antiplatelet, antikoagulan
DESCRIPTION
Slides tentang antiplatelet, antikoagulan, antithrombotic/fibrinolytic oleh dr Niko FKUPHTRANSCRIPT

Antiplatelets, Anticoagulant, Antithrombotic/Fibrinolytic
Dr. dr. Nicolaski Lumbuun, SpFKFaculty of Medicine Universitas Pelita Harapan

Learning Objectives
• To describe the role of Oral antiplatelets, Antithrombotic-fibrinolytic, and rTPA therapy.
• To know the pharmacology of antiplatelet medication, including the drug mechanism.
• To know the pharmacology of anticoagulant medication, including the drug mechanism.

Key-Words
• Platelets >< Antiplatelets
• Coagulation >< Anticoagulation
• Thrombus >< Fibrinolytic
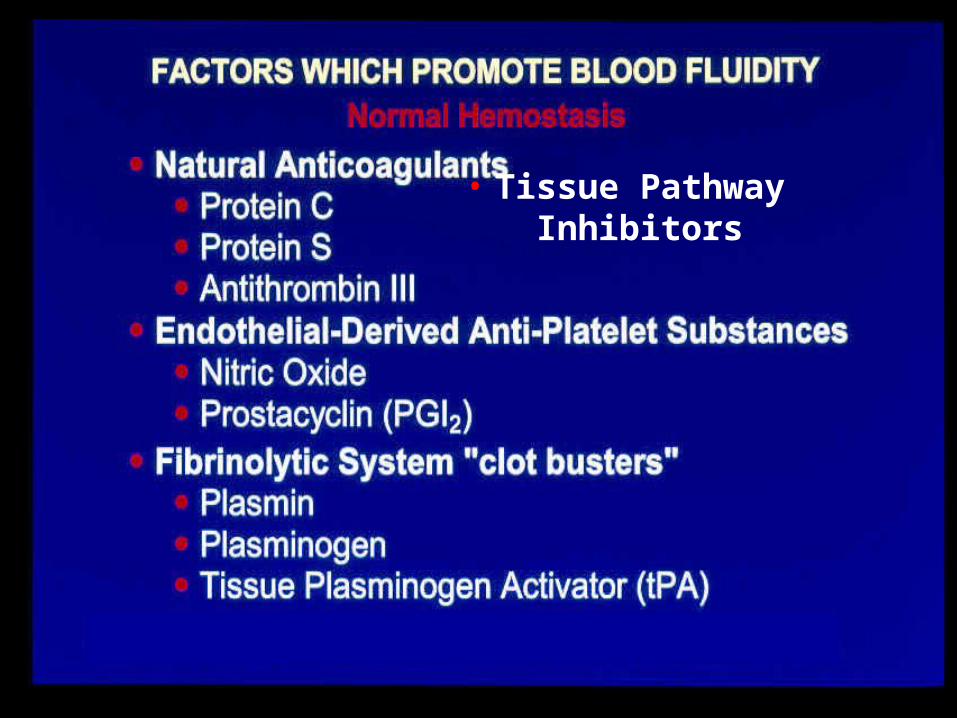
• Tissue Pathway Inhibitors
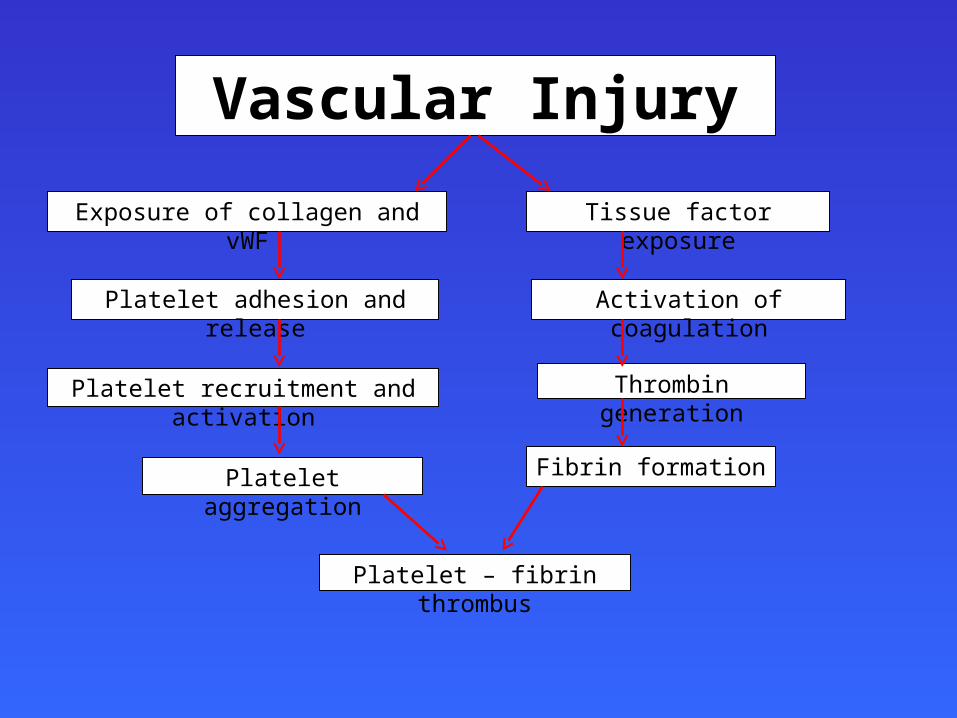
Vascular Injury
Exposure of collagen and vWF Tissue factor exposure
Platelet adhesion and release Activation of coagulation
Platelet recruitment and activation Thrombin generation
Fibrin formationPlatelet aggregation
Platelet – fibrin thrombus


III


Antiplatelet drugs
• Effective in the arterial. Circulation coagulation process have lack of effect.
• Decrease platelet aggregation inhibit thrombus formation• Widely used in primary and secondary prevention of
cerebrovascular (occlusive stoke) or cardiovascular disease & prevent end-stent thrombosis after PCI.
• Sometimes used in peripheral arterial disease.
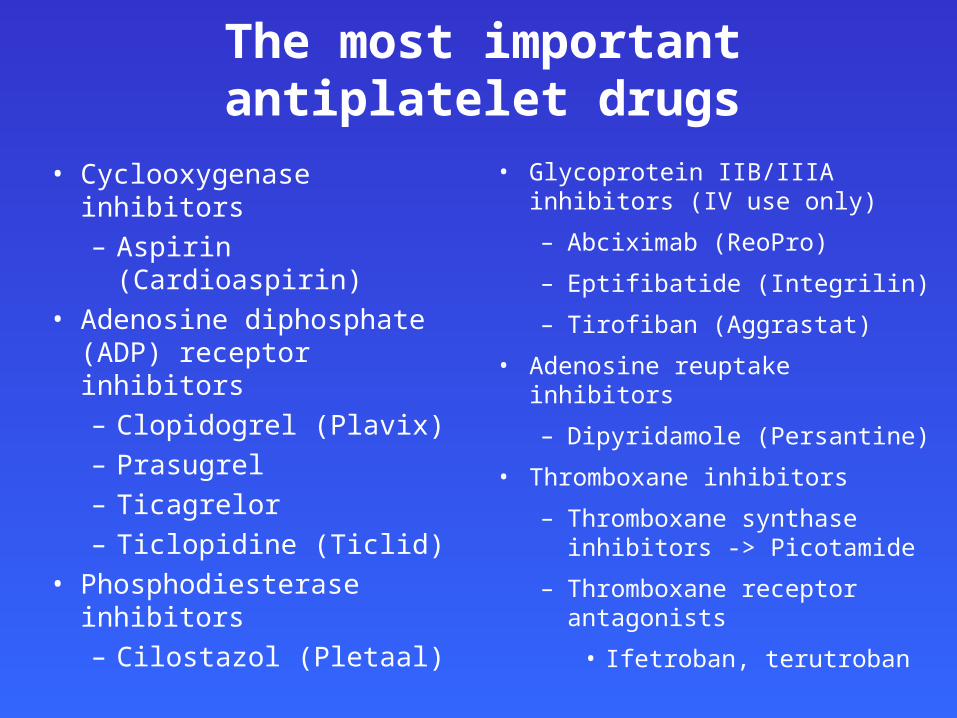
The most important antiplatelet drugs
• Cyclooxygenase inhibitors– Aspirin (Cardioaspirin)
• Adenosine diphosphate (ADP) receptor inhibitors– Clopidogrel (Plavix)– Prasugrel – Ticagrelor– Ticlopidine (Ticlid)
• Phosphodiesterase inhibitors– Cilostazol (Pletaal)
• Glycoprotein IIB/IIIA inhibitors (IV use only)
– Abciximab (ReoPro)
– Eptifibatide (Integrilin)
– Tirofiban (Aggrastat)
• Adenosine reuptake inhibitors
– Dipyridamole (Persantine)
• Thromboxane inhibitors
– Thromboxane synthase inhibitors -> Picotamide
– Thromboxane receptor antagonists
• Ifetroban, terutroban
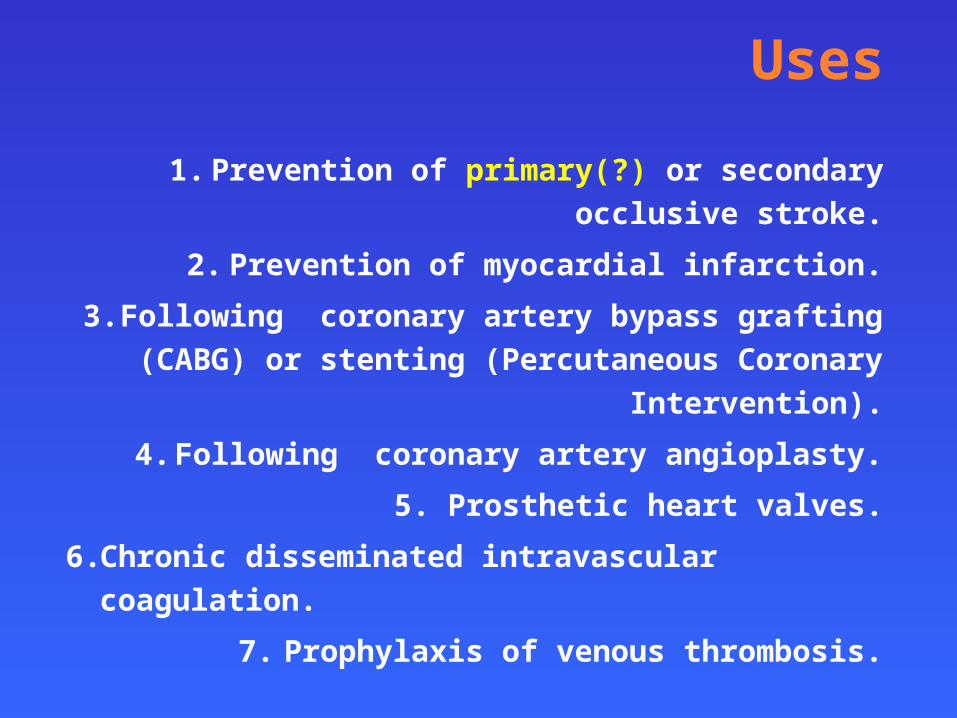
Uses
1. Prevention of primary(?) or secondary occlusive stroke.
2. Prevention of myocardial infarction.
3. Following coronary artery bypass grafting (CABG) or
stenting (Percutaneous Coronary Intervention).
4. Following coronary artery angioplasty.
5. Prosthetic heart valves.
6. Chronic disseminated intravascular coagulation.
7. Prophylaxis of venous thrombosis.

Aspirin ( Acetylsalicylic Acid )
Mechanism of ActionAspirin irreversibly acetylates the active site of cyclooxygenase, which is required for the production of thromboxane A2, a powerful promoter of platelet aggregation.
Indication :Patients who survived a prior occlusive event (including MI, occlusive stroke or transient ischemic attack, or other high risk categories including unstable and stable angina, angioplasty, or CABG & PCI).
Aspirin, prevents ~25% of serious vascular events, including significant reductions on MI, stroke, and CVD death.
Side effects Peptic Ulcer, Increased incidence of GIT bleeding
ADP pathway inhibitors (Ticlopidine & Clopidogrel)
Mechanism of Action Inhibits binding of ADP to its platelet receptor by irreversibly
modifying the platelet ADP receptor.
Pharmacokinetics of ticlopidine• Given orally.
• Extensively bound to plasma proteins.
• Metabolized in the liver to give active metabolites.
• Slow onset of action (3 - 5 days).• is taken twice ( 250 mg twice daily ).
Adverse EffectsSevere neutropenia, Bleeding (Prolong bleeding time), CYP450
inhibitors, G.I.T : Diarrhoea, Nausea, Dyspepsia, Allergic Reactions.

Clopidogrel– Clopidogrel is more potent.
– Less side effects ( less neutropenia).– Less Frequency of administration (75 mg once daily).
– Bioavailability is unaffected by food.
Clinical UsesAlternative prophylactic th/ to aspirin in secondary prevention
of stroke and myocardial infarction and unstable angina.
New Oral Antiplatelet Drugs
Prasugrel– Thienopyridine– More rapid onset of action
than clopidogrel– Irreversible inhibitor of the
P2Y12 receptor
Ticagrelor *– Cyclo-pentyl-triazo-pyrimidine
(CPTP)– More rapid onset of action
than clopidogrel– Reversible inhibitor of the
P2Y12 receptor
Adenosine Diphosphate-Receptor AntagonistsAdenosine Diphosphate-Receptor Antagonists
* Not approved by FDA

Dipyridamole
Phosphodiestrase inhibitor thus cAMP in the blood platelets inhibition of platelet aggregation.
Uses• Taken orally.
• Primary prophylaxis in patients with prosthetic heart values (in combination with warfarin ).
• Prophylactic therapy for angina pectoris in combination with aspirin .
Disadvantages : Headache Advantage : No excess risk of bleeding

Glycoprotein IIb/ IIIa receptor inhibitors
Is a receptor for fibronectin, fibrinogen, vitronectin and von Willebrand factor.
1. Abciximab• a monoclonal antibody that inhibits glycoprotein IIb/ IIIa
receptor.
• Inhibits all the pathways of platelet activation (Final common pathway).
• Given I.V. infusion
• Uses : adjuncts to heparin and aspirin for prevention of cardiac ischemic complications.
• Side effect is immunogenicity

2. Tirofiban & Eptifibatide • Eptifibatide (peptide)
• Tirofiban (non-peptide) – are synthetic mimetics of arginine-glycine-aspartic
sequence of fibrinogen
– inhibits glycoprotein IIb/ IIIa receptor at site that interacts with arginine-glycine-aspartic sequence of fibrinogen (by occupancy of the receptor) fibrinogen like mimetic agent
– Given I.V.
– Uses : Acute coronary syndromes to decrease incidence of thrombotic complications

Recent Issue of Antiplatelets
• Adverse events :Un-tolerate of ADE of Aspirin GI symptom, bleedingUnacceptable risk of bone marrow toxicity Ticlopidine
• Antiplatelet Drug Resistance :Resistance of Aspirin, Clopidogrel & Glycoprotein
IIB/IIIA inhibitors The issue is whether it is clinically important to routinely
screen patients for antiplatelet drug resistance.

ANTI COAGULANTS
Indirect Thrombin Inhibitors
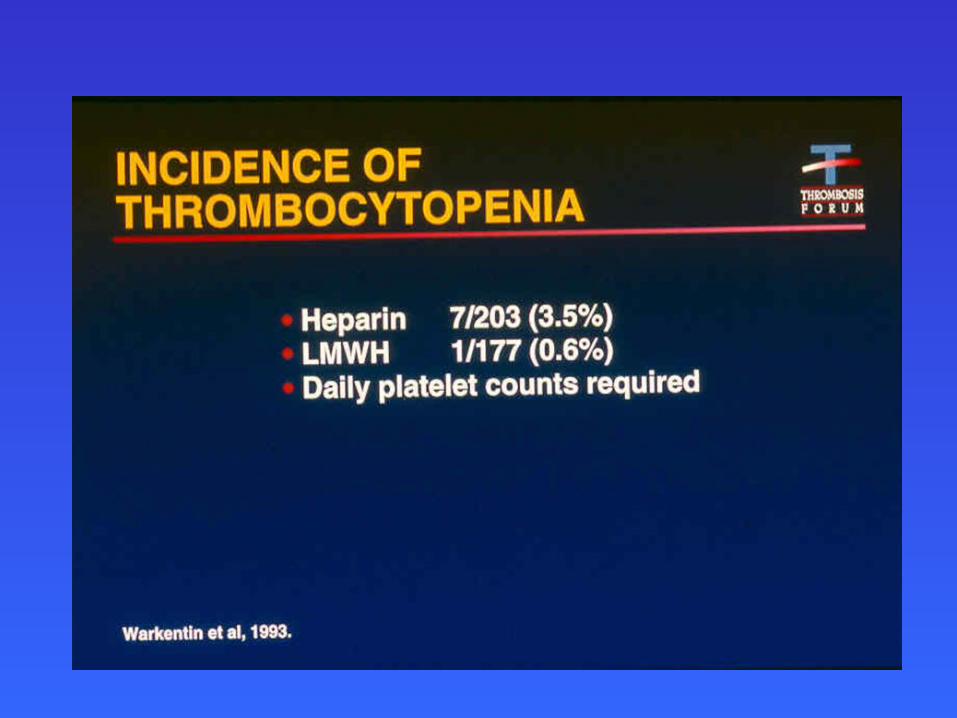
•Unfractionated Heparin
•LMWH – Enoxaparin, dalteparin
•Fondaparinaux
•Rivaroxiban (1st oral factor Xa inhibitor)
Direct Thrombin Inhibitors
•Hirudin – Lepirudin
•Bivalirudin
•Argatroban
•Melagatran
•Ximelagatran (oral)
•Dabigatran (oral)
Indications For Antithrombotic Therapy
• Venous thromboembolic disease– Deep venous thrombosis (DVT)– Pulmonary embolism (PE)– Primary prophylaxis of DVT or PE
• Arterial thromboembolic disease• Prosthetic heart valves• Mitral valve disease, especially with atrial fibrillation• Congestive cardiomyopathies, especially with atrial fibrillation• Atrial fibrillation• Mural cardiac thrombi• Transient ischemic attacks• Stroke in evolution
• Disseminated intravascular coagulation• Maintenance of patency of vascular grafts, shunts, bypasses
• Preventing the formation of clots and extension of existing
clots within the blood.
• Does not break down clots that have already formed
(unlike tissue plasminogen activator), it allows the body's
natural clot lysis mechanisms to work normally to break
down clots that have already formed.
• Antidote of heparin intoxication : protamine sulphate
Heparin

Anticoagulant Properties of Heparin
1. Activation anti-thrombin III Inhibits the thrombin-
mediated conversion of fibrinogen to fibrin
2. Inhibits the aggregation of platelets by thrombin
3. Inhibits activation of fibrin stabilizing enzyme
4. Inhibits activated factors XII, XI, IX, X and II

Unfractionated Heparin
• High Dose– Treatment of venous/arterial thrombi– Requires monitoring– IV- 5,000 Units bolus, then 30,000-35,000 units/24 hrs– 80 Units/kg bolus, then 18 Units/kg/hr to maintain aPTT in
therapeutic range
• Low Dose– Surgical Prophylaxis
• 5,000 Units SC 2 hr pre-op• 5,000 Units SC every 12 hours
– Medical Prophylaxis• 5,000 Units SC every 12 hours
– No monitoring required






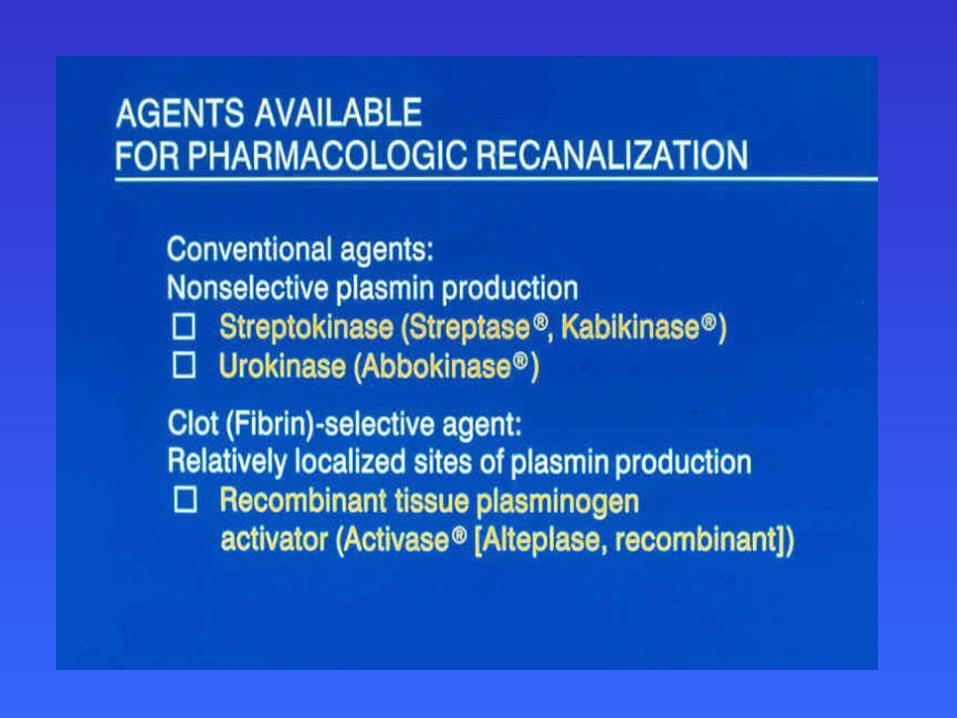
FIBRINOLYTICS
• Streptokinase
• Urokinase
• Anistreplase
• t-PA
• Reteplase
• tenecteplase

Thrombolytic Agents = Fibrinolytic drugs
• Dissolve blood clots by activating plasminogen, which forms a cleaved product called plasmin.
• Plasmin is a proteolytic enzyme that is capable of breaking cross-links between fibrin molecules, which provide the structural integrity of blood clots.
Tissue plasminogen activator produces clot lysis through :
1. tPA binds to fibrin on the surface of the clot
2. Activates fibrin-bound plasminogen 3. Plasmin is cleaved from the
plasminogen associated with the fibrin
4. Fibrin molecules are broken apart by the plasmin and the clot dissolves


Anisolated Plasminogen Streptokinase
Activator Complex

Keep in mind about Streptokinase
• Is a bacterial product, the body has the ability to build up an immunity to it.
• Recommended that this medication should not be used again after four days from the first administration, as it may not be as effective and can also cause an allergic reaction.
• For this reason, it is usually given only for a person's first heart attack. Further thrombotic events could be treated with Tissue plasminogen activator (tPA).
• Overdose of streptokinase or tPA can be treated with aminocaproic acid.

Take Home Message
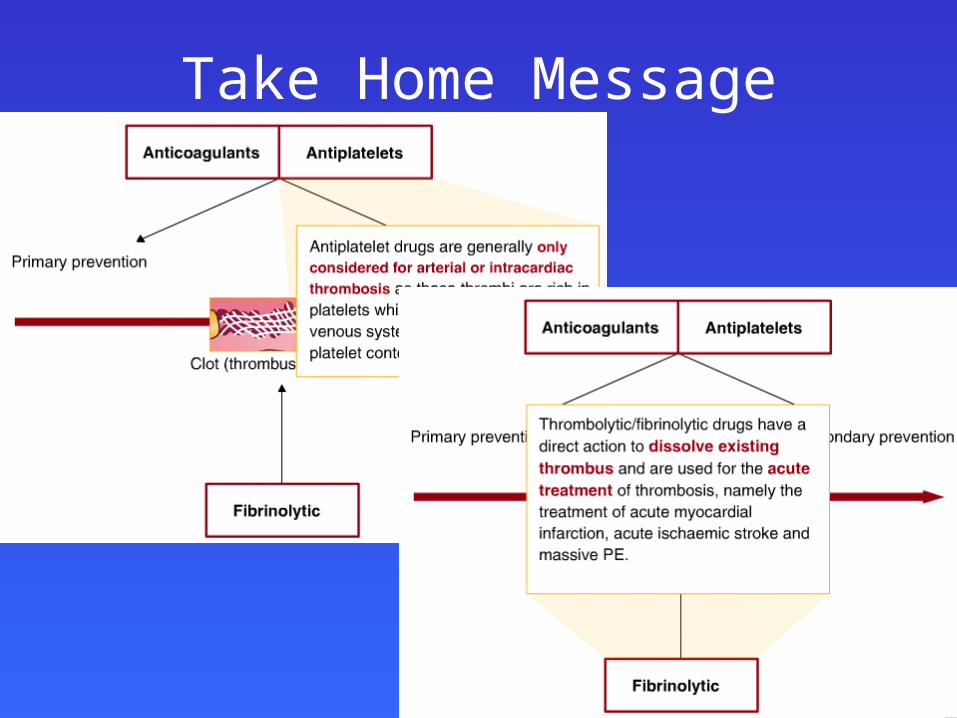
Take Home Message

THANK
YOU
Thank You