aplastic anemia dr. bhavesh s. jarwani. aplastic anaemia empty marrow syndrome is a disorder...
TRANSCRIPT
APLASTIC ANEMIA
Dr. Bhavesh S. Jarwani
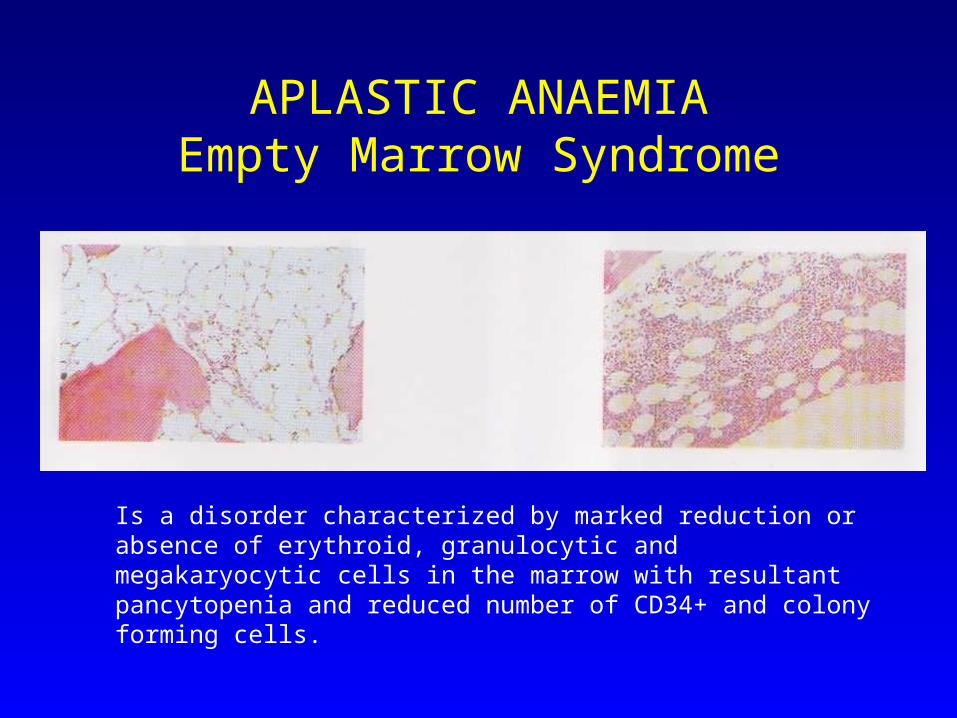
APLASTIC ANAEMIAEmpty Marrow Syndrome
Is a disorder characterized by marked reduction or absence of erythroid, granulocytic and megakaryocytic cells in the marrow with resultant pancytopenia and reduced number of CD34+ and colony forming cells.
Hematopoitic cell destruction by Immune Mechanisms in Acquired Aplastic Anemia.
There is normal stromal cells but decreased number of colony forming cells and stem cells asit can be seen in Ps, radiographically, and also the stem cells number
Immune Mechanics in Aplastic Anemia
• T cells: mononuclear cells from the ps or marrow suppressed the csf by the progenitor cells have elevated numbers of the cytotoxic T Lymphocytes
• Cytokines: peripheral blood from this patients had raised levels of the soluble cytokines as y-INF and TNF and also y-INF mRNA , evidence of the gene expression
• Incidence:5-10 cases per million persons per year
• Age: Bimodal distribution– young adults (15-30 years)– elderly (above 60 years)
• Same incidence in Male and Female• Geographic distribution
– more common in Asia than in North America and Europe
Etiology
• Acquired:– Drugs: Antimetabolites, antimitotic agents, gold, chloramphenicol,
phenylbutazone and sulfonamides– Radiation– Chemicals: benzenes, Solvents, insecticides– Viruses : Hepatitis A,B,C, E, G, and Parvo B19, CMV– PNH– Misc: pregnancy, connective tissue disorders, Graft-vs-Host disease
• Hereditary:– Fanconi’s Anemia– Dyskeratosis congenita– Shwachman Syndrome
• Idiopathic:– 50-65 % of cases
Etiology
• Drugs may be having direct dose dependent toxicity to the marrow or having Idiosyncrasy to the drugs:– Antineoplastic and antimetabolites are having direct dose dependent toxicity
– Chloramphenicol having first immediate dose dependent toxicity and long term Idiosyncrasy after one to two weeks later
• Radiation:– Chronic exposure to low-dose and localized exposure leading to development
of aplastic anemia
• Benzene and insecticides: – direct and also induction of the hapten leading to immune mediated bone
marrow suppression• Virus:
– Hepatitis A,B,C,E and G. Parvovirus B19, CMV
• Pregnancy:
Etiology
• PNH:– defect in PIG-A gene, so partial or complete inability to
construct Glycosylphosphatidylinositol(GPI) anchor for the attachment of CD55, CD59
– diagnosis: Ham’s test, Flow cytometry using antibodies against cell surface antigens CD55, CD59 which are lacking in disease
• Congenital disorders:– Fanconis Anemia– Shwachaman syndrome– Dyskeratosis congenita
Pathogenesis:
• Having stem cell defect: how?• Having immune mechanism in this disease progress• Evidence:• immunosupresion better results in BMT, • Better treatment with Antithymocyte globulin and also
immuno-suppression having comparable results to BMT
• Activated T cells: overproduction of the cytokines as interferon y and TNFb that in turn leading to hematopoietic progenitors
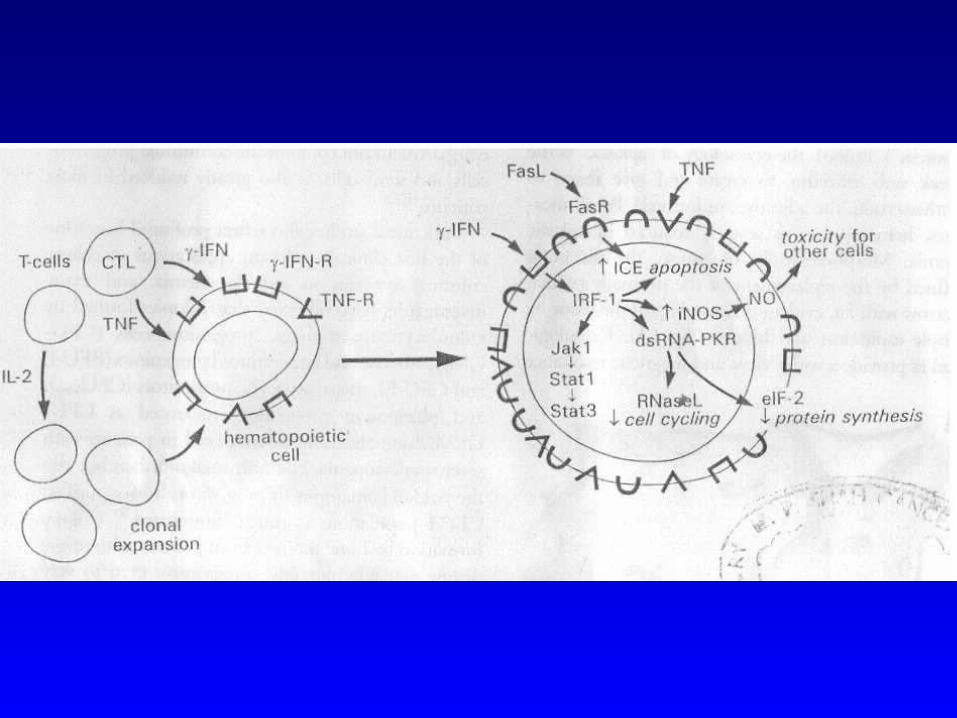
How the destruction occurs:
• induction of the killing through programmed cell death.
• Progenitor cells have Fas receptor , triggering that though the cytokines induces the apoptosis.
• Also induces the production of the nitric oxide by marrow cells that in turn leads to the cell destruction
• transcription regulator is required, I.e. IRF, interferon regulatory factor-1, and this is required for the negative action of the INF-y.
ANTIGENS ENCITING APLASTIC ANEMIA:
• Either endogenous or exogenous:– exogenous: hepatitis, drugs
– endogenous: somatic mutation in the HSC leading to autoimmunity and at last the marrow failure immune response to peptides derived from the aberrantly processed proteins like GPI
• Determinants of the autoimmunity:– HLA class I and II are associated with many human autoimmune
diseases, HLA-DR2 is over expressed in American and Europe.
– specific class 2 haplotypes in Japanese that are respondent to the CSA
• Drugs:– genetically defined metabolic detoxification pathway in aplastic
anemia
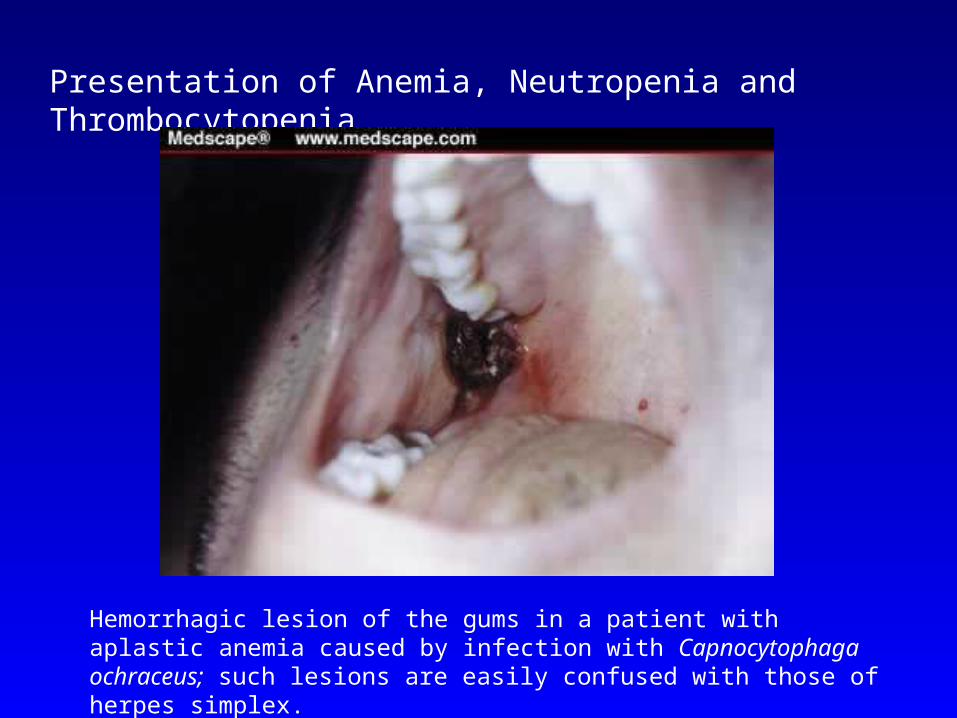
Presentation of Anemia, Neutropenia and Thrombocytopenia
Hemorrhagic lesion of the gums in a patient with aplastic anemia caused by infection with Capnocytophaga ochraceus; such lesions are easily confused with those of herpes simplex.
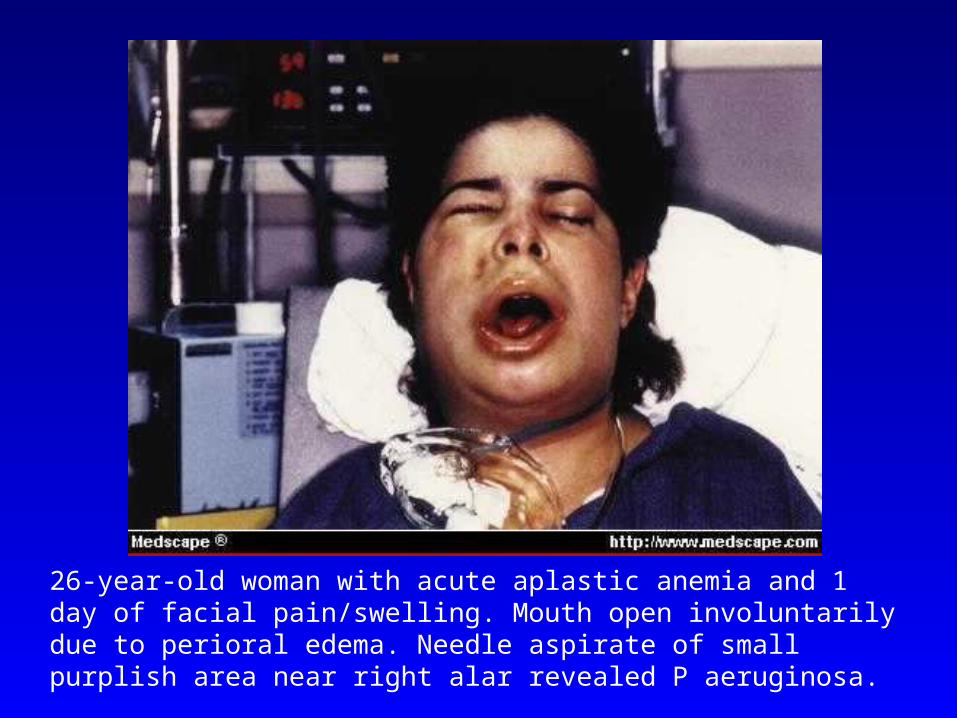
26-year-old woman with acute aplastic anemia and 1 day of facial pain/swelling. Mouth open involuntarily due to perioral edema. Needle aspirate of small purplish area near right alar revealed P aeruginosa.
Diagnosis and differential Diagnosis
• Peripheral Smearnormocytic, and normochronic with low reticulocyte count index <2% .i.e. hypoproliferative marrow
• Bone Marrowmarrow spicules with empty fat cells and very few hematopoietic cells. Presence of dysplasia suggest MDs, so as karyotype anomaly suggest MDS.
• Other tests:LDH, haptoglobulin, hams test, flow cytometry to know about
PNH and also for fancony’s anemiahairy cell Leukemia: cytochemical I.e. tartrate-resistent acid phosphatase, and phenotypic, I.e. CD25+ monoclonal B cells
• Classification:Severe: when nautrophic <500, platelets <20,000/microL, and reticulocyte <20,000/microL
• Supersevere: when neutrophic count<200/microL
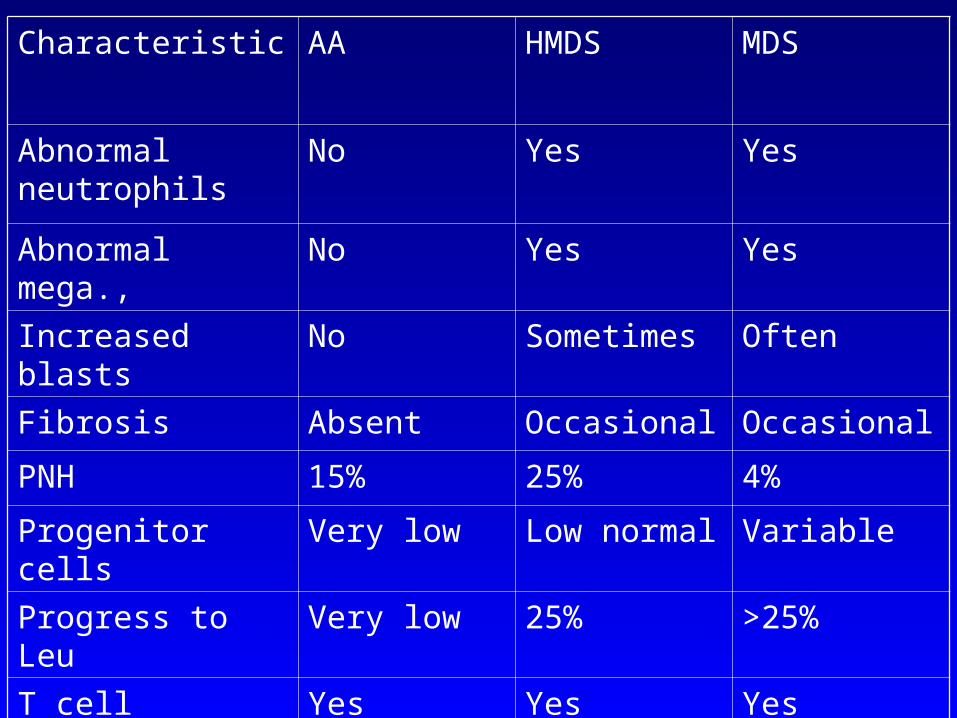
Characteristic AA HMDS MDS
Abnormal neutrophils
No Yes Yes
Abnormal mega., No Yes Yes
Increased blasts No Sometimes Often
Fibrosis Absent Occasional Occasional
PNH 15% 25% 4%
Progenitor cells Very low Low normal Variable
Progress to Leu Very low 25% >25%
T cell activation Yes Yes Yes
Increased TNF, INKy
Yes Yes yes
• Course and prognosis of the disease:– with transfusion support alone: 80 % of cases succumb to death in 18 to 24
months, related to PMN count– with MBT and Immunosuppresion: curative in 60 to 90 % of cases, risk of
CGVH threat
• Supportive care:– transfusion of the blood products, CMV seronegative should be given
transfusion from the family members should be avoided to prevent sensitization.
– pooled donor platelets but leads to sensitization– in refractory cases need HLA matched transfusion– packed cells filtrated to remove leukocyte and platelets– iron overload : give chelating therapy deferoxamine– CMV prophylaxis– Staph. Aeureus * hospitalization * menses
• Treatment modalities:– ATG: purified monomeric IgG from hyperimuune horse with human
thymocyte and thoracis duct lymphocytes– 50 - 70 % good response– 20-30 complete and durable recovery– 70-80 have partial response
• Complication: – MDS 30-6- %– also secondary solid tumors– response after 8 to 12 weeks
• Other drugs to suppress immunity:– cyclosporine and cyclophosphamide and also high dose steroid
• Growth factors:– Erythropoeitin, CG-CSF, GM-CSF, ILs 1,3, 6
• Response is slow• Response is often incomplete• Response may require successive course of
immunosuppression• Relapse is common and require maintenance therapy
• Evolution to clonal disease is common:• Overall 15% of the cases develop clonal disease like
MDS or PNH• Much higher after immunossuppression that BMT
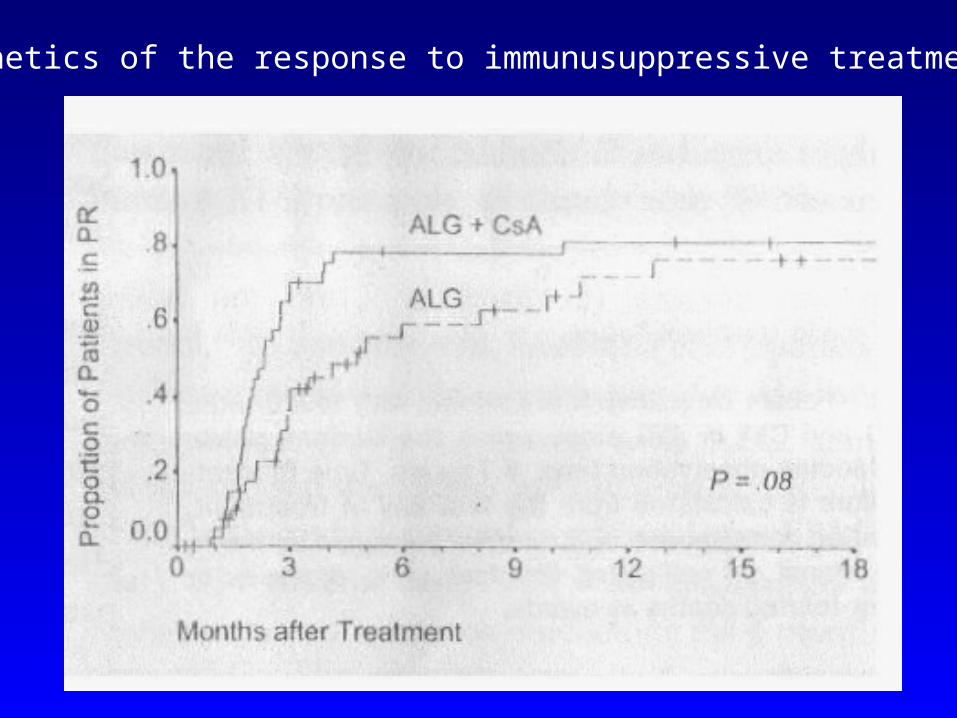
Kinetics of the response to immunusuppressive treatment:
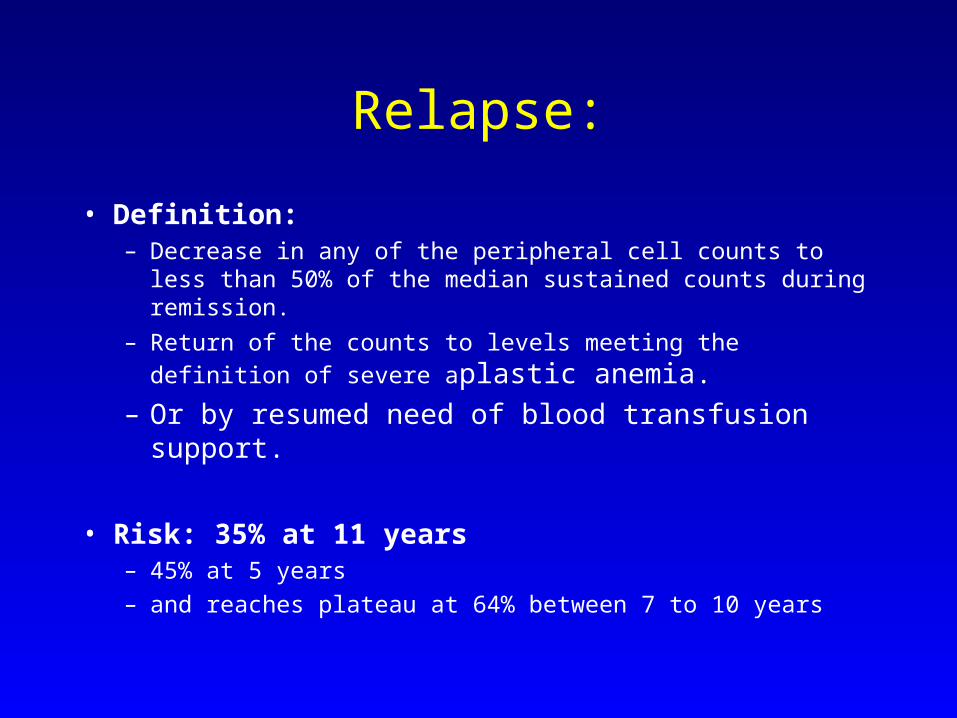
Relapse:
• Definition:– Decrease in any of the peripheral cell counts to less than
50% of the median sustained counts during remission.
– Return of the counts to levels meeting the definition of
severe aplastic anemia.– Or by resumed need of blood transfusion support.
• Risk: 35% at 11 years – 45% at 5 years– and reaches plateau at 64% between 7 to 10 years
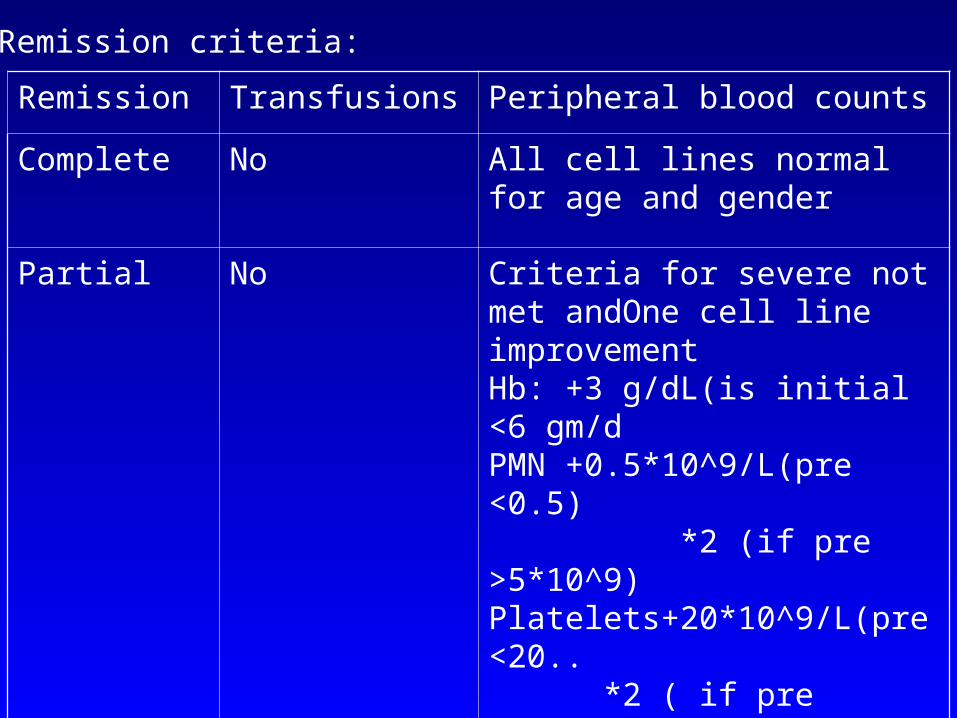
Remission criteria:
Remission Transfusions Peripheral blood counts
Complete No All cell lines normal for age and gender
Partial No Criteria for severe not met andOne cell line improvementHb: +3 g/dL(is initial <6 gm/dPMN +0.5*10^9/L(pre <0.5) *2 (if pre >5*10^9)Platelets+20*10^9/L(pre <20.. *2 ( if pre >20….)
No remission Yes Earlier criteria not met with
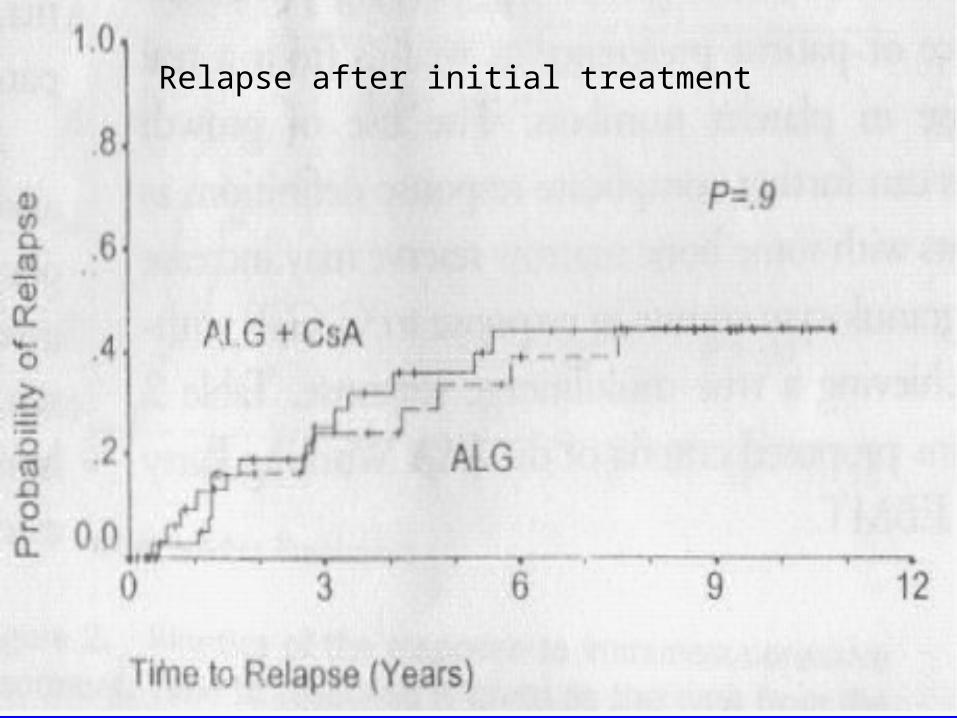
Relapse after initial treatment
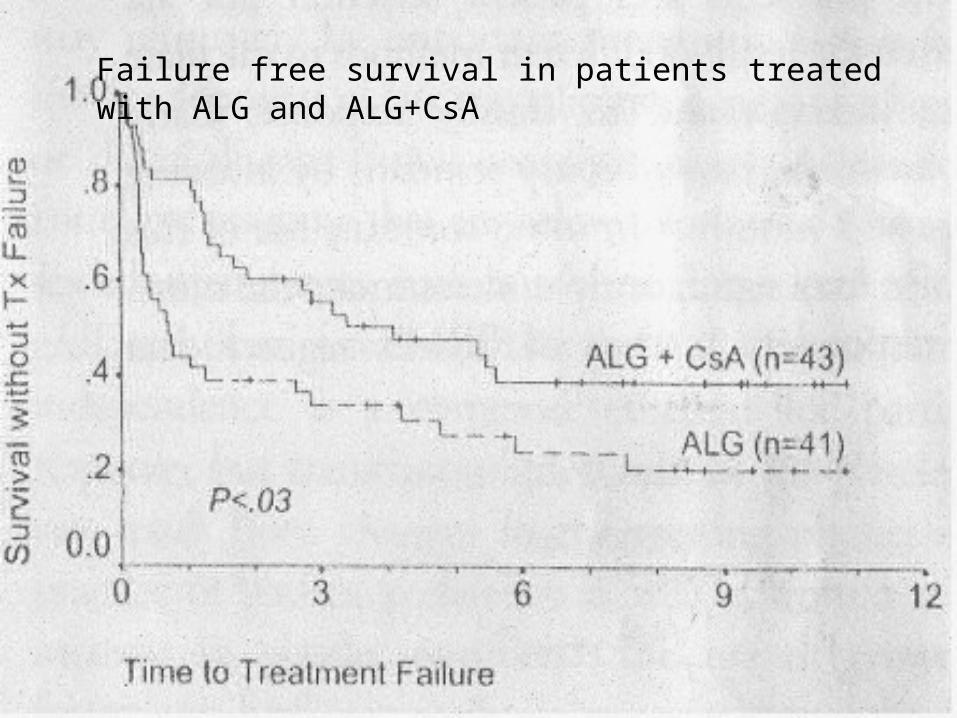
Failure free survival in patients treated with ALG and ALG+CsA
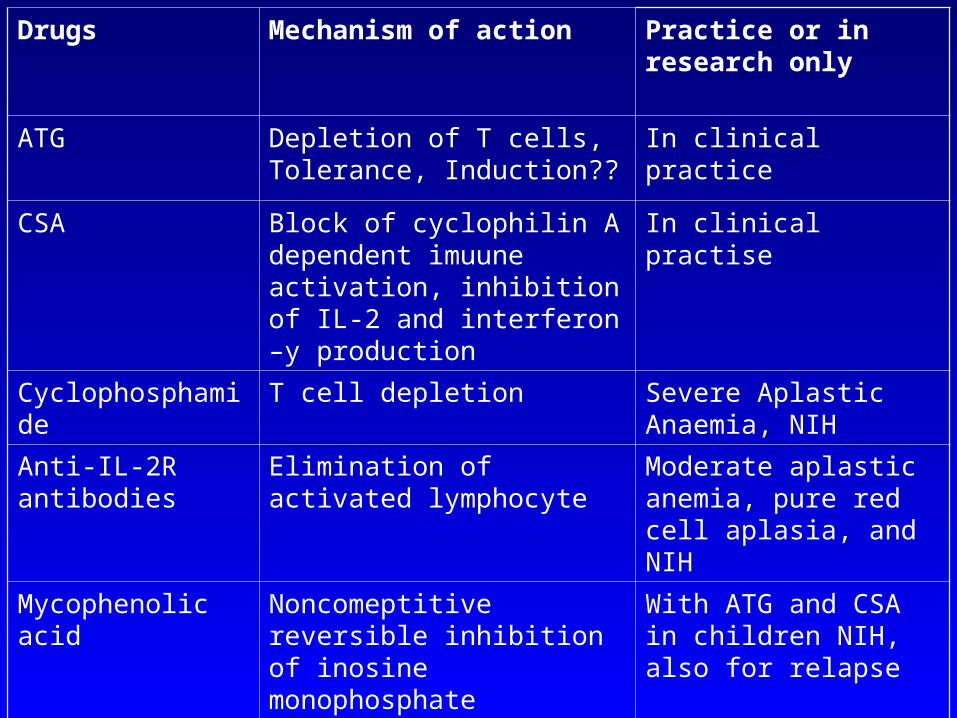
Drugs Mechanism of action Practice or in research only
ATG Depletion of T cells, Tolerance, Induction??
In clinical practice
CSA Block of cyclophilin A dependent imuune activation, inhibition of IL-2 and interferon –y production
In clinical practise
Cyclophosphamide T cell depletion Severe Aplastic Anaemia, NIH
Anti-IL-2R antibodies
Elimination of activated lymphocyte
Moderate aplastic anemia, pure red cell aplasia, and NIH
Mycophenolic acid Noncomeptitive reversible inhibition of inosine monophosphate dehydrogenase, inhibition of T cell proliferation
With ATG and CSA in children NIH, also for relapse
Sirolimus Inactivate of Protein kinase p70, block in IL2 dependent proliferation of T cells
Only for solid organ transplantation
Current and Future treatment strategies
• Evaluation of the best timing of immunosuppression• Multidrug immunosuppression vs sequencial
immunosuppression• Early retreatment with immunosuppression• Improvement of current protocol
– dose of G-CSF– newer growth factors like stem cell factor
• New immunosuppresive protocol– high dose cyclophosphamides– new immunosuppressive treatment