anatomy of the hand
TRANSCRIPT
1989; 69:1007-1013.PHYS THER. Christine A MoranAnatomy of the Hand
http://ptjournal.apta.org/content/69/12/1007be found online at: The online version of this article, along with updated information and services, can
Collections
Injuries and Conditions: Hand Anatomy and Physiology: Musculoskeletal System
in the following collection(s): This article, along with others on similar topics, appears
e-Letters
"Responses" in the online version of this article. "Submit a response" in the right-hand menu under
or click onhere To submit an e-Letter on this article, click
E-mail alerts to receive free e-mail alerts hereSign up
by guest on December 27, 2013http://ptjournal.apta.org/Downloaded from by guest on December 27, 2013http://ptjournal.apta.org/Downloaded from

Anatomy of the Hand
The anatomy of the hand is efficiently organized to cany out a variety of complex tasks. These tasks require a combination of intricate movements and finely controlled force production The shape of the bony anatomy in conjunction with the arrangement of soft tissues contributes to the complex kinesiology of the hand. Injury to any of these structures can alter the overall function of the hand and therefore complicate the therapeutic management. The purpose of this article is to review the anatomy of the hand with special emphasis on structures that relate to management of hand injuries. [Moron CA: Anatomy of the hand. Phys Ther 69:1007-1013, 1989]
Key Words: Anatomy; Hand; Hand injuries; Kinesiology/biomechanics, upper extremity; Upper extremity, hand and wrist.
Christine A Moran
The hand is a complex anatomical system of dynamic and static structures. Very often the general clinician is wary of treating patients with hand injuries because of the hand's anatomical and kinesiological complexity. These injuries are further complicated by traumatic or surgical processes. The purpose of this article is to review the anatomy of the hand emphasizing important structures related to therapeutic management.
Arthrokinematics
Finger
The carpometacarpal (CMC) joints of the fingers are classified as plane joints with one degree of freedom. However, the fifth CMC joint is often classified as a semisaddle joint with conjunctional rotation.1 The
metacarpophalangeal (MCP) joints are classified as ellipsoidal or condylar joints with two degrees of freedom.1,2 Specifically, the metacarpal condylar surface is asymmetrical with a greater sloping configuration of the radial shoulder than the ulnar shoulder.3 This articular configuration plays a role in ligamentous orientation and subsequent kinesiology of the joint. Therefore, it is of functional importance in describing certain pathological conditions such as ulnar drift.3
The proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints are both bicondylar with subsequently greater congruency between bony surfaces. They have one degree of freedom.1,2 In addition, the axis of motion has an obliquity of 6 to 13 degrees in the coronal plane because of the
unevenness of the condylar articulating surfaces at both PIP and DIP joints.2-4 This divergence of the distal aspect of these joints is accentuated by the pull of the flexor digito-rum sublimus (FDS) tendons and allows for opposition with the thumb. This divergence of the interphalangeal (IP) joint is important clinically when restoring motion via joint mobilization techniques. Volar gliding of the middle phalanx should be accomplished with this coronal tilt added to the gliding motion, thus more accurately stressing the capsular tissues.
Thumb
The CMC joint of the thumb is a sellar joint exhibiting two degrees of freedom with reciprocally convex-concave surfaces allowing for the motions of flexion and extension (concave-convex), abduction and adduction (convex-concave), and conjunctional rotation.1,2,5,6 The thumb MCP joint is similar to the finger MCP joints arthrokinematically. The thumb IP joint's articulating condyles also display an unevenness, resulting in an obliquity of the axis of motion of 5 to 10 degrees.
C Moran, MS, PT, is Director, The Richmond Upper Extremity Center, 7113 Three Chopt Rd, Suite 203, Richmond, VA 23226, Assistant Clinical Professor, Department of Physical Therapy, School of Allied Health Professions, Medical College of Virginia, Virginia Commonwealth University, PO Box 224, MCV Station, Richmond, VA 23298-0024, and Adjunct Assistant Clinical Professor, Program in Physical Therapy, Old Dominion University, Norfolk, VA 23508.
Address correspondence to Ms Moran at The Richmond Upper Extremity Center, 7113 Three Chopt Rd, Suite 203, Richmond, VA 23226 (USA).
Physical Therapy/Volume 69, Number 12/December 1989 1007/15 by guest on December 27, 2013http://ptjournal.apta.org/Downloaded from

Joint Capsule
The joint capsule is a fibrous structure composed of irregular, dense connective tissue that accepts stress and permits stretch in all directions of that joint's motion.2 Within the joint capsule is contained the synovial membrane from which synovial fluid is produced for these joints. The joint capsule of all the digital joints displays specific redundancies to accommodate for motion. Wise produced evidence for this configuration by demonstrating significant volar and dorsal redundancies in arthrograms of the digital joints.7 Bojsen-Moller identified a large, thin capsule surrounding the CMC joint of the thumb.8 Kuczynski noted that the joint surfaces could be distracted 3 mm when supporting capsular structures were removed.9
During periods when the hand is immo bilized for surgical or traumatic reasons, the finger joint capsule will adap-tively shorten in the immobilized position, preventing normal motion of the articular surfaces later. This configuration supports the clinical rationale to stress this structure during treatment for improved joint mobility. It would appear that maximal length is necessary for CMC joint rotation or opposition.
Minami et al observed that the dorsal MCP joint capsule provides stability during long-axis distraction and rotatory motions.11 Specifically, the volar capsule of all finger joints is taut in extension, whereas the dorsal capsule is taut in flexion.
Volar Plate
The volar plate is a fibrocartilagous structure that serves as a volar articulating surface, an attachment for ligaments, an additional confining structure for synovial fluid, and an inhibitor of dorsal dislocation during MCP joint extension.1,2,10,11 The volar-plate attachments at the MCP joint are capsular rather than bony, which permits hyper-extension. A similar volar-plate attachment is noted at the DIP joint level. The plate attachments are different at the PIP joint level. Bowers et al identified a bony attachment of the PIP
Fig. 1. Palmar view of dissected hand showing transverse intermetacarpal ligament, which arises from volar plate to attach to adjacent volar plate at level of metacarpal head. (Reprinted with permission from Guyot J, Atlas of Human Limb Joints, New York, NY, Springer-Verlag New York Inc, 1981, p 104.)
joint's volar plate that provides greater joint stability.12 In their analysis of joint ruptures, they observed that the static resistance to hyperextension is offered by the lateral insertion of the volar plate-collateral ligament at the margin of the phalangeal condyle.
Ligaments
There are important extracapsular and capsular ligaments that support and stabilize the hand. The most important extracapsular ligament is the transverse intermetacarpal ligament (TIML) (Fig. 1). It attaches to and courses between volar plates at the level of the metacarpal heads along the entire width of the hand. These structures, the TIML and the metacarpal heads, comprise the distal transverse arch.13 Full extensibility of this ligament is necessary for grasping activities and prehensile activities. Zancolli noted that the extensibility of the TIML between the third and fourth MCP joints and between the fourth and fifth MCP joints is particu
larly important because the fourth and fifth rays descend 5 to 7 mm with respect to the third ray when making a full fist.14 Therefore, if this mobility is restricted because of traumatic scarring or "immobilization tissue shortening," function is greatly hampered.
The capsular collateral ligaments of all finger and thumb joints provide important joint stability. The MCP joint collateral ligaments have been investigated in light of their probable involvement in the pathomechanics of ulnar drift.3 The radial and ulnar MCP joint collateral ligaments are eccentrically placed, which allows for selective tautness and slackness throughout their range of movement (Fig. 2). This placement also promotes the arthoki-nematic motions of roll and slide.1115
The change in ligament length is due to the prominent condylar shoulder that the collateral ligaments must pass over. In addition, Hakstian and Tubi-ana observed that the radial collateral ligament is consistently longer than the ulnar collateral ligament.3 This
16/1008 Physical Therapy/Volume 69, Number 12/December 1989 by guest on December 27, 2013http://ptjournal.apta.org/Downloaded from
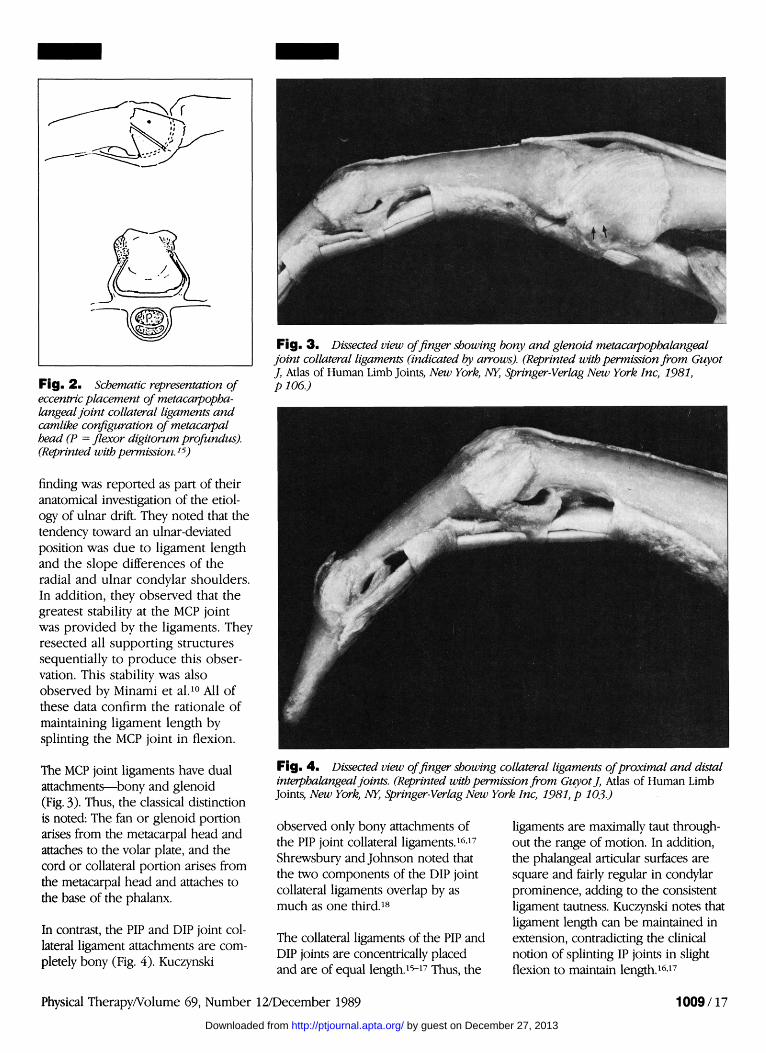
Fig. 2 . Schematic representation of eccentric placement of metacarpophalangeal joint collateral ligaments and camlike configuration of metacarpal head (P = flexor digitorum profundus). (Reprinted with permission.15)
finding was reported as part of their anatomical investigation of the etiology of ulnar drift. They noted that the tendency toward an ulnar-deviated position was due to ligament length and the slope differences of the radial and ulnar condylar shoulders. In addition, they observed that the greatest stability at the MCP joint was provided by the ligaments. They resected all supporting structures sequentially to produce this observation. This stability was also observed by Minami et al.10 All of these data confirm the rationale of maintaining ligament length by splinting the MCP joint in flexion.
The MCP joint ligaments have dual attachments—bony and glenoid (Fig. 3). Thus, the classical distinction is noted: The fan or glenoid portion arises from the metacarpal head and attaches to the volar plate, and the cord or collateral portion arises from the metacarpal head and attaches to the base of the phalanx.
In contrast, the PIP and DIP joint collateral ligament attachments are completely bony (Fig. 4). Kuczynski
Fig. 3 . Dissected view of finger showing bony and glenoid metacarpophalangeal joint collateral ligaments (indicated by arrows). (Reprinted with permission from Guyot J, Atlas of Human Limb Joints, New York, NY, Springer-Verlag New York Inc, 1981, p 106.)
Fig. 4- Dissected view of finger showing collateral ligaments of proximal and distal interphalangeal joints. (Reprinted with permission from Guyot J, Atlas of Human Limb Joints, New York, NY, Springer-Verlag New York Inc, 1981, p 103.)
observed only bony attachments of the PIP joint collateral ligaments.16,17
Shrewsbury and Johnson noted that the two components of the DIP joint collateral ligaments overlap by as much as one third.18
The collateral ligaments of the PIP and DIP joints are concentrically placed and are of equal length.15-17 Thus, the
ligaments are maximally taut throughout the range of motion. In addition, the phalangeal articular surfaces are square and fairly regular in condylar prominence, adding to the consistent ligament tautness. Kuczynski notes that ligament length can be maintained in extension, contradicting the clinical notion of splinting IP joints in slight flexion to maintain length.16,17
Physical Therapy/Volume 69, Number 12/December 1989 1009/17
by guest on December 27, 2013http://ptjournal.apta.org/Downloaded from

The thumb CMC joint displays a unique configuration of ligaments: three capsular, one extracapsular.5,6,8,9
They are the anterior oblique ligament, the dorsoradial ligament, the posterior oblique ligament, and the intermetacarpal ligament (Fig. 5). The capsular ligaments are oblique in orientation, suggesting the maximal support provided by these structures occurs during thumb rotation and pinch-prehensile activities. Pieron methodically recorded the positions that caused maximal span of these oblique ligaments.6 He observed that the dorsoradial position caused maximal span in 3½ of the 4 ligaments (Fig. 6). Therefore, according to his findings, that joint position would be the optimal splinting position to maintain ligament length. Eaton and Littler observed that the anterior oblique ligament provided stabilizing function by stabilizing the volar beak of the first metacarpal.5
The fourth ligament, which is extracapsular, is the intermetacarpal ligament, more commonly known as the "Y" ligament.6,8 This ligament arises from the volar aspect of the trapezium and courses distally between the first and second metacarpals. It then bifurcates and attaches to the bases of those metacarpals. The Y ligament has a tethering function of keeping the first metacarpal on the trapezium.8 This lack of congruency most often happens during thumb abduction and forceful key-pinch activities, and changes in this ligament have notably affected thumb function, particularly in the rheumatoid thumb.
Nerve-Muscle Arrangement
Movements of the hand are accomplished by a combination of intrinsic and extrinsic musculature. Specific kinesiological reviews of muscle function are beyond the scope of this article. The reader is urged to consult other references for this information.19-21
The three peripheral nerves of the upper extremity (radial, median, and ulnar) innervate the intrinsic and
Fig. 5 . Ligaments of thumb carpometacarpal joint: (Top) Anterior view showing anterior oblique ligament (AOL) and intermetacarpal ligament (IML); (Bottom) posterior view showing dorsoradial ligament (DRL) and posterior oblique ligament (POL). (MI = first metacarpal; MII = second metacarpal; td = trapezoid; tm = trapezium; JC = joint capsule; APL = abductor pollicis longus.) (Reprinted with permission.6)
extrinsic muscles of the hand. The forearm musculature are presented in Gardner et al as distinct layers
(Fig. 7).22 This approach aids the clinician in palpation and muscle testing and will be used in this review.
18/1010 Physical Therapy/Volume 69, Number 12/December 1989 by guest on December 27, 2013http://ptjournal.apta.org/Downloaded from

J
L
D
K
I
position of MI
ulno-dorsal
radio-dorsal
radio-volar
ulno-volar
ulnar
area of joint contact
ulno-dorsal quadrant
dorso-radial quadrant
dorso-radial quadrant radio-volar quadrant
ulno-volar quadrant
ulno-volar quadrant
maximal span of ligaments
1. anterior oblique ligament 2. dorso-radial ligament (radial half)
1. anterior oblique ligament 2. dorso-radial ligament (ulnar half) 3. posterior oblique ligament 4. intermetacarpal ligament
1. anterior oblique ligament 2. posterior oblique ligament 3. intermetacarpal ligament
1. dorso-radial ligament 2. anterior oblique ligament
1. dorso-radial ligament 2. anterior oblique ligament
Fig. 6 . Maximal span of carpometacarpal joint ligaments (MI = first metacarpal). (Reprinted with permission.6)
At the volar wrist level, the tendons assume a specific anatomical arrangement (Fig. 8). All volar tendons pass through the carpal tunnel with the exception of the flexor carpi ulnaris tendon as it attaches to the pisiform and the palmaris longus tendon, which passes superficial to the volar carpal ligament. Usually, the palmaris longus tendon lies superficial to the median nerve and, therefore, can be used as a landmark for palpation of the nerve. The volar carpal ligament attaches to the tubercle of the scaphoid and the tubercle of the trapezium radially and to the pisiform and hook of the hamate ulnarly to form the roof of the carpal tunnel. Within the carpal tunnel, passing laterally to medially, are the following structures: flexor carpi radialis (FCR) tendon, flexor pollicis longus (FPL) tendon, median nerve, FDS tendons, and flexor digito-rum profundus (FDP) tendons. The arrangement of the finger flexor tendons as shown in Figure 8 is important to remember when evaluating partial wrist lacerations. In this type of injury, the FCR tendon, median nerve, and some or all of the FDS tendons can be lacerated, leaving the FPL and FDP tendons intact because these tendons lie deep within the carpal tunnel. Clinically, the patient could dis
play inconsistent thumb and finger flexor motions.
The intrinsic muscles are categorically presented as the thenar muscle group, the hypothenar muscle group, and the interosseous muscles. The thenar muscle group is composed of the abductor pollicis brevis, flexor pollicis brevis, opponens pollicis, and adductor pollicis muscles. These muscles are primarily innervated by the motor branch of the median nerve with the exception of the adductor pollicis muscle, which is supplied by the deep motor branch of the ulnar nerve. The hypothenar muscle group is composed of the abductor digiti minimi, flexor digiti minimi, and opponens digiti minimi muscles. The hypothenar muscle group, the three volar interosseous muscles and the four dorsal interosseous muscles, are supplied by the ulnar nerve. The lum-brical muscles, which arise from the FDP tendon of each digit to insert laterally on the extensor hood, are innervated by both median and ulnar nerves. Specifically, the two lateral muscles are innervated by the median nerve, and the two medial muscles are innervated by the ulnar nerve.
The dorsal forearm muscles are innervated by the radial nerve (poste-
Volar musculature Superficial
Pronator teres Flexor carpi radialis Palmaris longus Flexor carpi ulnaris
Middle Flexor digitorum sublimis
Deep Flexor digitorum profundus Flexor pollicis longus Pronator quadratus
Dorsal musculature Superficial
Brachioradialis Extensor carpi radialis longus Extensor carpi radialis brevis Extensor digitorum communis Extensor digiti minimi Extensor carpi ulnaris Anconeus
Deep Supinator Abductor pollicis longus Extensor pollicis brevis Extensor pollicis longus Extensor indicis
Fig. 7 . Volar and dorsal forearm musculature. (Reprinted with permission from Donatelli R, Wooden M (eds), Orthopaedic Physical Therapy New York, NY, Churchill Livingstone Inc, 1989, p211.)
rior interosseous nerve). These muscles are also arranged within two layers in the forearm.
The extensor tendons are contained within six compartments at the level of the wrist (Fig. 9). The first compartment contains the extensor pollicis brevis and abductor pollicis longus tendons. When these tendons develop tenosynovitis from overuse or disease pathology, it is usually described as deQuervain's syndrome. Compartment two contains the extensor carpi radialis longus and extensor carpi radialis brevis tendons. Compartment three contains the extensor pollicis longus tendon. This tendon takes a 45-degree turn at Lister's tubercle to travel distally to the thumb. The extensor digitorum communis and extensor indicis tendons are found within the fourth compartment. Compartment five holds the extensor digiti minimi tendon, and the extensor
Physical Therapy/Volume 69, Number 12/December 1989 1011/19 by guest on December 27, 2013http://ptjournal.apta.org/Downloaded from

carpi ulnaris tendon is contained in compartment six.
The median nerve enters the hand through the carpal tunnel. Motor and sensory nerve fibers pass deep to the volar carpal ligament, and occasionally variation is observed in the routing of the motor branch of the median nerve. This branch, which innervates the thenar muscle groups, may pass deep to or superficial to the volar carpal ligament.23,24
The ulnar nerve enters the hand through the tunnel of Guyon, or Guyon's canal, which is a space formed under the pisohamate ligament.2,23,25 The nerve is subject to variation at this level because it can pass through the tunnel with both sensory and motor components or as the motor branch only. This anatomical variation of the ulnar nerve results in variation of clinical presentation following trauma or transient compression.
Dorsally, the radial nerve is present in the hand via its sensory branch, the superficial radial nerve. The motor branch, the posterior interosseous nerve, innervates the dorsal extrinsic musculature only and does not innervate the intrinsic musculature.
Skin
The most superficial structure of the hand is the skin. It provides a durable covering, which is highly innervated volarly for efficient tactile gnosis.26 The volar surface is endowed with fixed fat pads in addition to numerous eccrine glands, which aid in nonslip grasping. The various lines or creases of the skin follow the normal stresses imposed by the movements of the hand. Extensibility and innervation of the skin are extremely important to ultimate function of the hand.
The hand is innervated volarly by the median and ulnar nerves; dor-sally, it receives innervation from all three nerves. On the volar surface, the thumb and the index and long
fingers are innervated by the median nerve. The ulnar nerve supplies sensation to the ring and little fingers. Because the crossover area of the median and ulnar nerves can include shared innervation of the long and ring fingers, the autonomous zones for the median nerve and the ulnar nerve innervation are the index and little fingers, respectively.2,24,27
Dorsally, the superficial radial nerve supplies the area from the thumb to the long finger from the level of the wrist distal to the PIP joints of the index and long fingers. The area from the PIP joint to the tip is innervated by the median nerve. The ulnar nerve innervates the area from the wrist to the tip of the ring and little fingers on the medial aspect of the dorsal hand.
Fig. 8 . Volar and cross-sectional views of flexor tendons and volar structure at wrist level. In this representation, the flexor retinaculum is labeled the volar carpal ligament. (Reprinted with permission from Lampe EW. Surgical anatomy of the hand. Ciba Clin Symp 21(3)25, 1969.)
20/1012 Physical Therapy/Volume 69, Number 12/December 1989 by guest on December 27, 2013http://ptjournal.apta.org/Downloaded from
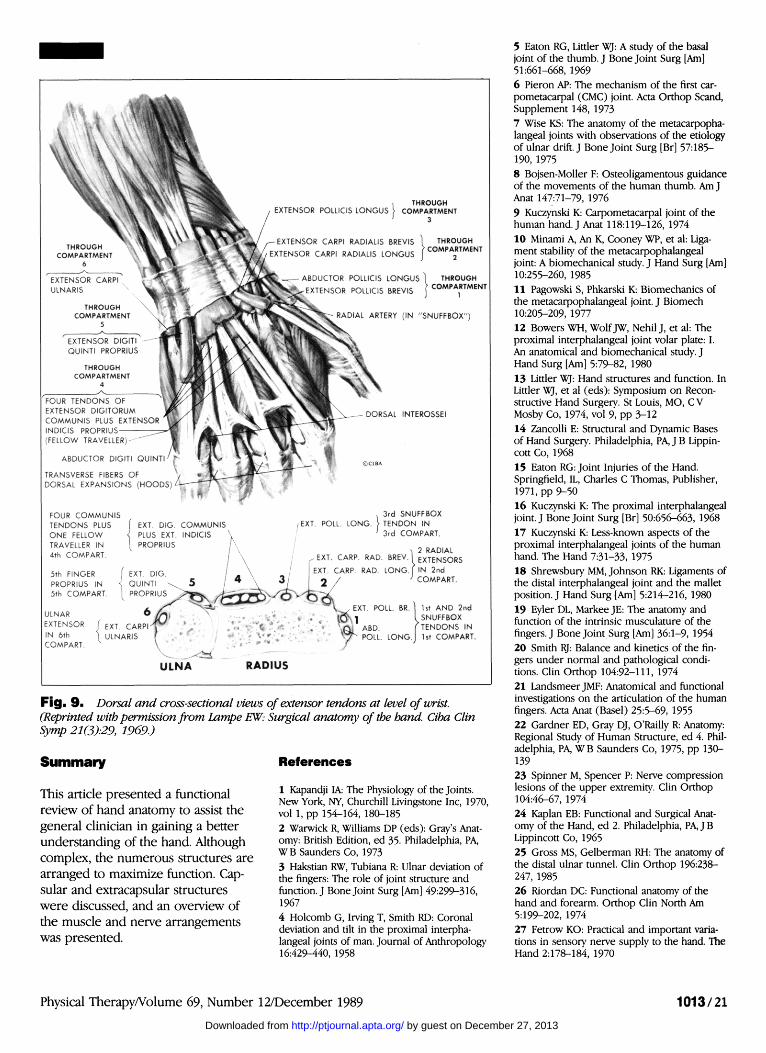
Fig. 9- Dorsal and cross-sectional views of extensor tendons at level of wrist. (Reprinted with permission from Lampe EW: Surgical anatomy of the hand. Ciba Clin Symp 21(3)29, 1969.)
Summary
This article presented a functional review of hand anatomy to assist the general clinician in gaining a better understanding of the hand. Although complex, the numerous structures are arranged to maximize function. Capsular and extracapsular structures were discussed, and an overview of the muscle and nerve arrangements was presented.
References
1 Kapandji IA: The Physiology of the Joints. New York, NY, Churchill Livingstone Inc, 1970, vol 1, pp 154-164, 180-185 2 Warwick R, Williams DP (eds): Gray's Anatomy: British Edition, ed 35. Philadelphia, PA, WB Saunders Co, 1973 3 Hakstian RW, Tubiana R: Ulnar deviation of the fingers: The role of joint structure and function. J Bone Joint Surg [Am] 49:299-316, 1967 4 Holcomb G, Irving T, Smith RD: Coronal deviation and tilt in the proximal interpha-langeal joints of man. Journal of Anthropology 16:429-440, 1958
5 Eaton RG, Littler WJ: A study of the basal joint of the thumb. J Bone Joint Surg [Am] 51:661-668, 1969 6 Pieron AP: The mechanism of the first carpometacarpal (CMC) joint. Acta Orthop Scand, Supplement 148, 1973 7 Wise KS: The anatomy of the metacarpophalangeal joints with observations of the etiology of ulnar drift. J Bone Joint Surg [Br] 57:185-190, 1975 8 Bojsen-Moller F: Osteoligamentous guidance of the movements of the human thumb. Am J Anat 147:71-79, 1976 9 Kuczynski K: Carpometacarpal joint of the human hand. J Anat 118:119-126, 1974 10 Minami A, An K, Cooney WP, et al: Ligament stability of the metacarpophalangeal joint: A biomechanical study. J Hand Surg [Am] 10:255-260, 1985 11 Pagowski S, Phkarski K: Biomechanics of the metacarpophalangeal joint. J Biomech 10:205-209, 1977 12 Bowers WH, Wolf JW, Nehil J, et al: The proximal interphalangeal joint volar plate: I. An anatomical and biomechanical study. J Hand Surg [Am] 5:79-82, 1980 13 Littler WJ: Hand structures and function. In Littler WJ, et al (eds): Symposium on Reconstructive Hand Surgery. St Louis, MO, C V Mosby Co, 1974, vol 9, pp 3-12 14 Zancolli E: Structural and Dynamic Bases of Hand Surgery. Philadelphia, PA, J B Lippin-cott Co, 1968 15 Eaton RG: Joint Injuries of the Hand. Springfield, IL, Charles C Thomas, Publisher, 1971, pp 9-50 16 Kuczynski K: The proximal interphalangeal joint. J Bone Joint Surg [Br] 50:656-663, 1968 17 Kuczynski K: Less-known aspects of the proximal interphalangeal joints of the human hand. The Hand 7:31-33, 1975 18 Shrewsbury MM, Johnson RK: Ligaments of the distal interphalangeal joint and the mallet position. J Hand Surg [Am] 5:214-216, 1980 19 Eyler DL, Markee JE: The anatomy and function of the intrinsic musculature of the fingers. J Bone Joint Surg [Am] 36:1-9, 1954 20 Smith RJ: Balance and kinetics of the fingers under normal and pathological conditions. Clin Orthop 104:92-111, 1974 21 Landsmeer JMF: Anatomical and functional investigations on the articulation of the human fingers. Acta Anat (Basel) 25:5-69, 1955 22 Gardner ED, Gray DJ, O'Railly R: Anatomy: Regional Study of Human Structure, ed 4. Philadelphia, PA, WB Saunders Co, 1975, pp 130-139 23 Spinner M, Spencer P: Nerve compression lesions of the upper extremity. Clin Orthop 104:46-67, 1974 24 Kaplan EB: Functional and Surgical Anatomy of the Hand, ed 2. Philadelphia, PA, JB Lippincott Co, 1965 25 Gross MS, Gelberman RH: The anatomy of the distal ulnar tunnel. Clin Orthop 196:238-247, 1985 26 Riordan DC: Functional anatomy of the hand and forearm. Orthop Clin North Am 5:199-202, 1974 27 Fetrow KO: Practical and important variations in sensory nerve supply to the hand. The Hand 2:178-184, 1970
Physical Therapy/Volume 69, Number 12/December 1989 1013/21 by guest on December 27, 2013http://ptjournal.apta.org/Downloaded from

1989; 69:1007-1013.PHYS THER. Christine A MoranAnatomy of the Hand
Information Subscription http://ptjournal.apta.org/subscriptions/
Permissions and Reprints http://ptjournal.apta.org/site/misc/terms.xhtml
Information for Authors http://ptjournal.apta.org/site/misc/ifora.xhtml
by guest on December 27, 2013http://ptjournal.apta.org/Downloaded from