water and electrolytes disturbances
DESCRIPTION
University of Medicine and Pharmacy, Iasi School of Medicine ANESTHESIA and INTENSIVE CARE Conf. Dr. Ioana Grigoras. MEDICINE 4 th year English Program Suport de curs. WATER AND ELECTROLYTES DISTURBANCES. PHYSIOLOGY. Body water = 55-60% of body weight Water distribution : - PowerPoint PPT PresentationTRANSCRIPT
WATER AND ELECTROLYTES DISTURBANCES
University of Medicine and Pharmacy, IasiSchool of MedicineANESTHESIA and INTENSIVE CAREConf. Dr. Ioana Grigoras
MEDICINE4th year
English ProgramSuport de curs

PHYSIOLOGY
Body water= 55-60% of body weight
Water distribution:– Intracellular water – 66% of total (2/3)
– Extracellular water – 33% of total (1/3)
– Intracellular water – 40% of body weight– Extracellular water – 20% of body weight
• Intravascular water (volemia) - 5% of body weight
• Interstitial water - 15% of body weight


WATER DISTRIBUTION Variation according to gender

PHYSIOLOGY Electrolytic composition of water compartments
~ 300~ 300
66
214Proteins
11Phosphat
2727HCO
110103Cl
11Mg
2,52,5Ca
55K
142142Na
Interst CIntravasc C
~ 300~ 300
-6Org. acids
8014Proteins
551Phosphat
1027HCO
0-5103Cl
131Mg
-2,5Ca
1505K
15142Na
Intracell CExtracell C.
Org. acids

WATER AND ELECTROLYTES BALANCE Evaluation
CLINICAL EVALUATION :– History
• Water and salt ingestion• Losses• Thurst
– Skin and mucous membranes examination • Oral mucosae humidity• Skin humidity• Skin colour and temperature• Cutaneous turgor
– Body weight– Respiratory system clinical exam
• Polypneea• Crackles at lung bases
– Clinical examination of peripheral veins– Haemodynamic parameters
• Arterial blood pressure • Pulse wave amplitude• Orthostatic challenge• CVP,...
– Urinary outflow– Evaluation of the counscience level

Clinical evaluation of
the intravascular compartment:– thurst
– BP, heart rate, orthostatic challenge
– central venous pressure
– pulmonary capillary wedge pressure, cardiac output
– organ function:• conscience
• urinary flow
• tissue perfusion
WATER AND ELECTROLYTES BALANCE
Evaluation

Clinical evaluation of
interstitial space:
unreliable– skin and mucous membrane examination
• colour
• humidity
• turgour
• edema
WATER AND ELECTROLYTES BALANCE
Evaluation

Clinical examination of intracellular compartment:
unreliable
– thurst– mental status disturbances– neurological signs
WATER AND ELECTROLYTES BALANCE
Evaluation
LABORATORY EVALUATION– Hematocrit and total proteins
– Blood and urinary electrolytes measurement
– Blood and urinary osmolarity
– ECG
WATER AND ELECTROLYTES BALANCE
Evaluation

OSMOLARITY• Plasma osmolarity =
the sum contributions of all osmotic active substances
• The main plasma osmotic active substances: Na, glucose, ureea
• Plasma osmolarity– measured osmolarity– estimated (calculated) osmolarity
• Calculated osmolarity = Na-mia x 2 + blood glucose/18 +ureea/2,8
Intracellular volume disturbances are the consequences of
effective osmotic pressure variation

WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)

WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)

VOLUME CONTRACTION

CLASSIFICATION OF HYPOVOLEMIC SHOCK
Class I Class II Class III Class IV
Blood loss- ml < 750ml 750-1500ml 1500-2000ml >2000ml
Blood loss-% <15% 15-30% 30-40% >40%
Pulse rate <100/min < 100/min 120-140/min >140/min
TA N N
Plus wave amplitude
N
Capillary refill N + + +
Respiratory rate 14-20/min 20-30/min 30-40/min >40/min
Urinary output >30ml/oră Oliguria Oligoanuria Anuria
Mental status Mild anxiety Anxiety Confused Lethargy

PRINCIPLES of TREATMENT• Treatment of causative disease • STOP THE LOSSES• Volume replacement

• Volume replacement– Routes of volume administration
– Solutions for volume replacement
– Rhythm of administration
– Monitorization of volume replacement efficiency

WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)
VOLUMEEXPANTION
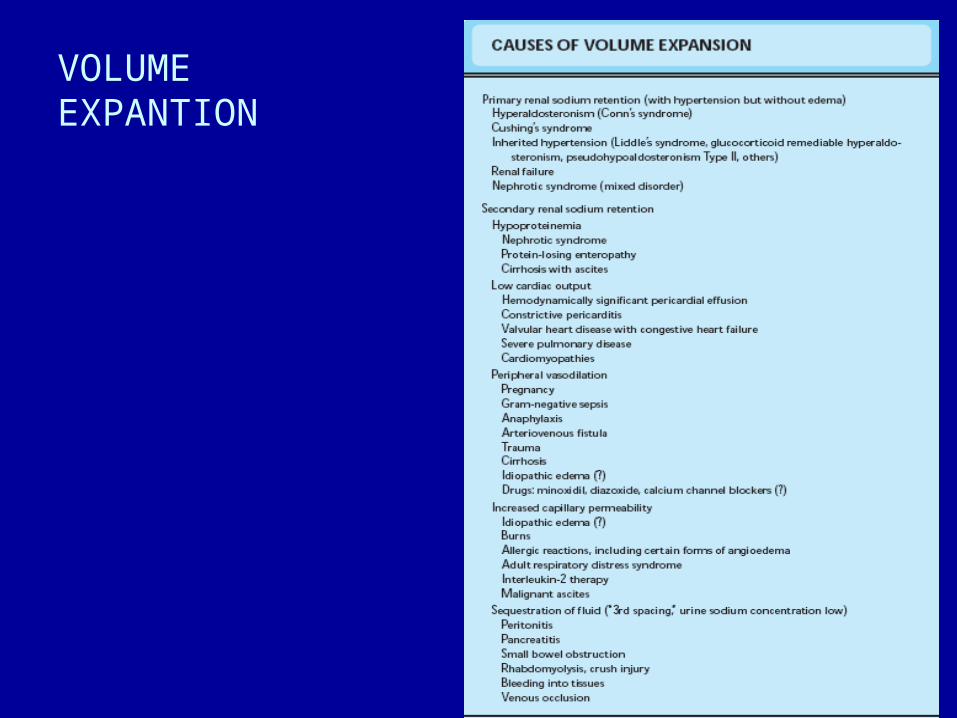
VOLUME EXPANTION

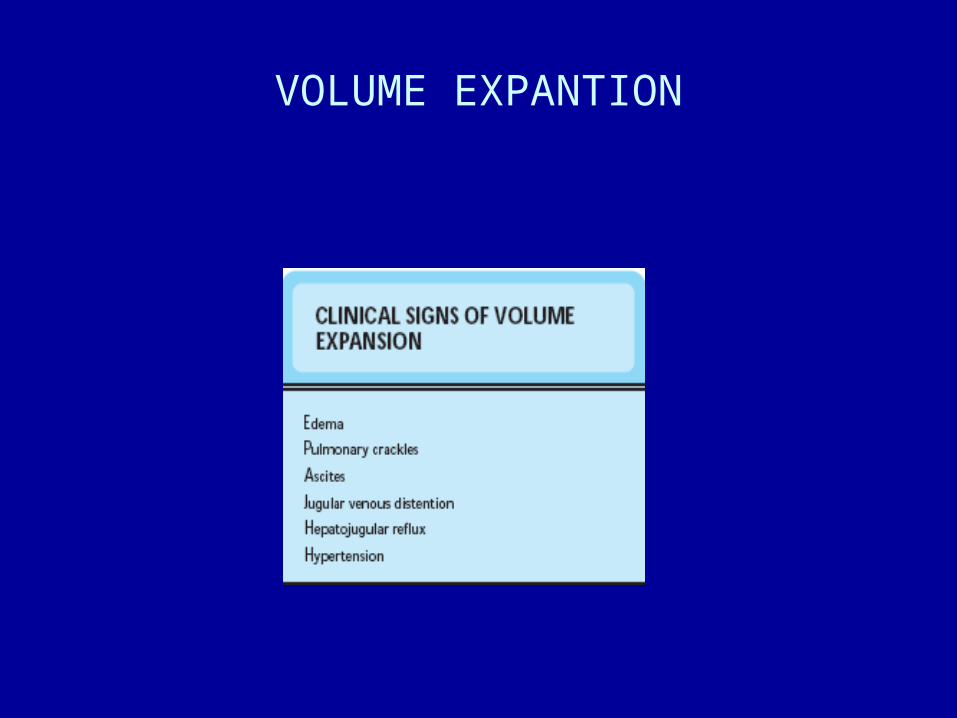
VOLUME EXPANTION
PRINCIPLES of TREATMENT
• Treatment of causative disease
• Limitation of water intake
• Diuretics

WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)

SODIUM DISTURBANCES
• Plasma sodium concentration =
extracellular water – sodium ratio
• Na-mia is not a predictor of intravascular volume

SODIUM DISTURBANCES
WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)

HYPERNATREMIANa-mia > 145mEq/l
• Physiological effects– Extracellular hyperosmolarity– Water movement out of the cell– Preservation of extracellular volume despite losses– Intracellular volume contraction

HYPERNATREMIANa-mia > 145mEq/l
HYPERNATREMIANa-mia > 145mEq/l
• Clinical picture– Clinical signs of intracellular volume contraction –
neurological signs– Restlessness, iritability, letargia, hyporeflexia,
coma, convultions– High mortality, neurological sequelae

HYPERNATREMIANa-mia > 145mEq/l

HYPERNATREMIANa-mia > 145mEq/l
• Treatment – Water administration in order to correct
hyperosmolarity– When clinical signs of extracellular volume
contraction (hypovolemia) are present, isotonic solution should be given untill correction of intravascular volume
– Calculation of water deficit0,6 x kg x (Na actual / 140 – 1)
– Speed of correction NO > 2mEq/hour
HYPERNATREMIANa-mia > 145mEq/l
CLASSIFICATION– HYPOVOLEMIC
• Water and Na deficit• Deficit of water > Na • Body total amount of Na
False hypernatremia– ISOVOLEMIC
• Water deficit • Body total amount of Na - normal
– HYPERVOLEMIC• Water and Na excess• Excess of Na > water • Body total amount of Na ↑
True hypernatremia

HYPOVOLEMIC HYPERNATREMIA Total body Na
MECHANISM- Water and Na deficit; deficit of water > Na; body total amount of Na
CAUSES– Extrarenal losses
• Skin losses (profuse sweating)• Digestive losses (cholera, infant diarrheea)
– Renal losses• osmotic diuresis• excess of diuretics• polyuria
DIAGNOSTIC– Clinical signs of extracellular volume contraction – Na urinary < 10mEq/l – extrarenal losses– Na urinary > 20mEq/l – renal losses
TREATMENT– Water and sodium administrationin isotonic proportions until correction of
hypovolemia; hypotonic solution (NaCl 0,45%)
ISOVOLEMIC HYPERNATREMIA total body Na normal
MECHANISM– water deficit; total body Na normal
CAUSES– Extrarenal losses
• Skin losses (profuse sweating)• Respiratory losses (tachypnea, mechanical ventilation)
– Renal losses • Central diabetes insipidus • Nephrogenic diabetes insipidus • Hypodipsia (decreased water intake)
DIAGNOSTIC– Signs: fever, oliguria, azotemia, drowsiness, coma, convultions– hypotension (late finding)– variable urinary Na
TREATMENT– Increased water intake (NaCl 0,45%,)

ISOVOLEMIC HYPERNATREMIA

ISOVOLEMIC HYPERNATREMIA

HYPERVOLEMIC HYPERNATREMIA total body Na ↑
MECHANISM– water excess; total body Na ↑
CAUSES– excess administration of hypertonic saline (NaCl 7,5%)
– Na bicarbonate administration
– Salt water drowning
DIAGNOSTIC– Signs of extracellular volume expansion
– Signs of intracellular volume contraction
TREATMENT– Diuretics
– Increased water intake

WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)

HYPONATREMIANa-mia < 135mEq/l
• Physiological effects– Extracellular hypoosmolarity– Water movement towards the cell– Signs of intracellular volume expansion

HYPONATREMIANa-mia < 135mEq/l
• Clinical picture– Dominated by neurological signs (cerebral edema)– Letargy, apatia, drowsiness, anorexia, nausea,
agitation, hyporeflexia, hypothermia, convulsions– Signs severity depends upon:
• severity of hypoNa-miei (Na < 120mEq/l)
• speed of hypoNa-mia occurrence (acute/chronic)

HYPONATREMIA

Speed of hypoNa-mia occurrence

HYPONATREMIA
• Treatment – Correction of extracellular osmolarity and water
excess removal– Speed of correction depens upon:
• severity of hypoNa-mia• prezence/absence of symptoms• speed of occurrence (acute/chronic)
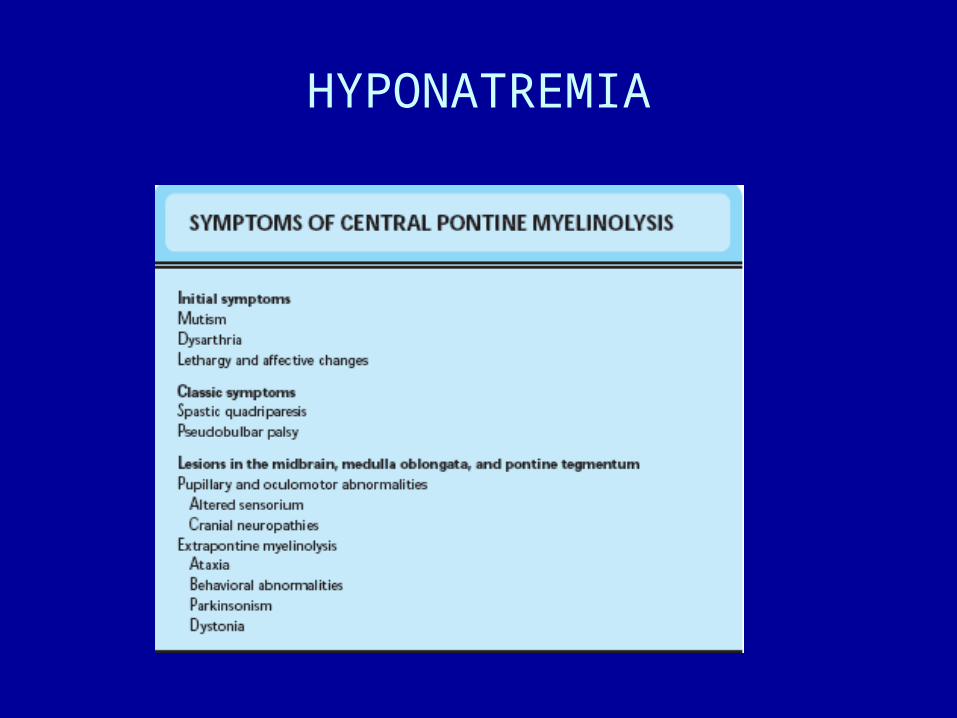
– Rapid correction of chronic hypoNa-mia – pontine mielinolysis (irreversible sequelae)
– In the prezence of symptoms, rapid correction until Na-mie 120mEq/l, than slow correction

HYPONATREMIA

HYPONATREMIA

HYPONATREMIANa-mia < 135mEq/l
CLASSIFICATION– Hypovolemic
• Water and Na deficit• Deficit of Na > water• Total body Na
True hyponatremia
– Isovolemic • Water excess of extracellular compartment• Total body Na - normal
Dilutional hyponatremia / Pseudohyponatremia
– Hypervolemic• Water and Na excess• Excess of water > Na• Total body Na ↑
Dilutional hyponatremia
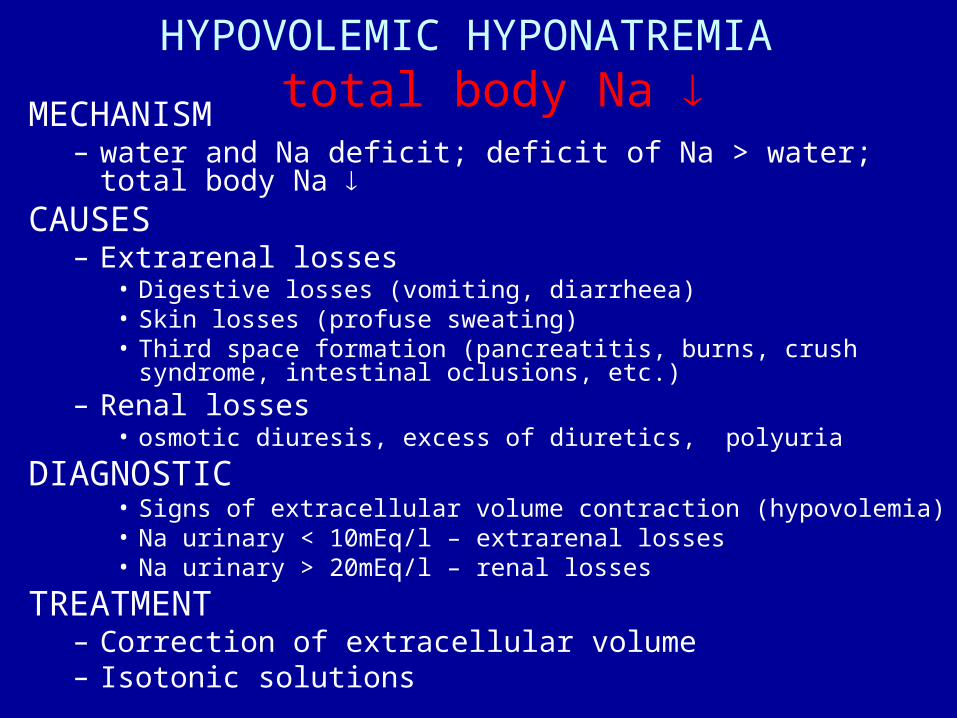
HYPOVOLEMIC HYPONATREMIA total body Na
MECHANISM– water and Na deficit; deficit of Na > water; total body Na
CAUSES– Extrarenal losses
• Digestive losses (vomiting, diarrheea)• Skin losses (profuse sweating)• Third space formation (pancreatitis, burns, crush syndrome, intestinal
oclusions, etc.)– Renal losses
• osmotic diuresis, excess of diuretics, polyuria
DIAGNOSTIC• Signs of extracellular volume contraction (hypovolemia)• Na urinary < 10mEq/l – extrarenal losses• Na urinary > 20mEq/l – renal losses
TREATMENT– Correction of extracellular volume– Isotonic solutions

ISOVOLEMIC HYPONATREMIA total body Na normal
MECHANISM– water excess of the extracellular space; total body Na normal
CAUSES– Syndrome of inappropiate antidiuretic hormone secretion (SIADH)
– Fear, excitement, pain, drugs, surgical procedures
– Hyperosmolar states (hyperglycemia, intoxications)
DIAGNOSTIC– Extracellular water excess; no clinical signs
– Na urinary > 20mEq/l
TREATMENT– Water restriction

ISOVOLEMIC HYPONATREMIA

HYPERVOLEMIC HYPONATREMIA total body Na ↑
MECHANISM– Excess of water and Na; excess of water > Na; total body Na ↑
CAUSES– Edematous syndromes (cardiac failure, liver cirhosis, nephrotic
syndrome)– Acute and chronic renal failure
DIAGNOSTIC– Signs of extracellular volume expansion (edema)– Na urinary < 10mEq/l in edematous syndromes– Na urinar > 20mEq/l in renal failure
TREATMENT– Water (and salt) restriction

WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)

POTASIUM• Body K distribution
• 98% intracellular – 150-160mEq/l• 2% extracellular – 3,5-5mEq/l
The main intracellular cation• Intracellular functions
» Cell volume regulation» Intracellular pH regulation» Proteins and glycogen synthesis» Cell grow regulation» Cell enzymes activation» Rest potential of cell membrane
The main function membrane potential

POTASIUM DISTURBANCES
• Factors which influence K intercompartmental distribution:
– Serum K
– pH: acidosis or alcalosis
– Hyperosmolarity
– Hormons: insulin and catecholamines
• Factors which influence K urinnary excretion:– Serum K level
– Aldosteron
– Urinay flow

Factors which influence K intercompartmental distribution

POTASIUM
Intercompartmental K movements according to pH
– Acidosis → extracellular H+ ↑ → H+ moves into cell
K+ moves out of cell
hyperpotasemia
– Alcalosis → extracellular H+ → H+ moves out of cell K+ moves into cell
hypopotasemia

HYPERPOTASEMIA
• Frequent causes of pseudohyperpotasemia:– Blood drawing: thin needles, intense negative
pressure (erythrocytes hemolysis, K release), garou, fist “pumping” (K muscle release), blood storage (erythrocytes K release);
– Leucocytosis / thrombocytosis - hyperpotasemia;

HYPERPOTASEMIACAUSES
– Increased K+ intake• enteral intake• parenterală intake
– K+ movement out of the cells• Metabolic acidosis• Hyperglycemia• Excessive excercise• Hypercatabolism• Drugs: β-blockers, succinilcholine, digitalis
– Decreased urinnary K+ ellimination• Hypovolemia• Hypoaldosteronism• Renal failure• Drugs: spironolactone, AINS, heparine

HYPERPOTASEMIA
CLINICAL PICTURE– Muscle signs
• paresthesia
• muscle weakness
• paralysis
– Cardiac signs• EKG signs
• Rhythm disturbances
• Dyastolic cardiac arrest

HYPERPOTASEMIA
HYPERPOTASEMIA
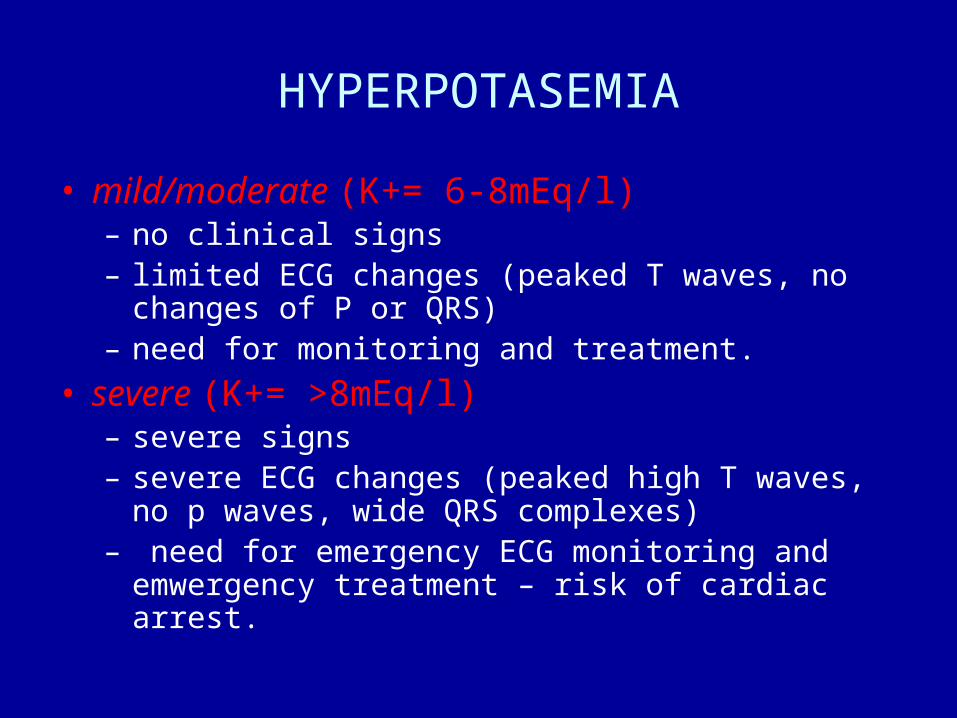
• mild/moderate (K+= 6-8mEq/l) – no clinical signs– limited ECG changes (peaked T waves, no changes of P or
QRS)– need for monitoring and treatment.
• severe (K+= >8mEq/l) – severe signs– severe ECG changes (peaked high T waves, no p waves,
wide QRS complexes)– need for emergency ECG monitoring and emwergency
treatment – risk of cardiac arrest.

HYPERPOTASEMIA
• ECG changes in hyperpotasemia:
• K+= 6-7mEq/l - peaked high T waves
• K+ =8-9mEq/l - absent P wave
• K+ =10mEq/l - wide QRS complex
• K+= 10-11mEq/l – biphasic QRST
• K+ =10-12mEq/l – ventricular fibrillation / dyastolic stillstand

ECG changes in hyperK-mie

HYPERPOTASEMIA
• Mild/modarate forms:• limitation /stop K intake • resins (ion chelation)• diuretics
• Severe forms:– emergency treatment – antagonization of membrane effects
and decreased plasma level by redistribution• calcium gluconate / chloride • Na bicarbonate• glucose + insulin
– K removal• resins• diuretics• hemodialysis
– stop K intake

HYPOPOTASEMIA
CAUSES– Normal total K – changes of intercompartmental distribution
• Respiratorie / metabolic alcalosis
– Low total K • Deceased intake
• Poor nutrition (alcoholics)
• Digestive losses– Vomiting, gastric fistulae, naso-gastric tube, …
– Diarrheea, laxatives
• Renal losses– Excess of mineralocorticoids – primary/secondary
– Diuretics
– Osmotic diuresis

HYPOPOTASEMIACLINICAL PICTURE
Changes of membrane potential • Neuro-muscle effects
– Parestesia– Muscle weakness– Hyporeflexia– Paralitic ileus
• Cardio-vascular effects – Changes of cardiac excitability– ECG changes– Enhancement of digoxin toxicity – Rhythm disturbances– HTA
• Vegetative effects– orthostatic hTA
• Hepatic effects– Aggravation of encephalopathy in liver cirhosis patients

HYPOPOTASEMIA
ECG ABNORMALITIES• Flat T wave
• U wave
• wide QRS complex
• ST depresion
• Atrial and ventricular rhythm disturbances

HYPOPOTASEMIA

HYPOPOTASEMIA
PROPHYLAXIS• Administration of K daily needs – 1mEq/kg day
TREATMENT• Correction of causative disease• K amount– depends upon severity of hypo-K
– K-mia > 3mEq/l – oral
– K-mia 2-3mEq/l – 10-20mEq/h
– K-mia < 2mEq/l – 20mEq iv + than 20mEq/h
ECG monitoring - mandatory