basic fluids and electrolytes douglas p. slakey. why listen to this? essential for surgeons based...
TRANSCRIPT

Basic Fluids and Electrolytes
Douglas P. Slakey

Why Listen to This?• Essential for surgeons• Based upon physiology
– Disturbances understood as pathophysiology
Most abnormalities are relatively simple, and many iatrogenic



Purpose of this Talk
To Encourage Thought
Not
Mechanical Reaction

You Have to Read!
It’s All About Balance
• Gains and Losses– Losses
• Sensible and Insensible
• Typical adult, typical day– Skin 600 ml
– Lungs 400 ml
– Kidneys 1500 ml
– Feces 100 ml
• Balance can be dramatically impacted by illness and medical care

Fluid Compartments
• Total Body Water– Relatively constant– Depends upon fat content and varies with age
• Men 60% (neonate 80%, 70 year old 45%)
• Women 50%

TOTAL BODY WATERTOTAL BODY WATER60% BODY WEIGHT60% BODY WEIGHT
ICF
2/3
Predominant solute
K+
ECF
1/3
Predominant solute
Na+
HH22OO

(mEq/L) Plasma IntracellularNa 140 12K 4 150Ca 5 0.0000001Mg 2 7Cl 103 3
HCO3 24 10Protein 16 40
Electrolytes
Fluid Movement
• Is a continuous process• Diffusion
– Solutes move from high to low concentration
• Osmosis– Fluid moves from low to high solute concentration.
• Active Transport– Solutes kept in high concentration compartment– Requires ATP

Movement of Water• Osmotic activity
– Most important factor– Determined by concentration of solutes
Plasma (mOsm/L)
2 X Na + Glc + BUN
18 2.8

Third Space
• Abnormal shifts of fluid into tissues
• Not readily exchangeable
• Etiologies– Tissue trauma– Burns– Sepsis

Fluid Status• Blood pressure
• Check for orthostatic changes
• Physical exam
• Invasive monitoring– Arterial line– CVP– PA catheter– Foley
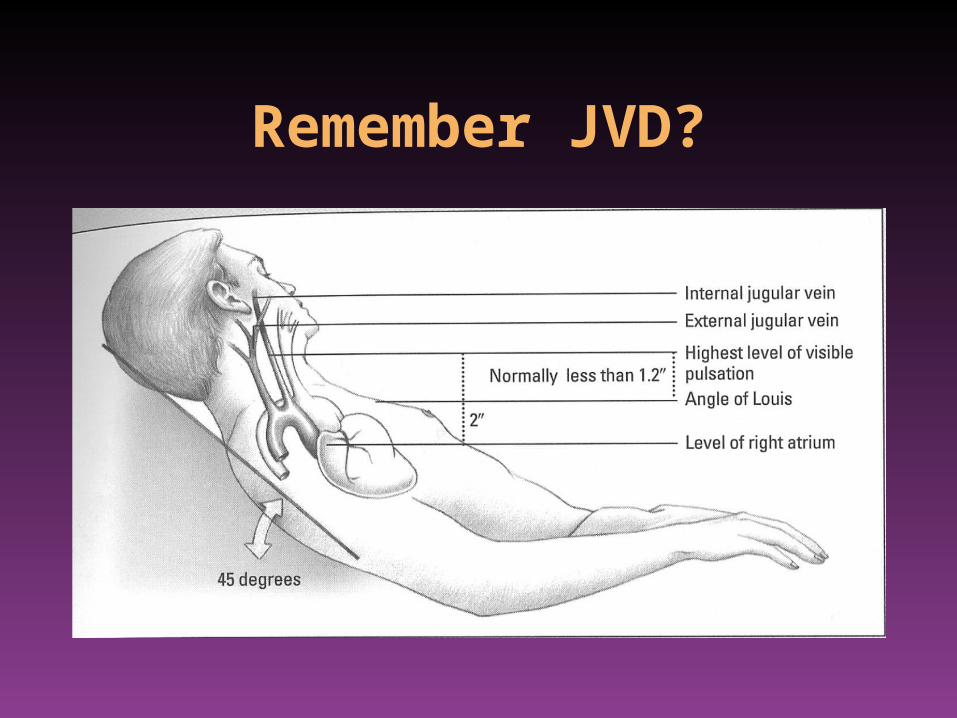
Remember JVD?

Fluid Imbalances
• Must assess organ function– Renal failure– Heart failure– Respiratory failure• Excessive GI fluid losses• Burns

Volume Deficit
• Most common surgical disorder• Signs and symptoms
– CNS: sleepiness, apathy, reflexes, coma– GI: anorexia, N/V, ileus– CV: orthostatic hypotension, tachycardia with
peripheral pulses– Skin: turgor– Metabolic: temperature

Dehydration
Chronic Volume Depletion
Affects all fluid components
Solutes become concentrated
Increased osmolarity
Hct can increase 6-8 pts for 1 L deficit
Patients at risk:
Cannot respond to thirst stimuli
Diabetes insipidus
Treatment: typically low Na fluids

HypovolemiaAcute Volume Depletion
Isotonic fluid loss, from extracellular compartmentDetermine etiology
Hemorrhage, NG, fistulas, aggressive diuretic therapyThird space shifting, burns, crush injuries, ascites
Replace with blood/isotonic fluid» Appropriate monitoring
» Physical Exam» Foley (u/o > 0.5 ml/kg/min)» Hemodynamic monitoring

Fluid Replacement

Fluid Replacement
• Isotonic/physiologic– NS, LR
• Less concentrated– 0.45NS, 0.2NS– Maintenance
• Hypertonic Na

Fluid Replacement
• Plasma Expanders– For special situations– Will increase oncotic pressure– If abnormal microvasculature, will extravasate
into “third space”Then may take a long time to return to circulation
Fluid Replacement
• Maintenance– 4,2,1 “rule”
• Other losses (fistulas, NG, etc)– Can measure volume and composition!!!– Should be thoughtfully assessed and
prescribed separately if pathologic
Maintenance Fluid
• Daily Na requirement: 1 to 2 mEq/kg/day
• Daily K requirement: 0.5 to 1 mEq/kg/day
• AHA Recommended Na intake: 4 to 6 grams per day

Maintenance Fluids
To Replace Ongoing Losses,
NOT Pre-existing Deficits
Maintenance Fluids
D5 0.45NS + 20 mEq KCl/L at 125 ml/H

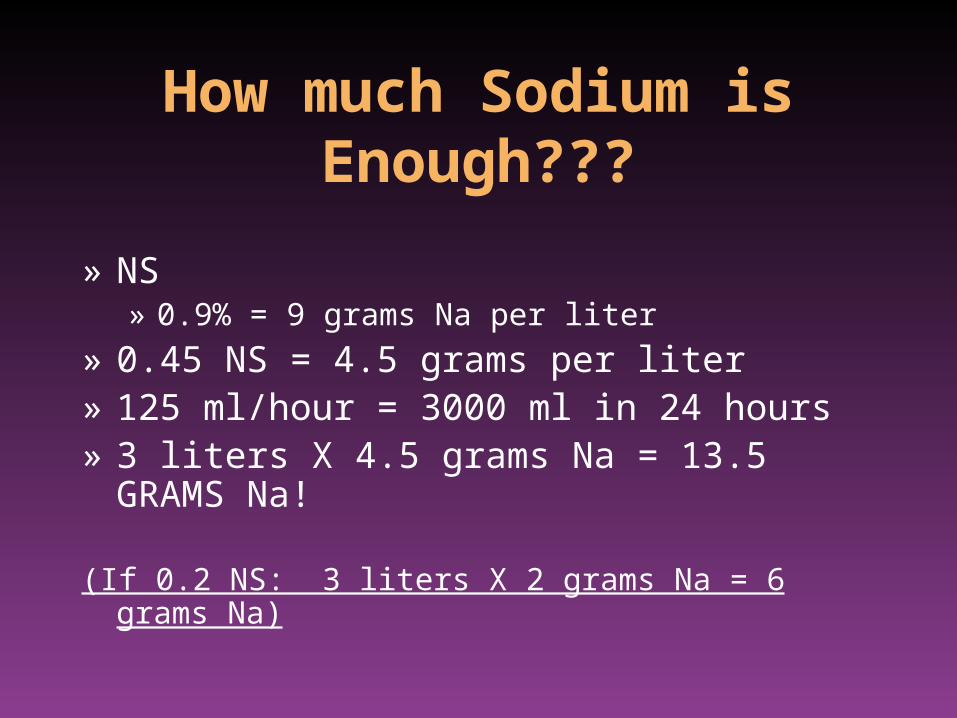
How much Sodium is Enough???
» NS» 0.9% = 9 grams Na per liter
» 0.45 NS = 4.5 grams per liter» 125 ml/hour = 3000 ml in 24 hours» 3 liters X 4.5 grams Na = 13.5 GRAMS Na!
(If 0.2 NS: 3 liters X 2 grams Na = 6 grams Na)

Assessment of Disorders of Volume
and Electrolytes• Effects are variable and complex
• Simplified treatment algorithms cannot address the variable and complex nature of these disorders
• Acid - Base balance is integral with these disorders

Hyponatremia• Na loss
– True loss of Na– Dilutional (water excess)– Inadequate Na intake
• Classified by extracellular volume– Hyovolemic (hyponatremia)
• Diuretics, renal, NG, burns
– Isotonic (hyponatremia)• Liver failure, heart failure, excessive hypotonic IVF
– Hypervolemic (hyponatremia)• Glucocorticoid deficiency, hypothyroidism

Na Volume
Check Ur Na
< 10 mmol/L
VomitingDiarrhea3rd spaceHepatorenal
Adrenal InsufficiencyDiureticsSalt-Wasting SyndromeSIADH
> 20 mmol/L

SIADH• Causes
– Cancers (pancreas, oat cell)– CNS (trauma, stroke)– Pulmonary (tumors, asthma, COPD)– Surgical stress– Medications
• Anticonvulsants, antineoplastics, antipsychotics, sedatives (morphine)
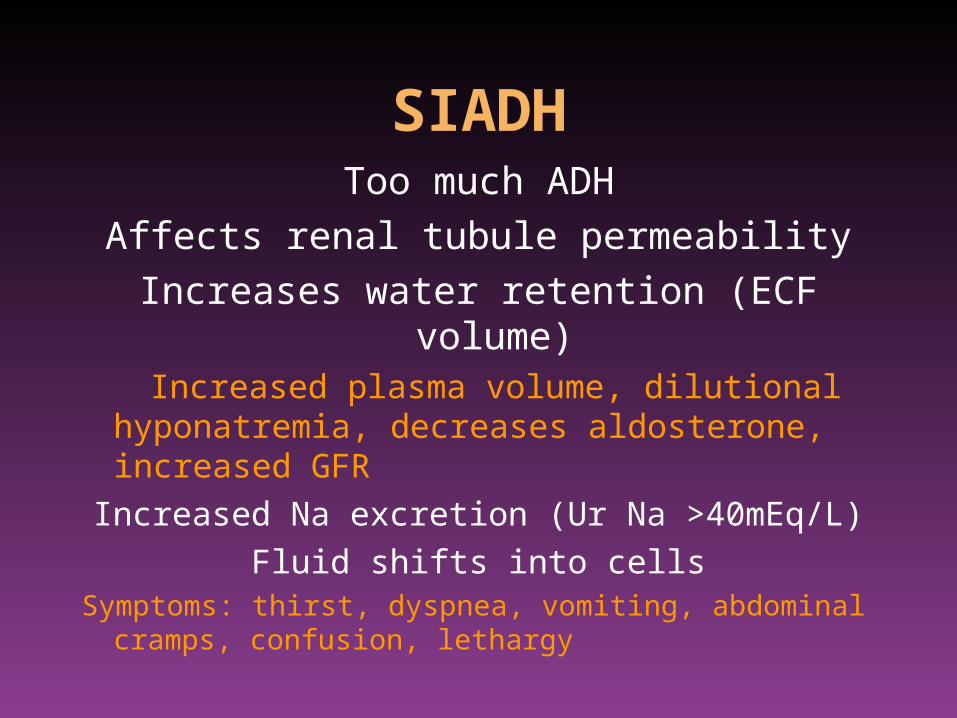
SIADHToo much ADH
Affects renal tubule permeability
Increases water retention (ECF volume) Increased plasma volume, dilutional hyponatremia,
decreases aldosterone, increased GFR
Increased Na excretion (Ur Na >40mEq/L)
Fluid shifts into cellsSymptoms: thirst, dyspnea, vomiting, abdominal cramps,
confusion, lethargy

SIADH Treatment
• Fluid restriction– Will not responded to fluid challenge
(distinguishes from pre-renal cause)
• Possibly diuretics


Hypovolemia and Metabolic Abnormality
• Acidosis– May result from decreased perfusion
• Alkalosis– Complex physiologic response to more chronic
volume depletion

Paradoxical Aciduria
Na
Cl
Na
H
K
Loop of Henle
HypochloremicHypovolemia
Hypernatremia
Relatively too little H2O
– Free water loss (burns, fever)– Diabetes insipidus (head trauma, surgery,
infections, neoplasm)• Dilute urine
– Nephrogenic DI• Kidney cannot respond to ADH

Hypernatremia
• Hypovolemic– GI loss, osmotic diuresis– Increased Na load (usually iatrogenic)
[0.6 X wt (kg)] X [Serum Na/140 - 1]
Free water deficit:
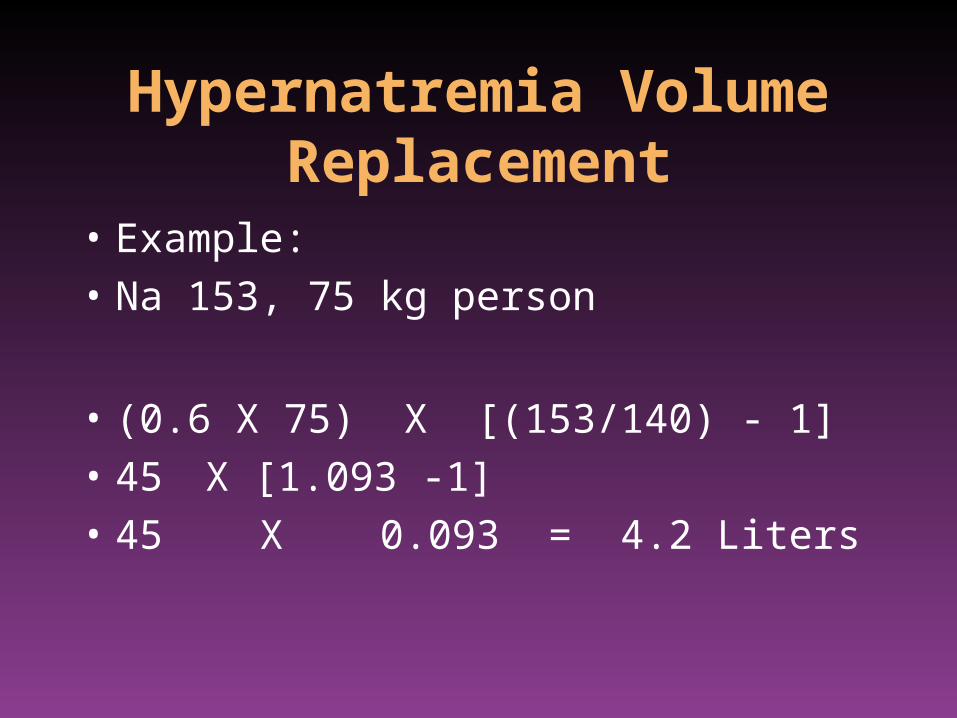
Hypernatremia Volume Replacement
• Example:
• Na 153, 75 kg person
• (0.6 X 75) X [(153/140) - 1]
• 45 X [1.093 -1]
• 45 X 0.093 = 4.2 Liters

Potassium
• 98% intracellular• 20 to 40 mEq/L of urine
– Kidneys cannot retain K
• Dietary sources– Chocolate, dried fruits, nuts– Fruits: oranges, bananas, apricots– Meats– Potatoes, mushrooms, tomatoes, carrots
Potassium and Ph
• Acidosis– Extracellular H+ increases, moves intracellular
forcing K+ extracellular
• Alkalosis– Intracellular H+ decreases, to keep intracellular
fluid neutral, K+ moves into cells

Hyperkalemia
• Associated medications– ACE inhibitors, beta-blockers, antibiotics,
chemotherapy, NSAIDS, spironolactone
• Treatment– Mild: dietary restriction, assess medications– Moderate: Kayexalate
• Do NOT use sorbitol enema in renal failure patients

Hyperkalemia
• Emergency (> 6 mEq/l)
• Treatment– Monitor ECG, VS– Calcium gluconate IV– Insulin and glucose IV– Kayexalate, Lasix + IVF, dialysis

