anatomical variations of internal carotid artery among...
TRANSCRIPT

أ
The National Ribat University
Faculty of Graduate Studies and Scientific Research
Anatomical Variations of Internal Carotid Artery
among Sudanese people
A thesis Submitted in Partial Fulfillment Required for MSc in Clinical
Human Anatomy
By: Yousra ELtereifi Ahmed Kormino
Supervisor: Dr. Kamal Eldin Elbadawi Babiker
2017

I
بسم هللا الرحمن الرحيم
قال تعالى :
) لقد خلقنا االنسان في أحسن تقويم (
صدق هللا العظيم
(4)سورة التين :

II
Acknowledgement
Foremost, I would like to express my sincere gratitude to my
supervisor dr Kamal Eldin Elbadawi Babiker for his continuous support of
my study and research, patience, motivation, enthusiasm, and immense
knowledge. His guidance helped me in all the time of research and writing of
this thesis. I could not have imagined having a better advisor and mentor for
my study.
Besides my supervisor, I would like to thank the rest of my study
committee: Prof Tahir and Dr Yasir, for their encouragement, insightful
comments and hard questions.
My sincere thanks also goes to Dr Hayder, for always being there for
us.
I thank my colleagues, for the stimulating discussions, sleepless nights
we were working together before deadlines, and for all the fun we have had.

III
Dedication
Every challenging work needs self efforts as well as guidance of elders
especially those who were very close to our heart.
My humble effort I dedicate to my sweet, loving and supporting family
(mother, father, husband and little leen), whose affection, love,
encouragement and prays of day and night make me able to get such success .
Along with all hard working and respected professors.
IV
بحثمستخلص ال
:الخلفية
سباتي الداخلي و هما الشريان ال ساسيينأدموية للمخ على شريانين تعتمد التغذية ال
الذي يحدث بين تفرعاتهما )دائرة ويليس(. و التفاغر الشريان القاعدي
:األهداف
السباتي الداخلي لدى ختالفات التشريحية للشريانصممت الدراسة للتعرف على اإل
و نسبة كل منها. السودانيين
:المواد و الطرق
ددوا بالمرضى الذين تر صورة مقطعية محوسبة لألوعية الدموية الخاصة 40تم جمع
2015في الفترة من يناير السودان –بالخرطوم شعه بمستشفى رويال كير العالميهعلى قسم األ
ختالفات التشريحية و جرت دراسة اإل، لشريان السباتي الداخلي ا و التي توضح 2017الى مايو
.ين السوداني لدى للشريان السباتي الداخلي
:النتائج
ختالف تشريحي في الشريان ( لديهم إ%12.5أشخاص ) 5الدراسة أن هناك وجدت
واحدة حيث كانت جميع هذه الحاالت من النوع الذي لم منهم ذكور و أنثى 4داخلي؛ السباتي ال
( حاالت في الجهة اليمنى و حالة واحدة %10) 4يتكون فيه الشريان السباتي الداخلي و كانت
%( في الجهة اليسرى.2.5)
:المناقشة
الشريان السباتي الداخلي لدى ختالفات كثيرة في ال توجد إ مقارنة بالدراسات السابقة
5 في ذو نسبة كبيرة فقطو ما وجد لم يكن ختالفات إل, حيث لم تجد الدراسة كل انواع ادانيينالسو
%.12.5تمثل نسبة حاالت
:الخالصة
و ضئيلة لدى السودانيين يان السباتي الداخلي ختالفات تشريحية في الشرإن نسبة وجود إ
.نها تكون عديمة االعراض و تكتشف بالصدفةإن وجدت فإ

V
Abstract
Background:
The anatomical variations of the internal carotid artery may be a major
causes or contributing factors to many diseases due to its critical place of
supply and should be known to avoid and reduce the complications during
the invasive procedures. Sometimes these variations pass undiscovered and
just found on routine examination.
Objective:
To study the anatomical variations of internal carotid artery among
Sudanese.
Materials and methods:
40 (12 MRA, 28 CTA) images of subjects who were attended to the
Radiology Department at Royal Care International Hospital in Khartoum _
Sudan. The internal carotid artery was assesed for any anatomical variant.
Results:
The study found that only 5 subjects (12.5%) had anatomical variation
of agenesis type, 4 of them were males and 1 female.
Disscusion:
The anatomical variation of the ICA is uncommon and discovered
accidentally, as revealed by this study.
Conclusion:
Knowing the normal anatomy and the normal variations of the ICA is
so important for the clinicians and neurosurgeons in their practice to avoid
damage and massive bleeding during surgeries.

VI
List of abbreviations
ACA Anterior cerebral artery
CCA Common carotid artery
CRM Carotid rete mirabile
CT Computed tomography
CTA Computed tomography angiogram
ECA External carotid artery
ICA Internal carotid artery
ICAA Internal carotid artery agenesis
Lt Left
MRA Magnetic resonance angiogram
PCA Posterior carotid artery
Rt Right
3rd Third

VII
List of figures
Fig Title Page
4.1 Gender distribution 11
4.2 Age distribution 12
4.3 Abnormality type distribution 13
4.4 Right side agenesis of the ICA 14
4.5 Abnormality side distribution 15
4.6 Main collateral circulation distribution 16
4.7 Relation between gender and abnormality
type
17
4.8 Relation between abnormality type and side 18

VIII
List of tables
Table Title Page
4.1 Gender distribution 11
4.2 Age distribution 12
4.3 Abnormality type distribution 13
4.4 Abnormality side distribution 15
4.5 Main collateral circulation distribution 16
4.6 Relation between gender and abnormality
type
17
4.7 Relation between abnormality type and
side
18

IX
The contents
Title Page
Alayah I
Acknowledgment II
Dedication III
Abstract in Arabic IV
Abstract in English V
List of abbreviations VI
List of figures VII
List of tables VIII
The contents IX
Chapter One: Introduction and Objectives
1.1 Introduction 1
1.2 Justification 2
1.3 Objectives 2
1.3.1 General objective 2
1.3.2 Specific objectives 2
Chapter Two: Literature Review
2.1 Gross Anatomy 3
2.1.1 development of ICA 3
2.1.2 Course of ICA 3
2.1.3 Relations 4
2.1.4 Carotid sheath 4
2.1.5 Segments 5
2.1.6 Branches 6
2.2 Clinical considerations 6
2.3 Previous studies 6
Chapter Three: Materials and Methods
3.1 Study Design 9
3.2 Study Area 9
3.3 Study Duration 9
3.4 Study Population 9
3.4.1 Inclusion Criteria 9
3.4.2 Exclusion Criteria 9
3.5 Variables 9
3.6 Sampling 9
3.6.1 Sample type 9
3.6.2 Sample size 9
3.7 Data collection 10
3.7.1 Data collection tools 10

X
3.7.2 Data analysis 10
3.8 Data management 10
3.9 Ethical consideration 10
Chapter Four: Results
4.1 Results 11
Chapter Five: Discussion
5.1 Discussion 19
Chapter Six: Conclusion and Recommendations
6.1 Conclusion 20
6.2 Recommendations 21
Chapter Seven: References
7.1 References 22
Annex: Data Collection Sheet
Data collection sheet 24

Chapter One
Introduction and Objectives
1
1. Introduction and objectives
1.1 Introduction:
The internal carotid artery arise at the bifurcation of the common
carotid arteries at the level of the upper border of the lamina of the thyroid
cartilage ( upper border of C4 vertebra) or at higher level near the tip of the
greater horn of the hyoid bone (C3 vertebra).(1)
The internal carotid artery along with the vertebral system supply the
cerebral hemispheres and the wall of the diencephalon, they anastomose with
each other around the optic chiasma and infundibulum of the pituitary stalk
forming the arterial circle of Willis.(2)
This circle is formed in the following way; the basilar artery from the
vertebral system ,divides at the upper border of the pons into the right and left
posterior cerebral arteries, each one receives a small posterior communicating
artery that runs backwards through the interpeduncular cistern from the
internal carotid artery at the anterior perforated substance on the same side.
Each internal carotid artery gives off an anterior cerebral artery; the circle of
Willis is completed by the anterior communicating artery, a small vessel that
unites the anterior cerebrals in the chiasmatic cistern, below the rostrum of the
corpus callosum.(2)
Because of the importance of the places where they supply blood, the
variations of the internal carotid arteries should be known to avoid and reduce
the complications during the invasive procedures, these anatomical variations
include its origin, course, branches and even presence or absence of the artery
itself.
Therefore the aim of this study is to evaluate the incidence of these
anatomical variations of the internal carotid artery.
2
1.2 Justification:
The normal blood flow to the brain is important to keep its normal
functions, and this is maintained by the fluent blood flow within the arteries
and their anastomoses.
Any disturbance to this may lead to serious lesions and dysfunction to
that part of the brain supplied by the affected artery. This may be either due to
anatomic variations or a disease. No previous studies conducted in Sudan
concerning this topic.
1.3 Objectives:
1.3.1 General objective:
To study the anatomical variations of the internal carotid artery
among Sudanese population.
1.3.2 Specific objectives:
• To determine the presence of the anatomical variation of ICA.
• To determine the incidence of each anatomical variation of ICA.
• To determine the association between gender and each anatomical
variant of ICA.

Chapter Two
Literature Review

3
2. Literature review
2.1 Gross anatomy:
The ICA begins at the bifurcation of the common carotid artery at the
level of the upper border of the thyroid cartilage. It supplies the brain, the eye,
the forehead, and part of the nose. The artery ascends in the neck passing
through the carotid sheath with the internal jugular vein and vagus nerve. At
first it lies superficially; it then passes deep to the parotid salivary gland.(3)
The ICA leaves the neck by passing into the cranial cavity through the
carotid canal in the petrous part of the temporal bone. It then passes upward
and forward in the cavernous venous sinus (without communicating with it).
The artery then leaves the sinus and passes upward again medial to the
anterior clinoid process of the sphenoid bone. The ICA then inclines
backward, lateral to the optic chiasma, and terminates by dividing into the
anterior and the middle cerebral arteries.(3)
2.1.1 Development of ICA:
The ICA arises from the third arch artery and the dorsal aorta. These
two components unite, with a proximal process from the capillary network
that exists in the walls of the forebrain and midbrain. This union forms a
primitive ICA that is identified approximately by the fourth week. (12)
2.1.2 Course of ICA:
In the neck the ICA is lateral to the external carotid at its origin, but soon
passes up posteriorly to a medial and deeper level. It has no branches and
passes straight up in the carotid sheath, beside the pharynx to the carotid canal
in the base of the skull.(4)

4
In the skull The ICA curves upwards from the foramen lacerum to enter
the posterior part of the sinus and runs forwards within the sinus, deeply
grooving the body of the sphenoid and the base of its greater wing. The artery
then curves upwards again to pierce the roof of the sinus, medial to the
anterior clinoid process, and turns backwards. The artery is accompanied by a
plexus of postganglionic sympathetic fibres from the superior cervical
ganglion.(5)
The ICA emerges from the roof of the cavernous sinus medial to the
anterior clinoid process and curves immediately backwards, lying on the roof
of the sinus before curving upwards lateral to the optic chiasma. At the
anterior perforated substance it divides into its terminal branches. The curve
of the internal carotid artery in and above the cavernous sinus as seen in a
lateral carotid arteriogram (like a U on its side, opening backwards) is
commonly called the carotid siphon.(6)
2.1.3 Relations:
The ICA has very important relations, in the neck; anterolaterally:
below the digastric, lie the skin, the fascia, the anterior border of the
sternocleidomastoid, and the hypoglossal nerve. Above the digastric lie the
stylohyoid muscle, the stylopharyngeus muscle, the glossopharyngeal nerve,
the pharyngeal branch of the vagus, the parotid gland, and the external carotid
artery; posteriorly: the sympathetic trunk, the longus capitis muscle, and the
transverse processes of the upper three cervical vertebrae; medially: the
pharyngeal wall and the superior laryngeal nerve; laterally: the internal
jugular vein and the vagus nerve.(3)
2.1.4 Carotid sheath:
This is not a fascia in the sense of a demonstrable membranous layer,
but consists of a feltwork of areolar tissue that surrounds the common and

5
internal carotid arteries, internal jugular vein, vagus nerve and some deep
cervical lymph nodes. It is thin where it overlies the internal jugular vein,
allowing the vein to dilate during increased blood flow. The sheath is attached
to the base of the skull at the margins of the carotid canal and jugular fossa,
and is continued downwards along the vessels to blend with the adventitia of
the aortic arch. In front the lower part of the sheath fuses with the fascia on
the deep surface of the sternocleidomastoid. Where they lie alongside, the
sheath blends with the pretracheal fascia. Behind the carotid sheath there is a
minimum of loose areolar tissue between it and the prevertebral fascia; the
cervical sympathetic trunk lies here in front of the prevertebral fascia.(7)
2.1.5 Segments:
There are several classification systems of the ICA, the most recent of
which was described by Bouthillier et al in 1996. Their classification system
is used clinically by neurosurgeons, neuroradiologists and neurologists and
relies on the angiographic appearance of the vessel and histological
comparison rather than on the embryonic development, there are seven
segments of ICA described by Bouthillier classification: C1 cervical
segment, which extends from the carotid bifurcation to the skull base; C2
petrous segment,which courses through petrous temporal bone I the carotid
canal; C3 lacerum segment, which together with C2 comprise the petrous
portion; C4 cavernous segment,which ends at the roof of the cavernous sinus
(proximal dural ring); C5 clinoid segment, which lies beneath the anterior
clinoidal process and between the proximal and distal dural rings; C6
ophthalmic segment, which is the first subarachnoid segment; C7
communicating segment, C6 and C7 comprise the intradural or supraclinoidal
portion.(8)

6
2.1.6 Branches:
Except for the terminal segment (C7) the odd numbered segments
usually have no branches, whereas the even numbered segments (C2, C4, C6)
each have two branches; C1: none; C2: caroticotympanic and vidian arteries;
C3: none; C4: meningohypophyseal and inferolateral trunks; C5: none; C6:
ophthalmic and superior hypophyseal arteries; C7: posterior communicating,
anterior choroidal, anterior cerebral, middle cerebral arteries. (9)
2.2 Clinical considerations:
Congenital anomaly of the carotid artery is a rare abnormality. It is
usually discovered incidentally by color Doppler carotid sonography,
angiography CT or MRI of the head and neck taken for some other reasons.
Most patients are not symptomatic because of sufficient cerebral circulation
supplied to the defective area by the communicating arteries of the circle of
Willis, intercavernous anastomoses, communicating arteries from external
carotid artery and by persistent embryologic arteries to the carotid artery
territory. However, sometimes, this anatomic variation may eventually lead to
some clinical signs and symptoms in particular circumstances in the head and
neck of which surgeons are unaware.These variations include congenital
absence; hypoplasia; rete mirabele; retropharyngeal; agenesis.
2.3 Previous studies:
In a study done by Tasar M, et al which studied five thousand one
hundred cerebral MRI and/or catheter angiograms performed between
February 1988 and March 2002, were reviewed for carotid artery abnormality,
and the results were seven (0.13%) patients with congenital absence or
hypoplasia ;4 (0.07%) of these patients were presented with hypoplasia of
ICA, 3 (0.05%) with absence of ICA were identified. The radiologic and

7
clinical study of 5 patients with unilateral (3 of these patients were presented
with hypoplasia and 2 with absence of ICA) and 2 patients with bilateral (one
was presented with absence of ICA, whereas the other was hypoplastic). The
congenital abnormality with absence or hypoplasia of ICA demonstrated that
those patients were asymptomatic and diagnosed incidentally.(10)
In another study done by Tode in which he reported the first case of
ICA agenesis in 1787, which was accidentally encountered after a cadaveric
dissection. The prevalence of congenital absence of ICA was estimated as
0.01%. The prevalence of absence of ICA was 0.058% and that of hypoplasia
of ICA was 0.079% in his series. Unilateral absence or hypoplasia of ICA
was more frequent on the left and bilateral absence or hypoplasia were more
exceptional and reported to be less than 10% of unilateral involvement.(10)
In a study done by Fuwa I, he found that the carotid rete mirabile
(CRM) was a very rare pathological condition; only six cases have been
reported in the English and Japanese literature. All previously reported case
subjects were adults with an age of 39 years. To his knowledge, this was the
first patient who presented with symptoms of CRM in childhood. CRM is a
physiological network between the external carotid and internal carotid
systems in lower mammals. Very rarely, these arterial channels were observed
in humans.(11)
Another study done by Lee et al in 1992, reviewed nine patients with
ICA aplasia. Of these, three patients had subarachnoid hemorrhages as the
presenting syndrome, three others had ischemic syndromes, one presented
with recurrent headache, and two were incidentally diagnosed by
angiography.(12)
Also in a study done by Handa et al, in 1980, they reported a case of
unilateral ICA agenesis in a 52-year-old female that presented with a
subarachnoid hemorrhage.(12)

8
A case reported by Mousa A Y and A F Aburahma, outlined an
unusual anatomic variant which was a retropharyngeal ICA and raised certain
considerations among clinicians during perioperative planning.(13)
Although the majority of retropharyngeal carotids are asymptomatic,
when symptoms occur, different presentations may be encountered, such as
submucosal pulsating masses in the posterior pharyngeal wall. It is also
important to recognize other possible presentations of this rare anomaly, such
as dysphagia, cervical bolus sensation, and even glossopharyngeal neuralgia.
In addition, extreme degrees of medialization of the carotid arteries may result
in progressive symptoms, including hoarseness and upper respiratory distress,
and the risk of the spread of infection in the oropharyngeal area. Erosion of
the oropharyngeal mucosa, perhaps from a nasogastric tube or during
tonsillectomy with or without adenoidectomy, may precipitate bleeding.(13)
A case study by Fons C et al, reported a 7-year old boy with right
miosis, mild blepharoptosis and iris hypopigmentation detected in a
routine pediatric follow-up without ipsilateral facial anhydrosis, flushing
or pain. There was no history of birth trauma and test with cocaine
provoked, no response of the right pupil, suggesting right Horner’s
syndrome. Mediastinal tumor was ruled out and brain MRI incidentally
showed absence of flow in the right internal carotid artery. Subsequent
MRA demonstrated agenesis of the right internal carotid artery without
other vascular - associated malformations. The final diagnosis was right
congenital Horner’s syndrome due to ipsilateral internal carotid agenesis.
(14)

Chapter Three
Materials and Methods
9
3. Materials and Methods
3.1 Study design:
This is an observational descriptive cross-sectional study.
3.2 Study area:
The study was conducted at Royal Care International Hospital,
Department of Radiology, Khartoum state, Sudan.
3.3 Study duration:
The study was held during the period between (Jan 2015 _ May 2017).
3.4 Study population:
All individuals underwent CTA or MRA for ICA in Khartoum state
(Royal Care International Hospital, Radiology Department).
3.4.1 Inclusion Criteria:
All individuals underwent CTA or MRA for ICA in Khartoum state
(Royal care international hospital) with normal ICA.
3.4.2 Exclusion criteria:
All patients with history of ICA (occlusion or stenosis).
3.5 Study variables:
Age, gender, abnormality type of ICA, abnormality side of ICA.
3.6 Sampling:
3.6.1 Sample type:
The sample group of this study was selected randomly among Sudanese
population.
3.6.2 Sample size:
40 subjects (28 CTA and 12 MRA).
3.7 Data collection:
3.7.1 Data collection tools:
Data collected was CTA and MRA by data collection sheet.

10
3.7.2 Data analysis:
Data analyzed by SPSS (Social Package for Statically Science), version
24, 2016.
3.8 Data management:
Data was analyzed as mentioned above and then it was presented and
described by using the pie, tables, charts and figures.
3.9 Ethical consideration:
• Confidentiality of name or personal data was considered.
• Approval statement was considered from institutional authorities.
• Ethical Committee approval was taken.

Chapter Four
Results

11
4. Results
A total of 40 individuals were examined, 29 of them underwent CTA and
11 underwent MRA, twenty-four of them were males (60%) and sixteen
(40%) were females. As shown in Table (4.1) and fig (4.1).
Table (4.1): Distribution of gender.
Gender Frequency Percent
Male 24 60%
Female 16 40%
Total 40 100%
Fig (4.1): Represents gender distribution.
0%
10%
20%
30%
40%
50%
60%
70%
Male Female
60%
40%
Gender
Per
cen
tage

12
The age of subjects was arranged into seven groups ranged from (0
_>70) yrs, as shown in table (4.2) and fig (4.2).
Table (4.2): Age group distribution among individuals.
Age group/yrs Frequency Percent
0 - 20 4 10%
21 - 30 4 10%
31 - 40 5 12.5%
41 - 50 9 22.5%
51 - 60 7 17.5%
61 - 70 6 15%
> 71 5 12.5 %
Total 40 100%
Fig (4.2): Represents age distribution.
0%
5%
10%
15%
20%
25%
20-0 30-21 40-31 50-41 60-51 <71
10% 10%12.50%
22.50%
17.50%
12.50%
Age groups
Per
cen
tage

13
The study found that 5 (12.5%) individuals had agenesis type, while the
remaining 35(87.5%) individuals were normal, as shown in table (4.3) and fig
(4.3, 4.4).
Table (4.3): Abnormality type distribution.
Abnormality type Frequency Percent
Hypoplastic 0 0%
Agenesis 5 12.5%
None 35 87.5%
Total 40 100%
Fig (4.3): Represents abnormality type distribution.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Hypoplasia Agenesis None
0
12.5%
87.5%
Per
cen
tage
Abnormality type of ICA

14
Fig (4.4): MRA image shows the right side agenesis of the ICA (the arrow
shows the left side ICA).
The abnormality was found in 4 (10%) cases in the right side, 1 (2.5%)
case in the left side, while the remaining 35(87.5%) cases were normal, as
shown in table (4.4) and fig (4.5).

15
Table (4.4): Shows the abnormality side distribution
Abnormality side Frequency Percent
Right 4 10%
left 1 2.5%
None 35 87.5%
Total 40 100%
Fig (4.5): Shows the abnormality side distribution
Concerning the main collateral circulation the study showed that 2
(5%) of the cases originated from the ACA, while 3 (7.5%) cases from
the PCA and the remaining subjects were normal, as shown in table (4.5)
and fig (4.6).
10%2.5%
87.5%
Right
Left
None
Abnormality side of ICA

16
Table (4.5): Shows the main collateral circulation distribution
Main collateral circulation Frequency Percent
ACA 2 5%
PCA 3 7.5%
Fetal type 0 0%
Adult type 0 0%
Third type 0 0%
None 35 87.5%
Total 40 100%
Fig (4.6): Shows the main collateral circulation distribution
In comparing the abnormality type with the gender, the study revealed
that the agenesis type was found in 1 (2.5%) female and 4 (10%) males
while the hypoplastic type wasn't found in any case; as shown in table
(4.6) and fig (4.7).
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
ACA PCA Fetal type Adult type Third type None
5% 7.5%0% 0% 0%
87.5%
Collateral circulation of ICA
per
cen
tage

17
Table (4.6): Shows the relation between the gender and abnormality
type
Fig (4.7): Shows the relation between gender and abnormality type.
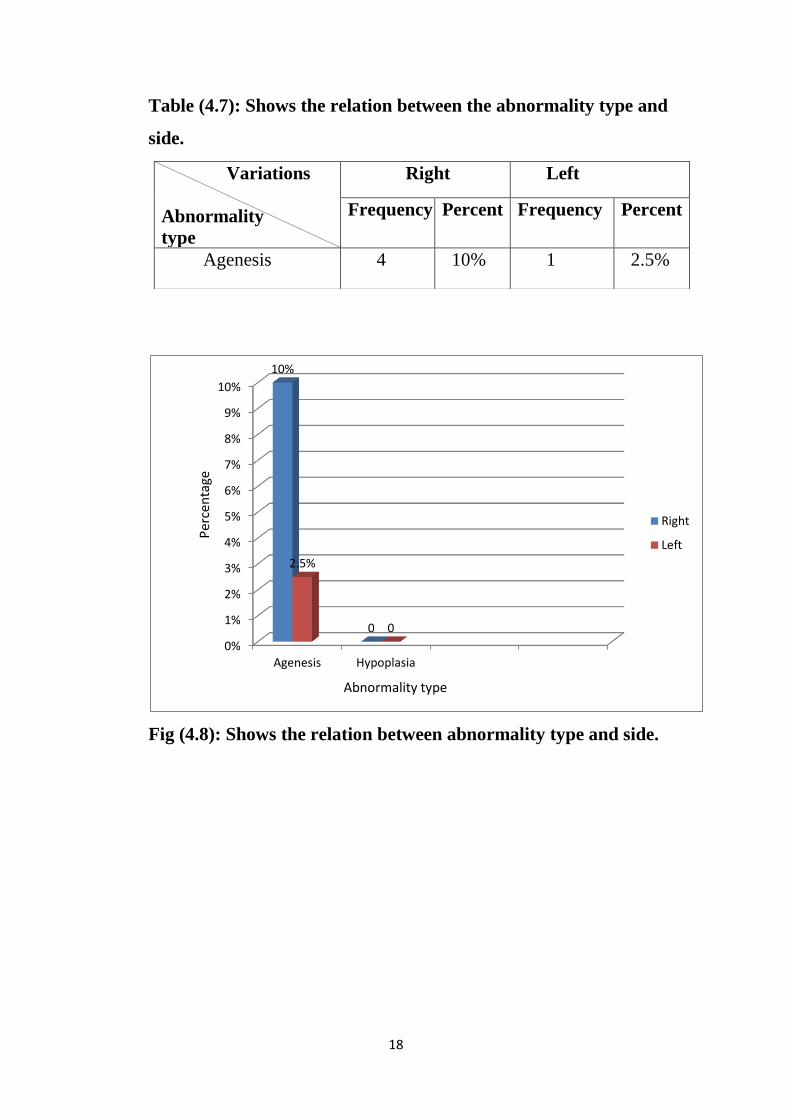
In comparing between the abnormality type and the abnormality side it
was observed that 4 (10%) cases were in the right side and 1 (2.5%) case was
in the left side; as shown in table (4.7) and fig (4.8).
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Agenesis Hypoplasia
10%
0%2.5% 0%
Males
Females
Abnormality type
Per
cen
tage
Variations
Gender
Agenesis Hypoplasia
Frequency Percent Frequency Percent
Male 4 10% 0 0%
Female 1 2.5% 0 0%
18
Table (4.7): Shows the relation between the abnormality type and
side.
Fig (4.8): Shows the relation between abnormality type and side.
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
Agenesis Hypoplasia
10%
0
2.5%
0
Right
Left
Abnormality type
Per
cen
tage
Variations
Abnormality
type
Right Left
Frequency Percent Frequency Percent
Agenesis 4 10% 1 2.5%

Chapter Five
Discussion

19
5. Discussion
The present study focused on two main types of the anatomical
variations of the ICA; agenesis and hypoplasia.
Among the 40 cases studied, there were only 5 (12.5%) cases were
found to have an anatomical variant; the agenesis type, which was distributed
as follows: 4 (10%) cases in the right side and 1 (2.5%) case on the left side
which disagree with what mentioned in the literature in the study done by
Luis F. Gonzalez-Cuyar.
As observed in this study, 4 (10%) cases were males and 1 (2.5%) case
was female which agree with what mentioned by Mustafa Tasar.
These 5 cases were found in different age groups; one of them was
found in a 6 yrs old child, which agree with a case reported in the literature by
Fons et al, i.e it should be expected in any age.
All the cases found in this study encountered unilateral agenesis of
ICA with a rate of 12.5% in contrast with what mentioned in the literature by
Fons et al, who reported a rate of 0.36%. All these cases were asymptomatic
and discovered incidentally as mentioned in the literature by Mustafa Tasar.
The hypoplastic type wasn't found in any case under the study (0%)
which coincide with what mentioned in literature as it is a rare congenital
anomaly.
In comparing this study with previous studies done in other countries,
the results obtained here are almost of the same value; in the study done by
Tasar M, et al the congenital absence or agenesis of the ICA in the subjects
under study were asymptomatic and discovered incidentally, because they got
their blood supply from the developed collateral circulations as mentioned in
the literature by Mustafa Tasar.

20
The main collateral circulation of 2 (5%) cases is from the ACA, while
3 (7.5%) cases from the PCA and the remaining cases were normal which
agree with the study done by Tasar M.
The other types of collateral circulation (fetal, adult and third types)
were not found in the present study.
Chapter Six
Conclusions and Recommendations

21
6. Conclusions and Recommendations
6.1 Conclusions:
This study showed that the anatomical variations of the ICA were
present in some cases but not as common as anywhere else and to be
considered in mind while performing any surgery involving this area, and to
be kept in mind that these cases were discovered incidentally.
The study stated that the more common anatomical variant of the ICA
in the Sudanese subjects was the agenesis type.
Also the study concluded that the agenesis type of congenital anomaly
was common in males, and was found in the right side than the left one.
The study remarks that the collateral circulation usually originates from
the PCA, then followed by the ACA.
The subjects were of different age groups; one of them was 6 yrs old
child, so it means that it is not related to specific age.

22
6.2 Recommendations:
The study recommends the followings:-
• All surgical procedures involving the area of the ICA must be preceded
by CTA or MRA.
• The neurosurgeons and neurologists should know about these
anatomical variations of the ICA.
• Another study should be done in the future to shed more light on the
anatomical variations of the ICA by studying a large number of cases.

Chapter Seven
References

23
7. References
1-Chummy S Sinnatamby. Head and Neck and Spine. In: Chummy S
Sinnatamby (ed). Last's anatomy 12th edition. Edinburgh: Churchill
Livingstone Elsevier; 2011; p.342.
2-Chummy S Sinnatamby. Central nervous system. In: Chummy S
Sinnatamby (ed). Last's anatomy12th edition . Edinburgh: Churchill
Livingstone Elsevier; 2011; p.471.
3-Richard S. Snell. Head and Neck. In: Richard S Snell (ed). Clinical anatomy
by regions 8th edition. Philadelphia. Lippincott; 2008; p.750.
4-Chummy S Sinnatamby. Head and Neck and Spine. In: Chummy S
Sinnatamby (ed). Last's anatomy 12th edition. Edinburgh: Churchill
Livingstone Elsevier; 2011; p.343.
5-Chummy S Sinnatamby. Head and Neck and Spine. In: Chummy S
Sinnatamby (ed). Last's anatomy 12th edition. Edinburgh: Churchill
Livingstone Elsevier; 2011; p.447.
6-Chummy S Sinnatamby. Head and Neck and Spine. In: Chummy S
Sinnatamby (ed). Last's anatomy 12th edition. Edinburgh: Churchill
Livingstone Elsevier; 2011; p.449.
7-Chummy S Sinnatamby. Head and Neck and Spine. In: Chummy S
Sinnatamby (ed). Last's anatomy 12th edition. Edinburgh: Churchill
Livingstone Elsevier; 2011.
8-Segments of the ICA were found in: http//rhoton.ineurodb.org/?page=22507
9-Branches of the ICA were found in:
http://radiopaedia.org/articles/internal-carotid-artery-1
10-Tasar M, et al. Congenital absence or hypoplasia of the carotid artery:
radioclinical issues. Am J Otolaryngol, 2004; 25 (5): p. 339-49.
11-Fuwa I. A pediatric case of carotid rete mirabile. Stroke, 1994; 25 (6): p.
1268-70.
12-Gonzalez-Cuyar LF, et al. Bilateral internal carotid absence: a case report
of a rare congenital anomaly. Cardiovasc Pathol, 2008; 17 (2): p. 113-6.

24
13-Mousa AY and AF AbuRahma. Retropharyngeal internal carotid artery: a
rare presentation with significant clinical implications. Ann Vasc Surg, 2013;
27 (8): p. 1189.
14-Fons C, et al. Agenesis of internal carotid artery in a child with ipsilateral
Horner's syndrome. J Child Neurol, 2009; 24 (1): p. 101-4.

25
The National Ribat University
Faculty of Graduate Studies and Scientific Research
Anatomical Variation of Internal Carotid Artery among
Sudanese people attending to the Radiology Department, Royal
Care International Hospital, Khartoum Sudan
Data collection sheet
Index number
Name …………………………………………………………………
Age......................years
Sex Male Female
Abnormality side: Rt Lt
Abnormality type : Hypoplastic Agenesis
Main collateral circulation: ACA PCA Fetal type
Adult Third type
Associated abnormality:
…………………………………………………...................................
…………………………………………………………………………
Symptoms (main features):
…………………………………………………………………………
Note:
…………………………………………………………………………