aspect irm de la cytosteatonecrosepe.sfrnet.org/data/moduleconsultationposter/pdf/2004/1/7...cohen...
TRANSCRIPT

J.VILLEVAL(1), F.DELAUNAY(1), M de GRAEF(1),
C.PIGNODEL(3),R.GUILLON(1), C. PROUST(2)
A.MAUBON(2), JP.ROUANET(1)
ASPECT IRM DE LA
CYTOSTEATONECROSE
(1) Imagerie médicale, CMC Beausoleil, Montpellier,
France
(2) Service de radiologie, CHU Dupuytren, Limoges,
France
(3) Anatomo-pathologie, CHU Nimes

INTERET
•Une cytostéatonécrose peut survenir après un
traitement chirurgical conservateur, un acte
biopsique, une radiothérapie ou plus généralement
tout traumatisme du sein.
• Dans ce contexte, un foyer de cytostéatonécrose
mammaire peut ressembler à une récidive
tumorale clinique, mammographique ou
échographique.

BASES ANATOMO-
PATHOLOGIQUES
•La cytosteatonécrose est définie par la
dégradation enzymatique du tissu adipeux par les
propres lipases cytoplasmiques des adipocytes.
Sous l ’action lipasique, les triglycérides sont
scindés en glycérol rapidement résorbé et en
acides gras : une petite quantité de ces derniers se
cristallise sur place ; la majeure partie subit une
saponification aboutissant à la formation de
savon, spécialement de savon calcaire.

BASES ANATOMO-
PATHOLOGIQUES
• La morphologie d ’un foyer de cytostéatonécrose est stéréotypé. Toute structure locale normale a disparu à ce niveau.
• Il est constitué par un matériel nécrotique granuleux, irrégulièrement acidophile, dans lequel persistent, par plages, des noyaux pycnotiques et des membranes cellulaires dessinant les contours de « fantômes adipocytaires ».
• Un granulome lipophagique entoure tardivement la zone de cytostéatonécrose ; puis, l ’évolution se fait vers une sclérose d ’encerclement.

BASES ANATOMO-
PATHOLOGIQUES
• Il peut en résulter une rétraction fibreuse périphérique
plus ou moins vascularisée pouvant en imagerie
classique prendre l’aspect d’une masse irrégulière et
spiculée.
• La lésion s’entoure d’une pseudo-capsule fibreuse dense
avec des zones focales de calcifications.
• A l ’œil nu, le foyer de cytostéatonécrose est blanchâtre
comme du suif avec une consistance crayeuse classique qui
tranche avec le fond jaune du tissu adipeux normal
environnant.
BASES ANATOMO-
PATHOLOGIQUES
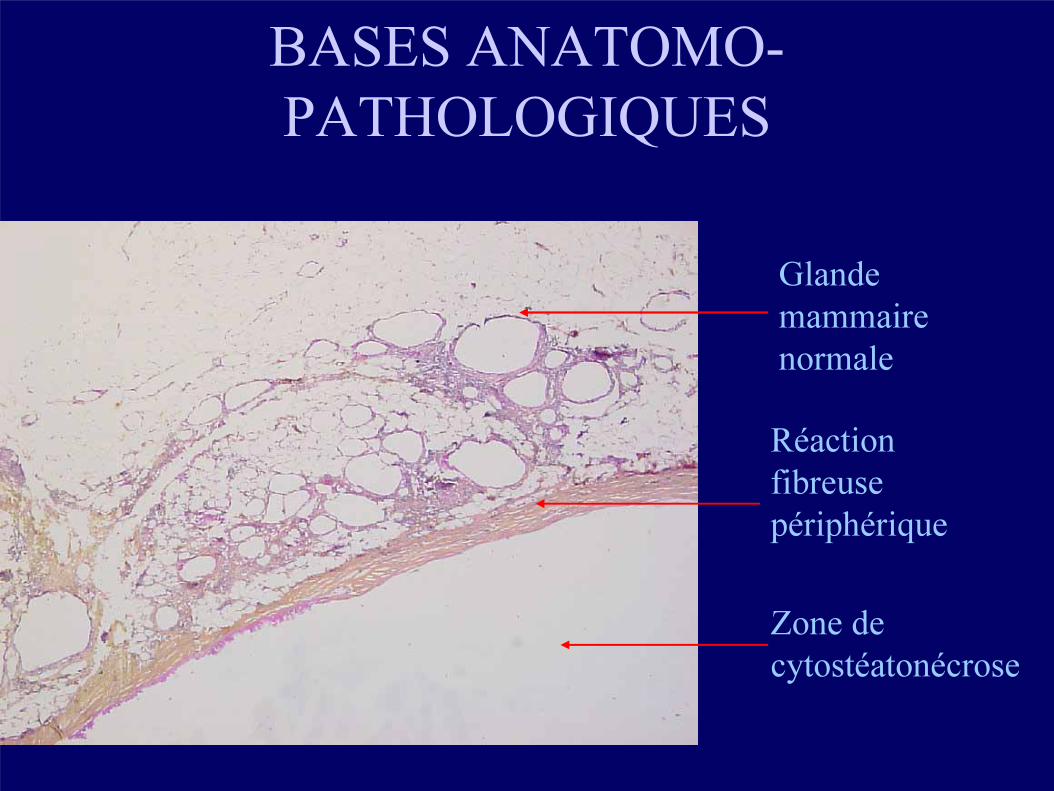
Glande
mammaire
normale
Réaction
fibreuse
périphérique
Zone de
cytostéatonécrose

BASES ANATOMO-
PATHOLOGIQUES
Aspect macroscopique
Glande mammaire normale
Réaction fibreuse périphérique
Zone de cytostéatonécrose
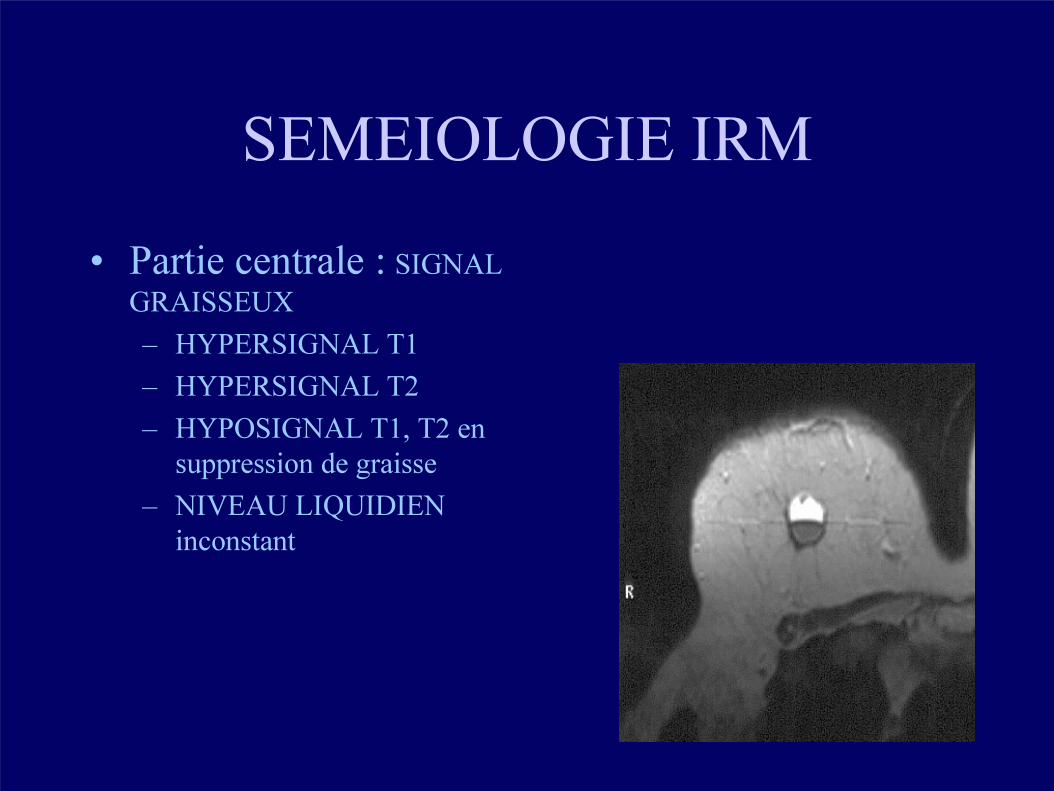
SEMEIOLOGIE IRM
• Partie centrale : SIGNAL
GRAISSEUX
– HYPERSIGNAL T1
– HYPERSIGNAL T2
– HYPOSIGNAL T1, T2 en
suppression de graisse
– NIVEAU LIQUIDIEN
inconstant

SEMIOLOGIE IRM
SE T1 SE T2

SEMEIOLOGIE IRM
ECHO DE GRADIENT T1avec suppression du signal graisseux

SEMEIOLOGIE IRM
• Partie périphérique annulaire:
– SIGNAL TISSULAIRE FIBREUX
– HYPOSIGNAL T1
– HYPERSIGNAL T2

SEMIOLOGIE IRM
• T1 GADOLINIUM
• VARIABLE
– ABSENCE DE PRISE DE CONTRASTE DE LA PARTIE CENTRALE
– PRISE DE CONTRASTE PERIPHERIQUE :• ABSENTE OU MINIME
• LOCALISEE OU ANNULAIRE
• PRECOCE (1min 30)
• vasculaire SANS WASHOUT
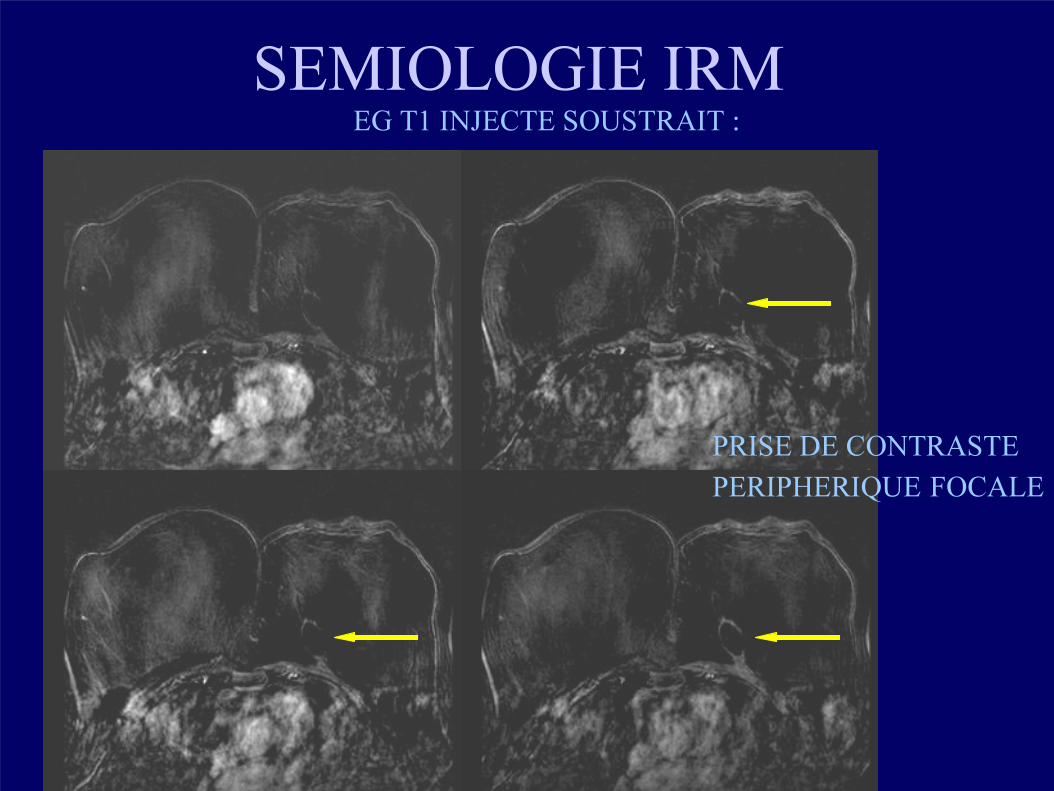
SEMIOLOGIE IRM EG T1 INJECTE SOUSTRAIT :
PRISE DE CONTRASTE
PERIPHERIQUE FOCALE

SEMIOLOGIE IRM • PENTE
L12 : partie périphérique
L13 : graisse
L14 : glande
PAS DE REHAUSSEMENT
SIGNIFICATIF
L12
L13
L14

CAS CLINIQUES

Femme 67 ans ,antécédents de chirurgie conservatrice du
sein.
Contrôle mammographique.

IRM
Ax T1
Ax T1
Suppression
de graisse
Ax T1
Gadolinium
Suppression de graisse
Lésion apparaîssant en hypersignal T1.
S’effaçant sur la séquence T1 suppression de graisse. Pas de
prise de contraste après injection de Gadolinium.
Foyer de cytostéatonécrose.
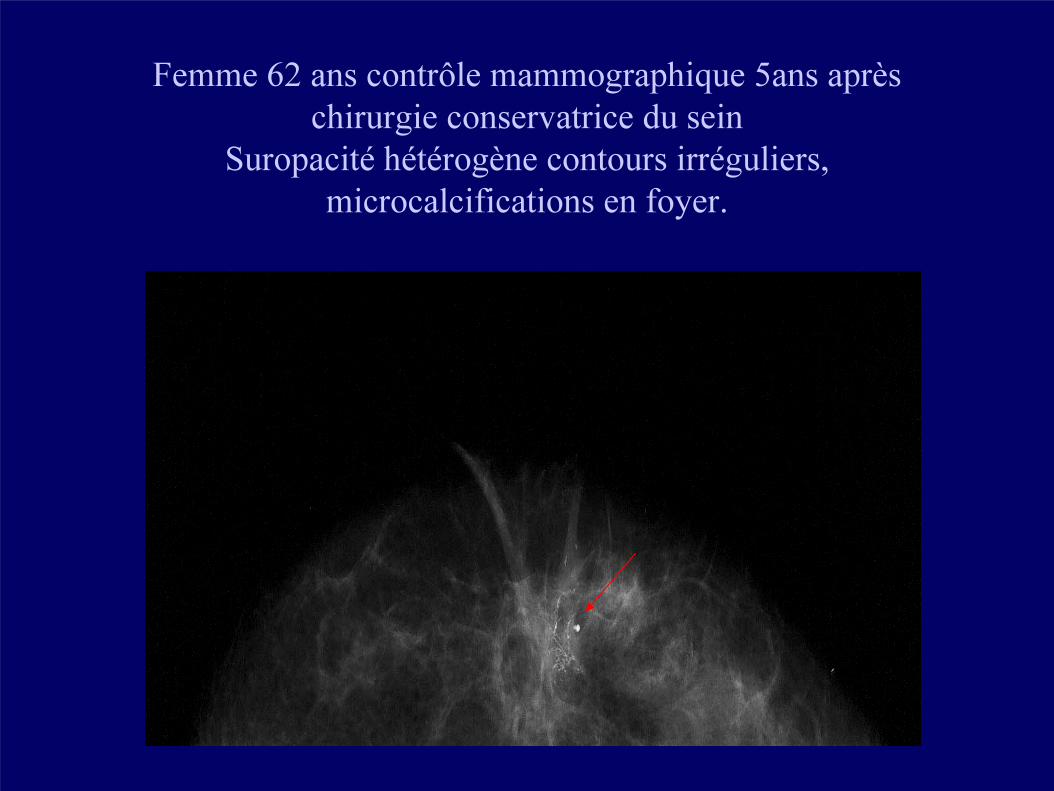
Femme 62 ans contrôle mammographique 5ans après
chirurgie conservatrice du sein
Suropacité hétérogène contours irréguliers,
microcalcifications en foyer.

IRM
Ax T2 suppression de graisse Ax T1
Ax T1 suppression de graisseAx T1 suppression
de graisse gadolinium
Hyposignal plus marqué en T1 et T2 suppression de graisse.Pas
de prise de contraste. Probable foyer de cytostéanécrose.

Femme 58ans antécédents de carcinome mammaire traité par
chirurgie conservatrice et radiothérapie.
Ax T1
Ax T2
Ax T2 suppression de graisse
Foyer de cytostéatonécrose, pas de réhaussement significatif
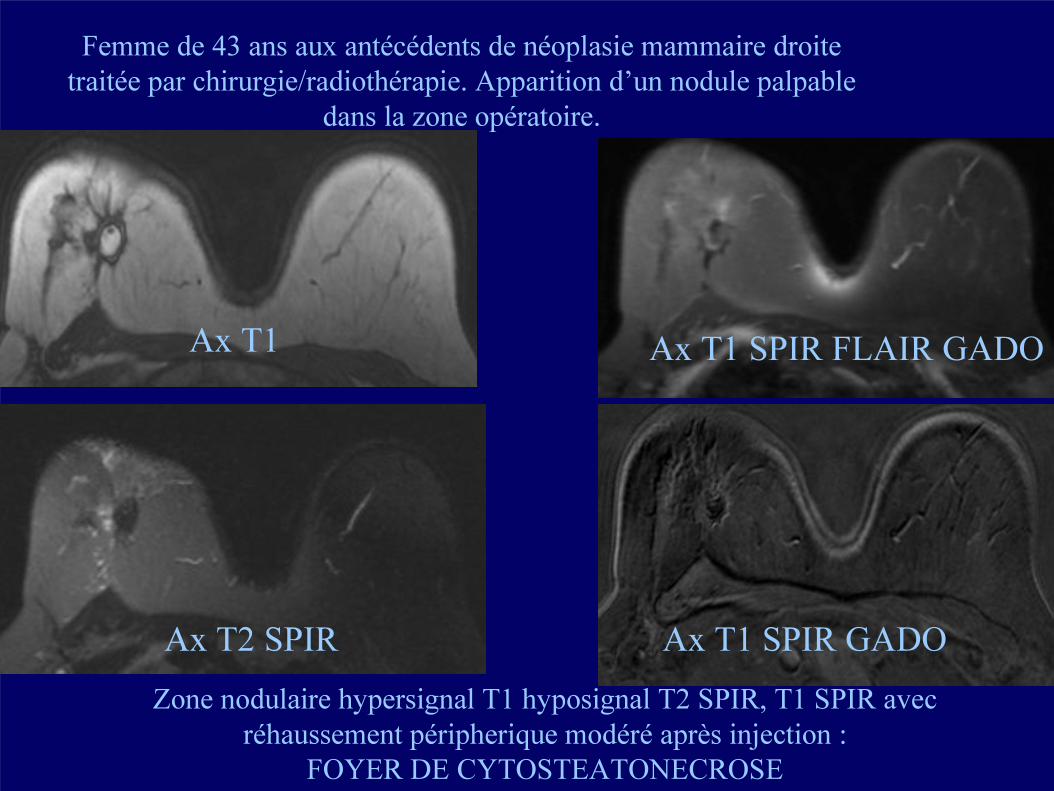
Femme de 43 ans aux antécédents de néoplasie mammaire droite
traitée par chirurgie/radiothérapie. Apparition d’un nodule palpable
dans la zone opératoire.
Ax T1
Ax T2 SPIR
Ax T1 SPIR FLAIR GADO
Ax T1 SPIR GADO
Zone nodulaire hypersignal T1 hyposignal T2 SPIR, T1 SPIR avec
réhaussement péripherique modéré après injection :
FOYER DE CYTOSTEATONECROSE
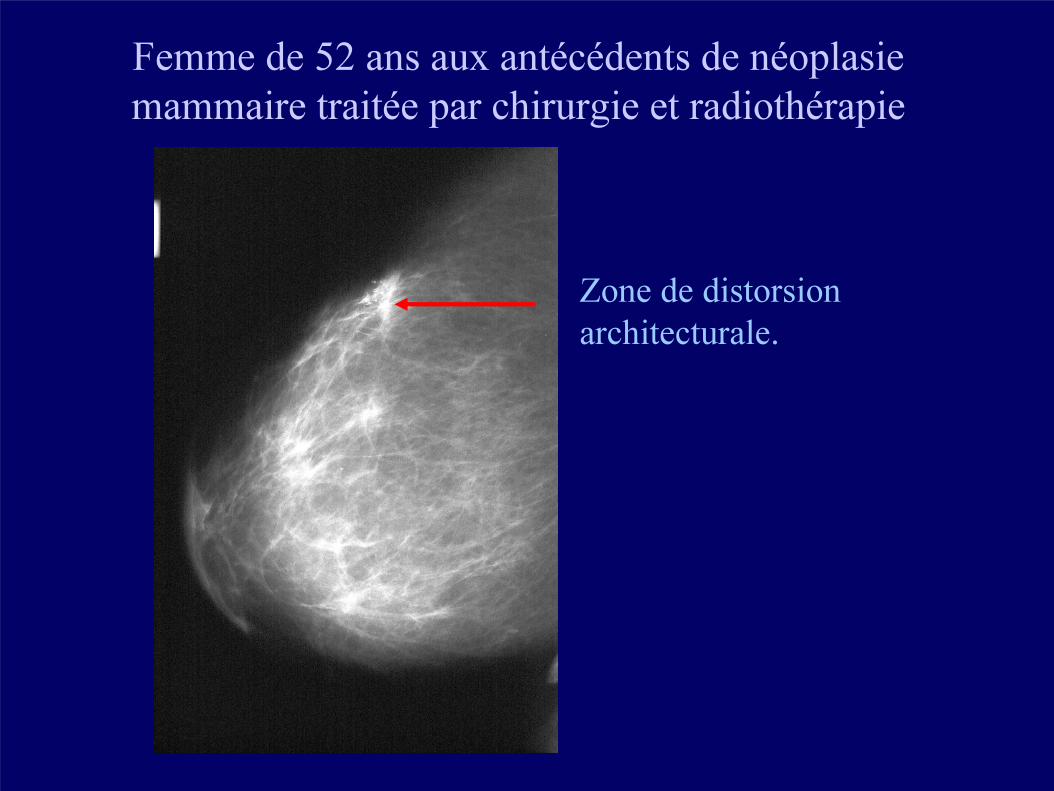
Femme de 52 ans aux antécédents de néoplasie
mammaire traitée par chirurgie et radiothérapie
Zone de distorsion
architecturale.
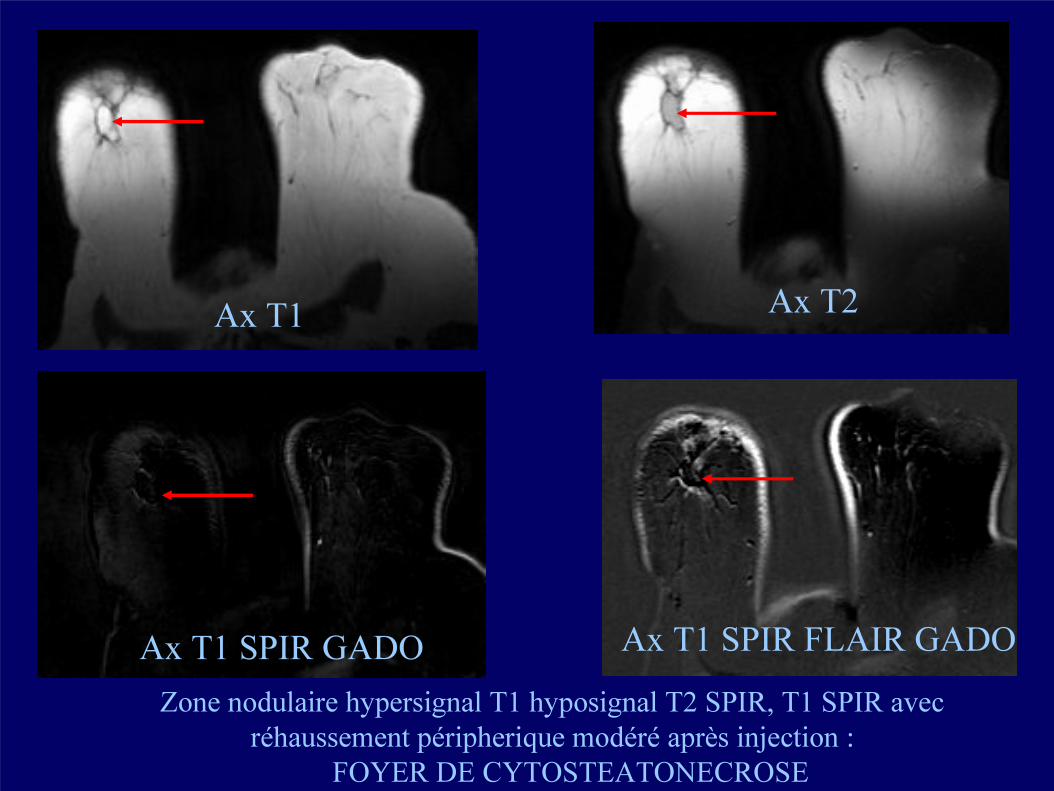
Ax T1 Ax T2
Ax T1 SPIR GADO Ax T1 SPIR FLAIR GADO
Zone nodulaire hypersignal T1 hyposignal T2 SPIR, T1 SPIR avec
réhaussement péripherique modéré après injection :
FOYER DE CYTOSTEATONECROSE

• l’ IRM mammaire est indispensable dans une surveillance discriminative des cancers du sein opérés.
• Toute prise de contraste nouvelle évoque a priori une récidive ; la sémeiologie IRM de la cytostéatonécrose est très proche de l’anatomie pathologique macroscopique, ce qui majore encore l’importance de l’IRM pour la surveillance post-thérapeutique des cancers du sein.
• Recours à la ponction biopsie si doute en particulier, en cas de prise de contraste non spécifique associée.
CONCLUSION

BIBLIOGRAPHIE
1. Kinoshita T, Yashiro N, Yoshigi J, Ihara N, Narita M.
Fat necrosis of breast: a potential pitfall in breast MRI.Clin Imaging. 2002 Jul-Aug;26(4):250-3.
2. Gilles R.
Clinical case 2. Magnetic Resonance Imaging and PET of the breastJ Radiol. 2002 Apr;83(4 Pt 2):578-80.
3. Solomon B, Orel S, Reynolds C, Schnall M.
Delayed development of enhancement in fat necrosis after breast conservation therapy: a potential pitfall of MR imaging of the breast.AJR Am J Roentgenol. 1998 Apr;170(4):966-8.

BIBLIOGRAPHIE
4. Coady AM, Mussurakis S, Owen AW, Turnbull LW
Case report: MR imaging of fat necrosis of the breast associated with lipid cyst formation following conservative treatment for breast carcinoma.Clin Radiol. 1996 Nov;51(11):815-7.
5. Kurtz B, Achten C, Audretsch W, Rezai M, Zocholl G.
MR mammography of fatty tissue necrosis
Rofo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr. 1996 Oct;165(4):359-63.
6. Cohen EK, Leonhardt CM, Shumak RS, Soutar IC, Bukhanov K, Fishell EK, Plewes DB
Magnetic resonance imaging in potential postsurgical recurrence of breast cancer: pitfalls and limitations.Can Assoc Radiol J. 1996 Jun;47(3):171-6.
7. Kurtz B, Audretsch W, Rezai M, Achten C, Zocholl G
Initial experiences with MR-mammography in after-care following surgical flap treatment of breast carcinomaRofo Fortschr Geb Rontgenstr NeuenBildgeb Verfahr. 1996 Apr;164(4):295-300.
BIBLIOGRAPHIE
8. Cohen EK, Leonhardt CM, Shumak RS, Soutar IC, Bukhanov K, Fishell EK, Plewes DB. Magnetic resonance imaging in potential postsurgical recurrence of breast cancer: pitfalls and limitations.Can Assoc Radiol J. 1996 Jun;47(3):171-6.
9. Kurtz B, Audretsch W, Rezai M, Achten C, Zocholl G.Initial experiences with MR-mammography in after-care following surgical flap treatment of breast carcinomaRofo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr. 1996 Apr;164(4):295-300.
10. Gilles R, Guinebretiere JM, Shapeero LG, Lesnik A, Contesso G, Sarrazin D,
Masselot J, Vanel D
Assessment of breast cancer recurrence with contrast-enhanced subtraction MR
imaging: preliminary results in 26 patients.
Radiology. 1993 Aug;188(2):473-8.

BIBLIOGRAPHIE
10. Gilles R, Guinebretiere JM, Shapeero LG, Lesnik A, Contesso G, Sarrazin D,
Masselot J, Vanel D
Assessment of breast cancer recurrence with contrast-enhanced subtraction
MR imaging: preliminary results in 26 patients.
Radiology. 1993 Aug;188(2):473-8.
11. Pierce WB, Harms SE, Flamig DP, Griffey RH, Evans WP, Hagans JE
Three-dimensional gadolinium-enhanced MR imaging of the breast: pulse
sequence with fat suppression and magnetization transfer contrast. Work in
progress.
Radiology. 1991 Dec;181(3):757-63.

BIBLIOGRAPHIE
13. F. Cabanne, JL Bonenfant. Anatomie pathologique : principes de pathologie générale, de pathologie spéciale et d ’aetopathologie. p394-395. Maloine SA Editeur. Paris.
14. H. Iwasaki, K. Morimoto, M. Koh, T. Okamura, T. Wasaka, H. Kinoshita. A case of fat necrosis after breast quadrantectomy in whish preoperativediagnosis was enable by MRI with fat suppression technique. MagneticResonance Imaging. 22(2):285-90, 2004 Feb.
15. T. Kinoshita, N. Yashiro, J.Yoshigi, N. Ihara, M. Narita. Fat necrosis of breast: a potential pitfall in breast MRI.Clinical Imaging. 26(4):250-3, 2002 Jul-Aug.
16. JA Lopez, F Saez, J Alejandro Larena, A Capelastegui, JI Martin, B Canteli. MRI diagnosis and follow-up of subcutaneous fat necrosis. Journal ofMagnetic Resonance Imaging. 7(5):929-32, 1997 Sep-Oct.