analgesia for people with acute ankle sprain · pdf fileankle instability, pain and further...
TRANSCRIPT
April 2015 | Volume 23 | Number 1 EMERGENCY NURSE24
Art & science | The synthesis of art and science is lived by the nurse in the nursing act JOSEPHINE G PATERSON
PEOPLE WITH ankle sprains commonly present to general practice and urgent care settings (Slimmon and Brukner 2010), and an estimated 302,000 are seen in UK emergency departments (EDs) every year. These ankle sprains occur predominately on sports grounds in people aged under 25 and at home in patients aged over 50 (Ferran and Maffulli 2006). Boyce (2004) concludes that the highest incidence of ankle injuries are in people aged between 16 and 20. Waterman et al (2010) found an incidence rate of 5,840 per 100,000 people a year at the United States
Military Academy and that physical activity is a major contributory factor in ankle sprain.
In a clinical knowledge summary (CKS) on the management of sprains and strains, the National Institute for Health and Care Excellence (NICE) (2012) advocates the use of paracetamol or topical non-steroidal anti-inflammatory drugs (NSAIDs) with protection, rest, ice, compression and elevation as first-line treatment for ankle sprain.
The CKS suggests that NSAIDs should not be used in the first 48 hours post-injury because they can delay the healing process. In the experience of the principal author (DC), however, practitioners in urgent care settings often prescribe NSAIDs as initial treatment for soft-tissue injuries (NICE 2012).
NSAIDs can be administered as analgesics, anti-pyretics and anti-inflammatories. Those licensed for use in the UK include ibuprofen, diclofenac and naproxen (NHS Choices 2014).
PathophysiologyThe ankle joint comprises the tibia, fibula, calcaneum and talus, as well as the cuboid, navicular and cuneiform bones, all of which are connected by ligaments (Purcell 2010). These ligaments are made up of elastin and collagen, and sudden tension that takes a ligament beyond its stretching capacity results in a sprain. There are three grades of sprain (Weintraub 2003):1. Where the ligament returns to resting length but
there is micro-failure in some fibres.2. Where the ligament does not recover to resting
length, some ankle instability exists and fibres sustain a larger amount of rupture.
ANALGESIA FOR PEOPLE WITH ACUTE ANKLE SPRAIN
David Carter and Jeshni Amblum-Almer discuss the results of a literature review on using non-steroidal anti-inflammatory drugs in the management of a common injury
AbstractAround 302,000 people with soft-tissue ankle injuries present to UK emergency departments every year (Ferran and Maffulli 2006). These patients are generally treated conservatively with analgesia, ice, compression and elevation, and rest. There is some discussion in the literature about whether or not people with these injuries should be treated with non-steroidal anti-inflammatory drugs (NSAIDs), with some authors claiming that the inflammatory response following injury is part of the healing process and should not be halted. This article examines the literature on the efficacy of administering NSAIDs as the first-line drug management for ankle sprain. It also considers cost of treatment, prescribing practice and contraindications of NSAIDs.
KeywordsAnalgesia, ankle injuries, non-steroidal anti-inflammatory drugs, NSAIDs, pain management
David Carter is an urgent care centre emergency care practitioner at West Middlesex University Hospital NHS Trust
Jeshni Amblum-Almer is a senior lecturer-practitioner in primary care at Kingston and St George’s University, London
Date of submissionFebruary 2 2015
Date of acceptanceMarch 16 2015
Peer reviewThis article has been subject to double-blind review and has been checked using antiplagiarism software
Author guidelinesjournals.rcni.com/r/en-author-guidelines

Scie
nce
Phot
o Li
brar
y

April 2015 | Volume 23 | Number 1 EMERGENCY NURSE26
Art & science | anti-inflammatory drugs
3. Where there is gross fibre failure and severe ankle instability.
Ligaments have a poor blood supply so it is vital that the appropriate treatment is given in a timely manner to minimise chronic stiffness and calcification (Purcell 2010).
Soft-tissue injuries go through three phases of healing: inflammation, proliferation and maturation. During the initial inflammatory phase, patients experience erythema, swelling and pain (Tortora and Derrickson 2011), which prevent activity. To help patients return to their normal activities quickly, the pain is often reduced and the swelling inhibited by NSAIDs. However, Bowie (2011), citing ‘controversial evidence’ of side effects associated with NSAIDs advises paracetamol and rest, ice, compression and elevation (RICE) instead.
In ankle sprains, the inflammatory phase typically lasts between two and seven days (Purcell 2010). Prostaglandin is responsible for localised swelling during this phase (Joint Formulary Committee (JFC) 2014) and NSAIDs work by inhibiting the action of cyclo-oxygenase-1 (COX-1) and cyclo-oxygenase-2 (COX-2), which reduce prostaglandin production.
The inflammatory phase is followed by the proliferative phase, when macrophages remove haematomas, fibroblasts produce collagen, and the capillary networks begin to rebuild. During the final maturation phase, which usually begins several weeks after injury and can last more than a year, collagen organisation increases and capillary networks return to normal levels.
Healed ligaments often have reduced tensile strength, often between 50% and 70% that of uninjured tissue. However, joint function remains unchanged due to increased tissue volume (Schepsis and Busconi 2006).
Literature review In 2014, the principal author undertook a literature review to assess the efficacy of NSAIDs as the first-line drug management for ankle sprain. Initially, the author searched for articles about randomised control trials of NSAID use in the treatment of acute ankle sprain, but later expanded the search to include musculoskeletal injuries in general.
Using combinations of the search terms ‘NSAIDs’, ‘non-steroidal anti-inflammatory drugs’, ‘sprain’, ‘ankle sprain’, ‘analgesia’, ‘randomised control trial’ and ‘anti-inflammatory’, he searched the Emergency Nurse, Hunter, PubMed, Science Direct and Springer databases. Initial inclusion criteria were articles in English published between 1995 and 2015. A total of 100 articles were identified.
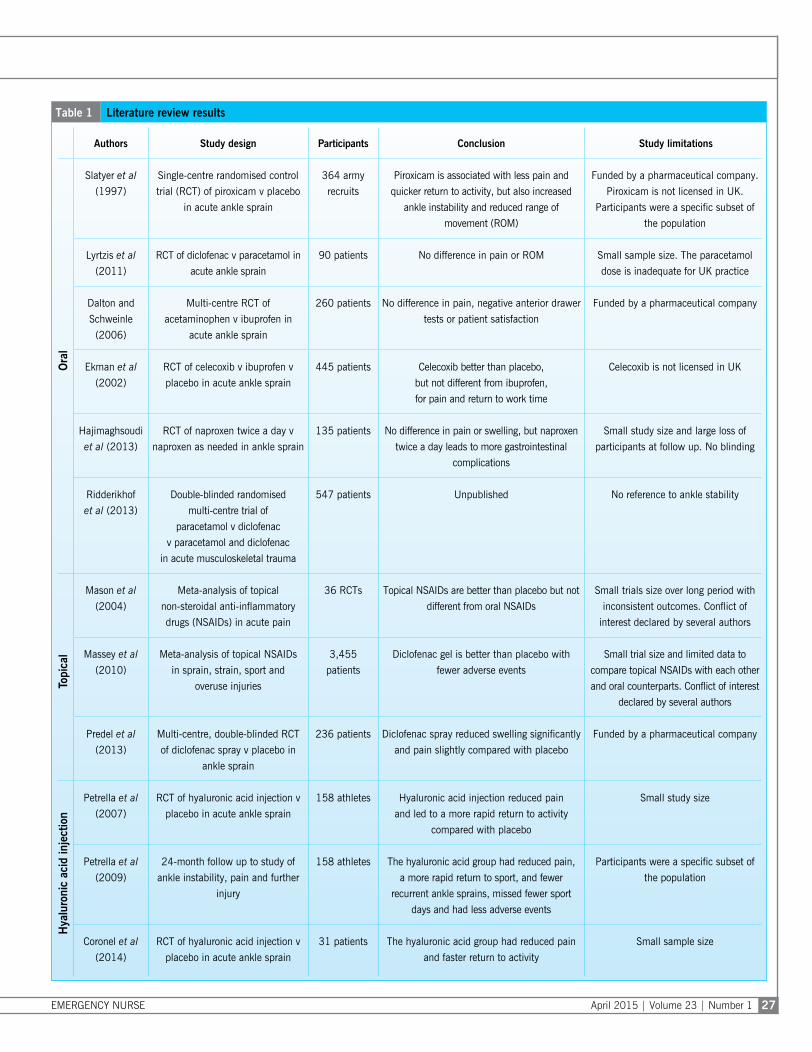
Articles were included in the review if they compared NSAIDs and paracetamol and/or placebo for musculoskeletal injury, and considered one of the following outcomes: pain, ankle instability, return to activity time or reduction in swelling. Those that focused on chronic conditions, such as osteoarthritis and back pain, were excluded, leaving a total of 12 relevant articles (Table 1).
Guidelines The NICE (2012) guidelines do not advocate the early administration of NSAIDs for ankle sprains due to concerns about delays in healing. The CKS on the management of sprains and strains states: ‘Use of oral NSAIDs should be delayed until 48 hours after the initial injury. Early use of NSAIDs coincides with muscle repair, regeneration, and growth. Inflammation is a necessary part of the healing process, therefore decreasing inflammation may impair the healing process’ (NICE 2012).
On the other hand, a recent review by van den Bekerom et al (2014) states that the benefits of using NSAIDs outweigh their adverse effects, such as gastrointestinal discomfort, and suggests using them in the initial management of patients with acute ankle sprains.
Oral NSAIDs In a single-centre trial conducted in Australia, Slatyer et al (1997) treated 364 army recruits with acute ankle sprain with either piroxicam, an NSAID, or placebo. Those treated with piroxicam experienced less pain and lost fewer training days, although some had concerns about ankle instability and reduced range of movement.
In reference to Slatyer et al’s (1997) study, Bellomo et al (2009) state that ‘changing practice or issuing strong recommendations on the basis of single-centre trials seem premature and ill advised’.
However, it should be noted that piroxicam is not licensed in the UK due to an increased risk of gastrointestinal side effects (JFC 2014) so application of Slatyer et al’s (1997) findings to UK practice would be difficult.
Lyrtzis et al (2011) conducted a small (n=90) study of the effects of diclofenac and paracetamol on pain and range of movement in patients with ankle sprain. The patients had been treated with either diclofenac sodium 75mg twice daily or paracetamol 500mg three times a day. It is unclear why patients did not receive the standard paracetamol dose of 1g and it seems likely this sub-therapeutic dose would have been insufficient in adult patients.
All patients had been blinded to treatment and advised RICE for ten days (NICE 2012). Three patients treated with diclofenac had stopped
EMERGENCY NURSE April 2015 | Volume 23 | Number 1 27
Table 1 Literature review results
Authors Study design Participants Conclusion Study limitations
Ora
l
Slatyer et al
(1997)
Single-centre randomised control
trial (RCT) of piroxicam v placebo
in acute ankle sprain
364 army
recruits
Piroxicam is associated with less pain and
quicker return to activity, but also increased
ankle instability and reduced range of
movement (ROM)
Funded by a pharmaceutical company.
Piroxicam is not licensed in UK.
Participants were a specific subset of
the population
Lyrtzis et al
(2011)
RCT of diclofenac v paracetamol in
acute ankle sprain
90 patients No difference in pain or ROM Small sample size. The paracetamol
dose is inadequate for UK practice
Dalton and
Schweinle
(2006)
Multi-centre RCT of
acetaminophen v ibuprofen in
acute ankle sprain
260 patients No difference in pain, negative anterior drawer
tests or patient satisfaction
Funded by a pharmaceutical company
Ekman et al
(2002)
RCT of celecoxib v ibuprofen v
placebo in acute ankle sprain
445 patients Celecoxib better than placebo,
but not different from ibuprofen,
for pain and return to work time
Celecoxib is not licensed in UK
Hajimaghsoudi
et al (2013)
RCT of naproxen twice a day v
naproxen as needed in ankle sprain
135 patients No difference in pain or swelling, but naproxen
twice a day leads to more gastrointestinal
complications
Small study size and large loss of
participants at follow up. No blinding
Ridderikhof
et al (2013)
Double-blinded randomised
multi-centre trial of
paracetamol v diclofenac
v paracetamol and diclofenac
in acute musculoskeletal trauma
547 patients Unpublished No reference to ankle stability
Topi
cal
Mason et al
(2004)
Meta-analysis of topical
non-steroidal anti-inflammatory
drugs (NSAIDs) in acute pain
36 RCTs Topical NSAIDs are better than placebo but not
different from oral NSAIDs
Small trials size over long period with
inconsistent outcomes. Conflict of
interest declared by several authors
Massey et al
(2010)
Meta-analysis of topical NSAIDs
in sprain, strain, sport and
overuse injuries
3,455
patients
Diclofenac gel is better than placebo with
fewer adverse events
Small trial size and limited data to
compare topical NSAIDs with each other
and oral counterparts. Conflict of interest
declared by several authors
Predel et al
(2013)
Multi-centre, double-blinded RCT
of diclofenac spray v placebo in
ankle sprain
236 patients Diclofenac spray reduced swelling significantly
and pain slightly compared with placebo
Funded by a pharmaceutical company
Hya
luro
nic
acid
inje
ctio
n
Petrella et al
(2007)
RCT of hyaluronic acid injection v
placebo in acute ankle sprain
158 athletes Hyaluronic acid injection reduced pain
and led to a more rapid return to activity
compared with placebo
Small study size
Petrella et al
(2009)
24-month follow up to study of
ankle instability, pain and further
injury
158 athletes The hyaluronic acid group had reduced pain,
a more rapid return to sport, and fewer
recurrent ankle sprains, missed fewer sport
days and had less adverse events
Participants were a specific subset of
the population
Coronel et al
(2014)
RCT of hyaluronic acid injection v
placebo in acute ankle sprain
31 patients The hyaluronic acid group had reduced pain
and faster return to activity
Small sample size

April 2015 | Volume 23 | Number 1 EMERGENCY NURSE28
Art & science | anti-inflammatory drugs
treatment within three days due to stomach problems. Active and passive ranges of movement (ROM) were calculated through computer images, which removed the possibility of error associated with subjective measurement, and no difference between the two groups’ pain scores was found. Both groups also showed improvement in pain and there was no difference between the two groups’ pain and movement outcomes.
Although the study’s sample size was small and participants were given inadequate doses of paracetamol, it appears that pain experience and ROM among participants given paracetamol and those given NSAIDs were similar.
In a US-based multi-centre, double-blinded study, Dalton and Schweinle (2006) examined the treatments of 260 patients with ankle sprain who had been given standard doses of either paracetamol, known in the US as acetaminophen, or ibuprofen to evaluate the hypothesis that NSAIDs impair ligament healing by inhibiting the inflammation process (Braund and Abbot 2007). Participants undertook the anterior drawer test (Purcell 2010) of ROM, used a visual analogue scale to indicate the pain they experienced and stated how satisfied they were with their treatments. Although often overlooked, patient satisfaction is an important outcome because it can affect compliance with treatment (Neighbour 2005).
Results indicate no difference in pain scores, anterior drawer test results or patient satisfaction between participants who had taken paracetamol and those who had taken ibuprofen (Dalton and Schweinle 2006).
Bellomo et al (2009) point out that changing practice requires ‘suitably powered, robust, independently supervised and monitored multi-centre, randomised, controlled trials’, and Dalton and Schweinle’s (2006) study, which took place across 42 healthcare centres, meets these criteria. However, the researchers declare that funding was provided by a pharmaceutical company.
Ekman et al (2002) compared the use of celecoxib, ibuprofen and placebo for ten days in 445 patients with ankle sprains. One of the measurable outcomes was pain on weight bearing. Celecoxib was shown to be better than the placebo for pain management and return to activity, but there was no difference between celecoxib and ibuprofen. Ibuprofen was shown to be its equal in efficacy and superior to the placebo. It should be noted that celecoxib is not licensed for musculoskeletal pain in the UK (JFC 2014).
In a follow-up study, Petrella et al (2004) compared celecoxib with naproxen for acute ankle sprain and found no difference in pain score,
although naproxen was associated with increased adverse events, specifically dyspepsia.
In an Iran-based study, Hajimaghsoudi et al (2013) compared the efficacy, in terms of the pain and swelling experienced by patients, and safety of treatment with naproxen 500mg twice daily and RICE, and naproxen as required (PRN) and RICE.
The study, which took place over seven days, involved 135 patients with acute ankle sprain. Injuries were judged to be acute if they had been sustained during the previous 48 hours, which is longer than in most other trials in the literature review.
Although the study was randomised, its participants took naproxen regularly or when they felt they needed it, which meant that they could not be blinded. Both groups showed similar clinical outcomes, but those treated with naproxen twice daily had more minor gastrointestinal complications than those treated PRN. Although this study shows positive results for the use of NSAIDs PRN, it is limited because participants were not blinded and many were lost to follow up.
Loss of study participants to follow up can affect results. Miser (2006) states that an attrition rate of more than 10% in short-term studies can invalidate results and, in Hajimaghsoudi et al’s (2013) study, loss to follow up was just over this figure. Furthermore, the authors did not consider whether participants had undertaken RICE before they presented, or how length of time since injury affected pain and swelling.
Ridderikhof et al (2013) have submitted a proposal for a Dutch-based multi-centre, double- blinded, randomised, inferiority study of pain scores in 547 patients with acute musculoskeletal trauma who have been administered paracetamol, diclofenac or both.
An additional measure to assess ankle stability pre- and post-treatment would add to the evidence base related to the use of NSAIDs in the management of ankle sprains. At time of Emergency Nurse going to press, the results had not been published, but this study should add considerably to the evidence base for NSAID use. It also resembles studies of UK urgent care centres more than other research in non-UK populations (Slatyer et al 1997, Lyrtzis et al 2010).
Topical NSAIDs NICE (2012) suggests that, for immediate treatment of ankle sprain, paracetamol can be substituted by topical NSAIDs. This suggestion is based partly on Mason et al’s (2004) meta-analysis of 36 randomised control trials, although most of these trials were small and inconsistent. The researchers conclude that pain

EMERGENCY NURSE April 2015 | Volume 23 | Number 1 29
management with topical NSAIDs is no different from that with oral NSAIDs but is superior to that with placebo, and that there is a notable reduction in side effects with topical NSAIDs (Mason et al 2004).
In another meta-analysis involving 3,455 patients with acute ankle sprain, strain, sport and overuse injuries, Massey et al (2010) compared pain levels experienced by patients who had been given diclofenac gel with those given placebo.
The researchers found the former group experienced less pain than the latter, and that ‘adverse events were rare’ in the diclofenac group (Massey et al 2010), which suggests that diclofenac gel may be preferable to oral NSAIDS due to its apparent ability to reduce adverse reactions.
Predel et al (2013) conducted a Hungary-based multi-centre, double-blinded, randomised study of whether diclofenac spray gel reduces swelling in uncomplicated ankle sprains. To ensure consistency, all patients’ ankles were measured the same way, namely the figure-of-eight method (Tatro-Adams et al 1995), which has been validated by Petersen et al (1999). Pain scores were also monitored. Of the 236 people included in the trial, only 5% were lost to follow up.
Results showed that diclofenac spray reduced swelling when compared to placebo, which Predel et al (2013) suggest could lead to earlier recovery of function and return to normal activity. There was a small reduction in spontaneous pain when diclofenac spray was used and the treatment was well tolerated with only one adverse event, namely skin irritation.
It should be noted, however, that the researchers were employed and funded by a pharmaceutical company that produces diclofenac spray gel.
Hyaluronic acid injection Believed to be present in the early stages of wound healing, hyaluronic acid promotes inflammation (Aya and Stern 2014).
To test its efficacy in promoting a more rapid return to activity with less pain, Peterella et al (2007) undertook a study of 158 competitive athletes with ankle sprain who had been treated with hyaluronic acid injection and RICE, or placebo and RICE. They found that patients who had received hyaluronic acid reported reduced pain, a more rapid return to sport, fewer recurrent ankle sprains, fewer missed sport days and fewer adverse events than those given placebo.
It is important to note that participants were a physically fit group of competitive athletes who are not representative of the general population. Nevertheless this is the first study in which participants were followed up after 24 months.
Another single-centre study was undertaken in Canada by Coronel et al (2014). This study involved only 31 participants, but the researchers found reductions in pain and a more rapid return to activity in patients treated with hyaluronic acid. A large multi-centre trial is required to inform clinical practice further.
Sodium hyaluronate is licensed for pain relief and recovery from ankle sprain in the UK (JFC 2014). However, its cost, at about £139 for the two injections required (Trent Medicines Information Service 2012) is higher than that for oral and topical treatments.
Hyaluronic acid injection is not suitable for all patients suffering acute ankle sprain, but the fact that it promotes inflammation yet reduces pain and swelling might challenge traditional beliefs that patients should be managed with NSAIDs. Following publication of further research into hyaluronic acid injections, the treatment could be offered to patients whose jobs require their speedy return to pre-injury function, such as those in the armed forces or athletes.
DiscussionPrescribing practice Between 2010/11 and 2013/14, the number of times diclofenac was prescribed in England reduced from 64% to 28% of incidents (IMS Health 2014). This sharp fall is likely to be related to a Medicines and Healthcare products Regulatory Agency (MHRA) alert about risks associated with the drug in people with diabetes, high cholesterol and hypertension (MHRA 2013).
In the meta-analysis that informed the MHRA alert, Bhala et al (2013) found that diclofenac at 150mg a day and high-dose ibuprofen, at 2,400mg a day, resulted in three times the incidence of vascular events compared with placebo, but that naproxen at 1,000mg a day did not increase the incidence.
There has been a subsequent increase in naproxen and ibuprofen prescribing, with an approximately 250% increase in naproxen prescriptions between 2010 and 2014 (IMS Health 2014).
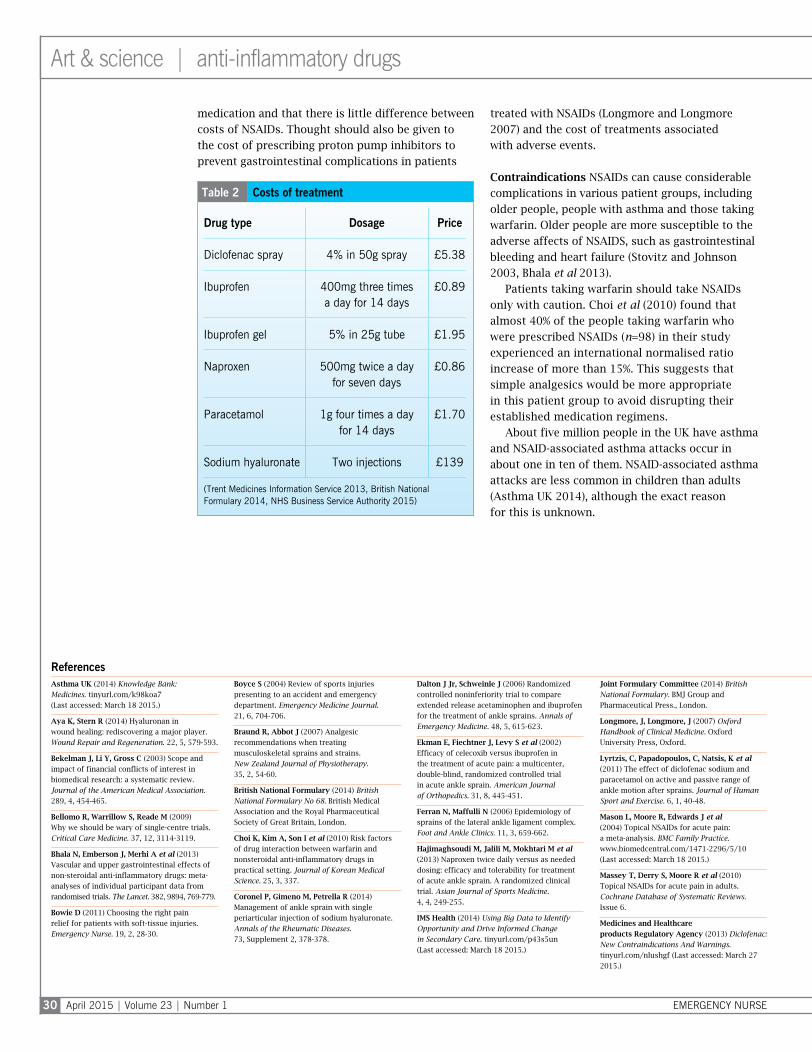
Cost implications Being a major factor in prescribing decisions, costs must be considered when assessing potential benefits and risks (Prosser and Wally 2005). The costs of treatment of a range of drugs are shown in Table 2 (page 30).
Diclofenac topical spray and ibuprofen gel are included in the table for purposes of comparison, and to illustrate the growing cost of topical medications (Massey et al 2010). The table shows that paracetamol is the most expensive oral
April 2015 | Volume 23 | Number 1 EMERGENCY NURSE30
Art & science | anti-inflammatory drugs
medication and that there is little difference between costs of NSAIDs. Thought should also be given to the cost of prescribing proton pump inhibitors to prevent gastrointestinal complications in patients
treated with NSAIDs (Longmore and Longmore 2007) and the cost of treatments associated with adverse events.
Contraindications NSAIDs can cause considerable complications in various patient groups, including older people, people with asthma and those taking warfarin. Older people are more susceptible to the adverse affects of NSAIDS, such as gastrointestinal bleeding and heart failure (Stovitz and Johnson 2003, Bhala et al 2013).
Patients taking warfarin should take NSAIDs only with caution. Choi et al (2010) found that almost 40% of the people taking warfarin who were prescribed NSAIDs (n=98) in their study experienced an international normalised ratio increase of more than 15%. This suggests that simple analgesics would be more appropriate in this patient group to avoid disrupting their established medication regimens.
About five million people in the UK have asthma and NSAID-associated asthma attacks occur in about one in ten of them. NSAID-associated asthma attacks are less common in children than adults (Asthma UK 2014), although the exact reason for this is unknown.
Asthma UK (2014) Knowledge Bank: Medicines. tinyurl.com/k98koa7 (Last accessed: March 18 2015.)
Aya K, Stern R (2014) Hyaluronan in wound healing: rediscovering a major player. Wound Repair and Regeneration. 22, 5, 579-593.
Bekelman J, Li Y, Gross C (2003) Scope and impact of financial conflicts of interest in biomedical research: a systematic review. Journal of the American Medical Association. 289, 4, 454-465.
Bellomo R, Warrillow S, Reade M (2009) Why we should be wary of single-centre trials. Critical Care Medicine. 37, 12, 3114-3119.
Bhala N, Emberson J, Merhi A et al (2013) Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. The Lancet. 382, 9894, 769-779.
Bowie D (2011) Choosing the right pain relief for patients with soft-tissue injuries. Emergency Nurse. 19, 2, 28-30.
Boyce S (2004) Review of sports injuries presenting to an accident and emergency department. Emergency Medicine Journal. 21, 6, 704-706.
Braund R, Abbot J (2007) Analgesic recommendations when treating musculoskeletal sprains and strains. New Zealand Journal of Physiotherapy. 35, 2, 54-60.
British National Formulary (2014) British National Formulary No 68. British Medical Association and the Royal Pharmaceutical Society of Great Britain, London.
Choi K, Kim A, Son I et al (2010) Risk factors of drug interaction between warfarin and nonsteroidal anti-inflammatory drugs in practical setting. Journal of Korean Medical Science. 25, 3, 337.
Coronel P, Gimeno M, Petrella R (2014) Management of ankle sprain with single periarticular injection of sodium hyaluronate. Annals of the Rheumatic Diseases. 73, Supplement 2, 378-378.
Dalton J Jr, Schweinle J (2006) Randomized controlled noninferiority trial to compare extended release acetaminophen and ibuprofen for the treatment of ankle sprains. Annals of Emergency Medicine. 48, 5, 615-623.
Ekman E, Fiechtner J, Levy S et al (2002) Efficacy of celecoxib versus ibuprofen in the treatment of acute pain: a multicenter, double-blind, randomized controlled trial in acute ankle sprain. American Journal of Orthopedics. 31, 8, 445-451.
Ferran N, Maffulli N (2006) Epidemiology of sprains of the lateral ankle ligament complex. Foot and Ankle Clinics. 11, 3, 659-662.
Hajimaghsoudi M, Jalili M, Mokhtari M et al (2013) Naproxen twice daily versus as needed dosing: efficacy and tolerability for treatment of acute ankle sprain. A randomized clinical trial. Asian Journal of Sports Medicine. 4, 4, 249-255.
IMS Health (2014) Using Big Data to Identify Opportunity and Drive Informed Change in Secondary Care. tinyurl.com/p43s5un (Last accessed: March 18 2015.)
Joint Formulary Committee (2014) British National Formulary. BMJ Group and Pharmaceutical Press., London.
Longmore, J, Longmore, J (2007) Oxford Handbook of Clinical Medicine. Oxford University Press, Oxford.
Lyrtzis, C, Papadopoulos, C, Natsis, K et al (2011) The effect of diclofenac sodium and paracetamol on active and passive range of ankle motion after sprains. Journal of Human Sport and Exercise. 6, 1, 40-48.
Mason L, Moore R, Edwards J et al (2004) Topical NSAIDs for acute pain: a meta-analysis. BMC Family Practice. www.biomedcentral.com/1471-2296/5/10 (Last accessed: March 18 2015.)
Massey T, Derry S, Moore R et al (2010) Topical NSAIDs for acute pain in adults. Cochrane Database of Systematic Reviews. Issue 6.
Medicines and Healthcare products Regulatory Agency (2013) Diclofenac: New Contraindications And Warnings. tinyurl.com/nlushgf (Last accessed: March 27 2015.)
References
Table 2 Costs of treatment
Drug type Dosage Price
Diclofenac spray 4% in 50g spray £5.38
Ibuprofen 400mg three times a day for 14 days
£0.89
Ibuprofen gel 5% in 25g tube £1.95
Naproxen 500mg twice a day for seven days
£0.86
Paracetamol 1g four times a day for 14 days
£1.70
Sodium hyaluronate Two injections £139
(Trent Medicines Information Service 2013, British National Formulary 2014, NHS Business Service Authority 2015)
EMERGENCY NURSE April 2015 | Volume 23 | Number 1 31
People with asthma should therefore be made aware that they may experience an NSAID-associated asthma attack. However, NICE (2012) states that ‘unless NSAIDs clearly cause severe exacerbations of asthma, people with asthma should not be denied the benefits of NSAIDs’.
NSAIDs should also be used with extreme caution in pregnant women due to their cardiovascular side effects and the risks of abortion (NICE 2012).
ConclusionOver the past five years, research into the use of analgesia and NSAIDs in the management of ankle sprains has increased. However, the value of this research to clinical practice is undermined because much of it is funded by pharmaceutical companies (Bekelman et al 2003).
In addition, much of it was undertaken in countries other than the UK.
Many of these studies show that there is no or little difference between the pain levels experienced by patients given paracetamol and those given NSAIDs, and those that report a benefit in using NSAIDs are backed by pharmaceutical companies. However, it is accepted that COX-1 and COX-2 NSAIDs cause
gastrointestinal and cardiovascular complications in people with asthma, older people and those on warfarin.
While a move towards the use of paracetamol and topical NSAIDs may be costly in the short term, it could prevent or reduce hospital admissions in patients with asthma or those suffering adverse events such as gastric bleeding.
Further research into hyaluronic acid injections is required to determine whether they can improve short- and long-term ankle sprain recovery times in the general population. Given the high cost of the injections, however, they may be reserved for use in specific groups, such as armed forces.
NICE (2012) advocates the use of paracetamol and PRICE as initial treatment for sprained ankle and, until results of the Ridderikhof et al (2013) study are known, it is sensible to continue this regimen with the addition of NSAIDs such as ibuprofen after 48 hours in individuals at low risk of side effects (Stovitz and Johnson 2003).
Topical NSAIDs can also be considered as an alternative or adjunct to paracetamol. Meanwhile, patients with sprained ankle should undertake RICE and be cautioned against returning to normal activities too soon.
Conflict of interestNone declared
Online archiveFor related information, visit our online archive and search using the keywords
Miser W (2006) Finding truth from the medical literature: how to critically evaluate an article. Primary Care: Clinics in Office Practice. doi.org/10.1016/j.pop.2006.09.012
NHS Business Service Authority (2015) Electronic Drug Tariff. tinyurl.com/oykftm7 (Last accessed: March 18 2015.)
National Institute for Health and Care Excellence (2012) Clinical Knowledge Summaries: Sprains and Strains. tinyurl.com/m4m2pqh (Last accessed: March 18 2015.)
Neighbour R (2005) The Inner Consultation. Radcliffe, Oxford.
Petersen E, Irish S, Lyons C et al (1999) Reliability of water volumetry and the figure of eight method on subjects with ankle joint swelling. Journal of Orthopedic Sports Physiotherapy. 29, 10, 609-615.
Petrella R, Ekman E, Schuller R et al (2004) Efficacy of celecoxib, a COX-2–specific inhibitor, and naproxen in the management of acute ankle sprain. Clinical Journal of Sport Medicine. 14, 4, 225-231.
Petrella R, Petrella M, Cogliano A (2007) Periarticular hyaluronic acid in acute ankle sprain. Clinical Journal of Sport Medicine. 17, 4, 251-257.
Petrella M, Cogliano A, Petrella R (2009) Original research: long-term efficacy and safety of periarticular hyaluronic acid in acute ankle sprain. Physician and Sportsmedicine. 37, 1, 64-70.
Predel H, Giannetti B, Seigfried B et al (2013) A randomized, double-blind, placebo-controlled multi centre study to evaluate the efficacy and safety of diclofenac 4% spray gel in the treatment of acute uncomplicated ankle sprain. Journal of International Medical Research. 41, 4, 1187-1202.
Prosser H, Walley T (2005) A qualitative study of GPs’ and PCO stakeholders’ views on the importance and influence of cost on prescribing. Social Science and Medicine. 60, 6, 1335-1346.
Purcell D (2010) Minor Injuries. Churchill Livingstone, Edinburgh.
Ridderikhof M, Lirk P, Schep N et al (2013) The PanAM study: a multi-centre, double-blinded, randomized, non-inferiority study of paracetamol versus non-steroidal anti-inflammatory drugs in treating acute musculoskeletal trauma. BMC Emergency Medicine. 13, 1, 19.
Schepsis A, Busconi B (2006) Sports Medicine. Lippincott Williams & Wilkins, Philadelphia PA.
Slimmon D, Brukner P (2010) Sports ankle injuries: assessment and management. Australian Family Physician. 39, 1, 18-22.
Slatyer M, Hensley M, Lopert R (1997) A randomized controlled trial of piroxicam in the management of acute ankle sprain in Australian regular army recruits: the Kapooka ankle sprain study. American Journal of Sports Medicine. 25, 4, 544-553.
Stovitz S, Johnson R (2003) NSAIDs and musculoskeletal treatment: what is the clinical evidence? Physician and Sportsmedicine. 31, 1, 35-52.
Tatro-Adams D, McGann S, Carbone W (1995) Reliability of the figure-of-eight method of ankle measurement. Journal of Orthopedic and Sports Physical Therapy. 22, 4, 161-163.
Tortora G, Derrickson B (2011) Principles of Anatomy and Physiology. Wiley & Sons, Hoboken NJ.
Trent Medicines Information Service (2012) New Product Bulletin April 2012. tinyurl.com/mpyke5v (Last accessed: March 18 2015.)
Trent Medicines Information Service (2013) Quality, Innovation, Productivity and Prevention DetailAid Support Document. tinyurl.com/ktc7936 (Last accessed: March 18 2015.)
van den Bekerom M, Sjer A, Somford M et al (2014) Non-steroidal anti-inflammatory drugs (NSAIDs) for treating acute ankle sprains in adults: benefits outweigh adverse events. Knee Surgery, Sports Traumatology, Arthroscopy. http://link.springer.com/article/10.1007/s00167-014-2851-6
Waterman B, Belmont P, Cameron K et al (2010) Epidemiology of ankle sprain at the United States military academy. American Journal of Sports Medicine. 38, 4, 797-803.
Weintraub W (2003) Tendon and Ligament Healing. Paradigm Publications, Taos NM.