anti tnf therapy in rheumatoid arthritis prof. marc feldmann · the screen versions of these slides...
TRANSCRIPT

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 1
1
Kennedy Institute of Rheumatology Division Kennedy Institute of Rheumatology Division Kennedy Institute of Rheumatology Division Kennedy Institute of Rheumatology Division F aculty of MedicineF aculty of MedicineF aculty of MedicineF aculty of Medicine
Anti TNF Therapy in Rheumatoid Arthritis
Marc Feldmann
Imperial CollegeLondon
Supported by
2
TNF: historyTumour necrosis Cachexia
Carswell et al., 1975 PNAS 72727272: 3666
Inflammation
Leucocyte recruitmentVascular damage and leak
e.g., trypanosomasis,cancer, catabolic state
muscle wasting, anaemia
A. Cerami
Cloning of TNFPennica et al., 1984, NatureBeutler et al., 1985, Nature
3
Why look for cytokines in rheumatoid arthritis?U pregulation of HLAU pregulation of HLAU pregulation of HLAU pregulation of HLA----DR in rheumatoid synoviumDR in rheumatoid synoviumDR in rheumatoid synoviumDR in rheumatoid synovium
(Klareskog, Wigzell, Panayi, Janossy etc. 1981/82)
Rheumatoid arthritis Osteoarthritis
Expression of HLA-DR on cells usually negative
indicates presence of inducers = cytokines
Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 2
4
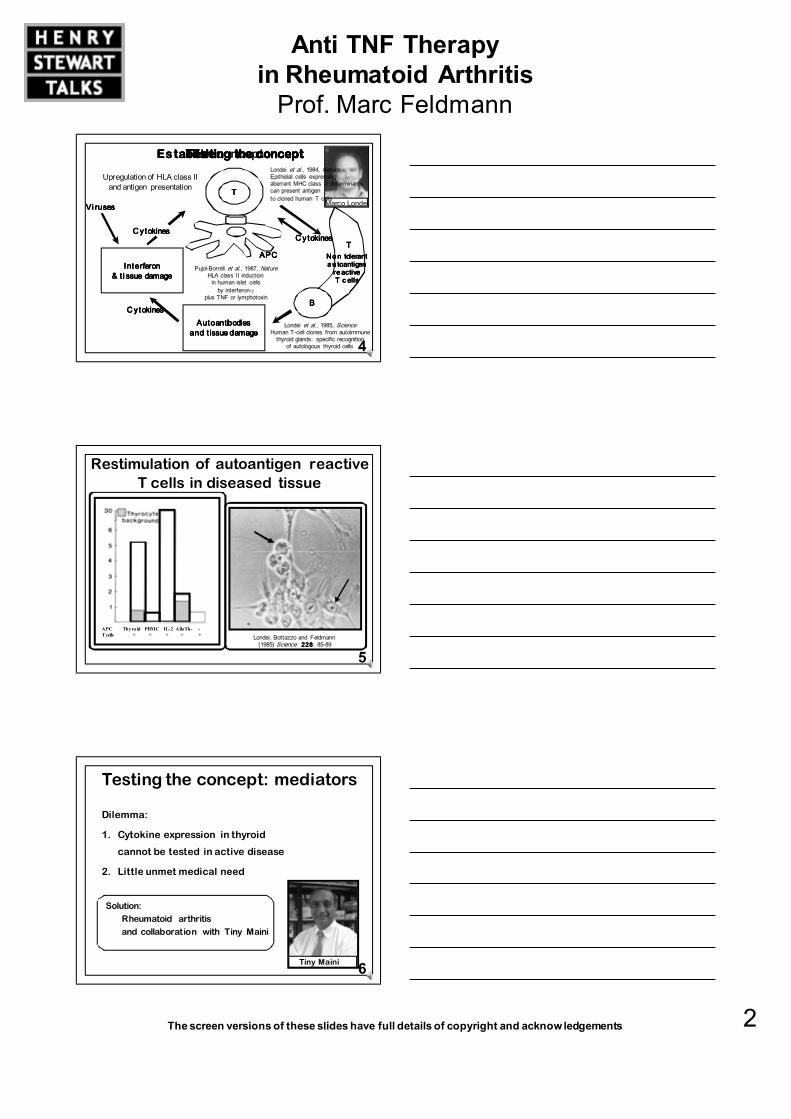
Establishing the conceptEstablishing the conceptEstablishing the conceptEstablishing the conceptTesting the conceptTesting the conceptTesting the conceptTesting the concept
Londei et al., 1985, ScienceHuman T-cell clones from autoimmune
thyroid glands: specific recognition of autologous thyroid cells
InterferonInterferonInterferonInterferon& t i ssue damage& t i ssue damage& t i ssue damage& t i ssue damage
AutoantibodiesAutoantibodiesAutoantibodiesAutoantibodiesand t issue damageand t issue damageand t issue damageand t issue damage
Vi rusesVi rusesVi rusesVi ruses
C ytokinesC ytokinesC ytokinesC ytokines
C ytokinesC ytokinesC ytokinesC ytokines
The concept
TTTT
Upregulation of HLA class II and antigen presentation
No n tolerant No n tolerant No n tolerant No n tolerant a u toantigen a u toantigen a u toantigen a u toantigen
re activere activere activere activeT c ellsT c ellsT c ellsT c ells
TTTT
BBBB
APCAPCAPCAPC
C ytokinesC ytokinesC ytokinesC ytokines
Marco Londei
Londei et al., 1984, NatureEpithelial cells expressing aberrant MHC class II determinants can present antigen to cloned human T cells
Pujol-Borrell et al., 1987, NatureHLA class II induction
in human islet cells by interferon-γ
plus TNF or lymphotoxin
5
APC Thyroid PBMC IL-2 AlloTh- -
T cells + + + + +
Restimulation of autoantigen reactiveT cells in diseased tissue
Londei, Bottazzo and Feldmann(1985) Science 228228228228: 85-89
6
Testing the concept: mediators
Dilemma:
1. Cytokine expression in thyroid
cannot be tested in active disease
2. Little unmet medical need
Tiny Maini
Solution:
Rheumatoid arthritis
and collaboration with Tiny Maini

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 3
7
Many cytokines are produced in rheumatoid synovium
Are any therapeutic targets?
Pro-inflammatory
e.g., IL-1, IL-6, TNFα, IL-12, IL-15, IL-17, IL-18,
IFNγ, IL-2, OncoM, GM-CSF
Anti-inflammatory
e.g., IL-10, IL-1Ra, TGFβ, IL-11, IL-13
Chemokines
e.g., IL-8, MIP-1α, MCP-1, RANTES, ENA-78, GROα
Growth Factors
e.g., VEGF, PDGF, FGF
8
Prolonged synthesis of IL-1αin rheumatoid synovium
0
1
2
3
4
5
6
1 2 3 4 50
IL-1αα ααmRNA
(units*)
Time (days)
Buchan et al., (1988) Clin Exp Immunol 73737373:449
Normal
Glenn Buchan * 1 unit = normal blood response to LPS
A l l curves are ILA l l curves are ILA l l curves are ILA l l curves are IL----1111αααα mRNAmRNAmRNAmRNAf rom different patients synovium or normalf rom different patients synovium or normalf rom different patients synovium or normalf rom different patients synovium or normal
9
Analysis of cytokine regulationrevealed importance of tumour necrosis factor
ApproachApproachApproachApproachOperative sample synovium,active RA cells isolated, placed in ‘tissue culture’ObservationObservationObservationObservationSpontaneous production of many mediators of disease-cytokines, enzymes etc.
Brennan et al. (1989) Lancet II 244-247
6310
10
20
30
control
anti LT
anti TNFα
IL-1
(U/m
l)
Days of culture
Rh eumatoid arthritisRh eumatoid arthritisRh eumatoid arthritisRh eumatoid arthritis Os t eoarthritisOs t eoarthritisOs t eoarthritisOs t eoarthritis
6310.00.20.40.60.81.0
Days of culture
IL-1
(U/m
l)
Fionula Brennan
ExperimentExperimentExperimentExperimentAntibody to TNF inhibitsproduction of otherpro-inflammatory cytokines

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 4
10
A useful oversimplification….
Cytokine cascade in rheumatoid arthritis
Immune system TNTNTNTNFFFFα
Anti-inflammatory
IL-10, IL-1rα, sTNF-R
Pro-inflammatory
IL-6, IL-8, GM-CSF etc.
IL-1
Feldmann, Brennan and Maini (1996) Cell, 85858585: 307
11
TNF is early onset Anti-TNF diminishes IL-1 and IL-6
0000 1111 2222 3333 4444 5555 6666Hour sHour sHour sHour s
0000 1111 2222 3333 4444 5555 6666Hour sHour sHour sHour s
TNFTNFTNFTNF
I LI LI LI L ---- 1111
I LI LI LI L ---- 6666
I LI LI LI L ---- 6666
I LI LI LI L ---- 1111
I LI LI LI L ---- 1+TNF1+TNF1+TNF1+TNFα I LI LI LI L ---- 6+TNF6+TNF6+TNF6+TNFα
Adapted from Fong et al., J. Exp. Med. 170170170170: 1627 (1989)
Cytokine cascade is physiological:occurs in response to infection
12
ModelGenetically susceptible mice (DBA/1) Injected collagen type II(major constituent cartilage)About 21 days later arthritis appearsand then spreads joints destroyed
TNF blockade protects joints in an animal model of rheumatoid arthritis
A nt iA nt iA nt iA nt i----TNF treatedTNF treatedTNF treatedTNF treated
I s otype IgG controlI s otype IgG controlI s otype IgG controlI s otype IgG control
Nor m alNor m alNor m alNor m alWilliams, Feldmann, Maini (1992)
Proc Natl Acad Sci (USA) 89898989, 9784
Histology
Results
0000 2222 4444 6666 8888 10101010 12121212 14141414Days after onset of arthritis
A n t iA n t iA n t iA n t i ----TNF (500 TNF (500 TNF (500 TNF (500 µµµµg)g)g)g)
A n t iA n t iA n t iA n t i ----TNF (50 TNF (50 TNF (50 TNF (50 µµµµg)g)g)g)
A n t iA n t iA n t iA n t i ----TNF (300 TNF (300 TNF (300 TNF (300 µµµµg)g)g)g)
control
Paw
thick
ness
(% in
crem
ent)
0000
10101010
2020202030303030
40404040
50505050
60606060
70707070
Richard Williams Bob Schreieber

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 5
13
Rationale for anti-TNFαααα therapy in rheumatoid arthritis
1. Disregulated cytokine network in RA synovium
is dependent on TNFα
2. TNFα/TNF-receptor upregulated in synovium
3. Animal model of RA responds very well to anti-TNFα administered after disease onset
14
From bench to bedside
• Jim Woody at Centocor agreed to help
• Clinical trial with cA2 (now infliximab)
started in May 1992 at CX Hospital
• By 1991 the stage was set for clinical translation
• Due to Cerami’s concept of TNF driving
sepsis anti-TNF antibodies had been made
Jim Woody
15
Remicade® (infliximab)
Knight DM et al., Mol Immunol., 1993; 16161616: 1443-1453
Jan Vilcek
John Ghrayeb
Harlan Weissman
• Chimeric IgG1
monoclonal antibody
• High affinity binding
to TNFα (Ka = 1010M-1)
• Administered
by intravenousinfusion over 1 hourevery 8 weeks

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 6
16
p < 0 .00 1 0.0 01 0 .00 2 0. 02 0 .00 1 0.0 01p < 0 .00 1 0.0 01 0 .00 2 0. 02 0 .00 1 0.0 01p < 0 .00 1 0.0 01 0 .00 2 0. 02 0 .00 1 0.0 01p < 0 .00 1 0.0 01 0 .00 2 0. 02 0 .00 1 0.0 01
0000
2 02 02 02 0
4 04 04 04 0
6 06 06 06 0
8 08 08 08 0
1 0 01 0 01 0 01 0 0
1 2 01 2 01 2 01 2 0
W eeksW eeksW eeksW eeksSc reenSc reenSc reenSc reen0000 1111 2222 3333 4444 6666 8888
CRPp < 0 .01 0.0 01 0 .00 1 0.0 01 0 .00 1p < 0 .01 0.0 01 0 .00 1 0.0 01 0 .00 1p < 0 .01 0.0 01 0 .00 1 0.0 01 0 .00 1p < 0 .01 0.0 01 0 .00 1 0.0 01 0 .00 1
Sc reenSc reenSc reenSc reen 0000 1111 2222 3333 4444 6666 8888
Swollen joint count
ResultsW e llW e llW e llW e ll ---- toleratedtoleratedtoleratedtoleratedUn i versal clinical responseUn i versal clinical responseUn i versal clinical responseUn i versal clinical responseRa p id suppression ESR and CRPRa p id suppression ESR and CRPRa p id suppression ESR and CRPRa p id suppression ESR and CRPNo n o n respondersNo n o n respondersNo n o n respondersNo n o n responders
In f l ix imab: 20 mg/kg In f l ix imab: 20 mg/kg In f l ix imab: 20 mg/kg In f l ix imab: 20 mg/kg ( total)( total)( total)( total)
W e ek W e ek W e ek W e ek ----4444 0000 2222 4444 6666 8888
An a lysisAn a lysisAn a lysisAn a lysis
wa shoutwa shoutwa shoutwa shout
Design
0000
4444
8888
1 21 21 21 2
1 61 61 61 6
2 02 02 02 0
2 42 42 42 42 82 82 82 8
Open-label treatment with infliximab in rheumatoid arthritis
Elliott, Maini, Feldmann et al., Arthritis Rheum 1993, 36363636: 1681-90
(mg/l)
W eeksW eeksW eeksW eeks
17
Randomised, placebo-controlled trialof infliximab in rheumatoid arthritis
R esultsR esultsR esultsR esultsWell-toleratedGood clinical responses in cA2 groupsDose-response relationship
DDDD es ignes ignes ignes ign
3, 10 or 20 mg/kg3, 10 or 20 mg/kg3, 10 or 20 mg/kg3, 10 or 20 mg/kg1 or 10 mg/kg1 or 10 mg/kg1 or 10 mg/kg1 or 10 mg/kgor HSAor HSAor HSAor HSA
Week -4 0 4
washout
c A 2:c A 2:c A 2:c A 2:
Elliott, Maini, Feldmann et al., Lancet 1994; 344: 1105-10
Placebo
1 mg/kg cA2
10 mg/kg cA2
4321000
10
20
30
40
50
60
70
80
Week
normal range
p<0.001
p<0.01
CRP
4321000
10
20
30
Week
Swollen joint count
p<0.001p<0.001
44%
8%
79%
1 mg/kg
Placebo
10 mg/kg
Responders
Non-responders
p=0.0083
p<0.0001
Paulus 20% responses at week 4Ferry Breedveld
Jochen Kalden
Josef Smolen
(mg/l)
18
Early evidence of efficacy of repeated infliximab therapy
Swollen
joint
count
(0-28)
CRP
(mg/l)
6050403020100-100
10
20
0
10
20
30
40
50
60
70
Week
1020 10 10
Dose infliximab (mg/kg)
Elliott, Maini, Feldmann et al. Lancet 1994; 344344344344:1125

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 7
19
Combination therapy - sub-optimal
anti-TNF plus anti-CD4
Time, days0000 1111 2222 3333 4444 5555 6666 7777 8888 9999 10101010
1.41.41.41.4
1.51.51.51.5
1.61.61.61.6
1.71.71.71.7
1.81.81.81.8
1.91.91.91.9
2.02.02.02.0
2.12.12.12.1
****
Williams et al., Proc Nat Acad Sci 91919191:2762-2766 (1994)
Paw
thic
knes
s m
m
C ontrol mAb C ontrol mAb C ontrol mAb C ontrol mAb
AntiAntiAntiAnti----TNF + TNF + TNF + TNF + ant i CD4 ant i CD4 ant i CD4 ant i CD4 Ant iAnt iAnt iAnt i----CD4 CD4 CD4 CD4
al one al one al one al one
Ant iAnt iAnt iAnt i----TNFTNFTNFTNF
* p < 0.05
20
% p
atie
nts
resp
ondi
ng
1 mg/kg cA2 3 mg/kg cA2 10 mg/kg cA2
Week
Paulus 50% responses to infliximab
60
80
40
20
0
20
60
80
40
0
0 4 8 12 16 26 0 4 8 12 16 26 Week0 4 8 12 16 26
100 100
Placebo MTX+ cA2 MTX- cA2 MTX+
Maini RN et al., (1998) Arthritis Rheum.; 41414141: 1552-1563
±±±±methotrexate: synergy
21Maini RN et al., (1998) Arthritis Rheum. 41414141:1552
Rationale of combination infliximab and MTX
100
75
50
25
0
(% o
f pat
ient
s)
Infliximab dose (mg/kg)1 3 10
Antibodies to infliximab
InfliximabInfliximab + MTX
Weeks
10
Seru
m in
flixi
mab
(mg/
ml)
0
51 mg/kg
100
75
50
25
00 2 6 1410 18 2622
10 mg/kg
3 mg/kg
20
15
10
5
Pharmacokineti cs

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 8
22
Attract: sustained prevention of structural damage
0.64.8 1.0 -0.5 -0.31.3 1.6 0.2-0.7
7.0 1.0 1.0 1.1 -0.412.6
-3
0
3
6
9
12
15
18
+ MTXPlacebo Infliximab
3mg/kg
q 8 wks
Infliximab 3mg/kg
q 4 wks
Infliximab 10mg/kg
q 8 wks
Mean (SE) change from baseline
0 - 30 Weeks
0 - 54 Weeks
0 - 102 Weeks
+ MTX + MTX + MTX
Infliximab 10mg/kg
q 4 wks
+ MTX
Lipsky et al., (2000) NEJM 343343343343(22): 1594
Peter Lipsky
At t ractA t t ractA t t ractA t t ract
23
Reversal of structural damage
Infliximab Infliximab Infliximab InfliximabPlacebo
+ MTX
+ MTX + MTX + MTX + MTX
*
Negative change in modified sharp score at week 54
p-value vs. MTX <0.001 <0.001 <0.001 <0.001
14%
45%
49%
39%
54%
0%
10%
20%
30%
40%
50%
60%
3 mg/kg q 8 wks
3 mg/kg q 4 wks
10 mg/kg q 8 wks
10 mg/kg q 4 wks
Percent with improvement
At t ractA t t ractA t t ractA t t ract
24
Combination of etanercept and methotrexateis more effective (tempo)
Reproduced from: Klareskog et al., (2004)Lancet 3 633 633 633 63: 675Therapeutic effect of the combinationof etanercept and methotrexate compared with each treatment alone in patients with rheumatoid arthritis: double-blind randomised controlled trial
Lars Klareskog
Time (months) 121
Time (months)126

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 9
25
Summary of anti-TNF therapy in rheumatoid arthritis
1. Control of symptoms: pain, stiffness, fatigue
2. Control of signs: swelling, tenderness
3. Control of joint destruction
4. Initiation of joint repair: reduced sharp score
5. Improvement in health (HAQ)
6. Approaching 106 treated patients
7. Long term benefit
26
Antibody based therapeutic proteins can be used for many years
27Breedveld FC, et al., Arthritis Rheum., 2003; 48 48 48 48 (Suppl):S118 [Abstract 198]
Months
% of patients
(n = 53) (n = 36)
6862
75
63
77
3036
50 50 46
8 11
2824 22
010
203040
5060
7080
12 24 36 48 60
ACR-20
ACR-50
ACR-70
18% retention18% retention18% retention18% retentionat 5 yearsat 5 yearsat 5 yearsat 5 years
Bob Kamen Jeff Leiden
Adalimumab (Humira) + MTX:sustained efficacy over 5 years

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 10
28From: Moreland et al., ACR 2004
7 years of etanercept therapy
29
Verifying mechanismof action in phase II useful
30Charles et al., (1999) J Immunol; 163163163163: 1521-28
Day282170 141 3
0
100
200
150
50
Ser
um IL
-6 (p
g/m
l)
P l aceboP l aceboP l aceboP l acebo1 m g/kg1 m g/kg1 m g/kg1 m g/kg1 0 mg/kg1 0 mg/kg1 0 mg/kg1 0 mg/kg
TNFα dependent cytokine cascadeis operative in vivo

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 11
31
Other cytokinesdown regulated also
e.g., IL-1, VEGF, MCP-1 etc.
32
TNF is the body’s fire alarm
Initiates leucocyte recruitment
33
3
TNFα blockade and inflammatory cell traffic - early clues
Paleolog et al., Arthritis Rheum 1996, 39393939; 1082
Weeks after infusion
†
0 1 2 3 4Pre-infusion
****
****** ***
***
***††
**
†††††††
†††
0
1
2
Lymphopenic range
Lym
phocyte
s x
10
9/l
H&E staining CD3+
Before
After
Tak, Taylor et al., Arthritis Rheum 1996, 39393939; 1077
10mg/kg anti-TNFαααα1mg/kg anti-TNFααααPlacebo
Pai red synovial biopsiesPai red synovial biopsiesPai red synovial biopsiesPai red synovial biopsies

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 12
34Knees Hands
Pre
-tre
atm
ent
2 w
eeks p
ost-
treatm
ent
Reduced PMN trafficking after infliximab therapy
Taylor et al., (2000) Arthritis Rheum 43434343:38-47R knee L Hand R handL knee
Perc
enta
ge c
hange
cpm
/pix
el
/MB
q
5
-5
-15
-25
-35
-45
-55
-65
Peter Taylor
35
Most chronic inflammatory diseases respond to anti-TNF
36
TNF is a good target in many chronic diseases
• Approved use
Rheumatoid arthritis, juvenile rheumatoid arthritis, Crohn’s,psoriatic arthritis, Ankylosing spondylitis, Psoriasis, ulcerative colitis
• Trials not completed and pilot studiesBehçet’s syndrome, vasculitis (wegeer’s and giant cell),
glomerulonephritis, SLE, joint prosthesis loosening, hepatitis, polymyositis, systemic sclerosis, amyloidosis, sarcoidosis, ovarian cancer, steroid resistant asthma, refractory uveitis
• Clinical failuresCongestive heart failure, multiple sclerosis, Sjogren’s syndrome
Common theme: inhibition leucocyte recruitment

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 13
37
-60
-50
-40
-30
-20
-10
0
+10
W e eks after infusionW e eks after infusionW e eks after infusionW e eks after infusion
P l aceboP l aceboP l aceboP l acebo
0000 1111 2222 3333 4444
1 m g/kg anti1 m g/kg anti1 m g/kg anti1 m g/kg anti ----TNFTNFTNFTNFαααα
1 0 mg/kg 1 0 mg/kg 1 0 mg/kg 1 0 mg/kg antiantiantianti ----TNFTNFTNFTNFαααα
Paleolog et al. (1998) Arthritis Rheum 41 41 41 41 1258-65
Decrease in serum VEGFafter single infusion of infliximab
von
Wille
bran
d fa
ctor
-pos
itive
vess
el co
unt/
field
Anti-TNFα reduces synovial vessel density
M e ans of 5M e ans of 5M e ans of 5M e ans of 5----8 fields per patient, 8 fields per patient, 8 fields per patient, 8 fields per patient, a d justed for the area of a single fielda d justed for the area of a single fielda d justed for the area of a single fielda d justed for the area of a single field
Pr ePr ePr ePr e Pos tPos tPos tPos t0
20406080
100120140160
Ballara, S. et al., (2001) A&R 44444444: 2055
Reduced angiogenesis after anti-TNF
Ewa Paleolog
38
1. Downregulati on of many proinflammatory cytokines in vivoIL-1, GM-CSF, IL-6, IL-8 and other chemoki nes (Feldmann et al., 1996)
2. Reduction in leukocyte traffickingReduction in adhesion molecul es and chemoki nes (Feldmann et al., 1997)
3. Reduction in angiogenesisReduction in VEGF (Paleolog et al., 1998)
4. Reduction in joint destructi onReduction in IL-1, MMPs �XR changes (Brennan et al., 1989, 1997, ACR 99)
5. Haematol ogi cal normalizationHaemogl obin �, platelets �, fibrinogen �: cardiovascular risk � ?
6. Others:Promotes apoptosi s (via Deventer, Klareskog)
Induces regulatory T cells (Ehrenstein et al., 2004)
Normalized T cell response to recall antigen (Cope, 1994)
How is cytokine washout with infliximab translated into clinical benefit?
Conclusion: TNFα close to core of disease
39
Nothing is perfect: problems
1. Efficacy
2. Safety:
Infection
Lymphomas
3. Cost
4. Convenience

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 14
40
Safety problems of TNF blockade
• Interferes host defence
• Infection TB < 1/2000Other opportunistic infections rarer
Common infection: URTI, pneumoniaInfected prosthesesHerpes Zoster
• B cell lymphomas
Quantifying frequency infection/B cell lymphomas
is difficult as rheumatoids have markedly increased risk, proportional disease severity
Safety needs to be seen
in context of reduced life span/life quality
41
Early treatment is more effective
BeSt Trial, Goekoop-Ruiterman….Breedveld …et al., 2005, A&R 52525252(11): 3381
Entry: active RA, median duration symptoms23 weeks, diagnosi s to inclusion 2 weeks
ACR70
Ferry Breedveld
05
1015
20
253035
40
45
3 6 9 12
Time, months (n)
Percentage
MonoStep-upCOBRAAnti-TNF
42From: Quinn and Emery et al., (2005) A&R 52525252: 27-35
Prolonged reduction in disease activity despite cessation of anti TNF
60% ACR 70 cf 0%
Paul Emery

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 15
43
Impact on medicine and research
1.1.1.1. New therapeutics for many diseases:New therapeutics for many diseases:New therapeutics for many diseases:New therapeutics for many diseases:
TNF as body’s fire alarm
2.2.2.2. Improvements in clinical trial designImprovements in clinical trial designImprovements in clinical trial designImprovements in clinical trial design,
speed, cost
3. Realization that profound joint protectionprofound joint protectionprofound joint protectionprofound joint protection
and even repair possible
4.4.4.4. Best resultsBest resultsBest resultsBest results
- EarlyEarlyEarlyEarly
- Combination with methotrexate
5.5.5.5. Importance of “translational research”:Importance of “translational research”:Importance of “translational research”:Importance of “translational research”:
Bench to bedside emphasized
44
Impact of TNF blockadeon pharmaceutical industry
1. Source of new therapeutics; commercial success
- 2 blockbusters (> $1bn/year) Remicade®, Enbrel®another soon (Humira®)
2. Appreciation that biologics can be used long term- For chronic diseases – less risk
3. Relative safety–mechanism related capacity to generate biologics- Almost half of all therapeutic candidates now biologics
4. Prime example of academic-industrial collaboration- Academic know how of disease, target, clinical needs
- Industrial capacity to make and develop therapeutic
45
Acknowledgements
Key external collaborators: reagents
Major contributors to relevant knowledge
Cloning TNF: D. Goeddel, P. Gray, B. Beutler
TNF biology: A. Cerami, C. Dinarello etc.
Tada
Taniguchi
Tadamitsu
Kishimoto
Mike
Shepard
Bob
Schreiber

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 16
46
Acknowledgements
Preclinical: key internal collaborators
D r Glenn Buchan team: D r Glenn Buchan team: D r Glenn Buchan team: D r Glenn Buchan team: Maija KissonerghisKatherine Barrett
Ini tial gene expression Ini tial gene expression Ini tial gene expression Ini tial gene expression i n j ointsi n j ointsi n j ointsi n j oints
Pr of. Fionula Brennan team:Pr of. Fionula Brennan team:Pr of. Fionula Brennan team:Pr of. Fionula Brennan team:David ChantryMartin Turner
Gene regulation in joints:Gene regulation in joints:Gene regulation in joints:Gene regulation in joints:T N F as pivotal cytokineT N F as pivotal cytokineT N F as pivotal cytokineT N F as pivotal cytokine
D r Richard Williams team:D r Richard Williams team:D r Richard Williams team:D r Richard Williams team:Lesley Mason
Amelioration of collagenAmelioration of collagenAmelioration of collagenAmelioration of collageni nduced arthritis i nduced arthritis i nduced arthritis i nduced arthritis
by anti TNF antibodyby anti TNF antibodyby anti TNF antibodyby anti TNF antibody
D r Ewa Paleolog team:D r Ewa Paleolog team:D r Ewa Paleolog team:D r Ewa Paleolog team:Sylvia YoungAngela Stark
R ol e of VEGF in arthritisR ol e of VEGF in arthritisR ol e of VEGF in arthritisR ol e of VEGF in arthritis
Clinical triallists: Elliott, Taylor, Woody, Weisman,
Breedveld, Kalden, Smolen, Lipsky, St Clair, Emery etc.
47
Acknowledgements
Sir Ravinder Maini
48
Acknowledgements: funding
arcKennedy Trust
Nuffield FoundationWellcome Trust
US NavyCentocor

Anti TNF Therapy
in Rheumatoid Arthritis
Prof. Marc Feldmann
The screen versions of these slides have full details of copyright and acknowledgements 17
49