atrial fibrillation: rate vs. rhythm - ocpe.mcw.edu · limitations of affirm and race •young,...
TRANSCRIPT

AtrialFibrillation:Ratevs.Rhythm
MichaelCurley,MDCardiacElectrophysiology

Ihavenorelevantfinancialdisclosurespertainingtothistopic.

AFibEpidemiology
#1Mostcommonheartrhythmdisturbance
Circulation2004;110:1042–1046

AFibEpidemiology
Circulation2004;110:1042–1046
1in4Americansover40willbediagnosed
AFibEpidemiology
JACC2016;68.5:525-568
3.5millionto6.1millionNumberofAmericanswhohaveAfib

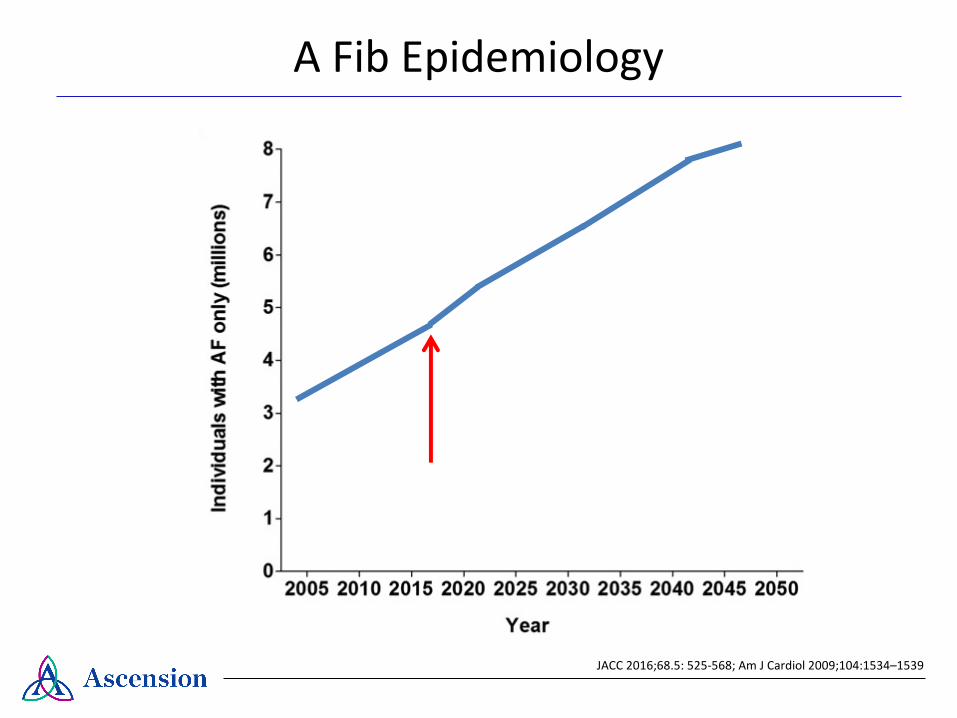
AFibEpidemiology
$6,000,000,000AnnualexpenditureinUSonAfibcare
www.cdc.gov/dhdsp/data_stastistics/fact_sheet/fs_atrial_fibrillation.htm
AFibEpidemiology
!"#$%
&%'()('*+,-./(01.23."%,4.5#(,,("%-6
7$+8
9$% 2,,
:
;
<
=
>
?
@
A?AA< ?A@A ?A@< ?A?A ?A?< ?A>A ?A>< ?A=A ?A=< ?A<A
JACC2016;68.5:525-568;AmJCardiol 2009;104:1534–1539

ImpactofAFib
• Markedlyreducesqualityoflife
• Increasesriskofstroke
• Increasesriskofdevelopingheartfailure
• Increaseslikelihoodofhospitalization
• Increasesriskofmortality
JAmColl Cardiol 2000;36:1303–1309Arch InternMed 1987;147:1561–1564
AmJCardiol 1998;82:2N–9NCirc CardiovascQualOutcomes 2011;4:313–4320
ImpactofAFib
JAMANeurol.2015;72(11):1288-1294

ImpactofAFib
JAMANeurol.2015;72(11):1288-1294
IndividualswithAFare≈2timesmorelikelytodevelopdementiathanthosewithoutAF
PrincipleGoalsofAFibManagement
1.SymptomControl
Imagefrom:www.health.harvard.edu/staying-healthy/step-lively-with-walking
2.Strokeprophylaxis
Definitions
Ratecontrol
• AstrategyemployingtheuseofAVnodalblockingagentssuchasbetablocks,calciumchannelblockersordigoxin.
• AVnodalablationplusventricularpacing

Definitions
Rhythmcontrol
• Astrategyemployingantiarrhythmicdrugtherapy,catheterablation(radiofrequency,cryoablation,laser)and/orasurgicalproceduretomaintainsinusrhythm.

Definitions
Rhythmcontrol
• Astrategyemployingantiarrhythmicdrugtherapy,catheterablation(radiofrequency,cryoablation,laser)and/orasurgicalproceduretomaintainsinusrhythm.
TrialDataAF
FIRM
Tria
lRA
CETria
l
NEngl JMed2002;347:1825-33NEngl JMed2002;347:1834-40

AFFIRM
NEngl JMed2002;347:1825-33
• Design:multi-center,prospective,randomized,controlled• Subjects:4060patients• Inclusioncriteria:AF,65years+(meanage70)• Primaryendpoint:all-causemortality

AFFIRM
NEngl JMed2002;347:1825-33
• Ratecontrolgroup:HR<80atrest,<110during6minutewalktest• Rhythmcontrolgroup:amiodarone,disopyramide,flecainide,propafenone,quinidine,sotalol,dofetilide oranycombination.If2+drugsfailed,ablationwasdeemedacceptable.

AFFIRM
NEngl JMed2002;347:1825-33
AFFIRM
NEngl JMed2002;347:1825-33
• Trendtowardsincreasedprimaryendpointinrhythmgroup• Nodifferenceinglobalfunctionalstatusorqualityoflife• Increasedriskofhospitalizationintherhythmcontrolgroup
• Trendtowardsincreasedprimaryendpointinrhythmgroup• Nodifferenceinglobalfunctionalstatusorqualityoflife• Increasedriskofhospitalizationintherhythmcontrolgroup

RACE
NEngl JMed2002;347:1825-33
• Design:multi-center,prospective,randomized,controlled• Subjects:522patients(mean68yearsofage)• Inclusioncriteria:persistentAForatrialflutter,1-2priorDCCVs• Primaryendpoint:Compositeofcardiovasculardeath,HF,thromboembolism,pacemakerimplantation,orsevereadversedrugeffect

RACE
• Ratecontrolgroup:HR<100• Rhythmcontrolgroup:sotalol initially;flecainide,propafenone oramiodaroneusedifarrhythmiarecurrencewithin6months
NEngl JMed2002;347:1834-1840

RACE
NEngl JMed2002;347:1834-1840

RACE
NEngl JMed2002;347:1834-1840
• Trendtowardsincreasedprimaryendpointinrhythmgroup• Nodifferenceincardiovascularmortality• Nodifferenceinqualityoflife• Increasedriskofheartfailure,thromboembolism,pacemakerinsertionandadversedrugreactions

LimitationsofAFFIRMandRACE
• Young,healthypatientsnotenrolled• Approximately50%ofAFFIRMpatientswithsymptomaticAFhadsymptomaticepisodeslessthanoncepermonth• Dataweregatheredlargelybeforethewidespreadutilizationofpulmonaryveinisolation• Bothtrialsallowedforcessationofanticoagulanttherapy4weeksafterrestorationofsinusrhythm
ArchInternMed2012;172:172-983

ORBIT-AF
JACCEP2016;2:221–229
• Design:multi-center,retrospective,registrydataset• Subjects:6,988patients• Inclusioncriteria:age>18,AFofanyvariety• Studyoutcomes:all-causedeath,cardiovasculardeath,firststroke/TIA,newonsetheartfailureandmajorbleeding

ORBIT-AF
JACCEP2016;2:221–229
Takeaway:Rhythmcontrolwasnotsuperiortoratecontrolstrategyforoutcomesofstroke,heartfailure,ormortality,butwasassociatedwithmorecardiovascularhospitalizations.
IsThereaRoleforRhythmControl?
• Youngpatients• Patientsearlyintheirnaturalhistory
- Reversibleetiology:hyperthyroidism,PE,pericarditis- Normalleftatrialsize
• Individualswhoaresymptomaticdespiteratecontrol• Inabilitytoadequatelyattainratecontrol

TakeHomePoints
• TheclinicalandeconomicburdenofAFislargeandwillcontinuetoincreaseinthecomingdecades.
• Impactiswideranging:heartfailure,stroke,dementia,etc.• Randomizedandobservationdatahavefailedtodemonstrate
benefitofrhythmcontrolstrategyonmortality,strokeorheartfailure.
• Rhythmcontrolstrategiesareassociatedwithincreasedhospitalization
• Rhythmcontrolstrategyshouldstillbeconsideredfor:youngerorsymptomaticindividuals,thosewithreversibleetiologies
