Out-of-Pocket Maximum Limit.
8. Coverage for obstetrical services as an inpatient in a general hospital or obstetrical services by a physician shall provide suchbenefits with durational limits, deductibles, coinsurance factors, and Copayments that are no less favorable than for physicalillness generally. If the Plan charges a Global Copayment for prenatal, delivery, and postpartum services You are entitled to arefund from the Delivering Obstetrician if the total amount of the Global Copayment for prenatal, delivery, and postpartumservices is more than the total Copayments You would have paid on a per visit or per procedure basis.
9. All Emergency, Urgent Care, Ambulance, and Emergency Mental/Behavioral Health Services may be subject to RetrospectiveReview to determine the Plan’s responsibility for payment. If the Plan determines that the condition treated was not anEmergency Service, the Plan will have no responsibility for the cost of the treatment and You will be solely responsible forpayment. Members who receive Emergency Services from Non-Plan Providers may be responsible for charges in excess of whatwould have been paid had the Emergency Services been received from Plan Providers. In no event will the Plan be responsiblefor payment for services from Non-Plan Providers where the service would not have been covered had the member receivedcare from a Plan Provider.
10. Preventive Care includes recommended preventive care services under the Patient Protection and Affordable Care Act (PPACA)listed below. You may be responsible for an office visit copayment or coinsurance when you receive preventive careOut-of-Network. Some services may be administered under Your prescription drug benefit under the Plan.
1. Evidence-based items or services that have in effect a rating of A or B in the recommendations of the U.S.Preventive Services Task Force as of September 23, 2010, with respect to the individual involved;
79

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
2. Immunizations for routine use in children, adolescents, and adults that have in effect a recommendation from theAdvisory Committee on Immunization Practices of the Centers for Disease Control and Prevention with respect tothe individual involved. For purposes of this subdivision, a recommendation from the Advisory Committee onImmunization Practices of the Centers for Disease Control and Prevention is considered in effect after it has beenadopted by the Director of the Centers for Disease Control and Prevention, and a recommendation is consideredto be for routine use if it is listed on the Immunization Schedules of the Centers for Disease Control andPrevention;
3. With respect to infants, children, and adolescents, evidence-informed preventive care and screenings in theRecommendations for Preventive Pediatric Health by the American Academy of Pediatrics and the RecommendedUniform Screening Panels by the Secretary's Advisory Committee on Heritable Disorders in Newborns andChildren; and
4. With respect to women, evidence-informed preventive care and screenings recommended in comprehensiveguidelines supported by the Health Resources and Services Administration. Services include well-woman visits,screening for gestational diabetes, human papillomavirus, testing (HPV), counseling for sexually transmittedinfections, counseling and screening for human immunodeficiency virus (HIV), FDA-approved contraceptionmethods, sterilization procedures, and patient education and counseling for women, breastfeeding support,supplies, and counseling, screening and counseling for interpersonal and domestic violence.
11. You do not need prior authorization from Optima Health or from any other person (including a Primary Care Provider) in order toobtain access to obstetrical or gynecological care from a health care professional in our network who specializes in obstetrics orgynecology. The health care professional, however, may be required to comply with certain procedures, including obtaining priorauthorization for certain services, following a pre-approved treatment plan, or procedures for making referrals. Look inYour Plan Document in the Utilization Management section for more information on pre-authorization.
80

OOptima Health
Point of Service (POS)
BASIC PLAN
81

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
OPTIMA POINT OF SERVICE (POS) BASIC 2019 Summary of Benefits
City of Virginia Beach & Virginia Beach City Public SchoolsThis document is not a contract or policy with Optima Health. It is a summary of benefits and services available through the Plan. If there are any differences between this summary and the employer group Plan Document, the provisions of those documents will prevail for all benefits, conditions, limitations and exclusions. This plan is a Qualified High Deductible plan compatible with a Health Savings Account.
Deductibles, Maximum Out-of-Pocket LimitsOptima Network / PHCS Network Out-of-Network
Deductibles per Calendar Year3 $2,000 Employee only coverage $4,000 per Family
$ 4,000 Employee only coverage $ 8,000 per Family
Maximum Out-of-Pocket Limit per Calendar Year
$4,000 Employee only coverage4
$8,000 per Family4 (not to exceed $7,900 for one individual)
$ 6,500 Employee only coverage 5
$13,000 per Family5
Physician ServicesIncludes Covered Services performed in the Physician’s office during the Physician office visit. Includes, but is not limited to, office consults and exams; In-office surgery; In-office lab, x-ray, injections, and diagnostic and treatment services. Family planning services including injectables and vasectomy; Physical, Occupational, and Speech Therapy; Cardiac, Pulmonary, and Vascular Rehabilitation Services; Chemo, Radiation, IV, and Respiratory therapy services; Dialysis treatments. Pre-Authorization is required for in-office surgery6.Physician Office Visits Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
MDLIVE Services After Deductible Covered at 85% Not ApplicableSentara Quality Care Network (SQCN) Primary Care Physician (PCP) Office Visit SQCN providers are currently available in Hampton Roads, Charlottesville and Rockingham zip codes only. Members who do not reside in those areas will pay the SQCN provider coinsurance.
Non-Sentara Quality Care Network (SQCN) Primary Care Physician (PCP) Office Visit
After Deductible Covered at 85%
After Deductible Covered at 75%
After Deductible Covered at 50%
Sentara Quality Care Network (SQCN) Specialist Office Visit SQCN providers are currently available in Hampton Roads, Charlottesville and Rockingham zip codes only. Members who do not reside in those areas will pay the SQCN provider coinsurance.
Non-Sentara Quality Care Network (SQCN) Specialist Office Visit
After Deductible Covered at 85%
After Deductible Covered at 75%
After Deductible Covered at 50%
Physician ServicesPreventive Care10 Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Routine Annual Physical Exams Well Baby Exams Annual GYN Exams and Pap Smears11 PSA Tests Colorectal Cancer Tests Routine Adult and Childhood Immunizations Screening Colonoscopy Screening Mammograms (including 3-D mammograms) Women’s Preventive Services
Covered at 100% After Deductible Covered at 50%
82
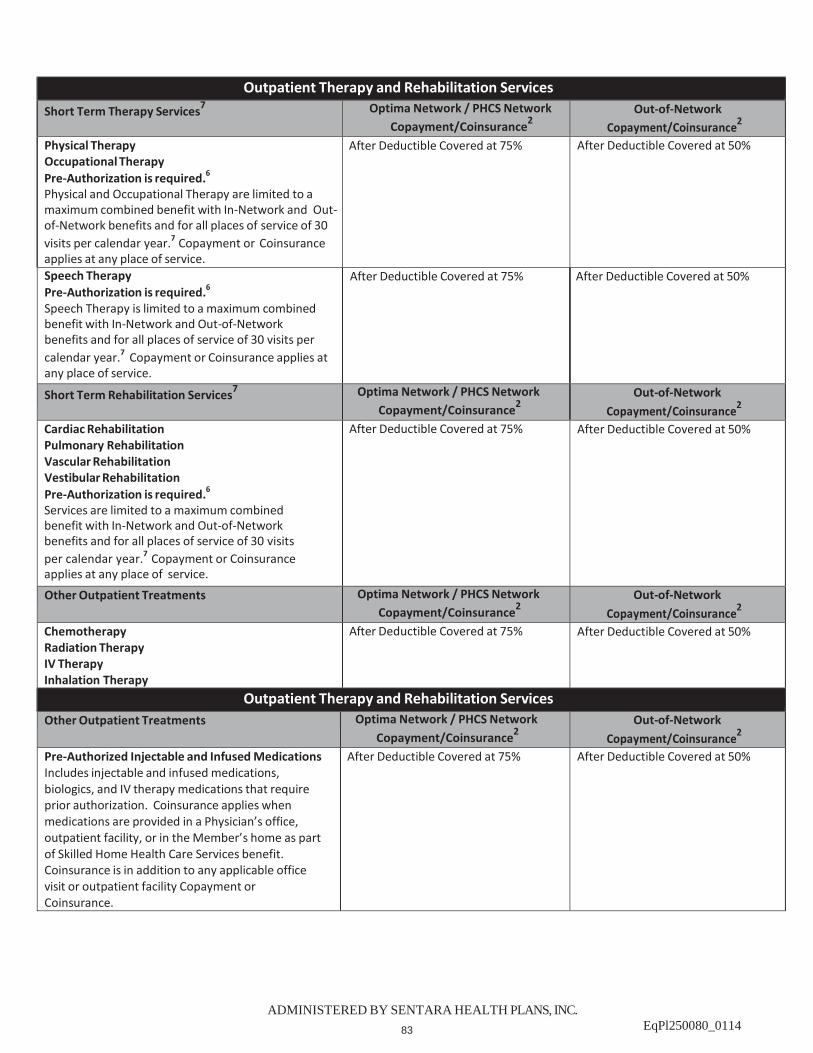
ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Outpatient Therapy and Rehabilitation ServicesShort Term Therapy Services7 Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Physical Therapy Occupational Therapy Pre-Authorization is required.6
Physical and Occupational Therapy are limited to a maximum combined benefit with In-Network and Out-of-Network benefits and for all places of service of 30 visits per calendar year.7 Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 75% After Deductible Covered at 50%
Speech Therapy Pre-Authorization is required.6
Speech Therapy is limited to a maximum combined benefit with In-Network and Out-of-Network benefits and for all places of service of 30 visits per calendar year.7 Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 75% After Deductible Covered at 50%
Short Term Rehabilitation Services7 Optima Network / PHCS Network Copayment/Coinsurance2
Out-of-Network Copayment/Coinsurance2
Cardiac Rehabilitation Pulmonary Rehabilitation Vascular Rehabilitation Vestibular Rehabilitation Pre-Authorization is required.6
Services are limited to a maximum combined benefit with In-Network and Out-of-Network benefits and for all places of service of 30 visits per calendar year.7 Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 75% After Deductible Covered at 50%
Other Outpatient Treatments Optima Network / PHCS Network Copayment/Coinsurance2
Out-of-Network Copayment/Coinsurance2
Chemotherapy Radiation Therapy IV Therapy Inhalation Therapy
After Deductible Covered at 75% After Deductible Covered at 50%
Outpatient Therapy and Rehabilitation ServicesOther Outpatient Treatments Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Pre-Authorized Injectable and Infused Medications Includes injectable and infused medications, biologics, and IV therapy medications that require prior authorization. Coinsurance applies when medications are provided in a Physician’s office, outpatient facility, or in the Member’s home as part of Skilled Home Health Care Services benefit. Coinsurance is in addition to any applicable office visit or outpatient facility Copayment or Coinsurance.
After Deductible Covered at 75% After Deductible Covered at 50%
83

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Outpatient Dialysis ServicesOutpatient Dialysis Services Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Dialysis Services Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 75% After Deductible Covered at 50%
Outpatient SurgeryOutpatient Surgery Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Outpatient Surgery Pre-Authorization is required.6
Coinsurance or Copayment applies to services provided in a free-standing ambulatory surgery center or hospital outpatient surgical facility.
After Deductible Covered at 75% After Deductible Covered at 50%
Outpatient Diagnostic ProceduresCopayment or Coinsurance will apply when a procedure is performed in a free-standing outpatient facility or lab, or a hospital outpatient facility or lab.Outpatient Diagnostic Procedures Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Outpatient Diagnostic Procedures After Deductible Covered at 75% After Deductible Covered at 50%Outpatient X-Ray Ultrasound Doppler Studies
After Deductible Covered at 75% After Deductible Covered at 50%
Outpatient Lab Work After Deductible Covered at 75% After Deductible Covered at 50%Outpatient Advanced Imaging and Testing Procedures
Outpatient Advanced Imaging and Testing Procedures
Optima Network / PHCS Network Copayment/Coinsurance2
Out-of-Network Copayment/Coinsurance2
Magnetic Resonance Imaging (MRI) Magnetic Resonance Angiography (MRA) Positron Emission Tomography (PET Scans) Computerized Axial Tomography (CT Scans) Computerized Axial Tomography Angiogram (CTA Scans) Sleep Studies Pre-Authorization is required.6
Copayment or Coinsurance applies at any place of service.
After Deductible Covered at 75% After Deductible Covered at 50%
Maternity CareMaternity Care Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Maternity Care 8,10,11
Pre-Authorization is required for prenatal services.6
Includes prenatal, delivery, postnatal, postpartum services, and home health visits. Copayment or Coinsurance is in addition to any applicable inpatient hospital Copayment or Coinsurance.
Sentara Quality Care Network (SQCN) SQCN providers are currently available in Hampton Roads, Charlottesville and Rockingham zip codes only. Members who do not reside in those areas will pay the SQCN provider coinsurance.
Non-Sentara Quality Care Network (SQCN)
After Deductible Covered at 85%
After Deductible Covered at 75%
After Deductible Covered at 50%
84

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Inpatient ServicesInpatient Services Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Inpatient Hospital Services Pre-Authorization is required.6
Transplants are covered at contracted facilities only.
After Deductible Covered at 75% After Deductible Covered at 50%
Skilled Nursing Facilities/Services7
Pre-Authorization is required.6
Following inpatient hospital care or in lieu of hospitalization. Covered Services include up to 100 days combined in and out-of-network per calendar year that in the Plan’s judgment requires Skilled Nursing Facility Services.7
After Deductible Covered at 75% After Deductible Covered at 50%
Ambulance ServicesAmbulance Services Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Ambulance Services9
Pre-Authorization is required for non-emergent transportation only.6
Includes air and ground ambulance for emergency transportation, or non-emergent transportation that is Medically Necessary and Pre-Authorized by the Plan. Copayment or Coinsurance is applied per transport each way.
After Deductible Covered at 75% *If transported by a Virginia BeachVolunteer Rescue Squad – Covered at 100%.
After Deductible Covered at 75%
Emergency ServicesEmergency Services Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Emergency Services9
Pre-Authorization is not required. Includes Emergency Services, Physician, and Ancillary Services provided in an emergency department facility. Inpatient copayment / coinsurance will apply if admitted.
After Deductible Covered at 75% After Deductible Covered at 75%
Urgent Care Center ServicesUrgent Care Center Services Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Urgent Care Services9
Pre-Authorization is not required. Includes Urgent Care Services, Physician services, and other Ancillary Services received at an Urgent Care facility. If You1 are transferred to an emergency department from an Urgent Care center, You1 will pay an Emergency Services Copayment or Coinsurance.
After Deductible Covered at 75% After Deductible Covered at 50%
85

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Mental/Behavioral Health CareIncludes inpatient and outpatient services for the treatment of mental health and substance abuse. Also includes services for Biologically Based Mental Illnesses for the following diagnoses: schizophrenia, schizoaffective disorder, bipolar disorder, major depressive disorder, panic disorder, obsessive-compulsive disorder, attention deficit hyperactivity disorder, autism, and drug and alcoholism addiction.Mental/Behavioral Health Care Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Inpatient Services Pre-Authorization is required.6
Residential treatment is not covered.
After Deductible Covered at 75% After Deductible Covered at 50%
Sentara Quality Care Network (SQCN) Outpatient Office Visits Pre-Authorization may be required.6
SQCN providers are currently available in Hampton Roads, Charlottesville and Rockingham zip codes only. Members who do not reside in those areas will pay the SQCN provider coinsurance.
Non-Sentara Quality Care Network (SQCN) Outpatient Office Visits Pre-Authorization may be required.6
After Deductible Covered at 85%
After Deductible Covered at 75%
After Deductible Covered at 50%
Other Outpatient Visits (Includes Hospital Outpatient and Freestanding Outpatient Centers) Pre-Authorization may be required.6
After Deductible Covered at 75% After Deductible Covered at 50%
Other Covered ServicesOther Covered Services Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Allergy Care Includes Allergy testing, Injections, Serum and RAST testing.
After Deductible Covered at 75% After Deductible Covered at 50%
86

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Other Covered ServicesOther Covered Services Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Autism Spectrum Disorder Pre-Authorization is required.6 Covered Services include “diagnosis” and “treatment” of Autism Spectrum Disorder in children from age two through 10.
“Autism Spectrum Disorder” means any pervasive developmental disorder, including (i) autistic disorder, (ii) Asperger’s Syndrome, (iii) Rett syndrome, (iv) childhood disintegrative disorder, or (v) Pervasive Developmental Disorder – Not Otherwise Specified, as defined in the most recent edition of the Diagnostic and Statistical Manual of Mental Disorders of the American Psychiatric Association.
“Diagnosis of autism spectrum disorder” means medically necessary assessments, evaluations, or tests to diagnose whether an individual has an autism spectrum disorder.
“Treatment for autism spectrum disorder” shall be identified in a treatment plan and includes the following care prescribed or ordered for an individual diagnosed with autism spectrum disorder by a licensed physician or a licensed psychologist who determines the care to be medically necessary: (i) behavioral health treatment, (ii) pharmacy care, (iii) psychiatric care, (iv) psychological care, (v) therapeutic care, and (vi) applied behavioral analysis when provided or supervised by a board certified behavioral analyst licensed by the Board of Medicine.
“Applied behavioral analysis” means the design, implementation, and evaluation of environmental modifications, using behavioral stimuli and consequences, to produce socially significant improvement in human behavior, including the use of direct observation, measurement, and functional analysis of the relationship between environment and behavior. Coverage for applied behavioral analysis under this benefit is limited to an annual maximum benefit of $35,000.6
Coverage for Autism Spectrum Disorder will not be subject to any visit limits, and will be neither different nor separate from coverage for any other illness, condition, or disorder for purposes of determining Deductibles, lifetime dollar limits, Copayment and Coinsurance factors, and benefit year maximum for Deductibles and Copayment and Coinsurance factors.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of treatment or service listed on the Summary of Benefits.
Coverage for Autism Spectrum Disorder will not be subject to any visit limits, and will be neither different nor separate from coverage for any other illness, condition, or disorder for purposes of determining Deductibles, lifetime dollar limits, Copayment and Coinsurance factors, and benefit year maximum for Deductibles and Copayment and Coinsurance factors.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of treatment or service listed on Summary of Benefits.
87

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Other Covered ServicesOther Covered Services Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Prosthetic Limbs and Components7
Pre-Authorization is required.6
Services include coverage for medically necessary prosthetic devices. This also includes repair, fitting, replacement and components.
Definitions: “Component” means the materials and equipment needed to ensure the comfort and functioning of a prosthetic device. “Limb” means an arm, a hand, a foot, or any portion of an arm, hand, a leg or foot. “Prosthetic device” means an artificial device to replace, in whole or in part, a limb. Prosthetic device coverage does not mean or include repair and replacement due to enrollee neglect, misuse, or abuse. Coverage also does not mean or include prosthetic devices designed primarily for an athletic purpose.
After Deductible Covered at 75% After Deductible Covered at 50%
Chiropractic Care7
Optima Health contracts with American Specialty Health Networks (ASHN) to administer this benefit. Pre-Authorization is required by ASHN for all chiropractic care services. 6
To receive services, contact ASHN's Member Services at 1-800-678-9133. Representatives are available from 8:00 AM to 9:00 PM Monday-Friday. Coverage is limited to a combined maximum benefit with in and out-of-network benefits of 30 visits per Person, per calendar year. This benefit also includes coverage of Chiropractic appliances up to a combined maximum benefit with in-and out-of-network benefits of 1 appliance per Person per calendar year when medically necessary.
For providers not in the ASHN network the Member will be responsible for payment of all charges in excess of ASHN’s allowable charge in addition to any coinsurance amount. Allowable charge is the lesser of the provider’s actual charge or ASHN’s In-Network fee schedule for the same services.
After Deductible Covered at 75% of ASHN fee schedule
After Deductible Covered at 50% of ASHN fee schedule
88

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Other Covered ServicesOther Covered Services Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Diabetic Supplies and Equipment Includes FDA approved equipment and supplies for the treatment of diabetes and in-person outpatient self-management training and education including medical nutrition therapy.
Insulin, syringes, and needles are covered under the Plan’s Prescription Drug Benefit for the applicable Copayment or Coinsurance per 31 day supply.
An annual diabetic eye exam is covered from an Optima Health Plan Provider, a participating EyeMed Provider, or a Non-Plan Provider at the applicable office visit Copayment or Coinsurance amount. For more information about how to access this benefit for meters, strips and lancets, please call one of the following providers: Home Care Delivered: 1-800-867-4412 EdgePark Medical Supplies: 1-888-394-5375
You may also call 552-7200 or 1-800-SENTARA for information on educational classes.
Blood glucose monitoring equipment and supplies including home glucose monitors, lancets, blood glucose test strips, and insulin pump infusion sets if prescribed by your physician: After Deductible Covered at 100%
Insulin pumps: After Deductible covered at 100%
Outpatient self-management training and education, including medical nutritional therapy: After Deductible covered at 100%
Blood glucose monitoring equipment and supplies including home glucose monitors, lancets, blood glucose test strips, and insulin pump infusion sets if prescribed by your physician: After Deductible Covered at 50%
Insulin pumps: After Deductible covered at: 50%
Outpatient self-management training and education, including medical nutritional therapy: After Deductible covered at: 50%
Durable Medical Equipment (DME) and Supplies7
Orthopedic Devices and Prosthetic Appliances7 Pre-Authorization is required for single items over $750.6
Pre-Authorization is required for all rental items.6
Pre-Authorization is required for repair and replacement.6
Covered Services include durable medical equipment, orthopedic devices, prosthetic appliances other than artificial limbs, colostomy, ileostomy, and tracheostomy supplies, suction and urinary catheters, and repair/replacement.
After Deductible Covered at 75% After Deductible Covered at 50%
Early Intervention Services Pre-Authorization is required.6
Covered for Dependents from birth to age three who are certified as eligible by the Virginia Department of Behavioral Health and Developmental Services.
Covered Services include: Medically Necessary speech and language therapy, occupational therapy, physical therapy and assistive technology services and devices.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of service.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of service.
89

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Other Covered ServicesOther Covered Services Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Family Planning Depo-Provera Injection:
Lunelle Injection:
Tubal Ligation: Pre-authorization required
Vasectomy:
Covered at 100%
Covered at 100%
Covered at 100%
After Deductible Covered at 100% Subject to any applicable outpatient/inpatient surgery copayment/coinsurance.
After Deductible Covered at 50%
After Deductible Covered at 50%
After Deductible Covered at 50%
After Deductible Covered at 50% Subject to any applicable outpatient/inpatient surgery copayment/coinsurance.
Hearing Aid Rider Pre-Authorization is required.6
The following services are covered up to the annual maximum benefit of $1,250 :
the hearing aid(s);audiometric specialist office visits for fitting,
including molds and dispensing; repair, replacement or refurbishment of the hearing
aid(s) Replacement is covered only every 36 months from date of acquisition. Batteries are not covered. Supplies are not covered.
After Deductible Covered at 75% After Deductible Covered at 50%
Home Health Care Skilled Services7 Pre-Authorization is required.6 Services are covered up to a maximum combined benefit with In-Network and Out-of-Network benefits of 100 visits per calendar year for Members who are home bound, and in the Plan’s judgment require Home Health Skilled Services.7
You will pay a separate outpatient therapy Copayment or Coinsurance amount for physical, occupational, and speech therapy visits received at home. Therapy visits received at home will count toward Your Plan’s annual outpatient therapy benefit limits.
You will pay a separate outpatient rehabilitation services Copayment or Coinsurance amount for cardiac, pulmonary, vascular, and vestibular rehabilitation visits received at home. Rehabilitation visits received at home will count toward Your Plan’s annual outpatient rehabilitation benefit limits.
After Deductible Covered at 75% After Deductible Covered at 50%
Hospice Care Pre-Authorization is required.6
After Deductible Covered at 75% After Deductible Covered at 50%
90

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
Other Covered ServicesOther Covered Services Optima Network / PHCS Network
Copayment/Coinsurance2Out-of-Network
Copayment/Coinsurance2
Vision Care and Materials7
Optima Health contracts with EyeMed Vision Care to administer this benefit. Medical conditions related to the eye, such as glaucoma, are covered under the medical plan. Coverage includes one examination every 12 months when done by a participating EyeMed Provider. To locate a participating EyeMed provider, please call 1-888-610-2268 or visit www.optimahealth.com.
Spectacle Exam: $20 Copayment then covered at 100%. OR
Contact Lens Exam: $40 Copayment then covered at 100%.
Limited to one exam every 12 months (from the date of last exam) by a participating EyeMed Provider.
Materials – By a participating EyeMed Provider: Lenses (single vision, bifocal, trifocal) covered in full. Frames: Covered in full up to $100 retail Contact Lenses (in lieu of glasses) covered in full up to $95 retail.
If you choose contact lenses when they are not medically indicated, you will receive an allowance of $95 toward the purchase price. (Contact lenses are deemed medically necessary following cataract surgery, to correct extreme visual acuity problems not correctable with spectacle lenses, or if you have certain conditions of anisometropia or keratoconus). If contact lenses are obtained, they are in lieu of spectacles.
For eye examinations from Out-of-Network providers, Members will be reimbursed up to $40 for an eye examination (once every 12 months from date of last exam).
No coverage for eyeglasses/contacts out-of-network.
Telemedicine Services Telemedicine Services means the use of interactive audio, video, or other electronic media used for the purpose of diagnosis, consultation, or treatment. Telemedicine services do not include an audio-only telephone, electronic mail message, or facsimile transmission.
Members are responsible for any applicable Copayment, Coinsurance, or Deductible depending on the type and place of treatment or service. Your out-of-pocket deductible, copayment, or coinsurance amounts will not exceed the deductible, copayment or coinsurance amount You would have paid if the same services were provided through face-to-face diagnosis, consultation, or treatment.
91

Basic POSOutpatient Prescription Drug Rider Schedule of Benefits
ADMINISTERED BY SENTARA HEALTH PLANS, INC.
This schedule of benefits describes Your outpatient prescription drug coverage. All drugs must be Food and DrugAdministration (FDA) approved and you must have a prescription. You will need to pay Your Copayment or Coinsurancewhen you fill your prescription at the pharmacy. If Your Plan has a Deductible you must meet that amount before yourcoverage begins. Some drugs require Pre-Authorization by Your Physician, and some quantities may be limited. Your drugcoverage has specific Exclusions and Limitations, so please read the next few pages carefully. Optima Health’s Pharmacyand Therapeutics Committee places covered drugs into the following Tiers. You will pay Your Copayment or Coinsurancedepending on which Tier Your Drug is in.
This Plan has a closed formulary and covers a specific list of drugs and medications. Drugs not included on the Plan’s formulary will be excluded from coverage.
Selected Generic (Tier 1) includes commonly prescribed generic drugs. Other drugs may be included in Tier 1if the Plan recognizes they show documented long-term decreases in illness.
Selected Brand & Other Generic (Tier 2) includes brand-name drugs, and some generic drugs with highercosts than Tier 1 generics, that are considered by the Plan to be standard therapy.
Non-Selected Brand (Tier 3) includes brand name drugs not included by the Plan on Tier 1 or Tier 2. Thesemay include single source brand name drugs that do not have a generic equivalent or a therapeutic equivalent.Drugs on this tier may be higher in cost than equivalent drugs, or drugs determined to be no more effective thanequivalent drugs on lower tiers.
Specialty Drugs (Tier 4) includes those drugs classified by the Plan as Specialty Drugs. Tier 4 also includescovered compound prescription medications. Specialty Drugs have unique uses and are generally prescribedfor people with complex or ongoing medical conditions. Specialty Drugs typically require special dosing,administration, and additional education and support from a health care professional. Specialty Drugs includethe following:
Medications that treat certain patient populations including those with rare diseases;
Medications that require close medical and pharmacy management and monitoring;
Medications that require special handling and/or storage;
Medications derived from biotechnology and/or blood derived drugs or small molecules; and
Medications that can be delivered via injection, infusion, inhalation, or oral administration.
Specialty Drugs are only available through Proprium Pharmacy at 757-553-3568 or 1-855-553-3568 (toll free). Specialty Drugs will be delivered to Your home address from Our Specialty mail order pharmacy. If You have a question or need to find out if Your drug is considered a Specialty Drug please call Member Services at thenumber on Your Optima Health ID Card. You can also log onto optimahealth.com for a list of Specialty Drugs.
A compound prescription medication is used to meet the needs of a specific individual and must have at leastone ingredient requiring a physician’s authorization by State or Federal Law. Compound prescriptions canusually be filled at Your local pharmacy.
Your Copayment, Coinsurance, and Deductible amounts for each Tier are listed on the following page. Your MaximumOut-of-Pocket Amount is also listed. If You need help please call Member Services or log on to optimahealth.com to findout which of the following Tiers Your drug is in.
92

Basic POSOutpatient Prescription Drug Rider Schedule of Benefits
ADMINISTERED BY SENTARA HEALTH PLANS, INC.
Specialty Drugs (Tier 4) After Deductible Covered at 75% (maximum $200)
Non-Preferred Pharmacy (all retail other than Walgreens, Walmart or Sam’s Club). You may purchase up to a 30-day supply.Selected Generic (Tier 1) After Deductible $25 Copayment (or the plan’s negotiated cost of the drug, if less)Selected Brand & Other Generic(Tier 2)
After Deductible $45 Copayment (or the plan’s negotiated cost of the drug, if less)
Non-Selected Brand (Tier 3) After Deductible Covered at 75% (maximum $75)
PLEASE NOTE: Prescription medications used to prevent any of the following medical conditions are not subject to thedeductible including medications for Hypertension, high cholesterol, diabetes, asthma, osteoporosis, stroke, prenatalnutrient deficiency.
Mail Order Pharmacy Benefit Copayments and CoinsurancesSome Outpatient prescription drugs are available through the Plan’s Mail Order Provider. This does not include Tier4 Specialty Drugs. You may call OptumRx Home Delivery at 866-244-9113 to find out if a drug is available. If Yourdrug is available You may purchase up to a 90-day supply for the Copayment or Coinsurance amount.Selected Generic (Tier 1) After Deductible $25 Copayment (or the plan’s negotiated cost of the drug, if less)Selected Brand & Other Generic(Tier 2)
After Deductible $60 Copayment (or the plan’s negotiated cost of the drug, if less)
Non-Selected Brand (Tier 3) After Deductible Covered at 75% (maximum $125)Specialty Drugs (Tier 4) No 90 day mail order benefits are available for Tier 4 Specialty Drugs
Non-formulary requests. You have the right to request a non-formulary prescription drug if You believe that You need a prescription drug that is not on the Plan’s list of covered drugs (formulary), or You have been receiving a specific non-formulary prescription drug for at least six months previous to the development or revision of the formulary and Your prescribing physician has determined that the formulary drug is inappropriate for Your condition or that changing drug therapy presents a significant health risk to You. Your physician must complete a medical necessity form and deliver it to the Optima Health pharmacy authorization department. After reasonable investigation and consultation with the prescribing physician, Optima Health will make a determination. Optima Health will act on such requests within one business day of receipt of the request. You will be responsible for all applicable Copayments, Coinsurance, or Deductibles depending upon which Tier a drug is placed in by the Plan.
PREFERRED NETWORK – You will pay a lower Copayment if you fill your prescriptions at a Walgreens, Walmart or Sam’sClub Preferred Pharmacy. You may purchase up to a 90-day supply for 3 Copayments or Coinsurance amounts.Selected Generic (Tier 1)Selected Brand & Other Generic(Tier 2)Non-Selected Brand (Tier 3)
After Deductible $10 Copayment (or the plan’s negotiated cost of the drug, if less)After Deductible $25 Copayment (or the plan’s negotiated cost of the drug, if less)
After Deductible Covered at 75% (maximum $50)
Deductibles and Maximum Out-of-Pocket LimitDeductibles You must meet the medical Deductible listed on the Your Plan’s Schedule of Benefits.Maximum Out-of-Pocket Outpatient Prescription Drug Copayments or Coinsurance apply to the Plan’s Maximum MedicalLimit Out-of-Pocket Limit.
Ancillary charges which result from a request for a brand name outpatient prescription drugwhen a generic drug is available are not Covered, do not count toward the Plan’s MaximumOut-of-Pocket Limit and must continue to be paid after the maximum out-of-pocket Limit hasbeen met.
Copayments and CoinsurancesFor a single Copayment or Coinsurance charge You may receive up to a consecutive 31-day supply of a covereddrug. A Copayment is a flat dollar amount. A Coinsurance is a percent of Optima Health’s Allowable Charge. Certainprescription drugs will be covered at a generic product level established by the Plan. If a generic product level has beenestablished for a drug and You or Your prescribing Physician requests the brand-name drug or a higher costing generic, Youmust pay the difference between the cost of the dispensed drug and the generic product level in addition to the Copaymentcharge (not to exceed $150 per each 31-day supply prescription).
93
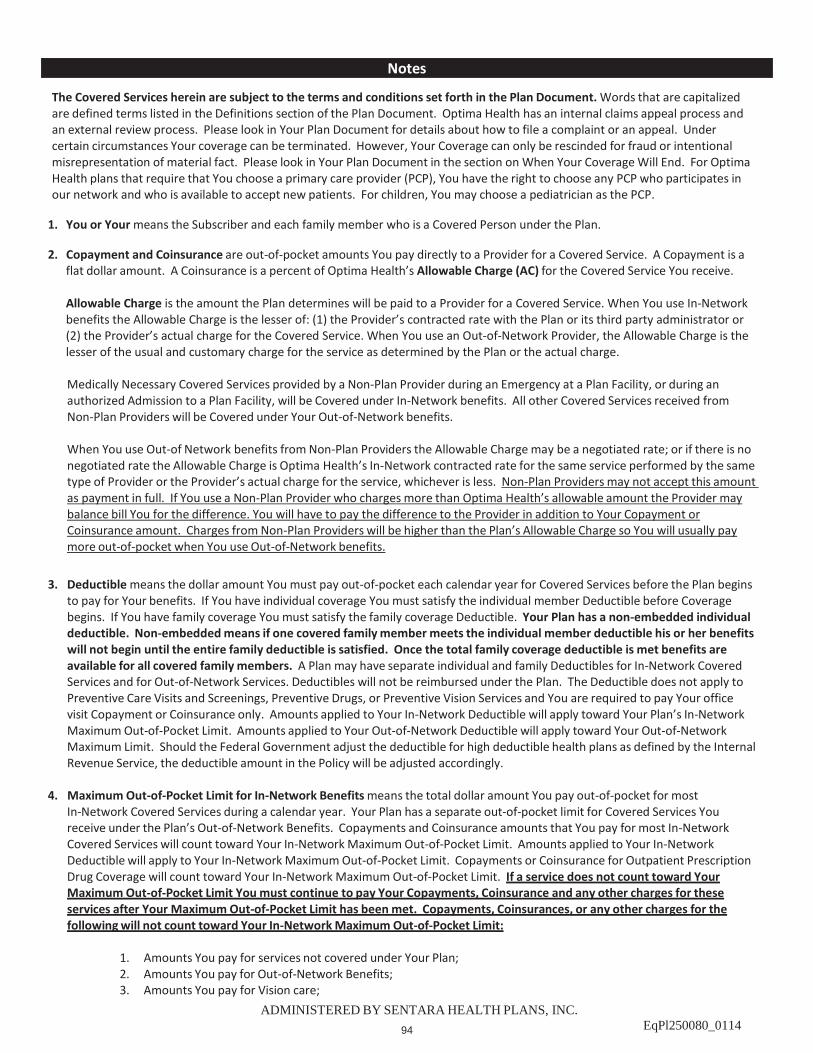
ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
The Covered Services herein are subject to the terms and conditions set forth in the Plan Document. Words that are capitalized are defined terms listed in the Definitions section of the Plan Document. Optima Health has an internal claims appeal process and an external review process. Please look in Your Plan Document for details about how to file a complaint or an appeal. Under certain circumstances Your coverage can be terminated. However, Your Coverage can only be rescinded for fraud or intentional misrepresentation of material fact. Please look in Your Plan Document in the section on When Your Coverage Will End. For Optima Health plans that require that You choose a primary care provider (PCP), You have the right to choose any PCP who participates in our network and who is available to accept new patients. For children, You may choose a pediatrician as the PCP.
1. You or Your means the Subscriber and each family member who is a Covered Person under the Plan.
2. Copayment and Coinsurance are out-of-pocket amounts You pay directly to a Provider for a Covered Service. A Copayment is aflat dollar amount. A Coinsurance is a percent of Optima Health’s Allowable Charge (AC) for the Covered Service You receive.
Allowable Charge is the amount the Plan determines will be paid to a Provider for a Covered Service. When You use In-Networkbenefits the Allowable Charge is the lesser of: (1) the Provider’s contracted rate with the Plan or its third party administrator or(2) the Provider’s actual charge for the Covered Service. When You use an Out-of-Network Provider, the Allowable Charge is thelesser of the usual and customary charge for the service as determined by the Plan or the actual charge.
Medically Necessary Covered Services provided by a Non-Plan Provider during an Emergency at a Plan Facility, or during anauthorized Admission to a Plan Facility, will be Covered under In-Network benefits. All other Covered Services received fromNon-Plan Providers will be Covered under Your Out-of-Network benefits.
When You use Out-of Network benefits from Non-Plan Providers the Allowable Charge may be a negotiated rate; or if there is nonegotiated rate the Allowable Charge is Optima Health’s In-Network contracted rate for the same service performed by the sametype of Provider or the Provider’s actual charge for the service, whichever is less. Non-Plan Providers may not accept this amountas payment in full. If You use a Non-Plan Provider who charges more than Optima Health’s allowable amount the Provider maybalance bill You for the difference. You will have to pay the difference to the Provider in addition to Your Copayment orCoinsurance amount. Charges from Non-Plan Providers will be higher than the Plan’s Allowable Charge so You will usually paymore out-of-pocket when You use Out-of-Network benefits.
3. Deductible means the dollar amount You must pay out-of-pocket each calendar year for Covered Services before the Plan beginsto pay for Your benefits. If You have individual coverage You must satisfy the individual member Deductible before Coveragebegins. If You have family coverage You must satisfy the family coverage Deductible. Your Plan has a non-embedded individualdeductible. Non-embedded means if one covered family member meets the individual member deductible his or her benefitswill not begin until the entire family deductible is satisfied. Once the total family coverage deductible is met benefits areavailable for all covered family members. A Plan may have separate individual and family Deductibles for In-Network CoveredServices and for Out-of-Network Services. Deductibles will not be reimbursed under the Plan. The Deductible does not apply toPreventive Care Visits and Screenings, Preventive Drugs, or Preventive Vision Services and You are required to pay Your officevisit Copayment or Coinsurance only. Amounts applied to Your In-Network Deductible will apply toward Your Plan’s In-NetworkMaximum Out-of-Pocket Limit. Amounts applied to Your Out-of-Network Deductible will apply toward Your Out-of-NetworkMaximum Limit. Should the Federal Government adjust the deductible for high deductible health plans as defined by the InternalRevenue Service, the deductible amount in the Policy will be adjusted accordingly.
4. Maximum Out-of-Pocket Limit for In-Network Benefits means the total dollar amount You pay out-of-pocket for mostIn-Network Covered Services during a calendar year. Your Plan has a separate out-of-pocket limit for Covered Services Youreceive under the Plan’s Out-of-Network Benefits. Copayments and Coinsurance amounts that You pay for most In-NetworkCovered Services will count toward Your In-Network Maximum Out-of-Pocket Limit. Amounts applied to Your In-NetworkDeductible will apply to Your In-Network Maximum Out-of-Pocket Limit. Copayments or Coinsurance for Outpatient PrescriptionDrug Coverage will count toward Your In-Network Maximum Out-of-Pocket Limit. If a service does not count toward YourMaximum Out-of-Pocket Limit You must continue to pay Your Copayments, Coinsurance and any other charges for theseservices after Your Maximum Out-of-Pocket Limit has been met. Copayments, Coinsurances, or any other charges for thefollowing will not count toward Your In-Network Maximum Out-of-Pocket Limit:
1. Amounts You pay for services not covered under Your Plan;2. Amounts You pay for Out-of-Network Benefits;3. Amounts You pay for Vision care;
Notes
94

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
4. Amounts You pay for any benefits covered under a plan rider;5. Amounts You pay for Reduction Mammoplasty benefits, except for procedures associated with reconstructive
breast surgery following mastectomy;6. Ancillary charges which result from Your request for a brand name outpatient prescription drug when a generic
drug is available. Ancillary charges are not Covered Services;7. Amounts You pay for any services after a benefit limit has been reached;8. Amounts You pay as a penalty for failure to comply with the Plan’s Pre-authorization procedures;9. Amounts applied to Your Out-of-Network Deductible.
5. Maximum Out-of-Pocket Limit for Out-of-Network Benefits means the total dollar amount You will pay during a calendar yearfor most Out-of-Network Covered Services. Your Plan has a separate Out-of-Pocket limit for Covered Services You receive underthe Plan’s In-Network Benefits. Copayments and Coinsurance amounts that You pay for most Out-of-Network Covered Serviceswill count toward Your Out-of-Network Maximum Out-of-Pocket Limit. Amounts applied to Your Out-of-Network Deductible willapply to Your Out-of-Network Maximum Out-of-Pocket Limit. If a service does not count toward Your Maximum Out-of-PocketLimit You must continue to pay Your Copayments or Coinsurance for these services after Your Maximum Out-of-Pocket Limithas been met. Copayments, Coinsurances, or any other charges for the following will not count toward Your Out-of-NetworkMaximum Out-of-Pocket Limit:
1. Amounts You pay for services not covered under Your Plan;2. Amounts You pay for In- Network Benefits;3. Amounts You pay for Vision care;4. Amounts You pay for any benefits covered under a plan rider;5. Amounts You pay for Reduction Mammoplasty benefits, except for procedures associated with reconstructive
breast surgery following mastectomy;6. Ancillary charges which result from Your request for a brand name outpatient prescription drug when a generic
drug is available. Ancillary charges are not Covered Services;7. Amounts You pay for any services after a benefit limit has been reached;8. Amounts You pay as a penalty for failure to comply with the Plan’s Pre-authorization procedures;9. Amounts applied to Your In-Network Deductible;10. Amounts that exceed the Plan’s Allowable Charge for a Covered Service
6. This benefit requires Pre Authorization before You receive services. Your benefits for Covered Services may be reduced ordenied if You do not comply with the Plan's Pre-Authorization requirements. The Plan may also apply a penalty of up to $500 toany benefits paid for Covered Services if You do not comply with the Plan’s Pre-Authorization requirements.
7. Coverage for this benefit or service is limited by a dollar amount and/or visit or day limits as stated. Maximum amounts arecombined maximums of both In-Network and Out-Of Network Covered Services unless otherwise stated. The Plan will not coverany additional services after the limits have been reached. You will be responsible for payment for all services after a benefitlimit has been reached. Amounts You pay for any services after a benefit limit has been reached are excluded from Coverage andwill not count toward Your Maximum Out-of-Pocket Maximum Limit.
8. Coverage for obstetrical services as an inpatient in a general hospital or obstetrical services by a physician shall provide suchbenefits with durational limits, deductibles, coinsurance factors, and Copayments that are no less favorable than for physicalillness generally. If the Plan charges a Global Copayment for prenatal, delivery, and postpartum services You are entitled to arefund from the Delivering Obstetrician if the total amount of the Global Copayment for prenatal, delivery, and postpartumservices is more than the total Copayments You would have paid on a per visit or per procedure basis.
9. All Emergency, Urgent Care, Ambulance, and Emergency Mental/Behavioral Health Services may be subject to RetrospectiveReview to determine the Plan’s responsibility for payment. If the Plan determines that the condition treated was not anEmergency Service, the Plan will have no responsibility for the cost of the treatment and You will be solely responsible forpayment. Members who receive Emergency Services from Non-Plan Providers may be responsible for charges in excess of whatwould have been paid had the Emergency Services been received from Plan Providers. In no event will the Plan be responsiblefor payment for services from Non-Plan Providers where the service would not have been covered had the member receivedcare from a Plan Provider.
10. Preventive Care includes recommended preventive care services under the Patient Protection and Affordable Care Act (PPACA)listed below. You may be responsible for an office visit copayment or coinsurance when you receive preventive careout-of-network. Some services may be administered under Your prescription drug benefit under the Plan.
95

ADMINISTERED BY SENTARA HEALTH PLANS, INC.EqPl250080_0114
1. Evidence-based items or services that have in effect a rating of A or B in the recommendations of the U.S.Preventive Services Task Force as of September 23, 2010, with respect to the individual involved;
2. Immunizations for routine use in children, adolescents, and adults that have in effect a recommendation from theAdvisory Committee on Immunization Practices of the Centers for Disease Control and Prevention with respect tothe individual involved. For purposes of this subdivision, a recommendation from the Advisory Committee onImmunization Practices of the Centers for Disease Control and Prevention is considered in effect after it has beenadopted by the Director of the Centers for Disease Control and Prevention, and a recommendation is consideredto be for routine use if it is listed on the Immunization Schedules of the Centers for Disease Control andPrevention;
3. With respect to infants, children, and adolescents, evidence-informed preventive care and screenings in theRecommendations for Preventive Pediatric Health by the American Academy of Pediatrics and the RecommendedUniform Screening Panels by the Secretary's Advisory Committee on Heritable Disorders in Newborns andChildren; and
4. With respect to women, evidence-informed preventive care and screenings recommended in comprehensiveguidelines supported by the Health Resources and Services Administration. Services include well-woman visits,screening for gestational diabetes, human papillomavirus, testing (HPV), counseling for sexually transmittedinfections, counseling and screening for human immunodeficiency virus (HIV), FDA-approved contraceptionmethods, sterilization procedures, and patient education and counseling for women, breastfeeding support,supplies, and counseling, screening and counseling for interpersonal and domestic violence.
11. You do not need prior authorization from Optima Health or from any other person (including a Primary Care Provider) in orderto obtain access to obstetrical or gynecological care from a health care professional in our network who specializes inobstetrics or gynecology. The health care professional, however, may be required to comply with certain procedures, includingobtaining prior authorization for certain services, following a pre-approved treatment plan, or procedures for making referrals.Look in Your Plan Document in the Utilization Management section for more information on pre-authorization.
96

Ph
arm
acy B
en
efi
ts
97

In order to maximize your pharmacy benefit, be sure to present your Optima Health member ID card whenever you have a
prescription filled. This is important whether the prescription is for a brand or a generic drug because the cost of many drugs
can be less than your Copayment. Some pharmacies advertise a $4 drug list; however that may not be the lowest price for you.
For some drugs the actual cost of the drug with your Optima Health member ID card may be less than the advertised $4 generic
program.
Here are a few examples where your cost may be less than $4:
Examples of Savings with Generics30-day supply
Drug Quantity What You Pay Pharmacy $4 ProgramSample Tier 1
Copayment
Amoxicillin 500mg capsules 30 $2.51 $4.00 $15.00
Atenolol 50mg tablets 30 $1.40 $4.00 $15.00
Fluoxetine 20mg capsules 30 $2.23 $4.00 $15.00
Hydrochlorothiazide (HCTZ) 25 mg tablets 30 $1.30 $4.00 $15.00
Ibuprofen 800 mg tablets 30 $2.35 $4.00 $15.00
Lisinopril 20 mg tablets 30 $2.23 $4.00 $15.00
Metformin 500 mg tablets 60 $2.47 $4.00 $15.00
The drugs and prices listed above are examples only. Prices are subject to change and prices may vary between pharmacies.
Optima Health offers an online tool that can help you determine what your cost will be for any of your prescription drugs. Simply
sign in to optimahealth.com and select Pharmacy Resources from the MyOptima menu. Then select the Price and Save button
and follow the directions to find out your cost for a specific drug.
WE WANT TO HELP YOU MAKE THE BEST OF YOUR PHARMACY DOLLARS
v7.18
Dear Member,
Thank you for choosing Optima Health!
To help ensure that you are paying the lowest
possible price for your medicines, make sure you
show your member ID card EVERYTIME you fill a
prescription!
98

OptumRx home delivery
Frequently asked questions
Why should I use OptumRx® for my prescriptions?Home delivery from OptumRx is a convenient and cost-effective way for you to order up to a 90-day supply of maintenance or long-term medication for delivery to your home, office or location of your choosing. You will minimize trips to the pharmacy and save money on your prescriptions.
What is a maintenance medicine?A maintenance medicine is taken on a regular basis for long-term conditions such as arthritis, diabetes, high blood pressure, ulcers and many others. You can save money on these medicines by filling a 90-day supply and using your OptumRx home delivery pharmacy benefit.
How do I use home delivery?1. Have your doctor write your prescription for the number of days your plan allows for home delivery
(for example, 90 days). Note: If you need your medicine right away, ask your doctor to write two prescriptions. Fill the first one at your local drug store. Mail the second one to OptumRx.
2. Fill out an order form. This form includes a confidential patient profile section for you and any family members. Write the member identification number, patient name and patient date of birth on the back of each prescription.
3. Mail the form with the prescription(s) and co-payment to: OptumRx, PO Box 2975 Shawnee Mission, KS 66201-1375
4. We will ship orders to the address entered on the form.
5. Check your order upon receipt. Make sure you review your order within 21 days of receipt. Contact us immediately to report any issues. Member service representatives and clinical pharmacists are available to discuss any questions at our toll-free number that is located on the back of your prescription ID card.
How do I refill a prescription I have already received through OptumRx?Do one of the following:
Visit our website: optimahealth.com/members.
Call OptumRx toll-free: 1-866-244-9113.
Send in the refill slip that came with your previous order. Be sure to include your co-payment. Mail it to OptumRx.
99

OptumRx | optumrx.com
OptumRx home delivery
Frequently asked questions
How do I fill a new prescription?• Fill out an order form. Write the member ID number, patient name and patient date of birth
on the back of each prescription.
• Mail the form to OptumRx. Include the prescription(s) and payment information.
How can my doctor order a prescription for me?• Doctors may call our toll-free number to prescribe your medication(s).
• Doctors may fax prescriptions to 1-888-637-5191.
• In addition to prescription information, your doctor must provide member ID number, patient name and patient date of birth.
Note: To be legally valid, the fax must originate from the physician’s office. All state laws apply.
Timing and shipping
When will I receive my order?You should receive your order within 14 days from the time OptumRx receives your prescription. Once received, a prescription typically takes one to two days to be processed and mailed if no additional information is required. Please allow a few extra days for your first order. If you have questions or do not receive your order within 14 days, please check the website at optimahealth.com/members or contact us at 1-866-244-9113.
What situations may cause a delay in prescription processing?Situations that may create a delay include an incomplete or unreadable prescription, manufacturer backorders and medications that require prior authorization. We will notify you if there will be a delay with your prescription shipment. Your prescriptions ship in separate packages if necessary.
Note: Orders received without payment may cause processing delays and extended delivery times.
Am I charged for shipping?No, shipping is free. However, OptumRx also offers expedited shipping for an extra charge.
How can I check on the status of my prescription order?Visit optimahealth.com/members or call us at 1-866-244-9113. Plan members who create an account on optimahealth.com/members will receive email notification when a prescription is shipped.
If I pay for rush shipping, when will it arrive?Rush shipping reduces the time in transit only. The actual prescription processing time does not change and can vary due to quality checks we perform or exceptions that may arise. Possible exceptions include needing additional information from your doctor, prior authorizations or drug interactions. These steps promote the health and safety of plan members and provide the highest level of quality when processing your prescriptions.
100

Why am I receiving overnight shipping when I did not request it?We ship certain medications overnight at our expense due to special handling requirements. This may apply to prescriptions for controlled substances or medications that are temperature sensitive.
What happens if I don’t receive my order?If you do not receive your order within 14 days, please contact us toll-free. We will reship your order to you as it is our priority to ensure you have the medication you need.
Prescription refills
How do I know whether I have refills remaining on my prescription?The number of refills allowed is noted at the bottom of your medication label, on your refill form and can also be found on the optimahealth.com/members website.
How soon can I order a prescription refill?For most prescriptions, you may reorder when you have approximately 3 weeks of your prescription left. Your medication label includes a target date for refilling the prescription.
• When ordering refills from OptumRx using the automated phone system, you will receive a message if your prescription is “too soon to refill.” You will be given the date when refills will be available.
• If you place a refill order after the expiration of your prescription, or if no refills are remaining, we will contact your physician for a new prescription. This may cause a slight delay.
I have a prescription on file at a retail pharmacy; can I order refills from OptumRx?Yes, however a new prescription from your doctor is recommended.
Medication coverage and cost
What drugs are covered?Your plan decides which medications are covered through OptumRx. To verify coverage please go to optimahealth.com/members, or call our toll-free number.
How much will my medicine cost me?The easiest way to determine the cost of your prescription is to log in to optimahealth.com/members.
How can I pay for my home delivery prescriptions?Checks, money orders or major credit cards can be used to cover your co-payments. Credit cards are preferred to allow for variations in the prices of drugs and are required when placing an order through our website. For your convenience, your credit card number will be maintained on a secured site for future orders.
101

OptumRx specializes in the delivery, clinical management and affordability of prescription medications and consumer health products. We are an Optum® company — a leading provider of integrated health services. Learn more at optum.com.
All Optum® trademarks and logos are owned by Optum, Inc. All other brand or product names are trademarks or registered marks of their respective owners.
© 2016 Optum, Inc. All rights reserved. ORX224877_160926
optumrx.com
Miscellaneous
How do I obtain additional order forms?You can print order forms at optimahealth.com/members. You also receive a reorder form, refill form and pre-addressed envelope with each prescription mailed to you.
Can I speak with a pharmacist if I use OptumRx home delivery?Yes, pharmacists are available to answer questions regarding your medication at 1-866-244-9113.
Can I fax my prescription that I received from my doctor?No. Legally, OptumRx is only allowed to accept faxed prescriptions from your doctor’s office.
Is my information kept private?Yes. We ask you for some personal information and we keep this information completely private. We use this information to help make sure you get the best care possible.
Why did I receive less than a 90-day supply of my prescription?The most common reason is that your doctor may have only written the prescription for 30 days or a prepackaged medication may not be packaged as a 30-, 60- or 90-day supply. Remember to ask your doctor to write a prescription for up to a 90-day supply, with up to three refills, if your doctor determines it’s appropriate.
What is a “controlled” medicine?A controlled medicine, such as a narcotic, has stricter guidelines and may be handled differently than non-controlled medicines, such as a medication for diabetes. We adhere to federal and state laws in the dispensing of all medicines. State law may require a copy of a state-issued ID, such as a driver’s license, for controlled medications to be dispensed.
Call OptumRx home delivery toll-free: 1-866-244-9113
or visit: optimahealth.com/members
102

How it works.
1 Order up to a three-month supply of your maintenance medications — ones you take regularly — by mail, phone or online.
2 OptumRx® fills your order, mails it to you and lets you know when to expect your delivery.
3 Your medication arrives within 7 to 10 days of placing the order. OptumRx will notify you if there will be a delay in your order.
Four easy ways to enroll:
Online.Log in to the website on the back of your member ID card.
Phone.Call the toll-free number on the back of your member ID card.
Mail.Complete the attached order form and mail it to OptumRx, P.O. Box 2975, Mission, KS 66201.
ePrescribe.Or your doctor can send an electronic prescription to OptumRx.
Manage your medication home delivery on the go.Order and track your prescriptions online or with our app.
Fill your prescriptions with home delivery.
OptumRx specializes in the delivery, clinical management and affordability of prescription medications and consumer health products. We are an Optum® company — a leading provider of integrated health services. Learn more at optum.com.
All Optum® trademarks and logos are owned by Optum, Inc. All other brand or product names are trademarks or registered marks of their respective owners.
© 2016 Optum, Inc. All rights reserved. ORX9542_160602
The benefits of home delivery.
Your medication is delivered right to your mailbox, saving you a trip to the pharmacy.
Your maintenance medication could cost less.
Pay nothing for standard shipping.
Phone, text1 and email reminders help you remember every dose and every refill.
1 OptumRx provides this service at no additional cost. Standard message and data rates charged by your carrier may apply.
103

NRX001
NEW PRESCRIPTION MAIL-IN ORDER FORMMember and physician information — please use black or blue ink. One form per member.
Member ID Number
(Additional coverage, if applicable) Secondary Member ID Number
Last Name First Name MI
Delivery Address Apt. #
City State ZIP
Phone Number with Area Code
Date of Birth (mm/dd/yyyy) Gender M F
Physician Name
Physician Phone Number with Area Code
Health historyMedication Allergies: Aspirin Erythromycin Quinolones Others:
None known Cephalosporins NSAIDs Sulfa Amoxil/Ampicillin Codeine Penicillin Tetracyclines
Health Conditions: Asthma Glaucoma High cholesterol Others: None known Cancer Heart condition Osteoporosis Arthritis Diabetes High blood pressure Thyroid Disease
Over-the-counter/herbal medications taken regularly:
Payment and shipping information — do not send cashStandard delivery is included at no charge. New prescriptions should arrive within about 10 business days from the date the completed order is received. Completed refill orders should arrive within about 7 business days. OptumRx will contact you if there will be an extended delay in delivering your medications.
For new prescription orders and maintenance refills, this credit card will be billed for copay/coinsurance and other such expenses related to prescription orders. By supplying my credit card number, I authorize OptumRx to maintain my credit card on file as payment method for any future charges. To modify payment selection, contact customer service at any time.
1
2
3
4
You may log on to optumrx.com to see if drug pricing information is available before enclosing payment. Once shipped, medications may not be returned for a refund or adjustment.
Mail this completed order form with your new prescription(s) to OptumRx, P.O. Box 2975, Mission, KS 66201. DO NOT STAPLE OR TAPE PRESCRIPTIONS TO THE ORDER FORM.
54777-032016 ORX5633_140915
Ship overnight. Add $12.50 to order amount (subject to change).
Check enclosed. All checks must be signed and made payable to: OptumRx.
Charge to my credit card on file. Charge to my NEW credit card.
Signature: Date:
New Credit Card Number
Expiration Date (Month/Year) Visa, MasterCard, AMEX and Discover are accepted.
104

FREQUENTLY ASKED QUESTIONS
What is a specialty pharmacy?
What services does Proprium Pharmacy provide?
What are the hours for Proprium Pharmacy and how do I contact you?
and coinsurance?
Call Proprium Pharmacy toll-free at 1-855-553-3568
105

FREQUENTLY ASKED QUESTIONS
What is the cost for delivery?
Call Proprium Pharmacy toll-free at 1-855-553-3568
106

Men
tal H
ealt
h a
nd
Em
plo
yee A
ssis
tan
ce P
ro
gram
107

Mental/Behavioral Health and Substance Use Disorder Services
Inpatient services and outpatient office visits for the treatment of mental health and substance use disorders are covered as medical benefits.
Pre-Authorization is required for inpatient services, partial hospitalization services, intensive outpatient program (IOP) services, Transcranial Magnetic Stimulation (TMS), and electro-convulsive therapy.
How to receive servicesCall Optima Behavioral Health at 1-800-648-8420 to be directed to a participating behavioral health provider. It is not necessary to go through the Primary Care Physician; or
Contact a participating behavioral health provider directly to arrange for an initial authorization.
If hospitalization is required, the behavioral health provider will arrange for admission to the appropriate facility.
Emergency servicesIf currently in treatment, contact the attending behavioral health provider.If not currently receiving care, call Optima Behavioral Health at 1-800-648-8420, and arrangements will be made for the member to be seen by a behavioral health professional. In order to ensure a prompt response to any clinical emergency, a 24-hour crisis hotline is available after normal business hours, on weekends, and on holidays.
If any member is engaged in behaviors that pose an immediate danger to themselves or to the life of another,please call 911 or go directly to an Emergency Department facility.
ExclusionsNon-medical ancillary services are not covered. These may include, but are not limited to: vocational rehabilitation services, employment counseling, health education, expressive therapies, or other non-medical services. Residential or sub-acute level of care or treatment is not covered by the Plan.
The member is responsible for all applicable Copayments, Coinsurances, and any Deductibles depending on the type and place of service as listed on the Plan’s Face Sheet or Schedule of Benefits.
Members should refer to Plan documents for Plan Copayments, Coinsurances, Deductibles, and Maximum Out-of-Pocket amounts, in addition to coverage exclusions and limitations.
Additional InformationCurrent members with questions regarding benefits may call Member Services at the number on the back of their member ID card or visit optimahealth.com to view Plan documents and find network physicians.If you are considering enrolling for the first time and have questions, please contact the group’s Benefits Administrator.
A telecommunications device for the hearing impaired can be accessed by dialing 1-800-828-1140 or 711.
108

Oth
er H
ealt
h In
su
ran
ce In
form
ati
on
109

1
Optima Equity HSA Plansoffered with a Health Savings Account (HSA)
Member Frequently Asked Questions
1. What is a health savings account?
A health savings account (HSA) is a savings and spending account that offers members a tax-advantagedway to pay for qualified medical expenses. You can also save for future medical and retirementhealthcare expenses. In order to open an HSA, you must be enrolled in a qualified high-deductiblehealth plan (HDHP).
2. What is a high-deductible health plan?
The Internal Revenue Service (IRS) defines HDHPs as plans with a deductible of at least $1,350 for anindividual, or $2,700 for a family. HDHPs tend to have higher deductibles than traditional health plans,which often results in a lower monthly premium. Your HDHP can be combined with an HSA allowing youto pay your qualified medical expenses, tax free.
3. Who is eligible to open an HSA?
Anyone who is enrolled in a qualified HDHP, is not covered by other health insurance, not enrolled inMedicare, and cannot be claimed as a dependent on someone else’s tax return.
4. Who can contribute to an HSA?
The member, their employer, or a third party can fund HSAs with tax-free dollars.
5. How much can be contributed each year?
For 201 , HSA holders can contribute up to $3, 0 for individual coverage, or $ , 00 for family coverage.HSA holders age 55 or older may also make an additional contribution of $1,000 per year (for a total of$4,5 0 for individual coverage or $ , 00 for family coverage).
These maximums are established by the IRS and are subject to change every year.
6. Who owns the HSA?
The member owns the account regardless of who contributes. The funds remain in the account and earntax-free interest and returns over time.
110

2
Optima Equity HSA Plans
offered with a Health Savings Account (HSA)
Member Frequently Asked Questions
7. What can I pay for with my HSA funds?
An HSA can be used to pay for any qualified medical expense as defined by the IRS. Qualified medicalexpenses include, but are not limited to: copayments, deductibles, coinsurance, vision care, and dentalcare. For a list of qualified medical expenses, please refer to IRS Publication 502 at www.irs.gov.
8. What are the benefits of using Optima Equity HSA, the integrated HSAs that Optima Health
offers?
After choosing the Optima Equity HSA benefit plan, the HSA account will be set up automaticallyduring the same enrollment process when the member elects to open an account. Our HSA Partner,HealthEquity®, administers the financial portion of the account.
The integrated Optima Equity HSA solution offers members a simpler experience. By signing in atoptimahealth.com, then selecting “Health Savings Account,” members have access to the followingfeatures all on one platform—the HealthEquity member portal:
• View medical claims.• Pay providers.• Store claims information to validate expenses.• View account balances.
9. What are the benefits of opening an HSA?
HSAs and qualified high-deductible health plans offer an option to save for retirement and pay formedical expenses. In order to determine if an HSA is right for you, compare your various benefit optionsand evaluate them based on your financial and health situation.
10.How can I use my HSA through Optima Equity HSA to pay for eligible services?
Account holders can make payments by debit card, online electronic funds transfer (EFT), or by phone.
The HealthEquity PayChoice® platform enables members to manage their account information, seeaccount balances, request reimbursements, or make payments from the account directly to providers.
Paper reimbursement checks to the member are also available for an additional fee. All records aremaintained electronically in the HealthEquity member portal for record keeping, tax purposes, or forfuture payment decisions.
Experienced HealthEquity Member Service representatives are available 24/7 at 866-346-5800 to answerquestions about your HSA or to assist you with phone transactions.
111

Optima Equity HSA Plans
offered with a Health Savings Account (HSA)
Member Frequently Asked Questions
11. What happens to HSA funds if the member changes jobs or retires?
The account belongs to the member account holder. You can keep your HSA even if you change or loseyour job, change your medical coverage, or move to another location. You own the account.
12. Can HSA funds be withdrawn at any time?
Yes, as long as they are used to pay for qualified medical expenses, the money is not taxed. If thefunds are used before age 65 for non-qualified expenses, the amount spent will be taxed and incur a20% penalty. Once the member reaches age 65 the funds can be used for non-qualified expenses, butwithdrawals will be subject to tax.
13. Can a retiree contribute to an HSA?
Yes, if they are covered by a qualified high-deductible health plan and not enrolled in Medicare, anotherhealth insurance plan, or are claimed as a dependent on someone else’s tax return.
14. Do members lose HSA funds at the end of the year?
No, the remaining funds roll over into the following year and grow tax-free.
15. Does an HSA earn interest?
Yes, and the interest accumulates tax-free.
16. Can HSA funds be invested?
Yes, once a $2,000 account balance is achieved, the first dollar above this amount can be invested. Themoney deposited into your HSA can earn interest or get investment returns—your choice. Your money isnever taxed if you use it for qualified medical expenses, regardless of your age.
17. Do I have to pay any additional out-of-pocket costs for wellness and preventive benefits*?
No, wellness or preventive benefits are paid by Optima Health and are not subject to the HDHPdeductible. Most preventive services are covered at 100% of the contracted provider rate.
*As defined under the Affordable Care Act (ACA).
3
112

Optima Equity HSA Plans
offered with a Health Savings Account (HSA)
Member Frequently Asked Questions
18. What happens after I open an HSA with my Optima Equity HSA plan?The
member account holder will receive the following items from HealthEquity:
• An HSA Member Welcome Letter, which lists all of the features of the HSA, including theHealthEquity Member Services contact information.
• A Member Guide providing the account holder with information on how to navigate theirHealthEquity member portal and manage their HSA.
• A Visa® debit card with activation sticker and card carrier.
• The PIN mailer, sent separately, which contains their debit card Personal Identification Number.
• Custodial account agreement for their records.
• HSA interest rate schedule.
19. How do I access my HSA account?
Sign in to your secure MyOptima site at optimahealth.com. Select “Health Savings Account” from yourMyOptima menu to navigate to your HealthEquity member portal.
If you are registering at optimahealth.com for the first time, you will need your member number fromyour Optima Health member ID card to create a username and password.
20. Where can I get information on investment funds?
You can access investment fund information from your HealthEquity member portal accessed throughyour secure MyOptima menu on optimahealth.com.
Optima Health is the tradename of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc. Optima Equity Plus HSA qualified high-deductible PPO health plans are underwritten by Optima Health Insurance Company. Optima Equity Vantage HSA qualified high-deductible HMO health plans are underwritten by Optima Health Plan. Self–funded qualified high-deductible health plans are administered but not underwritten by Sentara Health Plans, Inc. All health plans have benefit exclusions and limitations and conditions of coverage. For costs and complete details about coverage, ask your broker or employer. The information provided in this document is not tax or legal advice. The tax treatments vary for each situation. Please consult your tax or legal counsel for tax implication of your unique situation.
OEHSAFAQMBR_05184
113

Vision Care and Materials RiderThis benefit includes covered services for expanded vision care.
Optima Health contracts with EyeMed to administer this benefit for vision care services and materials. With the benefit, the member is eligible to receive a routine eye examination, refraction, lenses and frames/contact lenses once every 12 months (from the date of last exam) from a participating EyeMed Provider.
In-Network:Spectacle Exam - $20 copaymentContact Lens Exam - $40 copaymentLenses (single vision, bifocal, trifocal) – covered in fullFrames – covered in full up to $100 retailContact Lenses (in lieu of spectacles) – covered in full up to $95 retail
If an eye examination is received from an Out-of-Network provider, the member will be responsible for paying the provider in full at the time services are rendered. For eye examinations, members will be reimbursed $40 for an eye examination only.
Copayments or Coinsurance for covered services under this rider are not applied toward any Plan out-of-pocket maximum and must continue to be paid after the maximum is met.
After your primary eyewear benefit is exhausted, you are eligible to purchase glasses and contacts in unlimited quantities at the discounted prices listed on the next page (cannot be combined with any other promotion).
To receive covered services
Select a participating EyeMed network provider from the Plan's provider directory or by calling EyeMed at 1-888-610-2268. Automated location information is available 24 hours a day. Customer service representatives are available Monday through Saturday 7:30 a.m. – 11:00 p.m. ET and Sunday 11:00 a.m. – 8:00 p.m. ET.
Visit or call the participating provider and identify yourself as a member by providing your Member ID information. The provider will verify eligibility, your Plan's covered services, and any applicable costs. Payment is due when you receive services.
If the vision provider determines that you need additional medical care you should contact your Plan physician.
Additional Information
Current members with questions regarding benefits may call Member Services at the number on the back of their member ID card.
If you are considering enrolling for the first time and have questions, please contact the group’s Benefits Administrator.A telecommunications device for the hearing impaired can be accessed by dialing 1-800-828-1140 or 711.
114

Vision Discount Fee ScheduleA Defined Materials Discount
Vision Care Service Member Cost
Complete Pair of Glasses Purchase*: frame, lenses, and lens options must be purchased in the same transaction to receive full discount.
Standard Plastic Lenses:Single Vision $50Bifocal $70Trifocal $105
Frames: Any frame available at provider location 40% discount off retail price
Lens Options:UV Coating $15Tint (solid and gradient) $15Standard Scratch-Resistance $15Standard Polycarbonate $40Standard Progressive (add-on to bifocal) $65Standard Anti-Reflective Coating $45Other Add-ons and Services 20% discountContact Lens Materials:
(Discount applied to materials only)DisposableConventional
No discount on disposable 15% discount off retail price
Laser Vision Correction:
Lasik or PRK 15% discount off retail price or 5% discount off promotional price
*Items purchased separately will be discounted 20% off the retail price.
These discounts apply for all Optima Health members and do not, in any way, affect your premium, nor are they covered benefits under your health insurance plan.
These discounts cannot be used in conjunction with any other discount, rider, or benefit; and you will be responsible for applicable taxes.
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
115

Diabetes Treatment
Pre-Authorization is required for insulin pumps and pump infusion sets and supplies.
Coverage includes benefits for FDA-approved equipment, supplies, and in-person outpatient self-management training and education—including medical nutrition therapy—for the treatment of insulin-dependent diabetes, insulin-using diabetes, gestational diabetes, and non-insulin-using diabetes if prescribed by a healthcare professional legally authorized to prescribe such items.
Insulin pumps, pump infusion sets and supplies, testing supplies (test strips, lancets, lancet devices, blood glucose monitors, and control solution), and outpatient self-management training and education and nutritional therapy are covered under the Plan’s medical benefits.
Insulin, needles, and syringes are covered under the Plan’s pharmacy benefits.
To arrange for prescribed supplies to be delivered to their home, members may call one of the following providers, who are authorized to provide members who have diabetes with a new meter every 24 months at no cost to the member. Only these vendors can issue free meters:
Home Care Delivered at 1-800-867-4412; orEdgePark Medical Supplies at 1-888-394-5375.
Members may purchase covered diabetic testing supplies (not meters) from other sources and then submit receipts to have these costs applied to their plan.
Optima Health also covers in-person outpatient self-management training and education—including medical nutrition therapy. Training must be provided by a certified, registered, or licensed healthcare professional. Members may call 1-800-SENTARA for information on training and educational classes.
An annual diabetic eye exam is covered when received from an Optima Health Plan Provider or a participating EyeMed Provider.
The member is responsible for all applicable Copayments, Coinsurances, and any Deductibles depending on the type and place of service as listed on the Plan’s Face Sheet or Schedule of Benefits.
Members should refer to Plan documents for Plan Copayments, Coinsurances, Deductibles, and Maximum Out-of-Pocket amounts, in addition to coverage exclusions and limitations. Prior to receiving a member ID card, any member with questions may call Member Services at 1-877-552-7401. Members with ID cards may call the toll-free number on the ID card.
116

Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, Optima Health Group, Inc. and Sentara Health Plans, Inc. Optima Vantage HMO plans are underwritten by Optima Health Plan. Optima Preferred Provider Organization products are underwritten by Optima Health Insurance Company. Self-funded employer benefit plans are administered by Sentara Health Plans, Inc. All Optima Health plans have benefit exclusions and limitations and terms under which the policy may be continued in force or discontinued. For costs and complete details of coverage please call your broker or Optima Health at 1-800-741-4825 or visit optimahealth.com.
HearingAid_0119
Hearing Aid Rider
Pre-Authorization is required. Covered services include the following up to the annual maximum benefit amount of $1,250 and as specified on the Plan’s Schedule of Benefits:
hearing aid(s);audiometric specialist office visit(s) for fitting—including molds and dispensing;repair, replacement, or refurbishment of the hearing aid(s) up to the annual maximum benefitamount.
Replacement of the hearing aid(s) is covered every 36 months from date of acquisition. Batteries are not covered. Supplies are not covered.
The member is responsible for all applicable Copayments, Coinsurances, and any Deductibles depending on the type and place of service as listed on the Plan’s Schedule of Benefits. The member will be covered up to the annual maximum benefit amount.
Hearing aid providers are reimbursed using the Plan’s established fee schedule. If the member elects to get a hearing aid which exceeds the benefit maximum, the member will be responsible for the difference between the plan’s maximum allowable, or fee schedule, amount and the cost of the hearing aid.
Members should refer to Plan documents for Plan Copayments, Coinsurances, Deductibles, and Maximum Out-of-Pocket amounts, in addition to coverage exclusions and limitations.
Additional Information
Current members with questions regarding benefits may call Member Services at the number on the back of their member ID card or visit optimahealth.com to view Plan documents and find network physicians.
If you are considering enrolling for the first time and have questions, please contact the group’s Benefits Administrator.
A telecommunications device for the hearing impaired can be accessed by dialing 1-800-828-1140 or 711.
11

Chiropractic Care RiderFor covered services under this benefit, Optima Health contracts with American Specialty Health (ASH) to provide Chiropractic Services in the Plan's Service Area.
Pre-Authorization is required by ASH for all services.
To receive covered services
Call an ASH participating provider and schedule an appointment. You do not need a referral.
The ASH chiropractic provider is responsible for getting authorization from ASH before you receive care except for initial examination and Emergency Services.
If you have questions about what is covered or how to find an ASH provider, please call ASH toll-free at 1-800-678-9133, Monday through Friday 8 a.m. to 9 p.m. ET.
Covered services include examination, re-examination, manipulation, conjunctive therapy, radiology, chiropractic appliances, and laboratory tests related to the delivery of chiropractic services subject to the following:
An initial exam is performed by the participating provider to determine the nature of the Member's problem and, if Covered Services are needed, a treatment plan is prepared. One initial exam is provided for each new patient. A Copayment is required when services are rendered.A re-examination may be performed by the participating provider to assess the need to continue, extend, or change a treatment plan approved by ASH. A re-evaluation may be performed during a subsequent office visit or separately. If performed separately, a Copayment is required.Subsequent office visits may involve an adjustment, a brief re-examination, and other services. ACopayment is required for each visit to the office.Adjunctive therapy may involve modalities such as ultrasound, hot packs, cold packs, electrical muscle stimulation and other therapies.X-rays and clinical laboratory tests are payable in full when referred by a participating chiropractor and authorized by ASH. Radiological consultations are a covered benefit when authorized by ASH as Medically Necessary services and provided by a licensed chiropractic radiologist, medical radiologist, radiology group or hospital which has contracted with ASH to provide those services.Chiropractic appliances are covered up to a maximum benefit of one (1) appliance per year when prescribed by a participating chiropractor and authorized by ASH.
The following are excluded from Coverage:
Any services or treatments not authorized by ASH, except for initial exam and Emergency Services.Any services or treatments not delivered by participating chiropractors for the delivery of chiropractic care to members, except for Emergency Services.Services for exams and/or treatments for conditions other than those related to neuromusculoskeletal disorders from participating chiropractors.
118

Hypnotherapy, behavior training, sleep therapy, and weight programs.Thermograph.Services, lab tests, X-rays and other treatments not documented as clinically necessary as appropriate or classified as experimental or investigational and/or as being in the research stage.Services and/or treatments that are not documented as Medically Necessary services.Magnetic Resonance Imaging (MRI), CT scans, bone scans, nuclear radiology and any diagnostic radiology other than covered plain film studies.Transportation costs including local ambulance charges.Education programs, non-medical self-care or self-help or any self-help physical exercise training or any related diagnostic testing.Any services or treatments for pre-employment physicals or vocational rehabilitation.Air conditioners, air purifiers, therapeutic mattresses, supplies or any other similar devices or appliances; all chiropractic appliances or durable medical equipment, except as described as covered in this Rider.Drugs or medicines including a non-legend or proprietary medicine or medication not requiring a prescription order.Services provided by a chiropractor practicing outside the Service Area, except for Emergency Services. Hospitalization, anesthesia, manipulation under anesthesia and other related services.All auxiliary aids and services, including but not limited to, interpreters, transcription services, written materials, telecommunications devices, telephone handset amplifiers, television decoders and telephones compatible with hearing aids.Adjunctive therapy not associated with spinal, muscle or joint manipulation.Vitamins, minerals, or other similar products.
The member is responsible for all applicable Copayments, Coinsurances, and any Deductibles depending on the type and place of service as listed on the Plan’s Face Sheet or Schedule of Benefits.
Members should refer to Plan documents for Plan Copayments, Coinsurances, Deductibles, and Maximum Out-of-Pocket amounts, in addition to coverage exclusions and limitations.
Additional Information
Current members with questions regarding benefits may call Member Services at the number on the back of their member ID card or visit optimahealth.com to view Plan documents and find network physicians.
If you are considering enrolling for the first time and have questions, please contact the group’s Benefits Administrator.
A telecommunications device for the hearing impaired can be accessed by dialing 1-800-828-1140 or 711.
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, Optima Health Group, Inc. and Sentara Health Plans, Inc. Optima Vantage HMO plans are underwritten by Optima Health Plan. Optima Preferred Provider Organization products are underwritten by Optima Health Insurance Company. Self-funded employer benefit plans are administered by Sentara Health Plans, Inc. All Optima Health plans have benefit exclusions and limitations and terms under which the policy may be continued inforce or discontinued. For costs and complete details of coverage please call your broker or Optima Health at 1-800-741-4825 or visit optimahealth.com.
119

Complementary Alternative Medicine Discount Program
Each covered individual is offered a discount on acupuncture, chiropractic, therapeutic massage services, physical therapy, occupational therapy, and podiatry through the ChooseHealthy® Program. Participating providers extend a25% discount off their usual and customary charges.
How to Receive ServicesSelect a participating complementary healthcare provider from the Plan’s website at optimahealth.com.
Schedule an appointment with a participating provider. A physician referral is not necessary. The participating provider will develop, if necessary, a treatment plan for the member. There are no visit limitations. Changing your participating provider is permitted at any time.
In order to receive the complementary discount, present your member ID card at the time of service. The member is responsible for payment of services at each visit. There are no claim forms to file.
If chiropractic care is covered under the Plan’s medical benefit, the member may find it beneficial to use this discount program after the annual Plan limit has been met, or for services not covered under that benefit.
Additional InformationFor more information regarding this discount program, or to nominate a provider not yet in the network, please call ChooseHealthy Member Services at 1-877-335-2746 or refer to the Plan’s website at optimahealth.com. ASH’s Member Service representatives are available from 8 a.m. to 9 p.m. ET, Monday-Friday.
Current members with questions regarding benefits should call Member Services at the number on the ID card. If you are considering enrolling for the first time and have questions, please consult with your group’s Benefit Administrator.
A telecommunications device for the hearing impaired can be accessed by dialing 1-800-828-1140 or 711.
The ChooseHealthy Program is administered by ChooseHealthy, Inc., a subsidiary of American Specialty Health Incorporated (ASH). ChooseHealthy is a federally registered trademark of ASH and used with permission herein.
Please note that this program is not insurance. You should check any insurance benefits you have before using this discount program, as those benefits may result in lower costs to you than using this discount program. The discount program provides for discount specialty health care services from participating practitioners. You are obligated to pay for all health care services, but will receive a discount from those health care practitioners who have contracted with the discount program. The discount program has no liability for providing or guaranteeing services, and assumes no liability for the quality of services rendered.
120

Gym Network 360 Discount Program
Optima Health members have access to premier fitness, weight loss, and wellness brands at discounted pricing with Gym Network 360.
The Best Fitness Brands at the Best PricesGym Network 360, from Optima Health and GlobalFit, offers members great fitness brands at great prices, along with the education, resources, and tools to engage and motivate members to become more active and adopt healthier behaviors.
ExerciseMembers enjoy savings of 5-20% off retail rates of over 9,500 fitness facilities and programs designed to engage at all fitness levels.
Top brands include 24 Hour Fitness, Anytime Fitness, Curves, Gold’s Gym, LA Fitness, and more.Regional and specialty studio options include CrossFit, cycling, kickboxing, yoga, and more.Virtual fitness options include Group Fitness On Demand powered by Les Mills, and exercise videos from Zumba.
EatingMembers enjoy exclusive rates on top-ranked nutrition, weight loss, and healthy eating programs.
Variety of meal plans include fresh prepared meals, and diet delivery options.Discounts on top brands such as Nutrisystem, Jenny Craig, Diet-to-Go, and Kurbo.Discounts on vitamins, supplements, and other healthy food products.
EducationGym Network 360 provides wellness tools and resources to support and motivate members through their wellness journey all year long, including monthly promotions for additional savings.
How to Receive ServicesLook for the Gym Network 360 name on the Health and Wellness Discounts page at optimahealth.com/members.Members will be prompted to sign in (or first register* for their free, secure MyOptima online account) for more information. After sign in, members may choose to visit the Optima Health GlobalFit shopping platform to browse for services and activate their discount. GlobalFit Customer Service representatives are available by phone at1-800-294-1500, Monday – Friday 8:30 a.m. – 6 p.m. EST.
* If you have not yet registered for your free MyOptima online account, visit optimahealth.com/register. The information you provide must match the information on your Optima Health member ID card.
These discounts apply for all Optima Health members and do not, in any way, affect your premium, nor are they covered benefits under your health plan. These discounts cannot be used in conjunction with any other discount, rider, or benefit, and you will be responsible for applicable taxes. Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc. Optima Vantage HMO products and Point-of-Service products are underwritten by Optima Health Plan. Optima Plus PPO products and Optima Individual Plans are underwritten by Optima Health Insurance Company. Sentara Health Plans, Inc. provides administrative and TPA services for self-insured group health plans. The services listed on this page are value-added benefits available to Optima Health plan members, and not covered benefits under any Optima Health Plan.
121
Ad
dit
ion
al It
em
s
122

Disclaimers: MDLIVE does not replace the primary care physician. MDLIVE is not an insurance product nor a prescription fulfillment warehouse. MDLIVE operates subject to state regulation and may not be available in certain states. MDLIVE does not guarantee that a prescription will be written. MDLIVE does not prescribe DEA controlled substances, non-therapeutic drugs and certain other drugs which may be harmful because of their potential for abuse. MDLIVE physicians reserve the right to deny care for potential misuse of services. MDLIVE phone consultations are available 24/7/365, while video consultations are available during the hours of 7 am to 9 pm ET 7 days a week or by scheduled availability. MDLIVE and the MDLIVE logo are registered trademarks of MDLIVE, Inc. and may not be used without written permission. For complete terms of use visit www.mdlive.com/pages/terms.html 010113.
123

optimahealth.com
v7.2018
Do You Want to Save Time and Money?
Where to Go for Care
For non-emergency illness or injury:
Knowing where to go when you are sick or injured can keep money in your pocket and save you valuable time. In an emergency situation, you should always go to your nearest provider. Be sure it’s an emergency before you go to an Emergency Department for care, because emergency care is expensive. You have several options when dealing with non-emergency health situations, such as ear pain, throat pain, colds/flu, and rashes, which are often best treated by calling your doctor.
Step 1Call your doctor’s office first. If your doctor is available after hours, follow the instructions provided. If your doctor’s office is closed, and your doctor is unavailable by phone, call Care Coordination Program/After Hours Nurse Advice Line at
1-877-817-3037. This free call is your link to a licensed nurse who can assist you in determining your immediate next steps for care. If it is determined that you seek care somewhere other than your doctor’s office when it re-opens, then consider steps 2 and 3.
Step 2Consider calling MDLIVE prior to visiting an Urgent Care Center or the Emergency Department for non-emergent matters if your primary care physician is not available. When you need to connect with a physician, call 1-866-648-3638. From there, you can choose to connect to a physician via phone right away, or you can request an online video visit. Make sure to request that information from your MDLIVE visit is shared with your Primary Care Physician or doctor.
Step 3Urgent Care Centers may meet your needs and are usually a less expensive and faster option for treatment than a hospital Emergency Department. These facilities are usually open on evenings, weekends, and holidays when your doctor’s office may be closed. Be sure to request that information from your visit is shared with your Primary Care Physician or doctor.
Step 4Hospital Emergency Departments are the most expensive and often take longer than other treatment options in non-lifethreatening situations. If you choose to go to an Emergency Department, knowing which facilities participate with Optima Health can save you money. Be sure to request that information from your visit is shared with your Primary Care Physician or doctor.
For a complete list of doctors in the Optima Health network, visit optimahealth.com.
124

SQCN.org
Sentara Quality
Care Network
The goals of SQCN range from improving wellness and preventing disease to providing professional care coordination for patients with chronic disease or other complex medical conditions. SQCN aims to ensure that patients receive the right care, at the right place, at the right time.
Today, SQCN has more than 3,000 providers located in the Hampton Roads and Blue Ridge regions, as well as affiliations with Sentara Healthcare hospitals and Children’s Hospital of The King’s Daughters.
The Value of SQCN
The Sentara Quality Care Network (SQCN) is a community-wide network of healthcare providers who voluntarily work together to improve health care. SQCN is dedicated to the following:
• improving the quality of health care
• improving access to care and the overall patient experience
• reducing or controlling the costs of care (costs incurred by patients, payers and providers)
125

SQCN.org
Sentara Quality
Care Network
Even in today’s world of electronic messaging and electronic health records, there are gaps in communication and, at times, gaps in care. SQCN works to identify solutions and to invest in the staff and technology that will improve the way that patients experience health care, both within a practice and between practices.
Here are some examples of how SQCN works to become accountable for care:
• Helping to make sure that patients receive eligible cancer screenings within the timeframes set by national guidelines
• Educating providers on the most effective as well as cost-efficient prescription medications
• Creating a collaboration of SQCN pediatricians, local schools and athletic associations to educate parents on the importance of adolescent health evaluations in the pediatrician’s office. These evaluations can include what is required for sports physicals, but also include immunizations, depression screening and preventive counseling.
• Ensuring patients with chronic diseases see their primary care provider as frequently as needed
• Providing resources to help patients to understand their medical condition and to engage in the management of their disease
• Developing standards for diabetic patients including patient education and lab result monitoring, as well as developing individual care plans to stabilize and improve diabetic patient health
• Providing nurse care managers to coach, educate and follow-up with patients after a hospital stay or emergency room visit
Becoming More Accountable for Care
Your employer is generously supporting the Sentara Quality Care Network by offering you a reduced co-pay when you choose a SQCN healthcare provider. Take a look at your insurance card, or your health plan fee structure, for the discounted amount. The reduced co-pay applies to you, the member, as well as your covered family members.
Your Employee Member Benefit
126
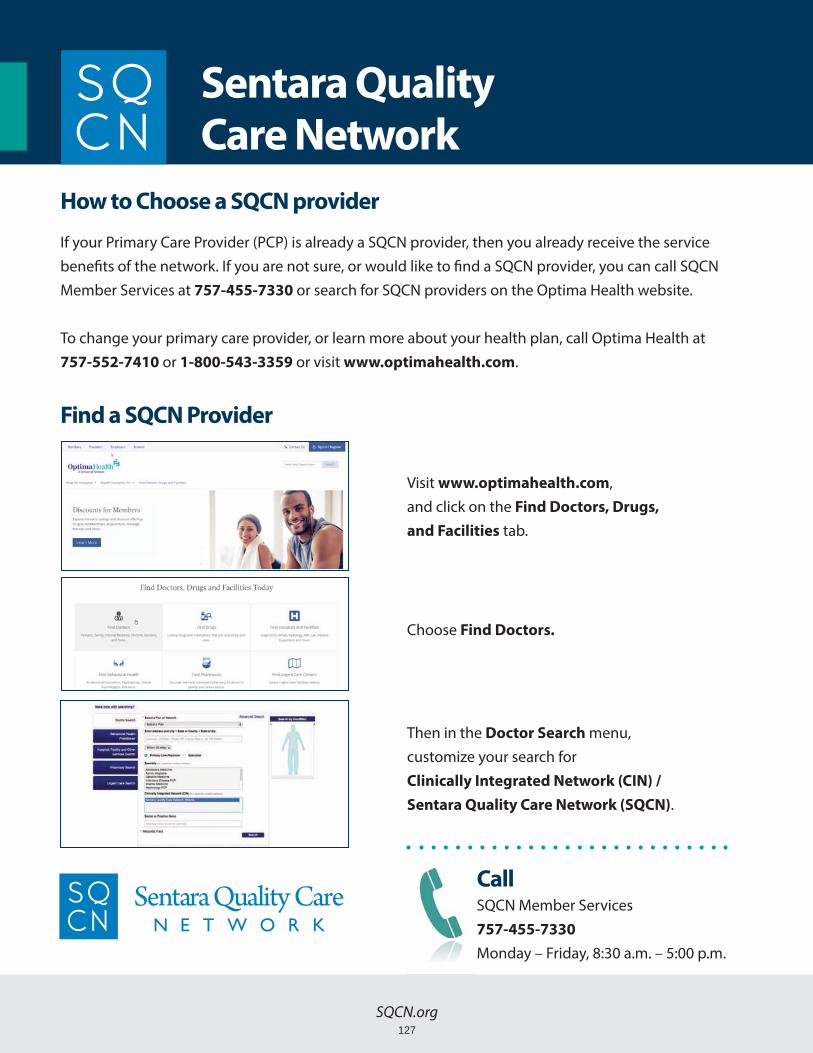
SQCN.org
Sentara Quality
Care Network
If your Primary Care Provider (PCP) is already a SQCN provider, then you already receive the service benefits of the network. If you are not sure, or would like to find a SQCN provider, you can call SQCN Member Services at 757-455-7330 or search for SQCN providers on the Optima Health website. To change your primary care provider, or learn more about your health plan, call Optima Health at 757-552-7410 or 1-800-543-3359 or visit www.optimahealth.com.
Visit www.optimahealth.com,and click on the Find Doctors, Drugs,
and Facilities tab.
Choose Find Doctors.
Then in the Doctor Search menu,customize your search forClinically Integrated Network (CIN) /
Sentara Quality Care Network (SQCN).
CallSQCN Member Services757-455-7330
Monday – Friday, 8:30 a.m. – 5:00 p.m.
How to Choose a SQCN provider
Find a SQCN Provider
127

Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc. v0318
Covered Under
Health Care Reform
P R E V E N T I V E S E R V I C E S
Covered Preventive Services for Adults
Abdominal aortic aneurysm screening: men
Alcohol misuse: screening and counseling
Aspirin use: adults aged 50–59 with risk of
cardiovascular disease
Blood pressure screening
Cholesterol screening for adults of certain ages
Colorectal cancer screening and generic and over-the-
counter prep medications: adults age 50–75
Consultation for screening colonoscopy
Depression screening
Diabetes screening: adults with high blood pressure
Falls prevention: adults 65 years or older—Vitamin D and
exercise or physical therapy
Healthy Diet Counseling
Hepatitis B screening
Hepatitis C virus infection screening: adults born between
1945 and 1965
HIV screening
Immunization vaccine: Herpes Zoster
Immunization vaccines:
Hepatitis A
Hepatitis B
Human Papillomavirus
Influenza
Measles, Mumps, Rubella
Meningococcal
Pneumococcal
Tetanus, Diphtheria, Pertussis
Varicella
Under the Affordable Care Act, certain preventive services and medications are covered at no cost to the member when administered by an in-network plan physician or pharmacy.
*†Statin medications: adults ages 40–75
with no history of cardiovascular
disease who have one or more risk
factors and calculated 10-year risk
Syphilis screening
Tobacco use counseling, generic and
over-the-counter medications, and
cessation
interventions
Tuberculosis screening
* Select medications only are covered at no cost to the member. Please contact Member Services or Pharmacy Services at the number on the back of your member ID card for more information.
† Effective at group or plan renewal on or after November 1, 2017.
128

Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc. v0318
Covered Preventive Services for Women,
Including Pregnant Women
Anemia screening: pregnant women
Bacteriuria screening
BRCA risk assessment and genetic counseling/
screening
Breast cancer chemoprevention counseling
*Breast cancer preventive medication
Breast cancer screening: women over age 40
Breast feeding support and counseling
Cervical cancer screening
Chlamydia infection screening
Contraception: All Food and Drug Administration-
approved contraceptive methods and intrauterine
devices (IUD); sterilization procedures including
tubal ligations and Essure; and patient education
and counseling; not including abort/facient
drugs. Generic oral contraceptives are eligible for
100% coverage. Please visit optimahealth.com to
determine member cost share for brand name oral
contraceptives.
Decision making/sharing by clinicians with women at
increased risk for breast cancer
Depression screening
Folic acid supplementation
Gestational diabetes mellitus screening
Gestational diabetes screening: women 24 to 28
weeks pregnant and those at high risk of developing
gestational diabetes
Gonorrhea screening
Hepatitis B screening at first prenatal visit
HIV screening: pregnant women
HPV Test
Intimate partner violence screening and counseling
Lactation support and counseling
Osteoporosis screening: women over 65 or at high risk
Preeclampsia screening and prevention
Rh incompatibility screening: first pregnancy visit and
between 24 and 28 weeks gestation
STI counseling
Syphilis screening
Well-woman visits
Tobacco counseling and intervention
* Select medications only are covered at no cost to the member. Please contact Member Services or Pharmacy Services at the number on the back of your member ID card for more information.
129
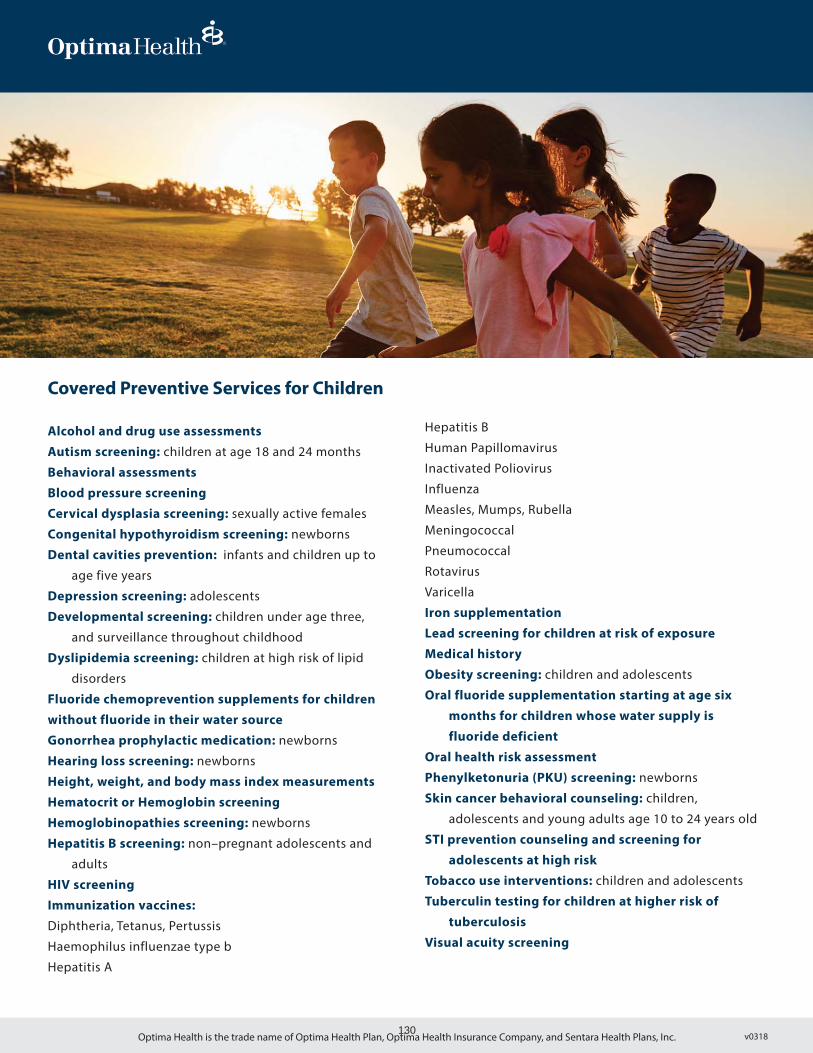
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc. v0318
Covered Preventive Services for Children
Alcohol and drug use assessments
Autism screening: children at age 18 and 24 months
Behavioral assessments
Blood pressure screening
Cervical dysplasia screening: sexually active females
Congenital hypothyroidism screening: newborns
Dental cavities prevention: infants and children up to
age five years
Depression screening: adolescents
Developmental screening: children under age three,
and surveillance throughout childhood
Dyslipidemia screening: children at high risk of lipid
disorders
Fluoride chemoprevention supplements for children
without fluoride in their water source
Gonorrhea prophylactic medication: newborns
Hearing loss screening: newborns
Height, weight, and body mass index measurements
Hematocrit or Hemoglobin screening
Hemoglobinopathies screening: newborns
Hepatitis B screening: non–pregnant adolescents and
adults
HIV screening
Immunization vaccines:
Diphtheria, Tetanus, Pertussis
Haemophilus influenzae type b
Hepatitis A
Hepatitis B
Human Papillomavirus
Inactivated Poliovirus
Influenza
Measles, Mumps, Rubella
Meningococcal
Pneumococcal
Rotavirus
Varicella
Iron supplementation
Lead screening for children at risk of exposure
Medical history
Obesity screening: children and adolescents
Oral fluoride supplementation starting at age six
months for children whose water supply is
fluoride deficient
Oral health risk assessment
Phenylketonuria (PKU) screening: newborns
Skin cancer behavioral counseling: children,
adolescents and young adults age 10 to 24 years old
STI prevention counseling and screening for
adolescents at high risk
Tobacco use interventions: children and adolescents
Tuberculin testing for children at higher risk of
tuberculosis
Visual acuity screening
130

O P T I M A H E A L T H
Treatment Cost Calculator
For more information, visitoptimahealth.com/features/treatment-cost-calculator
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc. v0718
View estimates on over 500 procedures and services in your
area, based on your specific benefit plan information.
B E T T E R I N F O R M AT I O N — B E T T E R D E C I S I O N S — B E T T E R H E A LT H
Shop and compare out-of-pocket costs for a
specific procedure at a specific doctor or medical facility.
Compare your options, plan for future expenses, and make
the best decisions for both your health and your wallet.
• Search or browse for a procedure/service or local healthcare provider.
• As you explore your options, view cost-saving tips and additional guidance on technical healthcare information relevant to your search.
• View out-of-pocket estimates* based on real-time balances of your health plan’s Deductibles and Out-of-Pocket Maximums.
• View maps, get directions, call for appointments, and print or email estimates.
S I G N I N AT O P T I M A H E A LT H . CO M TO C A LC U L AT E T R E AT M E N T CO S T S
X-ray SEARCH
Did you know ...< >
*Please Note: estimates provided within the Treatment Cost Calculator are not quotes. While every effort is made to provide members with the most accurate information, in some instances the actual charges from your healthcare provider may be different than the average estimate provided.
131

S A V I N G M O R E
Save on Products
and Services
MYLIFE MYPLAN
Optima Health members have the opportunity to save money
on health products and services including:
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
These discounts are value-added benefits available to Optima Health members and do not, in any way, affect your premium, nor are they covered benefits under your health plan. These discounts cannot be used in conjunction with any other discount, rider, or benefit, and you will be responsible for applicable taxes.
For more information, visit optimahealth.com/mylifemyplan
Acupuncture
Receive a 25% discount for acupuncture exams and treatment.
Chiropractic Care
Receive a 25% discount for chiropractic services.
Massage Therapy
Receive a 25% discount for massage therapy.
Health Products
Receive 25% discounts on vitamins and other health products with online ordering convenience and free shipping on most items.
For additional information, call toll-free
1-877-335-2746.
Hearing Extras
Receive a 20% - 50% savings for hearing care and services, including functional testing, hearing aid evaluation, fitting, programming, and training.
For additional information, call toll-free
1-866-956-5400.
Vision Extras
Receive significant savings on routine eye exams, lenses and frames, and contact lenses.
Laser Vision
Receive up to a 15% discount for the cost of laser vision surgery.
For additional information, call toll-free
1-877-552-7376.
Fitness Facilities
Access to savings of up to 20% off retail rates of big box gyms, specialty studios, virtual fitness programs, and more.
For additional information, visit the Saving More section of optimahealth.com/mylifemyplan.
v0718132

S A V I N G M O R E
Gym Network 360
from GlobalFit and
Optima Health
Optima Health members have access to premier fitness, weight loss, and
wellness brands at discounted pricing with Gym Network 360.
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
These discounts apply for all Optima Health members and do not, in any way, affect your premium, nor are they covered benefits under your health plan. These discounts cannot be used in conjunction with any other discount, rider, or benefit, and you will be responsible for applicable taxes. Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc. Optima Vantage HMO products and Point-of-Service products are underwritten by Optima Health Plan. Optima Plus PPO products and Optima Individual Plans are underwritten by Optima Health Insurance Company. Sentara Health Plans, Inc. provides administrative and TPA services for self-insured group health plans. The services listed on this flyer are value-added benefits available to Optima Health plan members and not covered benefits under any Optima Health Plan.
For access to Gym Network 360,visit our Health and Wellness Discounts pageat optimahealth.com/members
Optima Health and GlobalFit have teamed
up to offer Optima Health members the best
fitness brands at the best prices.
Gym Network 360 provides access to premier fitness, weight loss, and wellness brands at discounted pricing along with the education, resources, and tools to engage and motivate members to become more active and adopt healthier behaviors.
Exercise
Members enjoy savings of 5-20% off retail rates of over 9,500 fitness facilities and programs designed to engage at all fitness levels.
• Top brands include 24 Hour Fitness, Anytime Fitness, Curves, Gold’s Gym, LA Fitness, and more.
• Regional and specialty studio options include CrossFit, cycling, kickboxing, yoga, and more.
• Virtual fitness options include Group Fitness On Demand powered by Les Mills, and exercise videos from Zumba.
Eating
Members enjoy exclusive rates on top-ranked nutrition, weight loss, and healthy eating programs.
• Variety of meal plans include fresh prepared meals, and diet delivery options.
• Discounts on top brands such as Nutrisystem, Jenny Craig, Diet-to-Go, and Kurbo.
• Discounts on vitamins, supplements, and other healthy food products.
Education
Gym Network 360 provides wellness tools and resources to support and motivate members through their wellness journey all year long, including monthly promotions for additional savings.
v0318
MYLIFE MYPLAN
133

Cancer Tips
MYLIFE MYPLAN
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
For more information, visit optimahealth.com/mylifemyplan
References: Optima Health Clinical Guidelines, 2018
DON’T FORGET YOUR PREVENTIVE SCREENINGS!
Pap Test
Clinical Breast Exam
Mammogram
Digital Rectal Exam
PSA (prostate-specific antigen)
Colonoscopy or
Sigmoidoscopy or
Fecal Occult Blood Test
Start by age 21 and then retest per yourphysician’s recommendation.
Complete per your physician’s recommendation.
Start by age 45 and then retest per yourphysician’s recommendation.
Complete by age 50 and then yearly.
Complete by age 40 for those at risk, and then yearly.
Complete per your physician’s recommendation.
Complete by age 50 and then every 10 years.
Complete by age 50 and then every 5 years.
Complete by age 50 and then yearly.
All screening recommendations should be completed with the advice of your medical provider. See the other side for Skin Cancer Prevention Tips.
Early Cancer Detection - Female
Colorectal Cancer Screening
Early Cancer Detection - Male
SCREENING RECOMMENDATIONS
v0618
S T A Y I N G H E A L T H Y
134

MYLIFE MYPLANS T A Y I N G H E A L T H Y
SKIN CANCER PREVENTION TIPS
• Avoid the sun between 10 a.m. and 4 p.m.
• Cover up with protective clothing.
• Wear a wide brimmed hat.
• Use UVA protective sunglasses.
• Seek shade.
• Avoid reflective surfaces.
• Don’t use tanning salons or sun lamps.
• Use sunscreen with SPF 30 or higher.
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
— Apply 1/2 hour before sun exposure.
— Reapply every two hours.
Staying Healthy ProgramsFor more information, visit wellnessforme.com
Eating for LifeDevelop healthy eating and exercise habits
Get Off Your Butt: Stay Smokeless for LifeQuit tobacco to improve your health
Guided MeditationExperience a retreat from everyday stressors
Healthy Habits Healthy YouDevelop habits to prevent diabetes and heart disease
Tai ChiLearn to mentally and physically relax
WalkAbout With Healthy EdgeWalk your way to better health
YogaStretching and strengthening exercises
optimahealth.com/mylifemyplan
135

S T A Y I N G H E A L T H Y
Healthy Habits, Healthy You
MYLIFE MYPLAN
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
For more information, visit:optimahealth.com/mylifemyplan
Make Healthy Food Choices by Following the D.A.S.H. Eating Plan D.A.S.H. (Dietary Approaches to Stop Hypertension) is an eating plan designed to lower blood pressure. It emphasizes fruits, vegetables,
• Make half your plate vegetables and fruits, and aim for at least 8-10 servings a day.
• Choose 100% whole grains like whole wheat bread, oats, and brown rice.
• Choose lean meats, poultry without skin, and cook by grilling, baking, or broiling.
• Keep a healthy snack with you, like fresh fruit or a handful of nuts.
• Control your portions by putting less food on your plate, or using a smaller plate, bowl, or glass.
• Cut back on high-fat foods like whole milk, cheeses, and fried foods.
• Drink water instead of juice, sweet tea, or regular soda. Limit candy, pastries, and desserts.
• Reduce daily sodium intake to less than 2,300mg.
• Use oils to replace shortening and butter, and season with onion, garlic, and fresh herbs instead of salt, bacon, or cured meats.
• Try grilled chicken or salads instead of a cheeseburger or pizza at fast food restaurants.
Move More, Be Active• Try to be active for at least 30 minutes, 5 days a
week. Up to 60-90 minutes daily may be needed for weight loss.
• Walk in a safe place like the mall or at community centers.
• Dance and turn up the music when doing household chores.
• March in place while you watch TV.
Find Ways to Relax and Get More Sleep• Try deep breathing, taking a walk, or listening to
your favorite music.
• nicotine, or alcohol several hours before going to sleep.
• Think before you eat. Try not to snack when you are bored, upset, or unhappy.
• Avoid tobacco use.
Program to Prevent Type 2 Diabetes and Heart DiseaseTake steps to prevent diabetes and heart disease by making healthy food choices and moving more every day
Sources: The 2015 Dietary Guidelines for Americans, choosemyplate.gov, cdc.gov/sleep
v0817136

Build a healthy plate
• Make half your plate fruits and vegetables. Eat red, orange, and dark-green vegetables.
• Switch to skim or 1% milk, they have the same amount of calcium as whole milk with fewer calories and fat.
• Make at least half your grains whole. Choose 100% whole grain cereals, breads, and pastas.
• Vary your protein food choices. Choose seafood twice a week and eat beans for protein and fiber.
Cut back on foods high in solid fats, added sugars, and salt
• Choose foods and drinks with little or no added sugars.
• Reduce daily sodium intake to less than 2,300 milligrams (mg).
• Eat fewer foods that are high in solid fats. Pizza, cheese, hot dogs, and cakes are higher in saturated fat. Choose lean meats and use oils for cooking.
Eat the right amount of calories for you
• Enjoy your food, but eat less.• Cook more often at home, where you are in
control of what’s in your food.• When eating out, choose lower calorie
menu options.• Write down what you eat to keep track of
how much you eat.
Be physically active your own way
Pick activities that you like and start by doing what you can, at least 10 minutes at a time. Every bit adds up, and the health benefits increase as you spend more time being active.
C H O O S E M Y P L A T E F O R
HealthierEating
For more information, visit optimahealth.com/mylifemyplan
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
MYLIFE MYPLAN
Follow these tips to help you...
v0817137

A V O I D
PortionDistortion
For more information, visit optimahealth.com/mylifemyplan
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
MYLIFE MYPLAN
20 Years Ago Today Activity to Burn Extra Calories*
333 calories
500 calories
85 calories
270 calories
590 calories
*Based on a 160-pound person
850 calories
250 calories
630 calories
more calories
more calories
more calories
more calories
+ 257
+ 350
+ 165
+ 360
Ride a bike for 45 mins
Play golf while walking and carrying clubs for 1 hour
Work in the garden 35 mins
Do water aerobics for 1 hour and 15 mins
References: USDA Publication number: Home and Garden Bulletin No. 232-CP HHS Publication number: HHS-ODPHP-2010-01-DGA-B June 2011National Heart, Lung, and Blood Institute, NIH, https://www.nhlbi.nih.gov/health/educational/wecan/eat-right/portion-distortion.htmU.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015 - 2020 Dietary Guidelines forAmericans. 8th Edition. December 2015. Available at http://health.gov/dietaryguidelines/2015/guidelines/
138
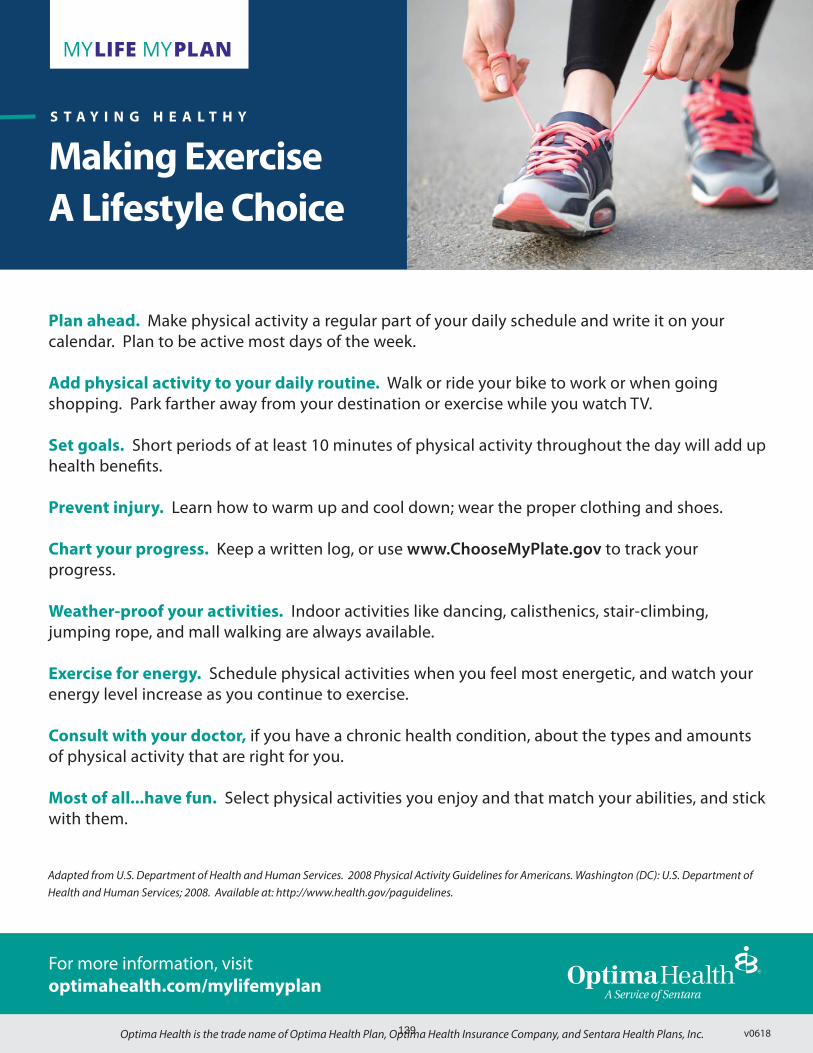
S T A Y I N G H E A L T H Y
Making Exercise
A Lifestyle Choice
MYLIFE MYPLAN
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
Plan ahead. Make physical activity a regular part of your daily schedule and write it on your calendar. Plan to be active most days of the week.
Add physical activity to your daily routine. Walk or ride your bike to work or when going shopping. Park farther away from your destination or exercise while you watch TV.
Set goals. Short periods of at least 10 minutes of physical activity throughout the day will add up health benefits.
Prevent injury. Learn how to warm up and cool down; wear the proper clothing and shoes.
Chart your progress. Keep a written log, or use www.ChooseMyPlate.gov to track your progress.
Weather-proof your activities. Indoor activities like dancing, calisthenics, stair-climbing, jumping rope, and mall walking are always available.
Exercise for energy. Schedule physical activities when you feel most energetic, and watch your energy level increase as you continue to exercise.
Consult with your doctor, if you have a chronic health condition, about the types and amounts of physical activity that are right for you.
Most of all...have fun. Select physical activities you enjoy and that match your abilities, and stick with them.
Adapted from U.S. Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans. Washington (DC): U.S. Department of Health and Human Services; 2008. Available at: http://www.health.gov/paguidelines.
For more information, visit optimahealth.com/mylifemyplan
v0618139

M Y H E A L T H A S S I S T A N T
Keeping You on Track Online
MYLIFE MYPLAN
Your 24/7 resource to help you keep your eyes on the prize.
Make checking in with My Health Assistant part of your regular routine, and you’ll have what it takes to start a good health routine and stick with it. My Health Assistant, powered by WebMD Health Services, uses the goals and activities you select to create simple weekly plans that get you from start to success. During your journey, you’ll enjoy an interactive online experience that’s motivational, fun, and invigorating.
Focus on one or more of the following areas:
• Nutrition
• Exercise
• Weight Loss
• Stress Management
• Emotional Health
• Tobacco Cessation
For more information, visitoptimahealth.com/mylifemyplan
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc. v0817140

My Health Assistant
Your Digital Health Assistant (DHA)The DHA is an online coach that creatively engages you to improve your overall health and wellness with
healthy habits and achieve your goals.
Ready – Accessing the Digital Health AssistantDHA activities are customized to you, your health plan, and your wellness program. You can access this tool from the Optima Health website:
• Sign in at optimahealth.com/mylifemyplan.• Select Wellness Tools from your MyOptima menu
on the left side of the screen to navigate to your personalized WebMD wellness home page.
Set – Setting Goals with the Digital Health AssistantOption One – Set a DHA goal based on your Personal Health Assessment (PHA) score.
• Complete the PHA questionnaire.• From your PHA results screen, click the green Let’s
Go! button to navigate to the My Health Assistant page and choose your goal(s).
Option Two – Set a DHA goal without taking the Personal Health Assessment.
• From your personalized WebMD wellness home page, select the Healthy Living tab at the top of the page.
• Select My Health Assistant.• Choose which goal(s) you would like to work
towards by clicking Manage My Goals.
Choose one or more of the following DHA goals: Eat Better, Enjoy Exercise, Lose Weight, Conquer Stress, Feel Happier, Quit Tobacco.
Success – Reaching Goals with the Digital Health AssistantOnce you have selected your DHA goal(s), you are ready to begin tracking your progress. Record your daily activities following these easy steps:
• Sign in at optimahealth.com/mylifemyplan and select Wellness Tools from your MyOptima menu.
• From your personalized WebMD wellness home page, select the Healthy Living tab at the top of the page and choose My Health Assistant.
• Click on the icon that best represents your daily activities towards each goal.
• Sign in daily or weekly to record your activities. Weeks begin on Sunday and end on Saturday; you may only back-track and record past activities completed since Sunday of the current week.
• •
DHA How to Record Your Daily Activities
Eat Better
Enjoy Exercise Click More than 20 Minutes, 20 Minutes, or Less than 20 Minutes
Lose Weight Enter your current weight
Conquer Stress
Enter your current stress level on a scale from low to high
Feel Happier Click Happy, Okay, Down, or Sad
Quit Tobacco Enter how many times you use tobacco daily
M Y H E A L T H A S S I S T A N T MYLIFE MYPLAN
For more information, visitoptimahealth.com/mylifemyplan
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.141

S T A Y I N G H E A L T H Y
Managing YourHigh Blood Pressure
MYLIFE MYPLAN
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
EAT A HEALTHY DIET• Consider the D.A.S.H (Dietary Approaches to Stop Hypertension) eating plan from National
Institutes of Health, which has been shown to reduce elevated blood pressure.
• Read food labels. Consume less than 2,300 mg of sodium a day.
• Limit sodium in the foods you eat, especially added salt, processed foods, and canned soups.
• Potassium helps to prevent and control high blood pressure. Choose fruits and vegetables such as potatoes, tomatoes, lima beans, and bananas.
• Learn more about healthy eating and the D.A.S.H. eating plan from the Optima Health “Eating for Life” program.
MAINTAIN A HEALTHY WEIGHT• Being overweight increases your risk of developing high blood pressure.
• overweight and already have hypertension.
STAY PHYSICALLY ACTIVE• Being physically active can prevent or control high blood pressure, and reduce your risk of heart
disease.
• Your goal should be at least 30 minutes of moderate-level physical activity on most days of the week, like brisk walking, bicycling, raking leaves, and gardening.
LIMIT ALCOHOL INTAKE• Drinking too much alcohol can raise blood pressure.
• If you drink alcoholic beverages, have only a moderate amount; one drink a day for women,
drinking alcohol.
Adapted from NHLBI Your Guide to Lowering High Blood Pressure 2011, http://www.nhlbl.nih.gov/hbp; Your Guide to Lowering High Blood Pressure with DASH Eating Plan, 2010, http://www.nhlbl.nih.gov/health/public/heart/hbp/dash/new_dash.pdf; and U.S Department of Health and Human Services and U.S Department of Agriculture 2015 - 2020 Dietary Guidelines for Americans. 8th Edition. December 2015. Available at http://health.gov/dietaryguidelines/2015/guidelines/.
For more information, visit optimahealth.com/mylifemyplan
v0817142

S T A Y I N G H E A L T H Y
Managing Your
Cholesterol
MYLIFE MYPLAN
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
WHAT IS CHOLESTEROL?
Cholesterol is a waxy, fat-like substance that the body uses to make hormones and other substances. High blood cholesterol can lead to heart disease. Two blood cholesterol measurements are:
LDL (low-density lipoprotein) cholesterol is the “bad” cholesterol because it leads to a buildup of cholesterol in the arteries.
HDL (high-density lipoprotein) cholesterol is the “good” cholesterol because it helps remove cholesterol from the body. An HDL of 60 mg/dL or higher will help lower your risk for heart disease.
WHAT AFFECTS CHOLESTEROL LEVELS?
Diet - Foods high in solid fat, like cheese, butter, pizza, and many fast foods, can make your cholesterol go up.
Weight - Being overweight is a risk factor for heart disease and can increase your cholesterol.
Physical Activity - Regular activity can lower your total cholesterol and can help you lose weight.
Age and Gender - As men and women get older, their cholesterol levels rise.
Heredity - Your genes partly determine how much cholesterol your body makes. High cholesterol can run in families.
HOW CAN I MANAGE MY CHOLESTEROL?
Healthy Eating
• Choose fat-free or low-fat dairy products, lean meats, skinless poultry, and 8 ounces of seafood weekly.
• Read food labels to avoid trans fat found in processed foods like baked goods. Look for soft and liquid margarines.
• Increase fiber in your diet from fruits, vegetables, and whole grains. Soluble fiber found in oats, dried peas, and beans can help lower your cholesterol.
• Learn more about healthy eating from the “Eating for Life” program.
For more information, visit optimahealth.com/mylifemyplan
v0618143

S T A Y I N G H E A L T H Y
Tobacco Cessation Tips
MYLIFE MYPLAN
DO:Be patient with yourself
Be positive; use self-talk
Be proud of small accomplishments
Take time for yourself
Believe that you can be a non-smoker
Get lots of rest
Use your sense of humor
Talk to someone
Drink water often
Remember why you chose to become tobacco-free
DON’T:Be impatient
Worry about ”forever”
Be negative
Neglect yourself
Drink a lot of alcohol
Overdo
Take yourself too seriously
Be afraid to ask for help
Believe you can have “just one”
Forget the reason you quit
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
For more information, visit optimahealth.com/mylifemyplan
v0817144

Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
MYLIFE MYPLANS T A Y I N G H E A L T H Y
TOBACCO CESSATION RESOURCES1. National Quitline Network 1-800-QUIT-NOW (1-800-784-8669).
2.for Life at-home program.
3. Visit Sentara.com to learn about the availability of free classesin your area.
4. Call (757) 687-6000 for free individual counseling with a tobacco cessation specialist.
ADDITIONAL RESOURCESFOR OPTIMA HEALTH MEMBERS ONLY1. To access WebMD Health Services tools, sign in at
optimahealth.com/mylifemyplan and select Wellness Tools fromyour MyOptima menu.
2. To work directly with a Case Manager, call the Member Servicesphone number on your Optima Health member ID card.
For more information, visit optimahealth.com/mylifemyplan
145

HEARING SERVICE PLAN
Welcome The EPIC Hearing Service Plan is the nation’s first specialty care plan devoted to the vital sense of hearing. EPIC is dedicated to delivering the highest quality of care at the best value to our members.
Provider Network The EPIC network is comprised of professional Audiologists and ENT physicians and represents the largest network of its kind in the nation with provider locations in all 50 states.
Hearing Aids The EPIC Hearing Service Plan gives you access to all name brand hearing aid technology by the top tier hearing aid manufacturers at reduced prices, 30%-60% below MSRP; maximizing your value and savings.
How it Works Contact an EPIC hearing counselor today. The hearing counselor can answer any questions you may have about the plan and coordinate your referral to a nearby participating provider. If the provider recommends you obtain hearing aids, an EPIC counselor will contact you to coordinate your coverage and payment. You will receive a 45 day trial period with a complimentary extended 3 year product warranty and one year supply of batteries*.
Prices for brand name products,
and services, starting as low as
$495
Call EPIC today to start the process to better hearing.
1 866.956.5400
*Excludes Basic Level Products
Group: Optima Health EPIC HSP Toll Free 866.956.5400
Email: [email protected]
The EPIC Hearing Service Plan (HSP) gives you access to the largest hearing care provider network in the country, and substantial savings on top tier manufacturer brand hearing devices.
Coverage for hearing exams &devicesReferrals to the largest nationalnetwork of Audiologists and ENTphysiciansFixed pricing reduced 30-60%below MSRPAccess to all name brand hearingaids and technologyMoney-back trial periodsFollow-up careOn call customer service support
Extended warranties
& complimentary
batteries
HEAR BETTER LIVE FULLYepichearing.com
Contact EPIC for a referral to a participating provider.
Reference Code: OptimaHealth 2015
146

1Members go to
www.listenhearlivewell.com and register with your name
and email address.
2Complete the 4 fun,
educational hearing healthactivities.
3Receive your reward couponfor additional savings off of
your purchase.
Welcometo the Listen Hear, Live Well
Hearing Health Wellness Program
Here’s How it Works:
Listen Hear, Live Well reward coupon savings are applied per each hearing device that is purchased--maximizing your value! Plus, these reward savings are applied on top of the 30% - 60% savings off of MSRP that is already available on an open selection of major brand hearing aids through the EPIC Hearing Service Plans. Simply complete the online wellness program on your desktop or mobile device and contact the EPIC Hearing Service Plan toll free at 1 866.956.5400 to redeem your reward, and start the process to better hearing!
Premium Devices: $200 offAdvanced Devices: $100 offStandard Devices: $50 off
Save
LISTENHEARLIVEWELL.COM [email protected]
ListenHear LiveWell
L147

WelcomeThe EPIC Hearing Service Plan is the nation’s first specialty care plan devoted to the vital sense of hearing. EPIC is dedicated to delivering the highest quality of care at the best value to our members.
Provider NetworkThe EPIC network is comprised of professionalAudiologists and ENT physicians and represents the largest accredited network of its kind in the nation, with provider locations in all 50 states.
Hearing AidsThe EPIC Hearing Service Plan gives you access to all name brand hearing aid technology by the top tier hearing aid manufacturers at reduced prices, 30%-60% below MSRP; maximizing your value and savings. Note: the following top tier manufacturer brands are available through EPIC: Phonak, Unitron, Lyric, GN Resound, Starkey, Siemens, Oticon, and Widex.
How it WorksContact an EPIC hearing counselor today. The hearing counselor can answer any questions you may have about the plan and coordinate your referral to a nearby participating provider. If the providerrecommends you obtain hearing aids, an EPIC counselor will contact you to coordinate your coverage and payment. You will receive a 45 day trial period with a com-plimentary extended 3 year product warranty and one year supply of batteries*.
*Excludes Basic Level Products
Hear Better Live Well
Call EPIC today to start the process to better hearing.
1 866.956.5400www.epichearing.com
HEARING SERVICE PLAN
Group: Optima HealthCoverage:Savings of 30% - 60% off MSRPon name brand hearing aids and related professional services.
Effective: 1/1/2016
PERKSEPIC Hearing Service Plan
The EPIC Hearing Service Plan (HSP) gives you access to the largest hearing care provider network in the country and substantial savings on top tiermanufacturer brand devices and related professional services.
PREMIUM
BASIC
STANDARD
ADVANCED
DEGREE OF HEARING
LOSS
TYPICALMSRP
EPICPRICING
Mild to
Moderate
Moderate
Moderateto
SevereModerate
toSevere
$1,400-$1,600
$1,601-$2,300
$2,301-$3,000
$3,001-$4,000
LEVEL OFHEARING AIDTECHNOLOGY
$495
$849-$1,499
$1,500-$2,099
$2,100-$2,500PREMIUM
Contact EPIC for a referral:1 866.956.5400
EPICSAV2016
148

ProgenyHealth partners with Optima Health to help deliver quality care for premature and medically complex newborns. ProgenyHealth is a national health company specifically focused on neonatal intensive care unit (NICU) care management.
With this partnership with ProgenyHealth, our impacted members are provided distinct comprehensive NICU case management services that enables us to provide the best care for our members and their families.
ProgenyHealth services include:
• A diverse, clinical team consisting of pediatricians, neonatologists, NICU nurses, case managers, and social workers.
• Managing the ongoing NICU health needs of babies through their first year of life.
• Case managers available 24/7 as a direct resource for families.
• Assigned case managers provide additional support and education to parents for their infant’s care.
• Supply member education and care management programs.
Quality Care for Premature and
Medically Complex Newborns
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc. v0818
ProgenyHealth Utilization Management and Case Management programs are NCQA and URAC accredited, and are overseen by seasoned neonatologists, pediatricians and NICU-experienced nurses with an average of 12 years clinical experience. The team works under the guidance of a unique Medical Advisory Board comprised of neonatologists from around the country.
For more information
about this program,
please contact your
Optima Health Case Manager.
Please feel free to visit www.progenyhealth.com for more information.
149

150

The Optima Health Cardiovascular Disease
Management program provides you with information to help keep your coronary artery disease (CAD) and/or congestive heart failure (CHF) under the best possible control. Members are encouraged to work with their physician to develop and stick with a treatment plan. If you have been diagnosed with CAD and/or CHF, you may be eligible to earn incentive points by participating in the program (see reverse side for program eligibility).
Criteria for Medical Program Participation
• Member is currently in active treatment for CAD or CHF
• Visit with physician at least once a year
• Obtain annual testing of LDL cholesterol levels and blood pressure
• Development of a CAD or CHF management plan and an appropriate nutrition and activity plan
To get started, contact Optima Health
at 1-866-503-2730
This program begins on January 1 and ends on December 31. Employees enrolling in the program after the end of the first quarter will be accepted but will not be able to complete the program in its entirety.
Earn 3,000 Virgin Pulse points
towards your BEWell program.
Points may be earned semi-annually for participating in the Optima Health Disease Management programs and completing the program requirements.
• Enrollment in program and first contact with Optima Health Coach
• Contact with Optima Health Coach at least every three months
• Compliance with medication (if applicable) during the first and second six months of the program
• Completion of Criteria for Medical Program Participation (listed to the left)
See reverse side for program eligibility.
VIRGINIA BEACH CITY & SCHOOL’S BEWELL
Cardiovascular
Disease Management
Program
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.151

VIRGINIA BEACH CITY & SCHOOL’S BEWELL
Cardiovascular
Disease Management
Program Eligibility
The following are eligible to participate in Disease Management programs:
• Full-time City employees enrolled in the COVB Optima Health Plan
• Full-time and full-time equivalent School employees enrolled in the VBCPS Optima Health Plan
• Retirees who are enrolled in the COVB/VBCPS Optima Health Plan
• Part-time/Temporary City and School employees enrolled in the COVB/VBCPS Optima Health Plan. (Note: Part-time/temporary employees are not eligible to earn BEWell Program points or incentives)
• Spouses enrolled in the COVB/VBCPS Optima Health Plan. (Note: Spouses are not eligible to earn BEWell Program points or incentives)
VIRGINIA BEACH CITY & SCHOOL’S BEWELL
v0818Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.152

The Optima Health Diabetes Disease
Management program provides you with information to help keep your diabetes under the best possible control. Members are encouraged to work with their physician to develop and stick with a treatment plan. If you have been diagnosed with diabetes, you may be eligible to earn incentive points by participating in the program (see reverse side for program eligibility).
Criteria for Medical Program Participation
• Member is currently in active treatment for diabetes
• Visit with physician at least once a year
• Obtain twice yearly A1c testing
• Obtain annual urine microalbumin and LDL cholesterol testing, a dilated eye exam, and regular foot exams
• Development of a diabetes management plan and an appropriate nutrition and activity plan
• Speak with an Optima Health Coach at least once every three months
To get started, contact Optima Health
at 1-866-503-2730
This program begins on January 1 and ends on December 31. Employees enrolling in the program after the end of the first quarter will be accepted but will not be able to complete the program in its entirety.
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
VIRGINIA BEACH CITY & SCHOOL’S BEWELL
Diabetes
Disease Management
Program
Earn 3,000 Virgin Pulse points
towards your BEWell program.
Points may be earned semi-annually for participating in the Optima Health Disease Management programs and completing the program requirements.
• Enrollment in program and first contact with Optima Health Coach
• Contact with Optima Health Coach at least every three months
• Compliance with medication (if applicable) during the first and second six months of the program
• Completion of Criteria for Medical Program Participation (listed to the left)
Note: Earn reduced copayments on diabetic medications when meeting all program criteria.
See reverse side for program eligibility.
153

VIRGINIA BEACH CITY & SCHOOL’S BEWELL
Diabetes
Disease Management
Program Eligibility
The following are eligible to participate in Disease Management programs:
• Full-time City employees enrolled in the COVB Optima Health Plan
• Full-time and full-time equivalent School employees enrolled in the VBCPS Optima Health Plan
• Retirees who are enrolled in the COVB/VBCPS Optima Health Plan
• Part-time/Temporary City and School employees enrolled in the COVB/VBCPS Optima Health Plan. (Note: Part-time/temporary employees are not eligible to earn BEWell Program points or incentives, including the copayment reduction on diabetic medications)
• Spouses enrolled in the COVB/VBCPS Optima Health Plan. (Note: Spouses are not eligible to earn BEWell Program points or incentives, including the copayment reduction on diabetic medications)
VIRGINIA BEACH CITY & SCHOOL’S BEWELL
v0818Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.154

The Optima Health Respiratory Disease
Management program provides you with information to help keep your asthma and/or COPD under the best possible control. Members are encouraged to work with their physician to develop and stick with a treatment plan.
If you have been diagnosed with asthma and/or COPD, you may be eligible to earn incentive points by participating in the program (see reverse side for program eligibility).
Criteria for Medical Program Participation
• Member is currently in active treatment for asthma or COPD
• Visit with physician at least once a year
• Speak with an Optima Health Coach at least once every three months
• Development of an asthma or COPD management plan and an appropriate nutrition and activity plan
To get started, contact Optima Health
at 1-866-503-2730
This program begins on January 1 and ends on December 31. Employees enrolling in the program after the end of the first quarter will be accepted but will not be able to complete the program in its entirety.
VIRGINIA BEACH CITY & SCHOOL’S BEWELL
Respiratory
Disease Management
Program
Earn 3,000 Virgin Pulse points
towards your BEWell program.
Points may be earned semi-annually for participating in the Optima Health Disease Management programs and completing the program requirements.
• Enrollment in program and first contact with Optima Health Coach
• Contact with Optima Health Coach at least every three months
• Compliance with medication (if applicable) during the first and second six months of the program
• Completion of Criteria for Medical Program Participation (listed to the left)
See reverse side for program eligibility.
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.155

VIRGINIA BEACH CITY & SCHOOL’S BEWELL
Respiratory
Disease Management
Program Eligibility
The following are eligible to participate in Disease Management programs:
• Full-time City employees enrolled in the COVB Optima Health Plan
• Full-time and full-time equivalent School employees enrolled in the VBCPS Optima Health Plan
• Retirees who are enrolled in the COVB/VBCPS Optima Health Plan
• Part-time/Temporary City and School employees enrolled in the COVB/VBCPS Optima Health Plan. (Note: Part-time/temporary employees are not eligible to earn BEWell Program points or incentives)
• Spouses enrolled in the COVB/VBCPS Optima Health Plan. (Note: Spouses are not eligible to earn BEWell Program points or incentives)
VIRGINIA BEACH CITY & SCHOOL’S BEWELL
v0818Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.156

The Optima Health Partners in
Pregnancy program provides you with information and support about making good choices throughout your pregnancy—whether this is your first pregnancy, or your last.
We are dedicated to providing guidance, support, and education to expectant moms. Partners in Pregnancy provides access to experienced pregnancy and childbirth nurses, clinical case managers, licensed social workers, and service coordinators to help you:
• Maintain good health throughout your pregnancy
• Develop a healthy nutrition and activity plan
• Maximize your benefits and resources
• Locate important resources, classes, and services
• Coordinate prenatal care and appropriate risk screenings
• Understand timely health tips, mailed directly to your home
To get started, contact Optima Health at 1-866-239-0618
Earn 3,000 Virgin Pulse points
towards your BEWell program.
Points may be earned semi-annually for participating in the Optima Health Partners in Pregnancy program and completing the program requirements.
• Enrollment in program and first contact with Optima Health Coach within the first three months of pregnancy (14 weeks)
• Visit your OB doctor within the first three months of pregnancy (14 weeks)
• Maintain monthly contact with your Optima Health Coach during your pregnancy
• Visit your doctor for a postpartum checkup within six weeks after delivery
Note: Your health plan pays for a breast pump if you are pregnant. See reverse side for details.
See reverse side for program eligibility.
VIRGINIA BEACH CITY & SCHOOL’S BEWELL
Partners in
Pregnancy Program
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.157

VIRGINIA BEACH CITY & SCHOOL’S BEWELL Partners in Pregnancy
Program Eligibility
The following are eligible to participate in Disease Management programs:
• Full-time City employees enrolled in the COVB Optima Health Plan
• Full-time and full-time equivalent School employees enrolled in the VBCPS Optima Health Plan
• Retirees who are enrolled in the COVB/VBCPS Optima Health Plan
• Part-time/Temporary City and School employees enrolled in the COVB/VBCPS Optima Health Plan. (Note: Part-time/temporary employees are not eligible to earn BEWell Program points or incentives)
• Spouses enrolled in the COVB/VBCPS Optima Health Plan. (Note: Spouses are not eligible to earn BEWell Program points or incentives)
Breast Pumps
Your health plan pays for a breast pump if you are pregnant.
• Hand breast pumps or non-hospital grade electric breast pumps are covered at 100% (no copayment or co-insurance) and can be purchased from:
» a Durable Medical Equipment store,
» a lactation specialist,
» a physician’s office,
» a pharmacy,
» LaLeche League, or
» any retail store.
• Breast pumps can also be ordered from Home Care Delivered by calling 1-800-867-4412.
The cost will be reimbursed through Optima Health by filing a claim with a receipt. Please note, the healthplan does not cover shipping, handling, or taxes. No authorization is necessary if the purchased breast pump is under $750.00.
VIRGINIA BEACH CITY & SCHOOL’S BEWELL
v0818Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.158

The AccordantCareTM Program from Optima
Health and Accordant Health Services provides you with an extra layer of healthcare support if you are living with any one of these chronic conditions:
• Amyotrophic Lateral Sclerosis (ALS, Lou Gehrig’s Disease)
• Chrohn’s Disease
• Chronic Inflammatory Demyelinating Polyradiculoneuropathy (CIPD)
• Cystic Fibrosis (CF)
• Dermatomyositis
• Epilepsy Disorders (seizures)
• Gaucher Disease
• Hemophilia
• Multiple Sclerosis (MS)
• Myasthenia Gravis (MG)
• Parkinson’s Disease (PD)
• Polymyositis
• Rheumatoid Arthritis (RA)
• Scleroderma
• Sickle Cell Disease (SCD)
• Systemic Lupus Erythematosus (SLE or Lupus)
• Ulcerative Colitis
To get started, call AccordantCare at
1-866-535-5439 or visit accordant.com.
A team of nurses is waiting to talk with you and answer your questions by phone or email, 24/7.
The AccordantCare Program can:
• Provide tips on how to manage your health and your busy life.
• Help you find ways to save money. Live well and still get the care you need, while cutting costs.
• Help you learn how to make the most of every visit with your doctor.
• Help you connect to resources near your home.
VIRGINIA BEACH CITY & SCHOOL’S BEWELL
AccordantCareTM
Program
Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.
Earn 3,000 Virgin Pulse points
towards your BEWell program.
Points may be earned semi-annually for participating in the AccordantCare program and completing the program requirements.
See reverse side for program eligibility.
159

VIRGINIA BEACH CITY & SCHOOL’S BEWELL AccordantCareTM Program
Program Eligibility
The following are eligible to participate in Disease Management programs:
• Full-time City employees enrolled in the COVB Optima Health Plan
• Full-time and full-time equivalent School employees enrolled in the VBCPS Optima Health Plan
• Retirees who are enrolled in the COVB/VBCPS Optima Health Plan
• Part-time/Temporary City and School employees enrolled in the COVB/VBCPS Optima Health Plan. (Note: Part-time/temporary employees are not eligible to earn BEWell Program points or incentives)
• Spouses enrolled in the COVB/VBCPS Optima Health Plan. (Note: Spouses are not eligible to earn BEWell Program points or incentives)
VIRGINIA BEACH CITY & SCHOOL’S BEWELL
v0818Optima Health is the trade name of Optima Health Plan, Optima Health Insurance Company, and Sentara Health Plans, Inc.160

4417 Corporation LaneVirginia Beach, VA 23462
optimahealth.com/members