analgesics & antibiotics in pediatric dentistry
DESCRIPTION
goodTRANSCRIPT

ANALGESICS & ANTIBIOTICS IN PEDIATRIC DENTISTRY
Dr.G.ThiruvenkadamPost graduate
Dept of Pedodontics & Preventive Dentistry
ANTIBIOTICS
The desire to take Medicine is perhaps the greatest feature,
Which distinguishes Man from Animals
- Sir William Osler
Synopsis
• Antibiotics in dentistry– Introduction– Definitions– Guidelines – Principles– Drug dosage calculations– Classifications– Indications– Commonly used antibiotics– Antibiotic prophylaxis

Introduction • Antibiotics are chemical substances that suppress the
growth of other microorganisms and may eventually destroy them.
• The purpose of antibiotic and antimicrobial chemotherapy is to aid the host defences in controlling and eliminating microbes that temporarily have overwhelmed the protective host mechanisms
• They play an essential role in the management of odontogenic infections as it can shorten the period of infection and minimize the associated risks.
Definitions • Antibiotics– The term antibiotic was first used in 1942 by Selman
Waksman and his collaborators to describe any substance produced by a microorganism that is antagonistic to the growth of other microorganisms in high dilution
– Antibiotics may be informally defined as the subgroup of anti-infectives that are derived from bacterial sources and are used to treat bacterial infections.
• Antimicrobials– They are synthetically derived agents which act against the
microbes, by killing the organisms or suppressing their growth.

Guidelines On Use Of Antibiotic Therapy For Pediatric Dental Patients• Conservative use of antibiotics is indicated to minimize the
risk of developing resistance to current antibiotic regimens.• Factors related to host risk (age, systemic illness,
malnutrition) and type of wound (laceration, puncture) must be evaluated when determining the risk of infection and subsequent need for antibiotics.
• The minimal duration of drug therapy should be limited to 5 days beyond the point of substantial improvement or resolution of signs and symptoms.
• The importance of completing a full course of antibiotic must be emphasized, if not the surviving bacteria can restart an infection that may be resistant to the original antibiotic.

Guidelines On Use Of Antibiotic Therapy For Pediatric Dental Patients
• Pulpitis/Apical periodontitis/Draining sinus– Antibiotic therapy usually is not indicated if the dental infection is
contained within the pulpal tissue or the immediately surrounding tissue, without any systemic signs
• Acute facial swelling of dental origin– Depending on clinical findings, treatment may be
• Treating/extracting the tooth with antibiotic coverage• Prescribing antibiotics to contain the spread of infection and then treating the
involving tooth
• Dental trauma– Local application of an antibiotic to the root surface of an avulsed tooth
with an open apex and less than 60 minutes extraoral dry time has been recommended to inhibit external resorption and aid in pulpal revascularization
– Systemic antibiotics have been recommended as an adjuctive therapy for avulsed permanent incisors with an open or closed apex.

Guidelines On Use Of Antibiotic Therapy For Pediatric Dental Patients• Pediatric periodontal diseases– In pediatric periodontal diseases like Neutropenias,
Papillon LeFevre syndrome and leukocyte adhesion deficiency, the immune system is unable to control the growth of periodontal pathogens, so treatment may involve antibiotic therapy.
• Viral diseases– Conditions such as Acute Primary Herpetic
Gingivostomatitis should not be treated with antibiotic therapy unless there is secondary bacterial infection.

Certain principles ….• When possible, identify the etiologic agent prior to prescribing antibiotics• Use local susceptibility patterns to help direct empirical treatment• Once aetiology and susceptibility are known, change regimen to narrowest
effective spectrum• Combination therapy is usually not indicated, but for certain purposes like
– To prevent emergence of resistance– For synergistic activity– Therapy against multiple potential pathogens
• Choose a therapeutic agent based on– Pharmacologic data– Adverse drug reaction profile– Site of infection– Host immune status– Evidence of efficacy in clinical trials
• Check for drug interactions and contraindications before prescribing antibiotics

Drug dosage calculations• Young Formula
– Dose= {Age/ (age + 12)} x adult dose
• Clarke Formula– Dose= (Weight in kg/70) x adult dose
or– Dose=(Weight in lbs/150) x adult dose
• Dilling Formula– Dose= (Age/20) x adult dose
• Fried’s Formula– Dose=(Age in Months/150) x adult dose
• Based on body surface area– Dose=BSA(m2)/1.7 x adult dose
• Augsberger’s Formula– (1.5 x Wt(Kg) + 10) x adult dose
A new easy rule………• Salisbury rule for calculating dosage for children– Less than 30 kg :Weight x 2 (% of adult dose)– More than 30 kg :Weight +30 (% of adult dose)
• For example– Weight of the child = 20 kg– Adult dose = 500 mg– Child dose = (20 x 2) % of adult dose
= 40 % of adult dose
= 200 mg– If weight of the child = 35 kg– Adult dose = 500 mg– Child dose = (35+30) % of adult dose
= 65 % of adult dose
= 325 mg

Classification • Based on chemical structure
– Ex: sulfonamides, quinolones, β-lactams, macrolides, nitroimidazoles etc
• Based on mechanism of action– Inhibit cell wall synthesis– Inhibit protein synthesis– Inhibit DNA gyrase ex. Cipro– Interfere DNA function ex. Rifampin, metronidazole– Interfere DNA synthesis ex. Acyclovir, Zidovudine
• Based on spectrum of Activity– Narrow spectrum– Broad spectrum
• Type of Action– Primarily bacteriostatic– Primarily bactericidal

Classification • Based on antibiotics source– Fungi penicillin, cephalosporin– Bacteria polymyxin B, colistin– Actinomycetes aminoglycosides, tetracyclines– Chemicals
• Based on organism susceptible– Active against Gram +ve bacteria– Active against Gram – ve bacteria– Active against bith Gram + and – ve bacteria– Active against acid fast bacilli.

Indications for antibiotics
Therapeutic •In Patients where host resistance is decreased by diseases•Acute severe rapidly spreading infection•Pericoronitis•Osteomyelitis•Soft tissue infections•Odontogenic infections •Fractures
Prophylactic •Postoperative wound infection•In prevention of bacterial endocarditis.

Commonly used antibiotics in pediatric dentistry
• β – lactam antibiotics– Ex: Penicillins, Cephalosporins
• Macrolides – Ex: Erythromycin
• Clindamycin • Ciprofloxacin • Metronidazole, Tinidazole
PenicillinsFirst antibiotic to be used clinically in 1941Originally obtained from the fungus Penicillium
notatum, but now, Penicillium chrysogenum• MOA:– Interfere with the bacterial cell wall synthesis– Transpeptidases enzyme is responsible for cross linkages
between peptide chains in bacterial cell wall, results in stability and rigidity of the cell wall.
– Penicillins inhibit transpeptidases, so that cross linking doesnot takes place.
– They are most effective against rapidly multiplying organisms and are bactericidal
Classification • Acid resistant alternative to penicillin G– Phenoxymethyl penicillin (Penicillin V)
• Penicillinase resistant penicillins– Oxacillin, Cloxacillin, Methicillin
• Extended spectrum penicillins– Aminopenicillins
• Ampicillin, Amoxicillin
– Carboxypenicillins• Carbenicillin, Ticarcillin
– Uriedopenicillins • Piperacillin, Mezlocillin
• β – lactamase inhibitors– Clavulanic acid, Sulbactam
Penicillin V• Penicillin VK is a beta-lactam antibiotic and is
bactericidal against gram-positive cocci and the major microbes of mixed anaerobic infections
• Unlike natural penicillin, it is acid stable and can be given orally
• Adverse reactions:– Adverse drug reactions include mild diarrhoea, nausea and
oral candidiasis– There is a 0.7 to 10% allergy rate among patients– The usual allergic responses exhibited are skin rashes that
usually respond to antihistamine therapy– Severe reactions of angioedema have occurred, characterized
by severe swelling of the lips, tongue, face, and periorbital tissues

Penicillin V• The usual daily dose of penicillin V for treating
odontogenic infections is:– Children ≤ 12 years of age: 25-50 mg/kg of body weight in
divided doses every 6-8 hours.– Children >12 years of age and adults: 250- 500 mg every 6
hours for at least 10 days.– Penicillin VK is supplied as 125 or 250 mg/5ml solution or
250 and 500 mg tablets.

Ampicillin• Active against Gm + ve and Gm – ve organism• Antibacterial activity is similar to that of natural
penicillins i.e, Penicillin G• It is effective against Strep.viridans, Enterococci,
Gonococci, Pneumococci and Meningococci• Adverse effects:– Diarrhoea, rashes, drug fever, oral candidiasis
• Drug dosage:– 50 – 100 mg/kg/day (maximum 2-3 g/day) orally– 100 – 200 mg/kg/day I.M/I.V

Amoxicillin• It is a close congener of Ampicillin; similar in all aspects except:
– Oral absorption is better, higher and more sustained blood levels are produced
– Incidence of diarrhoea is less
• Dosage:– Children 25 – 50 mg/kg in 3 divided doses
• Available as:– Capsules:
• Novamox, Mox, Wymox (250 mg, 500 mg)
– Dispersible tablets• Novamox (125 mg, 500 mg), Wymox (250 mg), Lamoxy (250 mg), Blumox (125 mg,
250 mg, 500 mg)
– Tablets– Kid tab
• Wymox, Lamoxy (125 mg)
– Syrups– Drops– Injections

Cloxacillin • It is a penicillinase resistant penicillin• It is less active against Penicillin G sensitive
organisms, so it should not be used as a substitute• It is used in conjunction with ampicillin or
amoxicillin to enhance the synergism• Dosage:– Children 50 – 100 mg/kg/day , orally or I.V
Combinations • Amoxicillin and Cloxacillin
– Children 50 – 100 mg/kg/day in 3 divided doses– Available as:
• Cap. Novaclox (Amox 250 mg + Clox 250 mg)• Cap. Mox Kid (Amox 125 mg + Clox 125 mg)
• Amoxicillin with LB– Cap Novamox LB (Amox 250 mg, Lactobacillus 6 million
Spores)
• Amoxicillin with Clavulanic acid– Clavulanic acid:
• Inhibits the β – lactamase enzyme produced by bacterias• It’s a progressive inhibitor, inhibition increases with time• It’s a suicide inhibitor, gets inactivated after binding to the enzyme
– Enhancin, Augumentin Duo, Clavam (375 mg, 625 mg)– Kid tab Amoxclav

Adverse reactions• Frequent adverse effects– Diarrhoea– Hypersensitivity– Nausea– Rash– Neurotoxicity– Urticaria– superinfection (including candidiasis).
• Infrequent adverse effects (0.1–1% of patients)– fever,vomiting, erythema, dermatitis, angioedema, seizures
(especially in epileptics), and pseudomembranous colitis

Cephalosporins • Semisynthetic antibiotics derived from fungus,
Cephalosporium acremonium• They are chemically related to penicillins• All cephalosporins are bactericidal and have the same
mechanism of action as penicillin– Inhibition of bacterial cell wall synthesis

Classification Parentral
• First generation– Cephalothin– Cefazolin
• Second generation– Cefuroxime– Cefoxitin
• Third generation– Cefotaxime– Ceftizoxime– Ceftriaxone– Ceftazidime– Cefoperazone
• Fourth generation– Cefepime– Cefpirome
Oral
• First generation– Cephalexin– Cephadrine– Cefadroxil
• Second generation– Cefaclor– Cefuroxime axetil
• Third generation– Cefixime– Cefpodoxime proxetil– Cefdinir– Ceftibuten

Range of action• First generation
– Mostly effective against gram positive and some gram negative bacteria, but not effective against anaerobes
• Second generation– Have wider range of action against gram negative bacilli, less active
against gram positive cocci
• Third generation– Poor activity against gram positive cocci, but are more active against
gram negative bacilli and variable activity against pseudomonas
• Fourth generation– They are resistant to β lactamases and can penetrate the blood brain
barrier
• Fifth generation– Recently discovered cephalosporin– Used in cases of severe infection – Ex: Ceftobirole
Cephalosporins • Commonly used cephalosporins
– Cefazolin• Susceptible to staphlococcal β lactamase • Preferred parentral cephalosporin for surgical prophylaxis
– Cephalexin• Orally effective first generation cephalosporin• Less active against penicillinase producing staphylococci• Most commonly used cephalosporin• Dosage : Children: 25 – 100 mg/kg/day orally• Ex: Sporidex, Ceff, Sepexin
– Cefadroxil• Close congener of Cephalexin• Antibacterial activity is similar to that of cephalexin• Dosage: Children: 30 mg/kg/day orally• Ex: Droxyl, Cefadur, Cefoxid
– Cefaclor• Dosage : 125 – 250 mg daily
– Cefixime• Highly active against enterobacteria• Dosage : 200 – 400 mg BD
Macrolides • These are antibiotics having macrocyclic lactone ring
with attached sugars• Drugs included in this category are Erythromycin,
Spiramycin, Roxithromycin, Clarithromycin and Azithromycin
• Commonly used macrolides are Erythromycin and Azithromycin
Erythromycin • Isolated from Streptomyces erythreus in 1952• Mechanism of Action:
– It is bacteriostatic– Interfere with protein synthesis by inhibiting enzyme transferase at the 50S
subunit of ribosome– It is effective against Gm + ve and Gm – ve bacteria and most importantly
against penicillin resistant staphylococci– Depending upon its serum concentration, it may be bactericidal.
• Uses in dentistry– Used as a prophylactic agent in infective endocarditis– Used in patients who are allergic to penicillin
• Dosage:– Children : 30-50 mg/kg daily in divided doses
• Adverse effects:– Abdominal pain, nausea, diarrhoea, stomatitis are common– Hepatic dysfunction is a relative contraindication for erythromycin therapy
Clindamycin • Clindamycin inhibits protein synthesis by reversibly
binding to the 50S subunit of the ribosomal thus blocking the transpeptidation or translocation reactions of susceptible organisms resulting to stunted cell growth.
• Uses:– Used in severe anaerobic infections– Used in infective endocarditis prophylaxis
• Dosage:– Children:3-6 mg/kg every 6 hr
• Adverse drug reactions:– Diarrhoea, nausea, vomiting, abdominal pain, exfoliative and
vesiculous dermatitis, urticaria– Causes Gasping syndrome in Neonates

Nitroimidazoles • Antibiotics included in this category are– Metronidazole– Tinidazole– Secnidazole– Ornidazole
• Commonly used drugs are– Metronidazole and Tinidazole
Metronidazole • Mechanism of action:
– After entry in to the anaerobic organism,Metronidazole is reduced at the 5-Nitro position, that interact with DNA to cause destruction of helical DNA structure and leading to protein synthesis inhibition and cell death in susceptible organisms.
• It is effective against a wide range of organisms including – E. histolytica – T. vaginalis – Giardia– Bacterioides sp– Fusobacterium sp – Clostridium sp– Peptococcus sp and Peptostreptococcus sp

Metronidazole • Uses:– Primarily used in the treatment of obligate anaerobes in the
oral cavity– Has been used in the treatment of periodontitis– Used along with other antibiotics to treat mixed dental
infections
• Dosage:– 7.5 mg/kg in thrice daily– Available as Metrogyl 200, 400 mg tabs
• Adverse reactions:– Nausea, anorexia, abdominal pain and metallic taste are the
common side effects

Quinolones • They constitute a group of 1,8-naphthydrine
derivatives• They are synthetically produced drugs• Nalidixic acid is the prototype of the quinolones
drugs and was introduced in 1964• Drugs are– Ciprofloxacin– Norfloxacin– Ofloxacin– Levifloxacin– Gatifloxacin– Lomfloxacin

Ciprofloxacin • Mechanism of action:
– Ciprofloxacin promotes breakage of double-stranded DNA in susceptible organisms and inhibits DNA gyrase, which is essential in reproduction of bacterial DNA.
• Uses:– It is the first oral broad spectrum antimicrobial agent with
good activity against Pseudomonas aeruginosa– Excellent activity against wide range of Gm – ve organisms.– Useful in the management of mixed infections– But most of the anareobic bacteria are resisitant.
• Dosage:5-15 mg/kg bid• Adverse reactions:
– Nausea, headache, diarrhoea, photosensitivity, skin rashes
Other antibiotics….• Tetracyclines• Aminoglycosides• Sulfonamides

Local application of antibiotics• Chlorhexidine 0.2 % as – Mouthwash – Intra canal irrigant
• 3Mix-MP as intra canal medicament– Ciprofloxacin 500 mg– Metronidazole 200 mg– Minocycine 100 mg
• Metronidazole as intra canal irrigant• Doxycycline hyclate in avulsed root surface to aid
revascularization

Antibiotic Prophylaxis • A prophylaxis is a measure taken to maintain health
and prevent the spread of disease.• Bacterial endocarditis is a microbial infection of the
inner layer of the cardiac muscle (endocardium).• Patients with congenital or acquired cardiac defects
are believed to be at high risk for developing bacterial endocarditis if a (dental) procedure causes a transient bacteremia.
• Blood-bourne bacteria may lodge on the abnormal endocardium or heart valves, causing endocardial infection
Bacterial endocarditis• . In 2007 the American Heart Association revised its
1997 guidelines on prevention of bacterial endocarditis.– Bacterial endocarditis is much more likely to result from
frequent exposure to random bacteremias associated with daily activities than form bacteremia caused by dental, GI tract, or GU tract procedures.
– Prophylaxis may prevent an exceedingly small number of cases bacterial endocarditis, in individuals who undergo dental, GI tract or GU tract procedures.
– The risk of antibiotic associated adverse events exceeds the benefit from prophylactic antibiotic therapy.
– Maintenance of optimal oral health and hygiene may reduce the incidence of bacteremia from daily activities and is more effective than prophylactic antibiotics for a dental procedure for reducing the risk of bacterial endocarditis.

• The revised guidelines clarified when antibiotic prophylaxis is/is not recommended, i.e.– Only an extremely small number of cases might be prevented by
antibiotic prophylaxis.– Antibiotic prophylaxis for dental procedures is recommended
only for patients with underlying cardiac conditions associated with the highest risk of adverse outcomes from bacterial endocarditis.
– For patients with these underlying cardiac conditions, prophylaxis is recommended for all dental procedures that involve manipulation of gingival tissues or the periapical region of teeth or perforation of the oral mucosa.
– Prophylaxis is not recommended based solely on an increased lifetime risk of acquiring bacterial endocarditis.
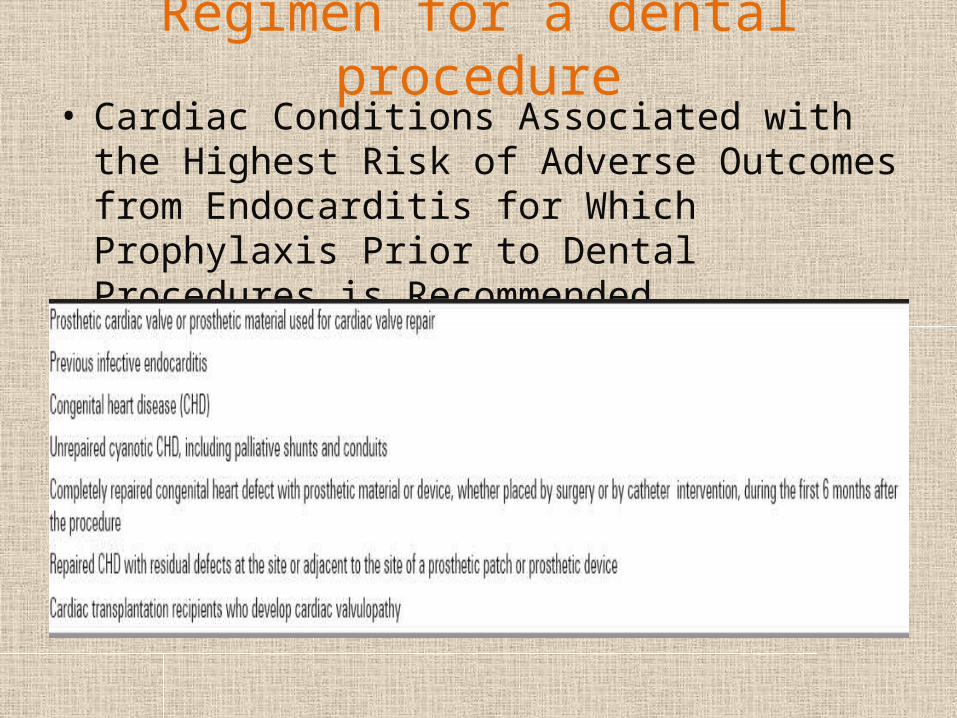
Regimen for a dental procedure• Cardiac Conditions Associated with the Highest Risk
of Adverse Outcomes from Endocarditis for Which Prophylaxis Prior to Dental Procedures is Recommended.
Regimen for a dental procedure• Recommended:– All dental procedures that involve manipulation of gingival
tissue or the periapical region of the teeth or perforation of the oral mucosa
• Not recommended:– Routine anesthetic injections through no infected tissue– Dental radiographs– Placement of removable prosthodontic or orthodontic
appliances.– Adjustment of orthodontic appliances– Placement of orthodontic brackets– Shedding of deciduous teeth– Bleeding from trauma to the lips and tongue


Administer single dose 30 to 60 minutes before procedure
Situation Agent Adults Children
Oral Amoxicillin 2 gm 50 mg/kg
Unable to take oral medicationAmpicillin
ORCefazolin or ceftriaxone
2gm IM or IV
1gm IM or IV
50 mg/kg IM or IV
50 mg/kg IM or IV
Allergic to penicillins or ampicillin-oral
CephalexinOR
ClindamycinOR
Azithromycin or clarithromycin
2 gm
600mg
500mg
50 mg/kg
20 mg/kg
15 mg/kg
Allergic to penicillin or ampicillin and unable to take oral medication
Cefazolin or ceftriaxoneOR
Clindamycin
1 gm IM or IV
600mg IM or IV
50 mg/kg IM or IV
20 mg/kg IM or IV

Analgesics • Drug that relieves pain without blocking nerve
impulse conduction or markedly altering sensory function
• A drug that selectively relieves pain by acting in the CNS or on peripheral pain mechanisms, without significantly altering conciousness
Types of Analgesics • Narcotic analgesics – also termed opioids, are all derived from opium– narcotic analgesics vary in potency, but all are effective in
treatment of visceral pain when used in adequate doses– act on CNS receptors to inhibit pain impulses
• Non Narcotic analgesics– Classified under NSAID’S– They do not depress CNS– Do not produce physical dependence or abuse liability– They act primarily on peripheral pain mechanism but also
in CNS to raise the pain threshold

Opioids• Dark brown resionous material obtained from
Papaver somniferum• Classification:– Natural opioids
• Morphine, Codeine
– Semisynthetic• Heroine, Pholcodeine
– Synthetic• Pethidine, Fentanyl, Tramadol, Methadone

Uses in dentistry• Morphine • Pethidine (Meperidine)• Codeine • Mechanism of Action:– They act directly on the receptor site in the CNS i.e, µ,κ,δ
to inhibit the release of excitatory transmittors from the primary afferent carrying pain impulses
– They also increase the pain perception threshold

Morphine • Strong analgesic• dull., poorly localized visceral pain is relieved better
than the sharply defined somatic pain• Degree of analgesia is directly proportional to the
dose• Adverse effects:– Sedation, Lethargy, Vomiting, Constipation, Respiratory
depression, – Antidote : Naloxone , Nalorphine
• Uses: – Indicated in case of severe pain – Especially in traumatic, visceral, ischemic (myocardial
infection), post operative, burn and cancer pain

Morphine • Dosage:– Children : 0.1 – 0.2 mg/kg
• Precautions– It is a drug of emergency, care has to be taken in
• Infants who are more susceptible to respiratory depression• Patient with bronchial asthma• Morphine is contraindicated in patients with head injury

Pethidine • Synthesized as an atropine substitute in 1939• Chemically unrelated to morphine• Mechanism of action is similar to that of morphine• Differences are
– Analgesic efficacy is little lower than morphine, but higher than codeine
– Onset of action is more rapid– Safer in asthmatics– Constipation and miosis are less marked
• Dosage:0.5- 2 mg/kg • Uses:
– Mostly used in post operative pain relief– Also as a preanesthetic medication

Codeine • It is a methyl morphine• Partly converted in the body to morphine• Less potent than morphine and also less efficacious • More effective in oral route• Codeine is usually given in combination with non-
narcotic analgesics, because the narcotic acts at a central site and the non-narcotic analgesic at a peripheral site providing enhanced analgesic activity.
• Dosage: 0.5-1mg codeine/kg/dose every 4-6 hours• Side effects: constipation, drowsiness, nausea,
vomiting, miosis, depression, and pardoxical coughing

NSAIDS• They are nonsteroidal, anti-inflammatory cyclo-
oxygenase inhibitors• Prostaglandins are the substances produced from the
Arachidonic acid(derived from membrane phospholipids at the injury site) by the enzyme Cyclo-oxygenase(COX)
• Prostaglandins play a part in formation of erythema, edema, and fever associated with inflammation and generates pain– By the direct action of PG’s– Sensitizing the pain receptors and reduces the pain
threshold– By release of substances such as bradykinin and histamine

Cyclo- oxygenases• There are two types of COX– COX 1
• Constitutive form present in blood vessels, GIT and kidney
– COX 2• Inducible form at the site of inflammation
General principles• AAPD guidelines
– recognize and assess pain, documenting in the patient’s chart;– use non-pharmacologic and pharmacologic strategies to reduce pain
experience pre-operatively;– be familiar with the patient’s medical history to avoid prescribing a
drug that would be otherwise contra- indicated;– comprehend the consequences, morbidities, and toxi- cities
associated with the use of specific therapeutics;– consider non-opioid analgesics as first line agents for post-operative
pain management;– utilize drug formularies in order to accurately pre- scribe
medications for the management of postopera- tive pain;– consider combining NSAIDs with acetaminophen to provide a
greater analgesic effect than the single agent alone; and– combine opioid analgesics with NSAIDs for post- operative
treatment of moderate to severe pain in children and adolescents.
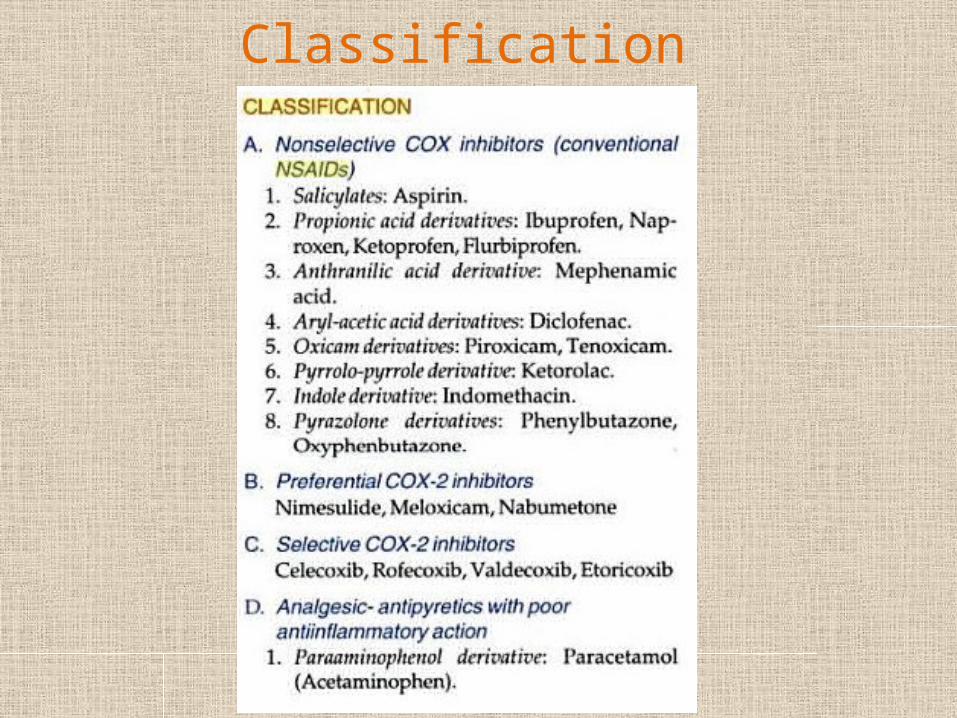
Classification

Most commonly used NSAIDS• Aspirin• Ibuprofen• Diclofenac• Piroxicam• Ketorolac• Paracetamol

Aspirin • It is developed by Bayer in 1899• It is an Acetyl Salicylic acid• It irreversibly inhibits both COX 1 and COX 2• Uses:
– As an analgesic in doses of 0.3 – 0.6 gm, 6-8 hourly– As an antipyretic– In acute rheumatic fever in the dose of 75-100 mg/kg/day– Also in cases of rheumatoid arthiritis, osteoarthritis– In low doses of 100 – 300 mg, it inhibits platelet aggregation
and is used in post myocardial infarction patients
• Dosage:– Analgesic and antipyretic: Oral, rectal: 10-15mg/kg dose every
4-6 hours up to a total of 4 g/day
Aspirin • Adverse reactions:– Peptic ulceration– Precipitation of asthma– Hemorrhage– Reye’s syndrome:
• Use of Aspirin in children below 12 years with viral infections cause life threatening condition characterized by– Vomiting– Lethargy– Coma– Even death– If patient survives, causes irreversible brain damage
• So, use of aspirin in children is prohibited in India

Ibuprofen • It’s a propionic acid derivative• Action: analgesic, antipyretic and anti inflammatory• Dosage:
– 4-10mg/kg/dose every 6-8 hours (maximum daily dose 40mg/kg/day)
• Adverse effects:– Less than that of aspirin– Gastric discomfort, nausea, vomiting, headache, dizziness,
dyspepsia, abdominal pain, heart burn, diarrhoea, epigastric pain
• Available as;– Tablets (200, 400, 600 mg)
• Brufen, Ibuprofen, Emflam
– Suspension (100mg/5ml)• Ibugesic, Ibrumac, Gesic

Diclofenac • Its an aryl – acetic acid derivative• Dosage:
– Children: 2 to 3 mg/kg/day orally in divided doses 2 to 4 times dailyMaximum dose: 200 mg daily.
• Adverse reactions:– GI disturbances; headache, dizziness, rash; GI bleeding, peptic
ulceration; abnormalities of kidney function. Pain and tissue damage at inj site (IM)
• Available as:– Tablets (50, 100 mg)
• Agile, Dan, Diclofen
– Dispersed tablets• Agile, Diclonac, Diclotal, Zobid - D
– Injections (IM)• Voveran, Osteoflam, Oxalgin

Piroxicam • Its an oxicam derivative• Dosage:
– 0.2 to 0.3 mg/kg orally once a day. Maximum daily dose is 15 mg
• Adverse effects:– GI disturbances, peptic ulcer, GI bleeding, headache, dizziness,
blurred vision, tinnitus, skin rashes and pruritus. Haematological changes and photosensitivity
– Piroxicam is contraindicated for the treatment of perioperative pain in patients undergoing coronary artery bypass graft (CABG) surgery.
– Patients with the "triad" of asthma, nasal polyps, and aspirin or other NSAID hypersensitivity (i.e. angioedema, bronchospasm, urticaria, rhinitis) may be cross-sensitive to piroxicam
• Available as:– Tablets (10, 20 mg)
• Pirox, Dolonex, Doloswift

Ketorolac • It’s a pyrrolo-pyrrole derivative• A novel NSAID with potent analgesic and modest
antiinflammatory activity• In post operative pain it has equalled the efficacy of
Morphine, without interacting with opioid receptors• Dosage:
– Children 0.5 mg/kg
• Uses:– Frequently in post operative pain– Acute musculoskeletal pain
• Adverse effects:– Abdominal pain, dyspepsia, ulceration, loose stools,
drowsiness, nervousness, pain at the injection site

Paracetamol • It is de-ethylated active metabolite of Phenacetin• It has analgesic and antipyretic action but no anti
inflammatory action– Paracetamol exhibits analgesic action by peripheral blockage
of pain impulse generation. – It produces antipyresis by inhibiting the hypothalamic heat-
regulating centre. – Its weak anti-inflammatory activity is related to poor
inhibition of prostaglandin synthesis
• Adverse reactions:– Nausea, skin rashes, acute renal tubular necrosis
• Dosage:– 10 to 15 mg/kg/dose every 4 to 6 hours as needed
(Maximum: 5 doses in 24 hours)

Choice of NSAIDS• Choice of drug is empirical• Factors
– Nature of the problem(acute/chronic, inflammation, severity)– Consideration of risk factors in individual patients
• Mild to moderate pain Paracetamol / Low dose Ibuprofen• Acute pain associated with inflammation high dose of
Ibuprofen, Diclofenac• Postoperative pain Ketorolac• Gastric intolerance to conventional NSAIDs Rofecoxib• Exacerbation of pain Piroxicam• Patients with history of Asthma or anaphylactoid reactions Nimesulide

CLINICAL CONSIDERATIONS

Bacterial resistance• Along with the dramatic benefits of systemic antibiotics,
there has also been an explosion in the number of bacteria that have become resistant to a variety of these drugs. The problem is not the antibiotics themselves. Instead, the problem is in the way the drugs are used.
• The inappropriate overuse of antibiotics has resulted in a crisis situation due to bacterial mutations developing resistant strains.
• Many worldwide strains of Staphylococcus aureus exhibit resistance to all medically important antibacterial drugs, including vancomycin, and methicillin-resistant S. aureus has become one of the most frequent nosocomial, or hospital-acquired,pathogens.

A Glimmer of Hope….• A report from Aker University in Oslo, Norway,
strongly suggests that bacterial resistance to antibacterial agents can be reversed
• Dr. John Haug, infectious disease specialist says “We don’t throw antibiotics at every person with a fever. We tell them to hang on, wait and see, and we give them a Tylenol to feel better"

Myths……• Evaluating the following eight misconceptions or
“myths” may help to establish general guidelines to aid us in making clinical decisions regarding the use of antibiotic therapy, thereby leading to optimum use and therapeutic success.

Myths…• Myth #1: Antibiotics cure patients.• Myth #2: Antibiotics are substitutes for surgical
intervention• Myth #3: The most important decision is which antibiotic to
use• Myth #4: Antibiotics increase the host’s defense to infection• Myth #5: Multiple antibiotics are superior to a single
antibiotic• Myth #6: Bactericidal agents are always superior to
bacteriostatic agents• Myth #7: Antibiotic dosages, dosing intervals and duration
of therapy are established for most infections• Myth #8: Bacterial infections require a “complete course”
of antibiotic therapy

• Baumgartner and Xia published a report of the susceptibility of bacteria recovered from acute apical abscesses to five commonly used antibiotics in dentistry, led to the following conclusions:– Pen-V-K is the antibiotic of choice for endodontic infections due to
its effectiveness in polymicrobial infections, its relative narrow spectrum of activity against bacteria most commonly found in endodontic infections, its low toxicity and low cost.
– Clindamycin is the antibiotic of choice for patients allergic to penicillins
– While amoxicillin and augmentin (amoxicillin plus clavulanate) demonstrated a higher antibacterial effectiveness than Pen-V-K, due to the broader antibacterial spectrum of amoxicillin and the increased cost of augmentin, the authors recommended that amoxicillin/augmentin be reserved for unresolved infections and patients who are immunocompromised.
– Metronidazole demonstrated the greatest amount of bacterial resistance and is only effective against anaerobes.Therefore, it should not be used alone for the treatment of endodontic infections

Endodontic infections that requires antibiotics
• 1st category irreversible pulpitis with moderate/ severe symptoms
• 2nd category irrversible pulpitis with an acute apical periodontitis
• 3rd category necrotic pulp, chronic apical periodontitis, no swelling and no/mild symptoms
• 4th category necrotic pulp, acute apical periodontitis, no swelling and moderate to severe symptoms
• 5th category necrotic pulp, chronic apical periodontitis and cases with sinus tracts
• 6th category necrotic pulp, abscess with swelling and moderate to severe symptoms of infection

Conclusion • Since their discovery eight decades ago, safe systemic
antibiotics have revolutionized the treatment of infections, transforming once deadly diseases into manageable health problems. However, the growing phenomenon of bacterial resistance, caused by the use and abuse of antibiotics, is now threatening to take us back to the pre-antibiotic era.
• A fundamentally changed view of antibiotics is needed. They must be looked on as a common good, where individuals must be aware that their choice to use an antibiotic will affect the possibility of effectively treating bacterial infections in other people.

References • Goodman & Gilman's The Pharmacological Basis of
Therapeutics• K.D.Tripathi’s Essential of medical pharmacology• Katzung’s Basic and Clinical pharmacology• Shoabha Tandon’s Textbook of Pedodontics• Ghom’s Textbook of oral medicine• Damle’s Textbook of pediatric dentistry• Antibiotics: Use and misuse in pediatric dentistry, Journal
of Indian Society of Pedodontics and Preventive Dentistry: Vol. 29, No. 4, October-December, 2011, pp. 282-287
• Use of systemic antibiotics in endodontic infections –A review, Journal of Indian academy of dental specialist researches,vol 1 issue 2:jul-sep2012

• AAPD reference manual: Vol 33/No 6• Baumgartner JC and Xia T. Antibiotic susceptibility
of bacteria associated with endodontic abscesses. J Endod 2003;29(1):44-47
• PallaschTJ. Global antibiotic resistance and its impact on the dental community. J Cal Dent Association 2000;28:215-233

THANK
YOU