apla positive pregnancy with peripartum complications
TRANSCRIPT
APLA Positive Pregnancy with Peripartum Complications
Presentor : Dr. Prashanthi Vemulapalli
Designation : Fellow OBSMED
Hospital : Fernandez Hospital, Hyderabad
Date of Presentation : 17.08.2016
Mrs. J.
Age:26 yrs
Resident of Hyderabad
Graduate, home maker. Earlier worked for
multinational Bank
Primi, booked at 8wks gestation
OBH:ML:1yr,NCM
MH: Irregular cycles
Past History
On and off episodes of unilateral Raynauds
phenomenon involving left hand on exposure to cold
weather
Started when she went to USA in 2013, (cold
temperatures), episodic lasting days during the
3months stay.
Excruciating pain in left index and thumb, followed by
bluish discolouration
MRI hand to r/o glomus tumour was normal
Past History
2014 admitted in NIMS when episode recurred due
to AC in office.
No arthralgias/mucosal ulcers/alopecia/sicca
symptoms/skin tightening
No photosensitivity/malar rash
No Red eye/claudication
No trauma/smoking/DM/HN
Evaluation- ?Secondary Raynauds or local causes
Ds DNA:Negative
ACL IgM :positive
LAC:positive
ANA:Speckled
VIT B12/FOLIC ACID :WNL
Arterial and venous DOPPLER HAND:NORMAL
Started on heparin/amlodepin
Maintained on warfarin
symptom free since then; she was off work
Symptoms recurred 1 year later when she rejoined work: exposed to AC
Stepped up warfarinwas Ok
Family H/O: No history of arthritis
Father died of bone malignancy
Personal H/o: gave up her job as symptoms got
aggravated by AC at workplace
Present Pregnancy
Married, conceived spontaneously
Booked in early pregnancy : 8wks
MULTIDISCIPLINARY CARE
Started on enoxaparin 60mg / Ecospirin 150mg
Follow ups regular
Occasional tingling of fingers; advised nifidepine 10mg
bd at 25 wks for an episode of Raynauds which lasted
10days but took irregularly
At 23 weeks had genital herpes treated with acyclovir
SCANS:WNL
Admitted at 32 weeks with swelling and tingling lower limbs
Admission BP 170/120 mm Hg
Urine albumin:4 +/LDH:331/PLT 49K; transaminases normal
Inj MGSO4/steroid 1st dose was given/
In v/o severe Preeclampsia, partial HELLP, she was taken for
LSCS
Received 6 units RDP intraoperatively: plt 49k
1.6KG boy baby.
Intraperitoneal drain :20cc
26 yrs pirmi At 32 wks
APLA: On Heparin/Ecospirin
Secondary Raynauds phenomenon
Sudden onset severe PE(BP>160/110,Urine
albumin:4+,LDH >,plt:49k)
LSCS
Received MGSO4
POD2
(POD 0 AND 1:Uneventful)
POD 2:Developed SOB/blurring of vision/
PR:120 /min;BP:150/100;SPO2:77%
RS: Normal
ABG: resp alkalosis
2D Echo: Mild pericardial effusion/no RV strain
ECG: Tachycardia
CXR: Pulmonary edema
Plt:21k.other parameters stable
Received lasix/morphine/ IV labetolol

Pulmonary Embolism
PPCM
Pulmonary edema
Blurring of vision: Retinal detachment/occipital
infarct/
Shifted to century hospital for multidisciplinary care
At Century Hospital
Urinary
metanephrines:wnl
Heparin Ab:negative
CXR:pulmonary edema
Usg abdomen:normlal
Renal Doppler:normal
2D ECHO:normal
MRI:PRES
MRV:normal
Fundoscopy:exudative
RD,Macular
edema,conjunctival edema
LFT: rising LDH:824
Procalcitonin:normal
NASAL SWAB:NO MRSA
RECTAL SWAB:NO VRE

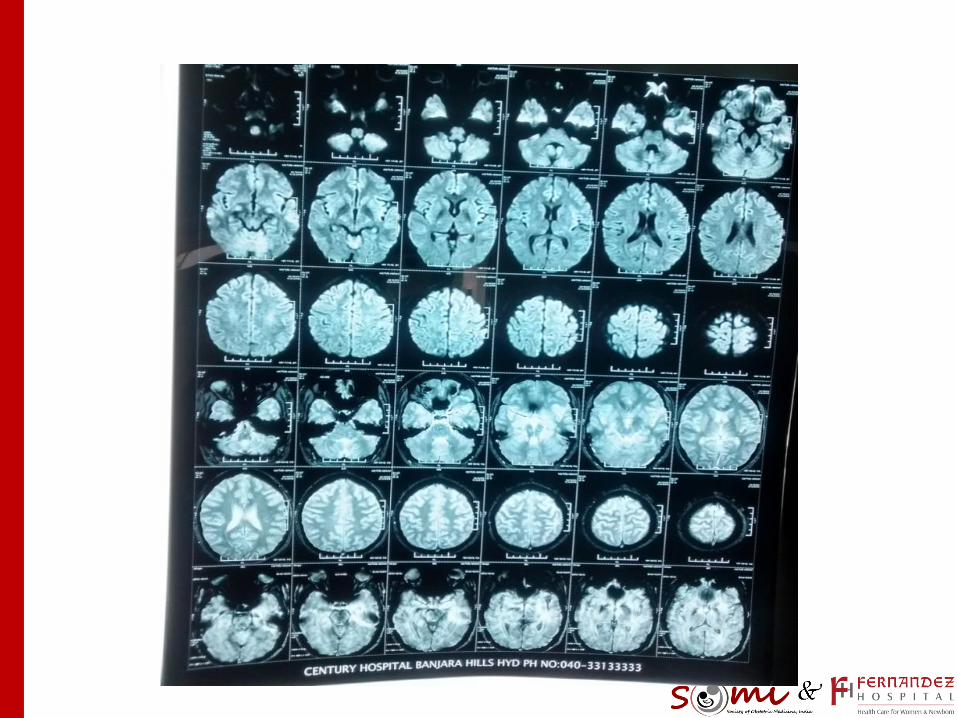
Pulmonary Edema:Hypertensive Crisis
Symptoms improved over 24 hrs
Treated symptomatically
Anti hypertensives:prazosin/amlodepin/ labetolol
Heparin withheld in v/o thrombocytopenia
Diuretics
Topical/systemic steroids for macular edema
Investigations
Platelet:20,000-1 lakh
Hemoglobin:6.0-10gm
Creatinine:1-3
Coagulation profile: WNL
DISCHARGED A WEEK LATER
Nifedepin 5mg od
wysolone 15mg
Topical steroids
Supplements
Opthalmology FU
Treatment

Steroids were being tapered at 5mg/week
Complained of severe pain, photophobia and
redness in both eyes since discharge from century
Referred to LVPEI- diagnosed as anterior uveitis-
local steroids given- improved over 5d-7 days
Retinal angio done at LVPEI. H/o fever one day prior
to the procedure
26th POD
Readmitted on…26th POD with high grade fever of
5days duration with dysuria/cough
Mild anemia 8-9gm/dl Platelet Trend:min-
max10K-1LAKH
Creatinine high 1.9mg/dl
Urine c/s:E coli 10^5 treated with Inj cefaperazone
sulbactum. ( UTI with AKI?)
26th POD
Clexane for 2days later stopped
Labetalol 100mg tid/ nifedepine sr 10mg tid
Fever subsided but mild cough persisted
Creatinine Showed rising trend/ worsening
thrombocytopenia, anemia
Transferred to NIMS for further care
Problems
APLA with secondary Raynauds
POSTPARTUM preeclampsia with ? Partial HELLP
Postpartum pulmonary oedema
PRES
ANTERIOR UVEITIS
Mild anemia, worsening thrombocytopenia
AKI
UTI
At NIMS
Fever, tacycardia, tachypnoea,
sPO2 91%,
BP 140/90
? CAPS triggered by infection
? Sepsis ARDS
TTP/HUS/PTE
At NIMS ANTI GBM Ab:negative:
Anti ccp:negative
IgM RF:negative
ANA by IF:negative
Anti dsDNA:negaive
ACL IgG/IgM:POSITIVE
LFT:WNL
Schistocytes:negative
Procalcitonin:2.6
Usg abdomen:hepatosplenomegalyb/l HUN/ increased cortical
echogenecity in kidneys
CT chest- fibrosing alveolitis with superimposed
infection
BAL cultures sterile
Blood and urine culture: sterile
Nephrologist consult taken
methyl prednisolone for 3 days, therapeutic
anticoagulation, other supportive measures
Creatinine reduced from 3mg to 1.1mg
Renal biopsy planned after correction of
thrombocytopenia ….. ? CAPS vs lupus
Wysolone 60mg od
HCQ 200mg od
Amlodepine 10 mg bd
Metoprolol xl 25mg bd
Prazosin 10mg bd
Warfarin 2mg od
Stabilised over 1week and discharged
Postpartum 5weeks
Readmitted ( 3days after discharge from NIMS)with
hemoptysis ( blood tinged sputum) and cough;
No bleeding from other sites
RS: Basal crepts
Sputum culture: sterile
Plt < 50k
HRCT:PAH/Diffuse alveolar haemorrhage
Bronchoscopy: Normal
– Received 2units SDP, 2 units PRBCs (Hb 6gm/dl)
– Underwent plasmapheresis:6 times
– Inj cyclophosphamide/mesna (1dose)
No clinical or lab improvement(one week……
IV IG over 4days
Multiple platelet transfusion
Inj Rituximab 1 dose given
leukopenia TLC 2000
Was on triple cover ( meropenem+ metrogyl and
antifungal)
Summary
26 yr primary APLA(3YRS)on anticoagulants
Pregnancy :on enoxaparin/Ecospirin
32 wks severe PE/HELLP:LSCS
POD 3:Hypertensive crisis(pul edema)/PRES
Retinal Detachment, uveitis
POD 26: UTI:E Coli
AKI: Creatinine-3; resolved with conservative treatment
Severe thrombocytopenia
Resistant to
wysolone/methylprednisolone/plasmapheresis/IVIG/rituximab
Persistent leukopenia 500 after plasmapheresis
Diffuse alveolar hemorrhage- persistent mild hemoptysis on and
off till 5days ago
Rituximab 2nd dose due next week (15days apart)
Platelets had improved to 1.5lakhs/ again falling trend now at
80k
Bonemarrow biopsy - Myeloid maturation arrest
D/D
CAPS: Trigger infection
???
APLA
Multisystem autoimmune condition
Minority develop life threatening multiple organ
thrombosis
Criteria For APLA
Clinical:
- Vascular thrombosis:venous/arterial/small vessel
thrombosis.
- Pregnancy events:fetal death >10wks/one or >PTB
due to severe PE/eclampsia/placental insufficiency
- 3 or> losses <10 wks(unexplained)
Lab Criteria
Presence of APL on two occasions 12 wks apart
Not >5yrs before clinical manifestation
One or > of following
aCL Ig G/M :Positive
B2 glycoprotein G/M
LA :Positive

Correlation….
LA is better predictor for thrombotic events
LA should be done off coagulation
ACL IgG relate to clinical events
Recently even isolated IgA, B2GP also relate
clinical events

Spectrum Of APLA
APL Positive: Only serology
APL positivity with noncriteria manifestations:
– Thrombocytopenia,hemolytic anaemia,cardiac
valve disease, nephropathy
A PL based on thrombosis/ pregnancy losses
CAPS
Diagnostic Challenges
Positive APS: Infections
APS negative: During thrombosis
Overlap:
- Sepsis: Thrombocytopenia
- HIT: Heparin Ab/heparin induced platelet activation
studies

1.CAPS(ASHERSON)
1% of APS
1. Thrombosis in 3 or more organs(in less than a week)
2. Microthrombosis in atleast one organ
3. APL positivity
4. Biopsy
ALL 4:CAPS
Three out of 4:probable CAPS
CAPS- Unique features
Rapid onset thrombosis resulting in MODS
Common association with other
microangiopathies:TMA’s
Evidence of SIRS
High risk of unusual organ involvement
High mortality despite treatment
CAPS Spectrum
CAPS
Probable CAPS
Microangiopathic APS
Thrombotic Storm
CAPS
50% Mortality:( 20%with newer treatments)
Triggering factor(25%):Infection
/viral/URTI/UTI/sepsis/surgery/anticoagulation
withdrawl/neoplasia/immunization
Infection contributes to 40% of CAPS cases; hence
antibiotics indicated
SIRS
APS vs CAPS
Macrothrombus
Large vessels
Thrombosis is sporadic
Confined to single site
%84 microthrombi
Small vessels
Thrombotic events occur simultaneously in many organs
Diffuse ischaemia in parenchyma

CAPS Vs SIRS
MOLECULAR MIMICRY
INFLAMMATION

CAPS VS TMA
ADAMTS 13
2. CAPS like
APS Positive
Criteria not fulfilled
Close monitoring
Medium-large vessel involvement
Pulmonary/adrenal bleed
Thrombocytopenia
HELLP
Single organ thrombosis
3.Microangiopathic APS
Small blood vessel occlusion
TMA+HEMOLYSIS:TMHA
TMA CAN OVERLAP WITH:
– MALIGNANT HTN
– TTP
– HUS
– HIT
4. Thrombotic Storm
Clinical phenotype
Severe thrombotic events
Macrovascular events
Our patient
Preeclampsia and related complications
Hematological
Eye
Renal
Lung
Overlap:
sepsis,
HELLP

Diagnosis
CAPS
CAPS LIKE
CAPS :HELLP/HUS/TMA/SEPSIS
Conclusion
APS is a systemic autoimmune disease
Thrombotic/nonthrombotic
CAPS: Severe form of APS
Urgent treatment
Most of overlap diagnosis: Same treatment
Mortality: High
Clinical suspicion and active treatment reduces
mortality
References
CAPS Registry
Journal of Rheumatology
Case Reports