anorexia nervosa: a case study by: colleen shank sodexo dietetic intern april 30, 2014
TRANSCRIPT

Anorexia Nervosa: A Case Study
By: Colleen ShankSodexo Dietetic Intern
April 30, 2014

“Up to 24 million people of all ages and genders suffer from an eating disorder (anorexia, bulimia and binge eating disorder) in the U.S (The Renfrew Center Foundation for Eating Disorders)”
“Only 35% of people that receive treatment for eating disorders get treatment at a specialized facility for eating disorders” (Noordenbox, 2002)
Presentation of Anorexia Nervosa
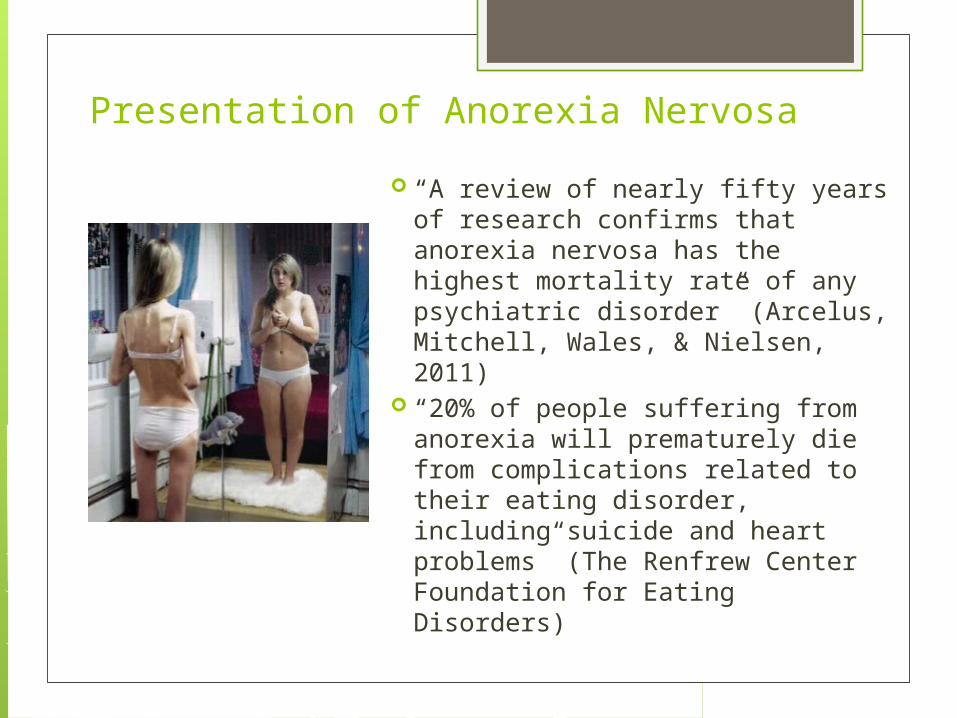
“A review of nearly fifty years of research confirms that anorexia nervosa has the highest mortality rate of any psychiatric disorder” (Arcelus, Mitchell, Wales, & Nielsen, 2011)
“20% of people suffering from anorexia will prematurely die from complications related to their eating disorder, including suicide and heart problems” (The Renfrew Center Foundation for Eating Disorders)
Presentation of Anorexia Nervosa

Presentation of Anorexia Nervosa
Overview of how one may suffer from AN: Body image distortion Restrictive intake and or binging/purging Excessive exercise Severe weight loss Fear of becoming fat Physiological changes Psychological changes

Two types:1. Restricting type
o Energy intake is restricted
2. Binge-eating/purge typeo Vomitingo Excessive exercising
Both types suffer from fear of gaining weight
Presentation of Anorexia Nervosa

Diagnosis criteria: DSM-51. Restriction of energy intake relative to
requirements leading to a significantly low body weight in the context of age, sex, developmental trajectory, and physical health.
2. Intense fear of gaining weight or becoming fat, even though underweight.
3. Disturbance in the way in which one's body weight or shape is experienced, undue influence of body weight or shape on self-evaluation, or denial of the seriousness of the current low body weight
Presentation of Anorexia Nervosa
The Alliance for Eating Disorders

Screening Tools: EDI-3 Eat-26 Can be given by
health Care professionals
Can be accessed online
Can help assess risk Do not diagnose
eating disorders
Types of Questions: Gender, height,
weight How often one feels,
experiences, likes, or avoids certain things Avoiding foods when
hungry, feeling guilty after eating, eat diet foods, etc.
How often one partakes in certain behaviors
Vomiting, binging, and exercising
Presentation of Anorexia Nervosa
Physical Signs & Symptoms: Weight loss Tiredness Thinning hair Hair loss Dry skin Swelling of arms/legs Lanugo Intolerance to cold
Presentation of Anorexia Nervosa

Internal Changes: Body systems are affected
Examples: cardiovascular, neuroendocrine, renal, and gastrointestinal systems Slow heart rate Anemia Stomach gets smaller Constipation Dehydration Amenorrhea Osteoporosis Hypothermia Hypotension
Presentation of Anorexia Nervosa

Psychological Signs & Symptoms: Not wanting to eat Fear of weight gain Extreme exercise Depression Preoccupation with food Lying Lack of social interaction
Presentation of Anorexia Nervosa

Tests/Labs: Height, weight,
BMI Look at
Heart Liver Kidneys Bones Thyroid Etc.
Tests/Labs: CBC Electrolytes Total protein Minerals H/H Glucose B12 Etc.
Presentation of Anorexia Nervosa

Examples of Abnormalities: Abnormal lipoprotein profile Low zinc Low vitamin B-12 Alkalosis Low chloride and potassium Elevated bicarbonate Hypomagnesmia Hypophosphatemia Lymphocytosis Low resting metabolic rate Mitral valve prolapse
Presentation of Anorexia Nervosa

Treatment: Requires a team
Physician, Psychologist/Psychiatrist, RD Not all treatment plans are the same
Everyone needs a treatment plan specific to them
Inpatient, outpatient, both
Presentation of Anorexia Nervosa

Treatment: Psychological One-on-one Group Family
Discover underlying issues
Treatment: Psychological Different types of
therapy CBT IPT SSCM Research?
Presentation of Anorexia Nervosa

Treatment: Pharmacotherapy Not to treat AN specifically
Used to treat underlying issues Antidepressants, antipsychotics
Olanzapine, Fluoxetine, Prozac, Risperidone Research?
Can drugs help improve weight gain?
Presentation of Anorexia Nervosa

MNT: AND Position Paper “Nutrition intervention, including
nutrition counseling by a registered dietitian, is an essential component of the team treatment of patients with anorexia nervosa, bulimia nervosa, and other eating disorders during assessment and treatment across the continuum of care”
Presentation of Anorexia Nervosa

MNT: RDs Role Assess the patient Determine nutrition risks Define nutrition diagnosis Identify nutrition intervention Write nutrition prescription Define nutritional goals
Presentation of Anorexia Nervosa

MNT: RD Assessment What is important to assess? Of course the RD will assess physical
signs and symptoms but there are other things that should be included in their assessment of the patient Current dietary intake Present eating patterns History related to foods Nutrient deficiencies Supplement use Risk of refeeding syndrome
Presentation of Anorexia Nervosa

Treatment: Current Guidelines Intake
recommendations Calculating needs Kcal
Starting point Increase by 100-
200kcals Macronutrients
CHO: 50-55% PRO: 15-20% Fat: 25-30%
Micronutrients?
Weight gain Differences
between in and out patient settings
Increase in kcal needs
Presentation of Anorexia Nervosa

Treatment: Refeeding Syndrome Refeeding a starved patient
Clinical implications Low Mg, K, P Thiamine deficiency
Must be aware of the affects Must follow protocol to help prevent
refeeding Monitor electrolytes and fluids
Presentation of Anorexia Nervosa

Treatment: Nutrition Support Need for nutrition support depends on
needs of the patient PN should only be used when medically
necessary
Presentation of Anorexia Nervosa

Basics: Age: 56 Sex: Female Lives at home with her mother and
sister Dates of hospital stay: January 15, 2014-
February 14, 2014 Date transferred to Manor Care:
February 14, 2014
Presentation of C.H.
Hospital Stay: Dx: FTT secondary to malnutrition,
Pancytopenia, Hypothermia related to malnutrition, Bradycardia related to hypothermia, and Hypotension related to dehydration
PMH: Anorexia, Anemia
Presentation of C.H.

Hospital Stay: Reason for going to ER: inability to ambulate and
weakness Vital 1.5 3 day calorie count Labs: Labs: BG 49, HGB 3.7, Creatinine 0.67, BUN
60 Per patient:
Reported that weight loss started several months ago
No menstruation anymore No diarrhea, blood in the stool Was on iron pill but stopped taking due to negative
side effects Has struggled with weight since age 11
Presentation of C.H.

Manor Care: Admit dx: FTT, (GERD), Refeeding
Syndrome, Pancytopenia, and History of intussusception
Her admission note states she was "in an anorexic and malnourished state"
Admit weight 76.6#, Height 62.0”, BMI 14.0 Stage 3 gluteal wound Left hip wound
Presentation of C.H.

Manor Care: No smoking, drinking, drug use history February 18, 2014
AOA involved Mother and sister were not allowed to bring
in food to patient
Presentation of C.H.

Manor Care: Plan Physical and occupational therapy Continue current diet, supplements, folic
acid, MVI, zinc, labs as scheduled Follow up with GI at the hospital as
scheduled Wound: local care with santyl, daily
dressing change/pressure relief, nutritional support
Presentation of C.H.

Manor Care: Labs from February
21, 2014 Random glucose: 78 BUN: 12 Creat: 0.40 K: 4.2 NA: 136 AST: 21 ALT: 30 Alk phos: 66 Total bilirubin: 0.3
Presentation of C.H.
Ca: 8.9 Alb: 3.6 Total pro: 6.3 GFR: >60 WBC: 6.6 RBC: 3.96 L HGB: 9.3 L HCT: 31.3 L MCV: 79.1 L MCH: 23.4 L

Manor Care: Medications Cholecalciferol 2000 unit po daily Heparin 5000 units SQ Folic acid 1mg po daily MVI po daily Protonix 40mg po daily Zinc sulfate 220mg po daily As needed: Miralax, Colace, Tylenol, MOM,
Dulcolax,
Ferrous liquid 220g po daily (added at a later date 3x/week)
Presentation of C.H.
Manor Care: On admission was placed on gluten
intolerance diet and enhanced food Prior to RD assessment
Was later changed to a regular diet No history of Celiac Disease
Presentation of C.H.

Manor Care: RD Assessment February 19, 2014 Current weight 77.2#, BMI 14.1 Interview
Pt prefers “plain foods” Pt reports allergy to guar gum
Consumption of meals 75-100% Eats meals slowly (1-1.5hours) No diarrhea, constipation, steatorrhea,
communication, dental/oral, or functional problems noted
Presentation of C.H.

Manor Care: RD Assessment Calculated needs (with IBW 110#:
35kcal/kg = 1750kcal/day 1.5g/kg pro= 75g/day 30mL/kg fluid= 1500mL/day
Diet order: Regular diet, Supplement TID No longer giving enhanced foods due to
pt liking plain foods Recommendations: weekly CMP, CBC, P,
Mg, LFTs, iron supplement
Presentation of C.H.

Manor Care: Weekly weights
2/14/14 76.6 # 2/18/14 77.2 # 2/24/14 77.6 # 3/4/14 82 #
Presentation of C.H.

Manor Care: Med Options Assessment Mental health evaluation (2 visits)
Main issue: AN Patient has difficulty with mood
functioning, behavioral functioning, and lack of insight
"I am not an anorexic" "I do eat- I like food but I have a difficult
time keeping the weight on"
Presentation of C.H.

Manor Care: My interaction with C.H Usual intake
3 meals per day (breakfast, lunch, and dinner) as well as snacks in between meals
UBW: 110-115# Since she has been sick she reports her weight
has been 85-90# States she does not usually keep track of weight Reports she could feel she was losing weight
when she started getting sick Reports when she was taking her iron pill that
would help her gain weight
Presentation of C.H.

Was d/c on March 4, 2014 D/c to home with mother and sister
No further info on AOA Weight at d/c 82#
Update on C.H.

Sources Eating Disorder Statistics. ANAD. http://www.anad.org. Accessed
April 20, 2014. Get the Facts on Eating Disorders. NEDA.
https://www.nationaleatingdisorders.org. Accessed March 13, 2014. Anorexia Nervosa. National Association of Anorexia Nervosa and
Associated Disorders. http://www.anad.org/. Accessed March 13, 2014.
Feeding and Eating Disorders. APAhttp://www.dsm5.org. Accessed March 13, 2014
DSM-5 Diagnostic Criteria. The Alliance for Eating Disorders. http://www.allianceforeatingdisorders.com. Accessed March 19, 2014.
The Eating Attitudes Test (EAT-26). Eat-26. http://www.eat-26.com/. Accessed April 3, 2014.
Mayo Clinic Staff. Anorexia Nervosa. Mayo Clinic. http://www.mayoclinic.org. Updated January 5, 2012. Accessed March 19, 2014.
Anorexia Nervosa. The New York Times. http://www.nytimes.com. Reviewed March 18, 2013. Accessed April 3, 2014.
Anorexia Nervosa Biochemical and Nutrient Issues. Academy of Nutrition and Dietetics Nutrition Care Manual. http://www.nutritioncaremanual.org. Accessed April 3, 2014.

Treatment Basics. NEDA. https://www.nationaleatingdisorders.org. Accessed April 4, 2014.
Eating Disorders. How can a psychologist help someone recover? APA. https://www.apa.org/. Revised October 2011. Accessed April 10, 2014.
Le Grange, D., Lock, J. Family-based Treatment of Adolescent Anorexia Nervosa: The Maudsley Approach. Maudsley Parents. http://www.maudsleyparents.org/whatismaudsley.html. Accessed April 10, 2014.
DeAngelis, T. Promising Treatments for anorexia and bulimia. Monitor on Psychology. March 2002; 33 (3): 38. http://www.library.illinois.edu/learn/research/citation/ama.html. Accessed April 10, 2014.
Schmidt U, Oldershaw A, Jichi F, et al. Out-patient psychological therapies for adults with anorexia nervosa: randomised controlled trial. The British Journal of Psychology. 2012, (201):392-399. DOI: 10.1192/bjp.bp.112.112078. Accessed April 10, 2014.
Carter, F, Jordan, J, McIntosh, V. V.W, et al. The long-term efficacy of three psychotherapies for anorexia nervosa: A randomized, controlled trial. Int. J. Eat. Disord. 2011; (44): 647–654. DOI: 10.1002/eat.20879. Accessed April 10, 2014.

Yager J, Devlin M, Halmi K, et al. Guideline Watch: Practice Guideline for the Treatment of Patients with Eating Disorders. 3 rd ed. APA. 2012. http://psychiatryonline.org/pdfaccess. Accessed April 10, 2014.
Mickley D. Medication for Anorexia Nervosa and Bulimia Nervosa. Eating Disorders Recovery Today. 2004; 2(4). http://www.eatingdisordersrecoverytoday.com. Accessed April 11, 2014.
Attia E, Kaplan A, Walsh B, et al. Olanzapine versus placebo for out-patients with anorexia nervosa [Abstract]. Psychological Medicine. 2011; 41(10): 2177-2182. DOI: http://dx.doi.org/10.1017/S0033291711000390 Accessed April 11, 2014.
Hagman J, Gralla J, Sigel E, et al. A Double-Blind, Placebo-Controlled Study of Risperidone for the Treatment of Adolescents and Young Adults with Anorexia Nervosa: A Pilot Study. JAACAP. 2011; 50(9): 915-924. DOI:10.1016/j.jaac.2011.06.009.
Walsh T, Kaplan A, Attia E, et al. Fluoxetine After Weight Restoration in Anorexia NervosaA Randomized Controlled Trial. JAMA. 2006;295(22):2605-2612. DOI:10.1001/jama.295.22.2605.
Ozier A, Henry B. Position of the American Dietetic Association: Nutrition Intervention in the Treatment of Eating Disorders. JADA. 2011;111:1236-1241. http://www.eatright.org/ Accessed April 11, 2014.

Waterhous T, Jacob M. Practice Paper of the American Dietetic Association: Nutrition Intervention in the Treatment of Eating Disorder. ADA. 2011; 11(8): 1261. http://www.eatright.org/ Accessed April 10, 2014.
Parent Toolkit. NEDA. 47. http://www.nationaleatingdisorders.org/sites/default/files/Toolkits/parenttoolkit/. Accessed April 11, 2014.
Anorexia Nervosa Nutrition Prescription. Academy of Nutrition and Dietetics Nutrition Care Manual. http://www.nutritioncaremanual.org. Accessed April 10, 2014.
Schebendach J. Nutrition in Eating Disorders. In: Mahan LK, Escott-Stump S. Krause’s Food & Nutrition Therapy. St. Louis, MO; Saunders Elsevier; 2008: 563-586.
Anorexia Nervosa Nutrition Support. Academy of Nutrition and Dietetics Nutrition Care Manual. http://www.nutritioncaremanual.org. Accessed April 11, 2014.
Robb A, Silber T, Orrell- Valente J, Valadez-Meltzer A, et al. Supplemental Nocturnal Nasogastric Refeeding for Better Short-Term Outcome in Hospitalized Adolescent Girls With Anorexia Nervosa. Am J Psychiatry. 2002;159:1347-1353. DOI:10.1176/appi.ajp.159.8.1347. Accessed April 11, 2014.