applied feline oral anatomy and tooth extraction
TRANSCRIPT
900 JFMS CLINICAL PRACTICE
Journal of Feline Medicine and Surgery (2014) 16, 900–913
C L I N I C A L R E V I E W
Alexander M ReiterDipl Tzt Dr med vet DAVDC DEVDC*
Maria M Soltero-RiveraDVM DAVDC
Department of Clinical Sciences, School of Veterinary Medicine, University of Pennsylvania,3900 Delancey Street, Philadelphia, PA, USA
*Corresponding author: [email protected]
doi: 10.1177/1098612X14552365
© iSFM and AAFP 2014
Alexander M Reiter and Maria M Soltero-Rivera
APPLIED FELINE ORAL ANATOMY ANDTOOTH EXTRACTION TECHNIQUESAn illustrated guide
Practical relevance: Tooth extraction is one of the most commonly performedsurgical procedures in small animalpractice.Clinical challenges: The clinician must
be familiar with normal oral anatomy,utilize nomenclature accepted in dentistry and
oral surgery, use the modified Triadan system fornumbering teeth, identify normal structures on adental radiograph, understand the tissues that holdthe teeth in the jaws, know the biomechanicalprinciples of tooth extraction, be able to choose themost appropriate instrument for removal of a tooth,extract teeth using closed and open techniques,and create tension-free flaps for closure ofextraction sites.Audience: This review is intended to familiarizeboth the general and referral practitioner with felineoral anatomy and tooth extraction techniques.Patient group: Tooth extraction is predominantlyperformed in cats with tooth resorption, chronicgingivostomatitis and periodontal disease.Equipment: The basic contents of a feline toothextraction kit are explained.Evidence base: The guidance contained withinthis review is based on a combination of thepublished literature, the authors’ personalexperience and the experience of colleagues.
Feline oral anatomy
Eruption and types of teethThe kitten’s 26 deciduous teeth erupt at between 2 and 6 weeks of age.The cat’s 30 permanent teeth erupt at between 3 and 6 months of age.Cats have incisors for cutting, prehending and grooming, canines for penetrating, grasping and defense, and cheek teeth (premolars and molars) for holding, carrying, breaking and tearing food. The maxillary fourth premolar and mandibular first molar are the carnas-sial teeth.1–3
Tooth structureEnamel covers the crown and cementum covers the root. These hardtissue layers meet at the cemento-enamel junction near the cervical
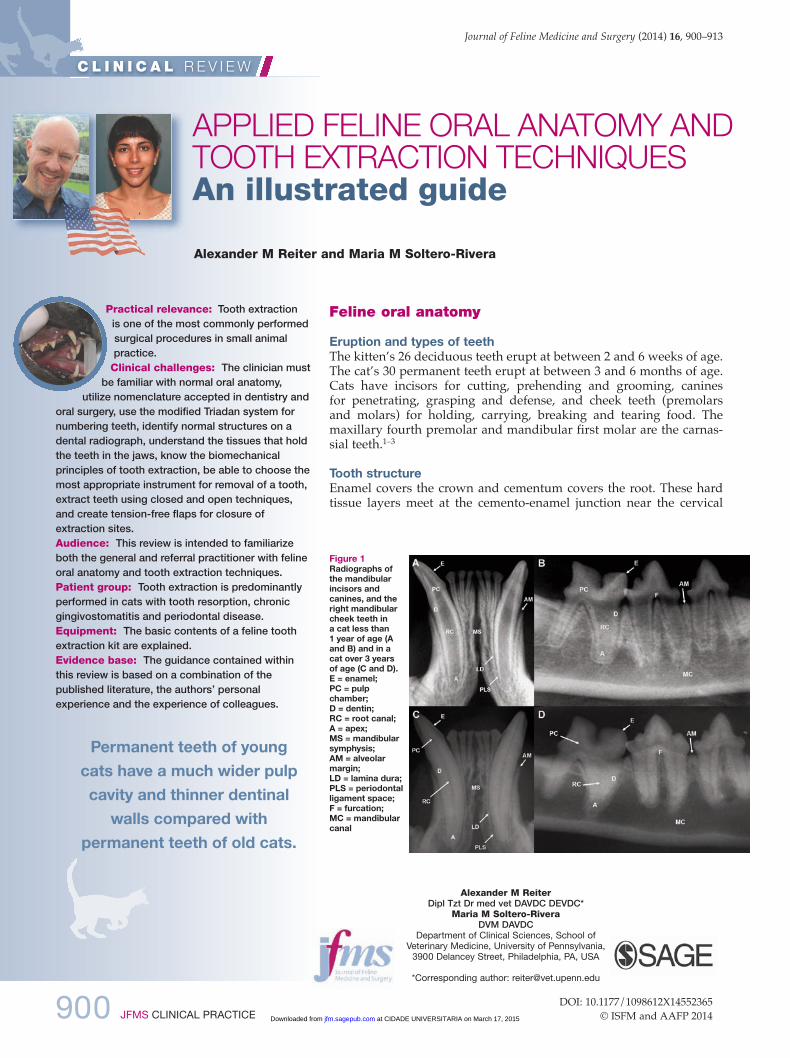
Figure 1Radiographs ofthe mandibularincisors andcanines, and theright mandibularcheek teeth in a cat less than 1 year of age (Aand B) and in acat over 3 yearsof age (C and D). E = enamel; PC = pulpchamber; D = dentin; RC = root canal; A = apex; MS = mandibularsymphysis; AM = alveolarmargin; LD = lamina dura; PLS = periodontalligament space; F = furcation; MC = mandibularcanal
Permanent teeth of youngcats have a much wider pulpcavity and thinner dentinalwalls compared with
permanent teeth of old cats.
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:33 Page 900
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from
JFMS CLINICAL PRACTICE 901
REV IEW / Oral anatomy and tooth extraction
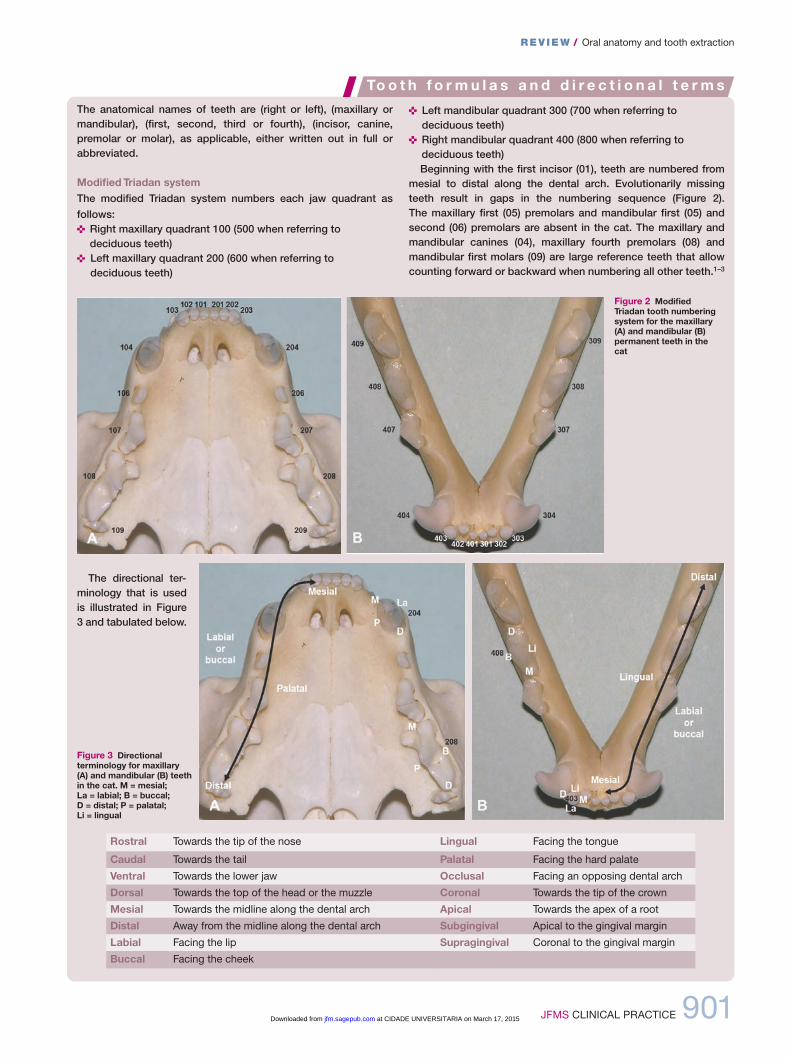
The anatomical names of teeth are (right or left), (maxillary ormandibular), (first, second, third or fourth), (incisor, canine, premolar or molar), as applicable, either written out in full or abbreviated.
Modified Triadan systemThe modified Triadan system numbers each jaw quadrant as follows:< Right maxillary quadrant 100 (500 when referring todeciduous teeth)
< Left maxillary quadrant 200 (600 when referring to deciduous teeth)
< Left mandibular quadrant 300 (700 when referring todeciduous teeth)
< Right mandibular quadrant 400 (800 when referring todeciduous teeth)Beginning with the first incisor (01), teeth are numbered from
mesial to distal along the dental arch. Evolutionarily missingteeth result in gaps in the numbering sequence (Figure 2). The maxillary first (05) premolars and mandibular first (05) andsecond (06) premolars are absent in the cat. The maxillary andmandibular canines (04), maxillary fourth premolars (08) andmandibular first molars (09) are large reference teeth that allowcounting forward or backward when numbering all other teeth.1–3
To o t h f o r m u l a s a n d d i r e c t i o n a l t e r m s
Figure 2 ModifiedTriadan tooth numberingsystem for the maxillary(A) and mandibular (B)permanent teeth in thecat
Figure 3 Directionalterminology for maxillary(A) and mandibular (B) teethin the cat. M = mesial; La = labial; B = buccal; D = distal; P = palatal; Li = lingual
Rostral Towards the tip of the nose Lingual Facing the tongue
Caudal Towards the tail Palatal Facing the hard palate
Ventral Towards the lower jaw Occlusal Facing an opposing dental arch
Dorsal Towards the top of the head or the muzzle Coronal Towards the tip of the crown
Mesial Towards the midline along the dental arch Apical Towards the apex of a root
Distal Away from the midline along the dental arch Subgingival Apical to the gingival margin
Labial Facing the lip Supragingival Coronal to the gingival margin
Buccal Facing the cheek
The directional ter-minology that is usedis illustrated in Figure3 and tabulated below.
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:33 Page 901
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from
902 JFMS CLINICAL PRACTICE
REV IEW / Oral anatomy and tooth extraction
portion of the tooth. dentin makes up the bulkof the mature tooth. The pulp cavity, whichcontains the pulp, is divided into the pulpchamber in the crown and the root canal(s) inthe root(s). The feline pulp connects with peri-apical tissues through several foramina in theroot apex (apical delta). Non-apical ramifica-tions exist in the furcation and other areas ofthe root. odontoblasts at the pulp’s peripheryproduce dentin throughout life in a vitaltooth. Therefore, permanent teeth of youngcats have a much wider pulp cavity and thin-ner dentinal walls (Figure 1) compared withpermanent teeth of old cats.1–3
incisors and canines are single-rooted teeth.Permanent maxillary second premolars andfirst molars often have two roots fused to each other (allowing them to be extractedwithout tooth sectioning). Permanentmandibular third and fourth premolars andfirst molars have two roots, while the maxil-lary fourth premolars have three roots. Thetwo-rooted permanent maxillary third pre -molars occasionally have a third root.4 Thefurcation is where two or more roots meet atthe crown.1–3
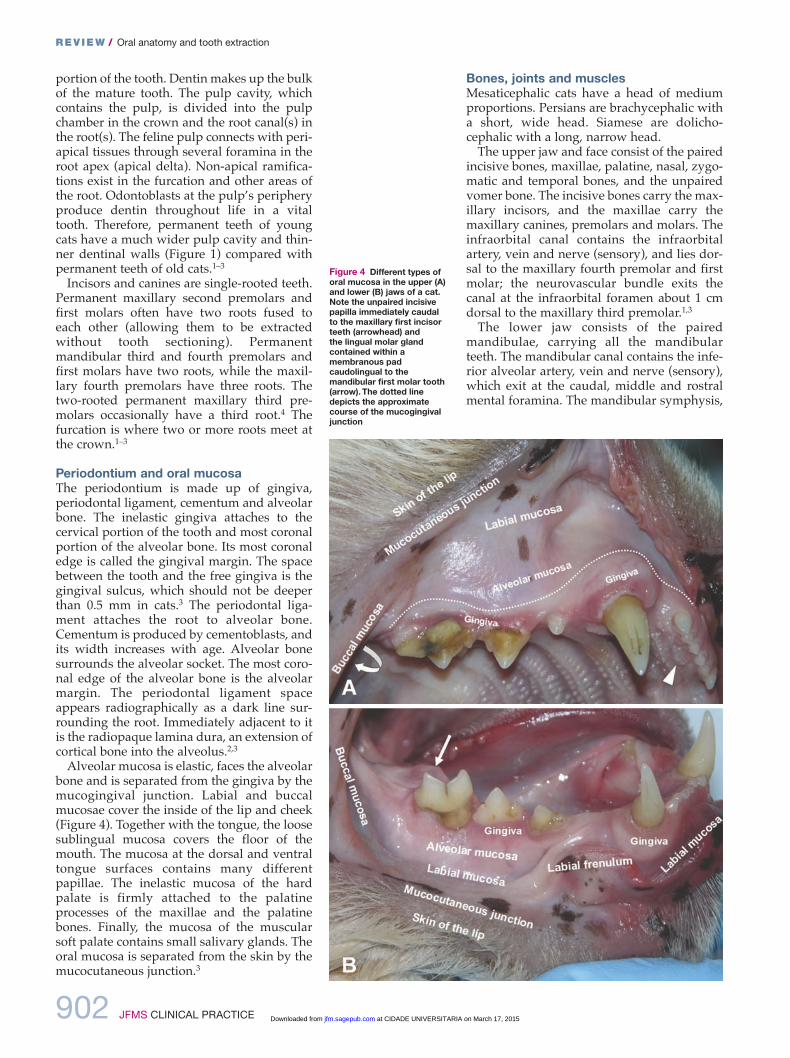
Periodontium and oral mucosaThe periodontium is made up of gingiva, periodontal ligament, cementum and alveolarbone. The inelastic gingiva attaches to the cervical portion of the tooth and most coronalportion of the alveolar bone. its most coronaledge is called the gingival margin. The spacebetween the tooth and the free gingiva is thegingival sulcus, which should not be deeperthan 0.5 mm in cats.3 The periodontal liga-ment attaches the root to alveolar bone.Cementum is produced by cementoblasts, andits width increases with age. Alveolar bonesurrounds the alveolar socket. The most coro-nal edge of the alveolar bone is the alveolarmargin. The periodontal ligament spaceappears radiographically as a dark line sur-rounding the root. immediately adjacent to itis the radiopaque lamina dura, an extension ofcortical bone into the alveolus.2,3
Alveolar mucosa is elastic, faces the alveolarbone and is separated from the gingiva by themucogingival junction. Labial and buccalmucosae cover the inside of the lip and cheek(Figure 4). Together with the tongue, the loosesublingual mucosa covers the floor of themouth. The mucosa at the dorsal and ventraltongue surfaces contains many differentpapillae. The inelastic mucosa of the hardpalate is firmly attached to the palatineprocesses of the maxillae and the palatinebones. Finally, the mucosa of the muscularsoft palate contains small salivary glands. Theoral mucosa is separated from the skin by themucocutaneous junction.3
Bones, joints and musclesMesaticephalic cats have a head of mediumproportions. Persians are brachycephalic witha short, wide head. Siamese are dolicho-cephalic with a long, narrow head.
The upper jaw and face consist of the pairedincisive bones, maxillae, palatine, nasal, zygo-matic and temporal bones, and the unpairedvomer bone. The incisive bones carry the max-illary incisors, and the maxillae carry the maxillary canines, premolars and molars. Theinfra orbital canal contains the infraorbitalartery, vein and nerve (sensory), and lies dor-sal to the maxillary fourth premolar and firstmolar; the neurovascular bundle exits thecanal at the infraorbital foramen about 1 cmdorsal to the maxillary third premolar.1,3
The lower jaw consists of the pairedmandibulae, carrying all the mandibularteeth. The mandibular canal contains the infe-rior alveolar artery, vein and nerve (sensory),which exit at the caudal, middle and rostralmental foramina. The mandibular symphysis,
Figure 4 Different types oforal mucosa in the upper (A)and lower (B) jaws of a cat.Note the unpaired incisivepapilla immediately caudalto the maxillary first incisorteeth (arrowhead) and the lingual molar glandcontained within amembranous padcaudolingual to themandibular first molar tooth(arrow). The dotted linedepicts the approximatecourse of the mucogingivaljunction
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:33 Page 902
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from
JFMS CLINICAL PRACTICE 903
a fibrocartilaginous synchondrosis, connectsthe two mandibles rostrally. The condylarprocess of the mandible and the mandibularfossa and retroarticular process of the tempo-ral bone form the temporomandibular joint.
The masseter, temporal and pterygoid(medial and lateral) muscles close the mouth.The digastricus muscles open the mouth.1,3
Lips and cheeksThe upper and lower lips meet at the commis-sure. The dorsal and ventral buccal branchesof the facial nerve (for motor innervation) runover the masseter muscle in a caudorostraldirection into the cheek. Traversing inbetween the two nerves is the parotid duct,which opens into the mouth at the parotidpapilla in the buccal mucosa near the maxil-lary fourth premolar.1–3
PalateThe roof of the mouth is divided into non-elas-tic hard palate and elastic soft palate. The hardpalate mucosa has several transverse ridges(palatine rugae). The unpaired incisive papillais immediately caudal to the maxillary first inci-sor teeth. The paired major palatine arteriescourse from the major palatine fora mina at thelevel of the maxillary fourth pre molars rostrallyto the palatine fissures. Palatoglossal foldsemerge when the tongue is withdrawn from themouth, running from the body of the tongue tothe rostrolateral aspect of the soft palate.1,3
TongueThe cat uses its muscular tongue to lap fluids,form food boluses and groom the fur. The ros-tral two-thirds are the body of the tongue; thecaudal one-third is the root of the tongue. Therough dorsal tongue surface has firm papillaepointing caudally. The lingual frenulum con-nects the lingual body to the floor of the mouth.The mandibular and sublingual ducts open atthe sublingual caruncles at the rostroventralbase of the frenulum. The paired lingual arteriessupply the tongue. The lingual and facial nerveprovide sensory function, while the hypoglossalnerve is responsible for motor function.1,3
Salivary glands, lymph nodes and tonsilsCats have four pairs of major salivary glands(parotid, sublingual, mandibular and zygo-matic). Scattered glandular tissue is presentsubmucosally in the lips, cheeks and softpalate. Caudolingual to each mandibular firstmolar tooth is a small lingual molar glandcontained within a membranous pad.2,5 Thereare three lymph centers in the head (parotid,mandibular and retropharyngeal). The pala-tine tonsils are attached to the dorsal aspect ofthe lateral pharyngeal walls, which are alsocalled the fauces.1–3
REV IEW / Oral anatomy and tooth extraction
Equipment, instruments andmaterials for tooth extraction
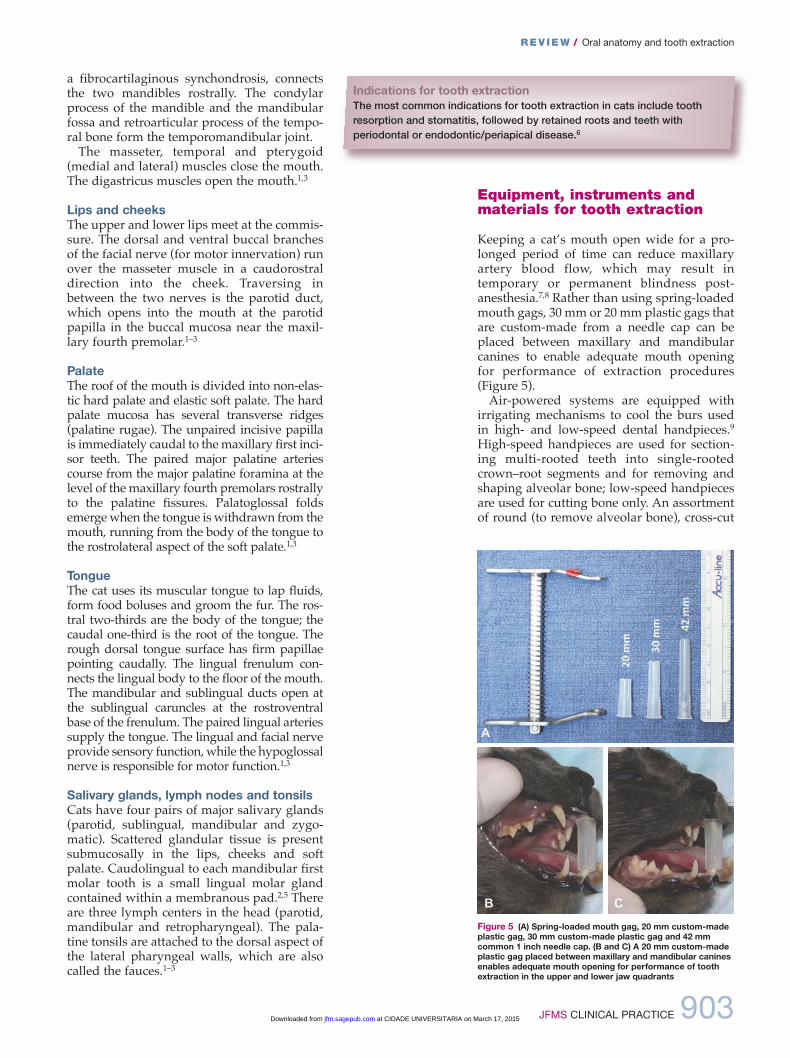
Keeping a cat’s mouth open wide for a pro-longed period of time can reduce maxillaryartery blood flow, which may result in temporary or permanent blindness post-anesthesia.7,8 Rather than using spring-loadedmouth gags, 30 mm or 20 mm plastic gags thatare custom-made from a needle cap can beplaced between maxillary and mandibularcanines to enable adequate mouth opening for performance of extraction procedures(Figure 5).
Air-powered systems are equipped withirrigating mechanisms to cool the burs used in high- and low-speed dental handpieces.9
High-speed handpieces are used for section-ing multi-rooted teeth into single-rootedcrown–root segments and for removing andshaping alveolar bone; low-speed handpiecesare used for cutting bone only. An assortmentof round (to remove alveolar bone), cross-cut
Indications for tooth extractionThe most common indications for tooth extraction in cats include toothresorption and stomatitis, followed by retained roots and teeth withperiodontal or endodontic/periapical disease.6
Figure 5 (A) Spring-loaded mouth gag, 20 mm custom-madeplastic gag, 30 mm custom-made plastic gag and 42 mmcommon 1 inch needle cap. (B and C) A 20 mm custom-madeplastic gag placed between maxillary and mandibular caninesenables adequate mouth opening for performance of toothextraction in the upper and lower jaw quadrants
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:33 Page 903
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from
904 JFMS CLINICAL PRACTICE
REV IEW / Oral anatomy and tooth extraction
Luxators andelevators are
grasped with thebutt of the handleseated in the palm,and the index fingerextended along the blade to act as a stop in case of
slippage.
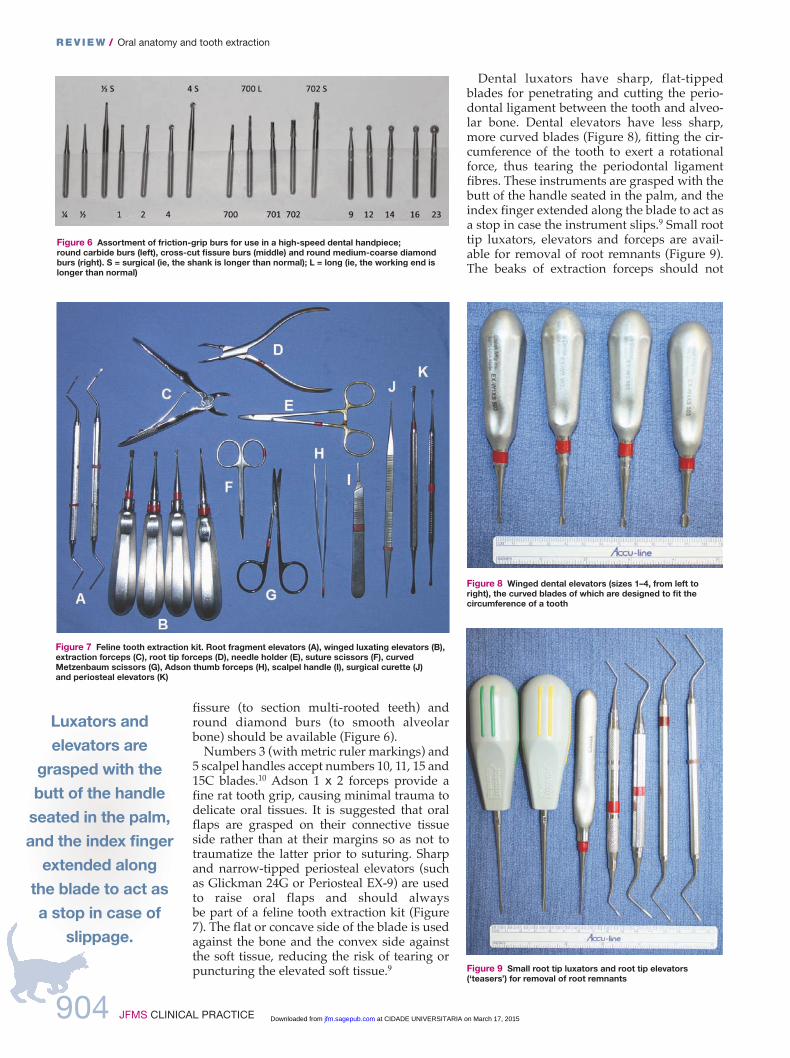
fissure (to section multi-rooted teeth) andround diamond burs (to smooth alveolarbone) should be available (Figure 6).
Numbers 3 (with metric ruler markings) and5 scalpel handles accept numbers 10, 11, 15 and15C blades.10 Adson 1 x 2 forceps provide afine rat tooth grip, causing minimal trauma todelicate oral tissues. it is suggested that oralflaps are grasped on their connective tissueside rather than at their margins so as not totraumatize the latter prior to suturing. Sharpand narrow-tipped periosteal elevators (suchas Glickman 24G or Periosteal EX-9) are usedto raise oral flaps and should always be part of a feline tooth extraction kit (Figure7). The flat or concave side of the blade is usedagainst the bone and the convex side againstthe soft tissue, reducing the risk of tearing orpuncturing the elevated soft tissue.9
dental luxators have sharp, flat-tippedblades for penetrating and cutting the perio -dontal ligament between the tooth and alveo-lar bone. dental elevators have less sharp,more curved blades (Figure 8), fitting the cir-cumference of the tooth to exert a rotationalforce, thus tearing the periodontal ligamentfibres. These instruments are grasped with thebutt of the handle seated in the palm, and theindex finger extended along the blade to act asa stop in case the instrument slips.9 Small roottip luxators, elevators and forceps are avail-able for removal of root remnants (Figure 9).The beaks of extraction forceps should not
Figure 6 Assortment of friction-grip burs for use in a high-speed dental handpiece; round carbide burs (left), cross-cut fissure burs (middle) and round medium-coarse diamondburs (right). S = surgical (ie, the shank is longer than normal); L = long (ie, the working end islonger than normal)
Figure 7 Feline tooth extraction kit. Root fragment elevators (A), winged luxating elevators (B),extraction forceps (C), root tip forceps (D), needle holder (E), suture scissors (F), curvedMetzenbaum scissors (G), Adson thumb forceps (H), scalpel handle (I), surgical curette (J) and periosteal elevators (K)
Figure 8 Winged dental elevators (sizes 1–4, from left toright), the curved blades of which are designed to fit thecircumference of a tooth
Figure 9 Small root tip luxators and root tip elevators(‘teasers’) for removal of root remnants
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:33 Page 904
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from

JFMS CLINICAL PRACTICE 905
REV IEW / Oral anatomy and tooth extraction
fully close but still fit the circumference offeline teeth, thus reducing the risk of toothfracture when a tooth or crown–root segmentis grasped as far apically as possible for itsremoval.11
Surgical curettes are used for removal ofdebris and granulation tissue from an alveolarsocket after tooth extraction. Curved, blunt-ended Metzenbaum scissors with serratedblades are used for dissecting the connectivetissue side of oral flaps and fine cutting oftheir edges prior to wound closure. Specificsuture scissors or a designated pair of Mayoscissors should be reserved for cuttingsutures.10 Halsey or deBakey needle holderswith serrated jaws are used to lock ontocurved needles by a ratchet mechanism. Theauthors prefer a size 5-0 synthetic, absorbablemonofilament ma terial with a swaged-on,taper-point round, non-cutting needle forsuturing tooth extraction sites in cats (Figure10). Square or surgeon’s knots should be followed by four more throws to ensure knotsecurity.9
Chlorhexidine gluconate (0.12%) is used forrinsing the mouth prior to tooth extraction.The results of a study conducted on caninefibroblasts suggest that the least toxic solutionfor rinsing open wounds is lactated Ringer’ssolution.9 Autogenous bone (cancellous boneand cortical bone chips) as well as allograft-based (demineralized bone of the samespecies) and ceramic-based (calcium phos-phate, calcium sulfate and bioglass) bone graftsubstitutes are most commonly used in veteri-nary dentistry, although they are not routinelyneeded in extraction sites.12,13 Gauze swabs(size 3 x 3 inches, 7.5 x 7.5 cm) allow digitalcontrol of hemorrhage during tooth extractionprocedures. Lavage with refrigerated lactatedRinger’s solution may also provide goodhemostasis. Excessive bleeding from toothextraction sites near tubular structures such asthe mandibular and infraorbital canals caneffectively be controlled by packing the alveo-lar sockets with a small amount of bone wax (asterile beeswax-based compound).9
Tooth extraction techniques
Closed extractionClosed extraction in the cat is primarily performed for maxillary and mandibular incisors, maxillary second premolars, maxil-lary first molars, and mobile teeth presentingwith significant attachment loss. Employing aclosed extraction technique for other teethrisks their fracture, which then warrants anopen extraction technique in order to removeroot remnants.
The gingival attachment around the tooth isincised with a number 15 scalpel blade. A den-tal elevator with a curved blade that best fitsthe circumference of the tooth is selected. Theinstrument is inserted into the periodontal lig-ament space between the tooth and alveolarbone. Careful and steady rotation of its handlewill create pressure on the tooth and causesthe periodontal ligament to stretch and tear.3
(Note that performing a ‘wiggling’ motion hasthe potential to crush adjacent alveolar bone.)As the periodontal ligament space is widened,the dental elevator can be advanced apicallyand rotational pressure is repeated. The instru-ment should be inserted at other sites aroundthe tooth until it is mobile enough for retrievalwith an extraction forceps. The apex of theextracted tooth is inspected and palpated,ensuring no fracture has occurred. The extrac-tion site is debrided with a surgical curette,and sharp bony edges are smoothed. Thewound is rinsed and then sutured closed in asimple interrupted pattern.6,14
Sectioning of multi-rooted teeth providestwo or more single-rooted crown–root seg-ments that are extracted as if they were single-rooted teeth. Gentle reflection of the gingivawith a periosteal elevator will reveal the exactlocation of the furcation, decreasing the risk ofdamage to the gingiva during tooth section-ing. Sectioning is accomplished with a fissurebur, starting from the furcation and progress-ing through the crown.3 Two-rooted teeth areseparated into two single-rooted crown–rootsegments. The three-rooted maxillary fourthpremolar tooth is separated into three one-rooted crown–root segments. in addition tovertical advancement of a dental elevator intothe periodontal ligament space, the instru-ment can also be inserted horizontally inbetween the sectioned crown–root segmentsto lever them out of their alveoli.6,14
Figure 10 Size 5-0 synthetic, absorbable monofilamentmaterial with a swaged-on, taper-point round, non-cuttingneedle
Closed extraction is primarily performed formaxillary and mandibular incisors, maxillary secondpremolars, maxillary first molars, and mobile teeth
presenting with significant attachment loss.
Practicalconsiderations < If a tooth needsto be extracted inthe area of previousradiation therapy,the procedureshould beperformed soonafter the acute sideeffects have wornoff (eg, after 6–8weeks) rather thanwaiting months oryears, as thepotential for woundhealing will notimprove butbecomeprogressivelyworse. < Obtainingsigned orwitnessed verbalconsent from theclient about thenumber of teeth to be removed isimportant prior toperforming anytooth extraction.
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:34 Page 905
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from
906 JFMS CLINICAL PRACTICE
REV IEW / Oral anatomy and tooth extraction
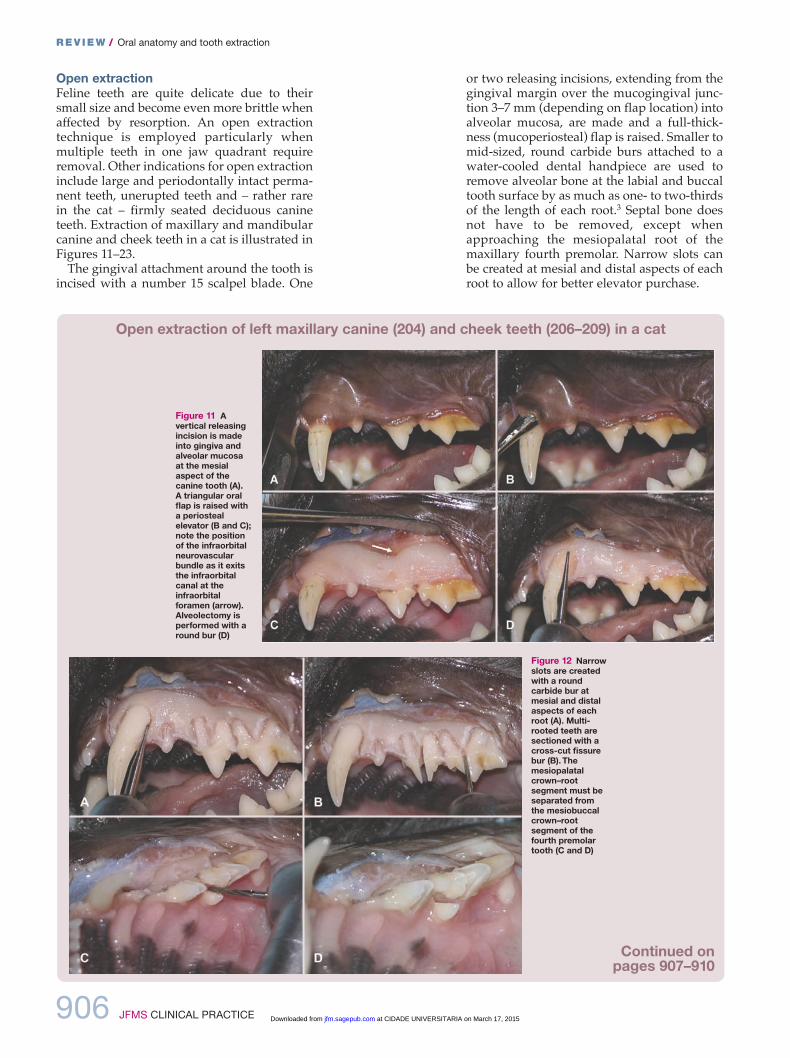
Figure 11 Avertical releasingincision is madeinto gingiva andalveolar mucosaat the mesialaspect of thecanine tooth (A). A triangular oralflap is raised witha periostealelevator (B and C);note the positionof the infraorbitalneurovascularbundle as it exitsthe infraorbitalcanal at theinfraorbitalforamen (arrow).Alveolectomy isperformed with around bur (D)
Figure 12 Narrowslots are createdwith a roundcarbide bur atmesial and distalaspects of eachroot (A). Multi-rooted teeth aresectioned with across-cut fissurebur (B). Themesiopalatalcrown–rootsegment must beseparated fromthe mesiobuccalcrown–rootsegment of thefourth premolartooth (C and D)
Open extractionFeline teeth are quite delicate due to theirsmall size and become even more brittle whenaffected by resorption. An open extractiontechnique is employed particularly whenmultiple teeth in one jaw quadrant requireremoval. other indications for open extractioninclude large and periodontally intact perma-nent teeth, unerupted teeth and – rather rarein the cat – firmly seated deciduous canineteeth. Extrac tion of maxillary and mandibularcanine and cheek teeth in a cat is illustrated inFigures 11–23.
The gingival attachment around the tooth isincised with a number 15 scalpel blade. one
or two releasing incisions, extending from the gingival margin over the mucogingival junc-tion 3–7 mm (depending on flap location) into alveolar mucosa, are made and a full-thick-ness (muco periosteal) flap is raised. Smaller tomid-sized, round carbide burs attached to awater-cooled dental handpiece are used toremove alveolar bone at the labial and buccaltooth surface by as much as one- to two-thirdsof the length of each root.3 Septal bone doesnot have to be removed, except whenapproaching the mesiopalatal root of the maxillary fourth premolar. Narrow slots canbe created at mesial and distal aspects of eachroot to allow for better elevator purchase.
Open extraction of left maxillary canine (204) and cheek teeth (206–209) in a cat
Continued on pages 907–910
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:34 Page 906
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from

JFMS CLINICAL PRACTICE 907
REV IEW / Oral anatomy and tooth extraction
Figure 14Fracture of themesial crown–rootsegment of thethird premolar hasoccurred (A).Additional alveolarbone around theroot remnant isremoved with around carbide bur(B). A special roottip elevator isused to elevateand retrieve theroot remnant (C and D)
Figure 13 Adental elevator is inserted into the periodontalligament spacebetween thecanine tooth andalveolar bone, androtated to stretchand tear theperiodontalligament (A andB). Once the toothis mobile enough,it is grasped as far apically aspossible with anextraction forcepsand removed (C and D)
Sectioning of multi-rooted teeth, extraction ofcrown–root segments, debridement and rinsingof the wound are performed as described forthe closed extraction technique. Slight deflec-tion of lingually/palatally located gingivaallows for safe smoothing of alveolar bone andavoids iatrogenic injury to soft tissues.3,6,14
irregular or necrotic flap margins aretrimmed with Metzenbaum scissors. The con-
nective tissue side of the flap is debrided witha surgical curette, ensuring removal of infect-ed and inflamed granulation tissue. Utilizingstay sutures or grasping a flap on its connec-tive tissue side with a thumb forceps will minimize iatrogenic trauma to the flap mar-gin. The periosteum at the base of the flap isincised in a distomesial direction, allowing theflap to become mobile.15 The back of a scalpelblade can be used to ‘strum’ and weaken theperiosteal layer, followed by blunt dissectionwith scissors. A small stab incision might alsobe made in the periosteum through which theblade tips of closed scissors are inserted andopened to undermine the periosteal layer. Thewound is rinsed and the flap sutured to thepalatal/lingual gingiva in a simple interrupt-ed pattern.3,16,17
Continued frompage 906
Open extraction is performed principally whenmultiple teeth in one jaw quadrant require removal,
as well as for large and periodontally intactpermanent teeth and unerupted teeth.
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:34 Page 907
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from
908 JFMS CLINICAL PRACTICE
REV IEW / Oral anatomy and tooth extraction
Continued frompages 906–907
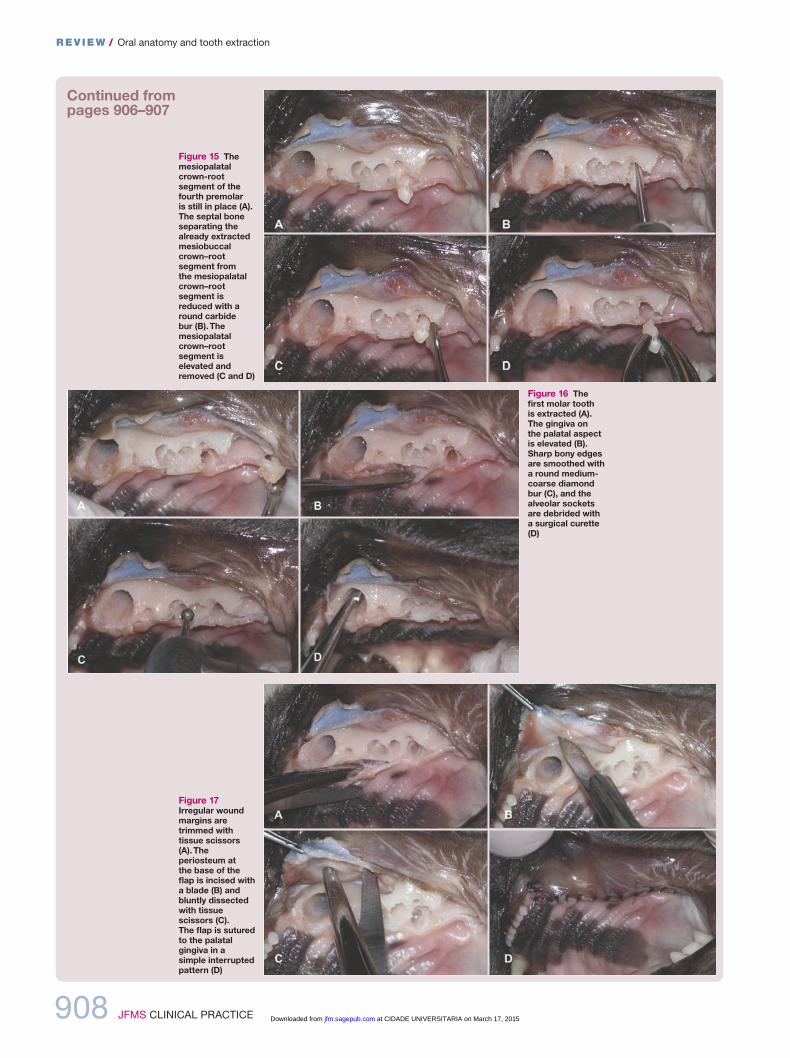
Figure 15 Themesiopalatalcrown-rootsegment of thefourth premolar is still in place (A).The septal boneseparating thealready extractedmesiobuccalcrown–rootsegment from the mesiopalatalcrown–rootsegment isreduced with around carbide bur (B). Themesiopalatalcrown–rootsegment iselevated andremoved (C and D)
Figure 16 Thefirst molar tooth is extracted (A).The gingiva on the palatal aspectis elevated (B).Sharp bony edgesare smoothed witha round medium-coarse diamondbur (C), and thealveolar socketsare debrided witha surgical curette(D)
Figure 17Irregular woundmargins aretrimmed withtissue scissors(A). Theperiosteum at the base of theflap is incised witha blade (B) andbluntly dissectedwith tissuescissors (C). The flap is suturedto the palatalgingiva in a simple interruptedpattern (D)
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:34 Page 908
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from
Continued frompages 906–908
JFMS CLINICAL PRACTICE 909
REV IEW / Oral anatomy and tooth extraction
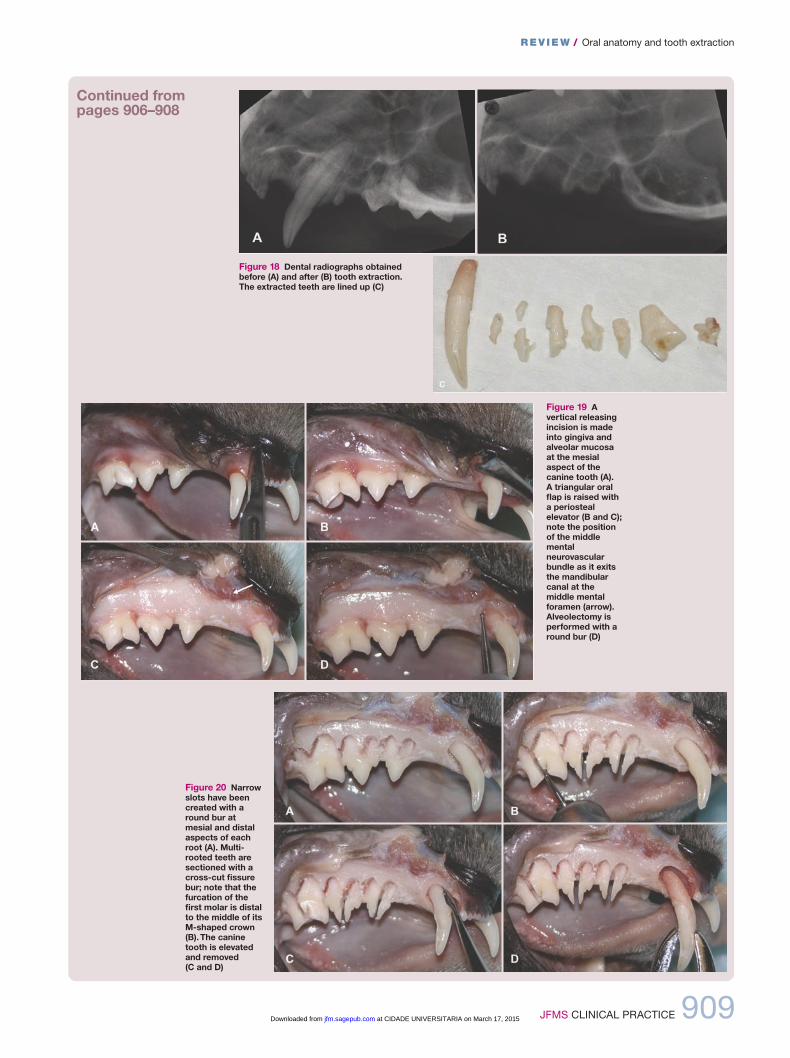
Figure 20 Narrowslots have beencreated with around bur atmesial and distalaspects of eachroot (A). Multi-rooted teeth aresectioned with across-cut fissurebur; note that thefurcation of thefirst molar is distalto the middle of itsM-shaped crown(B). The caninetooth is elevatedand removed (C and D)
Figure 19 Avertical releasingincision is madeinto gingiva andalveolar mucosaat the mesialaspect of thecanine tooth (A). A triangular oralflap is raised witha periostealelevator (B and C);note the positionof the middlementalneurovascularbundle as it exitsthe mandibularcanal at themiddle mentalforamen (arrow).Alveolectomy isperformed with around bur (D)
Figure 18 Dental radiographs obtainedbefore (A) and after (B) tooth extraction. The extracted teeth are lined up (C)
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:35 Page 909
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from
910 JFMS CLINICAL PRACTICE
REV IEW / Oral anatomy and tooth extraction
Continued frompages 906–909
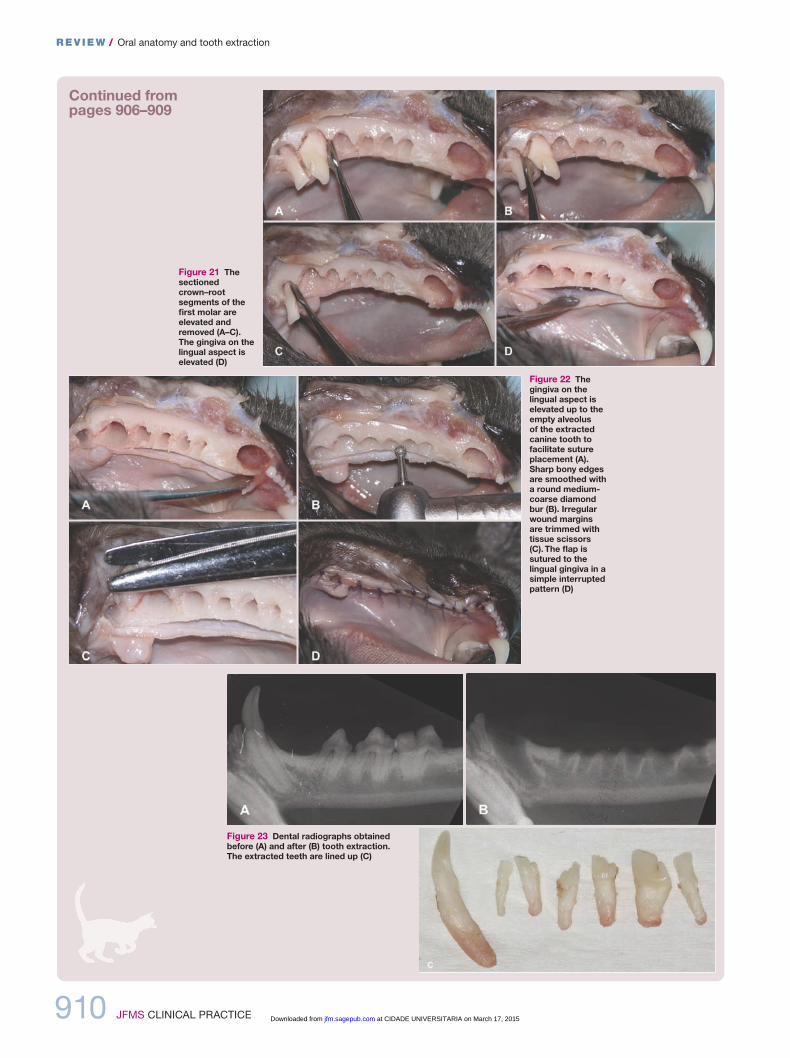
Figure 21 Thesectionedcrown–rootsegments of thefirst molar areelevated andremoved (A–C).The gingiva on thelingual aspect iselevated (D)
Figure 22 Thegingiva on thelingual aspect iselevated up to theempty alveolus of the extractedcanine tooth tofacilitate sutureplacement (A).Sharp bony edgesare smoothed witha round medium-coarse diamondbur (B). Irregularwound marginsare trimmed withtissue scissors(C). The flap issutured to thelingual gingiva in asimple interruptedpattern (D)
Figure 23 Dental radiographs obtainedbefore (A) and after (B) tooth extraction. The extracted teeth are lined up (C)
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:35 Page 910
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from
JFMS CLINICAL PRACTICE 911
REV IEW / Oral anatomy and tooth extraction
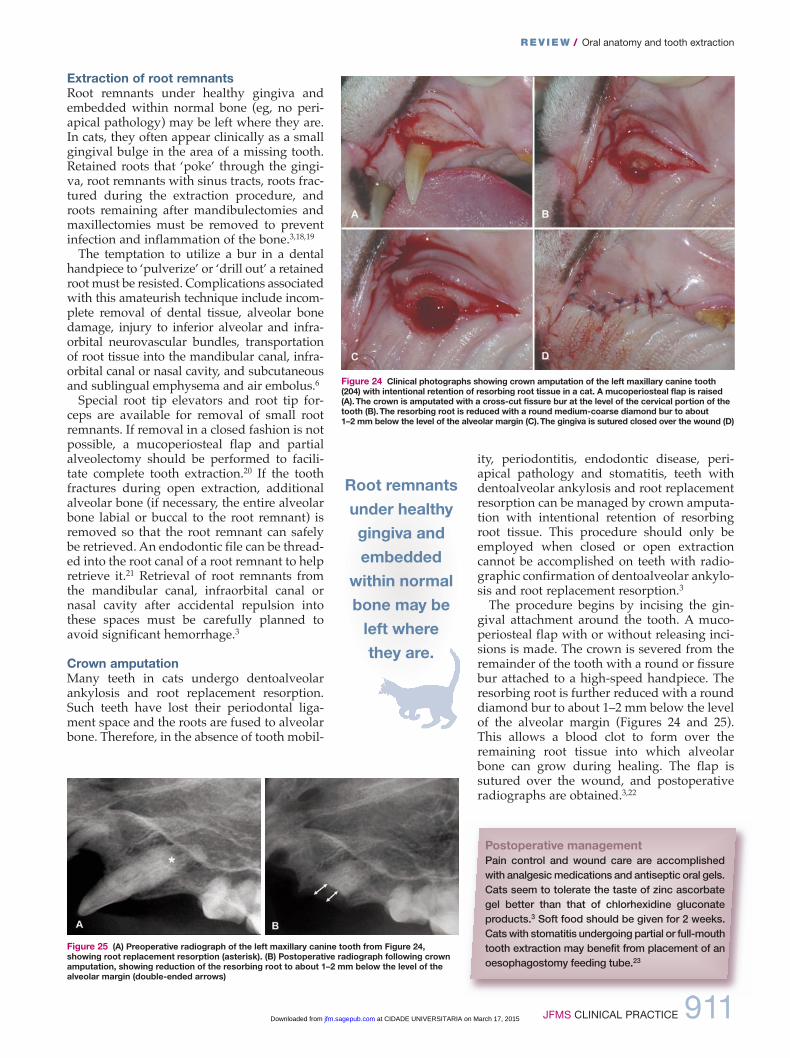
Extraction of root remnantsRoot remnants under healthy gingiva andembedded within normal bone (eg, no peri-apical pathology) may be left where they are.in cats, they often appear clinically as a smallgingival bulge in the area of a missing tooth.Retained roots that ‘poke’ through the gingi-va, root remnants with sinus tracts, roots frac-tured during the extraction procedure, androots remaining after mandibulectomies andmaxillectomies must be removed to preventinfection and inflammation of the bone.3,18,19
The temptation to utilize a bur in a dentalhandpiece to ‘pulverize’ or ‘drill out’ a retainedroot must be resisted. Complications associatedwith this amateurish technique include incom-plete removal of dental tissue, alveolar bonedamage, injury to inferior alveolar and infra -orbital neurovascular bundles, transportationof root tissue into the mandibular canal, infra-orbital canal or nasal cavity, and subcutaneousand sublingual emphysema and air embolus.6
Special root tip elevators and root tip for-ceps are available for removal of small rootremnants. if removal in a closed fashion is notpossible, a mucoperiosteal flap and partialalveolectomy should be performed to facili-tate complete tooth extraction.20 if the toothfractures during open extraction, additionalalveolar bone (if necessary, the entire alveolarbone labial or buccal to the root remnant) isremoved so that the root remnant can safelybe retrieved. An endodontic file can be thread-ed into the root canal of a root remnant to helpretrieve it.21 Retrieval of root remnants fromthe mandibular canal, infraorbital canal ornasal cavity after accidental repulsion intothese spaces must be carefully planned toavoid significant hemorrhage.3
Crown amputationMany teeth in cats undergo dentoalveolarankylosis and root replacement resorption.Such teeth have lost their periodontal liga-ment space and the roots are fused to alveolarbone. Therefore, in the absence of tooth mobil-
ity, periodontitis, endodontic disease, peri -apical pathology and stomatitis, teeth withdentoalveolar ankylosis and root replacementresorption can be managed by crown amputa-tion with intentional retention of resorbingroot tissue. This procedure should only beemployed when closed or open extractioncannot be accomplished on teeth with radio -graphic confirmation of dentoalveolar ankylo-sis and root replacement resorption.3
The procedure begins by incising the gin -gival attachment around the tooth. A muco -periosteal flap with or without releasing inci-sions is made. The crown is severed from theremainder of the tooth with a round or fissurebur attached to a high-speed handpiece. Theresorbing root is further reduced with a rounddiamond bur to about 1–2 mm below the levelof the alveolar margin (Figures 24 and 25).This allows a blood clot to form over theremaining root tissue into which alveolarbone can grow during healing. The flap issutured over the wound, and postoperativeradiographs are obtained.3,22
Figure 24 Clinical photographs showing crown amputation of the left maxillary canine tooth(204) with intentional retention of resorbing root tissue in a cat. A mucoperiosteal flap is raised(A). The crown is amputated with a cross-cut fissure bur at the level of the cervical portion of thetooth (B). The resorbing root is reduced with a round medium-coarse diamond bur to about 1–2 mm below the level of the alveolar margin (C). The gingiva is sutured closed over the wound (D)
Figure 25 (A) Preoperative radiograph of the left maxillary canine tooth from Figure 24,showing root replacement resorption (asterisk). (B) Postoperative radiograph following crownamputation, showing reduction of the resorbing root to about 1–2 mm below the level of thealveolar margin (double-ended arrows)
Postoperative managementPain control and wound care are accomplished with analgesic medications and antiseptic oral gels.Cats seem to tolerate the taste of zinc ascorbate gel better than that of chlorhexidine gluconateproducts.3 Soft food should be given for 2 weeks.Cats with stomatitis undergoing partial or full-mouthtooth extraction may benefit from placement of anoesophagostomy feeding tube.23
Root remnantsunder healthygingiva andembeddedwithin normalbone may beleft where they are.
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:35 Page 911
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from

912 JFMS CLINICAL PRACTICE
REV IEW / Oral anatomy and tooth extraction
Avoidance and management of complications
The entire tooth must be removed in order toavoid complications such as local or systemicinfection.18,19
< Retained root remnants if a root remnantcannot be retrieved, a note is made in thedental record and the client informed aboutthe complication. The surgical site should beevaluated periodically by means of clinicaland radio graphic follow-up examinations.11
< Hemorrhage Bleeding can usually becontrolled by means of digital pressure with a gauze swab. Severe bleeding is rare andlikely due to injury of vessels in themandibular or infraorbital canal or themucosa of the nasal cavity. Packing a smallamount of bone wax into an alveolus isusually sufficient to stop excessive bleeding.3
< Iatrogenic trauma Repeated brief‘wiggling’ motions during tooth extractionwill crush and soften adjacent alveolar bone,making elevation of a tooth more difficult.Excessive leverage against adjacent teethshould be avoided to prevent their elevationor fracture. developing permanent teethcould be injured when extracting adjacentdeciduous teeth.3 instrument slippage couldcause local or distant soft tissue trauma orinjury to the operator or assistant.24–26
< Sublingual edema iatrogenic trauma or excessive pharyngeal packing can result in sublingual edema. intravenousdexamethasone may be administered ifrespiratory compromise is present. < Sublingual sialocele injury to salivaryducts in sublingual tissues occasionallycauses a sublingual sialocele (ranula), whichis treated by marsupialization or resection ofthe sublingual and mandibular glands.3
< Mandibular fracture Mandibular fractureis usually due to insufficient preparationprior to extraction (eg, important pathologyremaining undetected because radiographswere not obtained) or the use of excessive
force. it is more likely in the presence ofsevere periodontitis or other pathology thathas weakened the jaw bone. When occurringnear the mandibular canine,27 the fractureoften is non-displaced, and creating twointraosseous sutures may be sufficient forhealing. < Oronasal fistula oronasal communicationin the area of a missing maxillary caninetooth is rare in the cat. An acute oronasalfistula may be encountered during extractionof maxillary teeth and is managed bysuturing a flap over the extraction site.3
< Bite trauma After extraction of amaxillary canine tooth, the tight upper lipmay position more palatally, allowing theispilateral mandibular canine tooth to biteinto it. Reducing the pointed tip of themandibular canine by 1 mm (be careful aboutpulp exposure!) is usually sufficient to solvethe problem; exposed dentin should betreated with a layer of unfilled resin (dentaladhesive) to reduce postoperative sensitivity.< Emphysema Emphysema sometimesoccurs after tooth sectioning or alveolectomywith air-driven high-speed equipment. Thisusually resolves spontaneously within days.Air must never be blown into alveolar socketsor onto bleeding surfaces, as it can cause airemboli.3,28
< Wound breakdown Wound dehiscence is primarily caused by tension on suturelines. The wound can be resutured or is left to granulate and epithelialize. A blood clotremaining in the alveolus, regardless ofwhether or not the extraction site is suturedclosed, will avoid local infection andinflammation such as alveolar osteitis (‘dry socket’). < Non-healing extraction site if anextraction site is not healing, a biopsy iswarranted to rule out neoplasia.
Note that temporary bacteremia during andafter tooth extraction procedures is not an indi-cation for the perioperative use of systemicantibiotics in an otherwise healthy patient.3
< The veterinarian should be familiar with the tissues that hold the teeth in the jaws.
< The client must consent to the number of teeth to be removed prior to the procedure being performed.
< Proper instrument handling is paramount in avoiding iatrogenic injury.
< Feline teeth are quite delicate and become brittle when affected by resorption.
< The entire tooth must be removed in order to avoid local or systemic infection.
< Tension is the most common reason for flap dehiscence.
< Roots remaining in the jaws must be recorded in the patient’s medical record.
KEY POINTS
Repeated‘wiggling’
motions duringtooth extractionwill crush andsoften adjacentalveolar bone,
makingelevation of a tooth
more difficult.
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:35 Page 912
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from
JFMS CLINICAL PRACTICE 913
REV IEW / Oral anatomy and tooth extraction
Funding
The authors received no specific grant from any
funding agency in the public, commercial or not-for-
profit sectors for the preparation of this article.
Conflict of interest
The authors do not have any potential conflicts of
interest to declare.
References
1 Gracis M. Orodental anatomy and physiology.
in: Tutt C, deeprose J and Crossley d (eds).
BSAVA manual of canine and feline dentistry.
3rd ed. Gloucester: BSAVA, 2007, pp 1–21.
2 orsini P and Hennet P. Anatomy of the mouth
and teeth of the cat. Vet Clin North Am Small
Anim Pract 1992; 22: 1265–1277.
3 Reiter AM. Dental and oral diseases. in: Little
SE (ed). The cat: clinical medicine and
management. St Louis, Mo: Saunders, 2012,
pp 329–370.
4 Verstraete FJ and Terpak CH. Anatomical
variations in the dentition of the domestic cat.
J Vet Dent 1997; 14: 137–140.
5 okuda A, inouc E and Asari M. The membra-
nous bulge lingual to the mandibular molar
tooth of a cat contains a small salivary gland.
J Vet Dent 1996; 13: 61–64.
6 Reiter AM. Dental surgical procedures. in: Tutt
C, deeprose J and Crossley d (eds). BSAVA
manual of canine and feline dentistry. 3rd ed.
Gloucester: BSAVA, 2007, pp 178–195.
7 Martin-Flores M, Scrivani PV, Loew E, et al.
Maximal and submaximal mouth opening
with mouth gags in cats: implications for max-
illary artery blood flow. Vet J 2014; 200: 60–64.
8 Stiles J, Weil AB, Packer RA, et al. Post-anes-
thetic cortical blindness in cats: twenty cases.
Vet J 2012; 193: 367–373.
9 Reiter AM. Oral surgical equipment for small
animals. Vet Clin North Am Small Anim Pract
2013; 43: 587–608.
10 Lipscomb V and Reiter AM. Surgical materials
and instrumentation. in: Brockman dJ and
Holt dE (eds). BSAVA manual of canine and
feline head, neck and thoracic surgery.
Gloucester: BSAVA, 2005, pp 16–24.
11 Smith MM. Exodontics. Vet Clin North Am Small
Anim Pract 1998; 28: 1297–1319.
12 da Silva AM, Souza WM, Souza NT, et al.
Filling of extraction sockets with autogenous
bone in cats. Acta Cir Bras 2012; 27: 82–87.
13 da Silva AM, Astolphi Rd, Perri SH, et al.
Filling of extraction sockets of feline maxil-
lary canine teeth with autogenous bone or
bioactive glass. Acta Cir Bras 2013; 28:
856–862.
14 deBowes LJ. Simple and surgical exodontia.
Vet Clin North Am Small Anim Pract 2005; 35:
963–984.
15 Smith MM. The periosteal releasing incision.
J Vet Dent 2008; 25: 65–68.
16 Blazejewski S, Lewis JR and Reiter AM.
Mucoperiosteal flap for extraction of multiple
teeth in the maxillary quadrant of the cat.
J Vet Dent 2006; 23: 200–205.
17 Smith MM. Extraction of teeth in the mandibu-
lar quadrant of the cat. J Vet Dent 2008; 25:
70–74.
18 Moore Ji and Niemiec B. Evaluation of extrac-
tion sites for evidence of retained tooth roots
and periapical pathology. J Am Anim Hosp
Assoc 2014; 50: 77–82.
19 Reiter AM, Brady CA and Harvey CE. Local
and systemic complications in a cat after
poorly performed dental extractions. J Vet Dent
2004; 21: 215–221.
20 Woodward TM. Extraction of fractured tooth
roots. J Vet Dent 2006; 23: 126–129.
21 Gengler B. Extraction of teeth in the dog and
cat. Vet Clin North Am Small Anim Pract 2013; 43:
573–585.
22 duPont GA. Crown amputation with inten-
tional root retention for dental resorptive
lesions in cats. J Vet Dent 2002; 19: 107–110.
23 Fink L, Jennings M and Reiter AM. Placement
of esophagostomy feeding tubes in cats and
dogs. J Vet Dent 2014; 31: 133–138.
24 Paiva SC, Froes TR, Lange RR, et al. Iatrogenic
nasolacrimal duct obstruction following tooth
extraction in a cat. J Vet Dent 2013; 30: 90–94.
25 Smith MM, Smith EM, La Croix N, et al. Orbital
penetration associated with tooth extraction.
J Vet Dent 2003; 20: 8–17.
26 Westermeyer Hd, Ward dA, Whittemore JC, et
al. Actinomyces endogenous endophthalmitis
in a cat following multiple dental extractions.
Vet Ophthalmol 2013; 16: 459–463.
27 Volker MK and Luskin iR. Surgical extraction
of the mandibular canine tooth in the cat. J Vet
Dent 2012; 29: 134–137.
28 Gunew M, Marshall R, Lui M, et al. Fatal
venous air embolism in a cat undergoing
dental extractions. J Small Anim Pract 2008; 49:
601–604.
Available online at jfms.com Reprints and permission: sagepub.co.uk/journalsPermissions.nav
For reuse of images only, contact the corresponding author
900_913_Applied anatomy.qxp_FAB 02/10/2014 11:35 Page 913
at CIDADE UNIVERSITARIA on March 17, 2015jfm.sagepub.comDownloaded from