assessing risk compensation post-voluntary medical male circumcision in zambia paul c. hewett a,...
TRANSCRIPT

ASSESSING RISK COMPENSATION POST-VOLUNTARY MEDICAL MALE
CIRCUMCISION IN ZAMBIAPaul C. Hewetta, Petra Toddb, Nicolas Grauc, Erica Soler-
Hampejsekc, Kumbutso Dzekedzeked, Barbara S. Menschc
aPopulation Council, Zambia, bUniversity of Pennsylvania, cUniversidad de Chile, dPopulation Council, New York, eDzekedzeke, Inc.

BackgroundGovernment of the Republic of Zambia has set ambitious targets for scaling up voluntary medical male circumcision (VMMC) services.
Target: MC 2.0 million HIV negative men aged 15−49, approximately 80% of the eligible population by 2015.
Objectives of this analysis: Assess risk compensatory behaviors post MC
• Focus on men in a population based cohort• Across 2 years of observation• Assessing 6 indictors of risk behavior• Estimation methods account of selectivity of uptake
of circumcision

Kisumu, Kenya: Mattson et al., 2008 (sub-study)• Propensity score of 18 risk behaviors
• Incident infections of gonorrhea, chlamydia, trich
•No stat sign. differences: MC, not MC; all declined
• HIV testing and counseling: 1m, 3m, 6m, 12m
Rakia, Uganda: Gray et al., 2012 • Post-trial FU for 2-years (control, MC) - 22% no MC
• No observable self-selection MC, ~MC
• Sex active 12m, # partners, condom use, alcohol
• No stat. sign. differences MC & non-MC
• HIV testing & health education : Enroll, 6m, 12m, 24m
Risk compensation: Evidence

Question
What about risk compensation in a program with national scale and less intensive counseling and follow-up?
Example: Zambia
Over 725,000 circumcisions conducted since 2008.

MethodsSince 2010, PC has been annually following a representative cohort of men & women in Zambia.
Primary objective: To assess the prevalence of risk compensation post-VMMC.
Information collected:• Demographics• VMMC Knowledge, beliefs and attitudes• VMMC status and timing• Sexual behavior and experiences of STIs • Perceptions of HIV risk

Methods (cont.)To-date, the study has collected three rounds of data within a 24 month timeframe
• Round 1 Nov 2010 to Apr 2011• Round 2 Sep 2011 to Dec 2011• Round 3 Sep 2012 to Jan 2013• Round 4 Oct 2013 to Feb 2014
Round 1 Round 2 Round 3N 2334 1968 1920
R1-R2 R1-R3Response rate 81 84 82
Attrition rate -- 16 18

Methods (cont.)
Indicators assessing risk compensation• Sex with 2+ partner in last year• Unprotected sex• Sex after alcohol use• Experience of STI symptom in last year• Paid for sex in last year
Statistical Analysis• Instrumental variables GMM regression• Logit regression with fixed effects• Difference-in-difference matching
Estimation approaches addresses endogeneity of circumcision uptake

Results – MC UptakeSince 2008 through early 2013…
21% of sample men were recently circumcised 16% between R1 (2010) & R3 (2013).
R1 R2 R30
5
10
15
20
25Percent of Men Circumcised
Round 1 Round 2 Round 3
Perc
ent
5%
12%
21%
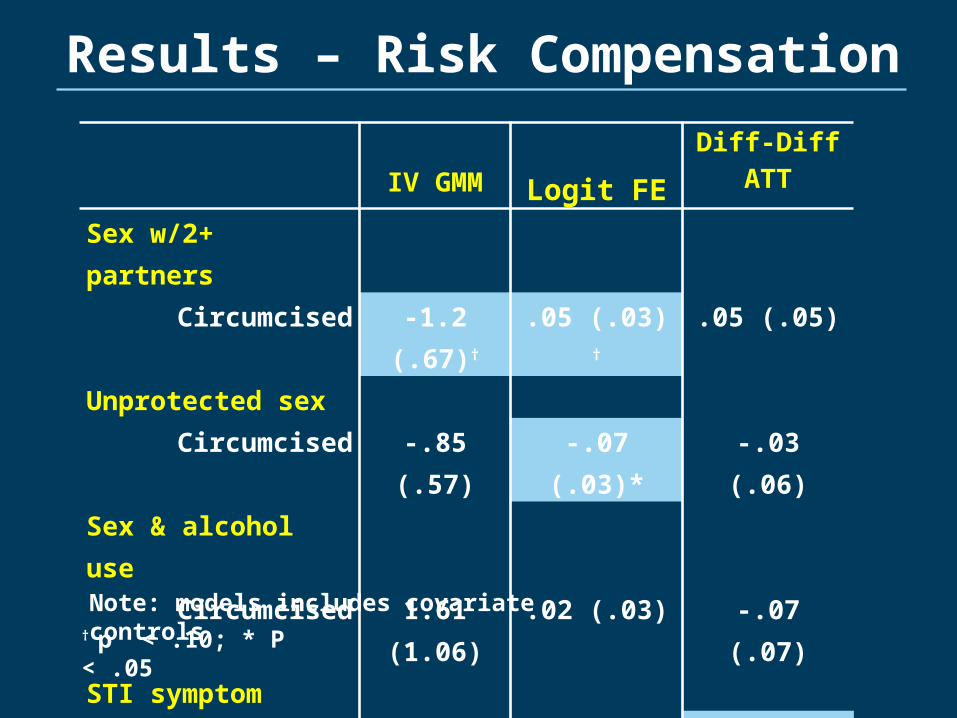
Results – Risk Compensation
IV GMM Logit FEDiff-Diff
ATT
Sex w/2+ partnersCircumcised -1.2 (.67)† .05 (.03) † .05 (.05)
Unprotected sexCircumcised -.85 (.57) -.07 (.03)* -.03 (.06)
Sex & alcohol useCircumcised 1.61 (1.06) .02 (.03) -.07 (.07)
STI symptomCircumcised -.08 (.27) .01 (.02) -.06 (.03)*
Paid for SexCircumcised -1.39 (.65)* .03 (.02) .09 (.04)*
† p < .10; * P < .05
Note: models includes covariate controls

Conclusions
10Source: Hallet et al., 2008 – Southern Africa
• MC men may be less risky than uncircumcised
• No evidence of risk compensation in 2-years
Controlling for endogeneity of circumcision uptake…

The Population Council conducts research and delivers solutions that improve lives around the world. Big ideas supported by evidence: It’s our model for global change.
Ideas. Evidence. Impact.