autoimmune disorders osama a. badary, phd clinical pharmacy department, faculty of pharmacy,
DESCRIPTION
Autoimmune Disorders Osama A. Badary, PhD Clinical Pharmacy Department, Faculty of Pharmacy, Ain Shams University, Cairo, Egypt. Immunity. Innate Immunity. Adaptive Immunity. Barriers (skin) Secretions (lysozyme) Complement Inflammation Granulocytes NK cells Macrophages - PowerPoint PPT PresentationTRANSCRIPT
Autoimmune Disorders
Osama A. Badary, PhD
Clinical Pharmacy Department,Faculty of Pharmacy,Ain Shams University,
Cairo, Egypt
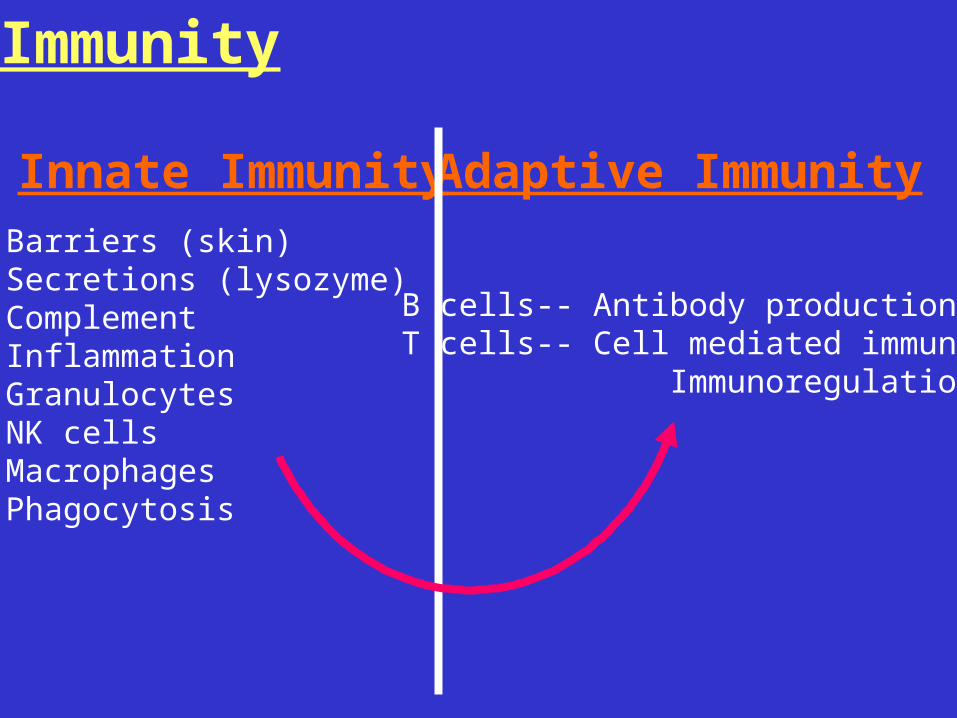
Innate Immunity Adaptive ImmunityBarriers (skin)Secretions (lysozyme)ComplementInflammationGranulocytesNK cellsMacrophagesPhagocytosis
B cells-- Antibody productionT cells-- Cell mediated immunity Immunoregulation
Immunity
Forms of Immunity
• Antibody Mediated Immunity– Helper T cells recognize non
self antigens and stimulate B cells to produce antibodies
– B cells release antibodies which bind to non self antigens present on infected cells
– B cells complete their maturation upon binding to non self antigens and destroying infected cells
• Cell Mediated Immunity– Macrophages phagocytize
pathogens– Upon phagocytosis
macrophages present non self antigens on their membranes
– Helper T cells recognize non self antigens and recruit cytotoxic T cells
– Cytotoxic T cells destroy infected cells
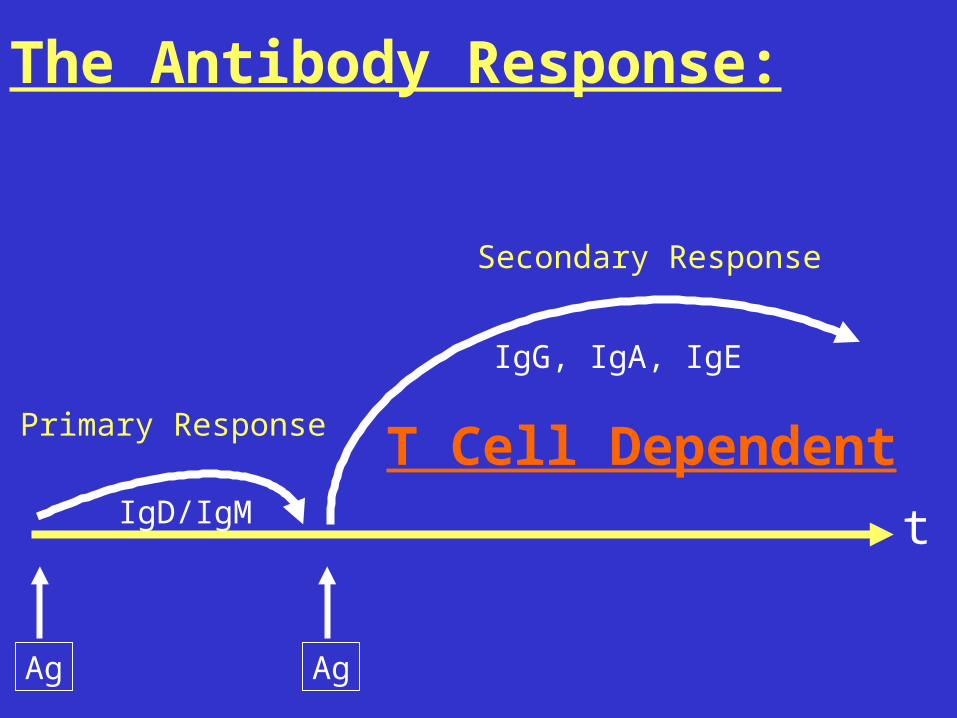
The Antibody Response:
t
Ag
IgD/IgM
Ag
IgG, IgA, IgE
Primary Response
Secondary Response
T Cell Dependent
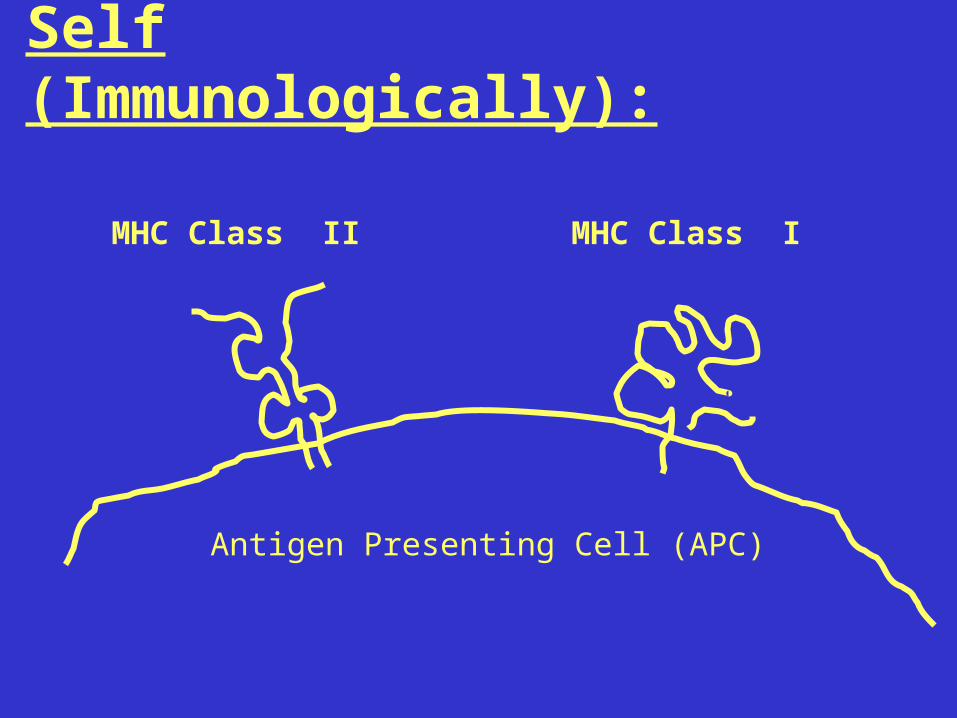
Self (Immunologically):
Antigen Presenting Cell (APC)
MHC Class II MHC Class I

Antigen Presenting Cell (APC)
MHC Class II + peptide MHC Class I + peptide

Antigen Presenting Cell (APC)
CD4 T cell CD8 T cell
T cell receptor (TcR)
TcR
Class IIClass I
Autoimmunity:
• Immune reactivity against self.
• Generally classed into systemic (e.g. SLE, RA,) and organ-specific (e.g. MS, IDDM, AITP etc.).
• Affect 5-7% of the population – often with debilitating symptoms
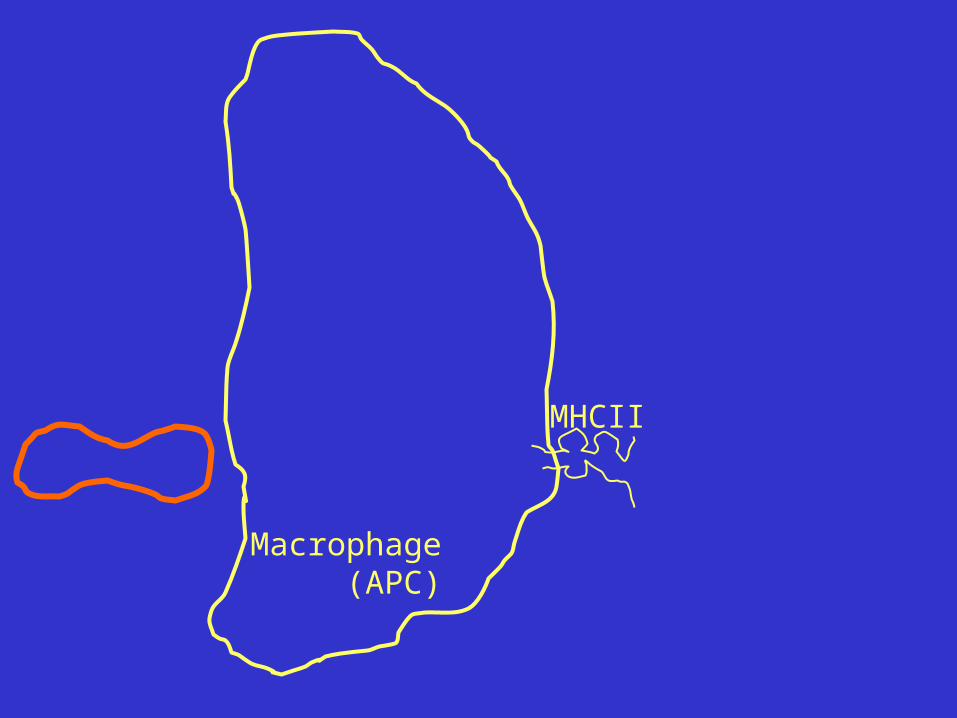
MHCII
Macrophage (APC)
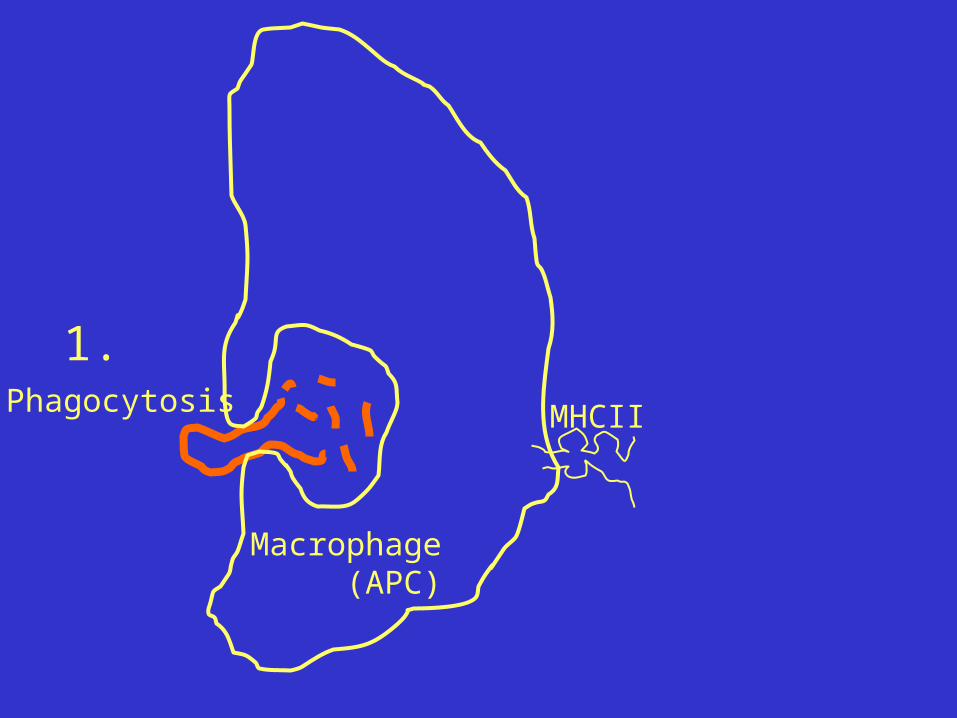
Phagocytosis
1.
MHCII
Macrophage (APC)
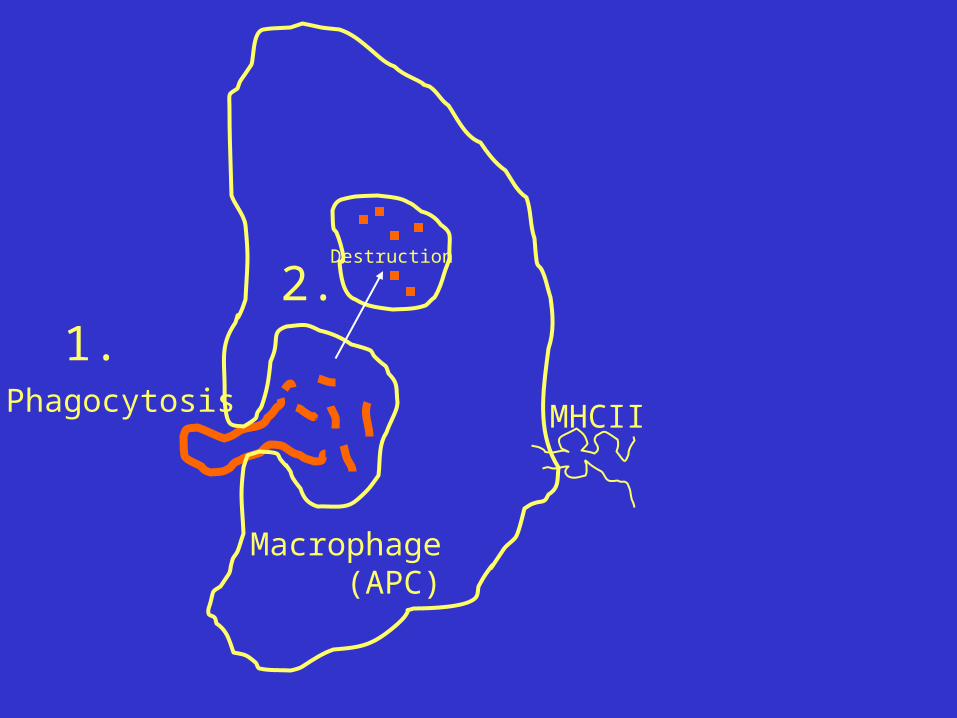
Phagocytosis
1.
MHCII
Macrophage (APC)
Destruction
2.

Phagocytosis
1.
MHCII
Macrophage (APC)
Destruction
2.
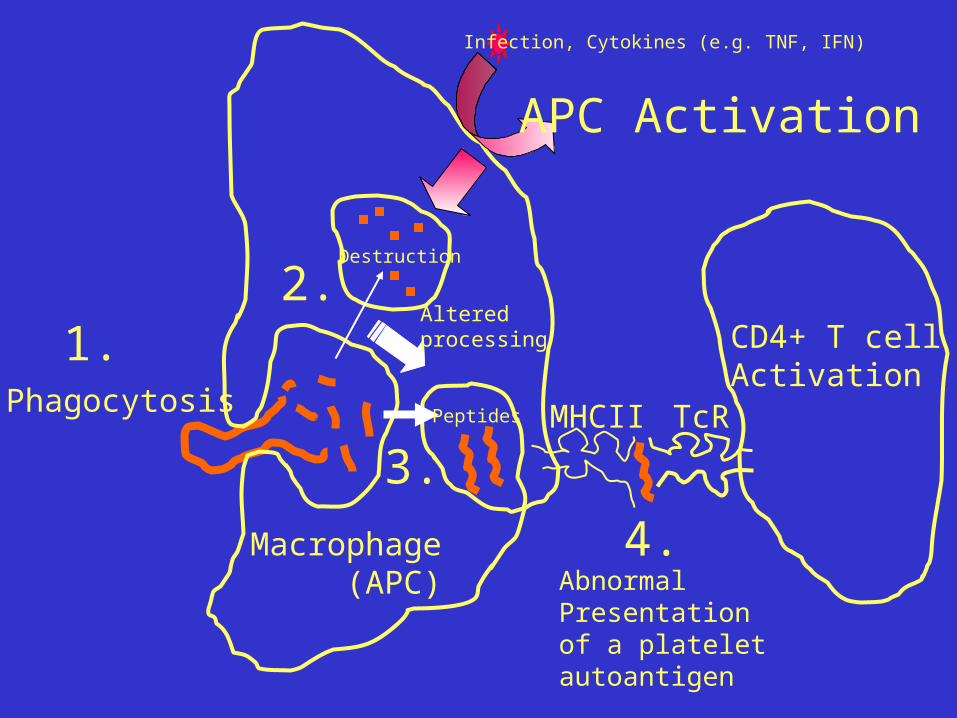
APC Activation
Infection, Cytokines (e.g. TNF, IFN)
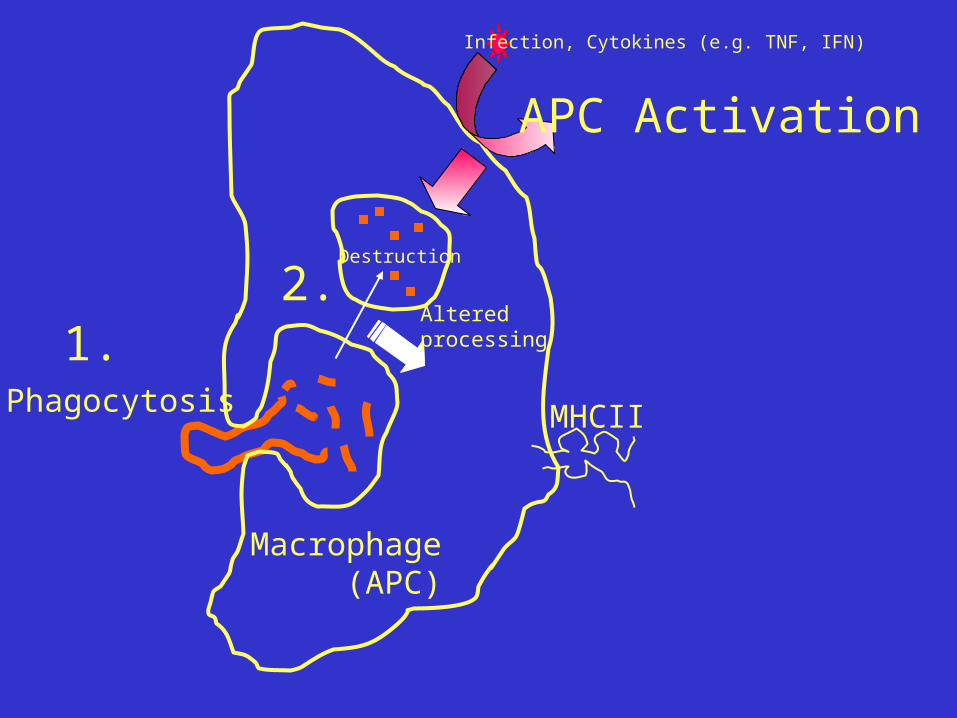
Phagocytosis
1.
MHCII
Macrophage (APC)
Destruction
2.Alteredprocessing
APC Activation
Infection, Cytokines (e.g. TNF, IFN)
Phagocytosis
1.
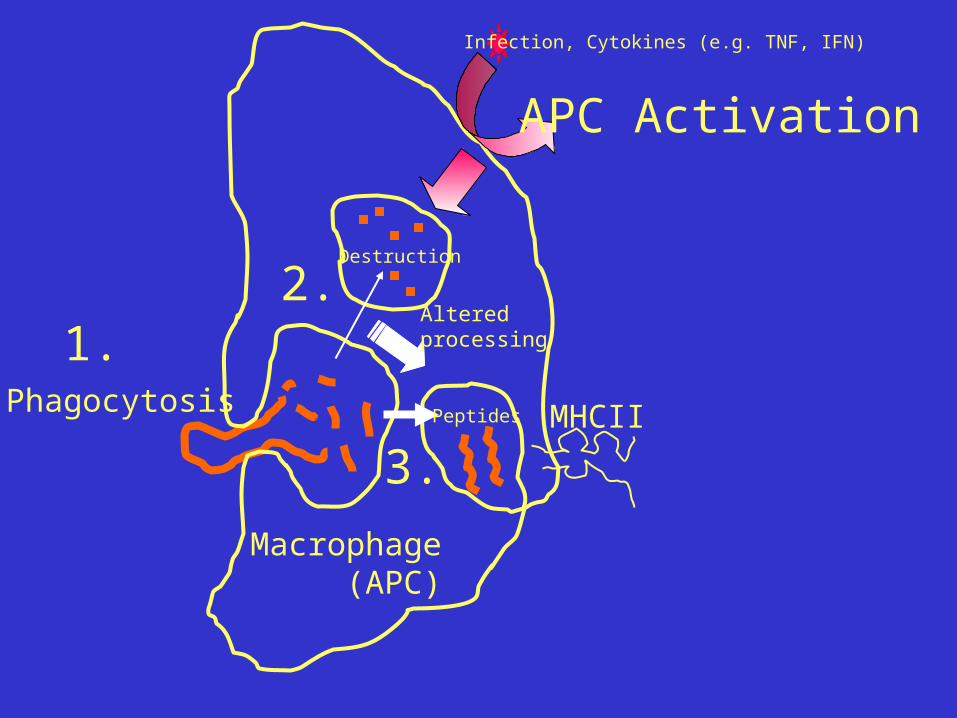
MHCII
Macrophage (APC)
Destruction
Peptides
2.
3.
APC Activation
Infection, Cytokines (e.g. TNF, IFN)
Alteredprocessing
Phagocytosis
1.
MHCII
Macrophage (APC)
Destruction
Peptides
2.
3.
APC Activation
Infection, Cytokines (e.g. TNF, IFN)
Alteredprocessing
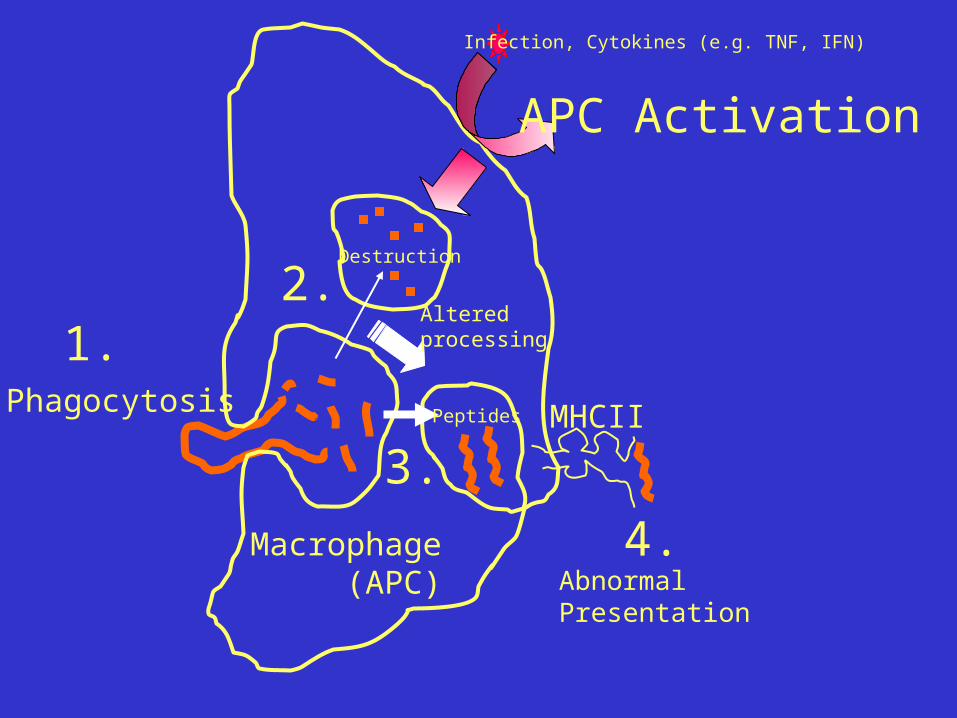
4.AbnormalPresentation
Phagocytosis
1.
MHCII
Macrophage (APC)
Destruction
Peptides
2.
3.
APC Activation
Infection, Cytokines (e.g. TNF, IFN)
Alteredprocessing
4.AbnormalPresentation of a plateletautoantigen
CD4+ T cellActivation
TcR
Diagnosis: Autoimmune Disease
• Genetic predisposition – coding for the variety of MHC molecules
• Demographics– most common among middle aged women
• Additional viral infections
• Disease specific environmental factors
• Aging, stress, hormones, pregnancy

Autoimmune Disease
• Three types of autoimmune disorders:
– Cytotoxic (Type II reactions)
– Immune complex (Type III reactions)
– Cell-mediated (Type IV reactions)
Autoimmune DiseasesA. Type II (Cytotoxic) Autoimmune Reactions
Involve antibody reactions to cell surface molecules, without cytotoxic destruction of cells.– Grave’s Disease:
• Antibodies attach to receptors on thyroid gland and stimulate production of thyroid hormone.
• Symptoms: Goiter (enlarged thyroid) and bulging eyes.
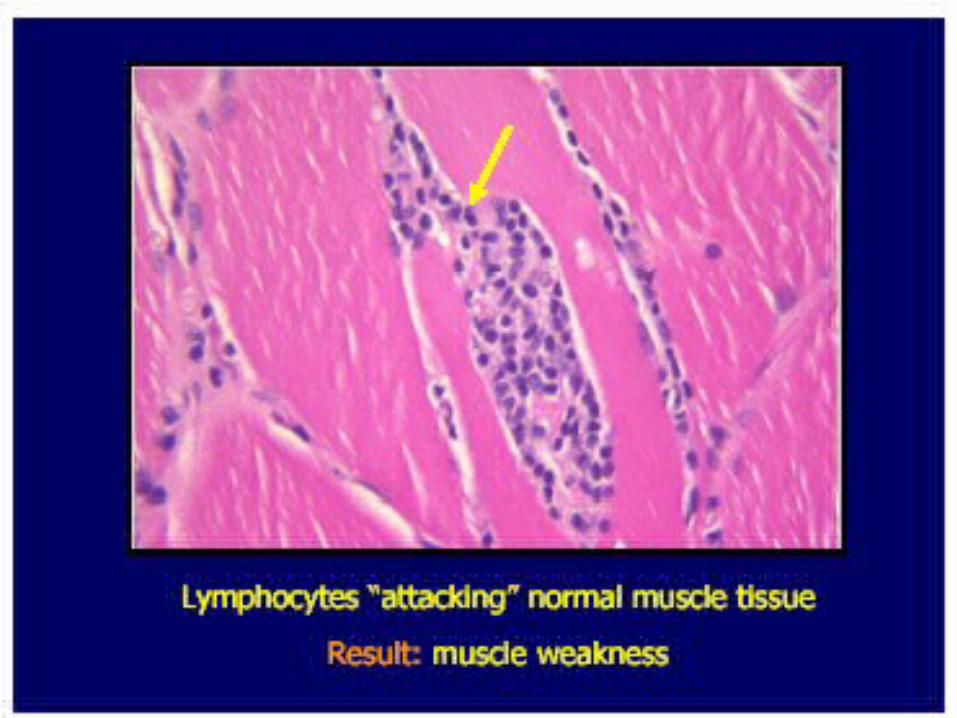
– Myasthenia gravis: • Progressive muscle weakness. Antibodies block
acetylcholine receptors at neuromuscular synapse.
Autoimmune DiseasesB. Type III (Immune Complex) Autoimmune
Reactions– Systemic Lupus Erythematosus
– Rheumatoid Arthritis
C. Type IV (Cell-Mediated) Autoimmune Reactions Insulin-dependent (Type I or Juvenile) Diabetes Mellitus

Autoimmune Disease
• Possible Causes:– Inefficient lymphocyte
programming– “Self proteins” circulate
without having been exposed to system (ex: sperm, eye lens, thyroid)
– Reactions between self-antigens and antibody production against foreign antigens
• Potential Treatments:– Control inflammation
(ex: diabetes mellitus)– Immunosuppressive
Medication
(ex: corticosteriods, cyclosporin, methotrexate)
– Therapeutic Antibodies against specific T cell molecules
(with fewer side effects)

Blood
• Autoimmune Thrombocytopenia
(AITP)
Autoimmune Thrombocytopenia:
• Acute:• Childhood disorder.• Abrupt onset.• Usually follows infectious
illness.• Spontaneous remission.
Chronic:• > 6 month duration.• Organ specific
autoimmune disease.• Autoantibodies enhance
platelet destruction.• Presence of GPIIIa-reactive
T cells.• Cytokine abnormalities.
Platelet count: <150x109/L
Nomenclature difficulties?:
ITP: Idiopathic Thrombocytopenic PurpuraImmune Thrombocytopenic Purpura
ATP: Autoimmune Thrombocytopenic Purpura- (adenosine triphosphate - oops)
AITP: AutoImmune Thrombocytopenic Purpura
- Organ-specific autoimmune disease againstplatelets..
- Primary effector phase of immunopathogenesis:
- IgG Opsonization of platelets forFc-receptor mediatedphagocytosis.
- IgG autoantibodies are primarily:
- IgG1 and IgG3 (IgM, IgA) - Antibody Targets:
- GP IIbIIIa, GPbIX, GPIV....
Autoimmune Thrombocytopenia:

AITP: Therapy
Chronic
Steroids(1950’s- )
Gammaglobulins(1981- )
Anti-CD40L(1998- )
Anti-D (1984- )
Vinca Alk., DanazolCyclophosphamide(1970’s)
Rituxan(1998- )
-Antigen- specific therapy
CyclosporinIFN, VitC etc.(1980’s- )
-Oral Tolerance

Gastrointestinal Autoimmune Disorders
• Crohn’s disease
• Ulcerative colitis
• Celiac disease
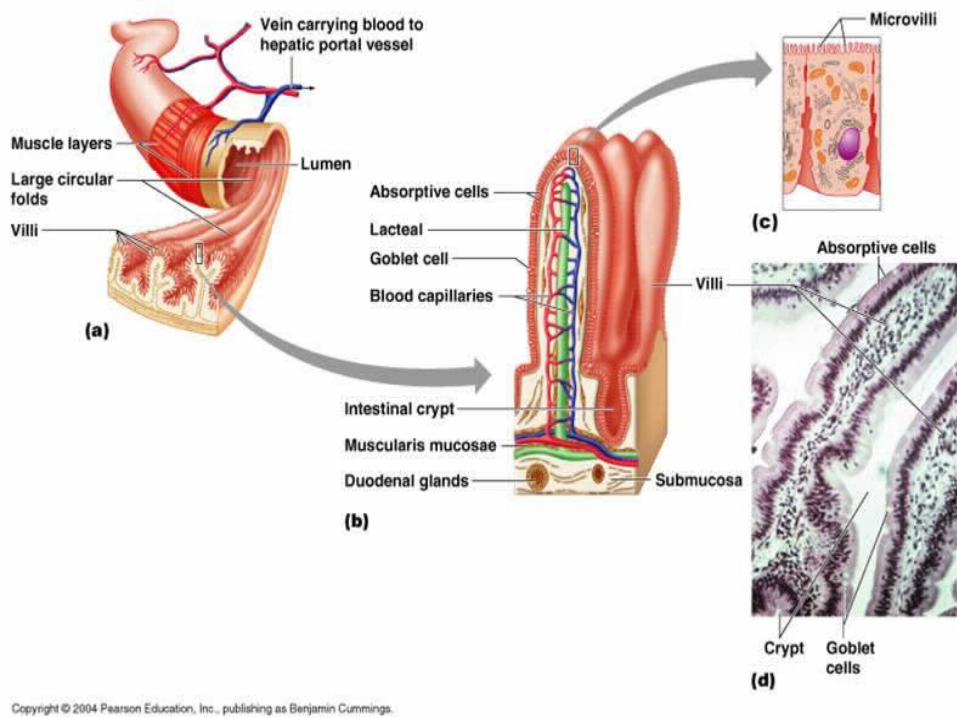
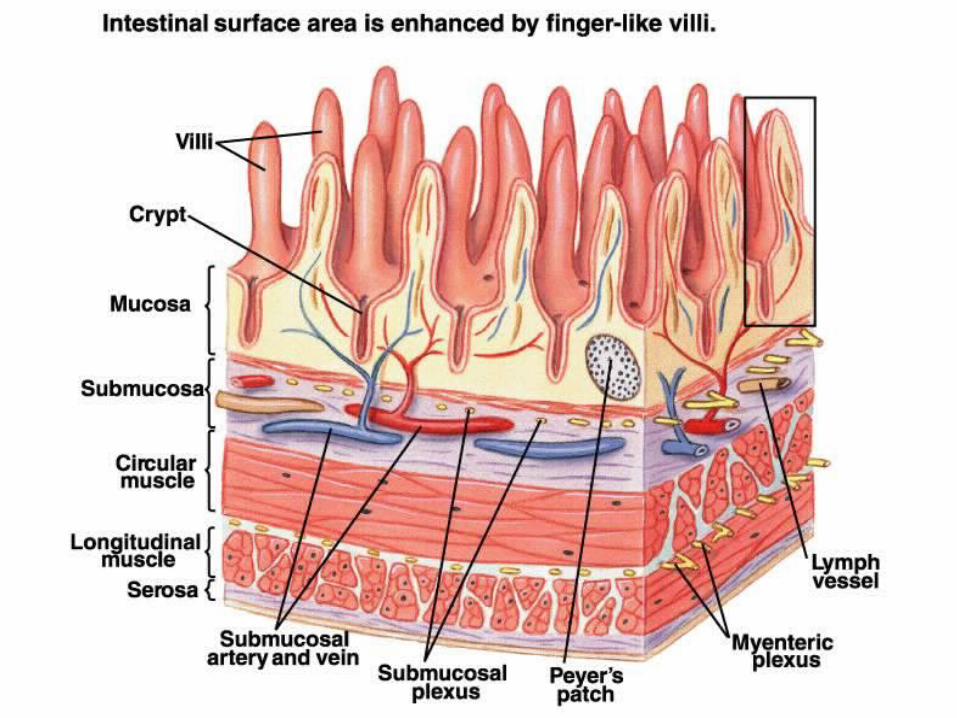
The Gut LumenThe Gut Lumen• Villi- Villi- ((singular: villus) are tiny, finger-singular: villus) are tiny, finger-
like structures that protrude from the like structures that protrude from the wall of the intestinewall of the intestine-Microvilli- -Microvilli- hairlike structure on the hairlike structure on the surface of absorptive and secretorysurface of absorptive and secretory epithelial cellsepithelial cells
• Epithelial Tissue- Epithelial Tissue- layer of cells which layer of cells which line the GI tract line the GI tract
• Enterocytes – Enterocytes – layer between gut layer between gut lumen and absorptive cellslumen and absorptive cells
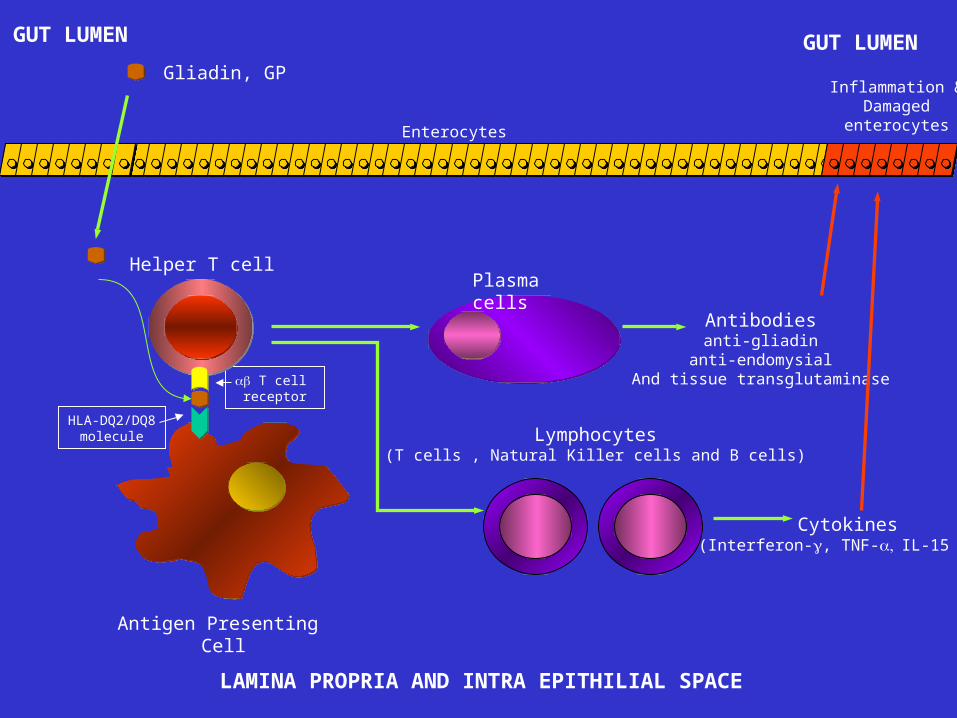
Gliadin, GP
Enterocytes
GUT LUMEN
Antibodiesanti-gliadin
anti-endomysialAnd tissue transglutaminase
Cytokines(Interferon-, TNF-IL-15 etc)
Lymphocytes(T cells , Natural Killer cells and B cells)
Plasma cells
T cell receptor
Helper T cell
HLA-DQ2/DQ8molecule
Antigen Presenting Cell
GUT LUMEN
LAMINA PROPRIA AND INTRA EPITHILIAL SPACE
Inflammation &Damaged
enterocytes
Deamidated Gliadin
• Gliadins are best known for their role, along with glutenin, in the formation of gluten.
• Deamidated gliadin is produced by acid or enzymatic treatment of gluten.
• The enzyme, tissue transglutaminase, converts some of the abundant glutamines to glutamic acid.
• This is done because gliadins are soluble in alcohol and cannot be mixed with other foods (like milk) without changing the foods qualities.
• Deamidated gliadin is soluble in water. • The cellular immunity to deamidated α-/β-gliadin is much greater than
α/β-gliadin and can result in symptomatic gluten-sensitive enteropathy.
Crohn's disease (ileitis or enteritis)
• abdominal pain (lower right area) and diarrhea
• Rectal bleeding, weight loss, (bleeding may be serious leading to anemia)
• arthritis, skin problems, and fever may also occur.
• Children with Crohn’s disease may suffer delayed development and stunted growth
Drug Therapy
• Anti-Inflammation Drugs: Sulfasalazine
• Cortisone: Prednisolone
• Immune suppressor: azathioprine
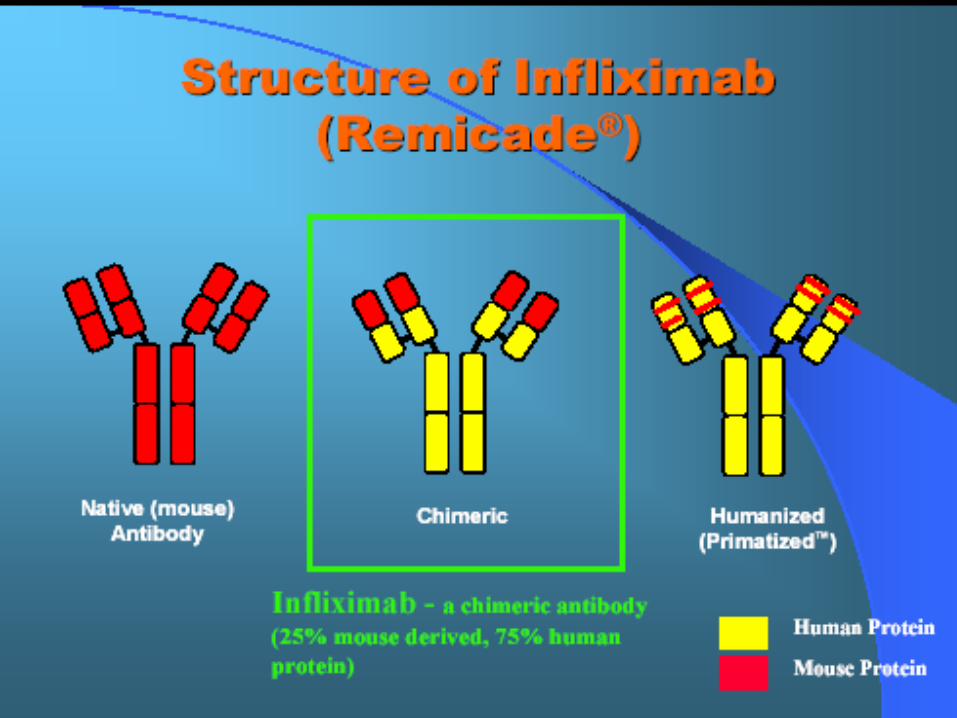
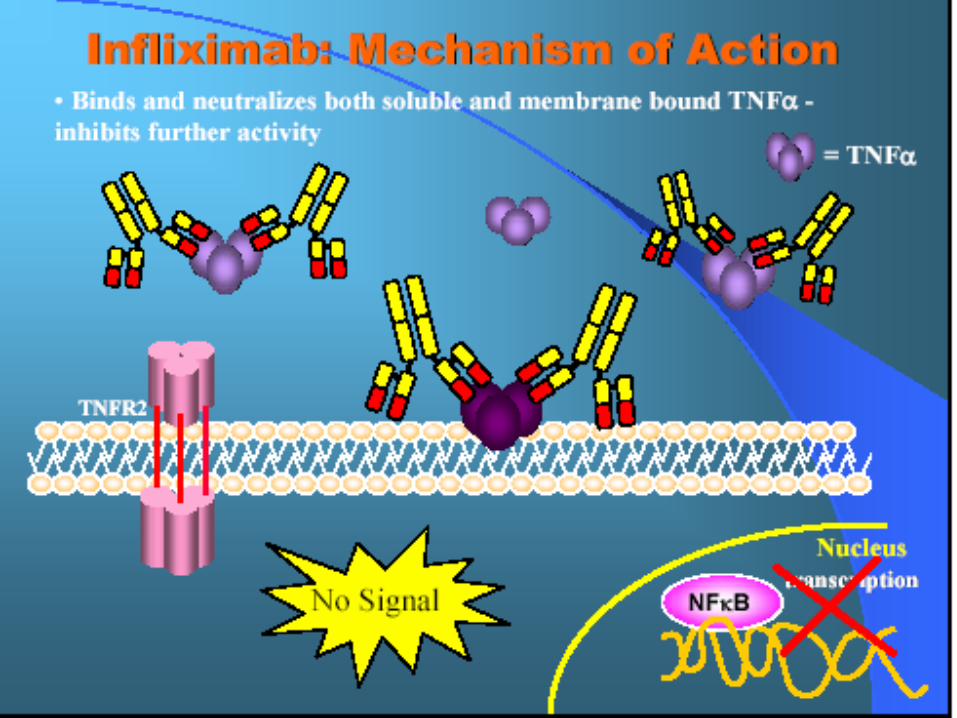
• Infliximab
• Surgery
Celiac diseaseCeliac disease ((gluten-sensitive enteropathygluten-sensitive enteropathy
• A digestive disease that damages the small A digestive disease that damages the small intestine and interferes with absorption of intestine and interferes with absorption of nutrients.nutrients.
• When people with celiac disease eat foods When people with celiac disease eat foods containing gluten, their immune system responds containing gluten, their immune system responds by damaging the small intestine.by damaging the small intestine.
Symptoms
• gas • chronic diarrhea • pale, foul-smelling• weight loss • fatigue • unexplained anemia • bone or joint pain • osteoporosis, osteopenia • behavioral changes • tingling numbness in the
legs (from nerve damage) • seizures
• missed menstrual periods (often because of excessive weight loss)
• infertility, recurrent miscarriage
• delayed growth • pale mouth sores • tooth discoloration or loss
of enamel • itchy skin rash called
dermatitis herpetiformis
Complications
• Blockage of the intestine.
• Sores, or ulcers,
• Infected fistulas (surgery)
• Nutritional complications
Ulcerative colitis
• Ulcerative colitis is an inflammatory bowel disease (IBD). It can be difficult to diagnose because its symptoms are similar to Crohn’s disease. It involves one section of inner lining of the colon starting of the rectum.
• Crohn’s disease differs because it causes inflammation deeper within the intestinal wall and can occur in other parts of the digestive system including the small intestine, mouth, esophagus, and stomach










SJÖGREN'S SYNDROMESjogren syndrome is a Systemic inflammatory disorder characterized by dry mouth, decreased tearing, and other dry mucous membranes. It is often associated with autoimmune rheumatic disorders.•The syndrome occurs most often in women 40 to 50 years old. It is rare in children.

Dry eye may be sight-threatening
Bacterial Keratitis Corneal ulcer
DRY EYE : Classification
DRY EYE
Aqueous tear deficiency (ATD)
(Tear deficient dry eye)
keratoconjunctivitis sicca
(KCS)
(Most common)
Evaporative tear deficiency (ETD)
(Evaporative dry eye)
Dry Eye: Main CausesTEAR DEFICIENT DRY EYE (KCS) EVAPORATIVE
DRY EYE
• Sjogrens • Non-Sjogrens
–Ageing
–Menopause
–Medicament
–Neurotrophic keratitis
• Lid surfacing/blinking anomalies
• Contact lens related
• Chronic allergy/toxicity

Management of Dry Eye
A rtific ia l tea rs
Tear rep lacem en t
P u n c ta l P lu g s
Tear P reserva tion
Trea tm en t
•Topical corticosteroids – fluorometholone
•Topical androgen
•Cyclosporine ophthalmic emulsion
Late KCS

Tests
• Positive antinuclear antibodies (ANA) test
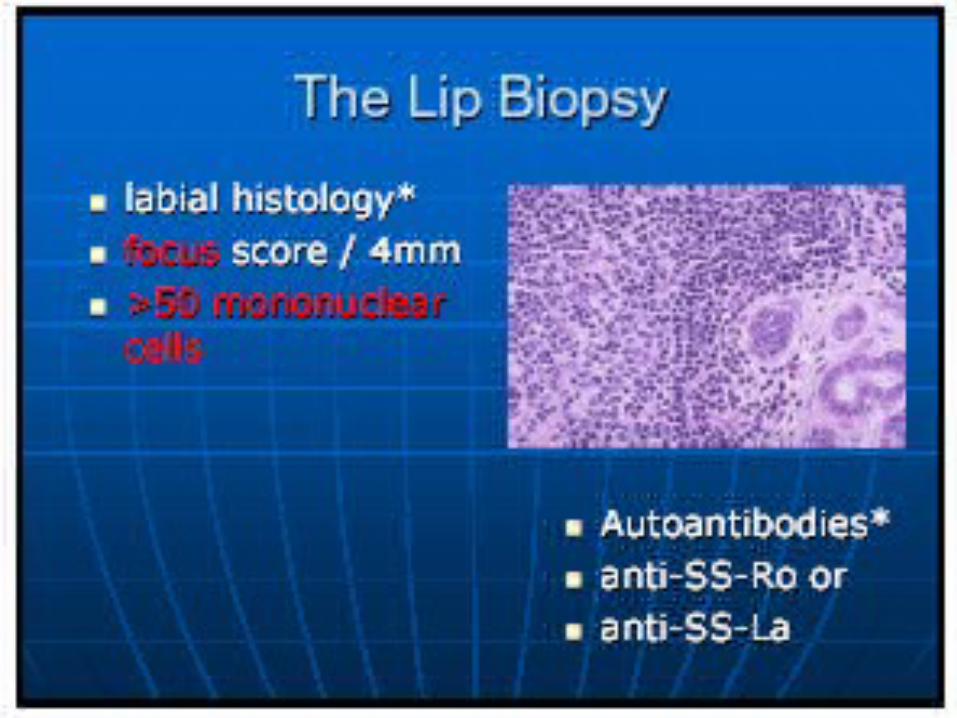
• Positive salivary gland biopsy
• Positive rheumatic factor (possible)
• Tear test
• Slit lamp exam with rose bengal dye
McMonnies’ Questionnaire
Do you experience any of the following eye symptoms?SorenessScratchinessDrynessGrittinessBurning
Symptoms “often” or “constantly”
Eyes unusually sensitive to cigarette smoke, smog, air conditioning, central heating?Do you suffer from arthritis?Do you suffer from thyroid abnormality?Eye irritation upon awakening?
Rose Bengal staining
• Rose Bengal solution 1% placed into the conjunctival sac.
• After a wait of 2 mins, degree of rose bengal staining on bulbar conjunctiva and cornea is quantitated by microscopic exam.
• Stains devitalized cells.
• Also stains mucous strands (very often present in KCS)
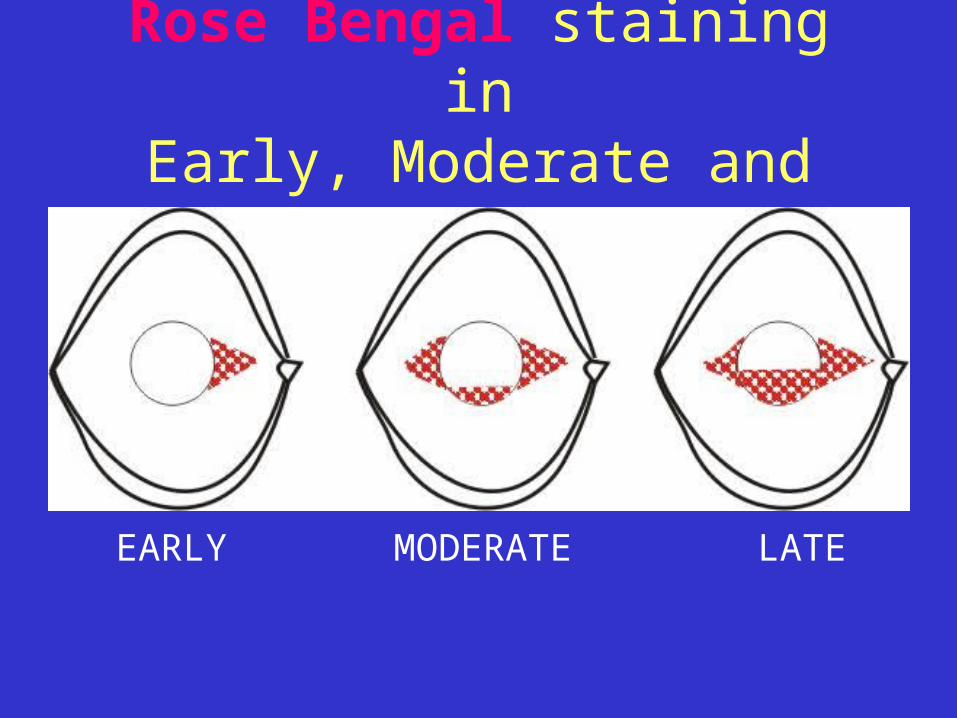
Rose Bengal staining inEarly, Moderate and Late KCS
EARLY MODERATE LATE

Schirmer test
• Without Anesthesia
– Measures Reflex Tear Secretion (dry eye = < 6mm wetting)
• With Anesthesia
– Measures Basal Tear Secretion (dry eye =< 3mm wetting)
SYSTEMIC LUPUS ERYTHEMATOSUS (SLE)
• SLE is an autoimmune disease characterized by immune dysregulation resulting in the production of antinuclear antibodies (ANA) and generation of circulating immune complexes.
• SLE is a chronic, usually life-long, potentially fatal autoimmune disease characterized by unpredictable exacerbations and remissions.
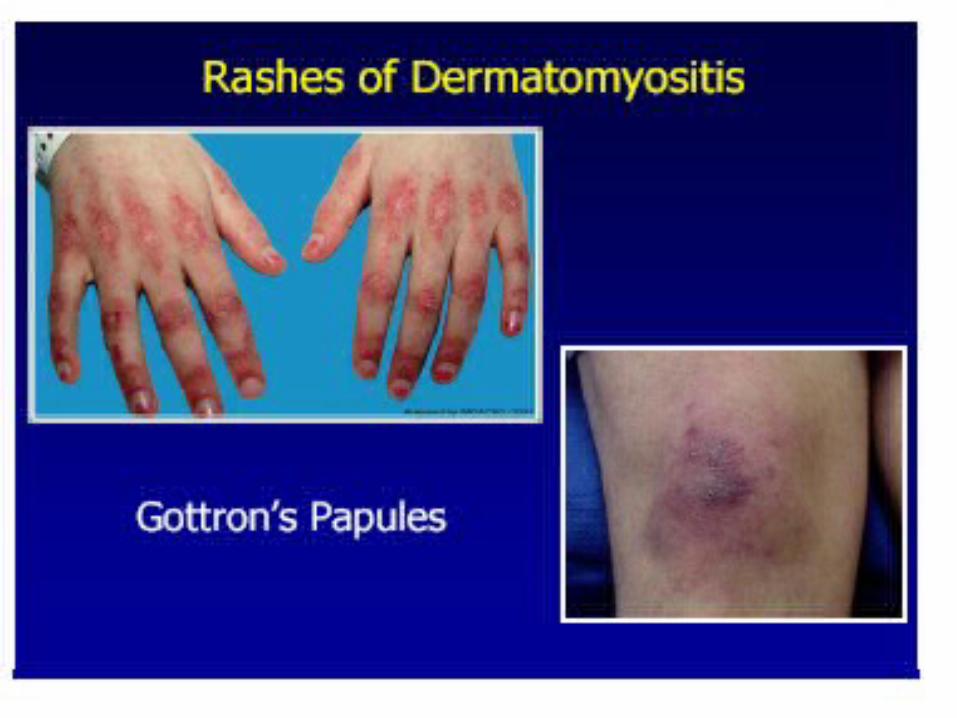
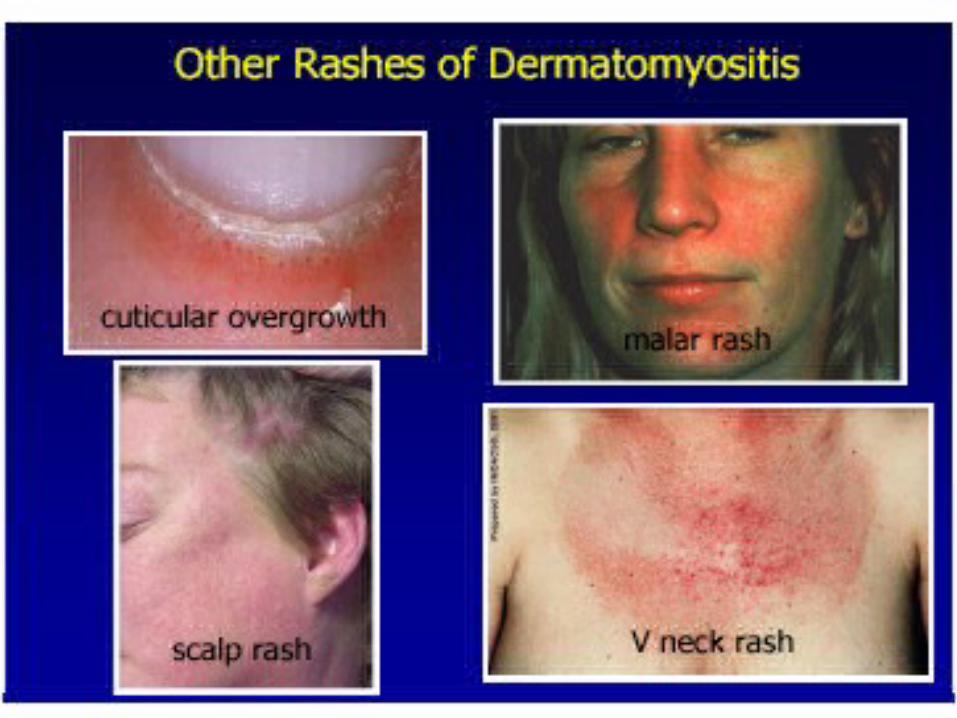
• In SLE there is a predilection for clinical involvement of the joints, skin, kidney, brain, lung, heart and gastrointestinal tract
Types of Lupus
• Discoid or cutaneous lupus.
• Systemic lupus
• Drug-induced lupus
Discoid or cutaneous lupus
• Discoid or cutaneous lupus is a condition that affects the skin.
• It presents itself as a rash on the neck, scalp, or face.
• The term “discoid” refers to the disk-like shape of the rash that forms
Systemic lupus
• Systemic lupus can affect almost any organ of the body.
• Most patients with this form will have symptoms in the joints and the skin.
• Other patients may have symptoms affecting the heart, kidneys, blood, and lungs.
Drug-induced lupus
• Drug-induced lupus occurs when certain medications are used for a long period of time.
• Symptoms typically present in a manner that is similar to SLE.
• Symptoms begin to decline within several days of discontinuing the medication with full resolution occurring within several weeks.
• The most common are procainamide, hydralazine , and quinidine
incidence, and risk factors
• SLE may be mild or severe enough to cause death.• SLE affects nine times as many women as men. It
may occur at any age, but appears most often in people between the ages of 10 and 50 years. African Americans and Asians are affected more often than people from other races.
• SLE may also be caused by certain drugs.




Tests used to diagnose SLE may include:
• Antinuclear antibody (ANA) panel including anti-DNA and anti-Smith antibodies
• Chest x-ray showing pleuritis or pericarditis • Urinalysis to show blood, casts, or protein
in the urine • CBC • Kidney biopsy

Management
• There is no cure for SLE. Treatment is aimed at controlling symptoms.
• NSAIDs are used to treat arthritis and pleurisy. • Corticosteroid creams are used to treat skin rashes.• hydroxychloroquine and low dose corticosteroids are
sometimes used for skin and arthritis symptoms.• wear protective clothing, sunglasses, and sunscreen when in
the sun.• Corticosteroids or medications to decrease the immune system
response may be prescribed to control the various symptoms. • Cytotoxic drugs to treat people who do not respond well to
corticosteroids or who must use high doses of corticosteroids.

Expectations (prognosis)
• Many of those with SLE have mild illness.• Women with SLE who become pregnant are often
able to carry the pregnancy safely to term and deliver normal infants, as long as there is no severe kidney or heart disease present and the SLE is being treated appropriately.The presence of anti-phospholipid antibodies may increase the possibility of pregnancy loss.

Complications
• Some people with SLE have deposits of antibodies within the cells (glomeruli) of the kidneys. This leads to a condition called lupus nephritis. Patients with this condition may eventually develop kidney failure and require dialysis or kidney transplantation.



Autoimmune Inner Ear Disease
Clinical Picture
• Middle-aged women
• progressive SNHL, weeks to months
• dizziness, aural fullness
• bilateral 79% no vestibular symptoms
• systemic autoimmune disease in 29%

Cogan’s Syndrome
• Interstitial keratitis• vertigo, tinnitus,
SNHL
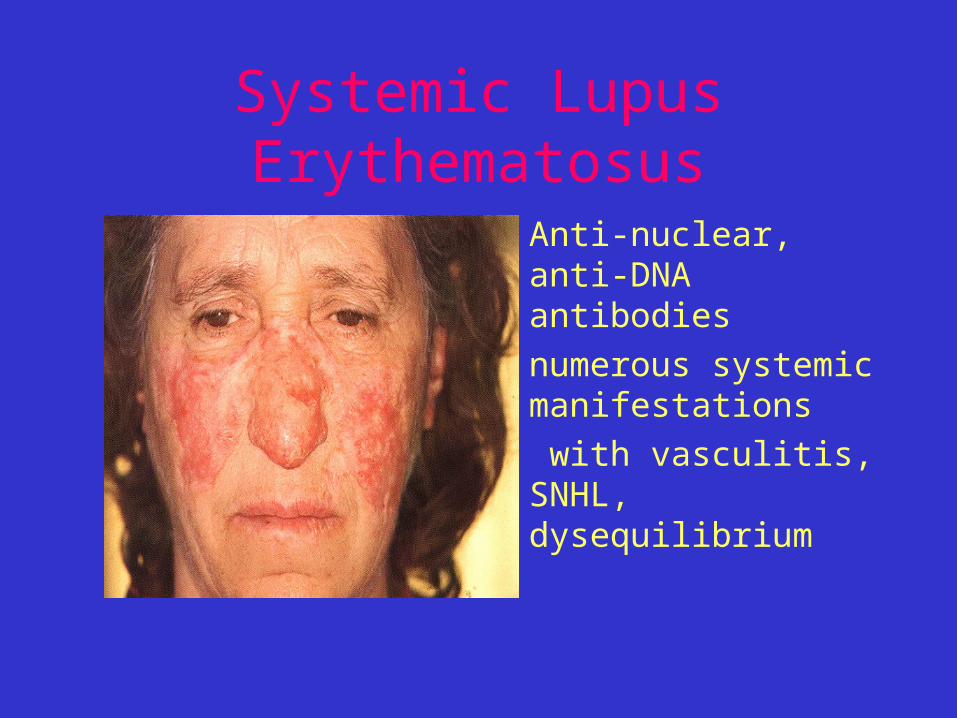
Systemic Lupus Erythematosus
• Anti-nuclear, anti-DNA antibodies
• numerous systemic manifestations
• with vasculitis, SNHL, dysequilibrium
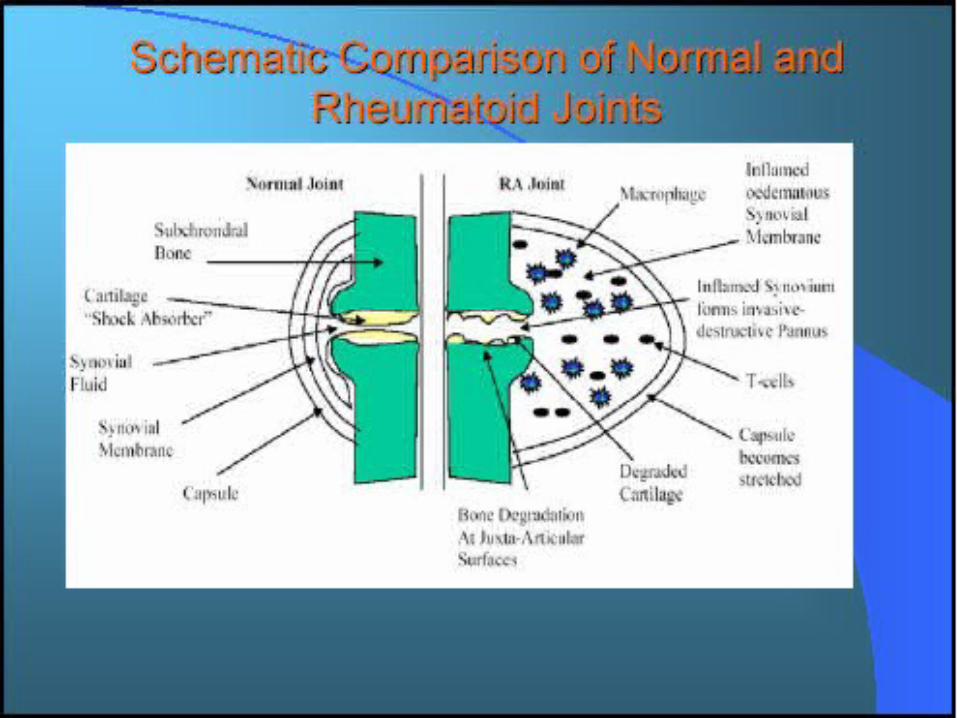
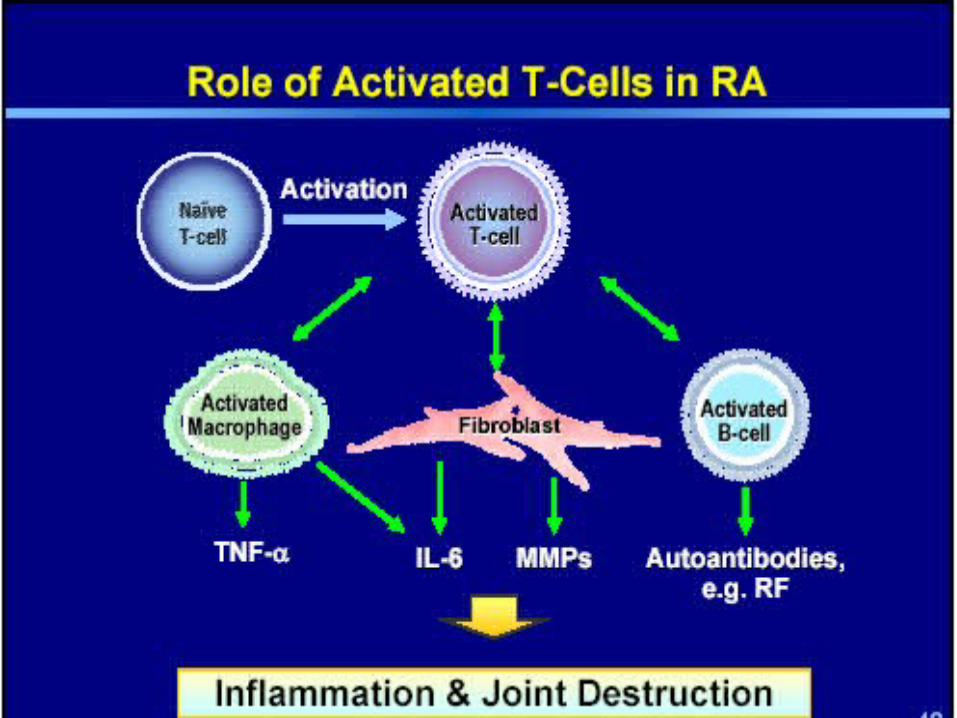
Rheumatoid Arthritis
• Small joints of hands and feet
• vasculitis, muscle atrophy, subcutaneous nodules, splenomegaly
• IgM 19S and 7S, IgG 7S 75%
• 44% bilateral SNHL
Meniere’s Disease
• Fluctuating SNHL, episodic vertigo, aural fullness
• ? Autoimmune etiology– 97% with CICs
(Derebery)– response to
immunotherapy– 32% with anti-68kDa
antibody
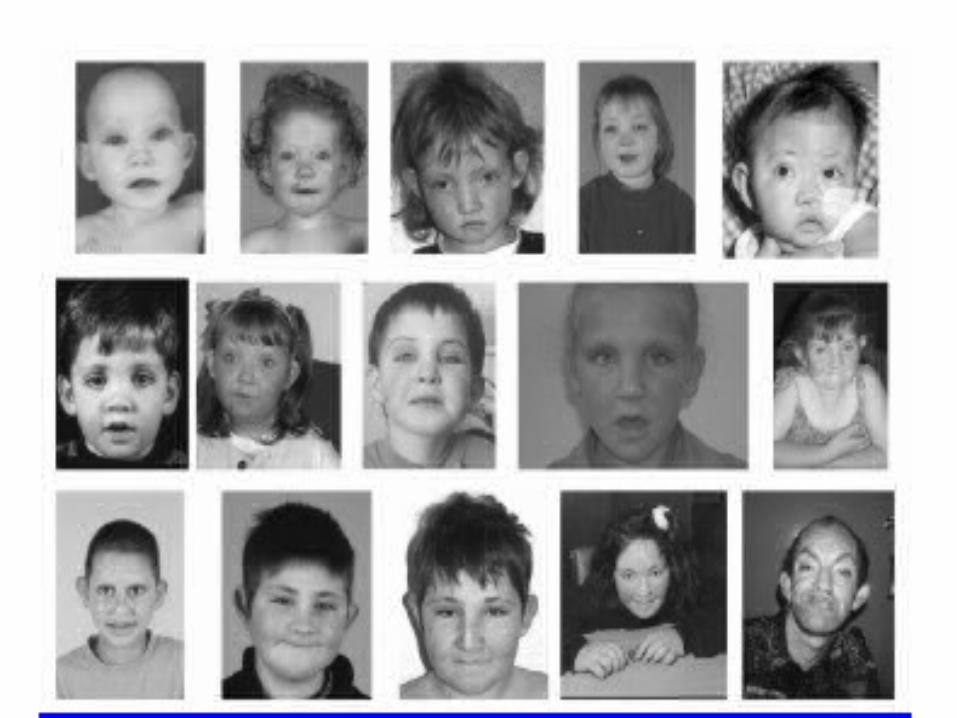
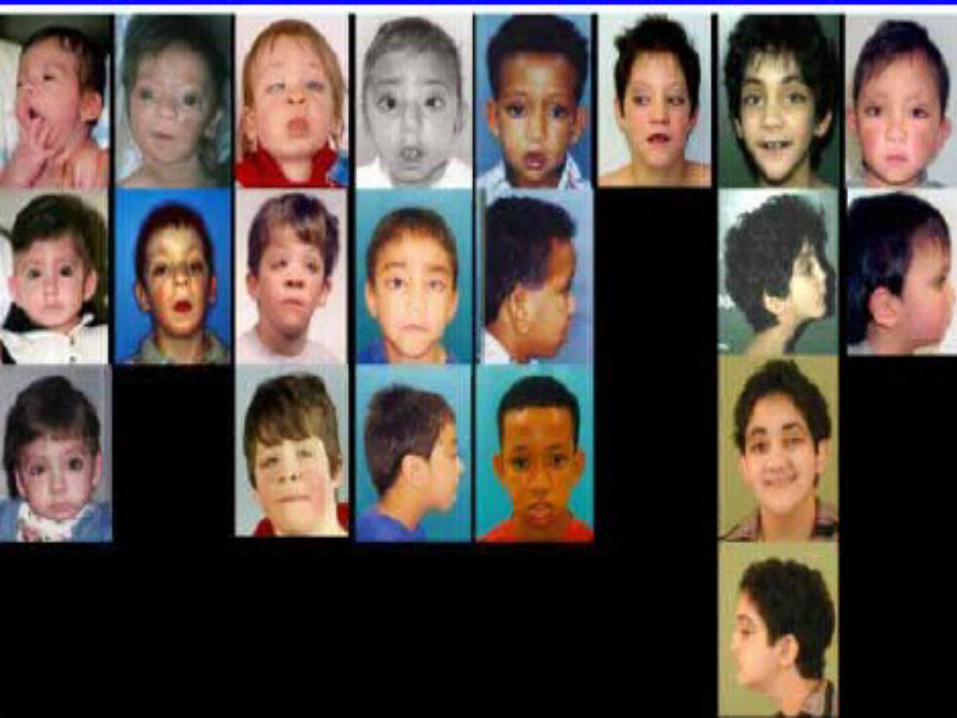
Kabuki Syndrome
• Kabuki Syndrome is associated with autoimmune disturbance


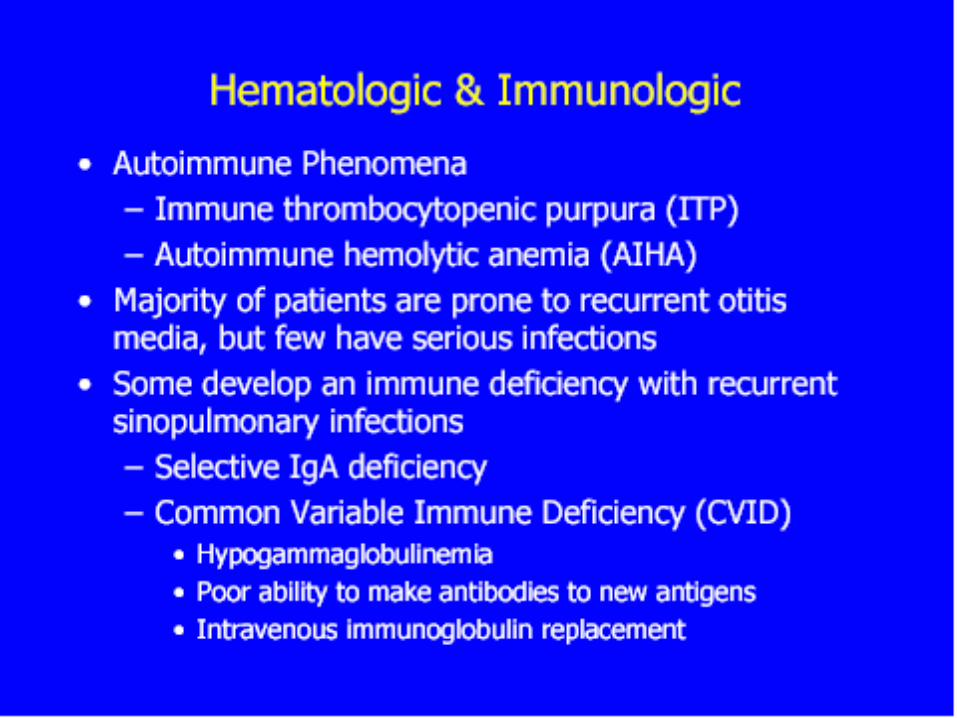

Kabuki SyndromeKabuki-makeup SyndromeNiikawa-Kuroki Syndrome
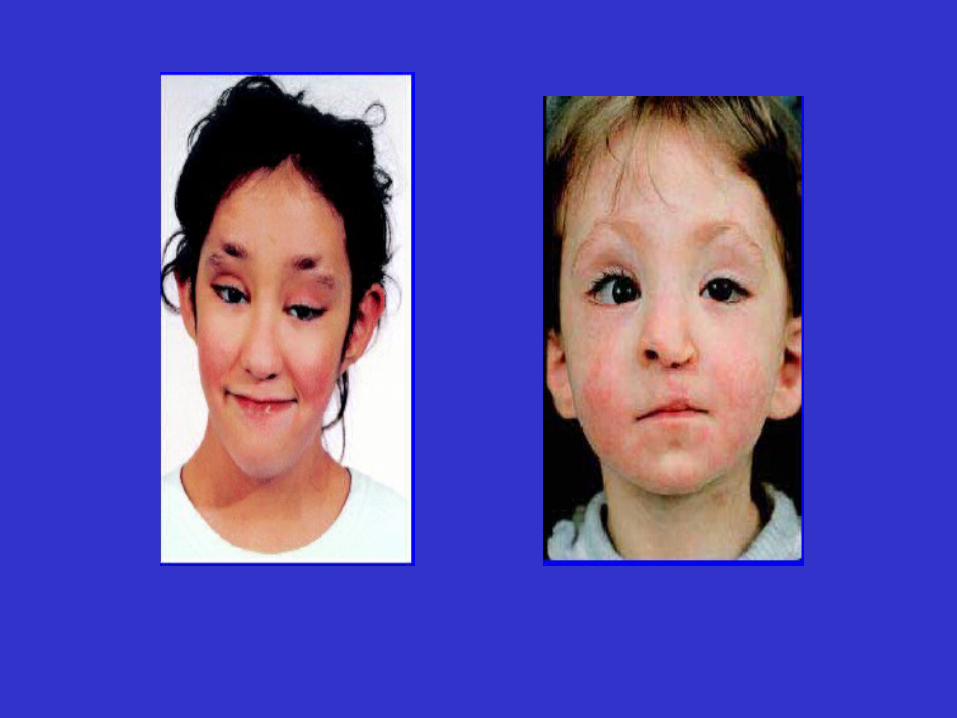
• Feature: mental retardation-malformation syndrome, characterized by a unique combination of craniofacial anomalies, congenital heart defects, skeletal anomalies, persistent fetal fingertip pads, dermatoglyphic abnormalities, mental retardation, and short stature.
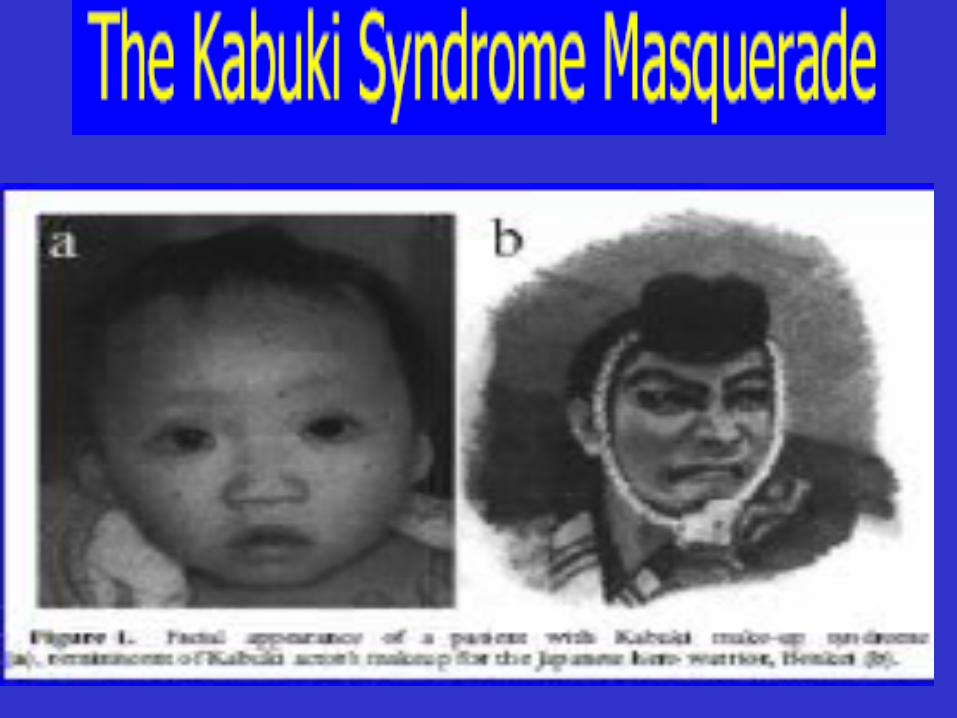
Kabuki Syndrome
• Because the peculiar facial appearance resembles the makeup of Kabuki actors in a traditional Japanese theater, the Niikawa-Kuroki syndrome is also known as Kabuki or Kabuki makeup syndrome.
• The prevalence of the syndrome is estimated to be 1 in 32,000 live births in Japan. The syndrome is increasingly recognized in other parts of the world.
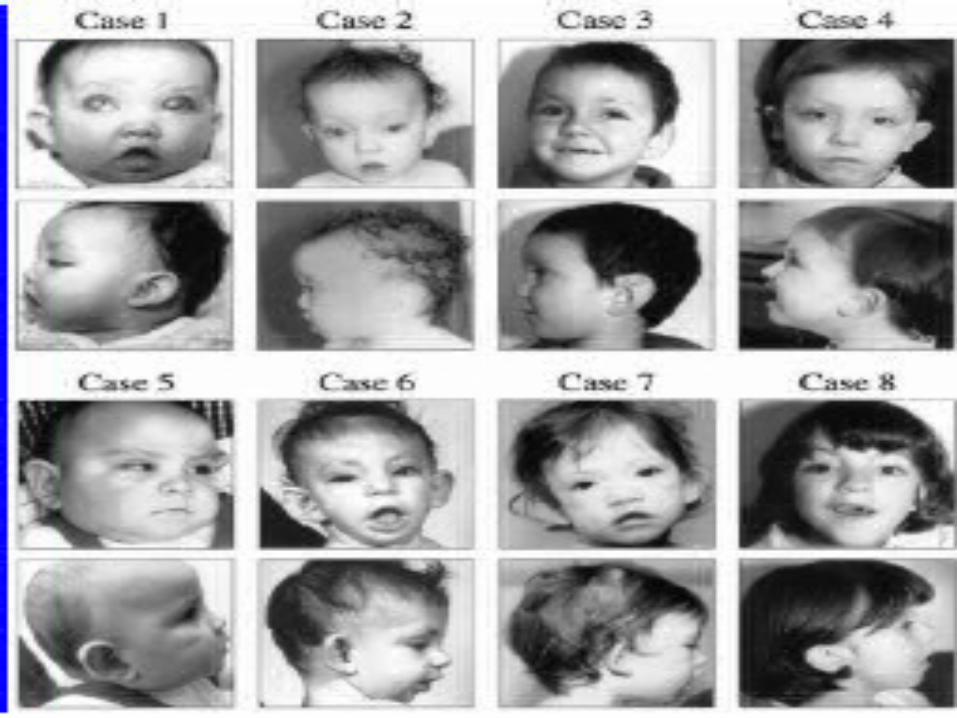

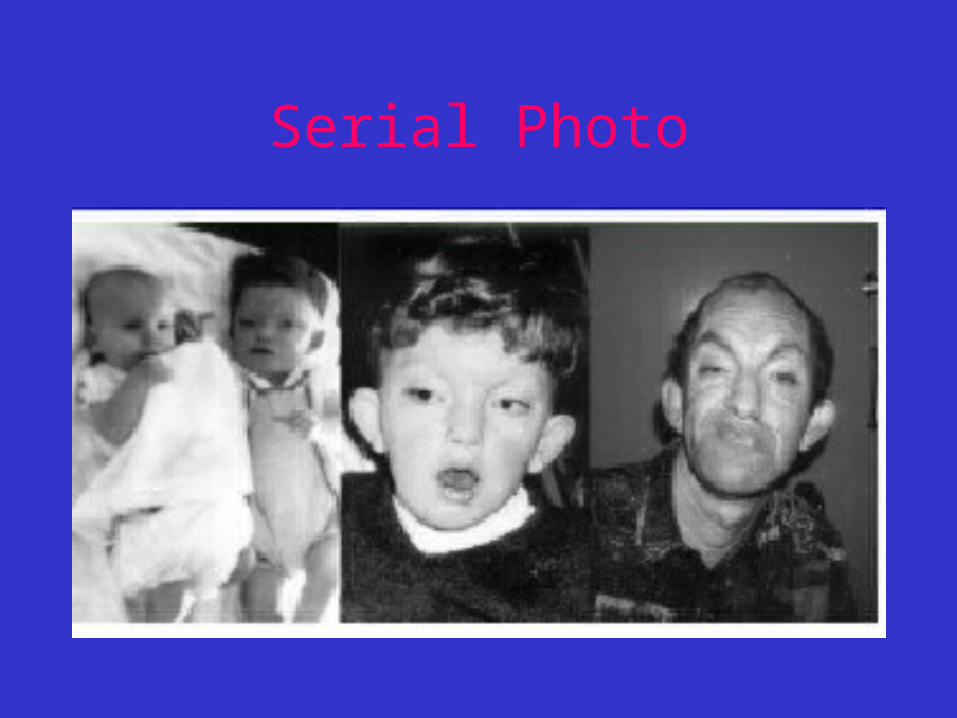
Serial Photo
Ka = Song bu = dance ki = skill
• Popular Japanese entertainment that combines music, dance, and mime in highly stylized performance.
• Kabuki dates from the end of the 16th cent., when it developed from the nobility's No theater and became the theater of townspeople.
• In its early years it had a licentious reputation, its actors often being prostitutes; women and young boys were consequently forbidden to perform, and kabuki is today performed by an adult all-male cast.


Kabuki

Kabuki actor