antiretroviral therapy the new patient with what &...
TRANSCRIPT

ANTIRETROVIRAL THERAPY
The New Patient With What & When?
17TH EUROPEAN MEETING ON HIV & HEPATITIS
22-24 MAY 2019, ROME, ITALY
PETER REISS, MD, PhDDirector HIV Monitoring foundation
Professor of MedicineAmsterdam UMC, University of Amsterdam
iStock.com/royalty-free image

Disclosures
• Grants support to my institution from EU FP7, ZonMW, AIDSfonds, Gilead Sciences, ViiVHealthcare, Janssen, and Merck
• Consultancy fees to my institution from GileadSciences, ViiV Healthcare, Janssen, Merck, andTeva pharmaceuticals

Outline
• What To Start?:
• Guidelines & Practice
• 2 Drugs for Initial Treatment
• Weight Gain on INSTI-based ART
• Long-acting ART: some perspectives
• When To Start?:
• What Happens in Daily Practice
• Same Day ART

WITH WHAT?
ANTIRETROVIRAL DRUG APPROVAL IN EUROPE1987-2019
Rosan van Zoest, Academic thesis, University of Amsterdam 2019 ( with permission)

Recommended, preferred regimens + Alternative/recommended incertain clin.situations
GUIDELINES
EACS (2018)1
DHHS (2018)2
IAS USA
(2018)3
BHIVA (2016)4
WHO (2018)5
TAF/FTC
TDF/FTC
ABC/3TC*
TAF/FTC
TDF/FTC
ABC/3TC*
TAF/FTC
ABC/3TC*
TAF/FTC
TDF/FTC
TDF/XTC
NRTI BACKBONE NNRTI INSTI PI
RPV*
−
−
RPV*
EFV
BIC
DTG
RAL
BIC
DTG
RAL
BIC
DTG
DTG
RAL
EVG/c
DTG
RAL (neonates)
DRV/c
or /r
−
−
DRV/r
ATV/r
−
NRTI-
REDUCING
DRV/c or /r + RAL
DTG + 3TC
DRV/c or /r + RAL
DTG + 3TC
DRV/c or /r + 3TC
DRV/c or /r + RAL
DTG + 3TC
DRV/c or /r + 3TC
DRV/c or /r + RAL
−
−
−
TDF/XTC
ABC/3TC*
AZT/XTC
EFV
DOR
EFV
RPV*
DOR
EFV
RPV
EFV
EFV 400
NVP
EVG/c
EVG/c
RAL
EVG/c
−
RAL(infants&
children if
DTG not
available)
ATV/c
or /r
DRV/c
or /r
ATV/c
or /r
DRV /c
or /r
−
−
First-line ART
*Use recommended only if baseline viral load <100,000 copies/mL.
3TC, lamivudine; ABC, abacavir; ATV, atazanavir; AZT, zidovudine; BIC, bictegravir; BHIVA, British HIV Association; c, cobicistat; DHHS, Department of Health and Human Services; DOR, doravirine; DRV, darunavir; DTG, dolutegravir;
EACS, European AIDS Clinical Society; EFV, efavirenz; EVG, elvitegravir; FTC, emtricitabine; IAS USA, International Antiviral Society–USA; LPV, lopinavir; NNRTI, non-nucleoside reverse transcriptase inhibitor;
NRTI, nucleoside reverse transcriptase inhibitor; NVP, nevirapine; PI, protease inhibitor; r, ritonavir; RAL, raltegravir; RPV, rilpivirine; TAF, tenofovir alafenamide fumarate; TDF, tenofovir disoproxil fumarate;
WHO, World Health Organization; XTC, FTC or 3TC.
1. EACS Guidelines Version 9.1. Available from: http://www.eacsociety.org/guidelines/eacs-guidelines/eacs-guidelines.html. Accessed January 2019;
2. DHHS Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Available from: https://aidsinfo.nih.gov/guidelines/html/1/adult-and-adolescent-arv/0. Accessed January 2019;
3. Saag MS, et al. JAMA 2018;320:379–396;
4. BHIVA Guidelines. Available from: http://www.bhiva.org/documents/Guidelines/Treatment/2016/treatment-guidelines-2016-interim-update.pdf. Accessed January 2019;
5. WHO. December 2018 Supplement to the 2016 Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. Available from: https://apps.who.int/iris/bitstream/handle/10665/277395/WHO-CDS-HIV-18.51-eng.pdf?ua=1 Accessed
January 2019.
Slide courtesy of Prof. Chloe Orkin (updated)

Shifts in Use of Initial cART regimens in the Netherlands (2013-2017)
2013 2014
2015 2016 2017
TAF/FTC/EVGc
ABC/3TC/DTG
TDF/FTC/DTG
TDF/FTC/EVGc
TAF/FTC/DTG
TDF/FTC/EFV
TDF/FTC/EFV
SYMTUZA Darunavir / COBI /
TAF / FTC
BIKTARVYBictegravir/TAF/FTC
DELSTRIGODoravirine + tenofovir DF +
lamivudine
https://www.hiv-monitoring.nl/en/resources/monitoring-report-2018

-10 -8 -6 -4 -2 0 2 4 6 8 10
Snapshot Outcomes at Week 48 for GEMINI-1 and -2
Cahn et al. AIDS 2018; Amsterdam, the Netherlands. Slides TUAB0106LB.
aBased on Cochran-Mantel-Haenszel stratified analysis adjusting for the following baseline stratification factors: plasma HIV-1
RNA (≤100,000 c/mL vs >100,000 c/mL) and CD4+ cell count (≤200 cells/mm3 vs >200 cells/mm3).
Virologic outcome Adjusted treatment difference (95% CI)a
Percentage-point difference
DTG + 3TC is non-inferior to DTG +
TDF/FTC with respect to proportion
<50 c/mL at Week 48 (snapshot, ITT-E
population) in both studies
DTG + TDF/FTC
-6.7 1.5
-4.3 2.9
GEMINI-1
GEMINI-2 -0.7
-2.6
DTG + TDF/FTC DTG + 3TC
90
4 6
93
26
93
25
94
2 4
0
20
40
60
80
100
Virologicsuccess
Virologicnonresponse
No virologicdata
HIV
-1 R
NA
<50
c/m
L, %
GEMINI-1 DTG + 3TC (N=356) DTG + TDF/FTC (N=358)
GEMINI-2 DTG + 3TC (N=360) DTG + TDF/FTC (N=359)
Cahn. Lancet. 2019;393:P143.
Two Drug Regimens for Initial Treatment

DHHS, IAS-USA, EACS Guidelines: Recommendations on 2DR for First-line ART
▪ Caveats to first-line DTG + 3TC use: HBV coinfection, GEMINI-1/2 excluded patients with HIV-1 RNA > 500,000 copies/mL, tuberculosis, pregnancy/woman with childbearing potential
▪ Data that could potentially support DTG + 3TC as a recommended initial regimen in DHHS guidelines: durability (96-wk GEMINI data), longer-term resistance data
DHHS*[1] IAS-USA†[2]
Consider when ABC, TAF, or TDF cannot be used or are not optimal:▪ DTG + 3TC▪ DRV/RTV + RAL BID, if HIV RNA < 100,000
copies/mL and CD4+ cell count > 200 cells/mm3
▪ DRV/RTV QD + 3TC
Initial 2DR only recommended when patient cannot take ABC, TAF, or TDF:▪ DTG + 3TC ( short term data may provide support)▪ DRV/RTV + RAL, if HIV RNA < 100,000 copies/mL
and CD4+ cell count > 200 cells/mm3
▪ DRV/RTV + 3TC
Modified from: clinicaloptions.com
EACS#[3]
Consider when none of the preferred regimens are feasible or available, whatever the reason :▪ DTG + 3TC▪ DRV/RTV or COBI QD + RAL BID, if HIV RNA <
100,000 copies/mL and CD4+ cell count > 200 cells/mm3
1.*DHHS Guidelines. October 2018. 2.† Saag. JAMA. July 24, 2018. 3.# EACS Guidelines vs 9.1, October 2018
Take-home message on DTG + 3TC: It is a new initial ART option for some patients

An Emerging Concern with IntegraseInhibitor-based Regimens:
More Weight Gain?
iStock.com/royalty-free image

NA-ACCORD: Weight Gain Among 24,001
ART-Naive Patients Initiating Treatment
▪ Multivariate analysis of weight gain following ART initiation (January 2007 - December 2016)
‒ INSTI-based regimens: n = 4740
‒ EVG: n = 2124; RAL: n = 1681; DTG: n = 935
‒ PI-based regimens: n = 7436
‒ NNRTI-based regimens: n = 11,825
▪ Higher weight gain with INSTI-based vs NNRTI-based regimens, with DTG or RAL vs EVG
‒ Weight gain with INSTIs did not vary by sex or race
Slide credit: clinicaloptions.comBourgi. CROI 2019. Abstr 670.

NA-ACCORD: Weight Gain by Class or Specific
INSTI
Slide credit: clinicaloptions.com
Pre
dic
ted
We
igh
t (k
g)
Yrs Since ART Initiation
86
84
82
80
0 1 2 3 4 5
Yr 2
Yr 5
INSTI
PI
NNRTI
+4.9
+4.4
+3.3
+6.0
+5.1
+4.3
Pre
dic
ted
We
igh
t (k
g)
86
84
82
80
Yrs Since ART Initiation0 0.5 1.0 1.5 2.0
Yr 2
DTG
RAL
EVG
+6.0
+4.9
+3.8
PI
NNRTI
Bourgi. CROI 2019. Abstr 670.

Weight Gain After Switch to INSTI-Based ART
▪ Prospective, observational cohort study of weight gain after switch to INSTI-based ART in patients enrolled on ACTG A5001, A5322 from 2007-2017 (N = 691)
‒ HIV-1 RNA < 200 copies/mL at time of switch required for inclusion
▪ Annual weight gain increased following switch to INSTI, with greater increases among women, blacks, and individuals 60 yrs of age or older
Slide credit: clinicaloptions.comLake. CROI 2019. Abstr 669.
Adjusted Annual Weight Change,* kg/yr (P Value)
Women Men Women Men Women ≥ 30 kg/m2
at SwitchBlack White Black White40 Yrs or Younger
60 Yrs or Older
40 Yrs or Younger
60 Yrs or Older
2 yrs pre-INSTI0.4
(.08)0.6
(.03)0.4
(.02)0.4
(< .0001)1.5
(.01)-0.2(.61)
0.8(.009)
0.1(.46)
0.2(.54)
2 yrs post-INSTI1.3
(< .0001)2.0
(< .0001)1.0
(.002)0.2
(.09)-1.0(.17)
1.8(.0005)
-0.1(.88)
0.9(.0008)
1.9(< .0001)
Post–pre difference
0.9(.04)
1.4(.02)
0.6(.11)
-0.2(.38)
-2.5(.02)
2.0(.008)
-0.9(.20)
0.8(.04)
1.7(.002)
*Adjusted for age at switch, sex, race/ethnicity, BL BMI and their interactions, nadir CD4+ cell count, smoking history, diabetes, and % time with HIV-1 RNA < 200 c/mL.

Weight Gain After Switch to INSTI-Based ART by
Agent, Pre-Switch ART Class, and NRTI Backbone
at Switch
▪ Change in weight gain rate greater with DTG vs EVG or RAL
▪ Increases in weight change per yr from pre- to post-INSTI periods statistically significant (P < .05) with:
‒ Switch to DTG from PI or NNRTI
‒ Switch to EVG from NNRTI
‒ Switch to any INSTI + ABC
‒ Switch to EVG + TAF
▪ However, analysis limited by small sample sizes in subsets
Slide credit: clinicaloptions.comLake. CROI 2019. Abstr 669.
Adjusted Annual Weight Change, kg/yr (P Value)
DTG (n = 198)
EVG(n = 204)
RAL(n = 289)
2 yrs pre-INSTI0.2
(.11)0.5
(.008)0.5
(< .0001)
2 yrs post-INSTI1.3
(< .0001)0.9
(< .0001)0.3
(.045)
Post–pre difference
1.0(.0009)
0.5(.11)
-0.2(.37)

Changes in Weight Through Wk 41 (Primary Endpoint)
▪ No significant weight gain with LA CAB vs PBO in HIV-uninfected individuals through Wk 41
‒ ≥ 5% weight gain: 22% with LA CAB vs 18% with PBO (P = .62)
‒ No differential effects by BMI category, sex at birth, race/ethnicity, dosing cohort, or smoking status
▪ No statistically significant differences in fasting glucose or lipid changes through Wk 41 with LA CAB vs PBO
Landovitz. CROI 2019. Abstr 34LB. Slide credit: clinicaloptions.com
LA CAB (n = 108) PBO (n = 38)
+0.9 (-1.2, 2.8)
+0.7 (-1.5, 2)
P = .65+1.1 (-0.9, 3)
+1.0 (-1.2, 3.2)
P = .66
+0.4 (-0.4, 1)
+0.1 (-0.6, 1)
P = .60
Overall Wks 0-41
Oral Phase Wks 0-4
Injection Phase Wks 5-41
Med
ian
Ch
ange
in W
eigh
t, k
g (I
QR
)
1.00
0.25
0.75
0.50
0
HPTN 077: Body Weight Change in Patients
Without HIV Enrolled in Long-Acting Cabotegravir
Safety Trial

What’s coming?
Longer acting approaches to HIV Treatment
• Oral: MK-8591 (NRTTI)
• Injectable• Subcutaneous: PRO140 (humanized IgG4 MoAb against
CCR5)
• Intramuscular: cabotegravir; rilpivirine
• Infusion: bNAb’s
• Implantable: MK-8591 (NRTTI)

Do we need LA-ARVs for treatment and why?
Many patients perfectly happy with daily STR
Some might prefer less frequently dosed ART
– Greater convenience
– Less stigma
LA-ART could enhance treatment of patients with
adherence challenges
– Adolescents
– Patients with substance use disorder, psychiatric
disease, chaotic lives

Long-acting cabotegravir plus rilpivirineFLAIR: Study Design
▪ Multicenter, randomized, open-label phase III noninferiority trial
Orkin. CROI 2019. Abstr 140LB. NCT02938520. Slide credit: clinicaloptions.com
LA CAB 400 mg IM +LA RPV 600 mg IM Q4W
(n = 278)
Continue DTG/ABC/3TC PO QD‡
(n = 283)
ART-naive patients withHIV-1 RNA ≥ 1000
copies/mL,HBsAg negative,no NNRTI RAMs*
(N = 629)
*K103N permitted. †Patients with HIV-1 RNA < 50 copies/mL from Wk 16 to Wk 20 continued to maintenance phase. ‡Alternative, non-ABC NRTIs permitted for intolerance or HLA-B*5701 positivity. §Loading dose: LA CAB 600 mg IM + LA RPV 900 mg IM; regular dosing begun at Wk 8.
CAB 30 mg +RPV 25 mg PO QD
(n = 283)
Current AnalysisWk 48 Wk 4§
DTG/ABC/3TC PO QD‡
Induction Phase†
Maintenance Phase
Wk 96Day 0
Wk 20
▪ Primary endpoint: HIV-1 RNA ≥ 50 copies/mL at Wk 48 by FDA Snapshot (6% noninferiority margin)
▪ Secondary endpoints: HIV-1 RNA < 50 copies/mL at Wk 48 by FDA Snapshot, resistance at confirmed virologic failure, safety and tolerability, patient-reported outcomes

Difference (%)
Difference (%)
FLAIR: Efficacy at Wk 48 in ITT-E Population
▪ Confirmed VF: n = 3 per arm; emergent NNRTI + INSTI resistance in all CAB + RPV failures (all HIV-1 subtype A1), no resistance in DTG/ABC/3TC failures
Orkin. CROI 2019. Abstr 140LB. Reproduced with permission. Slide credit: clinicaloptions.com
Pat
ien
ts (
%)
100
80
40
60
20
0Virologic
Nonresponse (≥ 50 c/mL)
Virologic Success
(< 50 c/mL)
No Virologic
Data
2.1 2.5
93.6 93.3
4.2 4.2
LA CAB + LA RPV(n = 283)
DTG/ABC/3TC(n = 283)
-10% NImargin
Difference (%)
-3.7
0.4
-10 -8 -6 -4 -2 0 2 4 6 8 10
4.5
-2.8 2.1
-0.4
6% NImargin
-10 -8 -6 -4 -2 0 2 4 6 8 10
Virologic Outcomes (FDA Snapshot) Adjusted Treatment Difference (95% CI)*
DTG/ABC/3TCLA CAB + LA RPV
DTG/ABC/3TC LA CAB + LA RPV
Key Secondary Endpoint(HIV-1 RNA < 50 copies/mL)LA CAB + LA RPV noninferior
to DTG/ABC/3TC
Primary Endpoint(HIV-1 RNA ≥ 50 copies/mL)LA CAB + LA RPV noninferior
to DTG/ABC/3TC
*Adjusted for sex, BL HIV-1 RNA (< vs ≥ 100,000 c/mL).
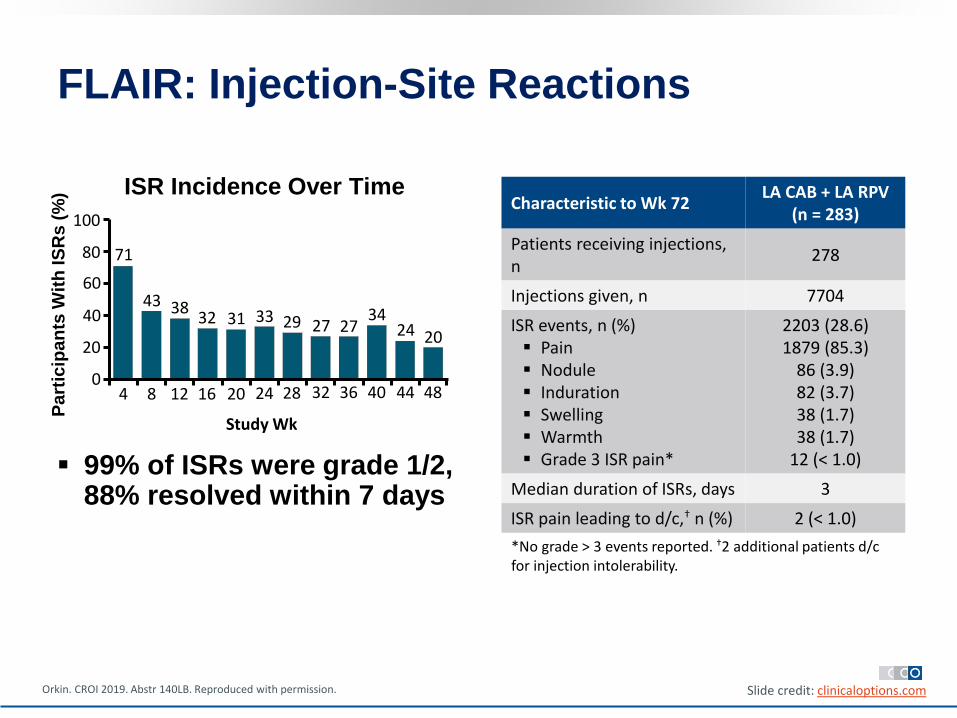
FLAIR: Injection-Site Reactions
▪ 99% of ISRs were grade 1/2, 88% resolved within 7 days
Orkin. CROI 2019. Abstr 140LB. Reproduced with permission. Slide credit: clinicaloptions.com
*No grade > 3 events reported. †2 additional patients d/c for injection intolerability.
ISR Incidence Over TimeCharacteristic to Wk 72
LA CAB + LA RPV (n = 283)
Patients receiving injections, n
278
Injections given, n 7704
ISR events, n (%)▪ Pain▪ Nodule▪ Induration▪ Swelling▪ Warmth▪ Grade 3 ISR pain*
2203 (28.6)1879 (85.3)
86 (3.9)82 (3.7)38 (1.7)38 (1.7)
12 (< 1.0)
Median duration of ISRs, days 3
ISR pain leading to d/c,† n (%) 2 (< 1.0)
Pa
rtic
ipa
nts
Wit
h IS
Rs
(%
)
Study Wk
100
80
60
40
20
04 8 12 16 20 24 28 32 36 40 44 48
71
43 3832 31 33 29 27 27
3424 20

FLAIR: Patient-Reported Outcomes
Orkin. CROI 2019. Abstr 140LB. Slide credit: clinicaloptions.com
‡Per single question in Wk 48 participant survey.
Drug Delivery Preference
of Patients in CAB + RPV Arm
Patient Satisfaction With
Regimen at Wk 48 vs Oral
Induction
HIVTSQc Mean Total Score*
Switch to LA CAB + LA RPV
(n = 263)
Continue DTG/ABC/3TC
(n = 266)
Wk 48† 29.6 25.5
PopulationPreferred Regimen,‡ % (n/N)
Long-Acting IM Daily PO
ITT-E 91 (257/283) 1 (2/283)
Responding participants
99 (257/259) NA*Scores can range from -33 to +33.†Difference: 4.1 (95% CI: 2.8-5.5; P < .001).

FLAIR: Plasma Trough Concentrations by
Visit
▪ Plasma concentrations with IM CAB and RPV similar to effective PO regimens
Orkin. CROI 2019. Abstr 140LB. Reproduced with permission. Slide credit: clinicaloptions.com
4 488 12 16 20 24 28 32 36 40 44
Visit (Wk)
0.1
1
10
Pla
sma
CA
B (
μg
/mL)
*
CAB (n = 278) PA-IC90 (0.166 µg/mL)
4 488 12 16 20 24 28 32 36 40 44
Visit (Wk)
10
100
Pla
sma
RP
V (
ng
/mL)
*
RPV (n = 278)PA-IC90 (12 ng/mL)
*Median (5th, 95th percentile) concentration–time data.
TDM-guided indidualized dosing a possibility?

Outline
• What To Start?:
• Guidelines & Practice
• 2 Drugs for Initial Treatment
• Weight Gain on INSTI-based ART
• Long-acting ART
• When To Start?:
• What Happens in Practice
• Same Day ART

Strategic Timing of AntiRetroviral Treatment(START) Study
23
Immediate ART Deferred ART
No. with Event (%) 42 (1.8%) 96 (4.1%)
Rate/100PY 0.60 1.38
HR (Imm/Def) 0.43 (95% CI: 0.30 to 0.62, p <0.001)
2.5
5.3
N Engl J Med 2015
Fred Gordin

In 2017 >85% of PWH entering care in NL started
treatment within 1 month(in 2016: 75%)
Time between entry into care and initiation of combination
antiretroviral therapy (cART) from 2007-2017
same day
within 7-13 days
within 14-20 days
within 21-31 days
within 1 week
https://www.hiv-monitoring.nl/en/resources/monitoring-report-2018

Universal rapid treatment initiation fairly
uniform across the 26 NL treatment centres
25
Proportion of patients started on cART within 6 months afterentering care, by year & treatment centre size
> 700 pts
400-700 pts < 400 pts

• In 2017, 45% overall of newly-diagnosed individuals had AIDS and/or CD4 cells <350/mm3 when entering care
At time of diagnosis far too many have likely
already been infected much longer (NL data)
% late presenters
>45 yrs <25 yrs
MSM 50% 23%
Other men 71% 48%
Women 59% 26%
63%
52%
37%
Late presentation even more common
in those over 45 at time of entry into
care (2015 or later)

Recommendations on Same-Day ART Initiation▪ DHHS guidelines, October 2018[1]:
‒ Same-day initiation of ART may be feasible and could potentially improve clinical outcomes . . . It should be emphasized, however, that ART initiation on the same day of HIV diagnosis is resource intensive . . . As these resources may not be available in all settings and the long-term clinical benefits of same-day ART initiation have yet to be proven in the United States, this approach remains investigational.
▪ IAS-USA guidelines, July 2018[2]:
‒ ART should be initiated as soon as possible after diagnosis, including immediately after diagnosis, unless patient is not ready to commit to starting therapy.
▪ EACS guidelines, October 2018 [3] :
‒ Evidence is accumulating that starting ART on the same day after establishing a diagnosis of HIV infection is feasible and acceptable to HIV-positive persons. Nevertheless, assessment of the readiness to start ART is essential to enable the HIV-positive person to express their preference and not feel pressured to start ART immediately, unless clinically indicated.
‒ Immediate (same day) start of ART should be considered, especially in thefollowing situations: In the setting of primary HIV infection, especially in case of clinical signs and symptoms of meningoencephalitis (within hours).
Slide credit: clinicaloptions.com1. DHHS Guidelines. October 2018. 2. Saag. JAMA. 2018;320:379. 3.# EACS Guidelines vs 9.1, October 2018

Phylogenetically Inferred Sources of Transmission in MSM with Recent HIV
Infection in The Netherlands

Amsterdam:
Rapid trajectory for Dx of acute/recent HIV (since 08-2015)
Dijkstra BMC Infectious Diseases 2017, Lin JAIDS 2018

Conclusions• INSTI-based therapy has become the preferred approach
• 2DR likely to become an initial option for some patients
• Issue of weight gain on INSTI-based ART is to be
resolved: watch the extremes!
• Long-acting ART:
• We’re only at the beginning with IM
cabotegravir+rilpivirine
• Use and utility in clinical practice is to be determined
• Immediate treatment increasingly being put into practice
• Early diagnosis remains the bottleneck to be resolved
• Early diagnosis of acute & recent infection + same
day ART important to contribute to epidemic control

Thank you for sharing slides:
Chloe Orkin Godelieve de Bree
Maartje DijkstraDan Kuritzkes
Christophe Fraser